The Distribution of Root Caries in Community-dwelling Elders in New England
9
Vol. 54, No. 1, Winter 1994 15 The Distribution of Root Caries in Community-dwelling Elders in New England Anil Joshi, BDS, MPH Assistant Professor Harvard School of Dental Medicine Chester W. Douglass, DMD, PhD Professor Harvard School of Dental Medicine Alan Jette, PhD Chief Research Scientist New England Research Institute and Lecturer in Applied Mathematics Harvard School of Public Health Boston, MA Henry Feldman, PhD Senior Research Scientist New England Research Institute Watertown, MA Abstract An in-home examination of a probability sample of elders aged 70 and older living in the six New England states was conducted to estimate the prevalence and extent of root caries. Oral examinations were conducted by the visual-tactile method using a portable lamp, ex- plorer, and a mouth mirror. Fifty-two percent of the study participants showed root caries experience and 22 per- cent had untreated root caries. In contrast to previous studies, this analysis showed that buccal root surfaces were no more likely than proximal surfaces to be affected by root caries. Logistic regression analysis showed that gingival recession and number of teeth were positively associated with rout caries, while better oral hygiene maintenance and regular dental visits were negatively associated with root caries lesions (all factors: Pc.05). The prevalence of root caries was found to increase with higher numbers of teeth except for a minority subgroup- i.e., those who retained 25 or more teeth. This study provides much-needed data on prevalence and extent of root caries in a probability sample of the oldest old in an entire region of the United States. Send correspondence and reprint requests to Dr. Joshi, Department of Dental Care Administration, Harvard School of Dental Medicine, 188 Longwood Avenue, Boston, MA 021 15. This work should be attributed to Department of Dental Care Administration at Harvard School of Dental Medicine, Boston, and New England Research Institute, Water- town, MA. This work was supported by NIA grant #ROl-AG07139. Manuscript received: 4/16/92; returned to authors for revision: 8/25/92; accepted for publication: 3/22/93. Key Words: root caries, elders, risk indicators, intraoral distribution. Root surface caries is a disease of clinical significance that-along with coronal caries, periodontal disease, xerostomia, and tooth loss-affects oral health of elders. Cementa1 lesions are more difficult to restore than enamel lesions (1,2), and root caries has been reported as one of the more difficult clinical problemsin geriatriccare (3). With advancing age, the prevalence of gingival reces- sion increases and root surfaces, which are less resistant to acid attack, are exposed to the cariogenic oral environ- ment. Moreover, many older individuals use medica- tions such as anticholinergic, antidepressants, and anti- hypertensives that can reduce the salivary production (4,5). The resulting hyposalivation has been shown to be associated with canes (6,7). These biological effects, com- bined with relative aging of the population and the ten- dency of older persons to retain natural teeth, exerts a compounded effect on the occurrenceof root cariesin the population (8). Several recent epidemiologc surveys have reported the prevalence and distribution of root caries (9-15). However, many of these surveys were conducted with samples of convenience,institutionalizedpopulations, or were limited to local communities, thus limiting the scope and generalizability of prevalence estimates ob- tained from these surveys. In addition, data on oral dis- J Public Health Dent 1994;54(1):15-23
-
Upload
anil-joshi -
Category
Documents
-
view
214 -
download
2
Transcript of The Distribution of Root Caries in Community-dwelling Elders in New England

Vol. 54, No. 1, Winter 1994 15
The Distribution of Root Caries in Community-dwelling Elders in New England
Anil Joshi, BDS, MPH Assistant Professor Harvard School of Dental Medicine
Chester W. Douglass, DMD, PhD Professor Harvard School of Dental Medicine
Alan Jette, PhD Chief Research Scientist New England Research Institute and Lecturer in Applied Mathematics Harvard School of Public Health Boston, MA
Henry Feldman, PhD Senior Research Scientist New England Research Institute Watertown, MA
Abstract
An in-home examination of a probability sample of elders aged 70 and older living in the six New England states was conducted to estimate the prevalence and extent of root caries. Oral examinations were conducted by the visual-tactile method using a portable lamp, ex- plorer, and a mouth mirror. Fifty-two percent of the study participants showed root caries experience and 22 per- cent had untreated root caries. In contrast to previous studies, this analysis showed that buccal root surfaces were no more likely than proximal surfaces to be affected by root caries. Logistic regression analysis showed that gingival recession and number of teeth were positively associated with rout caries, while better oral hygiene maintenance and regular dental visits were negatively associated with root caries lesions (all factors: Pc.05). The prevalence of root caries was found to increase with higher numbers of teeth except for a minority subgroup- i.e., those who retained 25 or more teeth. This study provides much-needed data on prevalence and extent of root caries in a probability sample of the oldest old in an entire region of the United States.
Send correspondence and reprint requests to Dr. Joshi, Department of Dental Care Administration, Harvard School of Dental Medicine, 188 Longwood Avenue, Boston, MA 021 15. This work should be attributed to Department of Dental Care Administration at Harvard School of Dental Medicine, Boston, and New England Research Institute, Water- town, MA. This work was supported by NIA grant #ROl-AG07139. Manuscript received: 4/16/92; returned to authors for revision: 8/25/92; accepted for publication: 3/22/93.
Key Words: root caries, elders, risk indicators, intraoral distribution.
Root surface caries is a disease of clinical significance that-along with coronal caries, periodontal disease, xerostomia, and tooth loss-affects oral health of elders. Cementa1 lesions are more difficult to restore than enamel lesions (1,2), and root caries has been reported as one of the more difficult clinical problemsin geriatric care (3). With advancing age, the prevalence of gingival reces- sion increases and root surfaces, which are less resistant to acid attack, are exposed to the cariogenic oral environ- ment. Moreover, many older individuals use medica- tions such as anticholinergic, antidepressants, and anti- hypertensives that can reduce the salivary production (4,5). The resulting hyposalivation has been shown to be associated with canes (6,7). These biological effects, com- bined with relative aging of the population and the ten- dency of older persons to retain natural teeth, exerts a compounded effect on the occurrence of root caries in the population (8).
Several recent epidemiologc surveys have reported the prevalence and distribution of root caries (9-15). However, many of these surveys were conducted with samples of convenience, institutionalized populations, or were limited to local communities, thus limiting the scope and generalizability of prevalence estimates ob- tained from these surveys. In addition, data on oral dis-
J Public Health Dent 1994;54(1):15-23

16 Journal of Public Health Dentistry
eases including root caries are sparse on elders aged 70 and older and especially for the oldest old (aged 85+ years), the fastest growing subgroup of the population in the United States (16). As older subgroups increasingly become part of clinical practice, it is important that dis- ease levels in these populations be estimated and the need for care identified. Equally important is the delin- eation of risk factors that characterize the distribution of disease in these groups.
The purpose of this paper is to describe the prevalence, extent, and intraoral distribution of root caries in a prob- ability sample of community-dwelling elders aged 70 and older. Sociodemographic and clinical factors associ- ated with root caries also are presented with special reference on the relationship of root canes with the num- ber of teeth.
Methods The New England Elder Dental Study (NEEDS) was
conducted in 1988-91 in a geographically stratified ran- dom sample of community- dwelling elders aged 70 and older living within the six New England states (17). The sampling frame for this study consisted of the Medicare Beneficiary List prepared by the Health Care Financing Administration (HCFA). The HCFA estimates that the beneficiary lists achieve an excellent sampling frame with 97 percent coverage of the population 65 years of age and older.
The sampling strategy used a two-stage, stratified, cluster sampling design. The first stage sampled cities and towns in New England stratified by population size into four categories: large metropolitan, urban, subur- ban, and rural. Within these strata, cities and towns were sampled with replacement and with sample size propor- tional to the size of the 65+ populations within that city or town. A total of 68 communities were selected: one large metropolitan (Boston), four urban, 13 suburban, and 50 rural. In the second stage of the sampling design, for each of these 68 sampled towns a 10 percent random sample of beneficiaries 70 years or older was obtained from HCFA, with a final sample of 3,668 individuals. The combined probability of selection was the same for all participants. Thus, it is a self-weighted sample.
Each of these 3,668 individuals was screened for study eligibility using several criteria (alive, 270 years of age, noninstitutionalized, free of specific conditions such as myocardial infarction within last six months, and -cur- rently residing in a sampled city or town). From this screening 2,598 individuals were determined eligible for the study. Approximately 35 percent of subjects excluded in the screening were institutionalized or had medical conditions; some others were excluded because of their inability to communicate in English or to provide a proxy person for the interview. The rest of the excluded subpcts had either died, moved, or the HCFA database had out- of-date information making it difficult to locate these
individuals. In stage I of this study, 2,057 (79.2% of eligibles) partic-
ipated in the telephone interview that provided informa- tion such as sociodemographics and oral hygiene main- tenance behavior. Stage 11 included an in-home dental examination and a personal interview. Stage I1 was com- pleted by 1,151 participants-i.e., 56percentof those who completed stage I and 45 percent of those determined eligible for the study.
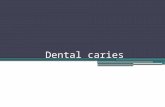
The personal interview gathered data on life-style be- havior such as tobacco and alcohol use, daily activities, dental insurance, and medication use. Detailed descrip- tions of the two-stage, stratified sampling strategy em- ployed in this study, and telephone and personal inter- view data collection methods are have been reported by Douglass et al. (17). Age and gender distribution of NEEDS participants who participated in stage I (tele- phone interview), those who participated both in stage I and stage 11, and the New England Medicarebeneficiaries are presented in Figure 1. These data suggest that al- though only 45 percent of those eligible for the study participated in the in-home dental examination, the age and gender distributions were similar to those of the New England elders population. Moreover, Table 1 shows a comparison of sociodemographic and dental characteris- tics between the dentate in-home respondents (our an- alysis is based upon their data) and nonrespondents. Except for an 11 percent difference in gender distribution, these respondents are similar to the nonrespondents (to in-home examinations) on variables of interest, thus pro- viding confidence in the generalizability of our findings to the 70+ dentate elderly population (target population) in New England.
Of the 1,151 study participants, root caries examina- tions were conducted on the 729 subjects who had one or
FIGURE 1 Age-Sex Distribution of Sample Compared to Sampling
Frame (All New England Elderly Persons)
Percent 25
rb
15
10
5
n " 70-74 75-79 80-84 85+ 70-74 75-79 80-84 85+
Male Female
N.E Medicare Pop. MTelephone Resp. HTeiephone+Exam Resp.
Age Group
(1,202,533) (2057) (1151)

Vol. 54, No. 1, Winter 1994 17
more natural teeth. These oral examinations were con- ducted in the participants’ homes by the visual-tactile method using a portable light lamp, explorer, and a mouth mirror (11). Root caries was measured only on those surfaces with at least 1 mm of gingival recession. When a tooth surface was determined to have gingival recession, it was classified into one of the following cate- gories: (1) sound; (2) initial decay; (3) recurrent decay; or (4) restored, the restoration being confined to a root surface. In addition, restorations that crossed the cementoenamel junction were classified into six catego- ries; the following three categories were included in root caries measurement: (1) restoration mostly on crown of the tooth, but secondary decay on root classified as recur- rent decay; (2) restoration mostly on root of the tooth and secondary decay on root classified as recurrent decay; and (3) restoration mostly on root and sound classified as a restoration. This classification was developed to avoid counting a restoration as root caries, when in fact the restoration was judged to be primarily placed because of enamel caries. Also, no attempt was made to distinguish filled root lesions from filled abrasion. Third molars were included and no radiographs were used in the examina- tion. Data were collected by trained interviewer-recorder on a laptop computer (19).
Four dentist examiners were involved throughout the
TABLE 1 Comparison of Respondents with Nonrespondents to
Dental Examination (Except for the dentate status category, all comparisons are between dentate subjects)
Respondents Nonrespondents Variables (n=718) (n=906)
Dentate status n dentate n edentulous n total
Gender (%) Female Male
Age groups (%) 70-74 75-79 8044 85
School years (212) (%) Visited dentist within
Brushing frequency
Number of teeth
1 year (%)
=/day (%)
mean (SD)
718 (62%) 433 (38%)
1,151 (100%)
57 43
39 31 19 11 70 74
65
16.9, (8.0)
507 (56%) 399 (44%) 906 (100%)
68 32
37 30 21 12 62 69
68
16.5-t (8.6)
‘Based on the dental examination. tBased on self-reports.
study. Initial standardization and calibration sessions were: held by the principal investigator (CWD), who was previously trained in the examination methods by NIDR. After the study began, recalibration sessions were held approximately every four months to maintain inter- examiner consistency. Level of interexaminer reliability actually achieved in the study under field conditions was then evaluated by conducting a reexamination of a ran- domly selected quadrant in 5 percent of subjects. Subjects for this quality assurance study were randomly selected from a pool of subjects with 12 or more teeth who lived in a specified geographic area. The primary examiner was blinded as to the subject’s eligibility for a reexamina- tion.
Kappa statistic (18, which provides the agreement between examiners (controlling for agreement by chance), on root examination was 0.84 at the beginning of the study and 0.73 at the quality assurance study (Table 2).
Statistical Analysis. All analyses in this report are restricted to the 718 subjects (63% of the sample) who had one or more natural teeth. Eleven subjects had root tips only and were excluded. Student’s T-test, ANOVA, and x2 tests were used to assess the statistically significant differences between groups as appropriate.
Logistic regression models were used to determine the relationship between root caries and several demo- graphic and clinical variables. The logistic regression analyses modeled the relationship between a binary re- sponse variable and multiple categorical and continuous predictor variables. Such analysis provides estimates of the effect of each predictor variable on the response variable while statistically adjusting for other variables in the model (20). From these analyses, odds ratios were computed that reflect the strength of associationbetween the response variable and each predictor variable. In our regression analysis, both main effects and interaction effects of pertinent variables were modeled. Interactions were modeled among (1) age and gingival recession; (2) number of teeth and gingival recession; (3) age and teeth; and (4) number of teeth and a binary variable “healthy survivor,” which classified subjects by a threshold value of number of teeth (Table 3). Except for category (4), none
TABLE 2 Root Caries Reliability: Surface Level Agreement Under
Field Conditions
Exam- % Agree- iner Subjects Teeth Calls ment Kappa
1 vs 2 22 1 78 690 89.3 0.83 1 vs 3 23 184 726 75.0 0.63 1 vs 4 7 56 224 86.6 0.80 Overall 52 416 1,640 82.5 0.73

18 Journal of Public Health Dentistry
TABLE 3 List of Variables Included in Regression Analysis
Outcome Variables Root caries experience
0: no decayed or filled surface I: 21 decayed or filled surface
0: no decayed surface 1: 21 decayed surface
Exvlanatoru Variables
Root decay
Age
Age group Age of the subject in years
70-74,7579,8044,285 Gender
Geographic region
Education
Income
Number of teeth
Gingival recession
Brushing frequency
Male, female
Rural, suburban, urban, metropolitan
4 2 years, 212 years
<$15,000,2$15,000
1-32
Percent of sites with gingival recession
0: <2 1: 22
0: <2 I: 22
0: <2 1: 22
0: subjects with 4 2 teeth 1: subjects with 222 teeth
0: did not visit dentist in past year 1: visited dentist in past year
Number of teeth * gingival recession Interaction term
Age number of teeth Interaction term
Number of teeth gingival recession Interaction term
Number of teeth *healthy survivors Interaction term
Age gingival recession Interaction term
flossing frequency
Brush and floss frequency per day
Healthy survivors
Dental utilization
of the interaction terms were found to be significant; therefore, only those main effects significantly associated with root canes are presented in this paper. Model build- ing relied upon inclusion of variables with biologic plau- sibility and statistical association with the outcome vari- able. In the initial stages of model building, variables were included showing a significance level of 0.15 or less.
TABLE 4 Mean Number of Teeth by Age and Gender k 7 1 8 )
Female Male
AgeGroup n Mean (SD) n Mean (SD)
7&74 1 45 17.8 (7.8) 134 18.1 (7.9) 7579 1 23 17.3 (8.4) 102 17.5 (8.0) 8 M 4 82 16.0 (7.4) 52 15.7(7.7) 85+ 57 15.2(8.3) 23 14.8(8.9) All 407 17.1 (8.0) 31 1 17.3 (8.0)
TABLE 5 Number and Percent of Respondents with Root Decay and Root Caries Experience by Number of Affected Surfaces
( n = 7 18 )
Number Surfaces
Affected
0 1 2 23
Root Decay (21 DS)
Root Caries Experience (21 DFS)
# %
558 77.7 67 9.3 37 5.2 56 7.8
- # %
342 47.6 105 14.6 112 15.6 159 22.1
TABLE 6 Percent of Respondents with Root Decay and Root Caries
Experience, by Age and Gender
Age Group
70-74 75-79 -4 85+
Root Caries Experience Root Decay (21 DFS) (21 DS)
Males Females Males Females
47 (3&54)* 46 (37-53) 22 (15-29) 19 (13-25) 66 (55-73) 45t (36-53) 23 (15-31) 13 (7-19) 58 (43-69) 66 (54-74) 35 (2247) 27 (1&37) 50 (30-67) 49 (36-60) 44 (24A2)t 23 (13-34)
*95% confidence limits. tChi-square test, Pc.05.
However, the final model was based upon only those variables significant at the 0.05 level.
The total number of statistical tests reported here is 24. The expected number of Type 1 errors, assuming all true effects were independent and null, is therefore 24 * 0.05 = 1.2.
Results Root Caries Prevalence. The age and gender distibu-
tion of the dentate sample (n=718) is presented in Table

Vol. 54, No. 1, Winter 1994 19
TABLE 7 Mean Decayed and Filled Surfaces by Age Group, Gender,
and Root Caries Experience
Subjects w/ Root Caries Exp. (n=376)
All Dentate Subjects (n=718)
AgeGroup Male Female
70-74 5.0 (5.2)* 3.3 (2.7)t 7579 4.2 (5.21 4.4 (5.1) 80-84 4.0 (3.3) 3.6 (3.0) 85+ 2.6 (1.6) 3.8 (3.2) All 4.4 (4.8) 3.8 (3.7)
Male Female
2.4 (4.4) 1.5 (2.5)t 2.7 (4.6) 2.0 (4.0) 2.3 (3.2) 2.4 (3.0) 1.3 (1.7) 1.9 (2.9) 2.4 (4.1) 1.9 (3.2)$
‘Numbers in parentheses and standard deviations of the means. tT-test, P=.O4. ST-test, P=.058.
TABLE 8 Extent of Root Canes in Individuals with Root Canes
Experience by Age Group (n=376) ~
Age Mean Group DFS
70-74 4.15 7579 4.29 80-84 3.76 85+ 3.42 All 4.03
~~
D/DFS* RD/TDt SD (%) (%)
4.2 35 5.7 5.1 33 4.9 3.1 32 8.3 2.9 44 6.6 4.2 34 6.4
*Ratio of number of decayed surfaces to number of decayed and filled surfaces. tRatio of recurrent decay to initial and recurrent decay.
TABLE 9 Gingival Recession and Root Canes by Type of Tooth Surface in Subjects with Root Caries (n=376)
Sites with Gingival Recession (EXP) Number of Affected Surfaces (D+F)/EXP
Surface # % D DF D/EXP Ratio* Ratiot
Mesial 2,190 33.4 116 199 .05 .09 Distal 2,590 39.5 146 263 .05 .10 Buccal 4,016 61.4 173 876 .04 .21 Lingual 2,644 40.4 86 177 .03 .06 All 11,440 43.6 521 1,515 .04 .13
*Two-way ANOVA; F<.001, lingual surface less than other surfaces. tTwo-way ANOVA; F<.OOl, buccal surface greater than other surfaces.
4. Fifty-six percent of the sample was female and, as expected, the proportion of females increased in higher age groups. In males the mean number of teeth decreased from 18.1 in the 70-74-year-old age group to 14.8 in the 85+ age group. The corresponding mean number of teeth in females was similar at 17.8 and 15.2. There were no age-specific or gender differences in the mean number of teeth.
Table 5 shows the proportion of subjects with (1) root decay, defined as having at least one unrestored decayed root surface; and (2) root caries experience, defined as having at least one decayed or restored surface. Twenty- two percent of the sample (95% confidence interval: 19.3- 25.4) had at least one unrestored decayed surface. Fifty- two percent (95% confidence interval: 48.8-55.9) of the sample had root caries experience, with 22.1 percent having more than three decayed and filled surfaces. Age- and gender-specific prevalence rates for untreated root decay and root caries experience are shown in Table 6. Males had more root canes experience in the 75-79 age group and more root decay in the 85+ age group (Pc.05).
Table 7 shows the extent of root caries in male and female subjects who had root caries experience. The data
are presented for subjects with root cries experience (n=376) and also for all dentate subjects (n=718). The only significant difference in mean number of decayed and filled surfaces in males and females was for the 70-74 age group (males had higher mean DFS than females) in the group with root caries experience. When data from all dentate subjects were analyzed, males had a significantly higher number of DFS than females in the 70-74 age group (T-test, P=.O4) and the 85+ age group (T-test, P=.058).
Table 8 shows the combined data for males and fe- males along with the ratio of D to DFS and recurrent caries as a percent of initial and recurrent root decay. The mean number of decayed and filled surfaces decreased only slightly with increasing age, from 4.15 in the 70-74 age group to 3.42 in the 85+ age group. Overall, the mean number of decayed and filled teeth was 3.02 (data not shown); on average, 34 percent of all involved surfaces were unrestored. Six percent of carious lesions were sec- ondary decay that had developed on the margins of prior restorations. The secondary decay varied from 4.9 per- cent to 8.3 percent across the four age groups.
Intraoral Distribution. Table 9 presents data on gingi-

20 Journal of Public Health Dentistry
TABLE 10 Logistic Regression Analysis: Pertinent Statistics on Variables Associated with Root Canes
Response Predictor Regression Coefficient 95% CI of
Root caries Age group (80-84) 0.53 0.21 .01 1.69 1.12-2.46
Variable Variable B SE P-value Odds Ratio Odds Ratio
1.09-1.18 experience* Number of teeth 0.13 0.02 .001 1.13 (model I) Number of teeth -0.12 0.04 .01 0.88 0.824.95 0: no healthy survivors
Root decayt Age group (75-79) -0.77 0.26 .004 0.42 0.28-0.81 (model 11) Gingival recession 0.016 0.005 .002 1.37 1.13-1.67 0: absent Last dental visit 0.71 0.28 .01 2.03 1.173.49
1: yes Gingival recession 0.03 0.003 .0001 1.82$ 1.63-2.03
1 : present Deficient oral hygiene 0.88 0.42 .03 2.41 1.06-5.47
*At least one decayed or filled root surface. tAt least one decayed surfaces. *Per 20% increase in gingival recession.
Val recession and root canes by type of tooth surface. In subjects who had root caries, 44 percent of root surfaces had gingival recession. Gingival recession was most prevalent on the buccal surface (61.4%) and least on the mesial surface (33.4%). Moreover, the buccal surface had the highest number of unrestored and restored root caries lesions. A two-way analysis of variance with ratios of number of decayed surfaces to exposed surfaces (D/EXP) as the dependent variable and subjects (376 levels) and surfaces (four levels) as factors showed that only the lingual surface had a significantly lower number of lesions per 100 exposed surfaces than other surfaces. The D/EXP ratio for buccal surfaces was no different than mesial or distal surfaces. In contrast, a similar an- alysis with ratio of decayed and filled surfaces to number of exposed surfaces [(D+F)/EXP: root caries index] as the dependent variable showed that buccal surfaces had sig- nificantly higher numbers of decayed and filled surfaces per 100 exposed surfaces. The Katz’s root caries index for the buccal surface was twice as high as for proximal surfaces, and three and a half times as high as lingual surfaces.
Risk Indicators. To assess the nature of differences between subjects with and without root caries, the first regression model (model I) used presence or absence of root caries experience as a response variable. Five socio- demographic factors (age, gender, education, income, and geographic region) were used as predictor variables. Clinical factors included in this model were number of teeth; percent of sites with gingival recession; frequency of brushing and flossing per day; and dental utilization, defined as having an office visit in the past one year (Table 3). Results showed that age, number of teeth, and percent of sites with gingival recession were the only significant factors in predicting the presence or absence of total root caries experience.
The odds ratio and 95 percent confidence interval of the odds ratio are presented in Table 10. For example, the 80-84-year-old age group had 1.7 times the odds of hav- ing root caries experience than the reference 70-74-year- old age group. None of the other age categories were significantly different from the reference group. Simi- larly, with an increase of one tooth the odds of having root caries experience increased by 13 percent; having three additional teeth increased the odds by 47 percent (data not shown in the table). Gingival recession was the strongest predictor of root caries experience. With each 20 percent increase in gingival recession, the odds of having root caries experience increased by 80 percent. The precision of this measure is reflected in the95 percent confidence interval with boundaries of 1.63 and 2.03. In addition to these main effects the interaction term “num- ber of teeth * healthy survivors” was significant. This finding suggests that the prevalence of root caries expe- rience increased as the number of teeth increased for those who had up to 21 teeth. However, the relationship between number of teeth and prevalence of root caries experience decreased for those who had 22 or more teeth.
A second regression model (model 11) was created using presence or absence of root decay as the response variable and the same demographic and clinical predic- tor variables used in model I (Table 10). This analysis suggested that age, increased gingival recession, poor oral hygiene practice (defined as brushing and flossing less than twice a day), and failure to visit a dentist in the past year increased the odds of having root decay.
Discussion Root Caries Prevalence. Cross-sectional studies are
important in estimating the prevalence of a disease in the population and for identifying the subgroups who need care (21). The strength of these studies springs from two

Vol. 54, No. 1, Winter 1994
important factors: the representativeness and the size of the sample. These two parameters provide confidence in the generalizability of the findings and precision of the estimated parameters. The root canes findings reported in this paper document much-needed data regarding prevalence and extent of root caries in the older adult population. Despite the predominantly white (94%) Sam- ple, it is the largest and the first study of a community- based probability sample covering one complete region (New England) of the United States.
The definition of root caries prevalence defies the tra- ditional definition of disease prevalence for three rea- sons. First, unlike other diseases such as lung cancer or diabetes, there are multiple lesions occurring on different teeth and surfaces; thus, it is difficult to discuss the prev- alence of root canes without considering the number of lesions in each individual. Second, a restored root surface is considered indicative of past disease. However, it is not always clear if those individuals with restored root sur- faces, but with no current disease, should be considered in the prevalence calculations. Third, restored root sur- faces may be the result of cervical abrasion and thus may not be indicative of even past root canes. These points should be considered when interpreting root canes data.
In this sample, 22.1 percent of dentate subjects showed at least one root caries lesion, indicating that about one- fourth of the 70+ population has the disease and needs treatment. These prevalence rates are similar to those found in the Iowa study (10) (25.3% in the 65+ popula- tion), in the North Carolina study (22) (24% in the 65+ population), and in the Finland study (23) (24% in the 30+ population). However, the rate is lower than reported for a group of older Canadians (13) (37.2% in 65+ popula- tion). The NIDR survey of seniors (11) visiting multipur- pose senior centers did not report the percent of popula- tion with at least one decayed surface. However, in the NIDR study 66 percent of the 70+ population of Region 1 had one or more decayed or filled surfaces, compared with 52.4 percent of subjects in the present study. As indicated by Beck (24), prevalence rates across studies may differ due either to actual differences in populations or to design differences. Conversely, similar rates found in populations with different age and gender composi- tions should be viewed with some caution. Important design differences among reported surveys include dif- ferences in sampling frames such as communitydwell- ing residents or institutionalized subjects, sampling methods such as representative or volunteer popula- tions, and measurement criteria for root canes.
If all restored surfaces are assumed to be due to past decay, then the mean number of decayed and filled sur- faces per person provides the extent of disease in the population. Unlike findings from the NIDR (11) study, we emphasized presentation of data that describe the mean DFS for individuals who had root canes experi- ence. Inclusion of subjects who show no signs of root
21
caries, present or past, in the denominator for calculating mean DFS may be misleading as it decreases the mean DFS and does not provide the extent of disease in indi- viduals who have the disease. Moreover, unlike coronal caries, the implicit assumption that by age 65 almost everyone has caries experience is not valid for root caries. However, the extent data for all 718 dentate subjects also are presented for comparison purposes. The D/DFSratio in this study followed the same pattern as in the NIDR study, but was lower for each of the corresponding age groups. In both studies, the oldest age group (85+ for NEEDS and 80+ for NIDR) had the largest untreated decay. This finding may reflect inaccessibility of care or an attitude of "dental fatalism" at an older age, as re- flected in the statement: "The tooth will be lost anyway; why have it treated?"
The rate of recurrent root canes among older adults was low in this Sample with only 6 percent of the subjects affected. Beck et al. (10) reported that 4 percent of subjects in the rural Iowa study had recurrent root caries. There are several possible explanation for this finding. First, the consistently low levels of recurrent root canes (5%-8%) across age groups may suggest that root canes is treated successfully. What was once thought to be a difficult part of geriatric dental care may not hold true. Availability of new materials and techniques might contribute to more successful restorations. Second, as suggested by Beck et al. (lo), in comparison to coronal caries, most root canes lesions are recently treated and are not present in the mouth long enough to show recurrent canes. Finally, when recurrent canes occurs, the individual and dentist might be more inclined to extract the tooth rather than to re-restore it. This behavior may be especially true in subjects with compromised natural dentitionsand where the treatment plan requires construction of dental pros- theses.
Intraoral Distribution. A comparative evaluation of two ratios, D/EXP and (D+F)/EXP, for different root surfaces (Table 9) reveals an interesting finding. Similar to the findings of Wallace et a1.(12) and Katz et al. (9), the root canes index was highest for the buccal surface. In contrast, the buccal surface did not have the highest rate of root decay. It is fair to assume that at a point in time, the distribution of root canes lesionson the four different root surfaces is reflective of the affliction of this disease for different surfaces. Therefore, D/EXP rather than (D+F)/EXP would be a more appropriate index for de- scribing the intraoral distribution of root canes. The filled component for buccal surfaces tends to be higher because of restoration due to abrasion. Also, decayed buccal sur- faces are more likely to be filled due to visibility and access. Finally, the "treatment effect" is introduced when filled surfaces are included in describing the intraoral distribution of this disease. Therefore, incrimination of this surface as the most likely to be affected by root canes may not be valid. Higher rates of decay per 100 exposed

22 Journal of Public Health Dentistry
mesial and distal surfaces obtained in this study suggest difficulty in maintaining hygiene at these sites, leading to increased bacterial colonization and production of de- mineralizing acid.
Risk Indicators. In none of the regression models pre- sented in this paper were gender, education, income, or geographic stratum significantly associated with root canes. This finding suggests that the role of these socio- demographic variables is not as important in predicting root caries as other factors such as gingival recession, number of teeth, age, dental utilization, and oral hygiene maintenance. Similarly, Locker et al. (13) used logistic regression analysis and stepwise multiple regression analysis and found no association between demographic variables such as gender and education and root caries. In contrast, Beck et al. (25), in a bivariate analysis of root decay and income controlling for race, found a higher prevalence of root decay in individuals with less than $15,000 per year income.
In this study, root canes was measured only on sur- faces that had gingival recession of at least 1 mm. Given this necessary but not sufficient condition, gingival reces- sion was much more prevalent in subjects who had root caries experience or who had untreated lesions. Associa- tion of oral hygiene with root decay in this study further emphasizes the importance of brushing and flossing in prevention of root caries. Perhaps in addition to the mechanical removal of plaque by brushing, the exposure to fluoride content in toothpaste is equally important in preventing root decay. Association of root caries with brushing and flossing frequency also has been reported by Kitamura et al. (6) in a nursing home population, and by Joshi et al. (26) in a study of root caries incidence in Boston metropolitan residents. Moreover, the fact that the odds of having root decay were twice as high in subjects who did not visit their dentists in the past 12 months underlines the importance of regular dental vis- its by these dentate elders. Thus, clinicians, insurance plans, and dental public health practitioners should con- tinue to advocate the importance of regular dental visits to their elderly patients.
The relationship of number of teeth and root canes as measured by DFS is complicated by the fact that with loss of a tooth, the number of decayed and filled surfaces on that tooth are lost also. In other words, if one loses teeth, the DFS index will not necessarily increase even when more carious lesions occur. Root caries is a predictor of tooth loss (27). Moreover, personal dental attitudes are considered an important factor in the decision for tooth extraction (27,28). In this study, the number of teeth were fewer in individuals who had root decay. The group with only root canes lesions (D only) had significantly fewer teeth (mean=12.0) in comparison with the group with no root decay (mean=19.0). Fromlogistic regressionanalysis (model II), it is also clear that subjects with root decay tend to have poor oral hygiene and less frequent dental
utilization. This finding could be due to attitude or will- ingness of this group to have a tooth extracted when decay occurs. Furthermore, the data from this study show that the probability of havingroot canesexperience (DF) increased as the number of teeth increased; that is, root caries as measured by DFS will tend to increase with higher numbers of teeth, provided the teeth are not ex- tracted when the disease occurs, thereby destroying the evidence of past disease. Thus, as the elderly population with natural teeth increases, root caries will continue to be a significant problem unless preventive strategies are pursued by private clinics, public health programs, and oral pharmaceutical industry.
Further analysis showed, however, a threshold effect in the relationship of number of teeth and root canes experience. The prevalence of root canes increased with increasing numbers of teeth until a threshold of 21 teeth was reached, suggesting that certain subgroups in the population maintain good oral health even in old age. For example, subjects in this study with 25 or more teeth (21.9% of dentate sample) had less disease than those with 13 to 24 teeth. This finding is similar to that of Locker et al. (13), who reported that "older adults with good oral health had low rates of root decay." In summary, al- though from our cross-sectional data we cannot conclude that as more teeth are retained, more root caries will develop on these teeth, it is clear that except for a minority subgroup who retained 25 or more teeth at the age of 70, the prevalence of root canes did increase with higher numbers of teeth.
References 1. Billings RJ, Brown LR, Kaster AG. Clinical and microbiological
evaluation of contemporary treatment strategies for root surface dental canes. Gerodontics 1985;1:20-7.
2. Seichter U. Root surface caries: a critical literature review. J Am Dent Assoc 1987;115:30510.
3. Farrell DJ. Prosthodonic problems of the patient. Dent Surv
4. Ettinger RL. Xerostomia: a complication of aging. Aust Dent J
5. Handelman SL, Baric JM, Espeland MA, Berglund KL. Prevalence of drugs causing hyposalivation in an institutionalized geriatric population. OralSurg Oral Med Oral Pathol1986;62:2&31.
6. Kitamura M, Kiyak HA, Mulligan K. Predictors of root canes in the elderly. Community Dent Oral Epidemiol1986;1434-8.
7. Slome BA. Rampant canes: a side effect of tricyclic antidepressant therapy. Gen Dent 198482:4946.
8. Stamm JW, Banting DW, Imery PB. Adult root canes survey of two similar communities with contrasting natural water fluoride levels. J Am Dent Assoc 1990;120143-9.
9. Katz RV, Hazen SP, Chilton NW, Mumma RD, Jr. Prevalence and intraoral distribution of root caries in an adult population. Caries Res 1982;16:26.5-71.
10. Beck JD, Hunt RJ, Hand JS, Field HM. Prevalence of root and coronal caries in a noninstitutionalized older population. J AM Dent Assoc 1985;111:964-68.
11. National Institute of Dental Research. Oral health of United States adults. National findings. Washington, D C US Department of Health and Human Services, 1987; NIH pub no 87-2868.
12. Wallace MC, Retief DH, Bradley EL. Prevalence of root canes in a population of older adults. Gerodontics 1988;484-9.
13. Locker D, Slade GD, Leake JL. Prevalence of and factors assodated with root decay in older adults in Canada. J Dent Res 1989;63:768-72.
14. Banting DW, Ellen RP, Fillery ED. Prevalence of root canes among
1971 ;47:21-3.
1981 ;26365-71.

Vol. 54, No. 1, Winter 1994 23
institutionalized older persons. Community Dent Oral Epidemiol 1980;8:84-8.
15. Papas A, Joshi A, Juinta J. Prevalence and intraoral dwtribution of coronal and root caries in middle-aged and older adults. Caries Res
16. US Bureau of the Census. Projections of the populations of the United States by age, sex, and race: 1988 to 2080. Current Pop Rep Jan 1989; series P-25; no 1018.
17. Douglass CW, Jette A, Tennstedt S, et al. Oral health status of the elderly in New England. J Gerontol Med Sci 1993;48:M3946.
18. Cohen J. A coefficient of agreement for nominal scales. J Educ Psycho1 Measures 1960;20:37-46.
19. Joshi A, McDermott S, Marcus, P, Douglass C W , Jette A. Improving epidemiologic data collection with computers. J Public Health Dent
20. Hosmer DW, Lemeshow S. Interpretation of the coefficients of the logistic regression model. In: Applied logistic regression. New York John Wiley & Sons, 1989.
1992;26459-65.
1992;52(4):232-8.
21. Kleinbaum DG, Kupper LL, Morgenstem H. Types of epidemiolog- ical research. In: Epidemiological research: prinaples and quanti- tative methods. New York Van Nostrand Reinhold, 1982.
22. Graves R, Disney J, Beck J, et al. Factors in root caries experience in NC adults aged 65+ [Abstract]. J Dent Res 1989;68184.
23. Vehkalahti MM. Relationship between root caries and coronal decay. J Dent Res 1987;66:160810.
24. Beck J. The epidemiology of root surface caries. J Dent Res 1989;69: 121&21.
25. Beck JD, Kohout F, Hunt RJ. Identification of high cariesrisk adults: attitudes, soda1 factors and disease. Int Dent J 198838:231-8.
26. Joshi A, Papas A. Root caries incidence and associated risk factors in middle-age and older adults. Gerodontology (in press).
27. Hunt RJ, Hand JS, Kohout FJ. Five-year incidence of tooth loss in Iowans aged 65 and older. Community Dent Oral Epidemiol
28. Burt BA. The oral health of older Americans (editorial). Am J Public 1991 ;1948-51.
Health 1985;75:11334.
CALL FOR NOMINATIONS
THE NORTON M. ROSS AWARD FOR EXCELLENCE IN CLINICAL RESEARCH
OBJECTWE To recognize individuals who have made significant contributions in clinical investigations that have advanced the diagnosis, treatment, and/or prevention of craniofacial-oral-dental diseases, as well as individuals with outstand- ing research accomplishments in areas such as human behavior, health care delivery, and material sciences.
CRITERIA Selection will be based on the scope of the nominee’s research, with special emphasis on its impact on clinical dentistry; and publications in refereed journals. The successful nominee will be a member of the American Dental Association, if eligible.
AWARD AND RECOGNITION The awardee will receive a $5000 cash prize and a plaque. The award, presented annually at a dinner for the Board of Trustees on a date preceding the Annual Session, will be made in October 1994 in New Orleans.
SPONSORSHIP The award is funded by the Warner-Lambert Company and administered by the American Dental Association in memory of Dr. Norton M. Ross. Dr. Ross, a dentist and pharmacologist, contributed significantly to the fields of oral medicine and dental clinical research.
NOMINATION PROCEDURE Letters of nomination describing the nominee’s accomplishments in the context of the objectives of this award and a cumculum vitae with a list of publications should be submitted. The letter(s) should be explicit in describing the impact of the nominee’s research on clinical dentistry.
DEADLINE Nominations must be received at ADA headquarters by May 1,1994. Please address nominations to Joan M. Reiser, Staff Coordinator, The Norton M. Ross Award, American Dental Association, 211 East Chicago Avenue, Chicago: IL 60611; (312) 440-2549.