The Management of Alzheimer’s Disease Laurel Coleman, MD Maine Medical Center Portland, Maine.
27
The Management of Alzheimer’s Disease Laurel Coleman, MD Maine Medical Center Portland, Maine
-
Upload
justina-hall -
Category
Documents
-
view
222 -
download
1
Transcript of The Management of Alzheimer’s Disease Laurel Coleman, MD Maine Medical Center Portland, Maine.

The Management of Alzheimer’s Disease
Laurel Coleman, MD
Maine Medical Center
Portland, Maine

Management of Alzheimer’s Disease
Managecognitive
symptoms
Manage BPSD
Support patient/family
Increased Increased quality of quality of
life for life for patient and patient and
familyfamily

Pharmacologic Options for AD
• Cognitive enhancers─ 2 classes
• Cholinesterase inhibitors (ChEIs)• NMDA-receptor antagonist
─ Do not cure the disease or reverse cognitive impairment
─ Can improve cognition and functional ability─ Reduce the rate of decline 9-12 months (ChEIs)─ Delay in nursing home placement was 17-21
months (ChEIs)
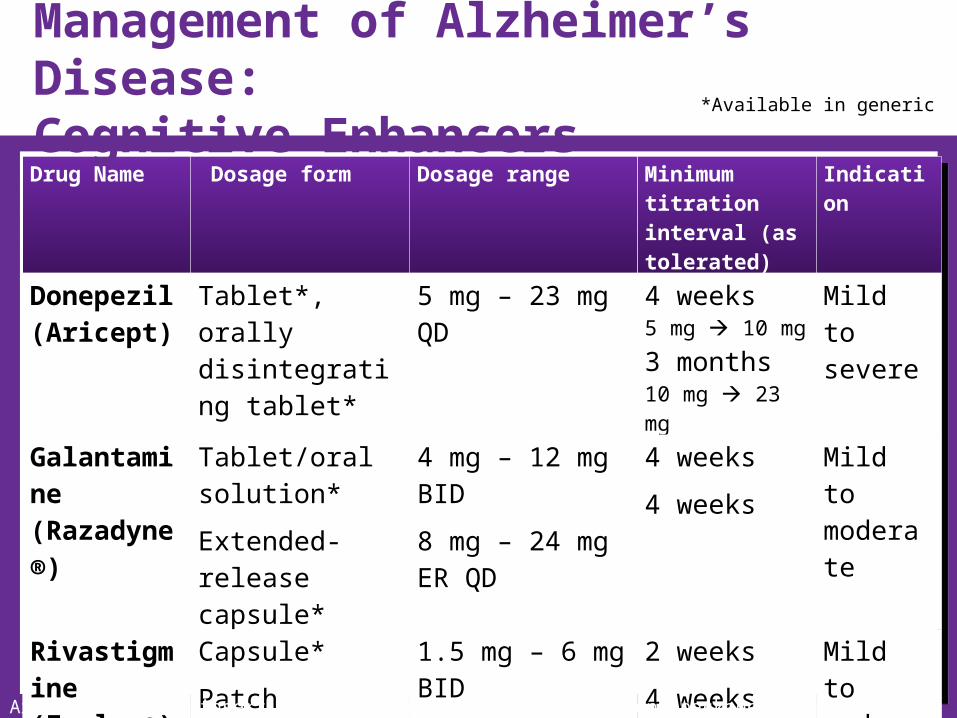
Drug Name Dosage form Dosage range Minimum titration interval (as tolerated)
Indication
Donepezil(Aricept)
Tablet*, orally disintegrating tablet*
5 mg – 23 mg QD 4 weeks5 mg 10 mg
3 months10 mg 23 mg
Mild to severe
Galantamine(Razadyne®)
Tablet/oral solution*
Extended-release capsule*
4 mg – 12 mg BID
8 mg – 24 mg ER QD
4 weeks
4 weeks
Mild to moderate
Rivastigmine(Exelon®)
Capsule*
Patch
1.5 mg – 6 mg BID
4.6 mg – 9.5 mg QD
2 weeks
4 weeks
Mild to moderate
Memantine(Namenda®)
Tablet*, oral solution*
5 mg – 10 mg QD 1 week Mod to severe
*Available in generic
Aricept® package insert. Razadyne® package insert. Exelon® package insert.
Management of Alzheimer’s Disease: Cognitive Enhancers

Cholinesterase inhibitors(Donepezil, galantamine, rivastigmine)
NMDA-receptor antagonist(Memantine)
• Nausea• Vomiting• Diarrhea• Weight loss• Loss of appetite• Muscle weakness• Vivid dreams/nightmares
(donepezil)
• Dizziness• Headache• Constipation• Confusion
Aricept® package insert. Razadyne® package insert. Exelon® package insert.
Pharmacologic Options for ADCommon Side Effects

Switching ChEIs
Lack or loss of therapeutic benefit
Tolerability issues
Noncompliance
Immediate switchNo washout needed
Washout period of 1-2 weeks before
starting another agent
Try an alternate dosage form before
switching

Discontinuation of Therapy
• Data for optimal duration of treatment as disease progresses is limited─ Modest cognitive and functional benefits associated with continued
therapy with (donepezil) in moderate to severe AD1
─ Discontinuation associated with adverse behavioral changes and reduced participation in activites2
• Consider discontinuation in the following situations:─ Inability to tolerate multiple ChEIs─ No improvement or greater than expected decline after one or
more therapeutic trials─ End-stage dementia
1. Howard et al. New Engl J Med. 2012;366:893-903. 2. Daiello et al. Am J Geriatr Pharmacother. 2009;7:74-83.

Impact of Coexisting Medical Conditions
Cognitive Impairment
2.4 conditions/ptHTN 82%DM 39%CAD 21%CHF 14%Stroke 10%
Schubert CC, et al. J Am Geriatr Soc. 2006;54(1):104–109.
Prevalence of coexisting conditions in PWD

Impact of Coexisting Medical Conditions
• PWD in primary care average 5.1 medications/pt1 ─ 50% take ≥1 anticholinergic medications
• Medications with anticholinergic activity─ Impairs cognition acutely (delerium) and
chronically2
• Anticholinergic burden
─ Interfere with the therapeutic effect of ChEIs3
1. Schubert CC, et al. J Am Geriatr Soc. 2006;54(1):104–109. 2. Campbell N, et al. Clin Interv Aging. 2009;4:225–233.3. Lu C, Tune LE. Am J Geriatr Psychiatry. 2003;11(4):458–461.
Behavioral and Psychological Symptoms of Dementia (BPSD)
• Apathy • Depressive symptoms• Anxiety• Agitation/irritability/
aggression• Psychotic symptoms
─ Delusions─ Hallucinations
• Disinhibition• Euphoria• Loss of appetite• Sleep disturbances• Stereotyped
behaviors (eg, pacing, wandering, rummaging, picking
Tampi et al. Clinical Geriatrics. 2011;19:41-46.

Managing BPSD
• Identify triggers─ Observe symptom timing and frequency─ Look for environmental triggers, eg noise, lighting─ Investigate potentially treatable causes, eg pain
• Make adjustments─ Address medical causes─ Adapt environment─ Adapt caregiving
• Modify as needed

Managing BPSDNonpharmacological Interventions
• Use the “3 Rs”—repeat, reassure, redirect
• Simplify the environment, task, routine
• Anticipate unmet needs
• Allow adequate rest between stimulating events
• Use cues
• Encourage physical activity
• Other interventions

Managing BPSD:Pharmacologic InterventionsDrug class Chemical name Dosage
range (mg)Side effects of class
Antipsychotics Aripiprazole*HaloperidolRisperidone*Quetiapine*Olanzapine*
2.5-150.5-50.25-225-2002.5-15
Sedation, EPS, NMS, metabolic syndrome, QTc prolongations, increased risk of CVE and mortality
Antidepressants FluoxetineCitalopramParoxetineSertralineTrazadone
10-8010-6010-5025-20025-200
Anxiety, headaches, sedation, GI symptoms, sexual dysfunction
Mood stabilizers CarbamazepineDivalproex sodiumOxcarbazepine
100-400250-1000300-600
Sedation, gait and balance issues, falls, liver dysfunction, hyperammonemia, thrombocytopenia
Adapted from Tampi et al. Clin Geriatr. 2011;19:31-32.
*2nd-generation antipsychotics
Alzheimer’s Disease
Education of Patientand Family

Education of Patient and Family
• Safety issues:─ Home environment─ Driving ─ Medication adherence─ Financial exploitation─ Elder abuse
• Address future needs: financial planning, advanced directives, power of attorney
Cindy Porter
Need more notes

Education of Patient and FamilyMedications
• Define treatment success─ Symptomatic benefit in
• Cognition• Physical function and ADLs• Behavior
─ Increases time to nursing home placement
• Discuss length of therapy─ Adequate trial is 6 months
Cummings JL. Am J Geriatr Psychiatry. 2003;11(2):131–145.Doody RS, et al. Arch Neurol. 2001;58(3):427–433.

Impact on CaregiversTasks Change Over Time
Early stage•Help with IADLS, eg, paying bills and preparing meals•Cope with mood swings and reluctance to engage
Mid stage•Help with ADLS, eg, dressing and toileting•Cope with increased memory loss, sleep disturbances, wandering, loss of driving
Late stage•Help with all personal care•Cope with unresponsiveness and end-of-life issues

Education of Patient and FamilyAlzheimer’s Association• 24/7 Nationwide Helpline
─ 800.272.3900─ Information and referral in 170 languages
• www.alz.org─ Current reliable information for healthcare professionals, people
with dementia, family members and caregivers
• 300 local offices─ Information and referral─ Support groups─ Care consultation─ Safety services─ Education, local conferences
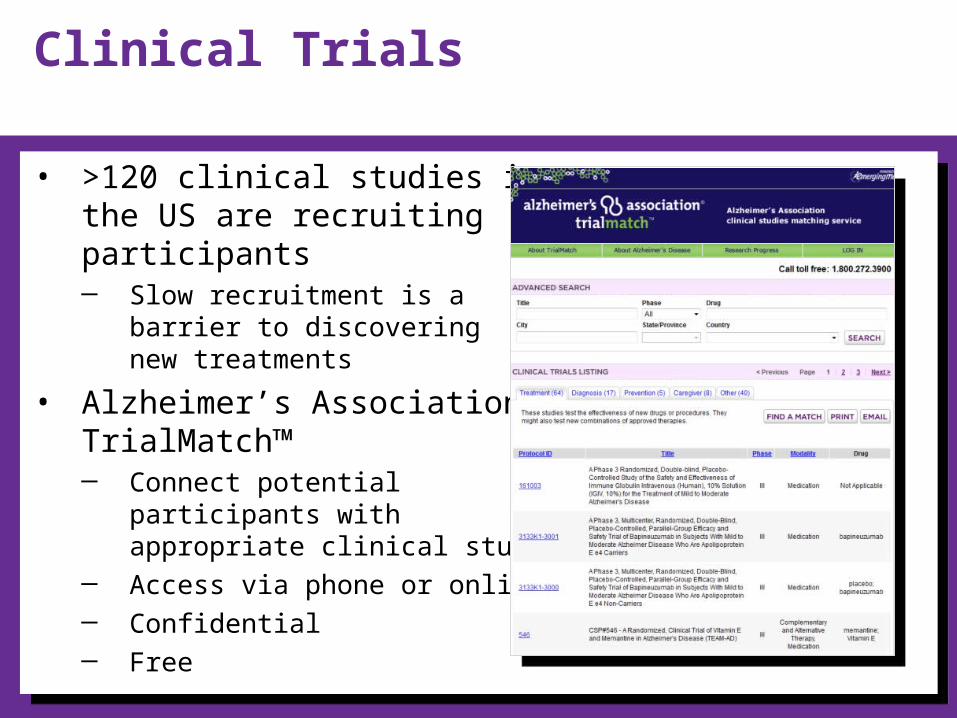
Clinical Trials
• >120 clinical studies in the US are recruiting participants─ Slow recruitment is a
barrier to discovering new treatments
• Alzheimer’s Association TrialMatch™─ Connect potential
participants with appropriate clinical studies
─ Access via phone or online─ Confidential─ Free

Understanding prevention research
• Much evidence comes from large epidemiological studies that show associations, not proof
• Study results apply to populations, not individuals
• Large randomized studies for many prevention strategies unlikely─ Cost prohibitive

PreventionFactors with a consistent association
• Heart-head connection
• Preventative drug treatments
• Physical exercise
• Diet
• Social connections
• Intellectual activity
• Head trauma prevention

PreventionFactors with a consistent association
Increased risk of AD
• Conjugated equine estrogen with progesterone*
• Diabetes• Depression• Smoking
Decreased risk of AD
• Physical activity• Mediterranean diet• Cognitive engagement
*Moderate evidence, all other factors had low evidence
The Future of Alzheimer’s Disease
• Earlier recognition─ Dependent on reliable biomarkers
• New medications─ Current medications only address symptoms─ New medications in development
• Disease-modifying therapy• Combination disease-modifying and symptomatic
therapy
• Prevention
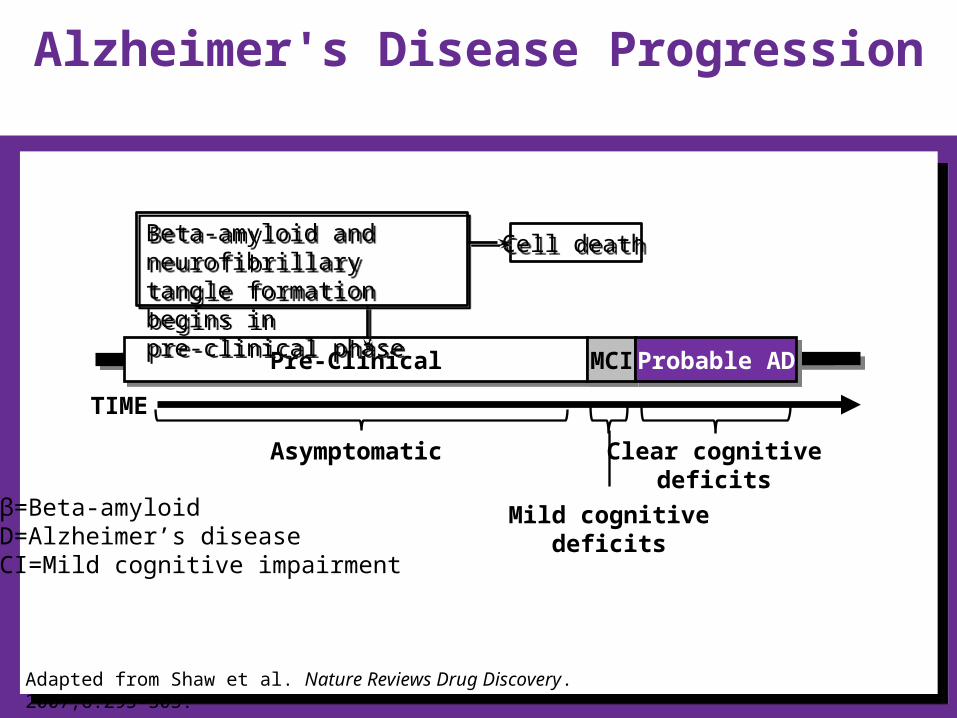
TIME
Pre-ClinicalPre-Clinical MCIMCI Probable ADProbable AD
Asymptomatic
Cell deathCell death
Alzheimer's Disease Progression
Adapted from Shaw et al. Nature Reviews Drug Discovery. 2007;6:295-303.
Aβ=Beta-amyloidAD=Alzheimer’s diseaseMCI=Mild cognitive impairment
Beta-amyloid and neurofibrillary tangle formation begins in pre-clinical phase
Beta-amyloid and neurofibrillary tangle formation begins in pre-clinical phase
Clear cognitive deficits
Mild cognitive deficits

Targets for Future Therapies
• A─ -secretase inhibitors─ -secretase inhibitors─ Monoclonal antibodies
• Tau protein
• Inflammation
• Insulin resistance
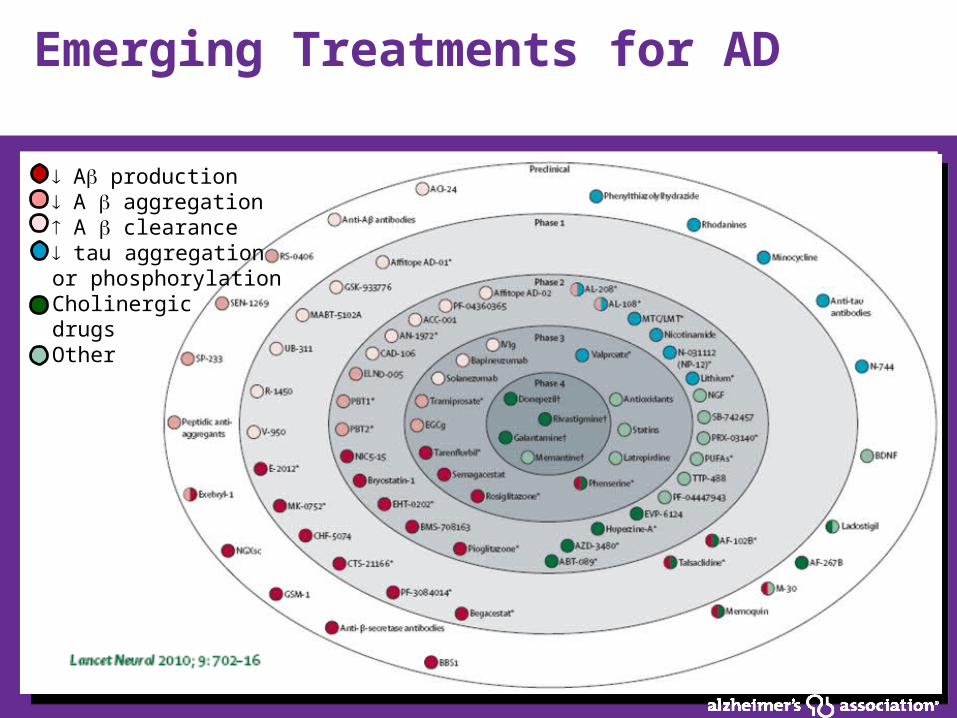
Emerging Treatments for AD
A production A aggregation A clearance tau aggregation or phosphorylationCholinergic drugsOther

Clinical Trials
Failed Phase 2 Moving to Phase III
Phase III
AN-1792 ACC-01 Lu AE58054 Solanezumab
Bapineuzumab Crenezumab EVP-6124 IVIg
Dimebon
Rosiglitazone
Semagacestat
Tarenflurbil
Tramiprosate