The Cost of Cure: Understanding Financial Toxicity in Head ...
1
+ $50,000 0 - $50,000 - $100,000 Financial Toxicity measured by FDQ No Yes Figure 3. Income Change from Diagnosis to Enrollment by FT (N=27) The Cost of Cure: Understanding Financial Toxicity in Head and Neck Cancer Survivors 1 University of Pittsburgh, Pittsburgh, PA, USA; 2 UPMC Insurance Services, Pittsburgh, PA, USA; 3 UPMC Hillman Cancer Center, Pittsburgh, PA, USA. BACKGROUND • Financial Toxicity (FT) is defined as the objective and subjective patient-level impact of the costs of cancer care. • It can afflict individuals even those with health insurance - from any socioeconomic background. 1,2 • Compared to individuals with other chronic illnesses, cancer survivors have been shown to have higher out-of-pocket expenses (OOPE) which may persist years after initial diagnosis. 2,3 • Several large-scale studies have suggested a link between cancer-related financial strain and decreased health-related quality of life (HRQOL). 4-6 • For patients with advanced or potentially curable cancer, discussion of treatment options vis-à-vis length of life, quality of life, and financial burden is at the crux of shared decision-making. • Rapid translation of breakthroughs in cancer biology into new therapies has led to increasing complexity in treatment choices, which often vary little in clinical effectiveness and toxicity, but have wide disparities in cost. 7 • Following treatment, up to 48% of head and neck cancer (HNC) survivors reduced work, among whom 33% ceased employment. 8 • Inability to return to work may reduce earnings or employment-based health insurance options, thereby exacerbating FT and influencing treatment choices and resources for medical care. • The purpose of our study is to understand HNC survivors’ treatment-related FT. Figure 1. Patient selection Venn diagram Khalil Baddour, MD 1 ; Meng Zhao 2 ; Michael Corcoran 2 ; Lingyun Lyu, MS 1 ; Maryanna S. Owoc 1 ; Shyamal D. Peddada, PhD 1 ; Teresa H. Thomas, PhD, RN 1 ; Lindsay M. Sabik, PhD 1 ; Jonas T. Johnson, MD 1 ; Marci L. Nilsen, PhD, RN 1 ; Robert L. Ferris, MD, PhD 1,3 ; Leila J. Mady, MD, PhD, MPH 1 MATERIALS AND METHODS • OOPE vary widely across different insurance plans and continue to rise as treatment length increases, highlighting the importance of shared-decision making prior to establishing a treatment plan and discussing costs of cancer treatment with patients prior to initiating treatment. • Subgroup analysis shows a great number of patients with negative income change from diagnosis and/or a gross income ceiling of $60,000 at survey with a significant proportion exhibiting subjective FT (by FDQ). • Medicaid patients displayed low objective FT (by OOPE) but the highest subjective FT (by COST, data not shown). The former may be explained by the comprehensive coverage programs like Medicaid offer while the latter may reflect the non-medical socioeconomic conditions patients may be experiencing. 1. Zafar SY. Financial Toxicity of Cancer Care: It's Time to Intervene. J Natl Cancer Inst. 2016;108(5). | 2. Zafar SY, Peppercorn JM, Schrag D, et al. The financial toxicity of cancer treatment: a pilot study assessing out-of-pocket expenses and the insured cancer patient's experience. Oncologist. 2013;18(4):381-390. | 3. Guy GP, Jr., Ekwueme DU, Yabroff KR, et al. Economic burden of cancer survivorship among adults in the United States. J Clin Oncol. 2013;31(30):3749-3757. | 4. Zafar SY, McNeil RB, Thomas CM, Lathan CS, Ayanian JZ, Provenzale D. Population-based assessment of cancer survivors' financial burden and quality of life: a prospective cohort study. J Oncol Pract. 2015;11(2):145-150. | 5. Fenn KM, Evans SB, McCorkle R, et al. Impact of financial burden of cancer on survivors' quality of life. J Oncol Pract. 2014;10(5):332-338. | 6. Kale HP, Carroll NV. Self-reported financial burden of cancer care and its effect on physical and mental health related quality of life among US cancer survivors. Cancer. 2016;122(8):283-289. | 7. Yu PP. Challenges in Measuring Cost and Value in Oncology: Making It Personal. Value Health. 2016;19(5):520524. | 8. Giuliani M, Papadakos J, Broadhurst M, et al. The prevalence and determinants of return to work in head and neck cancer survivors. Support Care Cancer. 2019;27(2):539-546. Retrospective Review Prospective Enrollment Study Sample Goal: Identify HNC-related objective FT data 7/2013 - 3/2018 Inclusion Criteria 18+ years old Primary HNC Diagnosis Treatment within a 2-year period UPMC Health Plan members Available Insurance Claims Data N=5,156 patients N=252 patients Goal: Acquire patient-reported data 1/2018 - 8/2018 UPMC Survivorship Clinic COmprehensive Score for financial Toxicity (COST) Continuous (0-44) Lower scores = worse subjective FT Financial Distress Questionnaire (FDQ) 2-item Questionnaire Ordinal Scoring of FT Demographic and Income Data Both Claims and Insurance Data Available N=71 patients CONCLUSIONS $3,099 $3,739 $3,409 $384 $4,264 $1,431 $3,309 $0 $1,000 $2,000 $3,000 $4,000 ASO Commercial Individual Exchange Medicaid Medicare Special Needs All Types $1,238 $1,690 $1,880 $2,523 $3,463 $2,814 $4,494 $0 $1,000 $2,000 $3,000 $4,000 0-3 4-6 7-12 13-24 25-36 37-48 49-60 A B Figure 2. Average Per-Member OOPE (N=71) by Insurance Type (A) and by Treatment Length (B) Treatment Length (months) Individual Exchange RESULTS Figure 4. Gross Income by Subjective FT (N=27) Financial Toxicity measured by FDQ No Yes Gross Income at Diagnosis Gross Income at Survey
Transcript of The Cost of Cure: Understanding Financial Toxicity in Head ...

+ $50,000
0
- $50,000
- $100,000Financial Toxicity measured by FDQ
NoYes
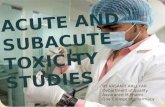
Figure 3. Income Change from Diagnosis to Enrollment by FT (N=27)
The Cost of Cure: Understanding Financial Toxicity in Head and Neck Cancer Survivors
1University of Pittsburgh, Pittsburgh, PA, USA; 2UPMC Insurance Services, Pittsburgh, PA, USA; 3UPMC Hillman Cancer Center, Pittsburgh, PA, USA.
BACKGROUND• Financial Toxicity (FT) is defined as the objective and subjective patient-level impact of the costs
of cancer care.• It can afflict individuals even those with health insurance - from any socioeconomic background.1,2• Compared to individuals with other chronic illnesses, cancer survivors have been shown to have
higher out-of-pocket expenses (OOPE) which may persist years after initial diagnosis.2,3• Several large-scale studies have suggested a link between cancer-related financial strain and
decreased health-related quality of life (HRQOL).4-6• For patients with advanced or potentially curable cancer, discussion of treatment options vis-à-vis
length of life, quality of life, and financial burden is at the crux of shared decision-making.• Rapid translation of breakthroughs in cancer biology into new therapies has led to increasing
complexity in treatment choices, which often vary little in clinical effectiveness and toxicity, buthave wide disparities in cost.7
• Following treatment, up to 48% of head and neck cancer (HNC) survivors reduced work, amongwhom 33% ceased employment.8
• Inability to return to work may reduce earnings or employment-based health insurance options,thereby exacerbating FT and influencing treatment choices and resources for medical care.
• The purpose of our study is to understand HNC survivors’ treatment-related FT.
Figure 1. Patient selection Venn diagram
Khalil Baddour, MD1; Meng Zhao2; Michael Corcoran2; Lingyun Lyu, MS1; Maryanna S. Owoc1; Shyamal D. Peddada, PhD1; Teresa H. Thomas, PhD, RN1; Lindsay M. Sabik, PhD1; Jonas T. Johnson, MD1; Marci L. Nilsen, PhD, RN1; Robert L. Ferris, MD, PhD1,3; Leila J. Mady, MD, PhD, MPH1
MATERIALS AND METHODS
• OOPE vary widely across different insurance plans and continue to rise as treatment length increases,highlighting the importance of shared-decision making prior to establishing a treatment plan anddiscussing costs of cancer treatment with patients prior to initiating treatment.
• Subgroup analysis shows a great number of patients with negative income change from diagnosis and/or agross income ceiling of $60,000 at survey with a significant proportion exhibiting subjective FT (by FDQ).
• Medicaid patients displayed low objective FT (by OOPE) but the highest subjective FT (by COST, data notshown). The former may be explained by the comprehensive coverage programs like Medicaid offer whilethe latter may reflect the non-medical socioeconomic conditions patients may be experiencing.
1. Zafar SY. Financial Toxicity of Cancer Care: It's Time to Intervene. J Natl Cancer Inst. 2016;108(5). | 2. Zafar SY, Peppercorn JM, Schrag D, et al. The financial toxicity of cancer treatment: a pilot study assessing out-of-pocket expenses and the insured cancer patient's experience. Oncologist. 2013;18(4):381-390. | 3. Guy GP, Jr., EkwuemeDU, Yabroff KR, et al. Economic burden of cancer survivorship among adults in the United States. J Clin Oncol. 2013;31(30):3749-3757. | 4. Zafar SY, McNeil RB, Thomas CM, Lathan CS, Ayanian JZ, Provenzale D. Population-based assessment of cancer survivors' financial burden and quality of life: a prospective cohort study. J Oncol Pract.2015;11(2):145-150. | 5. Fenn KM, Evans SB, McCorkle R, et al. Impact of financial burden of cancer on survivors' quality of life. J Oncol Pract. 2014;10(5):332-338. | 6. Kale HP, Carroll NV. Self-reported financial burden of cancer care and its effect on physical and mental health related quality of life among US cancer survivors. Cancer.2016;122(8):283-289. | 7. Yu PP. Challenges in Measuring Cost and Value in Oncology: Making It Personal. Value Health. 2016;19(5):520524. | 8. Giuliani M, Papadakos J, Broadhurst M, et al. The prevalence and determinants of return to work in head and neck cancer survivors. Support Care Cancer. 2019;27(2):539-546.
RetrospectiveReview
ProspectiveEnrollment
Study SampleGoal: Identify HNC-related objective
FT data7/2013 - 3/2018
Inclusion Criteria18+ years old
Primary HNC DiagnosisTreatment within a 2-year period
UPMC Health Plan membersAvailable Insurance Claims Data
N=5,156 patients N=252 patients
Goal: Acquire patient-reported data1/2018 - 8/2018
UPMC Survivorship Clinic
COmprehensive Score for financial Toxicity (COST)
Continuous (0-44)Lower scores = worse subjective FT
Financial Distress Questionnaire (FDQ)2-item QuestionnaireOrdinal Scoring of FT
Demographic and Income Data
Both Claims and Insurance Data Available
N=71 patients
CONCLUSIONS
$3,099
$3,739$3,409
$384
$4,264
$1,431
$3,309
$0
$1,000
$2,000
$3,000
$4,000
$5,000
ASO
Commercial
Individual
Exchan
ge
Medica
id
Medica
re
Special N
eeds
All Typ
es
$1,238$1,690 $1,880
$2,523
$3,463
$2,814
$4,494
$0
$1,000
$2,000
$3,000
$4,000
$5,000
0-3Months
4-6Months
7-12Months
13-24Months
25-36Months
37-48Months
49-60Months
A B
Figure 2. Average Per-Member OOPE (N=71) by Insurance Type (A) and by Treatment Length (B)
Treatment Length (months)
Individual
Exchan
ge
RESULTS
Figure 4. Gross Income by Subjective FT (N=27)
Financial Toxicity measured by FDQ
No
Yes
Gross Income at Diagnosis
Gross Income at Survey