The Multifunctional Value of Sunscreen-containing Cosmetics
8
Indexed by the US National Library of Medicine and PubMed Volume 16 • Number 7 • July-August 2011 ALSO IN THIS ISSUE: Practical Application of Genomics to the Development of a Topical Cosmetic Anti-aging Regimen (page 4) & Update on Drugs (page 8) Sunscreens are perceived as gooey, sticky, uncomfortable products that are difficult to apply and distasteful to wear. This accounts for dismal compliance when dermatologists ask patients to use daily sunscreen. Since the time delay between accumulated sun exposure and skin cancer can be more than 20 years, patients do not receive a short-term benefit from photoprotection. Any marketing genius will tell you that compliance requires both self-perceived short- and long-term benefits in order to reinforce positive behavior. This insight into the human psyche led skin care companies to develop the concept of the “multifunctional cosmetic,” which by definition delivers several benefits in one bottle. Currently, popular multifunctional cosmetics include sunscreen-containing moisturizers and facial foundations. Sunscreen-containing Moisturizers Sunscreen-containing moisturizers have dramatically improved photoprotection compliance. These products can provide moisturization by decreasing transepidermal water loss through creation of an environment that is optimal for barrier repair. Through the use of occlusive agents such as dimethicone, petrolatum, and mineral oil, as well as the use of humectants such as glycerin, propylene glycol, and hyaluronic acid, a therapeutic moisturizer can aid in the restoration of the corneocyte and intercellular lipid organization. In addition, a sunscreen- containing moisturizer can deliver effective ultraviolet B (UVB) and ultraviolet A (UVA) photoprotection, thereby contributing to the prevention of sunburn, photoaging, and skin cancer simultaneously. Through the inclusion of active ingredients such as retinol, niacinamide, and/or green tea, additional antiaging benefits may be achieved. In short, one bottle of sunscreen- containing moisturizer can be designed to moisturize the skin, repair the barrier, stop sunburn, prevent skin cancer, minimize photoaging, and potentially reverse oxidative insults. Most sunscreen-containing moisturizers are formulated at a sun protection factor (SPF) between 15 to 30. SPF 15 products can be designed with little UVA photoprotection and they may or may not be labeled as broad spectrum. SPF 30 products must contain both UVB and UVA photoprotective ingredients and are therefore preferred. This logic encouraged the American Academy of Dermatology to restate its sun protective recommendations and raise the minimum recommended SPF to 30. For most formulations, SPF 30 is a nice compromise between photoprotection and aesthetics. Once the SPF raises much above 30, the product becomes sticky. Many highly effective sunscreen filters, such as octocrylene, are thick oils and increasing their concentration in the final formulation leads to poor aesthetics. 1 Yet, for casual limited sun exposure, SPF 30 provides excellent daily photoprotection. 2 Sunscreen-containing Facial Foundations If a sunscreen-containing moisturizer is tinted to match the skin, it can then be classified as a facial foundation. Facial foundations are another category of multifunctional cosmetics that can be helpful in encouraging sun protection compliance. There are four basic facial foundation formulations: oil-based, water-based, oil- free, and water-free forms. The most popular facial foundations are liquid oil-in-water emulsions containing a small amount of oil in which the pigment is emulsified with a relatively large quantity of water. The primary emulsifier is usually a soap, such as triethanolamine or a nonionic surfactant. The secondary emulsifier, present in smaller quantity, is usually glyceryl stearate or propylene glycol stearate. The Multifunctional Value of Sunscreen-containing Cosmetics Zoe Diana Draelos, MD Department of Dermatology, Duke University School of Medicine, Durham, NC, USA ABSTRACT Cosmetic products containing ultraviolet light filtering agents are rapidly being developed and entering the marketplace. These advanced multifunctional formulations are intended to deliver both cosmetic and protective benefits. Herein, a brief discussion is presented of newer preparations and their features, as well as how their formulary attributes may contribute to improving photoprotection by encouraging adherence. Key words: cosmetics, photoprotection, SPF, sun protection factor, sunscreen, UV, ultraviolet light
Transcript of The Multifunctional Value of Sunscreen-containing Cosmetics
I n d e x e d b y t h e U S N a t i o n a l L i b r a r y o f M e d i c i n e a n d P u b M e dV o l u m e 1 6 • N u m b e r 7 • J u l y - A u g u s t 2 0 1 1
ALSO IN THIS ISSUE: Practical Application of Genomics to the Development of a Topical Cosmetic Anti-aging Regimen (page 4) & Update on Drugs (page 8)
Sunscreens are perceived as gooey, sticky, uncomfortable products that are difficult to apply and distasteful to wear. This accounts for dismal compliance when dermatologists ask patients to use daily sunscreen. Since the time delay between accumulated sun exposure and skin cancer can be more than 20 years, patients do not receive a short-term benefit from photoprotection. Any marketing genius will tell you that compliance requires both self-perceived short- and long-term benefits in order to reinforce positive behavior. This insight into the human psyche led skin care companies to develop the concept of the “multifunctional cosmetic,” which by definition delivers several benefits in one bottle. Currently, popular multifunctional cosmetics include sunscreen-containing moisturizers and facial foundations.
Sunscreen-containing MoisturizersSunscreen-containing moisturizers have dramatically improved photoprotection compliance. These products can provide moisturization by decreasing transepidermal water loss through creation of an environment that is optimal for barrier repair. Through the use of occlusive agents such as dimethicone, petrolatum, and mineral oil, as well as the use of humectants such as glycerin, propylene glycol, and hyaluronic acid, a therapeutic moisturizer can aid in the restoration of the corneocyte and intercellular lipid organization. In addition, a sunscreen-containing moisturizer can deliver effective ultraviolet B (UVB) and ultraviolet A (UVA) photoprotection, thereby contributing to the prevention of sunburn, photoaging, and skin cancer simultaneously. Through the inclusion of active ingredients such as retinol, niacinamide, and/or green tea, additional antiaging benefits may be achieved. In short, one bottle of sunscreen-containing moisturizer can be designed to moisturize the skin,
repair the barrier, stop sunburn, prevent skin cancer, minimize photoaging, and potentially reverse oxidative insults.
Most sunscreen-containing moisturizers are formulated at a sun protection factor (SPF) between 15 to 30. SPF 15 products can be designed with little UVA photoprotection and they may or may not be labeled as broad spectrum. SPF 30 products must contain both UVB and UVA photoprotective ingredients and are therefore preferred. This logic encouraged the American Academy of Dermatology to restate its sun protective recommendations and raise the minimum recommended SPF to 30. For most formulations, SPF 30 is a nice compromise between photoprotection and aesthetics. Once the SPF raises much above 30, the product becomes sticky. Many highly effective sunscreen filters, such as octocrylene, are thick oils and increasing their concentration in the final formulation leads to poor aesthetics.1 Yet, for casual limited sun exposure, SPF 30 provides excellent daily photoprotection.2
Sunscreen-containing Facial FoundationsIf a sunscreen-containing moisturizer is tinted to match the skin, it can then be classified as a facial foundation. Facial foundations are another category of multifunctional cosmetics that can be helpful in encouraging sun protection compliance. There are four basic facial foundation formulations: oil-based, water-based, oil-free, and water-free forms. The most popular facial foundations are liquid oil-in-water emulsions containing a small amount of oil in which the pigment is emulsified with a relatively large quantity of water. The primary emulsifier is usually a soap, such as triethanolamine or a nonionic surfactant. The secondary emulsifier, present in smaller quantity, is usually glyceryl stearate or propylene glycol stearate.
The Multifunctional Value of Sunscreen-containing Cosmetics
Zoe Diana Draelos, MDDepartment of Dermatology, Duke University School of Medicine, Durham, NC, USA
ABSTRACT
Cosmetic products containing ultraviolet light filtering agents are rapidly being developed and entering the marketplace. These advanced multifunctional formulations are intended to deliver both cosmetic and protective benefits. Herein, a brief discussion is presented of newer preparations and their features, as well as how their formulary attributes may contribute to improving photoprotection by encouraging adherence.
Key words: cosmetics, photoprotection, SPF, sun protection factor, sunscreen, UV, ultraviolet light

• Editor: Dr. Stuart Maddin • Volume 16, Number 7 • July-August 20112
Oil-free facial foundations contain no animal, vegetable, or mineral oils. They may, however, contain other oily substances, such as the silicone derivatives dimethicone or cyclomethicone. These foundations are usually designed for patients with oily skin and/or acne. The pigment is dissolved in water and other solvents, leaving the skin with a dry feeling that results from the absence of oils.
Facial foundations are designed to color, blend, and camouflage the underlying skin and create an illusion of perfect complexion beauty. The ability of a foundation to conceal or cover the underlying skin is known as “coverage.” Higher coverage products deliver better photoprotection while lower coverage products deliver less photoprotection. In this case, the photoprotection is due to inorganic filters in the formulation, which commonly include titanium dioxide, zinc oxide, talc, kaolin and precipitated chalk. Even coloring agents, such as iron oxide, can function as inorganic filters.
Sheer coverage foundations with minimal titanium dioxide are almost transparent and have an SPF around 2 while moderate coverage foundations are translucent and have an approximate SPF of 4 to 5. Thick, waterproof cream facial foundations that are used for camouflage purposes or post-surgically completely obscure the underlying skin and have an unlimited SPF because they function as a total physical block. For persons with severe photosensitive facial skin disease, such as lupus, these waterproof cream facial foundations offer superior photoprotection.
In addition to the normal photoprotective constituents of a facial foundation, other inorganic and organic filters can also be added. The most commonly added organic filter is octyl methoxycinnamate. It is an excellent UVB filter with no aesthetic issues and limited allergenicity.1 It may be combined with other filters, such as oxybenzone, to increase coverage in the UVA range.3,4 Some of the newer facial foundations even add avobenzone that has been photostabilized with octocrylene and oxybenzone. Selecting the proper mixture of sunscreen ingredients is key to providing superior photoprotection and aesthetics while offering a high broad spectrum SPF.
New sunscreen-containing facial foundation formulations are available in a variety of forms: liquid, mousse, water-containing cream, soufflé, anhydrous cream, stick, cake, and shake lotion. Liquid formulations are most popular because they are the easiest to apply, provide sheer to moderate coverage, and create a natural appearance. As previously mentioned, they contain mainly water, oils, and titanium dioxide. To this basic formulation, sunscreen filters can be added. For most patients, this type of sun protection through a facial cosmetic is the best way to increase compliance.
Other formulations of facial foundations can also be created. If the liquid is aerosolized, a foam foundation known as a mousse is produced. A cream foundation has the additional ingredient of wax, which makes a thicker, occlusive, more moisturizing formula. These thicker cream facial foundations also deposit more pigment on the skin surface and obscure more of the underlying skin. Cream formulations typically offer better photoprotection than liquids. Whipping the cream produces a soufflé foundation. Finally, an anhydrous cream with no water in its formulation provides enhanced occlusion and exceptional long-lasting
coverage. These products resist water removal better and can be used with greater success in persons who need superior photoprotection when perspiring heavily.
There are three final forms of facial foundation that have been adapted for sun protection. These include stick, cake, and powder facial foundations. Adding more wax to the cream facial foundation results in a stick that can be stroked across the face. These facial foundation sticks are also water-free and provide water resistant photoprotection. This is in contrast to the cake and powder facial foundations that are dusted over the face. A cake foundation is a compressed powder consisting of talc, kaolin, precipitated chalk, zinc oxide, and titanium dioxide compressed into a cake that is applied to the skin with a sponge. If the ingredients are not compressed into a cake, they can be left loose in a jar with a brush attached to one end. This loose powder facial foundation is sometimes called a mineral makeup.
Mineral makeup are some of the newest sun protective cosmetics. They are dusted onto the face and can be just easily dusted off the face. Powders do not provide water resistance characteristics, making them only appropriate for day wear with casual sun exposure. Also, the powder does not provide an even film over the face, allowing for uneven photoprotection. For the patient with serious sun protection needs, it is best to apply a sunscreen-containing moisturizer followed by a mineral makeup. The moisturizer will allow the powder to stay in place and offer increased photoprotection due to layering. It is important to note that the SPF rating of the powder and the moisturizer are not additive. For example, an SPF 15 sunscreen-containing moisturizer and an SPF 15 mineral makeup do not combine to confer SPF 30 photoprotection. Each product application will make a more even sun protective film, allowing closer approximation of the SPF 15 rating.
Multifunctional SPF Rated CosmeticsMultifunctional SPF rated cosmetics are increasing in the marketplace. Lipsticks, lip balms, facial serums, and eye creams are all commercially available formulations that can possess an SPF rating. Increasing patient compliance with sun protection through the inclusion of sunscreen filters in many commonly used facial products can be a synergistic effect. Patients do not wish to purchase or use multiple products that are expensive and time consuming to apply. The multifunctional cosmetic is an important dermatologic advance. This trend is expected to continue with extensions to male skin care, such as sunscreen-containing after shave preparations. Sunscreen filters are also finding their way into hair care products that claim to prevent color fading. Protection from UV exposure improves color purity and retention, lengthening the time a hair dye can be worn until repeat dyeing is required.5 This is a positive trend for dermatology as it reinforces our safe sun message to our patients.
ConclusionWith the widespread emergence of sunscreen-containing moisturizers, foundations, and various lip treatments, it is apparent that the cosmeceutical industry has embraced the importance of photoprotection. These multifunctional products have the potential to encourage patient adherence to regimented
• Editor: Dr. Stuart Maddin • Volume 16, Number 7 • July-August 2011 3
sunscreen use by facilitating ease of application, thus minimizing the need for any significant behavioral modification, particularly during the morning routine.
References1. Draelos ZD. Photoprotection in colored cosmetics. In: Lim HW, Draelos ZD (eds).
Clinical guide to sunscreens and photoprotection. New York: Informa Healthcare USA, (2008).
2. Draelos ZD. Sunscreens and hair photoprotection. Dermatol Clin 24(1): 81-4 (2006 Jan).
3. Steinberg D. Regulatory review: sunscreens. Cosmet Toiletries 121(11):41-6 (2006 Nov).
4. Caswell M. Sunscreen formulation and testing. Cosmet Toiletries 119(9):49-58 (2001 Sep).
5. Wakefield G, Stott J, Duggan A. UVA skin protection: issues and new developments. Cosmet Toiletries 122(2):57-62 (2007 Feb).
Content & instructions can be found at:http://www.skintherapyletter.com/ipad/about.html http://www.skintherapyletter.com/ipad/support.html
Provides instant access to all articles published to date. Powerful search functionality and intuitive navigation tools allow the user to find relevant information quickly.
The application is updated automatically to include the most recently published articles.
iPad version of
Browse our archive of past issuesWe welcome your feedback.
Please email us with your comments and topic suggestions to: [email protected]
Indexed Editionfor Dermatologists & Healthcare Professionals
www.SkinTherapyLetter.com
Family Practice Edition
www.SkinTherapyLetter.ca/fp
Pharmacist Edition
www.SkinPharmacies.ca
• Editor: Dr. Stuart Maddin • Volume 16, Number 7 • July-August 20114
Practical Application of Genomics to the Development of a Topical Cosmetic
Anti-aging RegimenJoseph R. Kaczvinsky, PhD1, Vince Bertucci, MD, FRCPC2, Juian-juian Jan Fu, MD, PhD3
1The Procter & Gamble Company, Cincinnati, OH, USA2University of Toronto, Toronto, ON, Canada
3In private practice, Mason, OH, USA
Conflicts of Interest: Dr. Bertucci and Dr. Fu are paid consultants to Procter & Gamble. Dr. Kaczvinsky is employed by Procter & Gamble.
This article has been adapted (with permission from the British Journal of Dermatology) from Fu JJ, Hillebrand GG, Raleigh P, et al. A randomized, controlled comparative study of the wrinkle reduction benefits of a cosmetic niacinamide/peptide/retinyl propionate
product regimen vs. a prescription 0.02% tretinoin product regimen. Br J Dermatol 162(3):647-54 (2010 Mar).
ABSTRACT
The development of topical cosmetic anti-aging products is becoming increasingly sophisticated. This is demonstrated by the benefit agents selected and the scientific approaches used to identify them, treatment protocols that increasingly incorporate multi-product regimens, and the level of rigor in the clinical testing used to demonstrate efficacy. Consistent with these principles, a new cosmetic anti-aging regimen was recently developed. The key product ingredients were identified based on an understanding of the key mechanistic themes associated with aging at the genomic level coupled with appropriate in vitro testing. The products were designed to provide optimum benefits when used in combination in a regimen format. This cosmetic regimen was then tested for efficacy against the appearance of facial wrinkles in a 24-week clinical trial compared with 0.02% tretinoin, a recognized benchmark prescription treatment for facial wrinkling. The cosmetic regimen significantly improved wrinkle appearance after 8 weeks relative to tretinoin and was better tolerated. Wrinkle appearance benefits from the two treatments in cohorts of subjects who continued treatment through 24 weeks were also comparable.
Key words: cosmetics, aging skin, niacinamide, peptides, retinyl propionate, tretinoin, vitamin A, wrinkles
BackgroundThe advent of new technologies in a variety of areas related to skin biology and clinical research is leading to an increasing level of sophistication in the development of topical cosmetic anti-aging products. The development of reliable, accessible, and cost effective methods of measuring change in tissue gene expression has led to enhanced mechanistic understandings of skin disease and the skin aging process.1-3 This, in turn, has led to better, more specific screening approaches to identify agents that can positively affect the key mechanisms identified via genomics.4 Finally, demands for more scientifically sound demonstrations of efficacy by dermatologists, patients, and oversight organizations have led to increased rigor in the clinical testing of cosmetic products. Adequate controls, appropriate statistical approaches, relevant treatment protocols, and the combination of both subjective and objective assessments are all important factors for more robust study designs. The composition and testing of a recently developed cosmetic anti-aging regimen5 reflects the influence of all the factors mentioned above.
Skin aging is a multifactorial process that combines intrinsic factors (i.e., genetically programmed decreases in cellular function over time) with the insults of extrinsic factors (e.g., exposure to ultraviolet [UV] radiation and environmental pollution). A genomic study of chronologically old and young
skin provided insights into some of the biological mechanisms associated with chronological and photoaging.1 Among the themes observed in chronologically aged skin were decreased expression of genes related to barrier repair, especially lipid biosynthesis and epidermal cellular differentiation pathways, and upregulation of inflammatory responses, cytokine activity, and protease activity. Many of these same pathways were found to also be enhanced in photoaged skin, especially those associated with inflammation, immune responses, and the degradation of elastin and extracellular matrix.
Consistent with these genomic themes, cosmetic anti-aging ingredients were identified via in vitro testing that 1) improve skin barrier function, 2) promote normal/natural exfoliation and skin turnover, 3) help control reactive oxygen species and oxidative stress, and 4) help maintain consistent synthesis and replacement of extracellular matrix components. Treatments containing some of these ingredients have been shown to improve the appearance of aged skin in previous clinical studies.6-11 The ingredients, listed in Table 1, were incorporated into a comprehensive cosmetic product regimen. Given the multifactorial aspect of skin aging, it was felt that a combination regimen approach would provide the greatest treatment flexibility, as well as yield the opportunity to use optimum levels of potentially incompatible anti-aging ingredients. As shown in the table, this niacinamide/peptide/
• Editor: Dr. Stuart Maddin • Volume 16, Number 7 • July-August 2011 5
retinyl propionate (NPP) regimen consisted of a lotion intended for use during the day, which included sunscreen with sun protection factor (SPF) 30, a nighttime cream, and a specialized product for localized treatment of more prominently wrinkled areas of the face.
The improvement in the appearance of facial wrinkles after treatment with this cosmetic regimen was compared to that from a prescription regimen including 0.02% tretinoin in an 8-week, randomized, and controlled clinical study, with cohorts from each treatment group using their regimen for an additional 16 weeks. Results of this clinical study were recently published12 and are summarized below.
Clinical Study FindingsThe study enrolled a total of 196 Caucasian female subjects aged 40 to 65 years with moderate to moderately severe periorbital
wrinkles. Following a 2-week washout period in which the participants used a mild facial cleanser (Olay® Foaming Face Wash) ad libitum and a facial moisturizer (Olay® Complete All Day Moisture Lotion Sensitive Skin SPF 15) twice daily, the subjects were divided into two treatment groups. One group used the described cosmetic wrinkle regimen consisting of the SPF 30 lotion daily in the morning and the night cream daily in the evening, each over the entire face, and the specialized wrinkle product twice daily on areas of patient concern, while the other group used a morning application of a SPF 30 sunscreen and an evening application of 0.02% tretinoin in an emollient base. The tretinoin treatment dosing was escalated from every other evening to every evening over the first 2 weeks to minimize irritation. After 8 weeks of use, a cohort of 25 subjects from each treatment group (selected before treatment began) continued treatment for an additional 16 weeks (total of 24 weeks).
IngredientDaytime
SPF 30 LotionNight Cream Wrinkle Treatment
Niacinamide X X X
Pal-KTTKS X X X
Pal-KT X X X
Carnosine X X X
Unique ingredientsSPF 30
Vitamin C Vitamin E
– Retinyl propionate
Table 1: Ingredients for NPP cosmetic wrinkle regimen products (in a moisturizing base)Palmitoyl pentapeptides: palmitoyl-lysine-threonine-threonine-lysine-serine (Pal-KTTKS) and palmitoyl-lysine-threonine (Pal-KT)
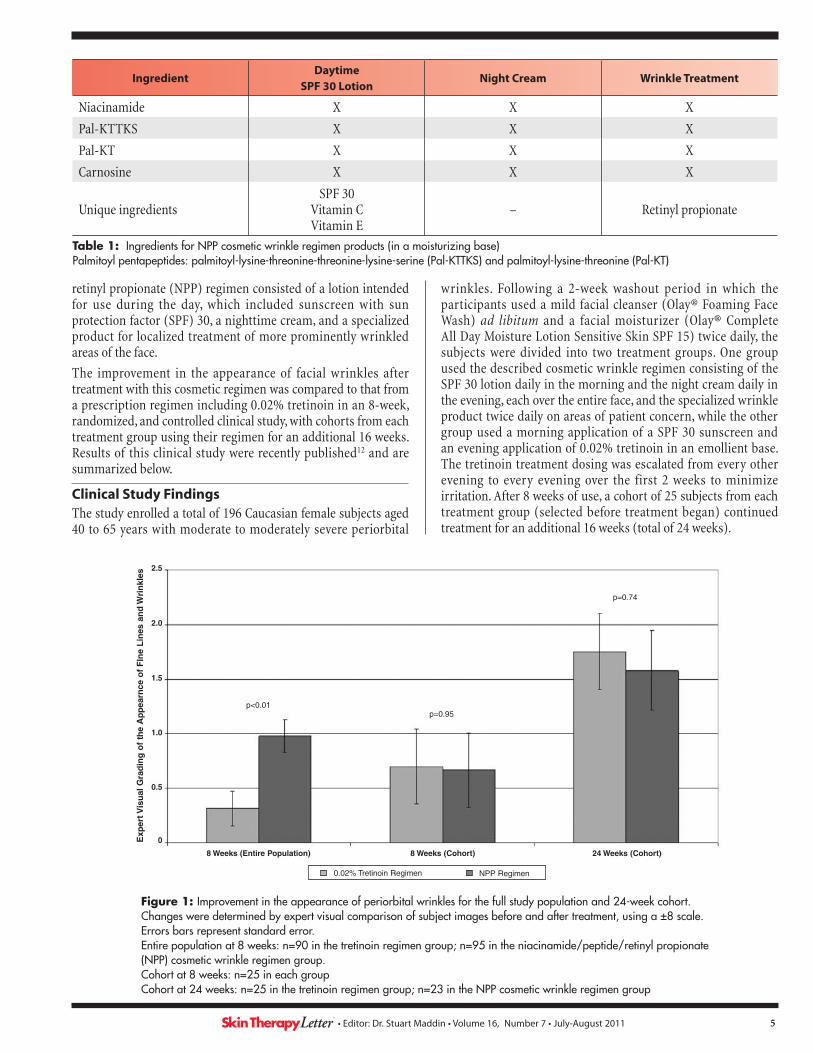
Figure 1: Improvement in the appearance of periorbital wrinkles for the full study population and 24-week cohort. Changes were determined by expert visual comparison of subject images before and after treatment, using a ±8 scale. Errors bars represent standard error. Entire population at 8 weeks: n=90 in the tretinoin regimen group; n=95 in the niacinamide/peptide/retinyl propionate (NPP) cosmetic wrinkle regimen group. Cohort at 8 weeks: n=25 in each group Cohort at 24 weeks: n=25 in the tretinoin regimen group; n=23 in the NPP cosmetic wrinkle regimen group
2.5
2.0
1.5
1.0
0.5
0
p<0.01p=0.95
p=0.74
8 Weeks (Entire Population) 8 Weeks (Cohort) 24 Weeks (Cohort)
Exp
ert V
isu
al G
rad
ing
of
the
Ap
pea
rnce
of
FIn
e L
ines
an
d W
rin
kles
0.02% Tretinoin Regimen NPP Regimen
• Editor: Dr. Stuart Maddin • Volume 16, Number 7 • July-August 20116
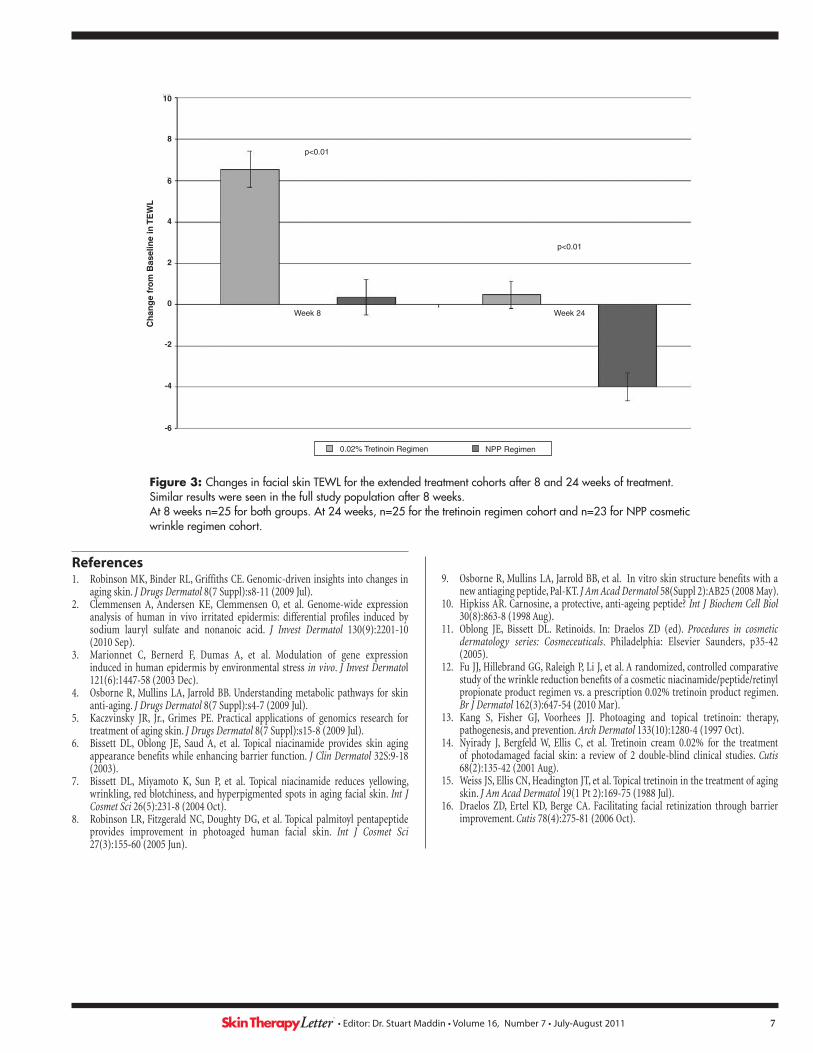
At baseline and after 8 and 24 weeks, standardized high resolution digital images were taken of both the left and right sides of the patients’ faces to capture the changes in facial wrinkles. These images were evaluated by expert grading for improved appearance of fine lines and wrinkles (+8 to -8 grading scale for improvement or worsening in the after treatment image) and were also assessed by computerized image analysis for changes in periorbital fine line and wrinkle area. Skin barrier integrity on each side of each subject’s face was determined via measurement of trans-epidermal water loss (TEWL) at the same time points. Subjects’ skin was also clinically graded for erythema and dryness periodically throughout the study, including baseline, 8 and 24 weeks, as well as intermediate times, to insure a thorough assessment of tolerance to treatment.
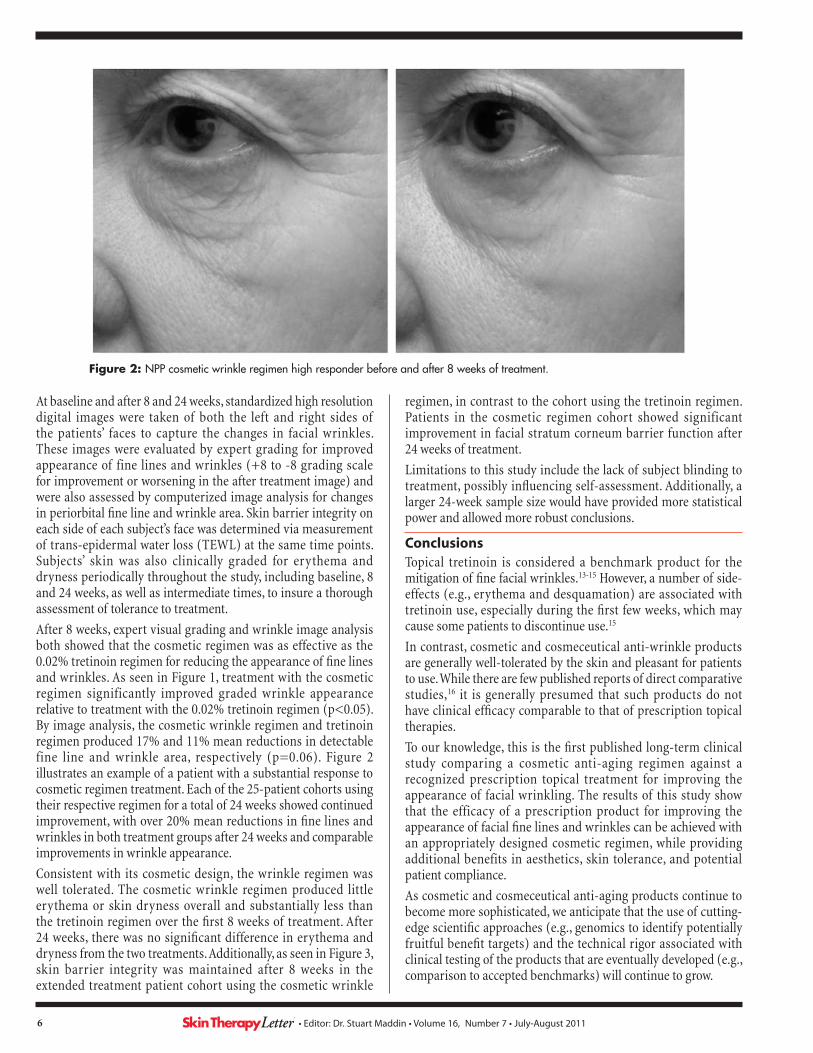
After 8 weeks, expert visual grading and wrinkle image analysis both showed that the cosmetic regimen was as effective as the 0.02% tretinoin regimen for reducing the appearance of fine lines and wrinkles. As seen in Figure 1, treatment with the cosmetic regimen significantly improved graded wrinkle appearance relative to treatment with the 0.02% tretinoin regimen (p<0.05). By image analysis, the cosmetic wrinkle regimen and tretinoin regimen produced 17% and 11% mean reductions in detectable fine line and wrinkle area, respectively (p=0.06). Figure 2 illustrates an example of a patient with a substantial response to cosmetic regimen treatment. Each of the 25-patient cohorts using their respective regimen for a total of 24 weeks showed continued improvement, with over 20% mean reductions in fine lines and wrinkles in both treatment groups after 24 weeks and comparable improvements in wrinkle appearance.
Consistent with its cosmetic design, the wrinkle regimen was well tolerated. The cosmetic wrinkle regimen produced little erythema or skin dryness overall and substantially less than the tretinoin regimen over the first 8 weeks of treatment. After 24 weeks, there was no significant difference in erythema and dryness from the two treatments. Additionally, as seen in Figure 3, skin barrier integrity was maintained after 8 weeks in the extended treatment patient cohort using the cosmetic wrinkle
regimen, in contrast to the cohort using the tretinoin regimen. Patients in the cosmetic regimen cohort showed significant improvement in facial stratum corneum barrier function after 24 weeks of treatment.
Limitations to this study include the lack of subject blinding to treatment, possibly influencing self-assessment. Additionally, a larger 24-week sample size would have provided more statistical power and allowed more robust conclusions.
ConclusionsTopical tretinoin is considered a benchmark product for the mitigation of fine facial wrinkles.13-15 However, a number of side-effects (e.g., erythema and desquamation) are associated with tretinoin use, especially during the first few weeks, which may cause some patients to discontinue use.15
In contrast, cosmetic and cosmeceutical anti-wrinkle products are generally well-tolerated by the skin and pleasant for patients to use. While there are few published reports of direct comparative studies,16 it is generally presumed that such products do not have clinical efficacy comparable to that of prescription topical therapies.
To our knowledge, this is the first published long-term clinical study comparing a cosmetic anti-aging regimen against a recognized prescription topical treatment for improving the appearance of facial wrinkling. The results of this study show that the efficacy of a prescription product for improving the appearance of facial fine lines and wrinkles can be achieved with an appropriately designed cosmetic regimen, while providing additional benefits in aesthetics, skin tolerance, and potential patient compliance.
As cosmetic and cosmeceutical anti-aging products continue to become more sophisticated, we anticipate that the use of cutting-edge scientific approaches (e.g., genomics to identify potentially fruitful benefit targets) and the technical rigor associated with clinical testing of the products that are eventually developed (e.g., comparison to accepted benchmarks) will continue to grow.
Figure 2: NPP cosmetic wrinkle regimen high responder before and after 8 weeks of treatment.
• Editor: Dr. Stuart Maddin • Volume 16, Number 7 • July-August 2011 7
Figure 3: Changes in facial skin TEWL for the extended treatment cohorts after 8 and 24 weeks of treatment. Similar results were seen in the full study population after 8 weeks. At 8 weeks n=25 for both groups. At 24 weeks, n=25 for the tretinoin regimen cohort and n=23 for NPP cosmetic wrinkle regimen cohort.
References1. Robinson MK, Binder RL, Griffiths CE. Genomic-driven insights into changes in
aging skin. J Drugs Dermatol 8(7 Suppl):s8-11 (2009 Jul).2. Clemmensen A, Andersen KE, Clemmensen O, et al. Genome-wide expression
analysis of human in vivo irritated epidermis: differential profiles induced by sodium lauryl sulfate and nonanoic acid. J Invest Dermatol 130(9):2201-10 (2010 Sep).
3. Marionnet C, Bernerd F, Dumas A, et al. Modulation of gene expression induced in human epidermis by environmental stress in vivo. J Invest Dermatol 121(6):1447-58 (2003 Dec).
4. Osborne R, Mullins LA, Jarrold BB. Understanding metabolic pathways for skin anti-aging. J Drugs Dermatol 8(7 Suppl):s4-7 (2009 Jul).
5. Kaczvinsky JR, Jr., Grimes PE. Practical applications of genomics research for treatment of aging skin. J Drugs Dermatol 8(7 Suppl):s15-8 (2009 Jul).
6. Bissett DL, Oblong JE, Saud A, et al. Topical niacinamide provides skin aging appearance benefits while enhancing barrier function. J Clin Dermatol 32S:9-18 (2003).
7. Bissett DL, Miyamoto K, Sun P, et al. Topical niacinamide reduces yellowing, wrinkling, red blotchiness, and hyperpigmented spots in aging facial skin. Int J Cosmet Sci 26(5):231-8 (2004 Oct).
8. Robinson LR, Fitzgerald NC, Doughty DG, et al. Topical palmitoyl pentapeptide provides improvement in photoaged human facial skin. Int J Cosmet Sci 27(3):155-60 (2005 Jun).
9. Osborne R, Mullins LA, Jarrold BB, et al. In vitro skin structure benefits with a new antiaging peptide, Pal-KT. J Am Acad Dermatol 58(Suppl 2):AB25 (2008 May).
10. Hipkiss AR. Carnosine, a protective, anti-ageing peptide? Int J Biochem Cell Biol 30(8):863-8 (1998 Aug).
11. Oblong JE, Bissett DL. Retinoids. In: Draelos ZD (ed). Procedures in cosmetic dermatology series: Cosmeceuticals. Philadelphia: Elsevier Saunders, p35-42 (2005).
12. Fu JJ, Hillebrand GG, Raleigh P, Li J, et al. A randomized, controlled comparative study of the wrinkle reduction benefits of a cosmetic niacinamide/peptide/retinyl propionate product regimen vs. a prescription 0.02% tretinoin product regimen. Br J Dermatol 162(3):647-54 (2010 Mar).
13. Kang S, Fisher GJ, Voorhees JJ. Photoaging and topical tretinoin: therapy, pathogenesis, and prevention. Arch Dermatol 133(10):1280-4 (1997 Oct).
14. Nyirady J, Bergfeld W, Ellis C, et al. Tretinoin cream 0.02% for the treatment of photodamaged facial skin: a review of 2 double-blind clinical studies. Cutis 68(2):135-42 (2001 Aug).
15. Weiss JS, Ellis CN, Headington JT, et al. Topical tretinoin in the treatment of aging skin. J Am Acad Dermatol 19(1 Pt 2):169-75 (1988 Jul).
16. Draelos ZD, Ertel KD, Berge CA. Facilitating facial retinization through barrier improvement. Cutis 78(4):275-81 (2006 Oct).
10
8
p<0.01
p<0.01
Week 8
0.02% Tretinoin Regimen NPP Regimen
Week 24
6
4
2
0
-2
-4
-6
Ch
ang
e fr
om
Bas
elin
e in
TE
WL
• Editor: Dr. Stuart Maddin • Volume 16, Number 7 • July-August 20118
Name/Company Approval Dates/Comments
Human papillomavirus (HPV) testCobas® HPV Test Cobas® 4800 SystemF. Hoffmann-La Roche Ltd.
The US FDA approved the cobas HPV test in April 2011 for identifying women at highest risk for developing cervical cancer. It individually identifies genotypes 16 and 18 (the two highest-risk HPV genotypes responsible for >70% of cervical cancer cases), as well as detects 12 other high risk HPV genotypes.
Betamethasone valerate 0.12% foamLuxiq®GlaxoSmithKline Inc.
Health Canada approved a prescription only, foam formulation of betamethasone valerate, a mid-potency corticosteroid, in May 2011 for the treatment of the inflammatory and pruritic manifestations of corticosteroid-responsive scalp dermatoses.
Drug NewsOn June 14, 2011, the US FDA announced changes to sunscreen labeling that would allow consumers to more easily decipher the commonly used terms on these products. Highlights from this press release include:• Sunscreen products are no longer able to use the term "broad spectrum" unless they
pass FDA efficacy testing for ultraviolet A (UVA) and ultraviolet B (UVB) protection.• Broad spectrum sunscreens with SPF 15 or higher that meet the FDA’s standards can
state that they prevent sunburn, reduce the risk of skin cancer, and limit photoaging when used properly and regularly.
• Sunscreens offering SPF between 2 to 14 with UVA protection can be labeled as "broad spectrum” if they meet FDA testing requirements. However, these products must carry a warning stating that their use has not been demonstrated to contribute to the prevention of skin cancer or premature skin aging.
• The new rules will no longer allow sunscreens to use the terms "waterproof," "sweatproof " or "sunblock" on product labels because they are misleading to consumers and do not actually confer the degree of protection as implied. However, the use of “water resistance” is permitted if they are effective for 40 or 80 minutes while swimming or sweating.
• Limiting the maximum SPF value on sunscreens to "50 +" is also under FDA consideration, as there is insufficient evidence supporting improved photoprotection with such products compared to those with SPF 50.
• Due to the unique delivery vehicle characteristics of sprays, the FDA has requested additional efficacy and safety data on these sunscreen formulations.
The new regulations will take effect by summer 2012.For more information: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm258940.htm
The US FDA1 and Health Canada2 issued separate advisories in May and June 2011, respectively, announcing that they are conducting safety reviews of drospirenone-containing oral contraceptive pills (OCPs) to evaluate their potential for increased risk of venous thromboembolism in women who use these products. Blood clots are a rare but well known side-effect associated with all OCPs. The affected product brands are Yaz® and Yasmin® in Canada, and in the US they include Yaz® (generics Gianvi™ and Loryna™), Yasmin® (generics Ocella™, Syeda™, and Zarah™), Beyaz™, and Safyral™.In May 2011, the European Medicines Agency (EMA)3 announced that it is updating the product information on OCPs containing drospirenone and ethinyl estradiol (Yasmin®, Yasminelle®, and other products) with respect to the risk of venous thromboembolism. Two new studies recently published in the British Medical Journal4,5 suggest the risk of blood clots with drospirenone-containing OCPs may be two to three times greater than with OCPs containing the progestin levonorgestrel.1. http://www.fda.gov/Drugs/DrugSafety/ucm257164.htm2. http://www.hc-sc.gc.ca/ahc-asc/media/advisories-avis/_2011/2011_74-eng.php3. http://www.ema.europa.eu/docs/en_GB/document_library/Report/2011/05/WC500106708.pdf4. Jick SS, Hernandez RK. BMJ 342:d2151 (2011 Apr 23). [Epub ahead of print]5. Parkin L, Sharples K, Hernandez RK, et al. BMJ 342:d2139 (2011 Apr 23). [Epub ahead of print]
EDITOR-IN-CHIEFStuart Maddin, MDUniversity of British Columbia, Vancouver, Canada
ASSOCIATE EDITORSHugo Degreef, MD, PhDCatholic University, Leuven, Belgium
Jason Rivers, MDUniversity of British Columbia, Vancouver, Canada
EDITORIAL ADVISORY BOARDMurad Alam, MDNorthwestern University Medical School, Chicago, USA
Kenneth A. Arndt, MDBeth Israel HospitalHarvard Medical School, Boston, USA
Wilma Fowler Bergfeld, MDCleveland Clinic, Cleveland, USA
Jan D. Bos, MDUniversity of Amsterdam, Amsterdam, Holland
Alastair Carruthers, MDUniversity of British Columbia, Vancouver, Canada
Bryce Cowan, MD, PhDUniversity of British Columbia, Vancouver, Canada
Jeffrey S. Dover, MDYale University School of Medicine, New Haven, USADartmouth Medical School, Hanover, USA
Boni E. Elewski, MDUniversity of Alabama, Birmingham, USA
Barbara A. Gilchrest, MDBoston University School of Medicine, Boston, USA
Christopher E.M. Griffiths, MDUniversity of Manchester, Manchester, UK
Aditya K. Gupta, MD, PhD, MBA/MCMUniversity of Toronto, Toronto, Canada
Mark Lebwohl, MDMt. Sinai Medical Center, New York, USA
James J. Leydon, MDUniversity of Pennsylvania, Philadelphia, USA
Harvey Lui, MDUniversity of British Columbia, Vancouver, Canada
Howard I. Maibach, MDUniversity of California Hospital, San Francisco, USA
Jose Mascaro, MD, MSUniversity of Barcelona, Barcelona, Spain
Larry E. Millikan, MDTulane University Medical Center, New Orleans, USA
Jean Paul Ortonne, MDCentre Hospitalier Universitaire de Nice, Nice, France
Ted Rosen, MDBaylor College of Medicine, Houston, USA
Alan R. Shalita, MDSUNY Health Sciences Center, Brooklyn, USA
Wolfram Sterry, MDHumboldt University, Berlin, Germany
Richard Thomas, MDUniversity of British Columbia, Vancouver, Canada
Stephen K. Tyring, MD, PhD, MBAUniversity of Texas Health Science Center, Houston, USA
John Voorhees, MDUniversity of Michigan, Ann Arbor, USA
Guy Webster, MDJefferson Medical College, Philadelphia, USA
Klaus Wolff, MDUniversity of Vienna, Vienna, Austria
Skin Therapy Letter © (ISSN 1201–5989) Copyright 2011 by SkinCareGuide.com Ltd. Skin Therapy Letter © is published 10 times annually by SkinCareGuide.com Ltd, 1004 – 750 West Pender, Vancouver, British Columbia, Canada, V6C 2T8. All rights reserved. Reproduction in whole or in part by any process is strictly forbidden without prior consent of the publisher in writing. While every effort is made to see that no inaccurate or misleading data, opinion, or statement appears in the Skin Therapy Letter ©, the Publishers and Editorial Board wish to make it clear that the data and opinions appearing in the articles herein are the responsibility of the contributor. Accordingly, the Publishers, the Editorial Committee and their respective employees, officers, and agents accept no liability whatsoever for the consequences of any such inaccurate or misleading data, opinion, or statement. While every effort is made to ensure that drug doses and other quantities are presented accurately, readers are advised that new methods and techniques involving drug usage, and described herein, should only be followed in conjunction with the drug manufacturer’s own published literature. Printed on acid-free paper effective with Volume 1, Issue 1, 1995.
Subscription Information. Annual subscription: Canadian $94 indi-vidual; $171 institutional (plus GST); US $66 individual; $121 insti-tutional. Outside North America: US$88 individual; $143 institutional. We sell reprints in bulk (100 copies or more of the same article). For individual reprints, we sell photocopies of the articles. The cost is $20 to fax and $15 to mail. Prepayment is required. Student rates available upon request. For inquiries: [email protected]
Update on Drugs