The Relationship Between the Esophageal Tissue Content of Neurotensin and the Presence or Absence of...
6
Digestive Diseases and Sciences, Vol. 49, No. 1 (January 2004), pp. 42–47 ( C 2004) The Relationship Between the Esophageal Tissue Content of Neurotensin and the Presence or Absence of Esophageal Inflammation ROY DEKEL, MD,* ROBERT E. CARRAWAY, PhD,† COLLEEN GREEN, MS,* and RONNIE FASS, MD* Neurotensin (NT) decreases lower esophageal sphincter pressure and impedes gastric emptying, thus exacerbating gastroesophageal reflux. The aim was to determine the content of esophageal tissue NT in patients with erosive esophagitis compared to those with normal endoscopy with or without abnormal acid exposure. Consecutive patients ( N = 21) with gastroesophageal reflux disease symptoms underwent an upper endoscopy, at which two biopsies from opposite walls were obtained from normal-appearing mucosa. Patients with normal upper endoscopy underwent a pH test. NT tissue content was determined using radioimmunoassay. Six patients had erosive esophagitis, seven normal endoscopy but abnormal acid exposure, and eight both normal upper endoscopy and normal acid exposure. The NT/protein ratio was significantly higher in patients with normal upper endoscopy and normal or abnormal pH test compared to those with erosive esophagitis (8.7 ± 1.4 and 8.0 ± 1.2 vs. 3.8 ± 0.5, respectively; P < 0.01). There was no significant difference in NT/protein ratio in patients with normal upper endoscopy with versus those without abnormal acid exposure ( P = 0.7). There was no correlation between the extent of acid exposure and the NT/protein ratio. We suggest that the lower tissue content detected in patients with erosive esophagitis may represent a local protective mechanism against gastroesophageal reflux. KEY WORDS: neurotensin; esophageal inflammation; gastroesphageal reflux; esophageal tissue. Gastric motility and lower esophageal sphincter (LES) tone are inhibited by neuroendocrine mechanisms that op- erate during food ingestion and are particularly sensitive to fatty foods (1). Neurotensin (NT) is one of several reg- ulatory peptides found in the intestine that are postulated to contribute to the inhibition of motility in the upper di- gestive tract (2). Although found throughout the digestive tract including the esophagus (3, 4), NT is primarily lo- Manuscript received. From *The Neuro-Enteric Clinical Research Group, Section of Gas- troenterology, Department of Medicine, Southern Arizona VA Health Care System and University of Arizona Health Science Center, Tucson, Arizona, and †Department of Physiology, University of Massachusetts Medical School, Worcester, Massachusetts, USA. Address for reprint requests: Ronnie Fass, MD, FACP, FACG, South- ern Arizona VA HealthCare System, 3601 South 6th Avenue (1-111G-1), Tucson, Arizona 85723, USA; [email protected]. calized to endocrine-like cells (N-cells) in the jejunum and ileum (5). The ingestion of fat and the presence of fatty acids in the small intestine are strong stimuli for NT secretion (6, 7). When infused into man, NT decreases LES pressure and inhibits gastric motility, gastric emp- tying, and intestinal motility (4, 8, 9). Additionally, NT stimulates intestinal fluid secretion, exocrine pancreatic secretion, gallbladder contraction, bile acid cycling, and absorption of intestinal lipids (7, 10). Teleologically, these effects appear to optimize conditions for the digestion and absorption of fat; however, they may also facilitate gas- troesophageal reflux. Low LES basal pressure, which is often displayed in patients with severe gastroesophageal reflux disease (GERD), is a predisposing factor for gas- troesophageal reflux. Similarly, delayed gastric emptying has been associated with increased episodes of gastroe- sophageal reflux, potentially by inducing transient LES 42 Digestive Diseases and Sciences, Vol. 49, No. 1 (January 2004) 0163-2116/04/0100-0042/0 C 2004 Plenum Publishing Corporation
Transcript of The Relationship Between the Esophageal Tissue Content of Neurotensin and the Presence or Absence of...

P1: ILT/FFU P2: ILT
PL252-ddas-481448 DDAS.cls January 7, 2004 19:42
Digestive Diseases and Sciences, Vol. 49, No. 1 (January 2004), pp. 42–47 (C© 2004)
The Relationship Between the Esophageal TissueContent of Neurotensin and the Presence or
Absence of Esophageal Inflammation
ROY DEKEL, MD,* ROBERT E. CARRAWAY, PhD,† COLLEEN GREEN, MS,* and RONNIE FASS, MD*
Neurotensin (NT) decreases lower esophageal sphincter pressure and impedes gastric emptying,thus exacerbating gastroesophageal reflux. The aim was to determine the content of esophagealtissue NT in patients with erosive esophagitis compared to those with normal endoscopy with orwithout abnormal acid exposure. Consecutive patients (N= 21) with gastroesophageal reflux diseasesymptoms underwent an upper endoscopy, at which two biopsies from opposite walls were obtainedfrom normal-appearing mucosa. Patients with normal upper endoscopy underwent a pH test. NTtissue content was determined using radioimmunoassay. Six patients had erosive esophagitis, sevennormal endoscopy but abnormal acid exposure, and eight both normal upper endoscopy and normalacid exposure. The NT/protein ratio was significantly higher in patients with normal upper endoscopyand normal or abnormal pH test compared to those with erosive esophagitis (8.7± 1.4 and 8.0± 1.2vs. 3.8± 0.5, respectively;P< 0.01). There was no significant difference in NT/protein ratio inpatients with normal upper endoscopy with versus those without abnormal acid exposure (P= 0.7).There was no correlation between the extent of acid exposure and the NT/protein ratio. We suggestthat the lower tissue content detected in patients with erosive esophagitis may represent a localprotective mechanism against gastroesophageal reflux.
KEY WORDS: neurotensin; esophageal inflammation; gastroesphageal reflux; esophageal tissue.
Gastric motility and lower esophageal sphincter (LES)tone are inhibited by neuroendocrine mechanisms that op-erate during food ingestion and are particularly sensitiveto fatty foods (1). Neurotensin (NT) is one of several reg-ulatory peptides found in the intestine that are postulatedto contribute to the inhibition of motility in the upper di-gestive tract (2). Although found throughout the digestivetract including the esophagus (3, 4), NT is primarily lo-
Manuscript received.From*The Neuro-Enteric Clinical Research Group, Section of Gas-
troenterology, Department of Medicine, Southern Arizona VA HealthCare System and University of Arizona Health Science Center, Tucson,Arizona, and†Department of Physiology, University of MassachusettsMedical School, Worcester, Massachusetts, USA.
Address for reprint requests: Ronnie Fass, MD, FACP, FACG, South-ern Arizona VA Health Care System, 3601 South 6th Avenue (1-111G-1),Tucson, Arizona 85723, USA; [email protected].
calized to endocrine-like cells (N-cells) in the jejunumand ileum (5). The ingestion of fat and the presence offatty acids in the small intestine are strong stimuli for NTsecretion (6, 7). When infused into man, NT decreasesLES pressure and inhibits gastric motility, gastric emp-tying, and intestinal motility (4, 8, 9). Additionally, NTstimulates intestinal fluid secretion, exocrine pancreaticsecretion, gallbladder contraction, bile acid cycling, andabsorption of intestinal lipids (7, 10). Teleologically, theseeffects appear to optimize conditions for the digestion andabsorption of fat; however, they may also facilitate gas-troesophageal reflux. Low LES basal pressure, which isoften displayed in patients with severe gastroesophagealreflux disease (GERD), is a predisposing factor for gas-troesophageal reflux. Similarly, delayed gastric emptyinghas been associated with increased episodes of gastroe-sophageal reflux, potentially by inducing transient LES
42 Digestive Diseases and Sciences, Vol. 49, No. 1 (January 2004)0163-2116/04/0100-0042/0C© 2004 Plenum Publishing Corporation

P1: ILT/FFU P2: ILT
PL252-ddas-481448 DDAS.cls January 7, 2004 19:42
ESOPHAGEAL CONTENT OF NEUROTENSIN
relaxations, the chief pathophysiologic event in GERD(11, 12).
NT induces inflammation, degranulation of mast cells,alteration of blood flow, and an increase in vascular perme-ability (13). Additionally, it stimulates chemotaxis, phago-cytosis, and proliferation of inflammatory cells (14–16).Since NT is present in submucosal and myenteric neurons,as well as mucosal endocrine cells, it can act by autocrine,paracrine, and endocrine mechanisms. NT releases acetyl-choline and substance P, which can mediate or potentiateits effects (17). NT receptor antagonists can inhibit stress-induced (18) and toxin A-induced (19) intestinal mast cellactivation and the associated changes in intestinal perme-ability and secretion of prostaglandin E2 and mucin.
Studies about the role of NT in GERD are scarce andconcentrated solely on serum levels of NT. Perdikis et al.have demonstrated a significantly higher fasting bloodlevel of NT in GERD patients with low LES pressure,compared to GERD patients with normal LES pressure orhealthy controls (20). This finding suggested that serumNT may contribute to the low LES basal pressure seen insome GERD patients. As a group, patients with erosiveesophagitis tend to have a lower LES basal pressure com-pared to patients with nonerosive reflux disease (NERD).Consequently, NT might be an important substance inmediating LES abnormalities that are responsible for theevolution of esophageal mucosal injury. Gadenstatter andcolleagues investigated NT levels in 20 GERD patientsbefore and after laparoscopic Nissen fundoplication and 9healthy controls (21). Serum NT levels were significantlyhigher in the GERD patients compared to the controls. Sixmonths after surgery, serum NT levels returned to normalin the operated patients. Additionally, GERD patients withimpaired esophageal motility (defined as simultaneous, in-effective, or nontransmitted contractions in at least 20% ofswallows) demonstrated a significantly higher serum NTlevel in the fasting state, compared to GERD patients withnormal esophageal motility. This study provides furthersupport for the potential role of NT in GERD, suggestingthat it may be associated with the presence or absence ofassociated esophageal motility abnormalities.
Information about esophageal mucosal NT productionand release in GERD patients could yield important datawith possible therapeutic implications. Nevertheless, thusfar there have been no studies investigating esophagealmucosal NT content in GERD patients.
In the present study, we hypothesized that esophagealmucosal NT content could be altered in GERD. Con-sequently, our aim was to determine the content ofesophageal tissue NT in patients with NERD (normal en-doscopy and abnormal or normal esophageal acid expo-sure) compared to those with erosive esophagitis.
MATERIALS AND METHODS
Patients. Consecutive patients with at least three episodesper week of typical GERD symptoms for a minimum of 3 months,presenting to the Southern Arizona VA Health Care System, Pri-mary Care and GI Clinics as well as GI Laboratory, were en-rolled in the study. All subjects agreeing to participate signed aninformed consent. The Human Subject Committee of the Uni-versity of Arizona approved this study.
Patients were excluded if they were unable to complete 24-hr esophageal pH monitoring, were using NSAIDs or aspirin,had a peptic stricture or duodenal or gastric ulcer on upper en-doscopy, or had a history of upper gastrointestinal surgery, scle-roderma, diabetes mellitus, or other neuropathy, myopathy, func-tional bowel disorder, or any underlying disease or medicationthat may affect LES pressure or delay acid clearance time and ifthey were unable or unwilling to complete all stages of the studyor provide an informed consent.
Subjects underwent an upper endoscopy to assess the presenceof esophageal mucosal injury. During endoscopy, two biopsiesfrom opposite walls were obtained at 10 cm above the esoph-agogastric junction for the purpose of determining tissue NTcontent. Special emphasis was given to obtaining the biopsiesonly from normal-looking mucosa. Thereafter, in those patientswith a normal upper endoscopy ambulatory 24-hr esophagealpH monitoring was carried out to quantify the extent of acidexposure in the distal esophagus.
Based on the results of the upper endoscopy and pH testing,patients were divided into three groups: patients with erosiveesophagitis, patients with no evidence of mucosal damage and anabnormal 24-hr pH test, and patients with no evidence of mucosalinjury and esophageal acid exposure within the normal range.
Upper Endoscopy. After an overnight fast, patients wereplaced in the left lateral position. Sedation was achieved witha combination of midazolam (Roche, Nutley, NJ) and meperi-dine (Sanofi Winthrop, New York). The endoscope (OlympusGIF 100) was inserted via the mouth and into the esophagus.The distal portion of the esophagus was carefully evaluated todetermine the presence of mucosal injury. The stomach and duo-denum were also inspected to exclude possible ulcers. The extentof esophageal mucosal damage was assessed using the modifiedHetzel–Dent grading system (22).
0= normal mucosa (no abnormalities)1= erythema, hyperemia, and/or friability present (no visi-
ble macroscopic erosions)2= superficial ulceration or erosion involving<10% of the
mucosal surface area of the last 5 cm of the esophagealsquamous mucosa
3= superficial ulceration or erosion involving≥10% but<50% of the mucosal surface area of the last 5 cm ofthe esophageal squamous mucosa
4= deep ulceration anywhere in the esophagus or confluenterosions of>50% of the mucosal surface area of the last5 cm of the esophageal squamous mucosa
5= stricture, which is defined as narrowing of the esopha-gus that does not allow easy passage of the endoscopewithout dilation
Grades 0 and 1 were considered diagnostic of nonerosive re-flux disease and Grades 2–4 as erosive esophagitis. Patients withGrade 5 were excluded from the study.
Digestive Diseases and Sciences, Vol. 49, No. 1 (January 2004) 43

P1: ILT/FFU P2: ILT
PL252-ddas-481448 DDAS.cls January 7, 2004 19:42
DEKEL ET AL.
Before obtaining biopsies, the gastroesophageal junction(GEJ) was carefully identified as the most proximal part ofthe gastric folds. Subsequently, using large-capacity biopsy for-ceps, two biopsies from opposite sides were obtained at 10 cmabove the GEJ. The biopsies were obtained strictly from normal-appearing mucosa.
Ambulatory 24-hr Esophageal pH Monitoring. After anovernight fast, a pH probe with a LES identifier (DigitrapperMK III; Medtronics, Minneapolis) was inserted through the nos-tril and into the stomach. The probe was positioned 5 cm abovethe upper margin of the LES and connected to a digital portablerecorder. A reference electrode was attached to the upper chest.Patients were instructed to keep a diary recording meal times,position changes, and time and type of their symptoms. Patientswere encouraged to pursue their normal daily activities and main-tain their usual diet. At the beginning and the end of the study, theelectrode and the system were calibrated in standard solutions ofpH 1 and pH 7. Reflux was defined as pH<4, and reflux time asthe interval until pH is>4. The 24-hr pH test was considered pos-itive when the percentage total time pH<4 was greater than 4.2%(23). Analysis of the recorded data was performed using stan-dard, commercially available computer software (Medtronics).
Determination of Tissue NT Content. Tissue samples werehomogenized in 2.0 ml ice-cold 0.1 N HCl using a Potter–Elvehjem tissue grinder. The lyophilized material was extracted(1 hr) with 1.2 ml ice-cold acid–acetone (made on the same dayby adding 2 ml 0.07 N HCl to 10 ml acetone). After centrifugationin a microfuge (2 min), the supernatant (NT fraction) was placedin a glass tube with 3 ml petroleum ether and the pellet (proteinfraction) was put aside. The upper phase of the NT fraction wasaspirated, the lower phase was placed in a 60◦C water bath toremove acetone, and the remaining water was lyophilized. Theprotein fraction was dissolved in 2.0 ml 0.2 N NaOH and pro-tein concentrations were measured using the Bio-Rad proteindye-binding assay with bovine serum albumin (BSA) as stan-dard. The NT fraction was dissolved in buffer and subjected toradioimmunoassay for NT using antiserum BSA-8 with sensi-tivity to 1 fmol (24).
Statistical Analysis. Results are shown as mean±SE. Com-parison of NT/protein ratio between the groups was performedusing a Studentt test. Additionally, a Pearson product–momentcorrelation coefficient was used to evaluate the association be-tween esophageal acid exposure and NT/protein ratio. AP value<0.05 was considered significant.
RESULTS
Twenty-one patients were enrolled in the study. Sixpatients (six males; mean age, 46.3± 4; range, 35–58)had evidence of erosive esophagitis on upper endoscopy.Seven patients (five males; mean age, 44± 3.6; range,25–54) had normal upper endoscopy but abnormal distalesophageal acid exposure. Eight patients (seven males;mean age, 43.8± 4.1; range, 23–59) had both normalupper endoscopy and normal distal esophageal acidexposure. The results of the pH studies are summarizedin Table 1.
The NT/protein ratio was significantly higher in pa-tients with normal upper endoscopy and normal pH test
TABLE 1. PATIENT DEMOGRAPHICS AND24-HR ESOPHAGEALpHMONITORING RESULTS
NERD
Erosive Normal pH Abnormal pHesophagitis (N= 6) test (N= 8) test (N= 7)
Mean age 46.3± 4 43.8± 4.1 44± 3.6range 35–58 23–59 25–54
Gender (M/F) 6/0 7/1 5/2pH monitoringMean % total N/A 1.8± 0.5 8.0± 0.8*Mean % erect N/A 2.3± 0.6 9.4± 1.9**Mean % supine N/A 0.7± 0.4 5.7± 2***
*P< 0.001; **P< 0.01; *** P< 0.05.Note.NERD, nonerosive reflux disease.
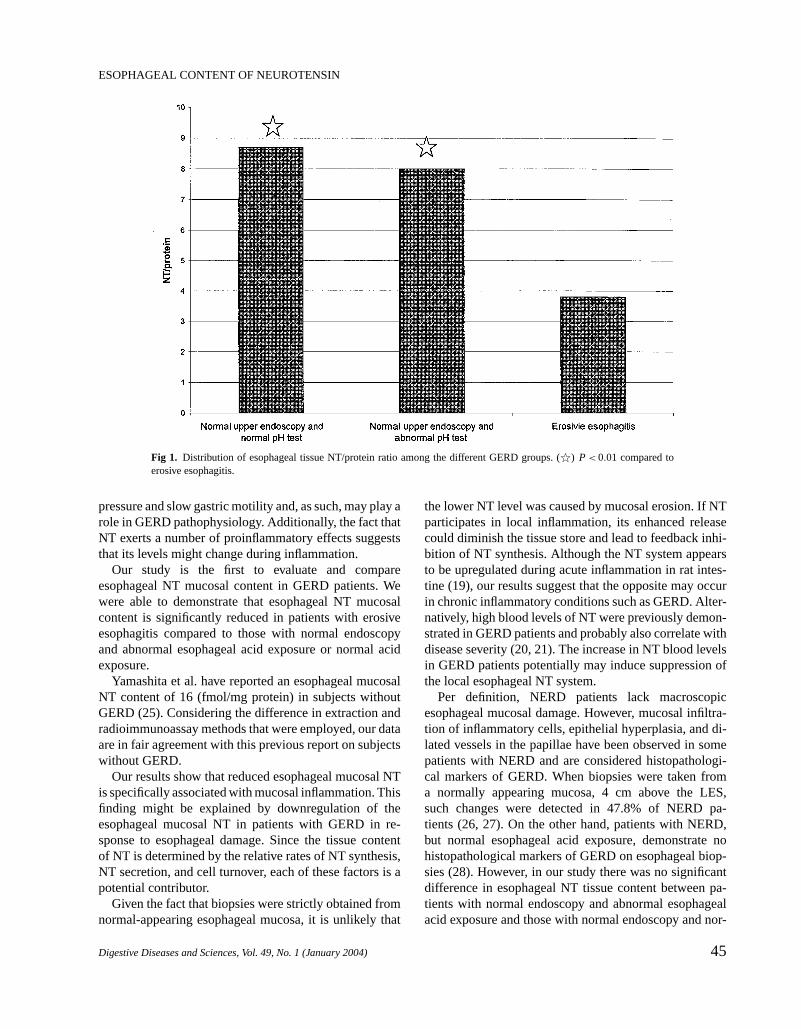
compared to patients with erosive esophagitis (8.7± 1.4vs. 3.8± 0.5, respectively;P< 0.01). Additionally, theNT/protein ratio of patients with normal upper endoscopyand abnormal esophageal acid exposure was also signif-icantly higher compared to the NT/protein ratio of pa-tients with erosive esophagitis (8.0± 1.2 vs. 3.8± 0.5;P< 0.01) (Table 2).
There was no significant difference in NT/protein ra-tio in patients with normal upper endoscopy with versuswithout abnormal esophageal acid exposure. (8.7± 1.4 vs.8± 1.2; P= 0.7) (Figure 1).
No correlation was found between the percentage oftime pH<4 (total, erect, or supine) and the esophagealtissue NT/protein ratio in patients without erosiveesophagitis.
DISCUSSION
NT is a potent neuropeptide with diverse biological ac-tivities in many target organs. In the upper gastrointestinaltract it appears to be associated with decreased LES basal
TABLE 2. NEUROTENSIN/PROTEIN RATIO IN THE DIFFERENTGROUPS
OF GERD PATIENTS
Normal upper Normal upperendoscopy endoscopyand normal and abnormal
Erosive esophageal esophagealesophagitis acid exposure acid exposure(N= 12) (N= 16) (N= 14)
NT (fmol) 1.2± 0.13 3.78± 0.6 3.7± 0.7range 0.75–2.1 1.2–8.3 0.93–9.5
Protein (mg) 0.35± 0.03 0.5± 0.06 0.54± 0.07range 0.14–0.53 0.18–0.94 0.1–0.9
Neurotensin/proteinratio (fmol/mg) 3.8± 0.5 8.7± .4* 8.0± 1.2*
range 1.4–7.0 2.2–21.6 2.2–14.3
Note.Results are mean±SE. N= number of biopsies obtained fromeach group. *P< 0.01.
44 Digestive Diseases and Sciences, Vol. 49, No. 1 (January 2004)
P1: ILT/FFU P2: ILT
PL252-ddas-481448 DDAS.cls January 7, 2004 19:42
ESOPHAGEAL CONTENT OF NEUROTENSIN
Fig 1. Distribution of esophageal tissue NT/protein ratio among the different GERD groups. (q) P< 0.01 compared toerosive esophagitis.
pressure and slow gastric motility and, as such, may play arole in GERD pathophysiology. Additionally, the fact thatNT exerts a number of proinflammatory effects suggeststhat its levels might change during inflammation.
Our study is the first to evaluate and compareesophageal NT mucosal content in GERD patients. Wewere able to demonstrate that esophageal NT mucosalcontent is significantly reduced in patients with erosiveesophagitis compared to those with normal endoscopyand abnormal esophageal acid exposure or normal acidexposure.
Yamashita et al. have reported an esophageal mucosalNT content of 16 (fmol/mg protein) in subjects withoutGERD (25). Considering the difference in extraction andradioimmunoassay methods that were employed, our dataare in fair agreement with this previous report on subjectswithout GERD.
Our results show that reduced esophageal mucosal NTis specifically associated with mucosal inflammation. Thisfinding might be explained by downregulation of theesophageal mucosal NT in patients with GERD in re-sponse to esophageal damage. Since the tissue contentof NT is determined by the relative rates of NT synthesis,NT secretion, and cell turnover, each of these factors is apotential contributor.
Given the fact that biopsies were strictly obtained fromnormal-appearing esophageal mucosa, it is unlikely that
the lower NT level was caused by mucosal erosion. If NTparticipates in local inflammation, its enhanced releasecould diminish the tissue store and lead to feedback inhi-bition of NT synthesis. Although the NT system appearsto be upregulated during acute inflammation in rat intes-tine (19), our results suggest that the opposite may occurin chronic inflammatory conditions such as GERD. Alter-natively, high blood levels of NT were previously demon-strated in GERD patients and probably also correlate withdisease severity (20, 21). The increase in NT blood levelsin GERD patients potentially may induce suppression ofthe local esophageal NT system.
Per definition, NERD patients lack macroscopicesophageal mucosal damage. However, mucosal infiltra-tion of inflammatory cells, epithelial hyperplasia, and di-lated vessels in the papillae have been observed in somepatients with NERD and are considered histopathologi-cal markers of GERD. When biopsies were taken froma normally appearing mucosa, 4 cm above the LES,such changes were detected in 47.8% of NERD pa-tients (26, 27). On the other hand, patients with NERD,but normal esophageal acid exposure, demonstrate nohistopathological markers of GERD on esophageal biop-sies (28). However, in our study there was no significantdifference in esophageal NT tissue content between pa-tients with normal endoscopy and abnormal esophagealacid exposure and those with normal endoscopy and nor-
Digestive Diseases and Sciences, Vol. 49, No. 1 (January 2004) 45

P1: ILT/FFU P2: ILT
PL252-ddas-481448 DDAS.cls January 7, 2004 19:42
DEKEL ET AL.
mal esophageal acid exposure. This finding implies thatoccult inflammation may not be sufficient to induce sup-pression of NT tissue content and that a more extensiveinflammatory process is required. Thus, we suggest thatthe reduction in esophageal NT tissue level may serve asa local protective mechanism in patients with esophagealmucosal injury.
We explored the possibility that the extent of esophagealacid exposure is the determining factor for downregula-tion of NT. However, we found no correlation between dis-tal esophageal acid exposure and mucosal esophageal NTlevels. Thus, it is unlikely that acid is the signal for down-regulation of the NT system. The concept of biochemi-cal adaptation of the esophageal mucosa to injury is notunique to NT. Taurine is an intracellular amino acid con-sidered to have cytoprotective effects. Esophageal taurinelevels were significantly higher in children with GERDcompared to children without GERD (29). In contrast toNT, high taurine levels were found in GERD patients re-gardless of whether esophagitis was present or absent andwere positively correlated with esophageal acid exposure.Thus, gastroesophageal reflux and the ensuing esophagealmucosal injury can initiate biochemical cascades thatare likely to play a role in protecting the esophagealmucosa.
The number of subjects in our study was relatively smallbut the results are statistically significant. Because of therelatively small number of patients with erosive esophagi-tis we were unable to assess a possible correlation betweenthe degree of esophageal inflammation and mucosal NTlevels. Such a correlation would have provided strong sup-port for the hypothesis of inflammation-induced downreg-ulation of NT.
In summary, our study demonstrated for the first timea significantly lower esophageal NT tissue content in pa-tients with erosive esophagitis compared to those withNERD (with or without abnormal acid exposure). Thischange could be primary or secondary to the disease andcould indicate a depleted tissue store due to increasedsecretion or downregulation of esophageal NT synthe-sis. The exact tissue mediators that are involved in thisprocess are yet to be elucidated. Knowing the delete-rious effects of NT on LES basal pressure and gastricmotility, the lower tissue level detected may represent alocal protective mechanism. Alternatively, knowing theNT proinflammatory properties, the downregulation mayfunction to alleviate inflammation. We believe that ourstudy suggests that NT may be an important factor in thepathophysiology of GERD and should serve as an impe-tus for future research on the role of this neuropeptidein GERD.
ACKNOWLEDGMENTS
This study was supported in part by a grant from the Glaxo–Wellcome Institute for Digestive Health (GIADH), a Universityof Arizona Dean’s research award, and AstraZeneca. This studywas presented during the Annual Meeting of the American Gas-troenterological Association (Digestive Disease Week), AtlantaGeorgia, 2001.
REFERENCES
1. Azpiroz F, Malagelada JR: Intestinal control of gastric tone. Am JPhysiol 249:G501–G509, 1985
2. Spiller RC, Trotman IF, Adrian TE, Bloom SR, Misiewicz JJ, SilkDB: Further characterisation of the ‘ileal brake’ reflex in man—Effect of ileal infusion of partial digests of fat, protein, and starchon jejunal motility and release of neurotensin, enteroglucagon, andpeptide YY. Gut 29:1042–1051, 1988
3. Carraway R, Leeman SE: Characterization of radioimmunoas-sayable neurotensin in the rat. Its differential distribution in thecentral nervous system, small intestine, and stomach. J Biol Chem251:7045–7052, 1976
4. Ferris CF: Neurotensin.In Handbook of Physiology. The Gastroin-testinal System. Bethesda, MD, American Physiological Society,1989, pp 559–586
5. Sundler F, Hakanson R, Hammer RA, Alumets J, Carraway R,Leeman SE, Zimmerman EA: Immunohistochemical localization ofneurotensin in endocrine cells of the gut. Cell Tissue Res 178:313–321, 1977
6. Rosell S, Rokaeus A: The effect of ingestion of amino acids, glucoseand fat on circulating neurotensin-like immunoreactivity (NTLI) inman. Acta Physiol Scand 107:263–267, 1979
7. Ferris CF, Hammer RA, Leeman SE. Elevation of plasma neu-rotensin during lipid perfusion of rat small intestine. Peptides 2:263–266, 1981
8. Rosell S, Thor K, Rokaeus A, Nyquist O, Lewenhaupt A, KagerL, Folkers K: Plasma concentration of neurotensin-like immunore-activity (NTLI) and lower esophageal sphincter (LES) pressure inman following infusion of (Gln4)-neurotensin. Acta Physiol Scand109:369–375, 1980
9. Andersson S, Rosell S, Hjelmquist U, Chang D, Folkers K: Inhi-bition of gastric and intestinal motor activity in dogs by (Gln4)neurotensin. Acta Physiol Scand 100:231–235, 1977
10. Gui X, Dobner PR, Carraway RE: Endogenous neurotensin facili-tates enterohepatic bile acid circulation by enhancing intestinal up-take in rats. Am J Physiol Gastrointest Liver Physiol 281:G1413–G1422, 2001
11. Schwizer W, Hinder RA, DeMeester TR: Does delayed gastric emp-tying contribute to gastroesophageal reflux disease? Am J Surg157:74–81, 1989
12. Mittal RK, Holloway RH, Penagini R, Blackshaw LA, Dent J:Transient lower esophageal sphincter relaxation. Gastroenterology109:601–610, 1995
13. Carraway R, Cochrane DE, Lansman JB, Leeman SE, Paterson BM,Welch HJ: Neurotensin stimulates exocytotic histamine secretionfrom rat mast cells and elevates plasma histamine levels. J Physiol323:403–414, 1982
14. Goldman R, Bar-Shavit Z, Shezen E, Terry S, Blumberg S:Enhancement of phagocytosis by neurotensin, a newly found biolog-ical activity of the neuropeptide. Adv Exp Med Biol 155:133–141,1982
46 Digestive Diseases and Sciences, Vol. 49, No. 1 (January 2004)

P1: ILT/FFU P2: ILT
PL252-ddas-481448 DDAS.cls January 7, 2004 19:42
ESOPHAGEAL CONTENT OF NEUROTENSIN
15. Moore RN, Osmand AP, Dunn JA, Joshi JG, Koontz JW, Rouse BT:Neurotensin regulation of macrophage colony-stimulating factor-stimulated in vitro myelopoisesis. J Immunol 142:2689–2694,1989
16. De la Fuente M, Garrido JJ, Arahuetes RM, Hernanz A: Stimulationof phagocytic function in mouse macrophages by neurotensin andneuromedin N. J Neuroimmunol 42:97–104, 1993
17. Carraway RE, Mitra SP: Binding and biologic activity of neurotensinin guinea pig ileum. Peptides 15:1451–1459, 1994
18. Castagliuolo I, Leeman SE, Bartolak-Suki E, Nikulasson S, Qiu B,Carraway RE, Pothoulakis C: A neurotensin antagonist, SR 48692,inhibits colonic responses to immobilization stress in rats. Proc NatlAcad Sci USA 93:12611–12615, 1996
19. Castagliuolo I, Wang CC, Valenick L, Pasha A, Nikulasson S,Carraway RE, Pothoulakis C: Neurotensin is a proinflammatory neu-ropeptide in colonic inflammation. J Clin Invest 103:843–849, 1999
20. Perdikis G, Wilson P, Hinger RA, Redmond EJ, Wetscher GJ, SaekiS, Adrian TE: Gastroesophageal reflux disease is associated withenteric hormone abnormalities. Am J Surg 167:186–191, 1994
21. Gadenstatter M, Prommegger R, Klingler A, Schwelberger H, WeissHG, Glaser K, Wetscher GJ: Alterations of gut neuropeptides ingastroesophageal reflux disease are resolved after antireflux surgery.Am J Surg 180:483–486, 2000
22. Hetzel DJ, Dent J, Reed WD, Narielvala FM, Mackinnon M,McCarthy JH, Mitchell B, Beveridge BR, Laurence BH, Gibson GG,et al.: Healing and relapse of severe peptic esophagitis after treat-ment with omeprazole. Gastroenterology 95:903–912, 1988
23. Wiener GJ, Morgan TM, Copper JB, Wu WC, Castell DO, SinclairJW, Richter JE: Ambulatory 24-hour esophageal pH monitoring. Re-producibility and variability of pH parameters. Dig Dis Sci 33:1127–1133, 1988
24. Carraway RE, Mitra SP, Evers BM, Townsend CM Jr: BON cellsdisplay the intestinal pattern of neurotensin/neuromedin N precursorprocessing. Regul Pept 53:17–29, 1994
25. Yamashita Y, Pedersen JH, Hansen CP: Distribution of neurotensin-like immunoreactivities in porcine and human gut. Scand J Gas-troenterol 25:481–488, 1990
26. Lewin KJ, Riddell RH, Weinstein WM: Inflammatory disorders ofthe esophagus, reflux and nonreflux type.In Gastrointestinal Pathol-ogy and Its Clinical Implications. New York, Igaku-Shoin, 1992,pp 401–439
27. Funch-Jensen P, Kock K, Christensen LA, Fallingborg J, KjaergaardJJ, Andersen SP, Teglbjaerg PS: Microscopic appearance of theesophageal mucosa in a consecutive series of patients submitted toupper endoscopy. Correlation with gastroesophageal reflux symp-toms and macroscopic findings. Scand J Gastroenterol 21:65–69,1986
28. Schindlbeck NE, Wiebecke B, Klauser A, Voderholzer WA, Muller-Lissner SA: Diagnostic value of histology in non-erosive gastro-oesophageal reflux disease. Gut 39:151–154, 1996
29. D’Eufemia P, Corrado G, Finocchiaro R, Celli M, Cavaliere M,Troiani P, Tote J, Cardi E, Giardini O: Increased taurine content inesophageal mucosa of children affected by gastroesophageal reflux.Dig Dis Sci 46:808–814, 2001
Digestive Diseases and Sciences, Vol. 49, No. 1 (January 2004) 47