The early and mid-term results of mitral valve repair for mitral regurgitation in children
6
ORIGINAL ARTICLE The early and mid-term results of mitral valve repair for mitral regurgitation in children Zhaolei Jiang • Ju Mei • Fangbao Ding • Chunrong Bao • Jiaquan Zhu • Min Tang • Nan Ma • Jianbing Huang • Saie Shen Received: 2 May 2013 / Accepted: 5 November 2013 Ó Springer Japan 2013 Abstract Purpose To review the surgical techniques and mid-term results of mitral valve repair in children with moderate or severe mitral regurgitation (MR). Methods One hundred and seven children with moderate or severe MR, aged 19.6 ± 8.5 months, were enrolled in this study. The surgical techniques used for mitral valve repair varied according to the mitral valve morphology, and included annuloplasty, annuloplasty ring, cleft closure, reconstruction of the posterior leaflet, etc. The concomitant cardiac anomalies were treated simultaneously. The results of repair were evaluated by transesophageal echocardiog- raphy performed during the operation and by serial trans- thoracic echocardiography performed during the follow-up. Results One hundred and six cases had no more than mild regurgitation intraoperatively, whereas only one case had moderate regurgitation. This patient underwent redo repair immediately, and the subsequent regurgitation was trivial. The in-hospital mortality rate was 0.9 % (1/107). The average follow-up was 46.5 ± 8.2 months. One patient died of heart failure 10 months postoperatively. The free- dom from moderate or severe regurgitation after mitral valve repair was 92.3 ± 3.3 %. Conclusion Pediatric patients with moderate or severe MR require early surgical treatment. The early and mid- term results of mitral valve repair in pediatric patients were satisfactory. Keywords Mitral regurgitation Á Mitral valve repair Á Children Introduction Mitral regurgitation (MR) is a common cardiac disease that occurs mainly due to degenerative valve disease, ischemic heart disease, rheumatic heart disease, congenital heart disease, infective endocarditis and Marfan comprehensive symptom in adults [1–4]. However, pediatric MR is rare, complex and frequently associated with other congenital cardiac abnormalities [5–8]. Mitral valve surgery (mitral valve repair and mitral valve replacement) can alleviate the clinical symptoms and prevent ventricular dilatation and heart failure, especially for patients with moderate or severe MR [9]. Since mitral valve replacement is associ- ated with a high mortality rate, high reoperation rate and issues with anticoagulation, mitral valve repair has been considered to be the preferred method for treating MR in pediatric patients [10, 11]. Currently, mitral valve repair has achieved satisfactory results in adults [1, 3]. However, mitral valve repair remains a challenge in pediatric patients, because the pathology of MR varies and the mitral valve apparatus is still growing in children [12, 13]. Some additional diffi- culties still exist in pediatric mitral valve repair [14]. For example, the pediatric valve tissue is fragile. And the spectrum of lesions is wide, including annular dilatation, leaflet clefts, leaflet defects, leaflet prolapsed, etc. [6, 10]. Z. Jiang Á J. Mei (&) Á F. Ding Á C. Bao Á J. Zhu Á M. Tang Á N. Ma Á J. Huang Department of Cardiothoracic Surgery, Xinhua Hospital, Shanghai Jiaotong University School of Medicine, 1665 Kongjiang Road, Shanghai 200092, China e-mail: [email protected] S. Shen Department of Anesthesiology, Xinhua Hospital, Shanghai Jiaotong University School of Medicine, Shanghai 200092, China 123 Surg Today DOI 10.1007/s00595-013-0816-x
Transcript of The early and mid-term results of mitral valve repair for mitral regurgitation in children

ORIGINAL ARTICLE
The early and mid-term results of mitral valve repair for mitralregurgitation in children
Zhaolei Jiang • Ju Mei • Fangbao Ding •
Chunrong Bao • Jiaquan Zhu • Min Tang •
Nan Ma • Jianbing Huang • Saie Shen
Received: 2 May 2013 / Accepted: 5 November 2013
� Springer Japan 2013
Abstract
Purpose To review the surgical techniques and mid-term
results of mitral valve repair in children with moderate or
severe mitral regurgitation (MR).
Methods One hundred and seven children with moderate
or severe MR, aged 19.6 ± 8.5 months, were enrolled in
this study. The surgical techniques used for mitral valve
repair varied according to the mitral valve morphology,
and included annuloplasty, annuloplasty ring, cleft closure,
reconstruction of the posterior leaflet, etc. The concomitant
cardiac anomalies were treated simultaneously. The results
of repair were evaluated by transesophageal echocardiog-
raphy performed during the operation and by serial trans-
thoracic echocardiography performed during the follow-up.
Results One hundred and six cases had no more than mild
regurgitation intraoperatively, whereas only one case had
moderate regurgitation. This patient underwent redo repair
immediately, and the subsequent regurgitation was trivial.
The in-hospital mortality rate was 0.9 % (1/107). The
average follow-up was 46.5 ± 8.2 months. One patient
died of heart failure 10 months postoperatively. The free-
dom from moderate or severe regurgitation after mitral
valve repair was 92.3 ± 3.3 %.
Conclusion Pediatric patients with moderate or severe
MR require early surgical treatment. The early and mid-
term results of mitral valve repair in pediatric patients were
satisfactory.
Keywords Mitral regurgitation � Mitral valve repair �Children
Introduction
Mitral regurgitation (MR) is a common cardiac disease that
occurs mainly due to degenerative valve disease, ischemic
heart disease, rheumatic heart disease, congenital heart
disease, infective endocarditis and Marfan comprehensive
symptom in adults [1–4]. However, pediatric MR is rare,
complex and frequently associated with other congenital
cardiac abnormalities [5–8]. Mitral valve surgery (mitral
valve repair and mitral valve replacement) can alleviate the
clinical symptoms and prevent ventricular dilatation and
heart failure, especially for patients with moderate or
severe MR [9]. Since mitral valve replacement is associ-
ated with a high mortality rate, high reoperation rate and
issues with anticoagulation, mitral valve repair has been
considered to be the preferred method for treating MR in
pediatric patients [10, 11].
Currently, mitral valve repair has achieved satisfactory
results in adults [1, 3]. However, mitral valve repair
remains a challenge in pediatric patients, because the
pathology of MR varies and the mitral valve apparatus is
still growing in children [12, 13]. Some additional diffi-
culties still exist in pediatric mitral valve repair [14]. For
example, the pediatric valve tissue is fragile. And the
spectrum of lesions is wide, including annular dilatation,
leaflet clefts, leaflet defects, leaflet prolapsed, etc. [6, 10].
Z. Jiang � J. Mei (&) � F. Ding � C. Bao � J. Zhu � M. Tang �N. Ma � J. Huang
Department of Cardiothoracic Surgery, Xinhua Hospital,
Shanghai Jiaotong University School of Medicine,
1665 Kongjiang Road, Shanghai 200092, China
e-mail: [email protected]
S. Shen
Department of Anesthesiology, Xinhua Hospital,
Shanghai Jiaotong University School of Medicine,
Shanghai 200092, China
123
Surg Today
DOI 10.1007/s00595-013-0816-x
In addition, the surgical exposure is limited. Since children
are still growing, some repair techniques are not applicable
or routinely used in pediatric patients, such as a continuous
annuloplasty ring, triangular resection of the anterior mitral
leaflet and chordal replacement. At present, only a few of
studies with a small sample of patients related to pediatric
mitral valve repair have been reported [12, 13, 15, 16].
In this study, we aimed to share our experience with
mitral valve repair for MR in children. We retrospectively
analyzed 107 pediatric cases of moderate or severe MR
who had undergone mitral valve repair, and observed the
early and mid-term outcomes of the repair.
Materials and methods
Patients
We retrospectively analyzed the pediatric patients with
moderate or severe MR who had undergone mitral valve
repair from 2005 to 2012 in Shanghai Xinhua hospital,
which was affiliated with Shanghai Jiaotong University.
One hundred and seven pediatric patients (45 males, 62
females) were identified. The age at the operation ranged
from 2 months to 6 years (median age 19.6 ± 8.5 months),
and 45 patients (42.1 %) were younger than 1 year. The
patients’ weight at the time of the operation ranged from 4
to 21 kg (median weight 12.3 ± 6.5 kg), and 51 cases
(47.7 %) were lighter than 10 kg. All patients underwent
preoperative transthoracic echocardiography (TTE) to
determine the mechanism of MR and evaluate the degree of
regurgitation. The etiology of MR included congenital
heart disease in 101 cases and infective endocarditis in six
cases. Eighty-nine MR patients had other associated car-
diac abnormalities, such as a ventricular septal defect, atrial
septal defect, patent ductus arteriosus, pulmonary stenosis,
left ventricular outflow tract obstruction, tetralogy of Fallot
or an anomalous origin of the left coronary artery
(Table 1).
Mitral pathology
MR was graded as none (0), trivial (?), mild (??),
moderate (???) or severe (????) based on the maxi-
mum length and width of the abnormal jet relative to the
left atrium [17, 18]. Echocardiography showed that there
was moderate regurgitation in 38 cases and severe regur-
gitation in 69 cases.
The mitral pathology was classified into three groups
according to the leaflet motion [6, 7]: type I indicated
normal leaflet motion (annular dilatation, leaflet cleft,
leaflet defect), type II was associated with prolapsed leaf-
lets (elongated chordae, elongated papillary muscle, absent
chordae, torn chordae) and type III was associated with
restricted leaflet motion (short chordae, papillary muscle
commissural fusion, papillary muscle hypoplasia)
(Table 2). Annular dilatation was the predominant pathol-
ogy in our series, which was present in 66 cases (61.7 %).
Surgical techniques
Mitral valvuloplasty (MVP) was performed with cardio-
pulmonary bypass under moderate systemic hypothermia.
The techniques used for MVP varied according to the
mitral valve morphology. The methods used for MVP
Table 1 Associated cardiac abnormalities
Associated abnormalities n
Ventricular septal defect 65
Atrial septal defect 13
Patent ductus arteriosus 4
Pulmonary stenosis 3
Left ventricular outflow tract obstruction 2
Tetralogy of fallot 1
Anomalous origin of the left coronary artery 1
Total 89
Table 2 Carpentier classification of mitral valve pathology
Classification of mitral valve pathology n
Normal leaflet motion (type I) 82
Annular dilatation 66
Leaflet cleft 13
Leaflet defect 3
Leaflet prolapse (type II) 22
Elongated chordae 12
Elongated papillary muscle 5
Absent chordae 3
Torn chordae 2
Restricted leaflet motion (type III) 3
Short chordae 1
Papillary muscle commissural fusion 1
Papillary muscle hypoplasia 1
Table 3 Mitral valvuloplasty techniques
Surgical techniques used for MVP n
Annuloplasty 85
Annuloplasty ring 19
Cleft closure 13
Reconstruction of the posterior leaflet 10
Chordal shortening 12
Papillary muscle shortening 5
Surg Today
123

included annuloplasty (n = 85), annuloplasty ring (n = 19),
cleft closure (n = 13), reconstruction of the posterior
leaflet (n = 10), chordal shortening (n = 12) and papillary
muscle shortening (n = 5) (Table 3). Annuloplasty,
including REED annuloplasty, posterior annuloplasty and
commissuroplasty, was commonly carried out for annular
dilatation, leaflet cleft, leaflet prolapse and restricted leaflet
motion. An annuloplasty ring was used in children with
significant annular dilatation. A band of pericardium trea-
ted with glutaraldehyde or polytetrafluoroethylene (PTFE)
could be sutured around the posterior annulus and mitral
commissure (Fig. 1). The continuity of the band could be
interrupted once or twice to allow for subsequent growth.
For posterior leaflet prolapse, we preferred to use posterior
leaflet quadrangular or triangular resection, pleating the
posterior annulus, suturing the cutting edge, and some
cases also required a prosthetic ring. Elongation of chordae
or papillary muscle could be used to treat chordal short-
ening or papillary muscle shortening. All patients with
leaflet cleft were repaired by interrupted simple prolene
sutures.
Several techniques were sometimes used in a single
patient. The concomitant cardiac anomalies were treated at
the same time. The results of repair were evaluated by
transesophageal echocardiography (TEE) after cardiopul-
monary bypass.
Follow-up
Follow-up information was obtained from the medical
records and outpatient interviews. All follow-up informa-
tion was recorded on standardized forms and entered
into the computerized database. The echocardiography
examinations were performed by one senior pediatric
cardiologist.
Statistical methods
The statistical analysis was performed with the SPSS ver-
sion 18.0 software program. The freedom from moderate or
severe MR after MVP was determined by the Kaplan–
Meier method. The data were expressed as proportions or
the mean ± SD. Intergroup comparisons were performed
using Student’s t test. Results were considered to be sig-
nificant for values of P \ 0.05.
Results
Perioperative data
MVP was successfully performed in all patients. The mean
cardiopulmonary bypass time was 80.6 ± 32.1 min. The
mean aortic clamp time was 43.2 ± 17.5 min. The results
of intraoperative TEE showed that 106 cases had no to mild
MR, whereas one case had residual moderate MR. This
patient underwent redo repair immediately, and the sub-
sequent regurgitation was trivial.
Early postoperative results
The in-hospital mortality was 0.9 % (1/107). This patient
was a female with a large ventricular septal defect (VSD)
and pulmonary hypertension (PH), who died as a result of a
pulmonary infection at 1 month postoperatively. The early
postoperative complications mainly included low cardiac
output syndrome (n = 3), respiratory dysfunction (n = 3),
pleural effusion (n = 2) and wound infection (n = 1). The
mean postoperative ventilation time was 30.7 ± 28.5 h.
The mean length of the ICU stay was 4.0 ± 3.2 days, and
the mean postoperative hospital stay was 8.6 ± 5.9 days.
Follow-up results
Follow-up data were available for 91 patients (85.8 %)
after hospital discharge. The average follow-up time was
46.5 ± 8.2 months (3–80 months). TTE at 30 days post-
operatively showed that the left atrial dimension (LAd) and
left ventricular end diastolic volume (LVEDV) were sig-
nificantly reduced in the postoperative period compared
with the preoperative values (Table 4). One patient died of
heart failure 10 months postoperatively. Echocardiography
showed that moderate MR was present in five patients, and
one patient had severe MR. The patient with severe MR
underwent reoperation by mitral valve replacement, and
Fig. 1 An annuloplasty ring
Table 4 A comparison of LAd and LVEDV: preoperative vs one
month postoperative
Value Preoperative
(n = 107)
1 month postoperative
(n = 91)
P
LAd (mm) 25.3 ± 7.2 21.5 ± 4.8 \0.05
LVEDV (ml) 55.8 ± 26.3 40.8 ± 23.2 \0.05
Surg Today
123
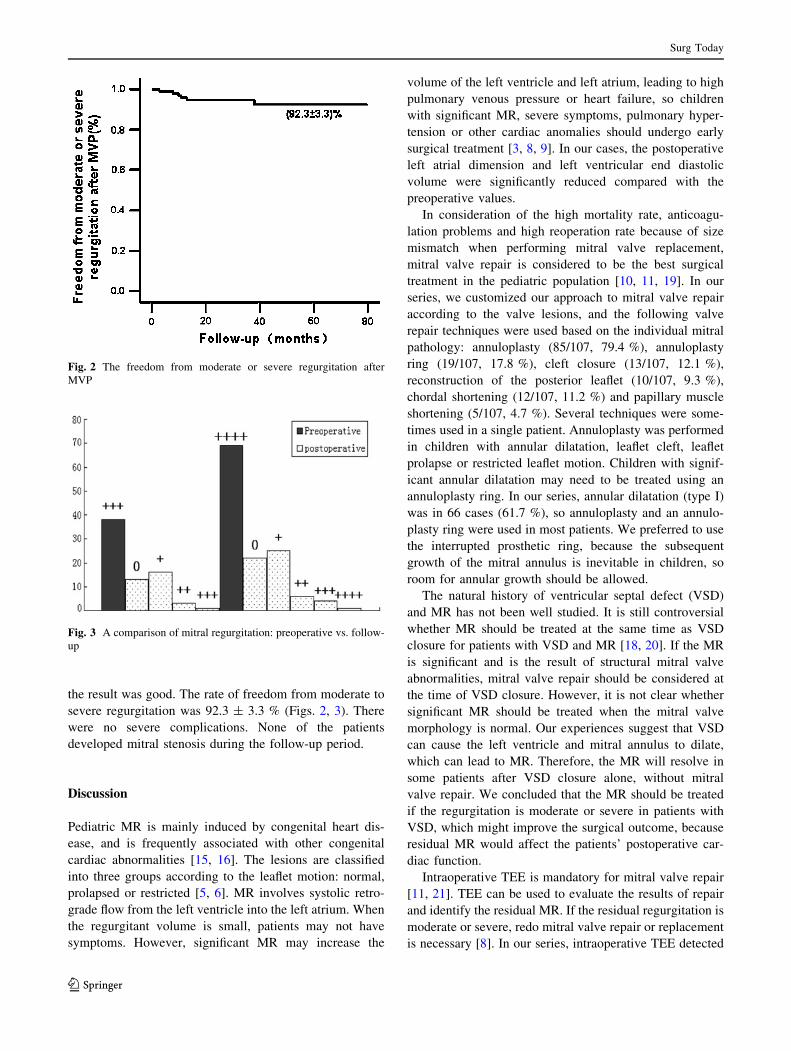
the result was good. The rate of freedom from moderate to
severe regurgitation was 92.3 ± 3.3 % (Figs. 2, 3). There
were no severe complications. None of the patients
developed mitral stenosis during the follow-up period.
Discussion
Pediatric MR is mainly induced by congenital heart dis-
ease, and is frequently associated with other congenital
cardiac abnormalities [15, 16]. The lesions are classified
into three groups according to the leaflet motion: normal,
prolapsed or restricted [5, 6]. MR involves systolic retro-
grade flow from the left ventricle into the left atrium. When
the regurgitant volume is small, patients may not have
symptoms. However, significant MR may increase the
volume of the left ventricle and left atrium, leading to high
pulmonary venous pressure or heart failure, so children
with significant MR, severe symptoms, pulmonary hyper-
tension or other cardiac anomalies should undergo early
surgical treatment [3, 8, 9]. In our cases, the postoperative
left atrial dimension and left ventricular end diastolic
volume were significantly reduced compared with the
preoperative values.
In consideration of the high mortality rate, anticoagu-
lation problems and high reoperation rate because of size
mismatch when performing mitral valve replacement,
mitral valve repair is considered to be the best surgical
treatment in the pediatric population [10, 11, 19]. In our
series, we customized our approach to mitral valve repair
according to the valve lesions, and the following valve
repair techniques were used based on the individual mitral
pathology: annuloplasty (85/107, 79.4 %), annuloplasty
ring (19/107, 17.8 %), cleft closure (13/107, 12.1 %),
reconstruction of the posterior leaflet (10/107, 9.3 %),
chordal shortening (12/107, 11.2 %) and papillary muscle
shortening (5/107, 4.7 %). Several techniques were some-
times used in a single patient. Annuloplasty was performed
in children with annular dilatation, leaflet cleft, leaflet
prolapse or restricted leaflet motion. Children with signif-
icant annular dilatation may need to be treated using an
annuloplasty ring. In our series, annular dilatation (type I)
was in 66 cases (61.7 %), so annuloplasty and an annulo-
plasty ring were used in most patients. We preferred to use
the interrupted prosthetic ring, because the subsequent
growth of the mitral annulus is inevitable in children, so
room for annular growth should be allowed.
The natural history of ventricular septal defect (VSD)
and MR has not been well studied. It is still controversial
whether MR should be treated at the same time as VSD
closure for patients with VSD and MR [18, 20]. If the MR
is significant and is the result of structural mitral valve
abnormalities, mitral valve repair should be considered at
the time of VSD closure. However, it is not clear whether
significant MR should be treated when the mitral valve
morphology is normal. Our experiences suggest that VSD
can cause the left ventricle and mitral annulus to dilate,
which can lead to MR. Therefore, the MR will resolve in
some patients after VSD closure alone, without mitral
valve repair. We concluded that the MR should be treated
if the regurgitation is moderate or severe in patients with
VSD, which might improve the surgical outcome, because
residual MR would affect the patients’ postoperative car-
diac function.
Intraoperative TEE is mandatory for mitral valve repair
[11, 21]. TEE can be used to evaluate the results of repair
and identify the residual MR. If the residual regurgitation is
moderate or severe, redo mitral valve repair or replacement
is necessary [8]. In our series, intraoperative TEE detected
Fig. 2 The freedom from moderate or severe regurgitation after
MVP
Fig. 3 A comparison of mitral regurgitation: preoperative vs. follow-
up
Surg Today
123

one patient with residual moderate MR after mitral valve
repair. This case had severe MR with an anterior leaflet
cleft preoperatively. We sutured the anterior leaflet cleft
directly, and the repair result was found to be satisfactory
by injecting saline through the valve orifice into the ven-
tricular cavity. However, intraoperative TEE showed
residual moderate MR, resulting in an immediate redo
repair with posterior annuloplasty, and the subsequent
regurgitation was trivial.
In the present study, MVP could be performed with an
acceptable early or late mortality rate, and a low reoperation
rate has previously been reported in adults [1, 11, 22].
However, MVP remains a surgical challenge in pediatric
patients [5, 6]. The early and mid-term results were encour-
aging at our institute, and these were comparable to or better
than those reported in the literature [15, 16, 23, 24]. This is
partly because of the different patient populations. The pre-
vious papers described both mitral stenosis and MR in their
patients, whereas our patients only had MR. In our cases, the
in-hospital mortality rate was only 0.9 % (1/107). During the
follow-up of our series (range from 3 to 80 months), only one
patient died of heart failure at 10 months postoperatively.
Follow-up echocardiography showed that moderate MR was
present in five patients, and one patient had severe regurgi-
tation. The patient with residual severe regurgitation was a
5-year-old female with severe regurgitation preoperatively,
and an annuloplasty ring was used to constrict the posterior
annulus. Follow-up echocardiography showed severe regur-
gitation 10 months postoperatively, and mitral valve
replacement was performed 1 year after surgery for this
patient. Poor quality of the leaflet and leaflet curl were the
main reasons for the residual severe regurgitation in this
patient. The other five patients with residual moderate
regurgitation were given pharmacological therapy, because
they were too young and their symptoms were alleviated
compared with the preoperative state. The freedom from
moderate or severe mitral regurgitation rate was 92.3 ±
3.3 % at 5 years. Therefore, the early and mid-term results are
satisfactory in our institute.
Conclusion
Pediatric patients with moderate or severe MR need
early surgical treatment. At present, MVP is the objec-
tive in children with significant MR, and the concomi-
tant cardiac anomalies should be treated at the same
time. Individualized treatment based on the specific
pathology is the key to successful surgical therapy for
pediatric MR.
Conflict of interest The authors have no potential conflicts of
interest to declare.
References
1. Cohn LH. Mitral valve repair. Mastery of cardiothoracic surgery.
2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins Inc;
2007. p. 341–52.
2. Rochae Silva A, Herdy GV, Vieira AA, Simoes LC. Surgical
mitral valve repair in children with rheumatic fever. Arq Bras
Cardiol. 2009;92(6):400–4 (417–21, 433–8).
3. Pedrazzini GB, Faletra F, Vassalli G, Demertzis S, Moccetti T.
Mitral regurgitation. Swiss Med Wkly. 2010;140(3–4):36–43.
4. Brizard C. Mitral valve repair in children. Mastery of cardio-
thoracic surgery. 2nd ed. Philadelphia, PA: Lippincott Williams
& Wilkins Inc; 2007. p. 1008–16.
5. Carpentier A, Branchini B, Cour JC, Asfaou E, Villani M,
Deloche A, et al. Congenital malformations of the mitral valve in
children. Pathology and surgical treatment. J Thorac Cardiovasc
Surg. 1976;72:854–66.
6. Chauvaud S, Fuzellier JF, Houel R, Berrebi A, Mihaileanu S,
Carpentier A. Reconstructive surgery in congenital mitral valve
insufficiency (Carpentier’s techniques): long-term results. J Tho-
rac Cardiovasc Surg. 1998;115:84–92 (discussion 92–93).
7. Minich LL, Atz AM, Colan SD, Sleeper LA, Mital S, Jaggers J,
et al. Partial and transitional atrioventricular septal defect out-
comes. Ann Thorac Surg. 2010;89(2):530–6.
8. Wood AE, Healy DG, Nolke L, Duff D, Oslizlok P, Walsh K.
Mitral valve reconstruction in a pediatric population: late clinical
results and predictors of long-term outcome. J Thorac Cardiovasc
Surg. 2005;130(1):66–73.
9. Shuhaiber J, Anderson RJ. Meta-analysis of clinical outcomes
following surgical mitral valve repair or replacement. Eur J
Cardiothorac Surg. 2007;31:267–75.
10. Beierlein W, Becker V, Yates R, Tsang V, Elliott M, de Leval M,
et al. Long-term follow-up after mitral valve replacement in
childhood: poor event-free survival in the young child. Eur J
Cardiothorac Surg. 2007;31(5):860–5.
11. Tesler UF, Cerin G, Novelli E, Popa A, Diena M. Evolution of
surgical techniques for mitral valve repair. Tex Heart Inst J.
2009;36(5):438–40.
12. Curi–Curi P, Ramırez-Marroquın S, Cervantes-Salazar J, Soule
M, Erdmenger J, Calderon-Colmenero J. Surgical repair of con-
genital mitral valve malformations. Arch Cardiol Mex. 2010;80(2):
87–94.
13. Zias EA, Mavroudis C, Backer CL, Kohr LM, Gotteiner NL,
Rocchini AP. Surgical repair of the congenitally malformed mitral
valve in infants and children. Ann Thorac Surg. 1998;66(5):
1551–9.
14. Oppido G, Davies B, McMullan DM, Cochrane AD, Cheung
MM, d’Udekem Y, et al. Surgical treatment of congenital mitral
valve disease: midterm results of a repair-oriented policy. J Tho-
rac Cardiovasc Surg. 2008;135:1313–21.
15. Stellin G, Padalino MA, Vida VL, Boccuzzo G, Orru E, Biffanti
R, et al. Surgical repair of congenital mitral valve malformations
in infancy and childhood: a single-center 36-year experience.
J Thorac Cardiovasc Surg. 2010;140(6):1238–44.
16. Hetzer R, Delmo Walter EB, Hubler M, Alexi-Meskishvili V,
Weng Y, Nagdyman N, et al. Modified surgical techniques and
long-term outcome of mitral valve reconstruction in 111 children.
Ann Thorac Surg. 2008;86(2):604–13.
17. Sheikh KH, Bengtson JR, Rankin JS, de Bruijn NP, Kisslo J.
Intraoperative transesophageal Doppler color flow imaging used
to guide patient selection and operative treatment of ischemic
mitral regurgitation. Circulation. 1991;84:594–604.
18. Mahadin DR, Srivastava S, Parness IA, Nguyen K, Love BA,
Walsh R, et al. Outcomes of mitral regurgitation associated with
large ventricular septal defect and a normal mitral valve
Surg Today
123

apparatus: does intact atrial septum have an impact? Pediatr
Cardiol. 2011;32(8):1128–31.
19. Gunther T, Mazzitelli D, Schreiber C. Mitral valve replacement
in children under 6 years of age. Eur J Cardio Thorac Surg.
2000;17(4):426–30.
20. Hisatomi K, Isomura T, Sato T, Kosuga K, Ohishi K, Katoh H.
Mitral valve repair for mitral regurgitation with ventricular
septal defect in children. Ann Thorac Surg. 1996;62(6):
1773–7.
21. Berrebi A. Mitral valve repair: echocardiography is its best
friend. Rev Esp Cardiol. 2011;64(7):554–6.
22. Sakaguchi T, Nishi H, Miyagawa S, Yoshikawa Y, Fukushima S,
Yoshioka D, et al. One-knot technique: a simple modification of
the loop technique for mitral valve repair. Surg Today.
2013;43(6):705–7.
23. Aharon AS, Laks H, Drinkwater DC, Chugh R, Gates RN, Grant
PW, et al. Early and late results of mitral valve repair in children.
J Thorac Cardiovasc Surg. 1994;107:1262–71.
24. Delmo Walter EM, Hetzer R. Mitral valve repair in children.
Mitral Valve Repair, II. Darmstadt, Germany: Steinkopff; 2011.
p. 41–56.
Surg Today
123