The overall significance of regenerative procedures in the treatment
8
Periodon tics The overall significance of regenerative procedures in the treatment of furcations Hans-Peter Müller*/Thomas Eger** Abstract A retn>speetive sttidy examined the frequency of a feasible or retnotely pos.sible indication for regenerative therapy of furcation involvement in a large group of periodontally diseased patients. The Judgment about thefeasibility of tiie indication was mainly based on results of current randomised controlled chnicai triais with regard to tooth type and iocation of the Jurcation lesion. Data from .i.^S patients treated by nvo periodonti.^ts, one experienced and one in training, were anaiyzed. Furcation involvement of at least one miiltirooted tooth was found in 40% and 63% ofthe two dentists' patients. In oniy 20% and 27% of tiieir patients was there a potetitiai indication for regenerative Jurcation treatment. Of I. ¡34 Jurcation lesions. ¡80 (15.9%) were conceivably suitable for this procedure. Only 17 sites with aj'easible or remotely possible indication were treated in that wax: In tnost cases, conventional furcational treatment (flap surgery- with scaling and root planing) was performed. (Quintessence Int ¡997;28:32l-328.) Clinical relevance One major indication for guided tissue regeneration procedures may be buecal and/or lingual furcation involvement of mandibular molars and buecal in- volvement of maxillary molars, but this type of periodontal lesion is rare, even in a selected population with periodontitis. Introduction Although it is generally accepted that the progression of a periodontal lesion into the interradicular area seriously affects the long-term prognosis of a multi- ' Depanment of Operalivc Dentistry and Periodonlotogy, tJniversity of Heidelberg, Heidelberg, Germany, ** Department of Denlistri', German Armed t-orces Central Hospital. Koblenz, Germany. • Reprint requests: Dr Hans-Peter Müller, Depanment of Operative Demistry and Periodontology, tJniveriity of Heidelberg, Im Neiien- heimer Feld 400, D-69120 Heidelberg, Germany, e mail: hani-peler [email protected],de The opinions e>,pressed in this anicte are Ihose ofthe autliorb and cannoi be conslrued as reileclmg the views of tlie German Armed Forées' Medical Serviee, the German Ariiied Forces at iarge, or ttie German Ministry of Defense, rooted tooth,' '' there is surprisingly little information with regard to the overall prevalence of interradieular periodontitis in a given population, and only a few studies have focused on that topic, ^ Whether furcation involvement plays a significant role in daily practice eleariy depends on the type of clientele referred to and preferred by the dentist. The periodontist will treat more patients with furcation invasions than will a dentist whose main emphasis is on restorative and prosthodontic treatment. A retro- spective analysis was made of treatment modalities of all patients of one of the authors, an experienced periodontist. Of 309 patients treated during 1987 through 1994, 193 (62,5%) presented with at least one furcation invasion. The operator was confronted with similar numbers of ineipient, moderately advanced, and through-and-thro ugh furcation involvements,'' In contrast, of 249 patients treated by the other author during his 3-year postgraduate training program, only 100 (40.2'Ä) had at least one multirooted tooth with interradieular periodontitis. The vast majority of those furcation invasions were diagnosed as being incipient. When the data were analyzed in more detail, it became clear that the treatment pattern of both operators was quite similar; conventional measures, ie, scaling, root planing, and furcation plasty, predomi- Quintessence International Volume 28, Number 5/1997 321
Transcript of The overall significance of regenerative procedures in the treatment
Periodon tics
The overall significance of regenerative procedures in the treatmentof furcations
Hans-Peter Müller*/Thomas Eger**
Abstract A retn>speetive sttidy examined the frequency of a feasible or retnotely pos.sibleindication for regenerative therapy of furcation involvement in a large group ofperiodontally diseased patients. The Judgment about the feasibility of tiie indicationwas mainly based on results of current randomised controlled chnicai triais withregard to tooth type and iocation of the Jurcation lesion. Data from .i.̂ S patientstreated by nvo periodonti.^ts, one experienced and one in training, were anaiyzed.Furcation involvement of at least one miiltirooted tooth was found in 40% and 63%ofthe two dentists' patients. In oniy 20% and 27% of tiieir patients was there apotetitiai indication for regenerative Jurcation treatment. Of I. ¡34 Jurcationlesions. ¡80 (15.9%) were conceivably suitable for this procedure. Only 17 siteswith aj'easible or remotely possible indication were treated in that wax: In tnostcases, conventional furcational treatment (flap surgery- with scaling and rootplaning) was performed. (Quintessence Int ¡997;28:32l-328.)
Clinical relevance
One major indication for guided tissue regenerationprocedures may be buecal and/or lingual furcationinvolvement of mandibular molars and buecal in-volvement of maxillary molars, but this type ofperiodontal lesion is rare, even in a selectedpopulation with periodontitis.
Introduction
Although it is generally accepted that the progressionof a periodontal lesion into the interradicular areaseriously affects the long-term prognosis of a multi-
' Depanment of Operalivc Dentistry and Periodonlotogy, tJniversity ofHeidelberg, Heidelberg, Germany,
** Department of Denlistri', German Armed t-orces Central Hospital.Koblenz, Germany.
• Reprint requests: Dr Hans-Peter Müller, Depanment of OperativeDemistry and Periodontology, tJniveriity of Heidelberg, Im Neiien-heimer Feld 400, D-69120 Heidelberg, Germany, e mail: [email protected],de
The opinions e>,pressed in this anicte are Ihose ofthe autliorb and cannoibe conslrued as reileclmg the views of tlie German Armed Forées'Medical Serviee, the German Ariiied Forces at iarge, or ttie GermanMinistry of Defense,
rooted tooth,' '' there is surprisingly little informationwith regard to the overall prevalence of interradieularperiodontitis in a given population, and only a fewstudies have focused on that topic, ̂
Whether furcation involvement plays a significantrole in daily practice eleariy depends on the type ofclientele referred to and preferred by the dentist. Theperiodontist will treat more patients with furcationinvasions than will a dentist whose main emphasis ison restorative and prosthodontic treatment. A retro-spective analysis was made of treatment modalities ofall patients of one of the authors, an experiencedperiodontist. Of 309 patients treated during 1987through 1994, 193 (62,5%) presented with at least onefurcation invasion. The operator was confronted withsimilar numbers of ineipient, moderately advanced,and through-and-thro ugh furcation involvements,'' Incontrast, of 249 patients treated by the other authorduring his 3-year postgraduate training program, only100 (40.2'Ä) had at least one multirooted tooth withinterradieular periodontitis. The vast majority of thosefurcation invasions were diagnosed as being incipient.
When the data were analyzed in more detail, itbecame clear that the treatment pattern of bothoperators was quite similar; conventional measures, ie,scaling, root planing, and furcation plasty, predomi-
Quintessence International Volume 28, Number 5/1997 321

Müller/Eger
nated by far, even in more advanced eases,^ Boththerapists extracted more than 40% of teeth with athrough-and-through furcation invasion. Regenerativemeasures, such as guided tissue regeneration' orcoronally repositioned and fixed mucoperiostealflaps,** were only rarely employed,''
A number of recent randomized and well-control ledstudies have convincingly indicated that guided tissueregeneration may provide considerable advantage overconventional treatment modalities. Especially in buccaland/or lingual class II itircation involvement of mandib-ular molars'''"' and buccal furcations of maxillarymolars, ' ' better results are to be expected. In contrast,through-and-through furcation involvements.'''-' fur-cation invasions of maxillary premolars,'"* and mesialor distal Ilircation invasions ofmaxiilary molars" '̂ areprobably not very suitable for these technically demand-ing procedures.
There is, at present, no information with regard tothe relative importance of regenerative procedures indaily periodontal practiee, Tlie aim of the presentstudy, therefore, was to detennine the prevalence ofapossible indication, as suggested by the results ofrandomized controlled trials, for a regenerative pro-cedure in the treatment of furcally involved multiroot-ed teeth. The analysis was based on charts of a largenumber of patients treated for periodontal disease bytwo operators mainly engaged in periodontics,^
Method and materialsPatients
The present study was based on retrospectively sampleddata of al! 309 patients treated by one ofthe authors(operator A), an experienced periodontist, during1987 through 1994, and 249 patients treated by theother author (operator B) during his 3-year post-graduate training program. Patients were between 16and 72 years of age and presented with moderatelyadvanced or advanced periodontitis.
Therapy
Patients entered an individual oral hygiene programconsisting of detailed education about the significanceof dental plaque for the development of periodontaldisease and instruction in proper oral hygiene mea-sures, Supragingival and, as far as possible, subgingivalbacterial deposits were earefully removed in a series ofweekly sessions. At multirooted teeth, the degree ofilircation itivolvement was estimated"' with a curved
Nabers' probe (PQ2N, Hu Friedy), Periodontal de-struction of about one third ofthe crown width in theinterradicular region was eonsidered a degree I in-volvement. If more than one third of, but not the entire,interradicular periodontium was destroyed, a degree IIfurcation was diagnosed. If the curved probe could bepassed through and through the furcation entrances,the tooth was eonsidered to have degree III involve-ment,
Periodontal surgery was performed at sites withpersisting periodontal probing depths of 5 mm or moreand bleeding on probing, Fureational lesions weretreated with one ofthe following therapies:
1, Conventional, ie, scahng and root planing and, ifindicated, furcation plasty. employing eurettes,periodontal files, and rotating fine diamonds
2, Resective measures, such as hemisection or rootresection
3, Tunnel preparation4, Regenerative procedures, either guided tissue re-
generation with expanded polytetrafluoroethylene(e-PTEE) membranes^ or coronally repositionedand fixed flaps'
5, Tooth extraction
In general, the actual degree of furcation involve-ment was reevaluated intraoperatively. The presentanalysis was based on ihis second estimate. Supportivecare was scheduled individually, depending on local,tooth-related, and general risk factors," Most patientswere recalled in 2- to 3-month intervals for subgingivalscaling at sites with a periodontal probing depth of5 mm or more and bleeding on probing.
Reasonable indications for regenerative procedures
In the retrospective analysis of the patient data, apossible indication for a regenerative procedure at afureational lesion was assumed in the followingsituations;
1, Buccal and/or lingual degree II ilircation involve-ment of first and second mandibular molars^'*
2. Buccal degree II furcation involvement of first andsecond maxiiiary molars"
The following was considered a remotely possibleindication;
1, Mesiopalatal degree II furcation involvement ofmaxillary molars
The following were considered to have no indica-tion for. or even a contraindication to. regenerativemeasures;
322 Quintessence International Volume 2a, Number 5/1997

MtJller/Eger
L Degree I furcation involvement2. Degree III irivolvement'-"3. Distopalatal degree II involvement of maxillary
molars"'^4. Buecal and/or mesiopalatal degree II furcation
involvement in the presence of degree II involve-ment ofthe distopalatal furcation or a through-and-through involvement between two furcation en-trances
5. Etircation involvement of third molars6. Furcation involvement of maxillary premolars'**
A number of teeth had been extracted in spite ofapossible indication for regenerative treatment. Be-cause, in most ofthese cases, the reason for extractioncould not be determined, a definite contraindicationwas supposed.
Results
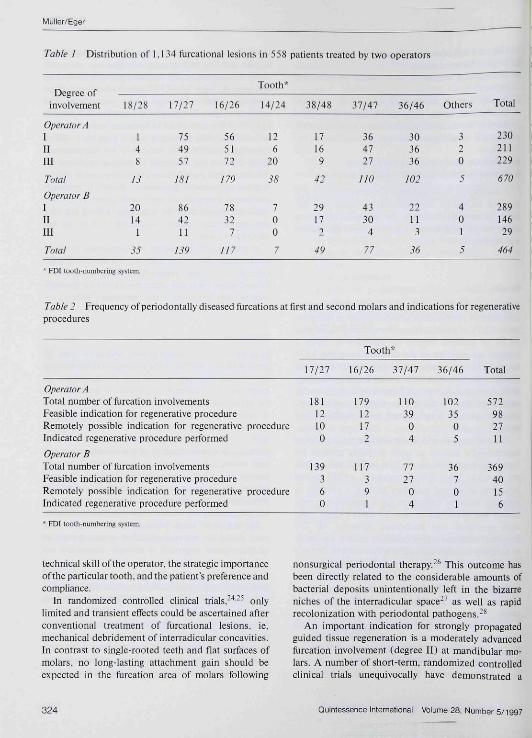
A total of 558 patients had been treated by the twooperators. A periodontitis-affected llircation was pres-ent in 62.5% of paiients treated by operator A, but only40,2% of patients treated by operator B, Table 1presents an overview ofthe distribution ofthe 1,134ftircation lesions treated by the two operators. About62.5% ofthe furcation lesions were found at maxillaryteeth. Operator A was confronted with considerablymore furcation invasions al maxillary premolars,whereas operator B had to treat more maxillary thirdmolars,
Eor operators A and B, the absolute frequencies ofinterradicular lesions at teeth probably suitable forregenerative procedures, ie, first and second molars,are shown in Table 2, Eor operator A. of 181 treatedfurcations at second maxillary molars, a possible orremotely possible indication for a regenerative pro-cedure was identified in only 22 cases (12.2%). Nosuch operation was performed, however. Of 179involved furcations at first maxillary molars, a possibleor remotely possible indication was present in 29 cases( 16,2/ii), but the procedure was only performed twice.In mandibular molars, regenerative measures wereindicated for 35,5% of second molars and 34,3% offu-st molars. The procedures were performed in ninecases.
Of 139 furcation involvements at maxillary secondmolars treated by operator B, nine (6,5%) exhibited apossible or remotely possible indication for a regenera-tive procedure. This operation was, however, not per-formed. The respective figures were 10,3% for maxil-
lary first molars and 35.1% and 19,4% for mandibularsecond and first molars, respectively.
Of 309 periodontally diseased patients treated byoperator A, only 84 (27,2%) had furcation lesionsprobably suitable for regenerative procedures. Therespective figure for operator B was 49 of 249 patients(19,7%), Ofa total of 1,134 furcation lesions treated,only 180 {15.9%) presented with a possible ( 140) orremotely possible (40) indication for regeneration.Table 3 shows the treatment modalities employed forfurcations with a possible or remotely possible indica-tion for regenerative procedures, Resective measuresand tunnel preparations were rarely performed. Con-ventional treatment ofthe furcations (scaling and rootplaning, Utrcation plasty) was carried out in the vastmajority of cases,
A regenerative procedure was performed in 17 in-dicated cases. When the study criteria are strictly con-sidered, in 15 cases a regenerative procedure was per-formed when it was not indicated, mostly for through-and-through furcations in the mandible (Table 4),
Discus.sion
In spite ofthe enormous growth within the past 30years ofthe knowledge ofthe etiology of inflammatoryperiodontal diseases, which has direct impact ondiagnosis and treatment of destructive periodontitis,the appropriate management of interradicular lesionsat multirooted teeth continues to be a major and, byand large, unsolved problem. This is especially true inlight of the rapid development of novel tools formechanical instrumentation ofthe complex root sur-face colonized by microorganisms as well as newperspectives for the regeneration of lost periodontaltissues. As in other areas of modern dentistry, inperiodontics the practitioner is faced with a be-wildering multitude of new methods and techniques.
On the other hand, when newly developed treat-ment modalities are recommended, in recetit years anevidence-based approach is strongly demanded notonly from the public but also from clinicians andscientists both in general medicine and dentistry,'̂ '-"^Different treatment modes for furcation-involved teethand their respective indications have been described inseveral recent publications and modern textbooks onperiodontology,-""-•' Although recommendations seemto depend mostly on the degree of involvement andtooth type, in practice, the decision for one or the othermodality, conventional, resective, or regenerative,seems to be guided by a number of other factors, eg, the
Quintessence International Volume 2B, Number 5/1997 323
Müller/Eger
Table I Distribution of 1.134 furcational lesions in 558 patients treated by two operators
Degree ofinvolvement
Operator A1IIIII
Total
Operator BIUIII
Total
18/28
148
¡3
2014
1
35
17/27
754957
¡81
864211
139
565172
179
7832
7
111
Tooth*
14/24
126
20
38
700
7
38/48
17169
42
29172
49
37/47
364727
HO
4330
4
77
36/46
303636
¡02
22113
Others
320
JÎ
401
5
Total
230211229
670
28914629
464
• FDt looth-numbering syslem.
Table J Frequency of periodontally diseased furcations at first and second molars and indications for regenerativeprocedures
Tooth*
Operator ATotal number of furcation involvementsEeasible indication for regenerative procedureRemotely possible indication for regenerative procedureIndicated regenerative procedure performed
Operator BTotal number of furcation involvementsEeasible indication for regenerative procedureRemotely possible indication for regenerative procedureIndicated regenerative procedure performed
* FDI tooih-numbering system.
Mill
18112100
139360
16/26
1791217
2
117391
37/47
11039
04
1111
04
36/46
10235
05
36701
Tota
572982711
36940156
techtiical skill of the operator, the strategic importanceofthe particular tooth, and the patient's preference andcompliance.
In randomized controlled clinical trials,"*—^ onlylimited and transient effects could be ascertained afterconventional treatment of furcational lesions, ie.mechanical debridement of interradicular concavities.In contrast to single-rooted teeth and flat surfaces ofmolars, no long-lasting attachment gain should beexpected in the furcation area of molars following
[ionsui;gical periodontal therapy.-^ Tbis outcome hasbeen directly related to the considerable amounts ofbacterial deposits unintentionally left in the bizarreniches of the interradicular space-' as well as rapidrecolonization with periodontal pathogens.-^
An important indication for strongly propagatedguided tissue regeneration is a moderately advancedfurcation involvement (degree II) at mandibular mo-lars. A number of short-term, randomized controlledclinical trials unequivocally have demonstrated a
324 Quintessence Intemational Volume 28, Number 5/ig97

M ü 11 er/E ge r
Table 3 Treatment of periodontitis-affected furcations with a feasible or remotely possible indication forregenerative procedures
Tooth*
Operator ATotal number of furcation involvementsScaling/root planing/flircation plastyHemisection/root resectionTunnel preparationRegenerative procedure
Operator BTotal number of ftircation involvementsScaling/root planing/flircation plastyHemisection/root resectionTunnel preparationRegenerative procedure
* FDl toottintimbering system.
17/27
2222
000
99000
16/26
2925
202
1292Ü
4
37/47
3933
!14
2723
004
36/46
3526
135
76001
Tota
1258644
11
5547
206
Table 4 Distribution of nonindicated regenerativeprocedures performed by two operators
involvement
Operator AIIII
Operator BI111
Total
17/27
00
10
/
Tooth*
37/47
13
00
4
36/46
19
00
10
Total
212
10
¡5
' FDT tooth numbering system.
distinct short- and probably long-term-" advantage ofregenerative procedures over conventional therapy.'̂ "'*'On the other hand, at maxillary molars, a morebeneficial effect is obtained only at buccal, but notmesial or distal, degree II furcations."'^ Also, nodiscernable advantage is apparent in infrabony pocketsaround maxillary premolars.''' Thus, in the presentstudy, the most feasible indications for regenerativeftircation therapy were considered to be degree IIinvolvement of mandibular molars and buccal degreeII involvement of maxillary first and second molars.
A remotely possible indication was a mesiopalataldegree II furcation involvement in maxillary molars.This, however, could not entirely be substantiated fromthe current literature. In a limited number of randomizedcontrolled clinical trials dealing with the regenerativetreatment of maxiilary molar flircations, no advantageor no clinically relevant advantage over conventionalmeasures was ascertained."'^ This (remotely possible)indication was therefore based on the impression ofthe authors that a mesiopalatal, in sharp contrast to thedistopalatal, Ilircation may allow effective instrumenta-tion of root concavities. It should be noted, however,that no such procedure was actually performed by theauthors.
Furcation involvement of third molars and maxillarypremolars were generally disregarded as indicationsfor regenerative therapy. Nevertheless, there might becircumstances where regenerative procedures shouldbe kept in mind for an attempt to improve long-termprognosis of a particular tooth of strategic importance.
In recent years, a number of attempts have beenmade to stabilize the wound area and allow periodon-tal regeneration, even in mandibular degree III furca-tions,'- "'" sometimes by employing citric acid condi-tioning and/or decalcified freeze-dried bone allograftsin combination with e-PTFE membranes or coronallyrepositioned fiaps.-"''- From the results of thesestudies it may be concluded that, in certain cases,especially with a small area ofthe furcation entrance,'^
Quintessence International Volume 28, Number 5/1997X
325

Müller/Eger
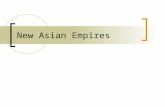
Fig 1a (¡eft) A highly standardized ver-tical bite-wing radiograph with occlusalimpressions reveals a through-and-through furcation involvement at tooth46. Atter thorough rootdebridement, thefiap was coronaiiy repositioned, andsutures were fixed at the crown of thetooth with resin
Fig 1b (righiJAverticalbite-wingradio-graph taken after 6 months revealscompiete closure. Ciinicaiiy, no furca-tion invoivement couid be probed.
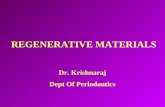
Fig 2a (left) A vertical bite-wing radio-graph reveáis a furcation lesion at toofh36. Clinically, a buecal degree li furca-tion was present. Foilowing debride-ment, an e-PTFE membrane was piaced
Fig 2b frighfj A vertical bite-wing radio-graph taken alter 7 months revealsalmost compiete ciosure Clinically, thelesion was converted to a class I in-voivement.
some degree of closure of mandibular degree IIIftircations might occur. However, at present, thereseems to be no procedure that provides any predictableresult. In the present study, regenerative procedures atdegree III furcations were performed in 12 easestreated by operator A before 1990 (sec Tahle 4),
Figures la and lb demonstrate a case in which theprocedure (coronally repositioned and fixed flap)
resulted in closure ofthe degree III furcation of toolh30 (46), A buecal degree II furcation at tooth 19 {36}in the same patient was treated with an e-PTFEmembrane and displayed partial closure after 7 months(Figs 2a and 2b),
The present study, based on data aequired in morethan 550 periodontitis parients, should reveal howoften a reasonable indication for regenerative furcation
326 Quintessence International Volume 28, Number 5/1997

fvl ulier/Eg er
treatment aetually occurred. This seemed to be the casein only 20% and 27% ofthe two clinicians" patients. Ofmore than 1,100 periodontally involved furcations, anindication for a regenerative procedure was found in15.9%, When other major limitations with regard toindication are considered, such as questionable stra-tegic importance of the particular tooth.*" insufficientcompliance ofthe patient, or excessive smoking'-̂ -"^ aswell as local factors such as the location ofthe gingivalmargin in relation to the llireation entrance, themorphology of the defect.'' the interproximal boneheight, or the height and concavity ofthe root trunk,this figure would have been llirther decreased. Theoperators performed an indicated regenerative pro-eedure in only 17 cases total ( 9,4% of all 180 furcationswith a feasible or remotely possible indication). Basedon the rather strong criteria inferred from the currentliterature, another 15 regenerative operations were notindicated.
The present results showed that regenerative treat-ment of periodontally involved furcations is indicatedin relatively rare instances, even in a mainly periodontitis-afFected patient population. Considering the numer-ous open questions regarding, eg, the superiority ofnewly developed, biodegradable barriers.^^"'^ alter-native regenerative procedures,̂ ^•'"* long-term progno-5J5̂ 29,.í3,4i g|._ Qj- utmost importance, the quality andfimctional capacity of the regenerated tissue.''-''^regenerative procedures should not be regarded asroutine operations for use in daily periodontal prac-tiee. Further studies should determine the overallelinieal relevance of other potential indications forregenerative procedures, such as inirabony pocketsand gingival recession.
References
1, Hirichfeld L, Wasserman BA. A longtem: survey of tooth Ios5 in 600Ireaied periodontal patients J Periodomol 1978;49:225-2."J7.
2, McFali WT. Tooth loss in 100 treated patients with periodontaldisease J Period onto I I983;í3;539-549,
3, Goldman MJ, Ross IF, GoteinerD, Effect of periodontal therapy onpatients maintained for 15 years or longer. A retrospective study JPeriodonrol I9S6;57J47-,i;3,
*. Wang HL, Burgett FG, Shyr Y, Ramfiord S. The influence of molarfurcation involvement and mobiiity on future clinical periodontalattachment lois. J Periodonlol l994;65:25-29.
5. Larato DC, Furcation involvements; Incidence and distribution, JPeriodontol 1970i46;499-50i.
6. Múiler ¡IP, Eger T, Large DE. Management of furcation^invoivedteeth, A retrospective anaijïis. J Ciin Periodontol Í995;22:9i 1-917,
7. Ponloriero R, Lindhe J, Nyman S, KarringT, Rosenberg E, Sanavi FGuided tissue regeneration in degree II furcation-involved mandib-uiar molars. A dinicai study J Clin Periodontol l988;l3i247-254.
8, Manin M, Gatites B, Garrett S, Egelberg J, Treatment of periodontalfijteation defects, I, Review ofthe literature and description ofaregenerative surgical technique, J Clin Periodontol 1988-15 227-231,
9. Lekovic V, Kenney EB, Kovacevic K., Carranza FA, Evaluation ofguided tissue regeneration in ciass II furcation defects. A clinicaire-entry study J Periodontoi 1989:60:694-698,
10. Mellonig JT, Seamons BC, Gray JL, Towie MJ, Ciinical evaluation ofguided tissue regeneration in ihe treatment of grade 11 moiarfurcation invasions. Int J Periodont Resl Dent Í994;l4:355-27i.
11. Pontonero R, Lindhe J. Guided tissue regeneration in the treatmentof degree 11 furcations in maxiiiary molars, J Ciin Periodoiitoi1995:22:756-763.
12. Pontoriero R, Lindhe J, Nyman S, Karring T, Rosenberg E. Sanavi F,Guided tissue regeneration in the treatment of furcation defects inmandibuiar molars, A clinical study of degree [II invoivemenls. JClin Penodontol Í989;I6:Í7O-I74,
13. Ponloriero R, Lindhe J. Guided tissue regeneration in the treatmentof degree III fijrcation defects in maxillary molars. J Chn Period-ontoi 1995:22:810-812.
14. Proestakis G, Bratthail G, Söderhoim G, Kullendorff B, GrondahiK, Rohlin M, Attsirom R, Guided [issue regeneration in thetreatment of infrabony defects on maxiiiary premolars A piiot study,J Ciin Periodontol 1992:19:756-773,
15. Metzler D, Seamons BC, Meiionig JT, Marlin GE, Gray JL. Clinicalevaluation of guided tissue regeneration in the treatment of maxiilarj'ciass ¡I moiar furcation invasions. J Periodontoi 1991:63:353-360.
16 Hamp SE, Nyman S. Treatment of furcation-involved teeth. In:Lindhe J (edl. Textbook of Clinicai Periodontology, ed 2, Copenha-gen: Munksgaard, 1989:515-533.
17, Lang NP, Tonelti MS. Periodontal diagnosis in treated periodontitis.Why, when and how to use clinical parameters, J Clin Periodontol1996:23.240-250,
18, Hujoel PP, Deñouen TA, A survey of endpoint characteristics inperiodontal clinical trials published 1988-1991, and implicatiotisfor future studies. J Clin Periodontoi Í995;23:397-4O7.
19. Egeiberg J, Peri odontics-The Scientific Way, Synopses of HumanClinical Studies, ed 2. Malmo, Sweden: Odonto Sei ence, 1995.
20. McGuire MK, Newman MG. Whitley N. Evidence-based period-ontal regenerative therapy, Curr Opin Periodontol 1996:3:109-117,
21, Rateitschak KH, Rateiischak EM, Wolf HF Color Atlas ofPeriodontology Stuttgart: Thieme, i985:22l-227.
22. Basaraba N, Furcation invasions. In: Schluger S, Yuodelis R, PageRC, Johnson RH (eds) Periodontal Diseases, ed 2, Philadelphia:Lea & Febinger, I99O-54Í-559.
2.1. CarnevaleG, Pontoriero R, HürzelerMB, Management of furcationinvolvement. In: Caffesse RG, Quiñones CR (eds¡. Surgical,nonsurgicai, occlusal and flircation therapies. Periodontology 2000I995;9 69-K9.
24. Kalkwarf KL, Kaldahl WB, Patil KD, Evaluation offurcation regionresponse to periodontal therapy. J Penodontol 1988:59:794-804,
25. Schroer M, Kirk C, Wahl T Hutchens L, MoriartyJ, Bergenholtz B,Closed versus open debridementoffacial grade ¡I molar furcations, JClin Periodontol l99l;l8:323-329.
26. Nordland R Garrett S, Kiger R, Vanooteghe R, Hutchens LH,Egelberg J. The effect of plaque control and root debridement inmolar teeth, J Clin Periodontol I9K7; 14:231-236,
27. FleischerHC, Mellonig JTBrayerWK, Gray JL.BarnettJD. Sealingand root planing elTieacy in muilirooled teeth, J Periodontoi1989:60:402-409,
28. Loos B, Nylund K, Claffey N, Egelberg J. Cünicai effects of rootdehridement in moiar and nonmolar teeth. A 2-year foiiow-up. JClin Periodontoi I989;I6:498-5O4,
Quintessence International Volume 28, Number 5/1997V
327
Muller/Eger
29. Maehtei E t , Grossi SG, Dunford R, Zambón JJ, Genco RJ,Longterm smbilily ol"class II furcmion detecti treated with barriermembranes. J Periodontol 1996;67;i23-527,
30. Becker W, Becker BE, Prieharil JF, Catresse R, Rosenberg E. Newattaehnient after treatment with root isolation procedures: reporLsfoi treated class [II and class II liircalions and vertical osseousdefects, Ini J Periodont Rest Dent I988;8I3):9-2.1,
. l i . Gantes BG, Synowsfci BN, Garrett S, Egelberg JH, Treatment ofperiodonlal furcation defects, Mandibuiar class 111 defects. JPeriodontoi I99I;63;J6I-J65.
32, Garrett S, Gantes B, Zimmerman O, Egelberg J. Treatment ofmandibular eiass 111 penodontal furcation delects. Coronally posi-tioned flaps with and withoul e PTFE membranes, J Periodontoit994;65:59:-597.
3-1. Cortellini P, Pini Prato GP, Toneni MS, Longterm stabiiity ofclinical attachment following guided tissue regeneration and conven-tional therapy. J Clin Periodontoi I996;23:IU6-I11.
34, Tonetti MS, Pini Prato G, Cortellini P. Effect of cigarette smokingon periodontal healing foiiowing GTR in infrabony defects, Apreliminary retrospective study, J Clin Periodontoi 1995i22:239-
35, Tarnow D, Retcher P Classification ofthe vertical component offurcation involvement. J Periodontoi I984;55,283-284.
36, Hugoson A, Ravald N, Fornell J, Johard G, Teiwik A, Gottlow J,Treatment of class II llircatiün involvements ¡n humans withbioresorbable and nonresorbablc guided tissue regeneration bar-riers. A randortiized multicenter study, J Penodontoi l995-6(ifi24-634,
37, BeckerW,BeckerBE,MeUonigJ,CaffesseRG.WarrerK,,CatonJG,Reid T. A prospective multicenter study evaluating periodontoiregeneration for class I I titrcation invasions and intrabony defectsafter treatment witii a bioabsoibable barrier membrane: 1-yearresults, J Periodontoi 1996;67:641-649,
38, Yuktia CN, Yukna RA, Multicenter evaluation of bloabsorbableeoUagen membrane for guided tissue regeneration in human class IIíijrcatiüns, J Periodontoi 1996;67:650-657.
anza FA, Martignom M, The use ofs barriers for the treatment of class 11;r molars. J Periodontoi I99I;61:775-
39. Lekovic V, Kcnney FB, Caiautogenous periosteal graftsfurcation involvements in io«7S0,
40. Bouchard P. Ouhayoun JP, Nilveus RF. Expanded poiytetrafluor-ethylene membranes and connective tissue gratis support boneregeneration for closing mandibular cias5 II furcations. J Periodon-toi 1993;64:M9-3I1!)8,
41. Weigd C, Bragger U, tiammerle CHF, Mombelli A, Lang NPMaintenance of new attacliinent 1 and 4 years following guidedtissue regeneration (GTR), J Chn Periodontoi 1995;22:66l-669.
42. SchroederHE. Biological problems of regenerative cementogenesis;Synthesis and attachment of coliagcnous matrices on growing andestablished root surfaces, Int Rev Cytol Í992J4?: 159,
43. Araûjo M. Betglundh T, Lindhe J, The penodontal tissues in healeddegree III tlircation defects. An expérimentai study in dogs, J ClinPeriodontoi 1996;33:5_12-54i. D
inimally InvasiveRestorations With BondingEdited by Midiel Degrange, DCD, DSO, DEOand jean-Erançois Roulet. Prof Dr Med Dent
THIS BOOK REVIEWS the state of theart in adhesive materials and tech-niques for restorative dentistry, empha-sizing their fole in minimizing the lossof sound tooth structure and improvingesthetics.
Direct and indirect composites andbonded ceramic restorations are coveredin depth, including recent developmentsin ceramic honding and high-strengthceramics based on alumina. Chapterson resin-bonded fixed partial denturesgive a complete and up-to-date surveyof the subject. Indications, design,effectiveness, reliabihty, and longevityare discussed, along with avoiding fail-ures and criteria for choosing betweenthe resin-bonded bridge and the single-tooth implant,
280 pp;.̂ 57 illus (263 color);ISBN 0-8671S-327-X;US$98
To Order
Call Toll Free 1-800-621-0387or Fax 1-630-682-3288
Quintessence Publishing Co, Inc boah/328