The Medicare Landscape and the Physicians Perspective Earl Berman, MD, FACP, MALPS-L Michael...
86
The Medicare Landscape and the Physician’s Perspective Earl Berman, MD, FACP, MALPS-L Michael Montijo, MD, MPH, FACP James Szarzynski, Director of Medical Review
-
Upload
keyshawn-boye -
Category
Documents
-
view
223 -
download
4
Transcript of The Medicare Landscape and the Physicians Perspective Earl Berman, MD, FACP, MALPS-L Michael...

The Medicare Landscape and the Physician’s Perspective
Earl Berman, MD, FACP, MALPS-L
Michael Montijo, MD, MPH, FACP
James Szarzynski, Director of Medical Review

WelcomeSchedule for This Evening’s Program
Pre-test
CMEs: AMA and OPMA PRA Category 1 credits (2.5)
CEUs: check with specific organization; certificate provided upon conclusion of session
Materials available on CGS website
Questions and discussion
Post-test and evaluations
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC2

Overview: Medicare as a defined benefit
Challenges across disciplines and facilities
Hospitalization challenges
The home health benefit
Physicians’ key role
Medical review focus for CGS
Future state and next steps
Questions and discussion
Agenda
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC3

Objectives
Identify key data sources for errors in Medicare claims and documentation
List topics and issues under increased scrutiny by Medicare contractors
Define the role of physicians in responding to challenges regarding documentation and payment errors
Name current and future areas of focus with respect to Medicare claims, documentation, and payment
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC4

Medicare as a Defined Benefit
Setting the stage
– Average monthly # of beneficiaries enrolled in Medicare A and/or B (estimated for FY 2013): 52 million
Approx. 73% enrolled in FFS Medicare
– Claims processed in CY 2012:
Part A: 208,144,073
Part B: 1,022,408,206
– Medicare benefits estimated to be paid in FY 2013: $590.2 billion
– Source: CMS Fast Facts (http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/CMS-Fast-Facts/index.html)
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC5

Medicare as a Defined Benefit
Setting the stage
– Ohio:
10th largest state by beneficiary population (approx. 1.1 million)
Allowed charges: over $111 million
– Kentucky:
22nd largest state by beneficiary population (approx. 609,000)
Allowed charges: over $48 million
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC6

Medicare as a Defined Benefit
“Defined benefit”: services and payment
– Statutory: Social Security Act (“medical necessity”: section 1862(a)(1)(A))
– May limit number of covered days, frequency, setting, or types of services covered or not covered
– May be irrespective of patient need
– Payment vs. treatment/care
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC7

Medicare as a Defined Benefit
Future state
– Bundled payments
– ACOs
– Ability to “flex” benefits
– Add additional “resources” – as deemed needed by the caregivers
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC8

Medicare as a Defined Benefit
Requirements for payment
– Statutory
– Federal (CMS-level)
– Local (Medicare contractors)
Documentation as a condition for payment
Purpose of documentation: treatment/orders vs. medicolegal vs. Medicare payment
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC9

Medicare as a Defined Benefit
“Reasonable and necessary” standard: determined by treating physician unless
– Treatment conflicts with clinical standards of care; or
– Substantial scientific evidence of risk or ineffectiveness (i.e., sizeable number of studies published in peer-reviewed journals meeting professionally recognized standards of quality)
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC10

Medicare as a Defined Benefit
“Reasonable and necessary” standard: AMA definition– "Health care services or products that a prudent physician
would provide to a patient for the purpose of preventing, diagnosing or treating an illness, injury, disease or its symptoms in a manner that is:
In accordance with generally accepted standards of medical practice
Clinically appropriate in terms of type, frequency, extent, site, and duration, and
Not primarily for the convenience of the patient, physician, or other health care provider”
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC11

Medicare as a Defined Benefit
Documentation challenges and consequences
– Impact on payment
– Data analysis and involvement of multiple Medicare contractors
– Further scrutiny: OIG, GAO, Congress, Recovery Auditors, MACs
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC12

Medicare as a Defined Benefit
Why are we here?
Key data sources:
– Comprehensive Error Rate Testing (CERT) program: www.cms.gov/cert
– CGS medical review outcomes
– PEPPER reports
– Comparative Billing Reports (CBRs): peer comparisons
– OIG reports and workplans: www.oig.hhs.gov/oas/cms.asp
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC13

Medicare as a Defined Benefit
Stats: setting the stage
– Medicare receives approx. 4.8 million claims per day.
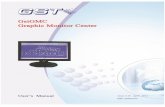
– In 2011, the Comprehensive Error Rate Testing (CERT) program identified $28.8 billion in incorrect payments (calculated, adjusted error rate = 8.6%)
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC14

Medicare as a Defined Benefit
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC
15

Improper Payments ($ in billions): 2011 CERT report
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC16

Challenges Across Disciplines & Facilities
Documentation
Signatures
Specificity of orders/requests
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC17

Challenges Across Disciplines & Facilities Documentation
– Demonstrate medical necessity (patient’s condition, care needed, setting)
– Nature/type of service provided
– Duration of the patient-physician relationship
– Clear rationale
– Consistency
– “Technical” requirements (e.g., dated signature)
– Must reflect care provided (not expected to precisely reflect every aspect of are provided)
– Is not direct patient care but is a component of care
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC18

Challenges Across Disciplines & Facilities: Signatures
Signatures
– Problem area in all disciplines and all provider types
– Acceptable electronic signatures – if using EMR, ensure your practice or facility’s system meets the requirements (complete list of requirements in CMS article MM6698, “Signature Requirements for Medical Review Purposes”)
– Legibility
– Stamped signatures? – NO
– Late signatures and attestations
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC19

Challenges Across Disciplines & Facilities: Signatures
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC20

Challenges Across Disciplines & Facilities: Signatures
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC21

Challenges Across Disciplines & Facilities: Specificity of Orders
Specificity of orders/requests
– Ambulatory Surgery Centers; Radiology; Clinical Laboratories; drugs & biologicals
– Must demonstrate medical necessity of test/service/ procedure (ICD-9 code alone may not be sufficient)
– Joint responsibility of testing/administering entity and ordering physician
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC22

Hospitalization Challenges
Elective admissions
One-day stays
Medical necessity & reasonableness: ambulatory sensitive diagnoses
Outpatient procedures
Skilled Nursing Facility (SNF) qualifying stay
Appropriate setting
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC23

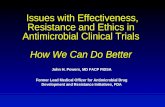
Short-Term National Q1FY13 Report − Top 20 Surgical DRGs for One-Day StaysDischarges for most recent 4 Quarters, ending Q1FY2013
In Descending Order by One-Day Stay Totals Per DRG
DRG DRG DescriptionOne-Day
Stay Count*Total Discharges
for DRG
Proportion of One-Day Stays to Total Discharges
Average Length of Stay for DRG
247 Perc cardiovasc proc w drug-eluting stent w/o MCC 27,545 98,291 28.0% 2.7
039 Extracranial procedures w/o CC/MCC 21,452 33,758 63.5% 1.9
473 Cervical spinal fusion w/o CC/MCC 16,034 27,589 58.1% 2.1
491 Back & neck proc exc spinal fusion w/o CC/MCC 11,623 30,688 37.9% 2.5
470 Major joint replacement or reattachment of lower extremity w/o MCC 10,363 415,888 2.5% 3.9
238 Major cardiovasc procedures w/o MCC 9,218 34,729 26.5% 4.2
254 Other vascular procedures w/o CC/MCC 8,902 27,053 32.9% 3.0
251 Perc cardiovasc proc w/o coronary artery stent w/o MCC 7,765 27,618 28.1% 3.2
484 Major joint & limb reattachment proc of upper extremity w/o CC/MCC 7,308 22,793 32.1% 2.5
708 Major male pelvic procedures w/o CC/MCC 7,101 12,887 55.1% 2.0
460 Spinal fusion except cervical w/o MCC 6,841 68,770 9.9% 4.0
227 Cardiac defibrillator implant w/o cardiac cath w/o MCC 6,747 15,861 42.5% 3.4
743 Uterine & adnexa proc for non-malignancy w/o CC/MCC 5,947 16,955 35.1% 2.3
249 Perc cardiovasc proc w non-drug-eluting stent w/o MCC 5,441 27,011 20.1% 3.1
244 Permanent cardiac pacemaker implant w/o CC/MCC 5,293 26,473 20.0% 3.1
627 Thyroid, parathyroid & thyroglossal procedures w/o CC/MCC 4,826 6,950 69.4% 1.8
038 Extracranial procedures w CC 3,843 12,060 31.9% 3.7
036 Carotid artery stent procedure w/o CC/MCC 3,718 5,107 72.8% 1.6
253 Other vascular procedures w CC 3,716 38,432 9.7% 5.9
419 Laparoscopic cholecystectomy w/o CDE w/o CC/MCC 3,660 22,216 16.5% 3.2
Top 20 Surgical DRGs 177,343 971,129 18.3% 3.5
All Surgical DRGs 300,316 2,763,240 10.9% 6.4
*Excludes deaths, transfers, leaves against medical advice, and claims with prior observation of 24 hours or greater.
One-Day Stays: Surgical DRGs
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC24

Short-Term National Q1FY13 Report − Top 20 Medical DRGs for One-Day StaysDischarges for most recent 4 Quarters, ending Q1FY2013
In Descending Order by One-Day Stay Totals Per DRG
DRG DRG DescriptionOne-Day
Stay Count*
Total Discharges
for DRG
Proportion of One-Day Stays to Total Discharges
Average Length of Stay for DRG
313 Chest pain 37,121 99,318 37.4% 2.2
310 Cardiac arrhythmia & conduction disorders w/o CC/MCC 33,573 107,281 31.3% 2.4
392 Esophagitis, gastroent & misc digest disorders w/o MCC 27,139 210,577 12.9% 3.6
312 Syncope & collapse 24,623 118,979 20.7% 3.0
287 Circulatory disorders except AMI, w card cath w/o MCC 21,405 102,126 21.0% 3.3
069 Transient ischemia 20,290 79,595 25.5% 2.7
641 Misc disorders of nutrition,metabolism,fluids/electrolytes w/o MCC 19,585 132,034 14.8% 3.7
812 Red blood cell disorders w/o MCC 17,823 88,757 20.1% 3.5
309 Cardiac arrhythmia & conduction disorders w CC 16,478 105,815 15.6% 3.4
690 Kidney & urinary tract infections w/o MCC 14,915 193,058 7.7% 4.0
192 Chronic obstructive pulmonary disease w/o CC/MCC 11,940 97,328 12.3% 3.4
292 Heart failure & shock w CC 10,814 201,820 5.4% 4.6
191 Chronic obstructive pulmonary disease w CC 10,267 137,205 7.5% 4.3
918 Poisoning & toxic effects of drugs w/o MCC 10,001 33,820 29.6% 2.8
293 Heart failure & shock w/o CC/MCC 9,766 78,011 12.5% 3.2
683 Renal failure w CC 9,718 154,529 6.3% 4.6
066 Intracranial hemorrhage or cerebral infarction w/o CC/MCC 9,158 59,692 15.3% 3.0
948 Signs & symptoms w/o MCC 9,067 51,182 17.7% 3.4
378 GI hemorrhage w CC 9,050 139,808 6.5% 4.0
305 Hypertension w/o MCC 8,683 31,672 27.4% 2.7
Top 20 Medical DRGs 331,416 2,222,607 14.9% 3.6
All Medical DRGs 704,383 7,343,966 9.6% 4.8
*Excludes deaths, transfers, leaves against medical advice, and claims with prior observation of 24 hours or greater.
One-Day Stays: Medical DRGs
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC25

Short-Term Acute Care PEPPER Visit PEPPERresources.org
PPS Hospitals for Demo Jurisdiction (DMSTR)1DS Top Medical DRGs
Jurisdiction Top 20 Medical DRGs for One-Day Stay Disch., Most Recent 4 Qtrs.In Descending Order by One-Day Stay Totals Per DRG
DRG Description
One-Day Stay
Count*Total Dis-charges
for DRG
Proportion of One-Day Stays to Total
Dis-chargesfor DRG
Jurisdict.AverageLength
ofStay
for DRG
313 Chest pain 3,045 7,282 41.8% 2.1392 Esophagitis, gastroent & misc digest disorders w/o MCC 2,274 14,697 15.5% 3.4310 Cardiac arrhythmia & conduction disorders w/o CC/MCC 2,163 7,037 30.7% 2.4312 Syncope & collapse 1,989 9,212 21.6% 3.0287 Circulatory disorders except AMI, w card cath w/o MCC 1,686 7,560 22.3% 3.2069 Transient ischemia 1,617 6,063 26.7% 2.6641 Misc disorders of nutrition,metabolism,fluids/electrolytes w/o MCC 1,405 8,381 16.8% 3.3309 Cardiac arrhythmia & conduction disorders w CC 1,087 7,278 14.9% 3.4812 Red blood cell disorders w/o MCC 1,076 5,359 20.1% 3.5690 Kidney & urinary tract infections w/o MCC 1,060 11,813 9.0% 4.1192 Chronic obstructive pulmonary disease w/o CC/MCC 909 6,723 13.5% 3.3191 Chronic obstructive pulmonary disease w CC 908 10,646 8.5% 4.2292 Heart failure & shock w CC 816 13,809 5.9% 4.4918 Poisoning & toxic effects of drugs w/o MCC 773 2,368 32.6% 2.6303 Atherosclerosis w/o MCC 713 2,344 30.4% 2.3683 Renal failure w CC 686 10,669 6.4% 4.5101 Seizures w/o MCC 680 3,541 19.2% 3.1378 GI hemorrhage w CC 662 9,581 6.9% 3.9948 Signs & symptoms w/o MCC 630 3,447 18.3% 3.3293 Heart failure & shock w/o CC/MCC 620 4,941 12.5% 4.0
Top Medical DRGs Jurisdiction-wide 24,799 152,751 16.2% 3.5All Medical DRGs Jurisdiction-wide 50,404 490,830 10.3% 4.7
*Excludes deaths, transfers, leaves against medical advice, and claims with prior observation of 24 hours
or greater.Note: DRGs will display if they had at least 11 one-day stay discharges in the most recent four quarters.
Short-Term Acute Stays: Med
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC26

Short-Term Acute Care PEPPER Visit PEPPERresources.org
PPS Hospitals for Demo Jurisdiction (DMSTR)1DS Top Surgical DRGs
Jurisdiction Top 20 Surgical DRGs for One-Day Stay Disch., Most Recent 4 Qtrs.In Descending Order by One-Day Stay Totals Per DRG
DRG Description
One-Day Stay
Count*Total Dis-charges
for DRG
Proportion of One-Day Stays to Total
Dis-chargesfor DRG
Jurisdict.AverageLength
ofStay
for DRG
247 Perc cardiovasc proc w drug-eluting stent w/o MCC 2,744 7,737 35.5% 2.5039 Extracranial procedures w/o CC/MCC 1,611 2,337 68.9% 1.7
470 Major joint replacement or reattachment of lower extremity w/o MCC 1,414 26,471 5.3% 3.3254 Other vascular procedures w/o CC/MCC 967 2,188 44.2% 2.5473 Cervical spinal fusion w/o CC/MCC 905 1,612 56.1% 2.0491 Back & neck proc exc spinal fusion w/o CC/MCC 727 1,834 39.6% 2.3251 Perc cardiovasc proc w/o coronary artery stent w/o MCC 641 1,885 34.0% 3.2238 Major cardiovasc procedures w/o MCC 615 2,140 28.7% 4.0249 Perc cardiovasc proc w non-drug-eluting stent w/o MCC 532 2,220 24.0% 2.9708 Major male pelvic procedures w/o CC/MCC 532 890 59.8% 1.7
484 Major joint & limb reattachment proc of upper extremity w/o CC/MCC 517 1,498 34.5% 2.1627 Thyroid, parathyroid & thyroglossal procedures w/o CC/MCC 500 629 79.5% 1.4227 Cardiac defibrillator implant w/o cardiac cath w/o MCC 473 1,051 45.0% 3.4743 Uterine & adnexa proc for non-malignancy w/o CC/MCC 465 1,166 39.9% 2.0460 Spinal fusion except cervical w/o MCC 372 4,796 7.8% 3.7253 Other vascular procedures w CC 352 2,683 13.1% 5.8244 Permanent cardiac pacemaker implant w/o CC/MCC 342 1,755 19.5% 3.1036 Carotid artery stent procedure w/o CC/MCC 315 398 79.1% 1.5581 Other skin, subcut tiss & breast proc w/o CC/MCC 269 564 47.7% 2.4038 Extracranial procedures w CC 267 825 32.4% 3.8
Top Surgical DRGs Jurisdiction-wide 14,560 64,679 22.5% 3.1
All Surgical DRGs Jurisdiction-wide 22,491 176,430 12.7% 6.0
*Excludes deaths, transfers, leaves against medical advice, and claims with prior observation of 24 hours
or greater.Note: DRGs will display if they had at least 11 one-day stay discharges in the most recent four quarters.
Short-Term Acute Stays: Surg
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC27

Short Term Acute Care PEPPER
Visit PEPPERresources.org
Chronic Obstructive Pulmonary Disease
Hospital
Q1 = Oct-Dec Q2 = Jan-Mar Q3 = Apr-Jun Q4 = Jul-Sep Time Periods
Target Area Discharge Count (Numerator) Denominator Count
Percent (Numerator / Denominator)
Target Area Average Length of Stay (ALOS)
Denominator Average Length of Stay (ALOS)
Target Average Medicare Payment
Target Sum Medicare Payments
Q2 FY 2010 43 185 23.2% 3.4 5.2 $5,103 $219,450
Q3 FY 2010 50 163 30.7% 3.3 4.6 $5,134 $256,705
Q4 FY 2010 37 114 32.5% 3.8 4.5 $4,878 $180,480
Q1 FY 2011 35 134 26.1% 3.8 5.4 $5,147 $180,157
Q2 FY 2011 64 188 34.0% 4.1 4.5 $5,183 $331,715
Q3 FY 2011 48 158 30.4% 3.9 4.7 $4,912 $235,781
Q4 FY 2011 40 122 32.8% 3.1 4.5 $4,807 $192,289
Q1 FY 2012 64 146 43.8% 3.4 3.9 $5,287 $338,366
Q2 FY 2012 48 158 30.4% 3.7 4.5 $5,328 $255,729
Q3 FY 2012 33 121 27.3% 3.7 4.0 $5,628 $185,732
Q4 FY 2012 32 136 23.5% 3.3 4.5 $5,173 $165,539
Q1 FY 2013 50 132 37.9% 3.2 5.1 $5,193 $259,665
Need to audit? When reviewing this information, you may want to consider auditing a sample of records if you identify:
• Percents (4th column in the table below) that are consistently red (high outlier) • A trend of increasing Percents over time resulting in outlier status• Your Percent is above the national 80th percentile (see graph on the following worksheet)
Short-Term Acute Stays: COPD
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC28

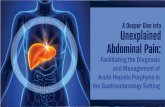
Short-Term Acute Care PEPPER
Single CC or MCC (New target area as of Q1FY13)
Q1 = Oct-Dec Q2 = Jan-Mar Q3 = Apr-Jun Q4 = Jul-Sep Time Periods
Target Area Discharge Count (Numerator) Denominator Count
Percent (Numerator / Denominator)
Target Area Average Length of Stay (ALOS)
Denominator Average Length of Stay (ALOS)
Target Average Medicare Payment
Target Sum Medicare Payments
Q2 FY 2010 194 547 35.5% 3.6 5.3 $5,755 $1,116,408
Q3 FY 2010 221 508 43.5% 3.5 4.8 $5,811 $1,284,128
Q4 FY 2010 188 459 41.0% 3.4 4.8 $6,701 $1,259,802
Q1 FY 2011 191 486 39.3% 3.7 5.1 $6,093 $1,163,806
Q2 FY 2011 228 584 39.0% 3.7 4.9 $6,079 $1,386,008
Q3 FY 2011 206 467 44.1% 3.8 5.0 $6,693 $1,378,843
Q4 FY 2011 198 470 42.1% 3.5 5.0 $6,067 $1,201,249
Q1 FY 2012 216 518 41.7% 3.3 4.5 $6,374 $1,376,693
Q2 FY 2012 177 604 29.3% 3.3 5.0 $5,943 $1,051,967
Q3 FY 2012 161 522 30.8% 3.2 4.9 $5,878 $946,417
Q4 FY 2012 182 539 33.8% 2.9 4.6 $6,233 $1,134,421
Q1 FY 2013 171 495 34.5% 3.1 4.9 $6,853 $1,171,783
Need to audit? When reviewing this information, you may want to consider auditing a sample of records if you identify:
• Percents (4th column in the table below) that are consistently red (high outlier) or green (low outlier)• A trend of increasing or decreasing Percents over time resulting in outlier status• Your Percent is above the national 80th percentile (see graph on the following worksheet)• Your Percent is below the national 20th percentile (see graph on the following worksheet)
Short-Term Acute Stays: Single CC or MCC
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC29

Short-Term Acute Stays
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC30

Medical Necessity & Reasonableness: Recovery Auditor Quarterly Stats
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC
31
Region B Top Error: Cardiovascular Procedures
– Medical necessity for cardiovascular procedures performed inpatient hospital are not supported in medical record

Short-Term Acute Care PEPPER
Visit PEPPERresources.org
Three-day Skilled Nursing Facility-qualifying Admissions000904 Hospital H0904
Q1 = Oct-Dec Q2 = Jan-Mar Q3 = Apr-Jun Q4 = Jul-Sep Time Periods
Target Area Discharge Count (Numerator) Denominator Count
Percent (Numerator / Denominator)
Target Area Average Length of Stay (ALOS)
Denominator Average Length of Stay (ALOS)
Target Average Medicare Payment
Target Sum Medicare Payments
Q2 FY 2010 37 195 19.0% 3.0 6.5 $7,219 $267,087Q3 FY 2010 33 147 22.4% 3.0 5.9 $6,445 $212,695Q4 FY 2010 38 161 23.6% 3.0 5.8 $6,819 $259,123Q1 FY 2011 43 175 24.6% 3.0 5.6 $7,090 $304,877Q2 FY 2011 40 207 19.3% 3.0 5.8 $6,604 $264,155Q3 FY 2011 28 152 18.4% 3.0 6.3 $6,744 $188,830Q4 FY 2011 31 153 20.3% 3.0 6.0 $7,223 $223,907Q1 FY 2012 43 170 25.3% 3.0 5.7 $6,977 $300,021Q2 FY 2012 38 209 18.2% 3.0 6.1 $6,255 $237,694Q3 FY 2012 37 148 25.0% 3.0 6.3 $7,796 $288,466Q4 FY 2012 45 185 24.3% 3.0 5.7 $7,849 $353,184Q1 FY 2013 32 155 20.6% 3.0 6.5 $8,499 $271,969
Need to audit? When reviewing this information, you may want to consider auditing a sample of records if you identify:• Percents (4th column in the table below) that are consistently red (high outlier) • A trend of increasing Percents over time resulting in outlier status• Your Percent is above the national 80th percentile (see graph on the following worksheet)
Three-Day SNF Qualifying Admissions
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC32

Three-Day SNF Qualifying Admissions
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC33

Hospitalization Challenges: Appropriate Setting
Observation vs. inpatient– Patient’s medical history and current medical needs
– Types of facilities available
– Hospital by-laws and admission policies
– Relative appropriateness of treatment in each setting
– Severity of signs and symptoms exhibited by the patient
– Medical predictability of something adverse happening to the patient
– Need for diagnostic studies that appropriately are outpatient services to assist in assessing whether the patient should be admitted
– Availability of diagnostic procedures at the time and location where the patient presents
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC34

Hospitalization Challenges: Appropriate Setting
Observation vs. inpatient
– An order simply documented as “admit” will be treated as an inpatient admission.
– A clearly worded order such as “inpatient admission” or “place patient in outpatient observation” will ensure appropriate patient care and prevent hospital billing errors.
– Order for observation must include rationale.
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC35

Hospitalization Challenges: Appropriate Setting
Inpatient vs. outpatient
– More than 20% of 2011 improper payments: inpatient claim denied, yet would have been payable in outpatient setting (source: 2011 CERT report)
– Resulted in A/B Rebilling Demonstration (now ended)
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC36

Hospitalization Challenges: Appropriate Setting
Readmission rates– “For conditions with both large numbers of stays and high
readmission rates, Medicare and especially Medicaid patients were more likely to be readmitted than privately insured or uninsured patients. For example, congestive heart failure readmission rates were
30.1% for Medicaid,
25.0% for Medicare,
19.5% for privately insured, and
17.1% for uninsured.”
– Source: AHQR Statistical Brief #153, April 2013
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC37

Hospitalization Challenges: Appropriate Setting
Changing scene– “Although diagnostic cardiac catheterizations was the fifth
most common procedure in 2010, the rate of hospitalization with this procedure decreased 23 percent since 1997.”
– “Rates of hospitalization with knee replacement and spinal fusion approximately doubled between 1997 and 2010.”
– Source: AHQR Statistical Brief #149, February 2013
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC38

Home Health Benefit
In 2012:
– Number of beneficiaries that received home health services: 3.5 million
– Number of home health agencies involved in providing this care: approx. 12,000
– Cost to the Medicare program for these home health services: approx. $18.2 billion
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC39

Home Health Benefit
Requirements for payment/coverage: CMS Pub. 100-02, chapter 7, section 20.1.1:
– “… payment can be made only if a physician certifies the need for services and establishes a plan of care.”
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC40

Home Health Benefit
Requirements for payment/coverage: Social Security Act (section 1814(a)(2)(C) and 1835(a)(2)(A)) - beneficiary must:
– Be confined to the home;
– Be under the care of a physician;
– Be receiving services under a plan of care established and periodically reviewed by a physician;
– Be in need of skilled nursing care on an intermittent basis or physical therapy or speech-language pathology; or
– Have a continuing need for occupational therapy.
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC41

Home Health Benefit
Physician must certify that patient is confined to his/her home. This means:
– Does not have to be bed-ridden
– Has “normal inability” to leave home, so leaving home would require a “considerable and taxing effort”
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC42

Home Health Benefit
Physician must certify that patient is confined to his/her home. This means:
– May still be considered homebound if absences from home are “infrequent or for periods of relatively short duration, or are attributable to the need to receive health care treatment,” including:
Adult day center, to receive medical care
Ongoing outpatient dialysis
Outpatient chemotherapy or radiation therapy
– Occasional absences permissible (e.g., visit to barber, walk around the block, attend wedding)
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC43

Home Health Benefit
Physician (or allowed NPP) must document face-to-face encounter with patient
Documentation requirements (Pub. 100-02, chapter 7, section 30.5.1.1):
– Date of face-to-face encounter and brief narrative by physician to describe “how the patient’s clinical condition as seen during that encounter supports the patient’s homebound status and need for skilled services”
– Document, sign and date encounter OR on addendum to certification
– May be dictated or generated from EMR
– May NOT be dictated to home health agency then signed by physician
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC44

Home Health Benefit
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC45

Home Health Benefit
Codes to consider for reimbursement for physician’s time (must maintain documentation):
– Care Plan Oversight: HCPCS codes G0181, G0182
Billing guidelines: CMS Medicare Claims Processing Manual (Pub. 100-04), chapter 12, sections 80 and 80.1
– Transitional Care Management: CPT codes 99495-99496
Billing guidance: CMS FAQs for transitional care management
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC46
CPT only copyright 2012 American Medical Association. All rights reserved. CPT is a registered trademark of the American Medical Association. Applicable FARS\DFARS Restrictions Apply to Government Use.

Physician’s Key Role
Coding
Clinical review judgment
Consistency across disciplines
Cloning, EMR, templating, and scribing
Certification: PT/OT/SLP plans of care, ambulance transport
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC47

Physician’s Key Role
Coding
– Importance of “being there”
– Role of coders: select CPT/HCPCS codes and modifiers and ICD-9 codes based on physician’s documentation and with physician’s input
– Medical necessity as the overarching criterion
– Weight/preponderance of documentation vs. physician’s assessment of the patient’s condition and appropriateness of care
– Documentation paints the picture; reviewer must be able to follow your rationale
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC48

Physician’s Key Role
“Reasonable and necessary” standard: AMA definition– "Health care services or products that a prudent physician
would provide to a patient for the purpose of preventing, diagnosing or treating an illness, injury, disease or its symptoms in a manner that is:
In accordance with generally accepted standards of medical practice
Clinically appropriate in terms of type, frequency, extent, site, and duration, and
Not primarily for the convenience of the patient, physician, or other health care provider”
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC49

Physician’s Key Role
Eddy, et. al. Benefit language, JAMA 275(8):650-657)Eisenberg et. al., Ten lessons for evidence-based technology assessments, JAMA 282(19):1865-1875http://www.cms.hhs.gov/FACA/Downloads/recommendations.pdf http://www.ama-assn.org/ama/basic/article/177-405-1.htm l
Criteria Reasonable Necessary
Safe and effective/not investigational ++ ++
Appropriate duration & frequency: + +++
Accepted standards of medical practice ++ ++
Appropriate setting +++
Qualified personnel (order/perform) +++
Meets, but does not exceed, medicalneed
+ +++
As beneficial as existing and availablemedically appropriate alternative
+++
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC50

Physician’s Key Role
Consistency across disciplines: challenges
– Multidisciplinary environments: review and oversight of documentation
– Disconnects: patient assessments
Condition varies by day or time of day
PT/OT vs. nurse
Hospital discharge summary vs. evaluation by speech pathologist
– Conflicting documentation: problematic
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC51

Physician’s Key Role
Documentation
– Challenges around electronic medical records: cloned documentation, use of scribes, role of electronic medical records
– Timeliness, changes, and addenda
– Who gathers and copies documentation? – trained staff, timeline for responses, what to send and to whom, quality control
– Definition of an “order” for Medicare purposes – specificity, signature
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC52

Cloning
– Medical documentation is exactly the same from beneficiary to beneficiary.
– It would not be expected that every patient had the exact same problem, symptoms, and required the exact same treatment.
– This "cloned documentation" does not meet medical necessity requirements for coverage of services rendered due to the lack of specific, individual information.
Physician’s Key Role
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC53

Cloning
– All documentation in the medical record must be specific to the patient and her/his situation at the time of the encounter.
– Considered a misrepresentation of the medical necessity requirement for coverage of services.
– Identification of this type of documentation will lead to denial of services for lack of medical necessity and recoupment of all overpayments made.
Physician’s Key Role
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC54

Templating
– Medical necessity is key
– Coding Manager DOES NOT = MN
– Do NOT preset visit template
– Adapt template to patient, NOT the reverse
Physician’s Key Role
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC55

Scribes
– “Living recorder," documenting actions and words of physician in real time
– The real time transcription must be clearly documented as noted, by both the scribe and the physician.
– Scribe does not act independently
– No separate payment
– Physician is ultimately accountable for the documentation, and should sign and note after the scribe's entry the affirmation above, that the note accurately reflects work done by the physician.
Physician’s Key Role
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC56

Involvement of ancillary staff:
– CGS is seeing components of E/M services completed or updated by nursing or other medical staff in the EMR. For example: in the Past Medical or Family/Social History sections, there is an electronic note stating "updated by Nancy Jones, Medical Technician" or an electronic statement of "medication list updated by Mary Smith RN."
– Physician must also review and address these components.
– Nurse or medical technician entry without physician review and documentation: may not be used in determining the level of E/M service provided as they do not reflect the work of the physician.
Physician’s Key Role
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC57

Timeliness, changes, and addenda
– We strongly encourage all health care providers to enter information into the patient’s medical record at the time the service is provided to the patient; that is, contemporaneously.
Physician’s Key Role
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC58

In all cases, regardless of whether the documentation is maintained or submitted in paper or electronic form, any medical records that contain amendments, corrections, or addenda must:
– Clearly and permanently identify any amendment, correction or delayed entry as such, and
– Clearly indicate the date and author of any amendment, correction, or delayed entry, and
– Not delete, but instead, clearly identify all original content.
Physician’s Key Role
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC59

Physician’s Key Role
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC60

For electronic medical records:
– Amendments, corrections, and delayed entries must be distinctly identified as such, and
– The record must provide a reliable means of clearly identifying the original content, the modified content, and the date and author of each modified record.
– More info: CMS Change Request 8105, which updates the CMS Program Integrity Manual (Pub. 100-08), chapter 3, section 3.3.2.5
Physician’s Key Role
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC61

Physician’s Key Role
Medical records staff:
– Requests from multiple contractors/entities and timeline for responses: CGS job aid – “Medical Record Requests: Keys to Success”
– What to send: only what is relevant and all of what is relevant
– Quality control: legibility, two-sided records, highlighting and holes punched, review requirements (signatures, orders, test results, plans of care, prior encounters)
– Basics:
Date of service; patient’s name; signed/dated notes
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC62

Physician’s Key Role
Certification: PT/OT/SLP
– Basis: Code of Federal Regulation (42 CFR 424.24(c))
– Requirements: patient is under your care; needs treatment
– Must relate to treatment during interval on claim
– Certification:
Applies to duration of plan of care or 90 calendar days from initial treatment date, whichever is less
Timely: signed w/in 30 days of first treatment day
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC63

Physician’s Key Role
Code of Federal Regulation (42 CFR 424.24(c)) language:
(c) Outpatient physical therapy and speech-language pathology services
– (1) Content of certification.
(i) The individual needs, or needed, physical therapy or speech pathology services.
(ii) The services were furnished while the individual was under the care of a physician, nurse practitioner, clinical nurse specialist, or physician assistant.
(iii) The services were furnished under a plan of treatment that meets the requirements of § 410.61 of this chapter.
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC64

Physician’s Key Role
Code of Federal Regulation (42 CFR 424.24(c)) language:(2) Timing. The initial certification must be obtained as soon as possible after the plan is established.
(3) Signature.
– (i) If the plan of treatment is established by a physician, nurse practitioner, clinical nurse specialist, or physician assistant, the certification must be signed by that physician or nonphysician practitioner.
– (ii) If the plan of treatment is established by a physical therapist or speech-language pathologist, the certification must be signed by a physician or by a nurse practitioner, clinical nurse specialist, or physician assistant who has knowledge of the case.
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC65

Physician’s Key Role
Recertification: PT/OT/SLP
– Can be by different physician from certification
– Required whenever significant modification to plan is evident or at least every 90 days after initiation of treatment under that plan
Provisions for delayed certification
Certification/recertification by DPMs – must be consistent w/ scope of practice, as defined by state
Chiropractors not permitted to certify/recertify therapy plans of care
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC66

Physician’s Key Role
Ambulance: “Medical necessity is established when the patient’s condition is such that use of any other method of transportation is contraindicated. In any case in which some means of transportation other than an ambulance could be used without endangering the individual’s health, whether or not such other transportation is actually available, no payment may be made for ambulance services.”
– CMS Pub. 100-02, chapter 10, section 10.2.1
– See also: Code of Federal Regulations, 42 CFR 410.40(d)
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC67

Physician’s Key Role
Non-emergency transport (from CFR):
– Bed-confinement or beneficiary’s condition is such that transportation by ambulance is medically required
– CFR defines “bed confinement”; not sole criterion for coverage
– Nonemergency, scheduled, repetitive services: Physician Certification Statement (PCS) required before service is furnished; dated no earlier than 60 days prior to transport.
– Other guidelines apply to PCS for nonemergency unscheduled or nonemergency non-repetitive transports
– PCS: ICD-9 codes, statement “bed confined,” or list of conditions not sufficient
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC68

Physician’s Key Role
Know what you’re being asked to sign and why
– Question about the guidelines? – call our Provider Contact Center (866.276.9558)
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC69

MR Strategy Development
Purpose– Protect Medicare Trust Fund
– CERT Error Rate
Driven by data: quantitative and qualitative– Sources
Claims data – raw data, probes, edit effectiveness
CERT Reports
PEPPER Reports
OIG Reports
Other external reports – IOM, Kaiser, etc.
Medical literature – emerging trends, issues
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC70

MR Strategy Development: Tools, Evaluation, & Interventional Strategy
Tools:– Statistical analytics: trending, significance
– Predictive models: clustering, targeting
Evaluation:– Periodic review for effectiveness, review
– New data drill downs
– Decision process to amend strategy (add or e-focus)
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC71

MR Strategy Development: Tools, Evaluation, & Interventional Strategy
Interventional strategy:– Educational
Webinars, web postings, articles, Carrier Advisory Committee, periodic meetings with compliance officers
– Provider-specific Face to face (Provider Outreach & Education
team, CMDs), brainstorming, comparison to peers reports, edit rates)
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC72

Medical Review
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC73

Pre-payment
– Conversion to prepayment review
Significant increase in prepayment review
– Changing behavior with targeted audit/educational activities
Post-payment
Automated vs. complex
Clinical review judgment
Reviewer guidance, QA, reliability
Medical Review
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC74

Corrective Actions
• Referred to accepted by ZPIC• Notified HHH MR of situation and referring agencies for possible data analysis • Fraudulently billed $92,000 in 4 months before acceptance by ZPIC
J-15 Evolution of Corrective Action
CPT only copyright 2012 American Medical Association. All rights reserved. CPT is a registered trademark of the American Medical Association. Applicable FARS\DFARS Restrictions Apply to Government Use.
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC75

Medical Review
Clinical review judgment
– Synthesis of information to create a longitudinal clinical picture; considers many factors
– Medicare guidelines: foundation (e.g., CMS/AMA Evaluation & Management Documentation Guidelines)
– May require clinician to make clinical judgments about a claim based on his/her clinical knowledge and/or experience
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC76

Medical Review
Clinical review judgment
– Role of clinical review judgment at CGS:
Efforts to reduce the paid claims error rate
Fewer claims denied inappropriately; fewer claims appealed
Fewer “dead-end” referrals to the Zone Program Integrity Contractor (ZPIC)
Reduce the “hassle factor” for providers
Not “forgiveness” for poor/inadequate documentation
Does not include re-interpretation or reinvention of existing policy to cover the care provided
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC77

Review criteria:
– Code of Federal Regulations
– CMS Rulings
– National Coverage Determinations (NCDs)
– CMS Guidance: Internet-Only Manuals (IOM)
– Local Coverage Determinations (LCDs)
– Peer-reviewed publications
– Compendia
– Gold standards
Medical Review
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC78

Assumptions:
– Medical Review believes in the “honor system”
– The provider delivered the service billed and the documentation is accurate
– The provider submits the claim honestly
– Clinical judgment should be applied appropriately to pay the claim when payable
Medical Review
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC79

Determines whether a service is:
– A covered benefit
– Reasonable and necessary
– Accurately coded
Is not:
– A means to deny claims
– Fraud investigation
– “Street justice”
Medical Review
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC80

Current areas of focus
– Highest level office visits
– One day stays
Future areas of focus
– Cross-claim review
– Elective surgeries
– SNF qualifying admissions
– SSOE
– Predictive modeling
Medical Review
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC81

MR Tools
Statistical Sampling with Overpayment Estimation (SSOE)– What is SSOE?
Define universe of claims Select statistically valid random sample Review claims post-payment and extrapolate denial % to universe
– Use Large providers “too big to prepay” Repeated education fails Biggest “stick” in contractor toolbox 1 claim denied may represent $$$ Protracted appeals process
– Goal Dramatic change in provider behavior
82Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC

MR Innovations/Enhancements
Predictive Modeling
– A statistical, customized model for J15 based on providers’ billing behavior within a specific policy group (instead of randomly targeting individual claims at the HCPCS level)
– Based on the premise of the providers’ profit motives
Providers will try to maximize their profits but not intentionally defraud Medicare
– Combines clinical necessity with statistical guidance
83Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC

Medical Review Predictive Modeling
How is this different from the current process?
84
Traditional Approach New CGS Approach
Randomly selects and evaluates individual claims for clinical necessity documentation
Evaluates a single HCPCS code for improper billing
Approaches the issue solely from clinical necessity
Does not account for common abusive billing patternsExamples: code shifting, location shifting, and bundling
Creates a risk score to identify abusive patterns at the supplier level
Identifies providers based on their overall billing pattern; the model includes multiple HCPCS codes
Probe reviews and education will focus on multiple codes to address the supplier’s overall billing pattern, not just a single HCPCS code
Models supplier behavior, but also integrates clinical necessity and guidelines, using LCDs and NCDs
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC

Go Forth
Consider internal compliance audits
– Corrective Action Plans (CAPs)
Monitor widespread data relevant to your practice
Practice-specific findings (from internal or external sources): implications for internal processes?
Tools available for your staff: staying informed
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC85

Questions?
Please complete:
– Post-test
– Participant evaluation
Revised July 18, 2013 © Copyright 2013, CGS Administrators, LLC86