
The Brain in Hereditary Hemorrhagic...
9
The Brain in Hereditary Hemorrhagic Telangiectasia BY THOMAS J. REAGAN, M.D.,* AND WILLIAM H. BLOOM, M.D.f Abstract: The Brain in Hereditary Hemorrhagic Telangiectasia • While neurological symptoms are often mentioned in reports of families with hereditary hemorrhagic telangiectasia (HHT) and are frequently assumed to be due to vascular anomalies of the central nervous system, documentation of such anomalies is surprisingly rare. Two cases of surgically treated symptomatic cerebral vascular malformations in HHT have been published previously. In addition, there are three descriptions of vascular anomalies discovered at autopsy in the brains of neurologically asymptomatic patients with HHT available in the literature. A complete postmortem examination of a patient with a symptomatic cerebral vascular anomaly associated with HHT has not been recorded previously. The patient reported in this paper presented with seizures and underwent surgical resection of infarcted brain tissue associated with a venous angioma. He died six months later and, at autopsy, was found to have multiple "cryptic" venous angiomas of the brain. Hypoxic damage to brain tissue related to small venous angiomas is one mechanism whereby these lesions may become symptomatic. Hemorrhage may also occur. Neurological symptoms in patients with HHT cannot be assumed to be due to cerebral vascular anomalies, and consideration must be especially given to the complications of pulmonary arteriovenous fistula such as polycythemia, embolism, and abscess. ADDITIONAL KEY WORDS cerebral vascular malformation cerebral infarction Rendu-Osler-Weber syndrome venous angioma Introduction • Hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome) is a domi- nantly inherited disorder whose cardinal mani- festation is the appearance, usually around puberty, of telangiectasias distributed variably over the skin and mucous membranes of the body. The most common symptom of the disease is hemorrhage from lesions of the nasal mucosa, and the vast majority of patients first present clinically with epistaxis. •Fellow in Neuropathology, New York University Medical Center, 550 First Avenue, New York, New York, 10016. •(•Consulting Neurosurgeon, Central Suffolk Hos- pital, Riverhead, Long Island, New York. This work was supported in part by Special Fellowship 2 F l l NS 2109-02 NSRB from the National Institute of Neurological Diseases and Stroke, Public Health Service. Send requests for reprints to Dr. Reagan. Stroke, Vol. 2, JulyAugutt 7971 Over 300 families affected with the condition have been recorded in the literature. 1 As experience with the clinical and pathologi- cal features of the disorder has grown, it has become apparent that the abnormalities are by no means confined to the small vessels of epithelial surfaces but may include major vascular anomalies in a variety of internal organs. 2 ' 8 The most frequently described visceral vascular anomaly is the arteriovenous fistula of the lung. Pulmonary arteriovenous fistulas occurred in 15.4% of individuals affected by the disease in the kinship reported by Hodgson et al. 4 Conversely, about 50% of pulmo- nary arteriovenous fistulas are said to occur in patients with hereditary hemorrhagic telangiectasia."• fl Much less common, and certainly less well documented, are vascular malformations 361 by guest on June 5, 2018 http://stroke.ahajournals.org/ Downloaded from
-
Upload
truongmien -
Category
Documents
-
view
236 -
download
4
Transcript of The Brain in Hereditary Hemorrhagic...

The Brain in Hereditary HemorrhagicTelangiectasiaBY THOMAS J. REAGAN, M.D.,* AND WILLIAM H. BLOOM, M.D.f
Abstract:The Brain inHereditaryHemorrhagicTelangiectasia
• While neurological symptoms are often mentioned in reports of familieswith hereditary hemorrhagic telangiectasia (HHT) and are frequently assumedto be due to vascular anomalies of the central nervous system, documentationof such anomalies is surprisingly rare. Two cases of surgically treatedsymptomatic cerebral vascular malformations in HHT have been publishedpreviously. In addition, there are three descriptions of vascular anomaliesdiscovered at autopsy in the brains of neurologically asymptomatic patientswith HHT available in the literature. A complete postmortem examination of apatient with a symptomatic cerebral vascular anomaly associated with HHT hasnot been recorded previously.
The patient reported in this paper presented with seizures and underwentsurgical resection of infarcted brain tissue associated with a venous angioma.He died six months later and, at autopsy, was found to have multiple "cryptic"venous angiomas of the brain. Hypoxic damage to brain tissue related to smallvenous angiomas is one mechanism whereby these lesions may becomesymptomatic. Hemorrhage may also occur. Neurological symptoms in patientswith HHT cannot be assumed to be due to cerebral vascular anomalies, andconsideration must be especially given to the complications of pulmonaryarteriovenous fistula such as polycythemia, embolism, and abscess.
ADDITIONAL KEY WORDScerebral vascular malformationcerebral infarction
Rendu-Osler-Weber syndromevenous angioma
Introduction• Hereditary hemorrhagic telangiectasia(Rendu-Osler-Weber syndrome) is a domi-nantly inherited disorder whose cardinal mani-festation is the appearance, usually aroundpuberty, of telangiectasias distributed variablyover the skin and mucous membranes of thebody. The most common symptom of thedisease is hemorrhage from lesions of the nasalmucosa, and the vast majority of patients firstpresent clinically with epistaxis.
•Fellow in Neuropathology, New York UniversityMedical Center, 550 First Avenue, New York, NewYork, 10016.
•(•Consulting Neurosurgeon, Central Suffolk Hos-pital, Riverhead, Long Island, New York.
This work was supported in part by SpecialFellowship 2 F l l NS 2109-02 NSRB from theNational Institute of Neurological Diseases andStroke, Public Health Service.
Send requests for reprints to Dr. Reagan.
Stroke, Vol. 2, JulyAugutt 7971
Over 300 families affected with thecondition have been recorded in the literature.1
As experience with the clinical and pathologi-cal features of the disorder has grown, it hasbecome apparent that the abnormalities are byno means confined to the small vessels ofepithelial surfaces but may include majorvascular anomalies in a variety of internalorgans.2'8
The most frequently described visceralvascular anomaly is the arteriovenous fistula ofthe lung. Pulmonary arteriovenous fistulasoccurred in 15.4% of individuals affected bythe disease in the kinship reported by Hodgsonet al.4 Conversely, about 50% of pulmo-nary arteriovenous fistulas are said to occurin patients with hereditary hemorrhagictelangiectasia."• fl
Much less common, and certainly lesswell documented, are vascular malformations
361
by guest on June 5, 2018http://stroke.ahajournals.org/
Dow
nloaded from
REAGAN, BLOOM
\k a a"5""
D" 0" d" 0" 0"O.IHICALLY 4JFICTXD WITH BUT
laUKBJXIC CTHFTCm
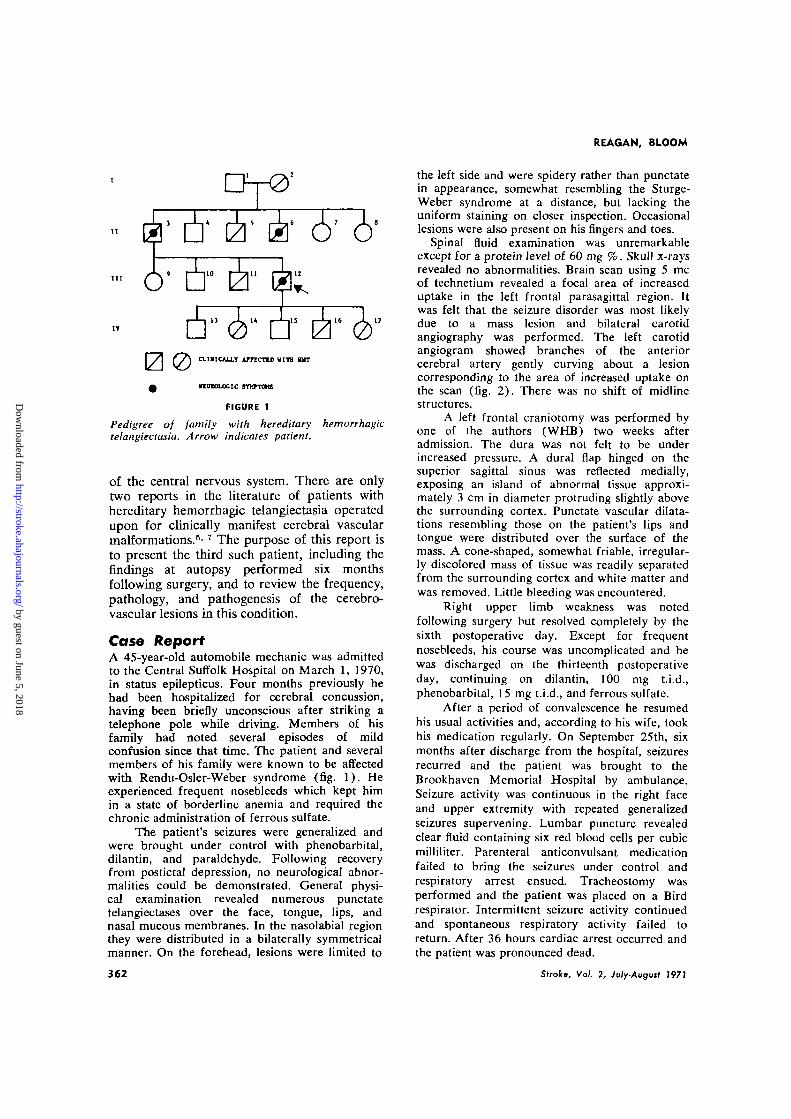
FIGURE 1
Pedigree of family with hereditary hemorrhagictelangiectasia. Arrow indicates patient.
of the central nervous system. There are onlytwo reports in the literature of patients withhereditary hemorrhagic telangiectasia operatedupon for clinically manifest cerebral vascularmalformations.5'7 The purpose of this report isto present the third such patient, including thefindings at autopsy performed six monthsfollowing surgery, and to review the frequency,pathology, and pathogenesis of the cerebro-vascular lesions in this condition.
Case ReportA 45-year-old automobile mechanic was admittedto the Central Suffolk Hospital on March 1, 1970,in status epilepticus. Four months previously hehad been hospitalized for cerebral concussion,having been briefly unconscious after striking atelephone pole while driving. Members of hisfamily had noted several episodes of mildconfusion since that time. The patient and severalmembers of his family were known to be affectedwith Rendu-Osler-Weber syndrome (fig. 1). Heexperienced frequent nosebleeds which kept himin a state of borderline anemia and required thechronic administration of ferrous sulfate.
The patient's seizures were generalized andwere brought under control with phenobarbital,dilantin, and paraldehyde. Following recoveryfrom postictal depression, no neurological abnor-malities could be demonstrated. General physi-cal examination revealed numerous punctatetelangiectases over the face, tongue, lips, andnasal mucous membranes. In the nasolabial regionthey were distributed in a bilaterally symmetricalmanner. On the forehead, lesions were limited to
362
the left side and were spidery rather than punctatein appearance, somewhat resembling the Sturge-Weber syndrome at a distance, but lacking theuniform staining on closer inspection. Occasionallesions were also present on his fingers and toes.
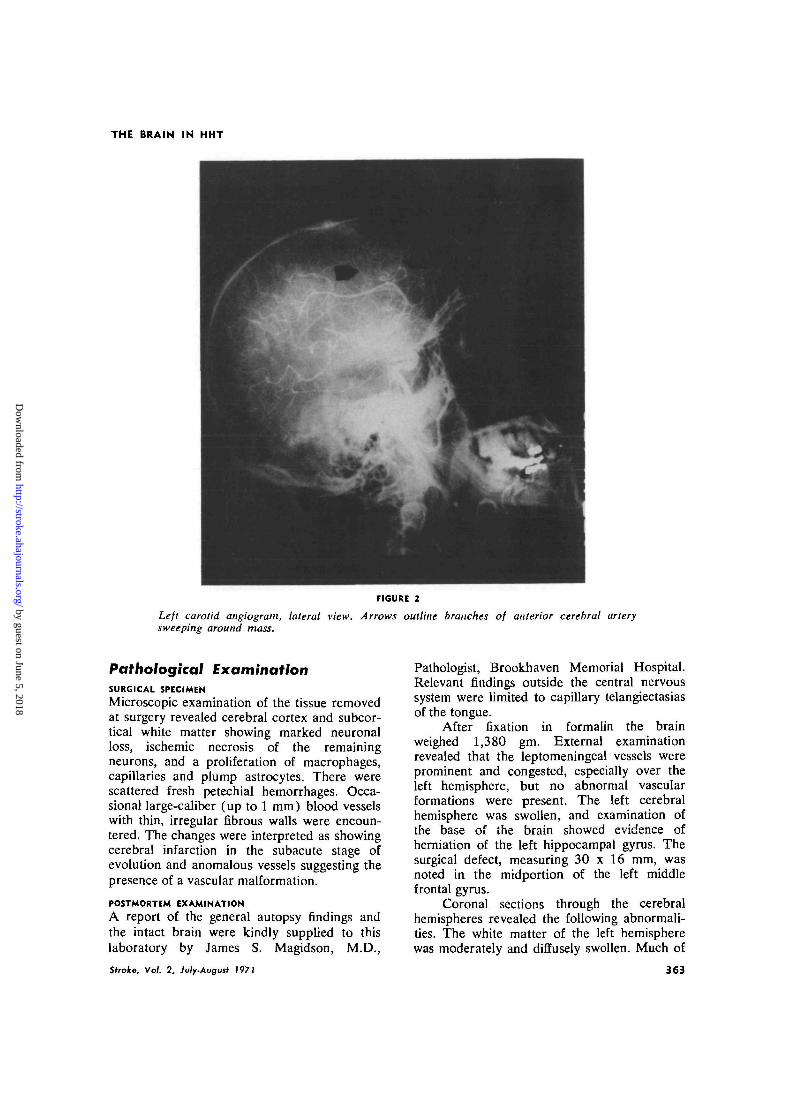
Spinal fluid examination was unremarkableexcept for a protein level of 60 mg %. Skull x-raysrevealed no abnormalities. Brain scan using 5 meof technetium revealed a focal area of increaseduptake in the left frontal parasagittal region. Itwas felt that the seizure disorder was most likelydue to a mass lesion and bilateral carotidangiography was performed. The left carotidangiogram showed branches of the anteriorcerebral artery gently curving about a lesioncorresponding to the area of increased uptake onthe scan (fig. 2). There was no shift of midlinestructures.
A left frontal craniotomy was performed byone of the authors (WHB) two weeks afteradmission. The dura was not felt to be underincreased pressure. A dural flap hinged on thesuperior sagittal sinus was reflected medially,exposing an island of abnormal tissue approxi-mately 3 cm in diameter protruding slightly abovethe surrounding cortex. Punctate vascular dilata-tions resembling those on the patient's lips andtongue were distributed over the surface of themass. A cone-shaped, somewhat friable, irregular-ly discolored mass of tissue was readily separatedfrom the surrounding cortex and white matter andwas removed. Little bleeding was encountered.
Right upper limb weakness was notedfollowing surgery but resolved completely by thesixth postoperative day. Except for frequentnosebleeds, his course was uncomplicated and hewas discharged on the thirteenth postoperativeday, continuing on dilantin, 100 mg t.i.d.,phenobarbital, 15 mg t.i.d., and ferrous sulfate.
After a period of convalescence he resumedhis usual activities and, according to his wife, tookhis medication regularly. On September 25th, sixmonths after discharge from the hospital, seizuresrecurred and the patient was brought to theBrookhaven Memorial Hospital by ambulance.Seizure activity was continuous in the right faceand upper extremity with repeated generalizedseizures supervening. Lumbar puncture revealedclear fluid containing six red blood cells per cubicmilliliter. Parenteral anticonvulsant medicationfailed to bring the seizures under control andrespiratory arrest ensued. Tracheostomy wasperformed and the patient was placed on a Birdrespirator. Intermittent seizure activity continuedand spontaneous respiratory activity failed toreturn. After 36 hours cardiac arrest occurred andthe patient was pronounced dead.
Stroke, Vol. 2, July-August 797?
by guest on June 5, 2018http://stroke.ahajournals.org/
Dow
nloaded from
THE BRAIN IN HHT
FIGURE 2
Left carotid angiogram, lateral view. Arrows outline branches of anterior cerebral arterysweeping around mass.
Pathological ExaminationSURGICAL SPECIMEN
Microscopic examination of the tissue removedat surgery revealed cerebral cortex and subcor-tical white matter showing marked neuronalloss, ischemic necrosis of the remainingneurons, and a proliferation of macrophages,capillaries and plump astrocytes. There werescattered fresh petechial hemorrhages. Occa-sional large-caliber (up to 1 mm) blood vesselswith thin, irregular fibrous walls were encoun-tered. The changes were interpreted as showingcerebral infarction in the subacute stage ofevolution and anomalous vessels suggesting thepresence of a vascular malformation.
POSTMORTEM EXAMINATION
A report of the general autopsy findings andthe intact brain were kindly supplied to thislaboratory by James S. Magidson, M.D.,
Stroke, Vol. 2, July-Augutf 1971
Pathologist, Brookhaven Memorial Hospital.Relevant findings outside the central nervoussystem were limited to capillary telangiectasiasof the tongue.
After fixation in formalin the brainweighed 1,380 gm. External examinationrevealed that the leptomeningeal vessels wereprominent and congested, especially over theleft hemisphere, but no abnormal vascularformations were present. The left cerebralhemisphere was swollen, and examination ofthe base of the brain showed evidence ofherniation of the left hippocampal gyms. Thesurgical defect, measuring 30 x 16 mm, wasnoted in the midportion of the left middlefrontal gyms.
Coronal sections through the cerebralhemispheres revealed the following abnormali-ties. The white matter of the left hemispherewas moderately and diffusely swollen. Much of
363
by guest on June 5, 2018http://stroke.ahajournals.org/
Dow
nloaded from

REAGAN, BLOOM
FIGURE 3
Coronal section of brain showing collections of large vessels in left superior and middletemporal gyri (arrows). White matter of superior temporal gyrus is discolored due todiffusion of blood pigment in edema fluid.
FIGURE 4
Coronal section through frontal lobes showing surgical defect in left middle frontal gyrus.A single large vein is present deep to defect (arrow).
the cortex of the left posterior frontal, superiortemporal, and occipital areas was softened andshowed dusky discoloration. The surgicaldefect in the left frontal lobe extended for a
364
depth of 30 mm and there was a scattering ofhemosiderin pigment in its walls. There werecollections of three to eight prominent bloodvessels, measuring up to 2 mm in luminal
Stroke, Vol. 2, July-Augutt 1971
by guest on June 5, 2018http://stroke.ahajournals.org/
Dow
nloaded from
THE BRAIN IN HHT
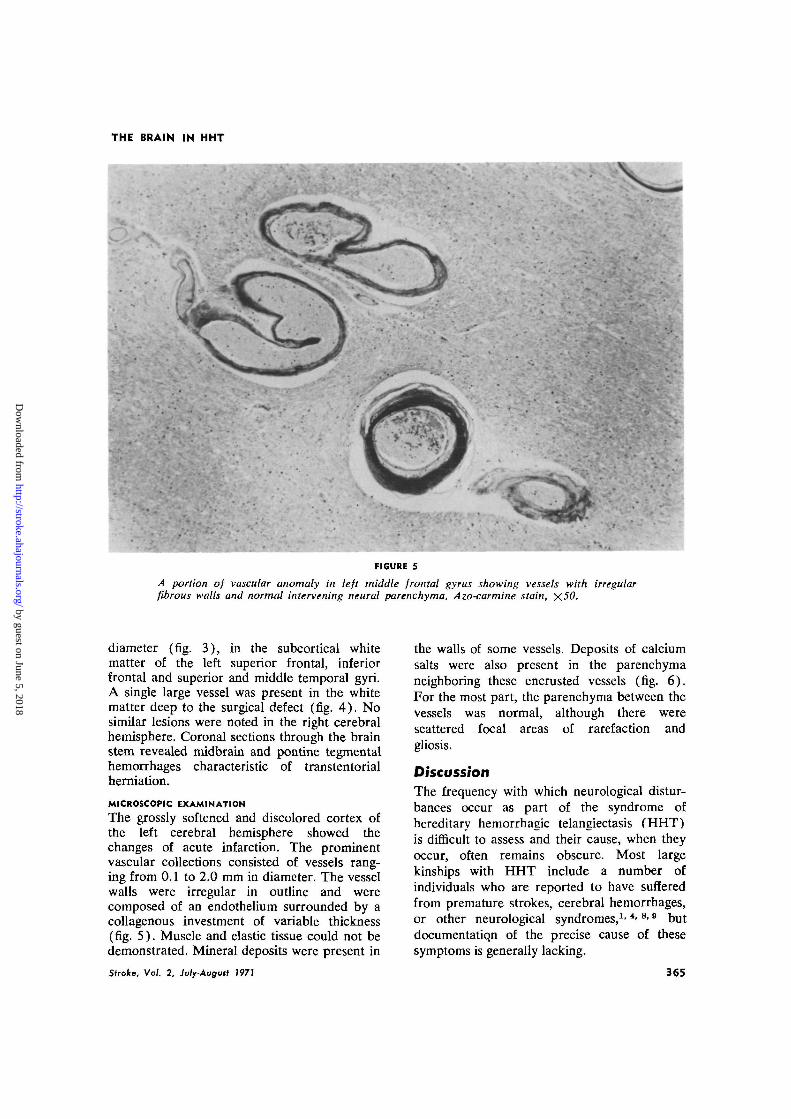
FIGURE 5
A portion of vascular anomaly in left middle frontal gyrus showing vessels with irregularfibrous walls and normal intervening neural parenchyma. Azo-carmine stain, X50.
diameter (fig. 3) , in the subcortical whitematter of the left superior frontal, inferiorfrontal and superior and middle temporal gyri.A single large vessel was present in the whitematter deep to the surgical defect (fig. 4 ) . Nosimilar lesions were noted in the right cerebralhemisphere. Coronal sections through the brainstem revealed midbrain and pontine tegmentalhemorrhages characteristic of transtentorialherniation.
MICROSCOPIC EXAMINATION
The grossly softened and discolored cortex ofthe left cerebral hemisphere showed thechanges of acute infarction. The prominentvascular collections consisted of vessels rang-ing from 0.1 to 2.0 mm in diameter. The vesselwalls were irregular in outline and werecomposed of an endothelium surrounded by acollagenous investment of variable thickness(fig. 5) . Muscle and elastic tissue could not bedemonstrated. Mineral deposits were present in
Stroke, Vol. 2, July-August 1971
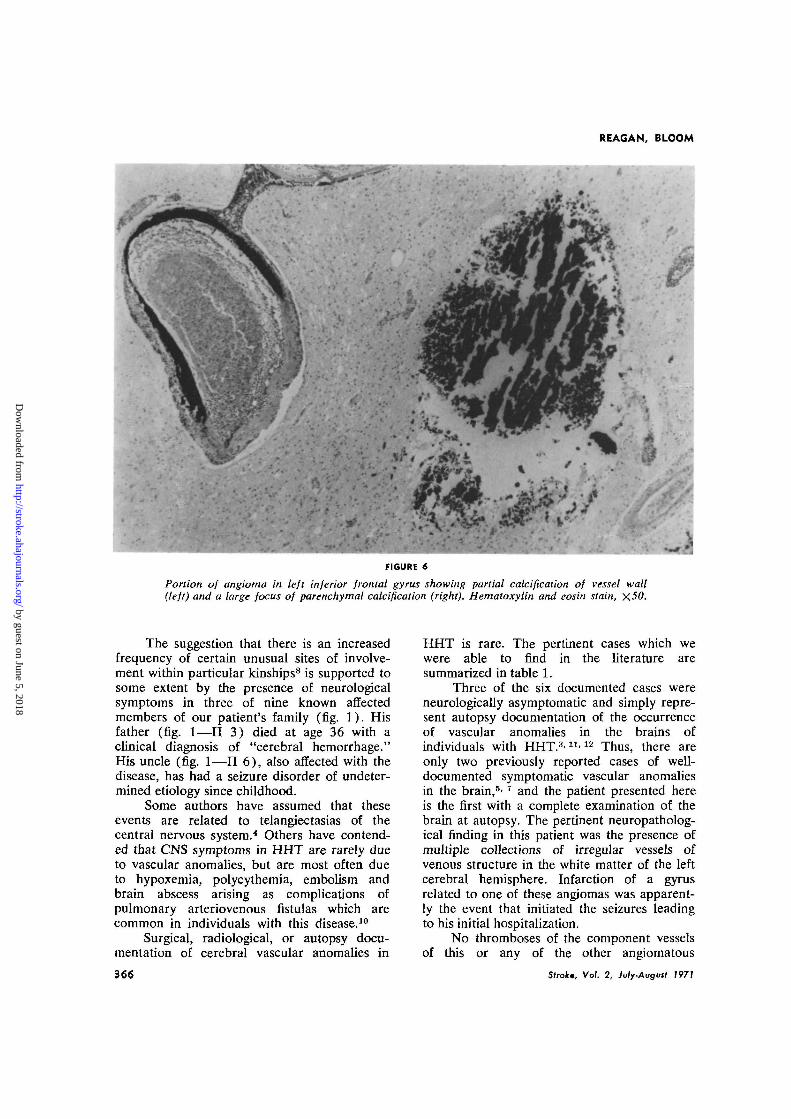
the walls of some vessels. Deposits of calciumsalts were also present in the parenchymaneighboring these encrusted vessels (fig. 6) .For the most part, the parenchyma between thevessels was normal, although there werescattered focal areas of rarefaction andgliosis.
DiscussionThe frequency with which neurological distur-bances occur as part of the syndrome ofhereditary hemorrhagic telangiectasis (HHT)is difficult to assess and their cause, when theyoccur, often remains obscure. Most largekinships with HHT include a number ofindividuals who are reported to have sufferedfrom premature strokes, cerebral hemorrhages,or other neurological syndromes,1' *• 8i 9 butdocumentatiqn of the precise cause of thesesymptoms is generally lacking.
365
by guest on June 5, 2018http://stroke.ahajournals.org/
Dow
nloaded from
REAGAN, BLOOM
FIGURE 6
Portion of angioma in left inferior frontal gyrus showing partial calcification of vessel wall(left) and a large focus of parenchymal calcification (right). Hematoxylin and eosin stain, X50.
The suggestion that there is an increasedfrequency of certain unusual sites of involve-ment within particular kinships8 is supported tosome extent by the presence of neurologicalsymptoms in three of nine known affectedmembers of our patient's family (fig. 1). Hisfather (fig. 1—II 3) died at age 36 with aclinical diagnosis of "cerebral hemorrhage."His uncle (fig. 1—II 6), also affected with thedisease, has had a seizure disorder of undeter-mined etiology since childhood.
Some authors have assumed that theseevents are related to telangiectasias of thecentral nervous system.4 Others have contend-ed that CNS symptoms in HHT are rarely dueto vascular anomalies, but are most often dueto hypoxemia, polycythemia, embolism andbrain abscess arising as complications ofpulmonary arteriovenous fistulas which arecommon in individuals with this disease.10
Surgical, radiological, or autopsy docu-mentation of cerebral vascular anomalies in
366
HHT is rare. The pertinent cases which wewere able to find in the literature aresummarized in table 1.
Three of the six documented cases wereneurologically asymptomatic and simply repre-sent autopsy documentation of the occurrenceof vascular anomalies in the brains ofindividuals with HHT."'11'12 Thus, there areonly two previously reported cases of well-documented symptomatic vascular anomaliesin the brain,5'7 and the patient presented hereis the first with a complete examination of thebrain at autopsy. The pertinent neuropatholog-ical finding in this patient was the presence ofmultiple collections of irregular vessels ofvenous structure in the white matter of the leftcerebral hemisphere. Infarction of a gyrusrelated to one of these angiomas was apparent-ly the event that initiated the seizures leadingto his initial hospitalization.
No thromboses of the component vesselsof this or any of the other angiomatous
Strok; Vol. 2, July-Augwt 1971
by guest on June 5, 2018http://stroke.ahajournals.org/
Dow
nloaded from

THE BRAIN IN HHT
TABLE 1
Pathologically Documented Cases of Cerebral Vascular Anomalies Associated With HHT
Cats
1
2
3
4
5
6
Author
Ytrehus12
Bird andJaques8
Zelman11
Chandler5
Quickel andWhaley7
Present case
PatientAg«,
54
68
56
?
17
45
M X
F
M
M
F
M
M
Documentation
Autopsy
Autopsy
Autopsy
Angiography,surgery
Angiography,surgery
Surgery,autopsy
Description ofmalformation
Dilated capillariesand veins
Thin-walled veins
Telangiectasis withthin fibrous walls
Arteriovenousmalformation
Capillary angioma
Venous angioma
Location
R. frontal
Widespread inwhite matter
Multiple
R. parietal
L. caudate
MultipleL cerebrum
Neurologicalsymptomi
None
None
None
Headaches,seizures
Subarachnoidhemorrhage
Seizures
collections were found. Hemodynamic altera-tions that led to shunting of arterial bloodaway from the involved gyrus might, therefore,be postulated. Degenerative changes such asdystrophic calcification, and focal rarefactionand gliosis which may have resulted from poortissue oxygenation, were found in relationshipto several of the vascular malformations. Ofconsiderable interest, in this regard, was acuteinfarction of large portions of the left cerebralhemisphere which occurred during his terminalepisode of status epilepticus. No vascularocclusions could be found, and we are forcedto postulate that the focal damage occurringduring a period of uniform systemic hypoxiawas due to focal hemodynamic alterationsrelated to the venous malformations.
The fundamental defect in HHT appearsto be a dysplasia of the walls of blood vesselsprimarily on the venous side of thecirculation.8' 1S This congenital weakness of thewall leads to the progressive dilatation andtortuosity of the involved vessels and accountsfor the progressive increase in the number andprominence of the mucocutaneous lesions withincreasing age. It appears that a similar processmay occur in almost any internal organ where,in addition to the capillary-venous ectasias,arterial ectasias and communications with thevenous lesions may open up, leading toarteriovenous shunting. In keeping with thisconcept, most lesions described in the brainhave consisted of ectatic vessels primarily ofvenous and capillary structure (table 1, cases1-3, 6) , with occasional development of
Stroka, Vol. 2, July-August I97J
arteriovenous communications (table 1, cases4 and 5) .
Small vascular malformations of the brainrarely cause clinical symptoms before acatastrophic hemorrhage occurs, and they have,therefore, been referred to as "cryptic."14-lr>
Purely venous anomalies are the rarest of thesecryptic malformations, and Wolf et al.lfi wereable to find only nine autopsy-proved examplesof bleeding from this sort of abnormality re-corded in the literature. None of those caseswere associated with HHT.
It appears that mechanisms other thanbleeding can cause these venous anomalies tobecome symptomatic. Ischemic necrosis oftissues related to venous anomalies has onlyoccasionally been mentioned in the literature.It is probably the mechanism whereby progres-sive spinal cord dysfunction occurs in at leastsome cases that have been designated the"Foix-Alajouanine syndrome,"16 and may wellbe the mechanism whereby progressive cere-bral degeneration occurs in relationship tothe predominantly leptomeningeal venousangiomas in the Sturge-Weber syndrome.17 Theanalogy of the Sturge-Weber syndrome isfurther amplified in our case by the fact thatthe abnormal venous collections were confinedto the left hemisphere, corresponding to thelateralization of an unusually dense accumula-tion of telangiectasias on the left forehead.
In an individual case, the differentialdiagnosis between infarction, hemorrhage, ab-scess, or some mass lesion unrelated to HHTmay be difficult. Cryptic venous angiomas are
367
by guest on June 5, 2018http://stroke.ahajournals.org/
Dow
nloaded from
REAGAN, BLOOM
rarely visualized as such on angiography18 andnonspecific displacement of vessels is a findingcommon to all the above conditions. Addition-al diagnostic methods may be required toresolve the problem including, in some cases,surgical exploration.
References1. Harrison DFN: Familial hemorrhagic telan-
giectasis. Quart J Med 23: 25-38, 19642. Borman JB, Schiller M: Osier's disease with
multiple large vessel aneurysms. Angiology20: 113-118, 1969
3. Bird RM, Jaques WE: Vascular lesion ofhereditary hemorrhagic telangiectasis. NewEng J Med 260: 597-599, 1959
4. Hodgson CH, Burchell HB, Good CA, et a l :Hereditary hemorrhagic telangiectasia andpulmonary arteriovenous fistula. New Eng JMed 261 : 625-636, 1959
5. Chandler D: Pulmonary and cerebral arterio-venous fistula with Osier's disease. Arch IntMed 116: 277-282, 1965
6. Sounders W H : Hereditary hemorrhagic telan-giectasis. Arch Otolaryng 76: 245-260, 1962
7. Quickel KE, Whaley RJ: Subarachnoid hem-orrhage in a patient with hereditary hemor-rhagic telangiectasia. Neurology 17: 716-719,1967
8. Landau J, Nelken E, Davis E: Hereditary
hemorrhagic telangiectasia (with retinal andconjunctival lesions). Lancet 2 : 230-231,1956
9. Walton JN: Subarachnoid hemorrhage ofunusual aetiology. Neurology 3: 517-543,1953
10. Dyer NH: Cerebral abscess in hereditaryhemorrhagic telangiectasia. J Neurol Neuro-surg Psychiat 30: 563-567, 1967
11. Zelman S: Liver fibrosis in hereditary hemor-rhagic telangiectasia. Arch Path 74: 66-72,1962
12. Ytrehus 0 : Hereditary hemorrhagic telangiec-tasis and cirrhosis of liver. Nord Med 38: 730-733 (Apr) 1948
13. Stefanini M, Dameshek W: The HemorrhagicDisorders. New York-London, Grune andStratton, 614 pp, 1962
14. Crawford JV, Russell DS: Cryptic arteriove-nous and venous hematomas of the brain. JNeurol Neurosurg Psychiat 19: 1-11, 1956
15. Wolf PA, Rosman NP, New PFJ: Multiplecryptic venous angiomas of the brain mimick-ing cerebral metastases. Neurology 17: 4 9 1 -501, 1967
16. Antoni N: Spinal vascular malformations (an-giomas) and myelomalacia. Neurology 12:795-804, 1962
17. Alexander GL, Norman RM: The Sturge-WeberSyndrome. Bristol, John Wright and Sons Ltd.,95 pp, 1960
368 Stroke, Vol. 2, July-August 1971
by guest on June 5, 2018http://stroke.ahajournals.org/
Dow
nloaded from
THOMAS J. REAGAN and WILLIAM H. BLOOMThe Brain in Hereditary Hemorrhagic Telangiectasia
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1971 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.2.4.361
1971;2:361-368Stroke.
http://stroke.ahajournals.org/content/2/4/361World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 5, 2018http://stroke.ahajournals.org/
Dow
nloaded from


















