
The International Legal Implications of the General ... · 10500 12000 Billio n $ Goods ......
84
Trade in Health Services & the General Agreement on Trade in Services (GATS) IMPLICATIONS FOR HEALTH POLICY Nick Drager M.D., Ph.D. Senior Adviser World Health Organization
Transcript of The International Legal Implications of the General ... · 10500 12000 Billio n $ Goods ......

Trade in Health Services&
the General Agreement on Trade in Services (GATS)
IMPLICATIONS FOR HEALTH POLICY
Nick Drager M.D., Ph.D.Senior Adviser
World Health Organization
2
Trade in Health Services and GATS
trade in health servicesunderstanding the GATS agreementmanaging the GATS negotiation processkey issues for policy makers

3
Co-contributors
Julia Nielson- Senior Trade Policy Analyst, OECDDavid Fidler – Professor of Law, Indiana UniversityRichard Smith – Senior Lecturer Health Economics, University of East AngliaRolf Adlung and Mireille Cossy –WTO Secreteriate

4
Growth of goods and services exports
1980/2000
0
100
200
300
400
1980 82 84 86 88 90 92 94 96 98
2000
Perc
enta
ge (
1980
=100
)
01500300045006000750090001050012000
Billi
on $
Goods Services
Services growth
Goods growth
GDP growth

5
10 largest cross-border M&A deals concluded in health services, 2000
Acquired
company Industry
Host
country Acquiring company Industry
Home
country
Transaction
Value ($
million)
Kuwait Invest Off-
Hospitals(3)
medical and
surgical
hospitals
United
Kingdom Columbia/HCA Healthcare Corp
General medical and
surgical hospitals United States 151
St Martins
Healthcare Ltd
medical and
surgical
hospitals
United
Kingdom HCA-Healthcare Co
General medical and
surgical hospitals United States 150
Total Renal Care
Hldgs-Intl
Kidney
dialysis
centers
United
States Fresenius AG
Electromedical and
electrotherapeutic
apparatus Germany 145
ImmGenics Inc
Medical
laboratories Canada Abgenix Inc
g p ,
except diagnostic
substances United States 77SHL Telemedicine
Ltd
Home health
care services Israel Koninklijke Philips Electronic
Household audio and
video equipment Netherlands 40Undisclosed Long
Term Care
Skilled
nursing care
United
States CPL Long Term Care Real Estate
Real estate investment
trusts Canada 39
Clinovia Ltd
Home health
care services
United
Kingdom LVL Medical Groupe
Home health care
services France 39
(Serologicals
Corp)
allied
services, nec
United
States Aventis SA
Health and allied
services, nec France 21
Clinica San Camilo
medical and
surgical
hospitals Spain United Surgical Partners Intl
General medical and
surgical hospitals United States 16

6
Trade in Health Services Globalization of Health
cross border delivery- telemedicine; e-healthconsumption abroad- patients travelling across borders for diagnosis and treatmentcommercial presence- establishments of hospitals, clinics through FDI, joint ventures, alliances, mergersmovement of personnel- doctors and nurses practising in other countries

7
Health implications ofcross border delivery of services
mode 1
Opportunitiesenable health care delivery to remote and underserviced areas -promoting equityalleviate some human resource constraintsenable more cost -effective surveillance of diseasesimprove quality of diagnosis and treatmentupgrade skills, disseminate knowledge through interactive electronic means
Risksgiven lack of telecommunications and power sector infrastructure -telemedicine may not be cost effectivecapital intensive, possible diversion of resources from basic preventive and curative serviceshurt equity if it caters to a small segment of the population- urban affluent

8
Health implications of consumption abroad
mode 2Opportunities
for exporting countriesgenerate foreign exchange earnings to increase resources for healthupgrade health infrastructure, knowledge, standards and qualityfor importing countriesovercome shortages of physical and human resources in speciality areasreceive more affordable treatment
Riskscreate dual market structure may crowd out local population -unless these services are made available t local populationdiversion of resources from the public health systemoutflow of foreign exchange for importing countries

9
Health implications of commercial presence
mode 3
Riskslarge initial public investments needed to attract FDIif public funds/subsidies used - potential diversion of resources from the public health sectortwo tier structure of health care establishmentsinternal brain drain from public to private sectorcrowding out of poorer patients, cream skimming phenomena
Opportunitiesgenerate additional resources for investment in upgrading of infrastructure and technologiesreduce the burden on public resources create employment opportunitiesraise standards, improve management, quality , improve availability, improve education (foreign commercial presence in medical education sector)

10
Health implications of movement of personnel
mode 4
Opportunitiesfrom the sending country
promote exchange of knowledge among professionalsupgrade skills and standards (provided service providers return to the home country)gains from remittances and transfers
from host countrymeet shortage of health care providers, improve access, quality and contain cost pressures
RisksFrom sending country
permanent outflows of skilled personnel -brain drainloss of subsidised training and financial capital investedadverse effects on equity, availability and quality of services

11
Implication of Globalization of Health Services
impact of liberalised trade in services on the access to, cost, quality of serviceswhat policies, regulations should be in place to ensure that trade in health services increases equity in health and is in the interest of those in greatest needwhat collective action across countries, at regional and global level is needed to take advantages of emerging global opportunities and mitigate potential risks – work towards policy coherence
12
General Agreement on Trade in Services (GATS)
GATS is one of the most important trade agreements to emerge from the Uruguay Round negotiations that created the World Trade Organization (WTO)
→Services are one of the fastest growing areas for many economies→Services of many kinds play important roles in the protection and
promotion of health→GATS provides the multilateral legal framework for liberalizing
international trade in services
GATS creates numerous challenges for people working in public health
→GATS is a complex legal agreement that borrows from existing international trade law to create new rules for services
→GATS has become the subject of significant controversy, especially with respect to how the Agreement will affect health-related services and health policy

13
““Tale of Two TreatiesTale of Two Treaties”” ProblemProblem
Debate about GATS’ impact on health policy has created a “tale of two treaties” problem for health policy communities
–GATS is the worst of treaties—GATS undermines the exercise of national sovereignty for health purposes–GATS is the best of treaties—GATS respects health sovereignty through its flexibility, which allows each WTO member to shape its obligations according to its national needs and interests
The “tale of two treaties” problem makes it difficult for the health policy communities to understand how the complex law of GATS may or may not affect their work

14
Legal Architecture of GATSLegal Architecture of GATS
Does a health-related service fall within the scope of GATS?
GATS rules that apply to health-related services within GATS’ scope
General Obligations
Specific Commitments
ProgressiveLiberalization
InstitutionalFramework

15
Scope of GATSScope of GATS
GATS’scope
Measures Affecting Trade inServices

16
What is covered by the AgreementWhat is covered by the Agreement
Measures affecting trade in services: measures related to production, distribution, marketing, sale and delivery of a service and can take any form : laws regulations, rules, procedures, decisions, administrative actions
GATS also applies to measures taken by central, regional or local governments and to NGOs where they are exercising delegated powers

17
Trade in ServicesTrade in Services
Trade inservices
Cross-bordersupply of services
(Mode 1): telemedicine
Consumption of services abroad
(Mode 2): hospitaltreatment overseas
Presence of naturalpersons (Mode 4):nurses working inother countries
Commercialpresence (Mode 3):establishment ofhealth facilities
abroad

18
GATS and Health Sovereignty: GATS and Health Sovereignty: Significant OverlapSignificant Overlap
Scope of GATS
HealthProfessional
EnvironmentalDistribution
FinancialBusiness
R&D
Scope of health sovereignty
Health-related services

19
Controversial Question: Controversial Question: Does GATS Apply to Does GATS Apply to
GovernmentGovernment--Provided Services?Provided Services?
Significant controversy about whether GATS applies to government-provided servicesGATS excludes “services supplied in the exercise of governmental authority”The “GATS and health” controversy involves disagreement among experts about how broad or limited the exclusion for “services supplied in the exercise of governmental authority” isThis controversy has not yet been authoritatively determined, meaning the scope of this exclusion is ambiguous – no interest so far in narrowing this exclusion

20
Threshold Question: Threshold Question: Does GATS Apply?Does GATS Apply?
Is the health-related service supplied by the government?
Is the health-related service supplied on a commercial basis?
Is the health-related service supplied in competition with
one or more service providers?
Is the health-related servicesupplied by a private actor
pursuant to delegated governmental authority?
GATS applies to measuresof WTO members that affect
trade in health-related services
No
YesYes
NoNo
Yes
GATS does not apply
No
Yes
START

21
Unfinished BusinessUnfinished Business
More time needed to undertake negotiations to determine whether or what type of discplines are necessary – ongoing negotiations
Government procurement- some provisions (MFN, MA/NT in sector commitments) do not apply e.g. hiring of temporary foreign nurses by a government department of health to address shortages in public hospitalsSubsidies- no specific disciplines to date-negotiations on disciplines to avoid trade distortive effect of subsidies
22
Entering the House of GATSEntering the House of GATS
GATS(Services)
Health Sovereign
ty

23
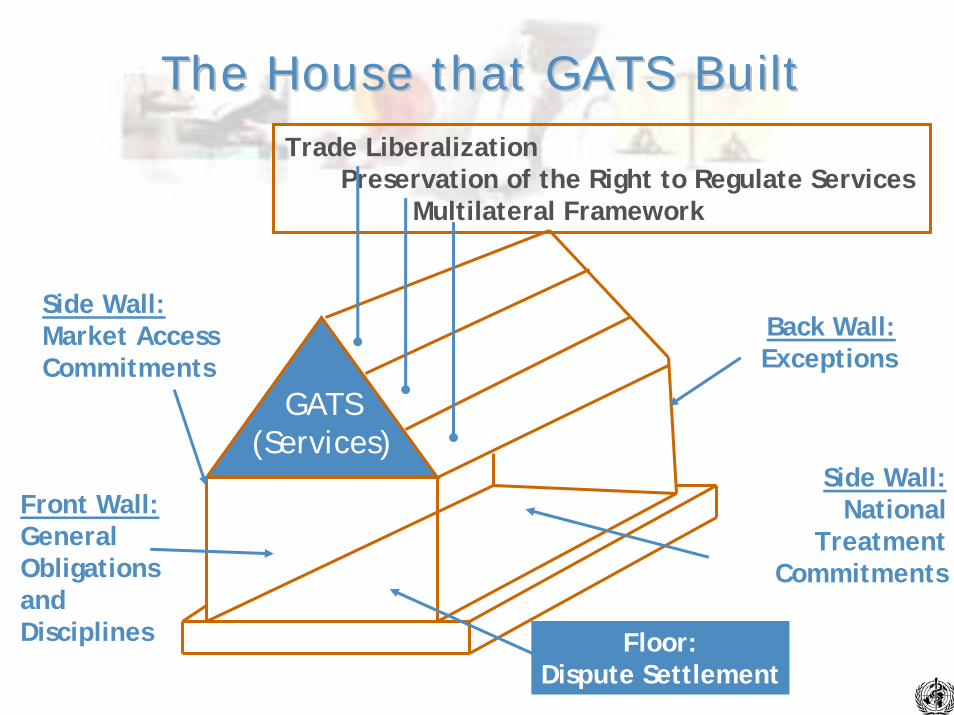
The House that GATS BuiltThe House that GATS Built
GATS(Services)
Trade LiberalizationPreservation of the Right to Regulate Services
Multilateral Framework of Rules

24
The House that GATS BuiltThe House that GATS Built
GATS(Services)
Trade LiberalizationPreservation of the Right to Regulate Services
Multilateral Framework
Front Wall:GeneralObligationsandDisciplines

25
General Obligations and DisciplinesGeneral Obligations and Disciplines
General Obligations and Disciplines
SubstantiveDuties
ProceduralDuties

26
Substantive DutiesSubstantive Duties
Substantive Duties
Most-Favored-NationPrinciple
Duties Affecting Domestic Regulatory
Powers
Rules not linked to specificcommitments
Rules that apply only to servicescovered by specific commitments

27
Rules Affecting Domestic Regulatory Rules Affecting Domestic Regulatory Powers:Powers:
ControversiesControversiesRules affecting domestic regulatory powers linked to specific commitments
– Article VI:5 on domestic regulations requires that licensing, qualification, and technical standards not be applied in manner that is not transparent, is more burdensome than necessary, and could not have reasonably been expected at the time the specific commitment was made
– Article VIII on monopoly service providers regulates how a WTO member may grant monopoly or exclusive service rights in a sector covered by a specific commitment
28
The Article VI:4 ControversyThe Article VI:4 Controversy
Article VI:4 requires WTO members to engage in negotiations to develop disciplines on licensing, qualification, and technical standard regulationsThe disciplines shall aim to ensure that regulations are– Based on objective and transparent criteria– Not more burdensome than necessary– In the case of licensing procedures, not in themselves a
restriction on the supply of services
No negotiations on disciplines affecting a health-related service have occurred or been proposed

29
Procedural DutiesProcedural Duties
Procedural Duties
Duties to provide information and toestablish government procedures
Duties to participate in negotiationsand/or consultations
Generallyapplicableprovisions
Provisionsrelated tospecific
commitments
Duties to negotiate
multilateral rules
Duties toconsult and cooperate

30
Summary on General Summary on General Obligations and DisciplinesObligations and Disciplines
Present impact of general obligations and disciplines of GATS on health sovereignty is not significant– General obligations that are universally binding are not large in
number or worrying from a health-policy perspective– Low level of specific commitments made in health-related
sectors mitigates the impact of general obligations linked to specific commitments
More concerns will arise in the future as the level and nature of specific commitments in health-related sectors may increase and as WTO members negotiate multilateral disciplines on trade in services

31
The House that GATS BuiltThe House that GATS Built
GATS(Services)
Trade LiberalizationPreservation of the Right to Regulate Services
Multilateral Framework
Front Wall:GeneralObligationsandDisciplines
Side Wall:Market AccessCommitments

32
The House that GATS BuiltThe House that GATS Built
GATS(Services)
Trade LiberalizationPreservation of the Right to Regulate Services
Multilateral Framework
Front Wall:GeneralObligationsandDisciplines
Side Wall:Market AccessCommitments
Side Wall:National Treatment
Commitments
33
CommitmentsCommitments
Liberalizing under the GATS means undertaking specific commitments on market access and national treatmentCommitments are recorded in national schedulesMembers can chose the sectors in which they want to undertake commitments (GATS does not require the liberalisation of health services)Absence of commitments does not necessarily mean absence of trading opportunities

34
Commitments do not AffectCommitments do not Affect
Non-discriminatory domestic regulation- (standards, licensing requirements, universal service obligations, etc.) Government procurement decisionsPrivate commercial actions

35
Scheduling and Modifying Scheduling and Modifying Specific CommitmentsSpecific Commitments
National schedules of specific commitments form part of the binding treaty, so the drafting of such schedules is very importantIn addition, GATS contains rules that make modifying schedules of specific commitments difficult because the rules require compensation for those WTO members adversely affected by the modification(s)

36
Specific CommitmentsSpecific Commitments
Countries decide which service sectors they want to allow foreign suppliers to enter and under what conditionsCommitments (guaranteed minimum treatment offered to other WTO members) in individual schedules -countries free to offer better treatment if they wish – but not worse)A list of 12 service sectors (160 subsectors ) was developed (not obligatory to use)Four possible modes

37
Defining the Health SectorDefining the Health Sector
Health related and social services: hospital services; other human health services, social servicesProfessional services: medical and dental services; services provided by mid-wives, nurses physiotherapists and para medical personnel

38
Modes of SupplyModes of Supply
Trade inservices
Cross-bordersupply of services
(Mode 1): telemedicine
Consumption of services abroad
(Mode 2): hospitaltreatment overseas
Presence of naturalpersons (Mode 4):nurses working inother countries
Commercialpresence (Mode 3):establishment ofhealth facilities
abroad

39
Horizontal vs. Horizontal vs. Sectoral CommitmentsSectoral Commitments
Commitments can be made for each sector or covering a single mode of supply across all sectors listed in their schedule (unless otherwise specified)
Horizontal commitments can be used to include important conditions which apply to all sectors in the schedule

40
Commitments Commitments cont'dcont'd
For each service sector or sub sector and for each mode of supply countries make commitments as to the level of market access and national treatment
Informs foreign suppliers about the access they will have to the market and any special conditions that
will apply to them as foreigners

41
CommitmentsCommitments3 Main Choices3 Main Choices
Full market access and /or national treatment for a particular mode- that is to maintain no restriction-indicated in the schedule by none
No commitment to provide anything on MA/NT for a particular mode – unbound
Partial commitments for MA/NT listing restrictions

42
Market AccessMarket Access
Commitments set out the conditions under which foreign suppliers are allowed to enter the market
Countries can chose to place no restrictions on market access (none) or to make no commitment (unbound) or to allow access subject to limitations and conditions (partial commitment)

43
Market Access RestrictionsMarket Access RestrictionsCan only be maintained if listed in the schedule. Can apply to both
national and foreigners or only foreignersRestrictions on the number of service suppliers- no of hospitalsRestrictions on the total value of service transactions or assets-foreign private clinics must not have assets worth more then USD50 millionRestrictions on the total number of service operations or the total quantity of service output – no. of surgical operations or hospital beds) Restrictions on the total number of natural persons that may be employed in a particular service sector or that a service supplier may employ – no. of doctors and nurses employedRestrictions on or requirements for certain types of legal entity or joint venture for the supply of a service- foreign private clinic must enter into a joint venture with a local clinic to enter into the marketLimitations on the participation of foreign capital in terms of maximum percentage limit on foreign shareholding or the total value of individual or aggregate foreign investment- foreign private clinic is limited to 30% of the equity in the newly established private clinic

44
National TreatmentNational Treatment
Foreign services and service suppliers are granted treatment no less favourable then that accorded to like national services and service suppliers
Likeness – WTO DU on a case by case basis taking into account consumer perceptions of the degree to which a particular good is like and its substitutability

45
National Treatment LimitationsNational Treatment Limitations
No specific list – members must judge whether a measure breaches national treatment and have to be scheduled
Measure may not be considered discriminatory if it is genuinely open to both nationals and foreigners to fulfil i.e. language proficiency
Examples of the types of measures that need to be listed in the schedule as limitations: eligibility for subsidies reserved to nationals; the ability to own land reserved to nationals, citizenship requirements for certain health professionals

46
How Schedules of Commitments How Schedules of Commitments are structured: Singaporeare structured: Singapore
Modes of supply: 1) Cross-border supply 2) Consumption abroad 3) Commercial presence 4) Presence of natural persons Sector or subsector
Limitations on market access
Limitations on national treatment
Additional commitments
Medical Services
1) Unbound* 2) None 3) None, other than the
number of new foreign doctors registered each year may be limited depending on the total supply of doctors
4) Unbound except as
indicated in the horizontal section
1) None 2) None 3) None 4) Unbound
*Unbound due to lack of technical feasibility

47
How Schedules of Commitments How Schedules of Commitments are structured: Indiaare structured: India
Modes of supply: 1) Cross-border supply 2) Consumption abroad 3) Commercial presence 4) Presence of natural persons Sector or subsector
Limitations on market access
Limitations on national treatment
Additional commitments
Hospital Services (CPC 9311)
1) Unbound* 2) Unbound 3) Only through
incorporation with a foreign equity ceiling of 51 per cent
4) Unbound except as
indicated in the horizontal section
1) Unbound 2) Unbound 3) None 4) Unbound except as
indicated in the horizontal section
*Unbound due to lack of technical feasibility

48
The House that GATS BuiltThe House that GATS Built
GATS(Services)
Trade LiberalizationPreservation of the Right to Regulate Services
Multilateral Framework
Front Wall:GeneralObligationsandDisciplines
Side Wall:Market AccessCommitments
Side Wall:National TreatmenCommitments
Back Wall:Exceptions
49
The House that GATS BuiltThe House that GATS Built
GATS(Services)
Trade LiberalizationPreservation of the Right to Regulate Services
Multilateral Framework
Front Wall:GeneralObligationsandDisciplines
Side Wall:Market AccessCommitments
Side Wall:National
TreatmentCommitments
Back Wall:Exceptions
Floor:Dispute Settlement

50

51
GATS Legal Review: Further GATS Legal Review: Further Documents and InformationDocuments and Information
Legal Review of the General Agreement on Trade in Services (GATS) from a Health Policy Perspective. Geneva: WHO, 2004. [xxx] pp. Also available at: www.who.int/. “The International Legal Implications of GATS for Health Sovereignty,” in Handbook on Trade in Health-Related Services and GATS. Geneva: WHO, 2004, at pp. []-[]. Also available at www.who.int/. GATS and Health-Related Services: Managing Liberalization of Trade in Services from a Health-Policy Perspective. Geneva: WHO, 2004, 7 pp. Also available at www.who.int/. WHO web site on GATS and health: www.who.int/.
52
Managing the Managing the GATS Negotiation ProcessGATS Negotiation Process
Threshold issues
10 step flow chart for decision making
Intragovernmental coordination

53
Four Policy Issues to ConsiderFour Policy Issues to Consider
Public, private or both? – whether and to what extent the private sector can participate in the provision and financing of health servicesNational or foreigners? – whether to allow participation by foreign service suppliersTrade vs. trade agreements – whether to make GATS commitments/RTAs/bilateral Liberalisation is not synonymous with de-regulation – regulation should be in place before market opening

54
Threshold IssuesThreshold Issues
Nationals or foreigners?– Can have only national private supply– Why include foreigners – e.g., to increase efficiency via
competition, meet key shortages in short-term, access other technologies or skills, increase available services
– BUT how ensure quality, impact local system.
Many issues same for national, as well as foreign private supply.
GATS only interested in foreign – not privatisation per se.

55
Threshold IssuesThreshold Issues
Trade vs. trade agreements
– Trade, and the regulatory challenges that accompany it, will be there without GATS
Many policies to manage this trade fall outside of GATS
– Why make GATS commitments? Attract FDI, flexibility vs. certainty
– Possible regional angle?Global vs. regional interests
56
Threshold IssuesThreshold Issues
Liberalisation and regulation– Liberalisation is NOT de-regulation but often re-regulation– Harder to regulate liberalised market, but failure also in
monopolies– Liberalisation must be underpinned by appropriate
regulationHuge challenge for some countriesEnforcement capacity also

57
Making Commitments under the Making Commitments under the GATS Agreement: Flow ChartGATS Agreement: Flow Chart
Implications of making commitments/guide to request market opening from other WTO members
10 (not so) easy stepsStop at any stageDo we understand what we are doing?Is this giving us what we want in terms of health policy outcomes?

58
Flow ChartFlow Chart
STEP ONE: Work out what is actually what on the table to request or offer– Excluded:
Governmental services: – Unfinished business: nothing at the moment
Government ProcurementSubsidies
STEP 2: Decide if I want to exclude health services from my GATS commitments- what basic obligations still apply?– Substantive duties- MFN– Procedural duties - Transparency

59
Flow ChartFlow Chart
STEP 3: If I want to make or request commitments decide how to define the scope of the health services I want covered by my request or commitment
W/120 – WTO 12 sectors and 160 subsectorsCPC- UNOwn definition (some WTO members underline the private commercial- not public- nature of the services for which access is being offered)
STEP 4: Decide if I want to include all ways of delivering health services in my request or commitment or not- or whether any existing or new horizontal commitments might be relevant
Modes of supplyHorizontal vs. sectoral commitments

60
Flow ChartFlow Chart
STEP 5: Decide what kind of commitment I want to make and what sort of conditions I want to place on foreign suppliers.– What does market access mean?
Monopolies?
– What does national treatment meanSubsidies for nationals but not foreigners
– Is a commitment necessarily liberalisation?– Do commitments start now?– As a developing country, do I have to liberalise?

61
Flow ChartFlow Chart
In summary, you can:– Exclude all or some health services– Exclude some modes of supply– Limit market access– Put additional conditions on foreign suppliers– Treat some foreign suppliers better than others (If
RTA or MFN exemption)– Commit to less than current access– Commit to liberalise in the future– Developing countries can open fewer sectors and
attach conditions
62
Flow ChartFlow Chart
STEP 6: Do other general obligations “kick in” once a commitment is made on health services? -procedural
→Transparency. notify new or changed measures annually to WTO
→Timely decisions on authorisations→Reasonable, objective, impartial
administration of measures→For professional services, adequate
procedures for verifying competence.

63
Flow ChartFlow Chart
STEP 7: What about the impact on how I regulate health services?
→GATS recognises the right to regulate and to introduce new regulations- regulatory framework still applies
→Additional regulatory requirements can be put in place for foreigners – foreign doctors can be required to undertake an additional year's training before being permitted to practice
→When no commitments are made - general obligations re transparency and MFN apply , and additional general ones where commitments made
→Certain types of measures (non-discriminatory, not market access, licensing and qualification requirements and procedures,technical standards) possibly be subject to additional disciplines developed under VI.4

64
RecognitionRecognition
GATS does not require recognition of the professional qualifications of other members nor does it require any particular standards to be appliedGATS allows members to recognise the qualifications of some WTO members and not others – i.e. permits countries to break the MFN rule in relation to recognition WTO members free to recognise the qualifications of some members and not others - must notify recognition agreements they are negotiating and give other interested WTO members the opportunity to prove that they meet the same standards.

65
Flow ChartFlow Chart
STEP 8: What if I change my mind? What if I no longer want to keep a commitment?
→Renegotiation of commitments - compensation→Suspend commitments for balance of payments
difficulties; emergency safeguards- under negotiation
→Exceptions to justify and defend its actions if challenged by another WTO member- necessary to protect human, animal or plant health

66
Flow ChartFlow Chart
STEP 9: What happens next?→Progressive liberalisation, not inexorable march
to a free market – remain free to keep service sector closed to foreign suppliers
→Flexibility for developing countries to extend market access progressively in line with their development situation and when granting market access to attach conditions to fulfil development objectives.

67
Flow ChartFlow Chart
STEP 10: A final thought→Dialogue, consultation, coordination→Can the GATS help us to achieve any
desired health policy outcomes?→How might we need to regulate that trade
to achieve our objectives?And do we have the regulatory capacity to do it?

68
Domestic Policy CoordinationDomestic Policy Coordination
What is the mechanism for coordination?– Working groups, contact points
Is the health authority involved in discussions on all sectors or just the health sector?How good is the mutual understanding and what steps have been taken to improve it?– Meetings, seminars, papers, joint consultations
Follow up mechanisms – Data collection, monitoring
Role of international organisations– Including WB and IMF
Involvement of other groups nationally?

69
Services NegotiationsServices Negotiations
Mandated by the GATS - started in 2000→Achieve progressively higher level of liberalization→Due respect for national policy objectives and levels
of development→Flexibility for developing countries
Negotiating guidelines and procedures adopted in March 2001
→No a priori exclusion of any sector or mode→No change to the structure and principles of the
GATS

70
Negotiating TimetableNegotiating TimetableDOHA MINISTERIAL DECLARATIONDOHA MINISTERIAL DECLARATION
Submission of initial requests by end of June 2002Submission of initial offers by end of March 2003Stock taking - Cancun 2003Conclusion not later than 1st January 2005 as part of DDA single undertaking: unlikely to be met- General Council decision Aug 2004 –intensify negotiations on rules and revised offers – review progress and full report for purpose of Sixth Ministerial meeting (Hong Kong - 2005)

71
0
20
40
60
80
100
120
140
160
DevelopedDeveloping
Sector Focus of Current Sector Focus of Current CommitmentsCommitments
(Developed/Developing Country Members, August 2003)

72
Progressive Liberalization and Progressive Liberalization and Health PolicyHealth Policy
WHO members will face decisions whether to liberalize trade in services through market access and national treatment commitments, including trade in health-related servicesGATS 2000 round of liberalization negotiations potentially affects health policy in two areas:– Evaluating requests from other countries for, and
offers to other countries of, specific commitments for market access and national treatment
– Negotiations on GATS rules

73
Managing the GATS Process from a Managing the GATS Process from a Health Policy Perspective: Health Policy Perspective:
PrinciplesPrinciplesLiberalized trade in health-related services should lead to an optimal balance between preventive and curative servicesInvolvement of both private industry and civil society is important to ensure that liberalization of health-related services promotes participatory health policyImproving access and affordability of health-related services should be a goal of liberalization of trade in health-related servicesDeveloping countries, and least-developed countries in particular, deserve special consideration in the process of liberalizing trade in health-related servicesThe status of health as a human right should inform and guide proposals to liberalize trade in health-related services.
74
Managing the GATS Process from a Managing the GATS Process from a Health Policy Perspective:Health Policy Perspective:
Key QuestionsKey QuestionsTo what extent is the sector already open to foreign service providers, and what have been the regulatory concerns posed by existing foreign competition?Do the commitments fit the strategies and directions identified by national health policy?What effect would the commitments have on government-provided health services?What regulatory burdens would the commitments create for the government in health-related sectors?Would the commitments eliminate or weaken regulatory approaches necessary for the protection and promotion of health?What evidence and principles can be brought to bear to analyze the possible effect of the commitments?Can the commitments be crafted both to protect health policy andto liberalize trade progressively?
75
Managing the GATS Process from a Managing the GATS Process from a Health Policy Perspective:Health Policy Perspective:
Check ListCheck ListIdentify a focal point for trade in health-related services within the Ministry of HealthEstablish contacts and systematic interactions with trade and other key ministries and with representatives from private industry and civil societyCollect and evaluate information on the effect of existing trade in health-related services within the countryObtain legal advice on GATS and other international agreements that may affect trade in health-related servicesDevelop a sustainable mechanism for monitoring the impact of trade in health-related servicesUtilize the assistance provided by the WHO on matters concerningtrade in health-related servicesSubject all requests for, and offers of, liberalization of trade in health-related services, to a thorough assessment of their health policy implications
76
Managing the GATS Process from a Health Managing the GATS Process from a Health Policy Perspective:Policy Perspective:
WHO RecommendationsWHO Recommendations
Get Your House in Order: National stewardship of the health system in the context of GATS requires a sophisticated understanding of how trade in health-related services already affects and may affect a country’s health systems and policy.
Know the Whole House Not Just Select Rooms: The GATS process can affect many sectors that related to health, which places a premium on health ministries understanding the importance of a comprehensive outlook on trade in health-related services.

77
Managing the GATS Process from a Health Managing the GATS Process from a Health Policy Perspective:Policy Perspective:
WHO RecommendationsWHO Recommendations
Remember Who Owns the House: GATS provides countries with choices and does not force them to make liberalization commitments that are not in their best interests. If a country is unsure about the effects of making specific commitments, it is fully within its rights to decline to make legally binding commitments to liberalize, or to liberalize unilaterally without making binding commitments.
Home Improvement Means Health Improvement: Health principles and criteria should drive policy decisions on trade in health-related services in the GATS negotiations.

78
Trade in Health Services and GATSTrade in Health Services and GATSImplications for Health Policy Implications for Health Policy
risks and opportunities of trade liberalisation/restrictioninternational rules and national health sovereignty government carve out - to what extent does it applygeneral exception to health - what flexibility in implementation potential new disciplines- domestic regulations, government procurement, emergency safeguards and subsidiesnew commitments in health and other sectors -insurance, telecommunications, transport, water

79
Informing the Negotiation ProcessInforming the Negotiation ProcessElements of Country AssessmentElements of Country Assessment
amount/value of exports and imports of health services in each modeexisting barriers to this tradethe objectives or interests (whose) served by these barrierscurrent national policies governing this trade: multilateral, regional and bilateral commitmentspotential gains/losses resulting from changes in health services trade : (changing barriers to the import or export of health services)

80
Elements of Country Assessment Elements of Country Assessment cont'dcont'd
import/export goals- how deep to liberalise/restrict; to which countries - gain market access, lower barrierswhat complementary domestic polices/regulations are needed to mitigate adverse effects and take advantage of opportunities - more opening /privatization- stronger regulatory systemliberalisation in other sectors affecting health-financial, professional, education, telecommunications, environmental serviceswhat should be legally bound

81
Macroeconomic and Macroeconomic and Trade EnvironmentTrade Environment
TIHS GATS
Current status
HealthPolicy
Capitalinfrastructure
Humanresources
Infrastructure ®ulatory capacity
GATS TIHS
Impact ofcurrent trade
Data sources andavailability
Current data/info& evidence
Mode 1 Mode 2(as mode 1)
Mode 3(as mode 1)
Mode 4(as mode 1)
State of domestic health care system
Macroeconomic and trade environment

82
Mode 4 ReceivingMode 4 Receiving
Most fall outside – happening anywayGATS options
Require training programs for nationalsEqual pay and conditions‘facilitate recognitionNegotiate bilateral agreements/codes of conductPermanent migration issue
Possible flanking measures
Reduced pressure to address underlying reasons for shortagesLoss for needy countriesPotential for exploitation
Possible costs
Meet key shortagesGain additional expertise
Benefits

83
Mode 4 Sending Mode 4 Sending
Some outside GATSSeek additional commitments on good regulatory practices
GATS options
Return of service requirementsTraining levy or bondEnhanced opportunities at homeNegotiate agreements with receiving countriesProblem of permanent migration
Possible flanking policies
Risk of permanent lossShort term loss of scarce skillsLoss of investment
Possible costs
Enhanced skills on returnRemittances
Possible benefits

84
Scope of Scope of AAnalysisnalysissp
ecifi
c co
mm
itmen
ts
Cross-industrial commitment
Bus
ines
sT
elec
omm
unic
atio
n
Con
stru
ctio
nD
istr
ibut
ion
Env
iron
men
tFi
nanc
eE
duca
tion
Hea
lth &
Soci
al se
rvic
es
Cul
ture
&sp
ort
Tou
rism
/Cou
rier
Tra
nspo
rtat
ion
Oth
e rs
National treatment
Market access
1. CB 2. CA3. CP 4. PN
Stew
ards
hip
Resour
ce ge
nera
tive
Serv
ice pr
ovisi
on
Financ
ing
1122
334411
2233
44


















