The effects of dexamethasone on experimental brain tumors: I. Transcapillary transport and blood...
10
Journal of Neuro-Oncology 25: 19-28, 1995. 1995 Kluwer Academic Publishers. Printedin the Netherlands. Laboratory Investigation The effects of dexamethasone on experimental brain tumors: I. Transcapillary transport and blood flow in RG-2 rat gliomas Peter Molnar, 1'2 Gregory D. Lapin 1'3and Dennis R. Groothuis 1'4 1Department of Neurology, Northwestern University Medical School, Evanston Hospital, Evanston, IL 60201, USA; 2 Mark Moritz Visiting Scholar (Present address: Hungarian-Japanese EM Center (HJEMC), University Medical School of Debrecen, P.O. Box 23, H-4014 Debrecen, Hungary); ~ Department of Biomedical Engineer- ing and the Neuroscience Institute, Northwestern University, Evanston, IL 60208, USA; 4 Department of Neuro- biology and Physiology and the Neuroscience Institute, Northwestern University, Evanston, IL 60208, USA Key words: brain tumors, steroids, blood-brain barrier, dexamethasone, capillary permeability, cerebral edema Summary Dexamethasone dramatically improves cerebral edema associated with malignant gliomas. Although the pathophysiology of this effect is not clearly understood, many investigators have postulated that tumor capil- lary permeability is reduced by dexamethasone. We studied blood-to-tissue transport and blood flow in 178 RG-2 transplanted gliomas in a control group and four groups given dexamethasone at doses of 3, 6, 9, and 12 mg/kg for four days. 14C-c~aminoisobutyric acid (AIB) was used to study blood-to-tissue transport in 31 animals; in an additional 27 animals 14C-AIB and 131I-iodoantipyrine (IAP) were used in double label experi- ments to study blood-to-tissue transport and blood flow. Regional measurements of the transfer constant (K) of AIB and blood flow (F) were made with quantitative autoradiography. There were significant differences between the control and dexamethasone-treated groups with regard to weight loss and plasma glucose. How- ever, there was no significant effect of dexamethasone on values of K or F, regardless of the tumor or brain region examined, and regardless of the dose of dexamethasone administered. Analysis of the profiles of the transfer constant of AIB in the brain around tumor showed that the K of AIB decreased within 0.5 mm of the tumor edge in direct relationship to the dexamethasone dose. These results do not support the hypothesis that dexamethasone reduces brain tumor capillary permeability, and suggest that dexamethasone may decrease tumor-associated cerebral edema by effects on bulk flow away from the tumor margin. Introduction Dexamethasone may be considered standard ther- apy for cerebral edema occurring in patients with malignant brain tumors. However, the pathophy- siology of tumor-associated cerebral edema is not well understood and the mechanism by which dexa- methasone reduces the edema is even less well un- derstood. Reulen reminds us: 'When trying to assess the effect of a drug on brain edema, we should exam- ine the various links of this pathological chain rather than concentrating only on one aspect of the phe- nomenon' [1]. The problem of studying the patho- physiology of cerebral edema is heightened by our limited analytic tools: all too often we must ignore Reulen's advice because our experimental method- ology allows us to examine only one, or at most, a few steps of the process at a time. The studies we report here concentrate on 'permeability'. The dif- ference in permeability between capillaries of nor-
-
Upload
peter-molnar -
Category
Documents
-
view
212 -
download
0
Transcript of The effects of dexamethasone on experimental brain tumors: I. Transcapillary transport and blood...

Journal of Neuro-Oncology 25: 19-28, 1995. �9 1995 Kluwer Academic Publishers. Printed in the Netherlands.
Laboratory Investigation
The effects of dexamethasone on experimental brain tumors: I. Transcapillary transport and blood flow in RG-2 rat gliomas
Peter Molnar, 1'2 Gregory D. Lapin 1'3 and Dennis R. Groothuis 1'4 1 Department o f Neurology, Northwestern University Medical School, Evanston Hospital, Evanston, IL 60201, USA; 2 Mark Moritz Visiting Scholar (Present address: Hungarian-Japanese EM Center (HJEMC), University Medical School o f Debrecen, P.O. Box 23, H-4014 Debrecen, Hungary); ~ Department o f Biomedical Engineer- ing and the Neuroscience Institute, Northwestern University, Evanston, IL 60208, USA; 4 Department of Neuro- biology and Physiology and the Neuroscience Institute, Northwestern University, Evanston, IL 60208, USA
Key words: brain tumors, steroids, blood-brain barrier, dexamethasone, capillary permeability, cerebral edema
Summary
Dexamethasone dramatically improves cerebral edema associated with malignant gliomas. Although the pathophysiology of this effect is not clearly understood, many investigators have postulated that tumor capil- lary permeability is reduced by dexamethasone. We studied blood-to-tissue transport and blood flow in 178 RG-2 transplanted gliomas in a control group and four groups given dexamethasone at doses of 3, 6, 9, and 12 mg/kg for four days. 14C-c~ aminoisobutyric acid (AIB) was used to study blood-to-tissue transport in 31 animals; in an additional 27 animals 14C-AIB and 131I-iodoantipyrine (IAP) were used in double label experi- ments to study blood-to-tissue transport and blood flow. Regional measurements of the transfer constant (K) of AIB and blood flow (F) were made with quantitative autoradiography. There were significant differences between the control and dexamethasone-treated groups with regard to weight loss and plasma glucose. How- ever, there was no significant effect of dexamethasone on values of K or F, regardless of the tumor or brain region examined, and regardless of the dose of dexamethasone administered. Analysis of the profiles of the transfer constant of AIB in the brain around tumor showed that the K of AIB decreased within 0.5 mm of the tumor edge in direct relationship to the dexamethasone dose. These results do not support the hypothesis that dexamethasone reduces brain tumor capillary permeability, and suggest that dexamethasone may decrease tumor-associated cerebral edema by effects on bulk flow away from the tumor margin.
Introduction
Dexamethasone may be considered standard ther- apy for cerebral edema occurring in patients with malignant brain tumors. However, the pathophy- siology of tumor-associated cerebral edema is not well understood and the mechanism by which dexa- methasone reduces the edema is even less well un- derstood. Reulen reminds us: 'When trying to assess the effect of a drug on brain edema, we should exam-
ine the various links of this pathological chain rather than concentrating only on one aspect of the phe- nomenon' [1]. The problem of studying the patho- physiology of cerebral edema is heightened by our limited analytic tools: all too often we must ignore Reulen's advice because our experimental method- ology allows us to examine only one, or at most, a few steps of the process at a time. The studies we report here concentrate on 'permeability'. The dif- ference in permeability between capillaries of nor-

20
mal brain and those of brain tumors is often pro- found; a change that alters the rules governing the movement of compounds from the blood into the brain and tumor tissue. Thus, the permeability of the capillaries becomes the initial control point in the 'pathological chain' to which Reulen referred and permeability becomes a focus of attention to understand the entire process. The effect of dexa- methasone on 'permeability' (usually measured as a blood-to-tissue transfer constant, K) has been studied many times, in both animal models [2-7] and in humans [8-11]. The results of these reports have varied dramatically, from showing no effect to a dramatic decrease in permeability after adminis- tration of dexamethasone. A clear consensus of the effects of dexamethasone on brain tumor capillary permeability has yet to be reached. Since capillary permeability (and to a lesser extent, capillary sur- face area) is the first control point in the 'patholog- ical chain' of cerebral edema, it is reasonable to con- tinue to study how it is affected by dexamethasone. We revisited the RG-2 rat glioma model, in which we had previously been unable to show a change in blood-to-tissue transport of albumin after adminis- tration of dexamethasone, to determine how large doses of dexamethasone would affect blood flow to, and the transport of c~-aminoisobutyric acid (AIB) into, RG-2 tumors.
Materials and methods
Animal preparation
All animal procedures were reviewed and ap- proved by an Institutional Animal Care and Use Committee. RG-2 brain tumors were produced in 58 Fischer-344 rats (Harlan Industries, Indianapo- lis, IN) by injecting 2 gl (105 tumor cells/ml) into the right hemisphere as previously described [12]. The animals were placed into treatment and control groups 14 days later, when they were asymptomatic. Each animal received an intraperitoneal injection twice daily of the same volume of either saline or saline plus dexamethasone (adjusted to produce a dose of 3 to 12 mg/kg/day). Injections were started four days prior to the autoradiographic studies;
eight doses were administered. On the day of a study animals were prepared as previously de- scribed [12]: femoral arterial and venous catheters were inserted under halothane-nitrous oxide-ox- ygen anesthesia and local anesthetic (2 % xylocaine jelly) was applied. The rats were immobilized by wrapping them with a loosely fitting two inch plas- ter bandage and allowed to recover from anesthesia for at least one hour prior to study. Arterial blood pressure and rectal temperature were monitored and rectal temperature was kept at 36-37 ~ with radiant heat lamps. Arterial blood gases were mea- sured during the recovery period from anesthesia and immediately prior to the experiment; arterial blood was collected at the end of the experiment for plasma glucose measurements.
Experimental procedures
In all experiments, 14C-alpha aminoisobutyric acid (AIB) was used to measure a unidirectional blood- to-tissue transfer constant. In 27 experiments, 13aI iodoantipyrine (lAP) was used to measure blood flow in double label experiments. Labeled AIB, 1-14C, 40 to 60 mCi/mmol, and 131I (reductant free, approximately 25 Ci/mg of iodine) were obtained from New England Nuclear (Boston, MA). [131I]IAP was synthesized by an exchange reaction with cold IAR Radiochemical purity of AIB was > 99% and of IAP was > 95% [13]. In each experi- ment, 50 gCi of 14C-AIB in i ml of 0.9% NaCI was administered as an intravenous bolus. Timed arte- rial samples were obtained, centrifuged, and plas- ma 14C radioactivity measured. For experiments in which blood flow was also measured, 500 gCi of 131I- IAP was administered by increasing ramp infusion as previously described [14]. Ten min after adminis- tration of AIB (30 sec after administration of IAP) the animal was decapitated, the brain rapidly re- moved (~ i min) and frozen in liquid freon cooled to - 40 ~ The preparation of brain sections, aut- oradiographs, and 131I standards has been described [15]. The range of twelve 131I standards was from 12.1 to 859.6 cpm/mg. Regional tissue measurements of radioactivity (nCi/g) were made at a resolution of 50 grrdpixel with a video based digitizing system

[16]. Blood flow calculations were made using Kety- Schmidt equations, with ;% = 0.8, as described by Sakurada et al. [17]. A unidirectional blood-to-tis- sue transfer constant, K, of AIB was calculated as previously described [14,18]. An image overlay sys- tem was used to assure that all measurements were based on the histological section. The lowest values of F and K measurable in these experiments were represented by film background: F = 0.5 ml/100 g/ min, K = 0.5 gl/g/min.
Methods o f analysis
Measurements of blood flow (F) and K were made in the following brain and tumor regions of interest (ROI): whole tumor (through maximum cross-sec- tional area), tumor center, tumor periphery, brain adjacent to tumor (BAT; a 250-500>gm wide zone surrounding the tumor), brain surrounding tumor (BST; a 250-500 ~tm wide zone outside BAT), and in ipsilateral and contralateral tumor-free cortex and corpus callosum. For each ROI, we obtained the mean + SD of all 50 x 50 gin pixels in the region.
To obtain a profile of K measurements as a func- tion of distance from the tumor margin, we selected
21
all intraparenchymal tumors that were completely surrounded by brain; we did not include tumors that were located near meninges, ventricles, or near an- other tumor. A rectangle, which measured 500 gm in height (ten 50 gm pixels), was placed over the histologic image with one end in the periphery of the tumor and extending radially into surrounding brain and perpendicular to the tumor margin. Each rectangle was divided horizontally into 100 gm sub- divisions and the K value of AIB (mean + SD) was obtained for each subdivision of the rectangle. The same size rectangular bar was used in each animal and data sets were combined: 12 tumors were from the control group, 14 from the 3 mg/kg, 6 from the 6 mg/kg, 15 from the 9 mg/kg, and 8 from the 12 mg/ kg dexamethasone-treated group. Since the value of K was not identical at the tumor margin in each of the groups, and for purposes of comparison and il- lustration, the values were normalized by dividing the K value at each distance by the K value at the edge of the tumor.
Table 1. Physiological characteristics of exper imental groups. Shown are the dexamethasone dose (mg/kg/day) for the control and four
experimental groups, the number of animals in each group (N), the hematocri t at the time of the exper iment (%), the arterial blood gases
at the time of the exper iment (tort), blood pressure (mmHg) , rectal tempera ture (~ C), the change in weight f rom the start of intraperito-
neal injections to the time of the exper iment (grams), and the plasma glucose at the time of the exper iment (gmol/L). Values are mean
• SD.
Exper imental group
Control Dexamethasone treated
Dexamethasone 0 mg/kg 3 mg/kg 6 mg/kg 9 mg/kg 12 mg/kg
Dose
N 11 12 12 12 11
Hematocr i t 40.4 • 3.5 30.5 + 8.8 29.6 + 8.7 34.6 + 7.2 30.2 + 8.2
pO 2 88.2 _+ 2.7 101.8 + 23.9 81.3 • 16.2 98.5 + 26.2 92.5 + 26.2
pCO z 40.8 +_ 29.5 23.0 +_ 7.4 28.4 • 7.4 26.2 +_ 6.6 26.7 +_ 4.8 pH 7.43 +_ 0.04 7.43 _+ 0.06 7.43 _+ 0.08 7.45 + 0.05 7.41 • 0.09
Blood pressure 122.9 _+ 15.0 96.0 _+ 26.4 98.3 + 13.7 109.1 _+ 13.7 101.2 _+ 23.9 Temperature 36.5 • 0.7 37.0 • 0.9 35.8 • 1.6 36.7 _+ 0.8 36.6 + 1.6
Weight change - 6.5 • 1.0 - 26.3 _+ 8.9 - 31.9 _+ 6.0 - 27.2 • 11.6 - 28.7 + 18.6 Plasma glucose 11.2 • 1.0 18.2 • 8.8 27.3 • 2.3 28.9 • 4.4 25.7 • 3.8

22
150
i 50"
[] K Otl/g/min)
[] F (ml/100g/min)
0 mg/kg 3 mg/kg 6 mg,'kg 9 mg/kg 12 mg/kg
Experimental Group, Dexamethasone Dose, rag/kg/day
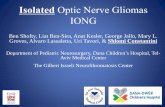
Fig. I. Blood flow and blood-to-tissue transport in RG-2 tumors
treated with dexamethasone. The mean + SD for all tumors in
each experimental group are shown for blood flow (E ml/100 g/
rain), and the rate of blood-to-tissue transport (K, gl/g/min) of
AIB. There is no effect of dexamethasone on either physiolog-
ical parameter , regardless of the dose that was used.
Results
Animal and tumor characteristics
A total of 178 intraparenchymal brain tumors were studied in 58 rats; 96 tumors were studied with AIB alone and 82 tumors were studied with both AIB and IAR Meningeal and subdural tumors were not included in the analysis. The histological patterns of tumor distribution and growth were similar to those already described [12].
The physiological values for each experimental group are shown in Table 1. There were differences between the control group, which did not receive dexamethasone, and all of the dexamethasone groups, particularly with regard to hematocrit, pCO2, blood pressure, weight change over the course of the experiment, and plasma glucose at the time of the experiment. Hematocrit, pCO2, blood pressure, and weight all decreased in the dexameth- asone treated animals while plasma glucose in- creased. The weight change in the control animals was significantly less than in any of the dexametha- sone treated groups (p < 0.05, ANOVA). Plasma glucose was significantly higher in each of the dexa- methasone treated groups than the controls (p < 0.05, ANOVA), although none of the dexametha-
sone-treated groups were significantly different from each other. None of the changes in the other categories was statistically significant.
Transfer constant (K) of AIB
Despite the dramatic changes of many of the physi- ological parameters of the experimental animals in the dexamethasone-treated groups, there was no significant difference in the whole tumor values of the transfer constant of AIB (Fig. 1) between any of the experimental groups (p > 0.05, ANOVA), i.e., there was no relationship between dexamethasone dose and the K value of AIB. There were no signif- icant differences between the values in tumor cen- ter or tumor periphery between any of the experi- mental groups, in BAT or BST (Fig. 2), nor in any of the tumor free brain regions that were examined (ipsilateral and contralateral white matter and cor- tex) (Fig. 2).
Because of concern that there may be a relation- ship between tumor size and the transfer constant of AIB [3], tumors were separated into three groups based on size in terms of maximum cross-sectional
15-
10-
-t
5-
; ~ ; 9 12 Dexamethasone Dose, rag&g/day
Brain Region
[] BAT
[] BST
[~ ILC
ILCC
[] CLC
[] CLCC
Fig. 2. Blood-to-tissue transport of AIB in the brain of animals with RG-2 tumors. Shown are the values (mean + SD) of the K of
AIB (gl/g/min) in a 250 g m zone of brain around all RG-2 tu- mors (BAT), brain 250-500 ].tm from the tumor edge (BST), and
in four areas of tumor free brain: ipsilateral cortex (ILC), ipsilat- eral corpus callosum (ILCC), contralateral cortex (CLC), and contralateral corpus callosum (CLCC). There is no effect of dex- amethasone on blood-to-tissue transport in any brain area.

area: small (< 1 mm2), medium (between 1 and 5 ram2), or large (> 5 mm 2) tumors. These size cate-
gories were intentionally selected to produce an even distribution of tumors per size category, e.g., about 12 tumors per size category per experimental group for the transfer constant. The numbers of tu- mors were evenly distributed between the experi- mental groups used for study of blood-to-tissue transport: control = 36, 3 mg/kg -- 38, 6 mg/kg -- 29, 9 mg/kg = 40, and 12 mg/kg = 35. There was no sig- nificant difference in the whole tumor values of the transfer constant of AIB (Table 2) between any of the experimental groups (p > 0.05, ANOVA), re- gardless of size. There was a tendency for smaller tumors (< 1 mm 2 cross-sectional area) to have lower
K values, but this was not consistent from group to group. When the relationship between tumor size and the K of AIB was examined for all tumors by linear regression, regardless of t reatment status, the fit gave a y-intercept of 32.5 gl/g/min and a slope of 0.284, and although the correlation coefficient was 0.16 (not significant), the slope had a p -- 0.03, which did indicate a small size effect.
When the regions of brain immediately outside
23
the tumor margin were examined (BAT and BST) by ROI analysis, there was no relationship between the K values in these regions and the administered dose of dexamethasone. Since we had previously re- ported a difference in the 125I-albumin distribution space in the brain around dexamethasone-treated animals with RG-2 tumors [3], we examined the dis- tribution profiles of 14C-AIB in each experimental
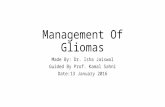
group. We selected those animals that had intrapa- renchymal tumors and that did not border on a lim- iting structure (e.g., ventricle, meninges, or another tumor). The data from this transition area was com- bined for all animals of each experimental group, and examined as a function of K versus distance from tumor edge. These results are presented in Fig. 3, in which there was a distinct trend for K val- ues to decrease more rapidly away from the tumor margin with increasing dexamethasone dose. The distance at which the normalized K value was 50% of its value at the tumor edge was 0.35 mm in the control group, 0.25 mm in the 3 mg/kg, 0.225 mm in the 6 mg/kg group, and 0.175 mm in both the 9 and 12 mg/kg groups.
Table 2. Transfer constant (K) of AIB and blood flow (F) for RG-2 tumors according to experimental group and size. For each experi- mental group, in terms of dexamethasone dose (mg/kg/day), the tumors have been separated into 3 different size categories (A = 0-1 mm 2, B = 1-5 mm 2, and C > 5 mm 2. For each category are shown the number of tumors studied (N), the size of the tumors, the value of the transfer constant of AIB (K, gl/g/min), and the blood flow value (F ml/100 g/min). Values are means _+ SD
Experimental Tumor size Transfer N Tumor size Blood flow group N (ram 2) constant (mm 2) (ml/100 g/rain)
(gl/g/min)
A 12 0.5• 25.1• 2 0.9• 73.5• 0mg/kg B 13 2.0• 38.9• 8 2.0• 108.6•
C 11 15.5• 40.5• 5 15.7• 64.2• A 16 0.6• 32.2• 10 0.6• 121.8•
3mg/kg B 10 2.4• 34.2• 6 2.6• 76.5• C 12 17.6• 37.2• 6 18.4• 85.8• A 11 0.6• 20.5• 2 0.4• 110.0•
6mg/kg B 11 2.1• 40.4• 3 2.1• 124.2• C 7 20.3• 37.6• 2 20.9• 55.5• A 14 0.5• 34.5• 6 0.4• 85.4•
9mg/kg B 15 2.6• 32.0• 4 2.2• 77.8• C 11 25.5• 46.0• 3 32.6• 55.5• A 11 0.6• 31.7• 7 0.5• 88.7•
12mg&g B 15 2.4• 31.3• 12 2.6• 100.2• C 9 18.9• 38.6• 6 23.0• 105.8•

24
0.75
>
0.5
0.25 -
Dexamethasone Dose
.... o---- 6 mg/kg
"~
,. -r& �9 . %..~
0, l 0 .2 0.3 0,4 0.5
Distance From Tumor Edge (ram)
Fig. 3. Blood-to-tissue transport values of AIB at tumor edge in
large intraparenchymal RG-2 tumors. Shown are the normalized
values of the K of AIB from tumor edge to 0.5 m m away from the
tumor edge. The values from each tumor were normalized by
dividing the value at each point by that tumor ' s value at the tu- mor edge. This resulted in a value of 1.0 for each tumor at its edge,
and allowed the values f rom several tumors to be combined.
There is a clear dose related effect of dexamethasone: with in-
creasing dose of dexamethasone the K of AIB decreases more
rapidly away from the edge of the tumor. A solid line is drawn at
0.5 on the vertical axis; at this point the K value is at 50% of its
maximum.
Blood f low
Figure i shows the values of blood flow, E to all tu- mors, according to experimental group. Table 2 summarizes the blood flow values in the different experimental groups according to tumor size. There was no significant difference in blood flow values between any of the groups (p < 0.05, ANOVA), nor were there any differences in other brain regions that were studied.
Discussion
Our experimental results do not support the con- cept that dexamethasone reduces cerebral edema by decreasing the permeability of brain tumor ves- sels or by affecting blood flow to the tumors. In these experimental RG-2 tumors, we were unable to demonstrate an effect of large doses of dexa- methasone (3 to 12 mg/kg/day) on the blood-to-tis- sue transport of AIB. In addition, we found no ef- fect of dexamethasone on the transport of AIB in
tumor-free brain regions. Finally, tumor blood flow was not affected by the administration of dexa- methasone.
It may be important to distinguish between the effects of dexamethasone on normal brain vessels, in which transcapillary transport is determined by simple diffusion, and tumor vessels, in which bulk flow predominates. Ziylan et al. have reported on the effects of dexamethasone on blood-to-tissue transport of AIB in normal brain [22, 23]. In one study the authors administered dexamethasone at a dose of 2 mg/kg daily for 3 days or in a single dose 3 h prior to the experiments [23]; although signif- icant, the magnitude of the decreased K values for AIB were small: the mean decrease for all brain re- gions was 0.55 gl/g/min in the 3 h group and 0.94 gl/ g/min in the 3 day group. In the other study [22] the authors administered dexamethasone at a dose of 0.8 mg/kg/day for three weeks; the mean decrease in the K of AIB was 0.63 gl/g/min. Our experiments were very similar to those of Ziylan et al. except that we used much larger doses of dexamethasone and we did not use a vascular space correction (less than 5 % of the amount of AIB-radioactivity is in the vas- cular space at 10 min [19]). Although we observed changes in the K of AIB of a similar magnitude in different brain regions (Fig. 2) as did Ziylan et al.,
the changes were not dose-related and were not consistent, perhaps related to the fact that these animals were tumor-bearing and were sick. Wheth- er or not dexamethasone effect on the permeability of normal brain vessels is clinically important will be determined by whether the small changes (< i gl/ g/min) are clinically relevant to the particular drug being considered.
With regard to brain tumors, the available litera- ture about the effects of dexamethasone suggests considerable variability from tumor to tumor, par- ticularly with regard to blood flow and blood-to-tis- sue transport of water-soluble compounds. In ani- mal studies, Yamada et al. reported a 40% decrease in the blood-to-tissue transport AIB after 5 days of treatment with methylprednisolone (15 mg/kg/day) [7]. In previous studies of the effects of dexametha- sone on RG-2 rat gliomas, we reported that dexa- methasone significantly reduced the size of the ex- tracellular space, and although not significant, dex-

amethasone also reduced the Ka of albumin, the plasma vascular volume, and the tissue vascular vol- ume [3, 4]. Luthert et aI. were unable to demon- strate a change in the K 1 of mannitol in transplanted A15A5 rat gliomas [2]. Shapiro et al. demonstrated a marked reduction in the K of AIB one hour after administration of dexamethasone to rats with trans- planted C6 gliomas [5]. In dogs, we observed a vari- able effect of dexamethasone on the K 1 of meglu- mine iothalamate in avian sarcoma virus-induced gliomas [24]. In human subjects, Leenders et al.
demonstrated a significant reduction in tumor blood flow, blood volume, and a variable change in oxygen extraction ratio using 150 2 positron emission tomography after dexamethasone administration, but no change in the K 1 of 82Rb [8, 11]. Jardin et al.
showed a significant reduction in K 1 of 82Rb in pri- mary and metastatic tumors after dexamethasone administration [9, 10].
In normal brain, the permeability of passively distributed solutes is determined by the ability of a solute to dissolve in and diffuse through the capil- lary membrane, and is related to the physical size and lipid solubility of the solute. However, in brain tumors the capillaries are structurally altered. In RG-2 tumor capillaries, both fenestrations and in- terendothelial discontinuities are found [unpub- lished observations]. These 'holes' change the na- ture of the movement of many substances across the blood-brain barrier from a process of simple diffu- sion into one in which bulk flow (convection) be- comes operative and the effects of hydrostatic and osmotic pressure gradients, which are so important in determining solute movement across systemic capillaries, come into play. In terms of the Starling equation, volume flux (Jv) across the capillary wall is given by:
= G [ - G m O - 2 Z Os(F .,v. - Fl. ,vs) ]
where Lp is hydraulic conductivity, Pmv is microvas- cular hydrostatic pressure, Ppmv is perivascular in- terstitial hydrostatic pressure, % is the reflection coefficient of solute s, I-Imv s and 1-Ipmw are the micro- vascular and perivascular osmotic pressures of sol- ute s, respectively. This is a general expression for bulk fluid flow across a capillary. It is important to
25
note that 'permeability' does not appear in the Star- ling equation, and of the terms that do appear, nei- ther hydraulic conductivity (Lp) nor the reflection coefficient (cy) lend themselves to experimental measurement. However, Lp, (y, and permeability (p), the three parameters that characterize a passive membrane [22], can be interrelated:
Jv 2
and
Jv
Unfortunately, Lp, •, and p cannot be measured di- rectly in in vivo experiments. Most experiments are designed to measure either a permeability-surface area product (PA or PS) or a blood-to-tissue trans- fer constant (K) [23], both of which are related to permeability.
If a true reduction in capillary permeability is not the only, nor perhaps not even the dominant mecha- nism in dexamethasone-induced reduction of tu- mor-associated cerebral edema in many brain tu- mors, it becomes important to consider other pos- sible mechanisms. Examination of Equation i sug- gests several ways in which dexamethasone could act to reduce total transcapillary movement. For ex- ample, if as a result of dexamethasone effect, capil- lary hydraulic conductivity (Lp) decreased or the re- flection coefficient (g) of albumin increased, then net flux of albumin across the capillary wall by bulk flow would be decreased. Operationally, this could be explained if dexamethasone decreased the size of interendothelial gaps between tumor capillaries and increased molecular sieving. In the latter situa- tion the rate of transcapillary movement of small molecules (e.g., AIB, meglumine iothalamate, or 82Rb) might not be affected, while the rate of tran- scapillary transport of albumin would be reduced and brain edema would concomitantly decrease. However, this hypothesis cannot be supported from observations in RG-2 gliomas, where dexametha- sone failed to change the K a of albumin in the tu- mors [3].
The two pressure gradients in Equation i can also

26
be examined. If the hydrostatic pressure gradient (Pmv-Ppmv) were decreased, either through a reduc- tion in Pray or an increase in Ppmv, then the hydrostat- ic pressure gradient across the capillary wall would decrease and Jv and K 1 would also decrease. Dexa- methasone has been reported to decrease brain tu- mor blood flow [8,11], and in a freeze lesion model, Fenstermacher and coworkers have suggested that blood flow may be decreased by increased resist- ance of arteries proximal to the lesion, which could be one mechanism by which microvascular hydros- tatic pressure is decreased [24, 25]. Increased inter- stitial pressure (Ppmv), reported in systemic tumors by Kristjansen et al. [26], was decreased after ad- ministration of dexamethasone. These authors pro- posed that the mechanism for the decrease in inter- stitial pressure was a reduction in capillary perme- ability.
Perhaps the most difficult part of the Starling equation to unravel experimentally is the osmotic pressure gradient (I'Imvs--I'Ipmvs), which works in a di- rection opposite to the hydrostatic pressure gra- dient. Assuming that plasma osmotic pressure did not change, increased osmotic pressure in the extra- cellular space of tumors would increase the bulk flow from blood to tissue; conversely, decreasing the osmotic pressure in the extracellular space would decrease the bulk flow into tissue. Movement of albumin, the principal component of the plasma osmotic pressure, into brain tumor extracellular space, is well documented. Clinically, it formed the basis for the original radionuclide brain scans. We demonstrated an increase in the KI of albumin from ~- 0.002 gl/g/min in normal brain to 2.36 gl/g/min in large RG-2 tumors, an ll00-fold increase [3]. Bothe et al. measured the protein in brain tumor extracel- lular fluid and found values of 1.9 gg/mg tissue in normal gray matter and 28.4 gg/mg at a distance of 2 mm from the edge of a brain tumor [27]. Hoss- mann et al. used semiquantitative techniques to demonstrate that corticosteroids 'reduced the wa- ter content of peritumoral brain tissue but did not affect increased permeability of tumor vessels, and only slightly improved peritumoral accumulation of serum proteins' [28]. Changes in the transcapillary osmotic pressure gradient that are unrelated to changes in capillary permeability hydraulic conduc-
tivity, or the reflection coefficient, although poorly understood at present, represent one of the most powerful ways of influencing bulk flow across the tumor capillary, and must be considered in the de- sign of future studies.
Finally, alternative effects of steroids unrelated to vascular physiology should not be neglected, such as effects on metabolism. Glucocorticoids, like dexamethasone, are powerful catabolic steroids, and may cause significant protein catabolism, as evidenced by the profound weight loss we observed in the experimental groups. If protein catabolism were increased in brain tumors, it would prove to be a simple and direct method of decreasing concen- trations of albumin in the tumor extracellular space, which would translate into a reduced osmotic gra- dient across the tumor capillary wall and a reduced movement of fluid and solutes into the tumor extra- cellular space, with any change in capillary perme- ability. Recently, Hassel et al. suggested that albu- min itself may be neurotoxic [29]. If dexamethasone increased catabolism of albumin in brain around tu- mor, the clinical improvement and reduced edema associated with administration of dexamethasone could conceivably be due to improved neuronal and glial 'health' and unrelated to vascular physiology.
In our original studies of albumin in RG-2 rats, we observed a decrease in the distribution space profile of 125 I-albumin at the tumor margin [3]. We observed similar profiles with AIB in the current experiments (Fig. 3). Earlier, we hypothesized that three mechanisms could explain this observation: (1) the vessels in BAT are intermediate in perme- ability between brain and tumor and show de- creased permeability after dexamethasone treat- ment; (2) the apparent rate of diffusion of albumin decreases after dexamethasone treatment; or, (3) the rate of bulk flow of edema fluid through brain is reduced by dexamethasone treatment. The same three possibilities exist to explain the AIB profiles in Fig. 3. However, unlike albumin, AIB crosses cell membranes by facilitated transport [3]. Therefore, diffusion of AIB in brain around tumor will prob- ably be a more complex event than for albumin, for which a facilitated transport system does not exist.
In light of these experimental results, it is impor- tant to briefly reconsider the consequences of dexa-

methasone-induced reduction in brain tumor capil- lary permeability. First, with a few exceptions, the magnitude of the reported decreases in K 1 values in brain tumors has not been large, especially in com- parison to the difference between the K 1 values in tumors and those of normal brain. Thus, dexameth- asone is not likely to significantly reduce the blood- to-tissue delivery of water-soluble chemother- apeutic drugs. Second, a dexamethasone-induced decrease in KI is not likely to be the complete expla- nation for the reduction of tumor-associated brain edema. Other mechanisms need to be explored to explain the effect. We continue to believe that it is important to understand how dexamethasone re- duces tumor-associated brain edema, since once the mechanism is understood perhaps other drugs could be found that produce the same result with- out the associated side effects of dexamethasone. Third, since our results differ markedly from those of Shapiro et al. [5], it is important to acknowledge that the effects of dexamethasone on brain tumor capillaries may vary from one tumor to the next, like so many other properties of malignant gliomas. RG-2, which is a highly reproducible tumor, might be expected to behave quite differently from other clonal brain tumor cell lines. Variability in dexa- methasone effect on permeability would be clinical- ly important to know, since it would greatly affect the design of therapeutic trials where a standar- dized dosing regimen is used with the assumption that the same amount of drug will reach each tumor.
Acknowledgments
Dr. Molnar was supported by the Mark Moritz Me- morial Brain Tumor Research Fund and by a Hun- garian Scientific Research Grant (OTKA # 1493). This work was supported by NIH grants RO1- NS12745 (Jacob Javits Neuroscience Investigator Award) and $10-RR03321, by the Richard M. Li- lienfeld Brain Tumor Research Fund and by the Neurooncology Research Fund of Evanston Hospi- tal Corporation.
27
References
1. Reulen H-J, Hadjidimos A, Phase A: Steroids in the treat- ment of brain edema. In: Schurmann K, Brock M, Reulen H-J, Voth D (eds) Cerebello Pontine Angle Tumors: Diag- nosis and Surgery. Springer-Verlag, Berlin, 1973, pp. 92-105
2. Luthert P J, Greenwood J, Lantos PL, Pratt OE: The effect of dexamethasone on vascular permeability of experimental brain tumors. Acta Neuropathologica (Bed). 69: 288-294, 1986
3. Nakagawa H, Groothuis DR, Owens ES, Fenstermacher JD, Patlak CS, Blasberg RG: Dexamethasone effects on 125I- albumin distribution in experimental RG-2 gliomas and ad- jacent brain. J Cerebral Blood Flow. Metab. 7: 687-701,1987
4. Nakagawa H, Groothuis DR, Owens ES, Patlak CS, Blasb- erg RG: Dexamethasone effects on vascular volume and tis- sue hematocrit in experimental RG-2 gliomas and adjacent brain. J Neuro-Oncol 6: 157-168, 1988
5. Shapiro WR, Hiesiger EM, Cooney GA, Basler GA, Lip- schultz LE, Posner JB: Temporal effects of dexamethasone on blood-to-brain and blood-to-tumor transport of ~4C-al- pha-aminoisobutyric acid in rat C6 glioma. J Neuro-Oncol 8: 197-204, 1990
6. Yamada K, Bremer AM, West CR: Effects of dexametha- sone on tumor-induced brain edema and its distribution in the brain of monkeys. J Neurosurg 50: 361-367, 1979
7. Yamada K, Ushio Y, Hayakawa T, Arita N, Yamada N, Mo- gami H: Effects of methylprednisolone on peritumoral brain edema: a quantitative autoradiographic study. J Neu- rosurg 59: 612-619,1983
8. Brooks D J, Beaney RE Leenders KL: The effect of dexa- methasone therapy on cerebral haemodynamics, oxygen utilization and blood-brain barrier permeability in patients with brain tumors. In: Capildeo R (ed): Steroids in Diseases of the Central Nervous System. John Wiley and Sons, New York, 1989, pp. 59-68
9. Jarden JO, Dhawan V, Poltorak A, J.B. P, Rottenberg DA: Positron emission tomographic measurement of blood-to- brain and blood-to-tumor transport of 82Rb: the effect of dexamethasone and whole-brain radiation therapy. Ann Neuro118: 636-646, 1985
10. Jarden JO, Dhawan V, Moeller JR, Strother SC, Rottenberg DA: The time course of steroid action on blood-to-brain and blood-to-tumor transport of 82Rb: a positron emission tomo- graphic study. Ann Neuro125: 239-245, 1989
11. Leenders, KL, Beany D J, Brooks D J, Lammertsma JD, Heather JD, McKenzie CG: Dexamethasone treatment of brain tumor patients: Effects on regional cerebral blood flow, blood volume, and oxygen utilization. Neuro135:1610- 1616,1985
12. Groothuis DR, Fischer JM, Pasternak JR Blasberg RG, Bigner DD, Vick NA: Regional measurements of blood-to- tissue transport in transplanted RG-2 rat gliomas. Cancer Res 43: 3368-3373, 1983
13. Blasberg RG, Groothuis DR, Molnar P: The application of

28
quantitative autoradiographic measurements in experimen- tal brain tumors. Sem Neurol 1: 203-223, 1981
17. Molnar R Blasberg RG, Groothuis DR, Bigner DD, Fen- stermacher JD: Regional blood-to-tissue transport in avian sarcoma virus (ASV)-induced brain tumors. Neuro133: 702- 711, 1983
15. Blasberg RG, Groothuis DR, Molnar P: The application of quantitative autoradiographic measurements in experimen- tal brain tumors. Sem Neurol 1: 203-221, 1981
16. Vriesendorp FJ, Groothuis DR, Vick NA: Murine sarcoma virus-induced brain tumors: concurrent measurements of blood flow and transcapillary transport. J Neuro-Oncol 2: 301-314, 1984
1% Sakurada O, Kennedy C, Jehle J, Brown JD, Carbin G, So- koloff L: Measurement of local cerebral blood flow with io- do[~4C]antipyrine. Am J Physiol 234: H59-H66, 1978
18. Blasberg R, Patlak C, Fenstermacher J: The transport of al- pha-aminoisobutyric acid across brain capillary and cellular membranes. J Cerebral Blood Flow Metab 3: 8-32, 1983
19. Ziylan YZ, Lefauconnier JM, Bernard G, Bourre JM: Re- gional alterations in blood-to-brain transfer of c~-aminoiso- butyric acid and sucrose, after chronic administration and withdrawal of dexamethasone. J Neurochem 52: 684-689, 1989
20. Ziylan YZ, LeFauconnier JM, Bernard G, Bourre JM: Ef- fect of dexamethasone on transport of c~-aminoisobutyric acid and sucrose across the blood brain barrier. J Neuro- chem 51: 1338-1342,1988
21. Warnke PC, Molnar PD, Lapin GD, Kuruvilla A, Groothuis DR: The effects of dexamethasone on transcapillary trans- port in experimental brain tumors: II. Canine brain tumors. J Neuro-Onco125: 29-38, 1995
22. Benedek GB, Villars FMH: Physics With Illustrative Exam- ples From Medicine and Biology. In (ed): Addison-Wesley Publ. Co., Reading, MA, 1979
23. Fenstermacher JD, Blasberg RG, Patlak CS: Methods for quantifying the transport of drugs across brain barrier sys- tems. Pharmacol Ther 14: 217-248, 1981
24. Tajima A, Yen M-H, Nakata H etaL: Effects of dexametha- sone on blood flow and volume of perfused microvessels in traumatic brain edema. In: Long DM (ed) Brain Edema: Pathogenesis, Imaging and Therapy. Raven Press, New York, 1990, pp 343-350
25. Yen M-H, Wright D, Nakagawa H e t al.: Effects of dexa- methasone on the blood-brain distribution of [~25I]albumin and [~4C]alpha-aminoisobutyric acid in vasogenic cerebral edema. In: Inaba Y, Klatzo I, Spatz M (ed) Brain Edema. Springer Verlag, Berlin, 1985, pp. 638-645
26. Kristjansen PEG, Boucher Y, Jain RK: Dexamethasone re- duces the interstitial pressure in a human colon adenocarci- noma xenograft. Cancer Res 53: 4764-4766, 1993
27. Bothe H-W, Bodsch W, Hossmann K-A: Relationship be- tween specific gravity, water content, and serum protein ex- travasation in various types of vasogenic brain edema. Acta Neuropathologica 64: 37-42,1984
28. Hossman K-A, Hurter T, Oschlies U: The effect of dexa- methasone on serum protein extravasation and edema de- velopment in experimental brain tumors of cat. Acta Neuro- pathologica 60: 223-231, 1983
29. Hassel B, Iversen EG, Fonnum F: Neurotoxicity of albumin in v~vo. Neurosci Lett 167: 29-32, 1994
Address for offprints: D.R. Groothuis, Burch Hall G21, Evanston Hospital, 2650 Ridge Avenue, Evanston, IL 60201, USA