The Gamma Secretase Inhibitor MRK-003 Attenuates Pancreatic Cancer Growth … · 1999. 11. 9. ·...
12
Preclinical Development The Gamma Secretase Inhibitor MRK-003 Attenuates Pancreatic Cancer Growth in Preclinical Models Masamichi Mizuma 1 , Zeshaan A. Rasheed 2 , Shinichi Yabuuchi 1 , Noriyuki Omura 1 , Nathaniel R. Campbell 1 , Roeland F. de Wilde 1 , Elizabeth De Oliveira 2 , Qing Zhang 3 , Oscar Puig 3 , William Matsui 2 , Manuel Hidalgo 2 , Anirban Maitra 1,2 , and N.V. Rajeshkumar 2 Abstract Pancreatic ductal adenocarcinoma (PDAC) is a lethal malignancy, with most patients facing an adverse clinical outcome. Aberrant Notch pathway activation has been implicated in the initiation and progression of PDAC, specifically the aggressive phenotype of the disease. We used a panel of human PDAC cell lines as well as patient-derived PDAC xenografts to determine whether pharmacologic targeting of Notch pathway could inhibit PDAC growth and potentiate gemcitabine sensitivity. MRK-003, a potent and selective g -secretase inhibitor, treatment resulted in the downregulation of nuclear Notch1 intracellular domain, inhibition of anchorage-independent growth, and reduction of tumor-initiating cells capable of extensive self-renewal. Pretreatment of PDAC cells with MRK-003 in cell culture significantly inhibited the subsequent engraftment in immunocompromised mice. MRK-003 monotherapy significantly blocked tumor growth in 5 of 9 (56%) PDAC xenografts. A combination of MRK-003 and gemcitabine showed enhanced antitumor effects compared with gemcitabine in 4 of 9 (44%) PDAC xenografts, reduced tumor cell proliferation, and induced both apoptosis and intratumoral necrosis. Gene expression analysis of untreated tumors indicated that upregulation of NF-kB pathway components was predictive of sensitivity to MRK-003, whereas upregulation in B-cell receptor signaling and nuclear factor erythroid-derived 2-like 2 pathway correlated with response to the combination of MRK-003 with gemcitabine. Our findings strengthen the rationale for small-molecule inhibition of Notch signaling as a therapeutic strategy in PDAC. Mol Cancer Ther; 11(9); 1999–2009. Ó2012 AACR. Introduction Pancreatic ductal adenocarcinoma (PDAC) is one of the most devastating human malignancies characterized by extensive local invasion, early systemic dissemination, and pronounced resistance to chemotherapy and radio- therapy (1). Outcomes for patients with advanced PDAC remain poor with limited clinical benefits seen with cur- rently available therapy. For example, gemcitabine as a systemic agent in the treatment of advanced PDAC results in a median survival of less than 6 months. A recent phase III trial of a combination regimen comprised of oxaliplatin, irinotecan, fluorouracil, and leucovorin (FOLFIRINOX) as first-line therapy has been shown to significantly improve median survival compared with gemcitabine alone in patients with advanced PDAC (2). Nonetheless, the safety profile of FOLFIRINOX was less favorable than that of gemcitabine, and many patients remain ineligible to receive FOLFIRINOX (3). Despite these ongoing advances, the continued poor survival in advanced PDAC under- scores the need for new systemic therapies. Notch signaling is an evolutionarily conserved path- way that plays an important role in multiple cellular and developmental processes (4). Although the Notch path- way plays a pivotal role in normal cell development, aberrant Notch signaling pathway has been extensively linked to a range of human malignancies, rendering this pathway a compelling target for drug development (5, 6). Activation of canonical Notch signaling involves a series of proteolytic processing steps following ligand binding. The interaction of Notch ligands (Jagged and Delta-like) with their receptors promotes g -secretase–dependent cleavage of the Notch receptor and release of the Notch intracellular domain, which translocates to the nucleus, a requirement for activation of gene targets. Accumulating evidence supports the use of small-molecule inhibitors of Authors' Affiliations: Departments of 1 Pathology and 2 Oncology, Johns Hopkins University School of Medicine, Baltimore, Maryland; and 3 Infor- matics and Analysis, Merck Research Laboratories, Kenilworth, New Jersey Note: Supplementary data for this article are available at Molecular Cancer Therapeutics Online (http://mct.aacrjournals.org/). Note: Current address for M. Mizuma: Division of Hepato-Biliary Pancreatic Surgery, Department of Surgery, Tohoku University Graduate School of Medicine, Seiryo-machi, Aoba-ku, Sendai, 980-8574, Japan. Email: [email protected] Corresponding Author: N.V. Rajeshkumar, Department of Oncology, Johns Hopkins University School of Medicine, 1650 Orleans Street, Room 485, Baltimore, MD. Phone: 410-502-8774; Fax: 410-614-9006; E-mail: [email protected] doi: 10.1158/1535-7163.MCT-12-0017 Ó2012 American Association for Cancer Research. Molecular Cancer Therapeutics www.aacrjournals.org 1999 on July 1, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from Published OnlineFirst July 2, 2012; DOI: 10.1158/1535-7163.MCT-12-0017
Transcript of The Gamma Secretase Inhibitor MRK-003 Attenuates Pancreatic Cancer Growth … · 1999. 11. 9. ·...
-
Preclinical Development
The Gamma Secretase Inhibitor MRK-003 AttenuatesPancreatic Cancer Growth in Preclinical Models
Masamichi Mizuma1, Zeshaan A. Rasheed2, Shinichi Yabuuchi1, Noriyuki Omura1, Nathaniel R. Campbell1,Roeland F. de Wilde1, Elizabeth De Oliveira2, Qing Zhang3, Oscar Puig3, William Matsui2, Manuel Hidalgo2,Anirban Maitra1,2, and N.V. Rajeshkumar2
AbstractPancreatic ductal adenocarcinoma (PDAC) is a lethal malignancy, with most patients facing an adverse
clinical outcome. Aberrant Notch pathway activation has been implicated in the initiation and progression
of PDAC, specifically the aggressive phenotype of the disease. We used a panel of human PDAC cell lines
as well as patient-derived PDAC xenografts to determine whether pharmacologic targeting of Notch
pathway could inhibit PDAC growth and potentiate gemcitabine sensitivity. MRK-003, a potent and
selective g-secretase inhibitor, treatment resulted in the downregulation of nuclear Notch1 intracellulardomain, inhibition of anchorage-independent growth, and reduction of tumor-initiating cells capable of
extensive self-renewal. Pretreatment of PDAC cells with MRK-003 in cell culture significantly inhibited the
subsequent engraftment in immunocompromised mice. MRK-003 monotherapy significantly blocked
tumor growth in 5 of 9 (56%) PDAC xenografts. A combination of MRK-003 and gemcitabine showed
enhanced antitumor effects compared with gemcitabine in 4 of 9 (44%) PDAC xenografts, reduced tumor
cell proliferation, and induced both apoptosis and intratumoral necrosis. Gene expression analysis of
untreated tumors indicated that upregulation of NF-kB pathway components was predictive of sensitivityto MRK-003, whereas upregulation in B-cell receptor signaling and nuclear factor erythroid-derived 2-like
2 pathway correlated with response to the combination of MRK-003 with gemcitabine. Our findings
strengthen the rationale for small-molecule inhibition of Notch signaling as a therapeutic strategy in
PDAC. Mol Cancer Ther; 11(9); 1999–2009. �2012 AACR.
IntroductionPancreatic ductal adenocarcinoma (PDAC) is one of the
most devastating human malignancies characterized byextensive local invasion, early systemic dissemination,and pronounced resistance to chemotherapy and radio-therapy (1). Outcomes for patients with advanced PDACremain poor with limited clinical benefits seen with cur-rently available therapy. For example, gemcitabine as asystemic agent in the treatment of advancedPDAC results
in amedian survival of less than 6months. A recent phaseIII trial of a combination regimen comprised of oxaliplatin,irinotecan, fluorouracil, and leucovorin (FOLFIRINOX) asfirst-line therapy has been shown to significantly improvemedian survival compared with gemcitabine alone inpatients with advanced PDAC (2). Nonetheless, the safetyprofile of FOLFIRINOX was less favorable than that ofgemcitabine, and many patients remain ineligible toreceiveFOLFIRINOX(3).Despite theseongoingadvances,the continued poor survival in advanced PDAC under-scores the need for new systemic therapies.
Notch signaling is an evolutionarily conserved path-way that plays an important role in multiple cellular anddevelopmental processes (4). Although the Notch path-way plays a pivotal role in normal cell development,aberrant Notch signaling pathway has been extensivelylinked to a range of human malignancies, rendering thispathway a compelling target for drug development (5, 6).Activation of canonical Notch signaling involves a seriesof proteolytic processing steps following ligand binding.The interaction of Notch ligands (Jagged and Delta-like)with their receptors promotes g-secretase–dependentcleavage of the Notch receptor and release of the Notchintracellular domain, which translocates to the nucleus, arequirement for activation of gene targets. Accumulatingevidence supports the use of small-molecule inhibitors of
Authors' Affiliations: Departments of 1Pathology and 2Oncology, JohnsHopkins University School of Medicine, Baltimore, Maryland; and 3Infor-matics and Analysis, Merck Research Laboratories, Kenilworth, NewJersey
Note: Supplementary data for this article are available at Molecular CancerTherapeutics Online (http://mct.aacrjournals.org/).
Note:Current address forM.Mizuma:Division ofHepato-Biliary PancreaticSurgery, Department of Surgery, Tohoku University Graduate School ofMedicine, Seiryo-machi, Aoba-ku, Sendai, 980-8574, Japan. Email:[email protected]
Corresponding Author: N.V. Rajeshkumar, Department of Oncology,Johns Hopkins University School of Medicine, 1650 Orleans Street, Room485, Baltimore, MD. Phone: 410-502-8774; Fax: 410-614-9006; E-mail:[email protected]
doi: 10.1158/1535-7163.MCT-12-0017
�2012 American Association for Cancer Research.
MolecularCancer
Therapeutics
www.aacrjournals.org 1999
on July 1, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 2, 2012; DOI: 10.1158/1535-7163.MCT-12-0017
http://mct.aacrjournals.org/
-
g-secretase (GSI) as a tractable avenue for Notch antago-nism against a number of cancers linked with increasedpathway activity (7, 8).
Several lines of preclinical evidence suggest that sus-tained activation of Notch signaling pathway contributesto the initiation and maintenance of PDAC (9). For exam-ple, in primary PDAC tissues, as well as in noninvasiveprecursor lesions of adenocarcinoma, multiple pathwaycomponents, including Notch ligands, receptors, and tar-get genes are overexpressed, relative to normal pancreas(10). In an autochthonous mouse model of PDAC, phar-macologicNotch inhibition attenuates thedevelopment ofintraductal precursor lesions and invasive cancer, impli-cating this pathway in tumor initiation (11). Furthermore,downregulation of Notch receptors by RNA interferenceor exposure toGSI in establishedhumanpancreatic cancercells results in reduced proliferative rates, increased apo-ptosis, decreased anchorage-independent growth, anddecreased invasive properties, suggesting a role forNotchsignaling in PDAC maintenance as well (11, 12).
In this study, we assessed the effects of MRK-003, apotent and selective GSI (13, 14), in preclinical models ofPDAC. MRK-003 is the preclinical analog of MK-0752, aGSI that is currently in clinical development (15, 16). Weused a panel of human PDAC cell lines, as well aspatient-derived PDAC xenografts, to determine wheth-er pharmacologic targeting of the Notch pathway usingMRK-003 could curb tumor growth and potentiate gem-citabine sensitivity. Herein, we also attempt to delineatea gene signature of responsiveness to Notch inhibition,which may aid in the selection of patient subsets morelikely to benefit from this strategy in the clinic.
Materials and MethodsDrugs
MRK-003 was provided by Merck Research Laborato-ries. Gemcitabine (Eli Lilly)was purchased from the JohnsHopkins Hospital Pharmacy. Structures of MRK-003 andgemcitabine are shown in Fig. 1 (17, 18).
Cell linesAuthenticated low-passage PDAC lines (Pa03C, Pa14C,
Pa16C, and Pa29C), established at Johns Hopkins, wereused for the study. Culture conditions and exome-widesomatic mutational status of these cell lines has beenpreviously described (19). In addition, we used Capan-1[American Type Culture Collection (ATCC)] on the basisof its Notch dependence (12). Cell line provider (ATCC)used cytochrome c oxidase I PCR assay, short tandemrepeat profiling, and Ouchterlony diffusion method tocharacterize the cell line.
Quantitative real-time reverse transcription PCRCells were collected after incubation with MRK-003 (2
or 5 mmol/L) for 48 hours. Total RNAwas extracted usingRNeasy Mini Kit (Qiagen). cDNA was synthesized withSuperScript First Strand System (Invitrogen). qRT-PCRwas conducted using FAST SYBR Green Master Mix(Applied Biosystems) on a Step One Plus Real-Time PCRSystem (Applied Biosystems). Human PGK1 and murineb-actinwere used as housekeeping genes. Relative expres-sion of themRNAwas estimated using the 2�DDCTmethod(20).
Anchorage-independent growthAnchorage-independent growth of cells was deter-
mined by soft agar assays in 6-well plates. Briefly, cellswere incubated inmedia containing 0.5%FBSwith vehicleorMRK-003 (2 or 5mmol/L).After incubation for 48hours,the treated cells were recovered by media with 10% FBSfor 24 hours. Thereafter, equal numbers of viable cellsfrom each condition were quantified using a hemocytom-eterwith trypanblue counterstain, and thenplated for softagar assays. A bottom layer of 1% agarose, a middle layerof 0.6% agarose including 10,000 cells and a top layer ofmedium only were applied into each well. After incubat-ing the plates for 3 weeks, colonies were stained withcrystal violet solution, visualized by trans-UV illumina-tion and counted using the analysis software QuantityOne (BioRad).
Stable overexpression of Notch1 intracellulardomain
Stable transfectants overexpressing the Notch1 intra-cellular domain (N1ICD) was established in Pa03C cells,as previously described (12). The stable transfectantsweremaintained in media supplemented with 600 mg/mL ofG418. Mock vector was transfected as a control. Over-expression of N1ICD comparedwith empty vector–trans-fected cells was confirmed by qRT-PCR (12).
Protein extraction and Western blottingBothN1ICD stable transfected as well as empty vector–
transfected Pa03C cells were cultured separately in tissueculture flasks. Cells were trypsinized and cell pellets werelysed using lysis buffer. Western blots were conducted aspreviously described (21). Membranes were incubatedwith primary antibodies against rabbit N1ICD (Val1744)
N
N
NH2
OO
OH
H
F
F
HH
HO
NSHN
CF
A B3O
O
N CF3
Figure 1. Chemical structures ofMRK-003 and gemcitabine.MRK-003 (A)and gemcitabine (B).
Mizuma et al.
Mol Cancer Ther; 11(9) September 2012 Molecular Cancer Therapeutics2000
on July 1, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 2, 2012; DOI: 10.1158/1535-7163.MCT-12-0017
http://mct.aacrjournals.org/
-
and Hes-1 (Cell Signaling Technology, Inc. and Abcam,respectively). Membranes were probed with secondaryHRP-conjugated antibody (GE Healthcare) and boundantibodies were detected by SuperSignal West Pico/Femto chemiluminescent substrate (Thermo Scientific).Equal loading was verified with b-actin antibody.
Engraftment of ex vivo pretreated PDAC cells inathymic miceMale athymic nude mice (6-week-old, Harlan) were
housed and maintained in accordance with the Institu-tional Animal Care and Use Committee and guidelines ofthe Association for Assessment and Accreditation of Lab-oratory Animal Care International. PDAC cells were trea-ted ex vivowith either vehicle orwithMRK-003 (5mmol/L)for 48 hours, followed by a recovery in full serum condi-tions for an additional 24 hours, before subcutaneousinjection. Viable 5 � 106 cells in a total volume of 200 mLof 1:1 (v/v) PBS/Matrigel (BD Biosciences) were injectedsubcutaneously into bilateral flanks (right flank, cellspretreated with vehicle; left flank, cells pretreated withMRK-003) ofmice (N¼ 6). Tumor sizewasmeasuredwithdigital calipers.
FACS analysis of tumor-initiating cells(CD44þCD24þ and ALDHþ cancer cells)PDAC cells were treatedwithMRK-003 (2 or 5 mmol/L)
for 48 hours. The cells were harvested and stained withALDEFLUOR.Briefly, 1million cellswere resuspended in1mLALDEFLUORbuffer and 1mLALDEFLUOR reagentin the presence or absence of theALDH1 inhibitor, diethy-lamino-benzaldehyde (DEAB), for 30 minutes in a 37�Cwater bath. The cells were washed and incubated at 4�Cfor 15minutes withmonoclonal anti-CD44-allophycocya-nin (APC) (1:20 dilution; clone G44-26, BD Biosciences)and anti-CD24-phycoerythrin (PE) (1:20 dilution; cloneML5, BD Biosciences) antibodies. The cells were washedand resuspended in ALDEFLUOR buffer containing2 mg/mL propidium iodide (PI). A FACSCalibur flowcytometer (BD Biosciences) was used for flow cytometricanalysis, as previously described (22). The cells were firstgated on the basis of side-scatter and forward-scatterproperties, followed by exclusion of nonviable (PI-positive) cells. The ALDHþ gate was created on the basisof DEAB-treated cells stained with ALDEFLUOR, anti-CD24-PE, and anti-CD44-APC. The CD44þCD24þ gateswere created on the basis of cells stained with ALDE-FLUOR, mouse-specific IgG2b k-APC (1:100 dilution; BDBiosciences) and IgG2a k-PE (1:100 dilution; BD Bios-ciences) antibodies (22, 23). Gates were created on thebasis of cellular staining with isotype control antibodies.FACS plots for these controls are shown as Supplemen-tary Fig. S1.
Notch1 gene expressionRNA isolated from baseline (untreated) tumors of 30
individual patient-derived pancreatic cancer xenograftswas profiled using Affymetrix U133 Plus 2.0 gene arrays.
Sample preparation and processing procedure was con-ducted as described in the Affymetrix GeneChip Expres-sion Analysis Manual (Affymetrix, Inc.). Gene expressionlevels were converted to a rank-based matrix and stan-dardized for each microarray (23).
Xenograft establishment and in vivo efficacy studiesLow-passage PDAC xenografts, established at Johns
Hopkins Hospital, were used for the study (24). Nineindependent patient-derived xenografts were selectedfor the in vivo efficacy study, based on elevated Notch1expression. Cohorts of athymic mice with tumor size ofapproximately 200 mm3 were randomized to 4 arms (5mice; 10 tumors per group): (i) vehicle control, (ii) MRK-003 150 mg/kg p.o. once weekly for 3 weeks, (iii)gemcitabine 30 mg/kg i.p. once weekly, for 3 weeks,and (iv) combination of MRK-003 and gemcitabine inthe above mentioned dose and schedule. Tumor sizewas evaluated twice weekly and tumor volume wascalculated using the following formula: tumor volume¼ (length � width2)/2.
Histology, immunohistochemistry, and fluorescencemicroscopy
Excised tumors were fixed in 10% buffered formalinbefore paraffin embedding. Immunohistochemical stain-ing of nuclear anti-Notch1 (Abcam; ab8925, 1:400 dilu-tions) and nuclear anti-Hes1 (Abcam; ab49170, 1:250 dilu-tions) were conducted as per the manufacture’s protocol.Immunohistochemistry for proliferation (Ki-67 antigen)was conducted using an anti-MIB-1 (Ki-67) antibody(clone K2, dilution 1:100, Ventana Medical Systems) aspreviously described (25). Terminal deoxynucleotidyltransferase-mediated dUTP nick end labeling (TUNEL)stainingwas done by a commercial apoptosis detection kit(DeadEnd Fluorometric TUNEL System; Promega),according to the recommendations of the manufacturer(25). We used Vectashield with 40,6-diamidino-2-pheny-lindole to preserve fluorescence and to counterstainnuclei. Sections were examined microscopically and theaverage number of cells stained positive for Ki-67 andTUNEL were counted in 5 random fields each from thetumors of 2 separate animals under at�20 magnification.
Gene expression analysisRNA isolated from the 9 parental (untreated) PDAC
xenografts was profiled using Affymetrix U133 Plus 2.0gene arrays at least in duplicates. This gene array hasapproximately 54,000 probes comprising approximately20,000 RefSeq genes. CEL files generated from the arraywere normalized using the robust multiarray averagealgorithm (26). Pearson correlation coefficients were cal-culated to identify genes that show significant correlation(P < 0.01) with tumor growth inhibition upon drug treat-ment. Pathway and biologic function analysis of gene setswas conducted using Ingenuity Pathway Analysis (IPA,Ingenuity Pathway Analysis), and overlap of gene setswith other publicly available gene signatures was
Notch Inhibition in Pancreatic Cancer
www.aacrjournals.org Mol Cancer Ther; 11(9) September 2012 2001
on July 1, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 2, 2012; DOI: 10.1158/1535-7163.MCT-12-0017
http://mct.aacrjournals.org/
-
examined using NextBio (NextBio). Microarray raw dataare available in GEO (Accession number: GSE37645).
Statistical analysisAll groups were studied in parallel and differences
between groups were analyzed by ANOVA, as appropri-ate, and Bonferroni multiple comparison tests conductedusing GraphPad Prism. The difference between experi-mental groups was considered significant when the Pvalue was
-
N1ICD and mock vectors were established in Pa03Ccells (Pa03C-N1ICD and Pa03C-mock, respectively).Stable expression of N1ICD was confirmed by upregu-lation of transcript corresponding to the ICD portion ofNOTCH1, as well as the overexpression of N1ICD andHes-1 protein compared with the mock-transfectedPa03C cells (Fig. 2D and E). Enforced N1ICD expressionper se augmented colony formation significantly com-pared with the Pa03C-mock clones in vehicle-treatedcells (Fig. 2F, P < 0.001). In Pa03C-mock cells, treatmentwith MRK-003 at 5 mmol/L reduced colony numbers byapproximately 50% (P < 0.001), whereas in Pa03C-N1ICD cells, equimolar MRK-033 attenuated colonyformation by approximately 10%, which was not statis-tically significant (Fig. 2G).
MRK-003 pretreatment delayed tumor engraftmentTo determine whether pretreatment with MRK-003
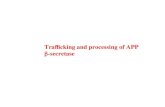
could modulate tumorigenicity in mice, we monitoredthe tumor growth of subcutaneously implanted Capan-1and Pa03C cells, which had been pretreated ex vivowitheither MRK-003 or vehicle. Engraftment was signifi-cantly delayed at day 14 and day 21 postimplantation inboth cell lines (Fig. 3A and B). In contrast, there was nodifference in engraftment rates for either Pa16C orPa29C cells, between the control andMRK-003 pretreat-ment arms (Fig. 3B). The differential sensitivity toMRK-003 was consistent with the prior data in anchor-age-independent growth obtained using this panel ofcells.
Effect of MRK-003 treatment on tumor-initiatingcells
We examined the effect of MRK-003 treatment on 2partially overlapping populations of cells, CD44þCD24þ
and ALDHþ, which have independently been associatedwith tumor-initiating properties in PDAC (22, 27). MRK-003 treatment in Capan-1 resulted in the reduction ofCD44þCD24þ tumor cells at 2 mmol/L, and eliminationof these cells at 5 mmol/L (Fig. 4A and B). A comparableobservation was noticed in the sensitive Pa03C cell line(Fig. 4B). Similarly, MRK-003 treatment reduced the pro-portion of ALDHþ cells in Capan-1 and in Pa03C (Fig. 4Aand C). However, MRK-003 treatment increased the rel-ative proportion of CD44þCD24þ and ALDHþ cells inresistant lines (Pa16C and Pa29C), respectively (Fig. 4Band C).
Effect of MRK-003 treatment on tumor growth,Notch targets, proliferation, and apoptosis
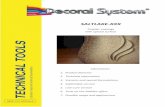
Thirty patient-derived PDACxenografts weremined insilico for relative expression ofNOTCH1 transcripts, usingmicroarray data (Fig. 5A). On the basis of the elevatedNOTCH1 expression in the baseline xenografts (relativeexpression is illustrated as red to green in order ofdecreasing values), we selected 9 individual patient-derived xenografts for further expansion in mice, andrandomization toMRK-003 or gemcitabinemonotherapy,or the combination of MRK-003 and gemcitabine. Asshown in Fig. 5B and C, MRK-003 monotherapy signifi-cantly reduced tumor volume in 5 of 9 xenografts (56%) as
B Capan-1
0 1 2 3 40
1,000
2,000
3,000VehicleMRK-003
Weeks
Tu
mo
r vo
lum
e (m
m3 )
Tu
mo
r vo
lum
e (m
m3 )
0
1,000
2,000
3,000
Tu
mo
r vo
lum
e (m
m3 )
Tu
mo
r vo
lum
e (m
m3 )
Pa03CCapan-1 Pa03C
0 1 2 3 4
Vehicle
MRK-003
Weeks
**
**
****
Pa16C
0 1 2 3 40
200
400
600
800Vehicle
MRK-003
Weeks
Pa29C
0 1 2 3 40
500
1,000
1,500VehicleMRK-003
Weeks
0 1 2 3 4
**
**
****
4
**
**
****
A
Figure 3. Ex vivo pretreatment with MRK-003 significantly inhibits engraftment in mice. A, representative photographs of mice injected with MRK-003pretreated Capan-1 and Pa03C cells (tumor generated from vehicle and MRK-003 pretreatment-treated cell lines are on the right and left side of mice,respectively). B, tumor growth curves show thatMRK-003 pretreatment significantly delayed engraftment inCapan-1 andPa03Ccells (��,P < 0.01) comparedwith the tumor generated from vehicle-treated cells. However, MRK-003 pretreatment did not impact the engraftment of Pa16C or Pa29C compared with thetumors generated from vehicle-treated cells.
Notch Inhibition in Pancreatic Cancer
www.aacrjournals.org Mol Cancer Ther; 11(9) September 2012 2003
on July 1, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 2, 2012; DOI: 10.1158/1535-7163.MCT-12-0017
http://mct.aacrjournals.org/
-
compared with control, which were Panc374 (P < 0.05),Panc219 (P < 0.05), Panc265 (P < 0.001), Panc420 (P < 0.01),and JH033 (P < 0.01). Moreover, there was a significantdecrease in tumor growth in 4 of 9 (44%) xenografts inthe combination therapy group as compared with thesingle-agent gemcitabine, and this subset of tumors wascomprised of Panc198 (P < 0.05), Panc219 (P < 0.01),Panc291 (P < 0.001), and JH033 (P < 0.05; Fig. 5C). BaselineNotch1 expression (Fig. 5A) was not predictive of GSI(MRK-003) sensitivity in this tumor model.
MRK-003 as well as combination of gemcitabine withMRK-003 treatments reduced the expression of bothnuclear Notch1 (N1ICD) and Hes-1 as compared withcontrol and gemcitabine-treated tumors (Fig. 6A and B).We then sought to determine the effects on proliferationand apoptosis in the posttreatment samples, using 2representative xenografts (Panc198 and Panc291). Com-pared with single-agent therapy, xenografts receivingMRK-003andgemcitabine showedsignificantly increasedapoptosis (as assessed by TUNEL staining; Fig. 7A), aswell as significantly reduced tumor cell proliferation (asassessed by Ki-67; Fig. 7B).
Gene expression analysis for predictive signatures ofresponse to MRK-003
Probe sets that show significant correlation withresponse to MRK-003, or the combination of MRK-003plus gemcitabine (692 and 967 probes, respectively, Sup-plementary Tables S1 and S2) were identified with Pear-son P value
-
gemcitabine treatment and other molecular targetedagents (24, 32). The overwhelming majority of PDACharbor activating mutations of KRAS (19), and sustainedNotch1 signaling was shown to be essential in maintain-ing the transformed phenotype of Ras-mutant cells (33).These multiple lines of evidence strongly support thepharmacologic targeting of Notch signaling in PDAC,particularly in combination with gemcitabine.
MRK-003 is a potent and selective GSI (13, 14), which isthe preclinical analog of MK-0752, currently in clinicaldevelopment (15, 16). As a "pan" Notch inhibitor, MRK-003 is expected to inhibit the enzymatic cleavage of all 4Notch receptors, which bypasses the need for receptor-specific targeting based on tumor context. For example,our studies have shown that Notch1 is the primary onco-genic influence in pancreatic cancer (10), whereas lung
Panc374
0 3 6 9 12 15 18 21 240
1,000
2,000
3,000VehicleMRK-003GEMMRK-003 + GEM
Days
Tu
mo
r vo
lum
e (m
m3 )
Panc198
0 3 6 9 12 15 18 21 240
1,000
2,000
3,000
4,000
5,000VehicleMRK-003GEMMRK-003 + GEM
Days
Tu
mo
r vo
lum
e (m
m3 )
A
B
0
25
50
75
100
Panc420 Panc374 Panc219 Panc265 Panc198 JH033 Panc253 Panc291 Panc215
Patient pancreatic tumors xenografted in mice
Tu
mo
r g
row
th in
hib
itio
n (
%)
MRK-003
GEM
MRK-003 + GEM
**
**
****
*
#
***
**
**
***
***
***
* #**
***
**
# #
****
#
C
Figure 5. In vivo efficacy of MRK-003, gemcitabine, and combination of MRK-003 and gemcitabine in a panel of patient-derived PDAC xenografts.A, 9 individual cases for this study were selected from a pool of 30 PDAC xenografts based on expression of NOTCH1 transcripts at baseline. In theillustrated heatmap, red to green indicates decreasing transcript expression. The numbers on the top panel indicate each individual patient-derived PDACxenograft. B, growth curves of 2 representative PDAC xenografts, Panc374 and Panc198, show that the combination of gemcitabine and MRK-003 cansignificantly inhibit tumor growth compared with the vehicle and/or gemcitabine-treated animals. Each treatment arm was comprised of 10 tumorsimplanted as bilateral subcutaneous xenografts in 5 mice. C, summary of tumor growth inhibition data. MRK-003 monotherapy significantly reduced tumorvolume in 5 of 9 xenografts compared with the vehicle-treated xenografts, which were Panc420, Panc374, Panc219, Panc265, and JH033. Therewas a significant reduction in tumor growth of 4 of 9 xenografts in the combination therapy group compared with the gemcitabine alone, which werePanc198, Panc219, Panc291, and JH033. (�, P < 0.05, ��, P < 0.01, ���, P < 0.001 versus vehicle-treated mice; #, P < 0.05, ##, P < 0.01 compared with thegemcitabine-treated mice). GEM, gemcitabine.
Notch Inhibition in Pancreatic Cancer
www.aacrjournals.org Mol Cancer Ther; 11(9) September 2012 2005
on July 1, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 2, 2012; DOI: 10.1158/1535-7163.MCT-12-0017
http://mct.aacrjournals.org/
-
cancers harbor greater dependence on Notch3 signaling(13), andmedulloblastomas onNotch2 (34). In the contextof breast cancer, activation of Notch1 is observed intumors exposed to trastuzumab, contributing to therape-utic resistance (35). On the contrary, combining MRK-003with trastuzumab completely prevented tumor recur-rence in trastuzumab-sensitive tumor, whereas the com-bination of lapatinib with MRK-003 significantly reducedtumor growth in trastuzumab-resistant cancers (36).
Our in vitro results confirm that MRK-003 exposureleads to differential effects in PDAC cells, with a subsetof lines unequivocally responding to the agent by signif-icant reduction in anchorage-independent growth anddelay in tumor engraftment in athymic mice; in contrast,other lines remain refractory to the drug. AlthoughMRK-003 treatment could diminish the proportion of CD24þ
CD44þ or ALDHþ subpopulation in Capan-1 and Pa03Ccells, the treatment leads to the enrichment of CD24þ
CD44þ and ALDHþ cells in Pa16C and Pa29C cells.Although our current study was entirely geared towardthe use of MRK-003 as a therapeutic strategy in estab-lished PDAC, Plentz and colleagues have previouslyshown the significant efficacy of MRK-003 in chemopre-
vention using a genetically engineeredmousemodel (11),further underscoring the importance ofNotch signaling totumor initiation in thepancreas. It is important to note thatthe cellular phenotypes implicated in tumor initiation arealso highly enriched in pancreatic cancer metastases(22, 37), and thus, pharmacologic Notch inhibition wouldconceivably be beneficial in advanced disease settings aswell.
A recent report indicated that a combination of MRK-003 and gemcitabine could induce intratumoral necro-sis in KPC mouse model (38). In light of this, weexamined the histologic sections from treated xeno-grafts and find that stroma-rich xenografts (e.g.,Panc374; Supplementary Fig. S3) do, in fact, showincreased necrosis in the combination therapy arm.Although central necrosis to some degree is observedin all of the cohorts, the MRK-003 plus gemcitabine-treated tumors show sheets of confluent necrosis. How-ever, this phenomenon was not uniformly observed,especially in stroma-poor xenografts (data not shown).We believe that the relative hypovascularity of stroma-rich xenografts (a feature also reflected in human pan-creatic cancers and the KPC model) may explain why
A BC
on
tro
lG
EM
+ M
RK
-003
GE
M +
MR
K-0
03M
RK
-003
MR
K-0
03G
EM
Panc291 Panc374
Co
ntr
ol
GE
M
Panc291 Panc374
N1ICD Hes-1
Figure 6. MRK-003 treatment downregulates nuclear N1ICD and Hes-1 protein expressions in PDAC xenografts as shown by immunohistochemical staining.A and B, representative photomicrographs of N1ICD and Hes-1 from Panc291 and Panc374 xenografts showing downregulation of nuclear N1ICDand Hes-1 expression in MRK-003 and combination of gemcitabine and MRK-003 treatment compared with the vehicle-treated and gemcitabine-treatedtumor samples. GEM, gemcitabine.
Mizuma et al.
Mol Cancer Ther; 11(9) September 2012 Molecular Cancer Therapeutics2006
on July 1, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 2, 2012; DOI: 10.1158/1535-7163.MCT-12-0017
http://mct.aacrjournals.org/
-
these tumors show increased necrosis in the setting ofcombination therapy.As an attempt to identify predictive signatures in
response to MRK-003, we examined the baseline geneexpression profiles of the 9 patient-derived xenograftsas it related to variable in vivo responses to either MRK-003 alone or the combination regimen. Upregulation ofNF-kB signaling components was correlated withresponse to single-agent MRK-003, a finding that attainssignificance in light of the recent observation of cross-
talk between Notch and NF-kB signaling in murinePDAC models (30). In that study, NF-kB activationcollaborated with basal Notch signals to enhance Notchtarget gene expression, suggesting that a signatureconsistent with NF-kB activation may indicate a greaterdegree of Notch dependence in PDAC cells. The exis-tence of crosstalk between Notch and NF-kB pathwayshas also been reported by other groups using in vitromodels of pancreatic cancer (39, 40), underscoring thevalidity of our findings. In terms of the combination
Co
ntr
ol
GE
M
GE
M +
MR
K-0
03
TUNEL
Cont
rol
MRK
-003
GEM
GEM
+ M
RK-0
030
10
20
30
40
50
PANC198
Po
siti
vely
sta
ined
cel
ls
Cont
rol
MRK-
003
GEM
GEM
+ MR
K-00
30
10
20
30
40
PANC291
Pos
itiv
ely
stai
ned
cel
ls
MR
K-0
03
Co
ntr
ol
GE
M
GE
M +
MR
K-0
03M
RK
-003
* *
Panc198 Panc291Panc198
A B Panc291
Ki-67
Cont
rol
MRK-
003
GEM
GEM
+ MR
K-00
30
100
200
300
400
PANC198
Po
sitiv
ely
stai
ned
cells
Cont
rol
MRK-
003
GEM
GEM
+ MR
K-00
30
100
200
300
400
500
PANC291
Po
sitiv
ely
stai
ned
cells
* *
Figure 7. Combination of gemcitabine andMRK-003 induces apoptosis and reduces cell proliferation in PDAC xenografts. A, representative photomicrographof TUNEL staining from Panc198 and Panc291. Histogram of TUNEL-positive nuclei per high-power field (bottom), showing that combination of gemcitabineand MRK-003 significantly enhanced apoptotic cells per field as compared with the gemcitabine treatment. B, representative photomicrograph ofKi-67 staining from Panc198 and Panc291. Histogram of Ki-67-positive nuclei per high-power field (bottom), showing that combination of gemcitabineand MRK-003 significantly reduced proliferating cells as compared with the gemcitabine treatment. Histograms for TUNEL and Ki-67 were generated byevaluating 5 high-power fields per xenograft section from 2 independent tumors per treatment arms; mean � SEM (�, P < 0.001 compared with thegemcitabine). GEM, gemcitabine.
Notch Inhibition in Pancreatic Cancer
www.aacrjournals.org Mol Cancer Ther; 11(9) September 2012 2007
on July 1, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 2, 2012; DOI: 10.1158/1535-7163.MCT-12-0017
http://mct.aacrjournals.org/
-
regimen, we identified 2 activation signatures that cor-related with response in xenografts, BCR signaling andNrf2, respectively. Although an interaction betweenBCR and Notch signaling has not been reported previ-ously in solid tumors, not unexpectedly a potentialsynergy does exist in normal and neoplastic hemato-poietic cells (41, 42). Thus, in both normal B-cells, aswell as in B-cell lymphoma lines, Notch promotes BCR-mediated proliferation, which is blocked by adminis-tration of GSI (41, 42). In these aforementioned studies,putative downstream effectors that have been implicat-ed in the observed synergy include the MAP kinasesignaling pathway and Myc, both of which retain con-siderable significance in PDAC pathogenesis. The cor-relation between sensitivity to GSI plus gemcitabine andNRF1/2 signaling (which was identified by 2 disparatestrategies, IPA and NextBio analyses, respectively) is, tothe best of our knowledge, previously unreported. Asrecently showed, NRF2 expression is crucial to mostoncogene-driven cancers (including PDAC), in light ofits ability to attenuate deleterious reactive oxygen spe-cies that accumulate from oncogene-induced cellularstress (43). The precise cellular mechanisms by whichan NRF2 activation signature leads to sensitivity toMRK-033/gemcitabine regimen remain to be deter-mined; nonetheless, the in silico correlations generatedwith regard to various activation signatures (NF-kB,BCR, and Nrf2) in PDAC and response to eithersingle-agent GSI or combination regimens should betestable hypotheses, as these agents are increasinglybeing evaluated in the clinic.
Substantial preclinical evidence supports the role ofNotch signaling in the initiation, progression, and main-tenance of PDAC. Pharmacologic targeting of Notchsignaling in PDAC patients using GSI such as MK-0752 are warranted on the basis of this evidence. Acombination regimen of gemcitabine and MK-0752 iscurrently being evaluated in advanced PDAC patients
(ClinicalTrials.gov, NCT ID: NCT01098344; 44). Ourresults strengthen the rationale for small-moleculeinhibition of g-secretase inhibition as a therapeuticstrategy in PDAC and identification of a putative sen-sitivity signature to the combination of gemcitabine andMRK-003 may provide insights into clinical response inthe ongoing and future trials.
Disclosure of Potential Conflicts of InterestQ. Zhang and O. Puig are employees of Merck Research Laboratories.
Authors' ContributionsConception and design: M. Mizuma, Z.A. Rasheed, E. De Oliveira,A. Maitra, N.V. RajeshkumarDevelopment ofmethodology:M.Mizuma, Z.A. Rasheed, E. DeOliveira,W. Matsui, M. Hidalgo, A. Maitra, N.V. RajeshkumarAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): M. Mizuma, Z.A. Rasheed, S. Yabuuchi, N.R.Campbell, R.F. de Wilde, E. De Oliveira, N.V. RajeshkumarAnalysis and interpretation of data (e.g., statistical analysis, biostatis-tics, computational analysis):M.Mizuma,Z.A.Rasheed, S. Yabuuchi, R.F.de Wilde, Q. Zhang, O. Puig, W. Matsui, A. Maitra, N.V. RajeshkumarWriting, review, and/or revision of themanuscript:Z.A. Rasheed, R.F. deWilde, Q. Zhang, O. Puig, M. Hidalgo, A. Maitra, N.V. RajeshkumarAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): M. Mizuma, N. Omura, E. DeOliveira, Q. ZhangStudy supervision: N.V. Rajeshkumar
AcknowledgmentsThe authors thank Shweta G. Pai (Johns Hopkins) for help in tissue
culture experiments.
Grant SupportN.V. Rajeshkumar, A.Maitra, andM.Hidalgo are supported by a Stand
Up To Cancer Dream Team Translational Cancer Research Grant, aProgram of the Entertainment Industry Foundation (SU2C-AACR-DT0509). A. Maitra is supported by Merck Research Laboratories andNIH CA113669.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received January 10, 2012; revisedMay 23, 2012; accepted June 15, 2012;published OnlineFirst July 2, 2012.
References1. Vincent A, Herman J, Schulick R, Hruban RH, Goggins M. Pancreatic
cancer. Lancet 2011;378:607–20.2. Conroy T, Desseigne F, Ychou M, Bouche O, Guimbaud R, Becouarn
Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreaticcancer. N Engl J Med 2011;364:1817–25.
3. Saif MW, Chabot J. Chemotherapy: metastatic pancreatic cancer—isFOLFIRINOX the new standard? Nat Rev Clin Oncol 2011;8:452–3.
4. KopanR, IlaganMX. ThecanonicalNotchsignalingpathway: unfoldingthe activation mechanism. Cell 2009;137:216–33.
5. Miele L, Golde T, Osborne B. Notch signaling in cancer. Curr Mol Med2006;6:905–18.
6. Aster JC, Pear WS, Blacklow SC. Notch signaling in leukemia. AnnuRev Pathol 2008;3:587–613.
7. van Es JH, vanGijnME, RiccioO, van denBornM, VooijsM, Begthel H,et al. Notch/gamma-secretase inhibition turns proliferative cells inintestinal crypts and adenomas into goblet cells. Nature 2005;435:959–63.
8. Rizzo P, Osipo C, Foreman K, Golde T, Osborne B, Miele L. Rationaltargeting of Notch signaling in cancer. Oncogene 2008;27:5124–31.
9. Leach SD. Epithelial differentiation in pancreatic development andneoplasia: new niches for nestin and Notch. J Clin Gastroenterol2005;39:S78–82.
10. Miyamoto Y, Maitra A, Ghosh B, Zechner U, Argani P, Iacobuzio-Donahue CA, et al. Notch mediates TGF alpha-induced changes inepithelial differentiation during pancreatic tumorigenesis. Cancer Cell2003;3:565–76.
11. Plentz R, Park JS, Rhim AD, Abravanel D, Hezel AF, Sharma SV, et al.Inhibition of gamma-secretase activity inhibits tumor progression in amousemodel of pancreatic ductal adenocarcinoma.Gastroenterology2009;136:1741–9.e6.
12. Mullendore ME, Koorstra JB, Li YM, Offerhaus GJ, Fan X, HendersonCM, et al. Ligand-dependent Notch signaling is involved in tumorinitiation and tumor maintenance in pancreatic cancer. Clin CancerRes 2009;15:2291–301.
13. Konishi J, Kawaguchi KS, Vo H, Haruki N, Gonzalez A, Carbone DP,et al. Gamma-secretase inhibitor prevents Notch3 activation andreduces proliferation in human lung cancers. Cancer Res 2007;67:8051–7.
Mizuma et al.
Mol Cancer Ther; 11(9) September 2012 Molecular Cancer Therapeutics2008
on July 1, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 2, 2012; DOI: 10.1158/1535-7163.MCT-12-0017
http://mct.aacrjournals.org/
-
14. ChenJ, Kesari S, RooneyC,StrackPR,ShenH,WuL, et al. Inhibition ofnotch signaling blocks growth of glioblastoma cell lines and tumorneurospheres. Genes Cancer 2011;1:822–35.
15. Deangelo DJ, Stone RM, Silverman LB, Stock W, Attar EC, Fearen I,et al. A phase I clinical trial of the notch inhibitor MK-0752 in patientswith T-cell acute lymphoblastic leukemia/lymphoma (T-ALL) and otherleukemias. J Clin Oncol 2006;24:6585.
16. Fouladi M, Stewart CF, Olson J, Wagner LM, Onar-Thomas A, KocakM, et al. Phase I trial of MK-0752 in children with refractory CNSmalignancies: a pediatric brain tumor consortium study. J Clin Oncol2011;29:3529–34.
17. Lewis HD, Leveridge M, Strack PR, Haldon CD, O'Neil J, Kim H, et al.Apoptosis in T cell acute lymphoblastic leukemia cells after cell cyclearrest induced by pharmacological inhibition of notch signaling. ChemBiol 2007;14:209–19.
18. Pourquier P, Gioffre C, Kohlhagen G, Urasaki Y, Goldwasser F, HertelLW, et al. Gemcitabine (20,20-difluoro-20-deoxycytidine), an antimetab-olite that poisons topoisomerase I. Clin Cancer Res 2002;8:2499–504.
19. Jones S, Zhang X, Parsons DW, Lin JC, Leary RJ, Angenendt P, et al.Core signaling pathways in human pancreatic cancers revealed byglobal genomic analyses. Science 2008;321:1801–6.
20. Livak KJ, Schmittgen TD. Analysis of relative gene expression datausing real-time quantitative PCR and the 2(-Delta Delta C(T)) method.Methods 2001;25:402–8.
21. Rajeshkumar NV, De Oliveira E, Ottenhof N, Watters J, Brooks D,Demuth T, et al. MK-1775, a potent wee1 inhibitor, synergizes withgemcitabine to achieve tumor regressions, selectively in p53-deficientpancreatic cancer xenografts. Clin Cancer Res 2011;17:2799–806.
22. Rasheed ZA, Yang J, Wang Q, Kowalski J, Freed I, Murter C, et al.Prognostic significance of tumorigenic cells with mesenchymal fea-tures in pancreatic adenocarcinoma. J Natl Cancer Inst 2010;102:340–51.
23. RajeshkumarNV,RasheedZA,Garcia-GarciaE,Lopez-RiosF, FujiwaraK, Matsui WH, et al. A combination of DR5 agonistic monoclonalantibody with gemcitabine targets pancreatic cancer stem cells andresults in long-term disease control in human pancreatic cancermodel.Mol Cancer Ther 2011;10:2582–92.
24. Garrido-Laguna I, Uson M, Rajeshkumar NV, Tan AC, de Oliveira E,Karikari C, et al. Tumor engraftment in nude mice and enrichment instroma- related gene pathways predict poor survival and resistance togemcitabine in patients with pancreatic cancer. Clin Cancer Res2011;17:5793–800.
25. Pramanik D, Campbell NR, Karikari C, Chivukula R, Kent OA, MendellJT, et al. Restitution of tumor suppressor microRNAs using a systemicnanovector inhibits pancreatic cancer growth inmice.MolCancer Ther2011;10:1470–80.
26. IrizarryRA,HobbsB,Collin F,Beazer-BarclayYD,AntonellisKJ, ScherfU, et al. Exploration, normalization, and summaries of high densityoligonucleotide array probe level data. Biostatistics 2003;4:249–64.
27. Li C, Heidt DG, Dalerba P, Burant CF, Zhang L, Adsay V, et al.Identification of pancreatic cancer stem cells. Cancer Res 2007;67:1030–7.
28. HeHH,MeyerCA,ShinH,BaileyST,WeiG,WangQ, et al.Nucleosomedynamics define transcriptional enhancers. Nat Genet 2010;42:343–7.
29. Kheirallah S, Caron P, Gross E, Quillet-Mary A, Bertrand-Michel J,Fournie JJ, et al. Rituximab inhibits B-cell receptor signaling. Blood2010;115:985–94.
30. Maniati E, Bossard M, Cook N, Candido JB, Emami-Shahri N, Nedos-pasov SA, et al. Crosstalk between the canonical NF-kappaB andNotch signaling pathways inhibits Ppargamma expression and pro-motes pancreatic cancer progression in mice. J Clin Invest 2011;121:4685–99.
31. Wang Z, Banerjee S, Ahmad A, Li Y, Azmi AS, Gunn JR, et al. ActivatedK-ras and INK4a/Arf deficiency cooperate during the development ofpancreatic cancer by activation of Notch and NF-kappaB signalingpathways. PLoS One 2011;6:e20537.
32. Feldmann G, Mishra A, Bisht S, Karikari C, Garrido-Laguna I, RasheedZ, et al. Cyclin-dependent kinase inhibitor Dinaciclib (SCH727965)inhibits pancreatic cancer growth and progression inmurine xenograftmodels. Cancer Biol Ther 2011;12:598–609.
33. Weijzen S, Rizzo P, Braid M, Vaishnav R, Jonkheer SM, Zlobin A, et al.Activation of Notch-1 signaling maintains the neoplastic phenotype inhuman Ras-transformed cells. Nat Med 2002;8:979–86.
34. Fan X, Mikolaenko I, Elhassan I, Ni X, Wang Y, Ball D, et al. Notch1 andnotch2 have opposite effects on embryonal brain tumor growth.Cancer Res 2004;64:7787–93.
35. Osipo C, Patel P, Rizzo P, Clementz AG, Hao L, Golde TE, et al. ErbB-2inhibition activates Notch-1 and sensitizes breast cancer cells to agamma-secretase inhibitor. Oncogene 2008;27:5019–32.
36. Pandya K, Meeke K, Clementz AG, Rogowski A, Roberts J, Miele L,et al. Targeting both Notch and ErbB-2 signalling pathways is requiredfor prevention of ErbB-2-positive breast tumour recurrence. BrJ Cancer 2011;105:796–806.
37. Feldmann G, Dhara S, Fendrich V, Bedja D, Beaty R, Mullendore M,et al. Blockade of hedgehog signaling inhibits pancreatic cancerinvasion and metastases: a new paradigm for combination therapy insolid cancers. Cancer Res 2007;67:2187–96.
38. Cook N, Frese KK, Bapiro TE, Jacobetz MA, Gopinathan A, Miller JL,et al. Gammasecretase inhibition promotes hypoxic necrosis inmousepancreatic ductal adenocarcinoma. J Exp Med 2012;209:437–44.
39. Wang Z, Zhang Y, Banerjee S, Li Y, Sarkar FH. Inhibition of nuclearfactor kappab activity by genistein is mediated via Notch-1 signalingpathway in pancreatic cancer cells. Int J Cancer 2006;118:1930–6.
40. Wang Z, Zhang Y, Li Y, Banerjee S, Liao J, Sarkar FH. Down-regulationof Notch-1 contributes to cell growth inhibition and apoptosis inpancreatic cancer cells. Mol Cancer Ther 2006;5:483–93.
41. He F, Wang L, Hu XB, Yin DD, Zhang P, Li GH, et al. Notch and BCRsignaling synergistically promote the proliferation of Raji B-lymphomacells. Leuk Res 2009;33:798–802.
42. Thomas M, Calamito M, Srivastava B, Maillard I, Pear WS, Allman D.Notch activity synergizes with B-cell-receptor and CD40 signaling toenhance B-cell activation. Blood 2007;109:3342–50.
43. DeNicola GM, Karreth FA, Humpton TJ, Gopinathan A,Wei C, Frese K,et al. Oncogene-induced Nrf2 transcription promotes ROS detoxifi-cation and tumorigenesis. Nature 2011;475:106–9.
44. ClinicalTrials.gov [homepage on the internet]. A service of the U.S.Natioanal Institutes of Health, Bethesda. [updated Feb 27, 2012].Identifier NCT01098344. Available from: http://clinicaltrials.gov.
Notch Inhibition in Pancreatic Cancer
www.aacrjournals.org Mol Cancer Ther; 11(9) September 2012 2009
on July 1, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 2, 2012; DOI: 10.1158/1535-7163.MCT-12-0017
http://mct.aacrjournals.org/
-
2012;11:1999-2009. Published OnlineFirst July 2, 2012.Mol Cancer Ther Masamichi Mizuma, Zeshaan A. Rasheed, Shinichi Yabuuchi, et al. Cancer Growth in Preclinical ModelsThe Gamma Secretase Inhibitor MRK-003 Attenuates Pancreatic
Updated version
10.1158/1535-7163.MCT-12-0017doi:
Access the most recent version of this article at:
Material
Supplementary
http://mct.aacrjournals.org/content/suppl/2012/07/02/1535-7163.MCT-12-0017.DC1
Access the most recent supplemental material at:
Cited articles
http://mct.aacrjournals.org/content/11/9/1999.full#ref-list-1
This article cites 43 articles, 16 of which you can access for free at:
Citing articles
http://mct.aacrjournals.org/content/11/9/1999.full#related-urls
This article has been cited by 4 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/11/9/1999To request permission to re-use all or part of this article, use this link
on July 1, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 2, 2012; DOI: 10.1158/1535-7163.MCT-12-0017
http://mct.aacrjournals.org/lookup/doi/10.1158/1535-7163.MCT-12-0017http://mct.aacrjournals.org/content/suppl/2012/07/02/1535-7163.MCT-12-0017.DC1http://mct.aacrjournals.org/content/11/9/1999.full#ref-list-1http://mct.aacrjournals.org/content/11/9/1999.full#related-urlshttp://mct.aacrjournals.org/cgi/alertsmailto:[email protected]://mct.aacrjournals.org/content/11/9/1999http://mct.aacrjournals.org/