Region Västra Götaland, HTA-centrum Metacarpophalangeal and ...

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
1 | P a g e
Research
The Diagnosis of Benign Joint Hypermobility Syndrome in Two Female Patients With Chronic Pain
Richard Strunk, DC, MS1*, Mark T. Pfefer, RN, MS, DC2, Lyndsay Andrews, R.T. (R) (CT)2 3. Address: 1Assistant Professor, Clinical Sciences/Research, Cleveland Chiropractic College, Overland Park, KS, USA, 2Professor and Director of Research, Cleveland Chiropractic College, Overland Park ,KS , USA, 3Graduate Student, Cleveland Chiropractic College, Overland Park, KS, USA. E-mail: Richard Strunk, DC, MS – [email protected] *Corresponding author Topics in Integrative Health Care 2011, Vol. 3(2) ID: 3.2005 Published on June 30, 2012 | Link to Document on the Web
Abstract
Introduction: Benign joint hypermobility syndrome (BJHS) is a hereditary connective tissue disorder frequently associated with joint pain. The purpose of this article is to demonstrate how BJHS was diagnosed in two female patients with chronic pain and to present other associated history and examination findings on these same two patients. Clinical Presentation: Two female patients, 27 and 32 years of age, with normal body mass indexes presented with a history of chronic spinal pain transiently lessened by multi-modal manual therapy. Each patient was diagnosed with BJHS. Both patients displayed joint hypermobility in the thumb(s), the fifth metacarpophalangeal joint and the lumbopelvic joints by having greater than normal range of motion in specific pre-determined directions. The 27 year old also had hyperextension of her elbows and myopia, while the 32 year had varicose veins and skin striae. Both had a history of back pain for greater than 3 months, key postural abnormalities and significant muscle imbalances. No treatment was administered to either patient since both patients were already currently receiving chiropractic treatment separate from this study.

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
2 | P a g e
Discussion: The diagnosis of BJHS can be challenging due to no gold standard test, however it’s an important entity to consider because of its unique characteristics and management implications. Conclusion: A detailed description of two patients with BJHS is presented. It is important for doctors to be aware of BJHS and to be able to diagnose it so these types of patients can be managed appropriately.
Introduction
Benign joint hypermobility syndrome (BJHS) is a hereditary connective tissue disorder defined by pain and hypermobility in multiple joints not linked to any systemic rheumatologic disease.1-4 It is also known as joint hypermobility syndrome or hypermobility syndrome and is seen as a separate entity to Marfan syndrome and most Ehlers-Danlos syndrome (EDS) types except for the hypermobility type or type III.5 BJHS is considered to be more common in African, Asian and Middle Eastern populations and is also more common in females and younger individuals.6-13 The true prevalence of BJHS is unknown but estimates range from 5% in the United States to 43% in African populations.7, 14 BJHS is diagnosed by patient history and or physical examination findings grouped into “Major” and “Minor” criteria called the Brighton Criteria (Table 1).15 Within the Brighton Criteria, the amount of joint hypermobility is calculated through the Brighton score (Table 2). Studies have shown that adults and children with BJHS frequently have arthralgia, with adults also being prone to generalized back pain.16-23 Despite published studies and articles in the medical literature on BJHS and its synonyms, BJHS is still not widely known or diagnosed by musculoskeletal health care providers.24 Due to the high costs and clinical challenges of effective management of patients with chronic spinal pain, appropriate diagnosis of musculoskeletal disorders such as BJHS is of utmost importance. With appropriate diagnosis, effective management will likely be enhanced. The purpose of this article is to describe how BJHS was diagnosed in two female patients with chronic pain and to present other associated history and examination findings.

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
3 | P a g e
Table 1. Brighton criteria for diagnosis of BJHS
Major Criteria
Beighton score of ≥ 4 (Table 2) Arthralgia for longer than 3 months in 4 or more joints
Minor Criteria
Beighton score of 1, 2, or 3 (Table 2) Arthralgia (>3-month duration) in one to three joints or back pain (>3-month duration) or
spondylosis, spndylolysis/spondylolisthesis . Dislocation or subluxation in more than one joint, or in one joint on more than one occasion. Three or more soft tissue lesions (eg, epicondylitis, tenosynovitis, bursitis) Marfanoid habitus (tall, slim, span greater than height (>1.03 ratio), upper segment less than
lower segment (<0.89 ratio), arachnodactyly) Skin striae, hyperextensibility, thin skin, or abnormal scarring Ocular signs: drooping eyelids, myopia, antimongoloid slant Varicose veins, hernia, or uterine or rectal prolapse, Mitral valve prolapse
Requirement for diagnosis BJHS is diagnosed in the presence of two major criteria; one major criterion plus two minor criteria; or four minor criteria. Two minor criteria will suffice where there is an unequivocally affected first degree relative in family history. The syndrome is excluded by the presence of Marfan’s or Ehlers-Danlos syndromes (other than the hypermobility type of Ehlers-Danlos syndrome formerly EDS III).
Table 2. Nine-point Beighton score for joint hypermobility
Passive dorsiflexion of the fifth metacarpophalangeal joint to at least 90 degrees. (1 point for left; 1 point for right) Passive opposition of the thumb to the volar aspect of the ipsilateral forearm (1 point for left; 1 point for right) Active hyperextension of the elbow to at least 10 degrees (1 point for left; 1 point for right) Active hyperextension of the knee to at least 10 degrees (1 point for left; 1 point for right) Lumbopelvic forward flexion with placement of hands flat on the floor without bending the knees (1 point) One point is gained for each side of the body for the first four maneuvers listed above, such that the hypermobility score is a maximum of 9 if all are positive.

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
4 | P a g e
Clinical Presentation
The two patients in this study were initially observed to have joint hypermobility during a chiropractic college class evaluating range of motion of the spine. At the end of the semester both patients consented for a more detailed evaluation of BJHS and any current complaints at the chiropractic college’s research department as part of this study.
Patient 1
History
A 27 year old, white female presented with persistent neck, low back, and left sacroiliac pain and intermittment left elbow pain. All painful areas were made worse by either prolonged postural positions (studying) or aerobic exercise and all areas except the left elbow were rated a 2/10 for average and current pain and 5/10 for worst pain using the numerical pain rating scale (NPRS). The patient’s left elbow pain was rated a 5/10 and would only occur with resistive elbow extension movements using an elliptical exercise machine. Pain would occur on average of 4 times per month and last only a few several seconds. The neck pain which began one and half years prior to the examination visit was reduced the most through spinal manipulation, Post Isometric Relaxation, and rest. The non-radiating, bilateral low back pain at L4-5 began three years prior to the examination visit with Sacral Occipital Technique (SOT), Applied Kinesiology and Brugger’s postural exercise providing the most relief. The patient’s left sacroiliac pain was reported to have begun 1 year prior to our first visit with rest and SOT used as palliative agents. All complaints began insidiously at their respective times. The patient denied any symptoms of pain, swelling or warmth in the hands or lower extremities. Other than the use of contact eye lenses to correct myopia, the patient’s past medical history was unremarkable including any previous systemic joint inflammatory conditions or previous diagnoses of Marfan syndrome or Ehlers-Danlos Syndrome (EDS).
Examination
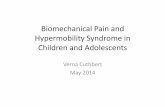
The patient’s Beighton’s score was a “6” out of “9” (see Figure 1). Her joint hypermobility was visually observed with left and right thumb opposition to the volar aspect of each ipsilateral forearm, 15 degrees of left elbow hyperextension, 20 degrees of right elbow hyperextension, left fifth metacarpophalangeal joint passive dorsiflexion to 90 degrees and lumbopelvic forward flexion with palmer surface of hands flat on floor with knees extended. A self report of myopia and a history of low back pain for greater than 3 months satisfied 2 minor criteria for the BJHS diagnosis.

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
5 | P a g e
Figure 1. Patient 1 Beighton score results. Beighton score equaled 6 out of 9 points.
a. Active left elbow hyperextension to at least 10° b. Active right elbow hyperextension to at least 10° c. Passive left thumb opposition to respective ipsilateral forearm d. Passive right thumb opposition to respective ipsilateral forearm e. Lumbopelvic flexion: palms flat on floor with knees extended f. Passive dorsiflexion of left 5th MCP to 90°

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
6 | P a g e
Physical examination findings revealed a body mass index of 20.4 (BMI) and normal strength of muscles innervated by cervical and lumbar nerve roots except for the right thumb which showed some weakness (4/5 on the 0-5 grading scale) in extension and adduction. Active range of motion (AROM) findings in the cervical and lumbar spine were equal to or above normal values in most directions with dull pain provoked in some directions (Table 3). Postural examination revealed an Upper Cross Syndrome presentation. Muscle movement pattern testing demonstrated bilateral over-activity of the upper trapezius/levator scapula, and lumbar paraspinals and some bilateral inhibition of the deep neck flexors, the serratus anterior, lower trapezius and gluteus maximus muscles.25 Hypertonicity and pain on palpation was noted in the cervical and lumbar paraspinals, the suboccipitals, rhomboids and peri-articular muscles of the left elbow, with joint dysfunction (hypomobility) at the cranio-cervical and thoraco-lumbar junctions.26

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
7 | P a g e
Table 3. Patient 1 active range of motion findings
Joint motiona Left Right
Cervical spine
Rotation 75 80*
Lateral Flexion 40 40*
Flexion 65
Extension 45
Lumbar spine
Flexion b
Extension 55*
lateral flexion 40 35*
Elbow
Extension 15 20
Flexion 145 145 a; measured in degrees with two method inclinometer or a goniometer, * presented with pain. b: Not measured.
Patient 2
History
A 32 year old, white female presented with right hip and thoracic spine pain which began 10 months and 10 years ago respectively. The right hip pain began insidiously as a deep, dull achy feeling localized in the anterior hip region near the anterior superior iliac spine. The hip pain was rated 2/10 on average, 1/10 at best, 2/10 at time of examination and 5/10 at worst according to the NPRS. Weight-bearing activities of daily living (ADL’s) such as walking/running increased the pain while non-weight-bearing ADL’s such as sitting decreased the pain. Spinal manipulation and ultrasound helped provide some improvement. The thoracic spine pain was also described as a stiff, dull achy feeling diffusely located throughout the thoracic spine bilaterally with no trauma associated with the onset. This pain was rated on the NPRS as a 1/10 at the time of the examination, on average and at best but when in static seated posture for prolonged periods the pain was rated a 3/10. Temporary palliative agents included hot moist pack therapy, and thoracic extension exercises. Other than being a smoker, having Type II Diabetes, Asthma, a thigh injury from an all terrain vehicle accident in 2000 (side unknown), the patient’s past medical history was unremarkable including any

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
8 | P a g e
previous systemic joint inflammatory conditions or previous diagnoses of Marfan syndrome or Ehlers-Danlos Syndrome (EDS).
Examination
The patient’s Beighton score was a “5” out of “9” (see Figure 2). Her score and joint hypermobility was demonstrated with left and right thumb opposition to the volar aspect of each ipsilateral forearm, left and right fifth metacarpophalangeal joint passive dorsiflexion to 90 degrees and lumbopelvic forward flexion with palmer surface of hands flat on floor with knees extended. This patient also reported a history of back pain for greater than three months (actual =10 years), and had varicose veins in right posterior calf and skin striae in posterior aspect of right axilla on observation.
Figure 2. Patient 2 Beighton score results. Beighton score equaled 5 out of 9 points.
a. Passive dorsiflexion of left 5th MCP to 90° b. Passive dorsiflexion of right 5th MCP to 90° c. Passive left thumb opposition to respective ipsilateral forearm d. Passive right thumb opposition to respective ipsilateral forearm e. Lumbopelvic flexion: palms flat on floor with knees extended

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
9 | P a g e

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
10 | P a g e
The patient’s BMI was calculated to be 24.9. A focused musculoskeletal examination revealed normal muscle strength in the lower extremities except for bilateral weak quadriceps and left Iliopsoas (4/5 on 0-5 grading scale). Active range of motion in the right and left hips were equal to normal range values in most directions with dull, anterior hip pain only reported on right active abduction and internal rotation (Table 4). Thoracolumbar AROM was within normal limits without pain except for right rotation which was painful and decreased by visual observation. Orthopedic testing of the right hip was unremarkable except for a stretching type pain produced in the anterior hip with the Patrick Fabere Test. Relevant postural examination findings showed a moderate hypo-kyphotic thoracic spine, hypertrophy of the thoracolumbar paraspinals, a mild externally rotated right foot and slight-moderate hyperextension of both knees. Muscle movement pattern testing demonstrated over-activity of the lumbar paraspinals and hip flexors and inhibition of both gluteus maximus muscles with greater severity on the right side. 25 Palpation of the back and hip region revealed hypertonicity of the left gluteus medius and pain in the right gluteal muscles, the right piriformis, the right anterior superior iliac spine region and the thoraco-lumbar paraspinals. Joint dysfunction (hypomobility) was noted by motion palpation in the upper and lower thoracic spine.26 No treatment was administered to either patient since both patients were currently receiving chiropractic treatment by either field practitioners and/or chiropractic interns separate from this project and because the purpose of this project was focused on the diagnosis of BJHS.
Table 4. Patient 2 active range of motion findings
Joint motiona Left Right
Hip
Flexion (supine) 90 90
Extension (prone) 20 15
Adduction (supine) b b
Abduction (supine) 45 40*
Internal Rotation ‡ 30 30*
External Rotation ‡ 20 35 a; measured in degrees with two method inclinometer or a goniometer, * presented with pain. b: Not measured, ‡ measured in seated position. Thoracic spine AROM not measured with inclinometer method.
Discussion
When considering a diagnosis of BJHS, other genetic disorders, inflammatory, infectious and autoimmune disorders need to be excluded as they can present with joint hypermobility and warrant unique or urgent management. Genetic disorders such as Marfan syndrome, Ehlers –Danlos syndrome (except type III), Osteogenesis Imperfecta, Down’s syndrome and autoimmune disorders such as

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
11 | P a g e
Rheumatoid arthritis (RA) can present with joint hypermobility. The common characteristic signs or symptoms of these genetic disorders or other conditions such as RA were not present in each of our patient’s history or though observation and palpation and subsequently these conditions were not likely to be present. Other more “benign” functional neuromusculoskeletal deficits were accessed through a focused neuromusculoskeletal examination including the Brighton criteria. Based on each of the patient’s history and examination findings including the Brighton criteria results and the Beighton scores both patients were diagnosed with BJHS. Patient one had a Beighton score of “6” and fulfilled two Brighton minor criteria while patient two had a Beighton score of “5” and fulfilled three Brighton minor criteria. The Brighton criteria used to diagnosis of BJHS could be considered subjective with certain criteria, but a recent inter-examiner reliability study with experienced rheumatologists showed either substantial or high levels of agreement for the Beighton tests with kappa values of 0.60 to above 0.8027 with similar values for the Brighton criteria. Other studies looking at intra-observer and inter-observer reliability reported similar findings.28, 29 While the reliability of the Brighton criteria and the Beighton tests show promise, the validity of both the Brighton criteria and Beighton tests is less clear. Validity inconsistencies with Beighton score cutoff levels, the different joints needed to diagnose BJHS and the correlation between the “minor criteria” and BJHS can cause challenges among practicing doctors and researchers. 28, 29 30-33 34 However, despite validity inconsistencies, the Brighton Criteria is the most widely used and recognized means to diagnose BJHS. One of the main limitations of our study was not using a goniometer to assess all the Beigton hypermobility criteria. Even though we followed the recommended BJHS guidelines, using a range of motion instrument would have allowed a more precise assessment of the knee joints and the MCP joints of the fifth digits. This would have assisted us with both of our patients when assessing knee hyperextension and dorsiflexion of the fifth MCP joints. Although not part of the Beighton criteria, an inclinometer ROM assessment of the thoracic spine would have aided our evaluation of patient two’s thoracic spine pain. A functional musculoskeletal examination was performed on each patient with special attention to muscle strength, coordination and ROM due to theorized affects of BJHS. As a result, specific orthopedic testing was not included. Specific orthopedic ligament integrity testing would have proved informative to see if these two patients had any ligament laxity in the same joints that were hypermobile according to the Beighton hypermobility assessment. Lastly, because there are some validity inconsistencies with the BJHS diagnostic criteria (lack of a gold standard test), it is possible that the two patients had localized joint hypermobility instead of BJHS. Despite some limitations inherent to diagnosing BJHS, it appears BJHS or at least some form of joint hypermobility is present in certain people with pain. As a result, screening for this joint condition would likely add value in determining the best course of treatment for people with this entity. Hakim and Grahame developed a simple five item questionnaire to screen patients for joint hypermobility (Table 5). The questionnaire has been shown to have good sensitivity and specificity for hypermobility in patients when two or more of the questions are affirmative.35 With this questionnaire, a health care provider wouldn’t have to use the Brighton criteria on every patient with pain, just on patients with two of more affirmative responses on the questionnaire. Health care providers who perform manual therapy or spinal manipulation might apply specific techniques to this population of patients with better results if they know their patient has BJHS. Due to the suspected nature of BJHS (a defect in collagen structure), high velocity, low amplitude spinal manipulation can be contraindicated to those joints that have laxity or hypermobility. Although not researched, low force joint manipulative techniques and or myofascial techniques might provide a safer and more efficacious approach for these types of patients within a

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
12 | P a g e
multidisciplinary care program. More research is needed on the best management approach and on the diagnostic criteria for patients with BJHS.
Table 5. Five item screening questionnaire for BJHS
1. Can you now (or could you ever) place your hands flat on the floor without bending your knees?
2. Can you now (or could you ever) bend you thumb to touch your forearm?
3. As a child did you amuse your friends by contorting your body into strange shapes or could you do splits?
4. As a child or teenager did your shoulder or kneecap dislocate on more than one occasion?
5. Do you consider yourself double jointed?
Answer in the affirmative to two or more items suggests hypermobility.
Conclusion
This case series is important because it describes history and examination findings on two patients diagnosed with BJHS who had chronic spinal pain. Practitioners, including doctors of chiropractic who diagnose and treat musculoskeletal based pain, should be able to rule out or diagnose BJHS. Proper diagnosis of musculoskeletal complaints is vital if effective treatment is to be rendered.
Safety and other human subject considerations
The study was approved by the college’s institutional review board before project onset, and both patients signed an informed consent form before any data collection or assessment.
Funding sources and conflicts of interest
The authors declare that they have no competing interests.
References
1. Child AH. Joint hypermobility syndrome: inherited disorder of collagen synthesis. J Rheumatol 1986;13(2):239-43.
2. Hakim AJ, Cherkas LF, Grahame R, Spector TD, MacGregor AJ. The genetic epidemiology of joint hypermobility: a population study of female twins. Arthritis Rheum 2004;50(8):2640-4. 3. Prockop DJ, Kivirikko KI. Collagens: molecular biology, diseases, and potentials for therapy. Annu Rev Biochem 1995;64:403-34.

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
13 | P a g e
4. Handler CE, Child A, Light ND, Dorrance DE. Mitral valve prolapse, aortic compliance, and skin collagen in joint hypermobility syndrome. Br Heart J 1985;54(5):501-8. 5. Tinkle BT, Bird HA, Grahame R, Lavallee M, Levy HP, Sillence D. The Lack of Clinical Distinction Between the Hypermobility of Ehlers-Danlos Syndrome and the Joint Hypermobility Syndrome (a.k.a. Hypermobility Syndrome). Am J Med Genet Part A 2009;149A:2368-70. 6. Beighton P, Solomon L, Soskolne CL. Articular mobility in an African population. Ann Rheum Dis 1973;32(5):413-8. 7. Birrell FN, Adebajo AO, Hazleman BL, Silman AJ. High prevalence of joint laxity in West Africans. Br J Rheumatol 1994;33(1):56-9. 8. Jansson A, Saartok T, Werner S, Renstrom P. General joint laxity in 1845 Swedish school children of different ages: age and gender specific distributions. Acta Paediatr 2004;93:1202-6. 9. Seow CC, Chow PK, Khong KS. A Study of joint mobility in a normal population. Ann Acad Med Singapore 1999;28:231-6. 10. Wordsworth P, Ogilvie D, Smith R, Sykes B. Joint mobility with particular reference to racial variation and inherited connective tissue disorders. Br J Rheumatol 1987;26:9-12. 11. Grahame R, Edwards JC, Pitcher D, Gabell A, Harvey W. A clinical and echocardiographic study of patients with the hypermobility syndrome. Ann Rheum Dis 1981;40(6):541-6. 12. Kraus VB, Li YJ, Martin ER, et al. Articular hypermobility is a protective factor for hand osteoarthritis. Arthritis Rheum 2004;50(7):2178-83. 13. Grahame R, Hakim A. Joint hypermobility syndrome is highly prevalent in general rheumatology clinics, its occurrence and clinical presentation being gender, age and race related. Ann Rheum 2006;65(suppl 2):263. 14. Jessee EF, Owens DS, Sagar KB. The benign hypermobile joint syndrome. Arthritis Rheumatism 1980;23(9):1053-56. 15. Grahame R, Bird HA, Child A. The revised (Brighton 1998) criteria for the diagnosis of benign joint hypermobility syndrome (BJHS). J Rheumatol 2000;27(7):1777-9. 16. El-Garf AK, Mahmoud GA, Mahgoub EH. Hypermobility among Egyptian children: prevalence and features. J Rheumatol 1998;25(5):1003-5. 17. Al-Rawi ZS, Al-Aszawi AJ, Al-Chalabi T. Joint mobility among university students in Iraq. Br J Rheumatol 1985;24(4):326-31. 18. Larsson LG, Baum J, Mudholkar GS, Kollia GD. Benefits and disadvantages of joint hypermobility among musicians. N Engl J Med 1993;329(15):1079-82.

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
14 | P a g e
19. Gedalia A, Press J. Articular symptoms in hypermobile schoolchildren: a prospective study. J Pediatr 1991;119(6):944-6. 20. Seckin U, Tur BS, Yilmaz O, Yagci I, Bodur H, Arasil T. The prevalence of joint hypermobility among high school students. Rheumatol Int 2005;25(4):260-3. 21. Acasuso Diaz M, Collantes Estevez E, Sanchez Guijo P. Joint hyperlaxity and musculoligamentous lesions: study of a population of homogeneous age, sex and physical exertion. Br J Rheumatol 1993;32(2):120-2. 22. Bravo JF, Wolff C. Clinical study of hereditary disorders of connective tissues in a Chilean population: joint hypermobility syndrome and vascular Ehlers-Danlos syndrome. Arthritis Rheum 2006;54(2):515-23. 23. El-Metwally A, Salminen JJ, Auvinen A, Kautiainen H, Mikkelsson M. Prognosis of non-specific musculoskeletal pain in preadolescents: a prospective 4-year follow-up study till adolescence. Pain 2004;110(3):550-9. 24. Grahame R, Bird H. British consultant rheumatologists' perceptions about the hypermobility syndrome: a national survey. Rheumatol (Oxford) 2001;40(5):559-62. 25. Page P, Frank CC, Lardner R. Assessment and Treatment of Muscle Imbalance: The Janda Approach. Champaign: Human Kinetics; 2010. 26. Peterson D, Bergman T. Chiropractic Technique: Principles and Procedures. 2nd Edition ed. St. Louis: Mosby; 2002. 27. Juul-Kristensen B, Rogind H, Jensen DV, Remvig L. Inter-examiner reproducibility of tests and criteria for generalized joint hypermobility and benign joint hypermobility syndrome. Rheumatol (Oxford) 2007;46(12):1835-41. 28. Bulbena A, Duro J, Porta M, Faus S, Vallescar R, Martin-Santos R. Clinical assessment of hypermobility of joints: assembling criteria. J Rheumatol 1992;19:115-22. 29. Mikkelsson M, Salminen J, Kautiainen H. Joint hypermobility is not a contributing factor to musculoskeletal pain in pre-adolescents. J Rheumatol 1996;23:1963-7. 30. Carter C, Wilkinson J. Persistent Joint Laxity and Congenital Dislocation of the Hip. J Bone Joint Surg Br 1964;46:40-5. 31. Kirk J, Ansell B, Bywaters E. The hypermobility syndrome. Musculoskeletal complaints associated with generalized joint hypermobility. Ann Rheum Dis 1967;26:419-25. 32. Beighton P, Horan F. Dominant inheritance in familial generalized articular hypermobility. J Bone Joint Surg Br 1970;52:145-7. 33. Rotes-Querol J, Duran J, Subiros R, Pifferer J, Gomez J. La laxite articularie comme facteur d'alterations de l'appareil locomoteur (Nouvelle etude 1971). Rhumatologie 1972;24:179-91.

TOPICS IN INTEGRATIVE HEALTH CARE [ISSN 2158-4222] – VOL 3(2) June 30, 2012
15 | P a g e
34. Remvig L, Jensen DV, Ward RC. Epidemiology of general joint hypermobility and basis for the proposed criteria for benign joint hypermobility syndrome: review of the literature. J Rheumatol 2007;34(4):804-9. 35. Hakim AJ, Grahame R. A simple questionnaire to detect hypermobility: an adjunct to the assessment of patients with diffuse musculoskeletal pain. Int J Clin Pract 2003b(57):163-66.