
The Assessment of Capacity for Myoelectric Control638531/...Abstract Helen Lindner (2013): The...
92
The Assessment of Capacity for Myoelectric Control
Transcript of The Assessment of Capacity for Myoelectric Control638531/...Abstract Helen Lindner (2013): The...

The Assessment of Capacity for Myoelectric Control

To my parents

Örebro Studies in Care Sciences 48
HELEN LINDNER
The Assessment of Capacity for Myoelectric Control
Psychometric evidence and comparison with upper limb prosthetic outcome measures

© Helen Lindner, 2013
Title: The Assessment of Capacity for Myoelectric Control - psychometric evidence and comparison with upper limb prosthetic outcome measures
Publisher: Örebro University 2013
www.publications.oru.se
Print: Ineko, Kållered 09/2013
ISSN 1652-1153 ISBN 978-91-7668-963-9

Abstract Helen Lindner (2013): The Assessment of Capacity for Myoelectric Control - psychometric evidence and comparison with upper limb prosthetic outcome measures. Örebro Studies in Care Sciences 48. Evaluation of outcomes using validated prosthetic outcome measures (OMs) is a current priority in upper limb (UL) prosthetics, and OMs with psychometric evidence toward UL prosthesis users are thus necessary. The “Assessment of Capacity for Myoelectric Control” (ACMC) is a tool that assesses the ability to control a myoelectric prosthetic hand. Some psycho-metric aspects of the ACMC have been previously investigated, but others are still lacking. A major part of this thesis was thus to search and assess the psychometric evidence of the ACMC. Data were collected from pros-thesis users of different ages, prosthetic sides, and sexes. Rasch analysis was used to search for validity evidence and activity influence on the users’ ACMC ability measures, while reliability statistics was used to search for reliability evidence. Overall, the validity evidence was satisfactory in terms of unidimensionality, item technical quality, item difficulty, and relation to prosthetic wearing time. In terms of activity influence, the majority of pros-thesis users received similar ability measures in different activities. Reliabil-ity evidence was also satisfactory in terms of test-retest reliability and rater agreements (intra- and interrater).
Besides the ACMC, several other prosthetic OMs have been developed in recent years. A comparison of these OMs would help professionals to select appropriate tools for clinical practice. Thus, a comparison of the validated UL prosthetic OMs was performed with an emphasis on what health aspects they cover. Eight OMs were chosen, and their contents were linked to the “International Classification of Functioning, Disability and Health” (ICF). The results showed that the contents from different OMs were linked to the ICF categories in “Body functions,” “Activity and Par-ticipation,” and “Environmental Factors.”
In conclusion, the use of a mixture of OMs is recommended to cover dif-ferent aspects of health. Based on the evidence in this thesis, the ACMC can be recommended to measure the ability to control a myoelectric hand. Keywords: Capacity, Comparison, ICF, Myoelectric Control, Psychometric evidence, Upper limb prosthesis. Helen Lindner, School of Health and Medical Sciences Örebro University, SE-701 82 Örebro, Sweden, [email protected]


List of publications underlying this thesis
I Lindner HY, Linacre JM, Norling Hermansson L (2009) Assessment of Capacity for Myoelectric Control: evaluation of construct and rating scale. Journal of Rehabilitation Medicine, 41(6): 467–474
II Lindner HY, Eliasson AC, Norling Hermansson LM (2013) Influence of standardized activities on validity of Assessment of Capacity for Myoelectric Control. Journal of Rehabilitation Re-search and Development (in press)
III Lindner HY, Langius-Eklöf A, Norling Hermansson LM (2013) Test-retest reliability and rater agreements of the Assessment of Capacity for Myoelectric Control version 2.0. (submitted)
IV Lindner HY, Nätterlund BS, Norling Hermansson LM (2010) Upper limb prosthetic outcome measures: review and content com-parison based on International Classification of Functioning, Disa-bility and Health. Prosthetics and Orthotics International, June 34(2):109-28

List of abbreviations
AA Acquired amputation of upper limb ACMC Assessment of Capacity for Myoelectric Control CAA Center for Arm Amputees CAPP-FSI Child Amputee Prosthetics Project - Functional Status Inventory CAPP-PSI Child Amputee Prosthetics Project - Prosthetics Satisfaction Inven-
tory CTT Classical test theory DIF Differential item functioning ICC Intraclass coefficient ICF International Classification of Functioning, Disability and Health κ Kappa LDAPC Limb Deficiency and Arm Prosthesis Centre LOA Limits of agreement MDC Minimal detectable change MDC95 Minimal detectable change at 95% confidence level MCID Minimal Clinical Important Difference MFRM Many-Facets Rasch model MnSq Mean Square OMs Outcome Measures OPUS Orthotics and Prosthetics Users’ Survey OT Occupational therapist PA Percentage agreement PCA Principal components analysis P & O Prosthetics and Orthotics PUFI Prosthetic Upper Functional Index RSM Rating Scale Model SE Standard error SEM Standard error of measurement SIRS Skilled Index Rank Scale SSC State-of-the-Science Conference TAPES Trinity Amputation and Prosthesis Experiences Scales UBET Unilateral Below Elbow Test UL Upper limb ULRD Upper limb reduction deficiency UNB University of New Brunswick Test Zstd Z-standardized

Table of contents
PREFACE................................................................................................. 11
1 INTRODUCTION ........................................................................... 13 1.1 The Assessment of Capacity for Myoelectric Control ....................... 13 1.2 Individuals who use upper limb prosthesis ....................................... 14 1.3 A myoelectric prosthetic hand – how to control it? .......................... 16 1.4 Aspects related to capacity for myoelectric control ........................... 18 1.5 Prosthetic training – an occupational therapy perspective ................ 20 1.6 A tool is needed to assess capacity for myoelectric control ............... 21 1.7 The development of ACMC ............................................................. 22
1.7.1 ACMC – a Rasch-built measure ............................................... 25 1.7.2 Validity aspects of the ACMC .................................................. 27 1.7.3 Reliability aspects of the ACMC ............................................... 29
1.8 Measuring outcomes with validated prosthetic outcome measures ... 30 1.8.1 Content comparison using the ICF ........................................... 31
1.9 Rationale of the thesis ...................................................................... 32
2 AIM ................................................................................................. 34
3 MATERIALS AND METHODS ...................................................... 35 3.1 Study Design ..................................................................................... 35 3.2 Participants in studies I, II and III ..................................................... 35 3.3 Materials in Study IV ....................................................................... 36 3.4 Data collection procedures ............................................................... 37 3.5 Data analyses .................................................................................... 38
3.5.1 Study I ...................................................................................... 39 3.5.2 Study II ..................................................................................... 40 3.5.3 Study III .................................................................................... 41 3.5.4 Study IV .................................................................................... 42
4 ETHICAL CONSIDERATIONS ...................................................... 43
5 RESULTS ......................................................................................... 44 5.1 Content, response processes, internal structure evidence (Study I) .... 44
5.1.1 Technical quality of ACMC items ............................................ 44 5.1.2 Rating scale functioning............................................................ 44 5.1.3 Item difficulty hierarchy and targeting ...................................... 45 5.1.4 Unidimensionality and presence of DIF .................................... 45
5.2 From version 1.0 to version 2.0 ........................................................ 47 5.3 Relations to other variables & construct-irrelevant variance(StudyII)49
5.3.1 Relations to prosthetic wearing time & hand dominance ......... 49

5.3.2 Influence of standardized activities ........................................... 49 5.4 Evidence on test-retest reliability and rater agreement (Study III) ..... 50 5.5 Content comparison using ICF (Study IV) ........................................ 50
6 DISCUSSION ................................................................................... 53 6.1 General discussion ............................................................................ 53 6.2 Validity Evidence of the ACMC (Study I and II) .............................. 53 6.3 Influence of activities - construct-irrelevant variance (Study II) ........ 56 6.4 Reliability evidence of the ACMC (Study III) ................................... 56 6.5 Comparison of UL prosthetic outcome measures (Study IV) ............ 57 6.6 Methodological considerations ......................................................... 58
6.6.1 Study I, II and III ...................................................................... 58 6.6.2 Study IV .................................................................................... 61
6.7 Further research on the ACMC ........................................................ 62 6.8 Current status of the selected prosthetic outcome measures ............. 63 6.9 Clinical implications ......................................................................... 64
6.9.1 Clinical use of the ACMC ......................................................... 64 6.9.2 Selection of an appropriate outcome measure ........................... 65
7 CONCLUSION ............................................................................... 66
SUMMARY IN SWEDISH (SVENSK SAMMANFATTNING) ............... 67
ACKNOWLEDGEMENTS ...................................................................... 69
REFERENCES ......................................................................................... 71
ERRATA .................................................................................................. 85

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 11
Preface When I started working at the prosthetic clinic, I met an old friend who had not been fitted with prostheses when we first met. During a tea break in the clinic’s kitchen, this friend now used the prostheses to make drinks and sandwiches. I asked if this friend would get together with other friends in town, to which this individual responded, ‘…now I can go out with friends because I have my prostheses…I use them to pick up my coffee mug and sandwiches…I can eat comfortably now in public.’ This friend even said, ‘I want to show you what I can do now compared with the first time you met me’ (shared with permission). This conservation always stays in my mind. It encourages me because it tells me that prosthetic fitting can give a normal life back to a person. It motivates me when I plan prosthetic training for my clients, with a focus on helping them to gain success in controlling their prostheses step by step. During my clinical practice, I have found that instruments that assess how my clients control their prostheses are helpful because the assessment results can help me to plan my training. At our clinic, we use an assessment method, the Assess-ment of Capacity for Myoelectric Control (ACMC), to evaluate how our clients control their prostheses. From time to time, however, my colleagues and I would discuss questions concerning the assessment results, namely the ACMC ability measures. We discussed questions such as, ‘Will the clients obtain different ability measures when they perform different activities?’, ‘How consistent is the ACMC ability measure?’, and ‘How do we know that there is a change in the ability of a patient when we compare the current and previous ability measures?’ All of these questions are relevant for us as clini-cians when we interpret the ACMC ability measures. Previous psychometric validations of the ACMC were satisfactory, but further validations are needed to answer the above questions. Therefore, my primary goal in embarking on this thesis has been to answer the above questions. Furthermore, apart from the ACMC, are they any other prosthetic outcome measures that we can use to assess our patients, such as prosthesis use in daily life? What are the similarities and differences among different prosthetic out-come measures? How do we select an appropriate measure for the aim of a given evaluation? In response to these questions, a minor but important part of this thesis involved comparison of upper limb (UL) prosthetic outcome measures to identify their similarities and differences. My hope is that this part of the thesis will help us as clinicians to select appropriate measures for the aims of our evaluations.


HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 13
1 Introduction Individuals with upper limb reduction deficiency (ULRD) or acquired ampu-tation of upper limb (AA) are often fitted with UL prostheses to compensate for limb absence.1 The goal of prosthetic fitting is to provide users with the means to function optimally within their social and physical environment.2 If a myoelectric prosthesis is chosen, the user will learn to control the prosthesis with voluntary muscle contraction. Training is usually offered to help users achieve an adequate level of control so that they are able to use the prostheses effectively in their daily lives.3 To monitor their progress in controlling their prostheses, it is necessary to assess in a standardized manner how UL prosthe-sis users control their prostheses. In response to this demand, the Assessment of Capacity for Myoelectric Control (ACMC) has been developed.4
1.1 The Assessment of Capacity for Myoelectric Control The ACMC is an observational assessment developed to assess the ability of a prosthesis user to control a myoelectric prosthetic hand.4 Each item in the assessment is an observable prosthetic hand movement or an observable pros-thetic hand movement in relation to other body parts (see Results - ‘From version 1.0 to version 2.0’ for the item lists). The assessment session is often carried out during the user’s performance of a bimanual activity. It is de-signed for upper limb (UL) prosthesis users of different ages, prosthetic levels and sides. The ACMC assesses capacity for myoelectric control. Let’s take a look at the following definitions:
Definitions Capacity - an individual’s mental or physical ability.5 It also refers to what a person can do in a standardized environment.6 Myoelectric - ‘myo’ means muscle in Greek and ‘myoelectric’ refers to electrical activity produced by a contracted muscle.7 Control - the skill in the use of a tool.5
Merriam-Webster defines ‘capacity’ as mental or physical ability of an indi-vidual.5 Indeed, for many UL myoelectric prosthesis users, it takes a lot of mental and physical effort to achieve an adequate level of capacity for myoe-lectric control.8 The International classification of functioning, disability and health (ICF) describes ‘capacity’ as an individual ability to execute a task or

14 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
an action.9 ‘Capacity’ is what an individual with a health condition can do in a standardized environment6 and the ICF suggests that using standardized environment for assessments allows international comparisons of individuals.9 ‘Capacity’ can be measured with or without assistive device9 and both ways of measuring capacity has been used in prosthetics.10, 11 In the ACMC, an individual’s capacity for myoelectric control is assessed when an individual is wearing his/her UL prosthesis and the assessment is often taking place in a standardized environment, such as prosthetic clinic. Myoelectric signal is the signal generated during muscle contraction.7 In the ACMC context, a skillful myoelectric prosthesis user is one that is capable to control the prosthesis with appropriate muscle contraction. The capacity for myoelectric control does not come instantly when an individual puts on a prosthesis, rather, it may take a lot of mental and physical effort, especially during the first months after prosthetic fitting.8, 12 The challenges in control-ling a myoelectric prosthesis can be described in terms of a number of aspects related to the capacity for myoelectric control. However, to understand these aspects, it is important to have a basic understanding of the individuals who use UL prostheses and the control of a myoelectric prosthetic hand. There-fore, these topics are presented in the next few sections.
1.2 Individuals who use upper limb prosthesis
Individuals with congenital upper limb reduction deficiency Congenital limb deficiency is suggested to occur between the 3rd and 8th week of embryogenesis.13 It is relatively rare, with an estimated worldwide rate of 2 to 7 per 10,000 live births14 (upper and lower limbs) and 3.7 per 10,000 in Sweden (UL).15 An estimated 12% to 33% of limb deficiencies are associated with other major congenital anomalies or genetic disorders,14 while the remaining limb deficiencies occur as isolated limb defects. Children with isolated limb defects of the UL often develop normally, and they can perform most age-appropriate activities, although the activities may be performed in an atypical manner such as with the help of chin, mouth, or elbow.16, 17 Pa-tients with unilateral below-elbow deficiency constitute the largest group that benefits most from myoelectric prosthetic fitting.18 They often have a healthy, intact UL on the nondeficient side and a functional shoulder and elbow on the deficient side.19 Prosthetic rehabilitation for children with ULRD emphasizes the development of the child.20 The prosthetic socket is changed regularly to accommodate residual limb growth, and the prosthetic hand size is chosen to match the

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 15
intact hand size. The activities used for training are age-appropriate.3 Pros-thetic fitting at an early age is recommended because it encourages motor learning and prosthesis integration into the body scheme.21 It has been sug-gested that prosthetic fitting promotes overall symmetry of development.22, 23 The type of prosthesis prescribed to the child is dependent on the child’s cog-nitive ability, attempt to hold objects manually, and attention span for train-ing.24 In Sweden, children are usually fitted with cosmetic prostheses before they have achieved sitting balance and are fitted with myoelectric prostheses between 2.5 and 4 years of age.25 Researchers have explored phantom sensa-tion in persons with ULRD,26, 27 but whether these individuals have an innate dominant side remains unknown. From clinical experience, those with right-sided ULRD are often more spontaneous in using their prostheses than are those with left-sided ULRD.
Individuals with acquired upper limb amputation Amputation refers to the surgical or spontaneous partial or complete removal of a limb or projecting body part covered by skin.28 Work-related injuries and traffic accidents are the two major causes of amputation.14, 29 In the last dec-ade, an increasing number of amputees have lost their limbs as a result of war.30 Therefore, it is difficult to precisely determine the incidence rate of AA, but in general, Scandinavia has a lower incidence rate than do other coun-tries.14 In Sweden, one study estimated a hand/forearm amputation incidence rate of 3.3 males/0.5 females per 100,000 persons.31 Another Swedish study estimated a rate of 5.21 per 100,000 persons for all types of amputations; 62% of them occurred at working age, and 16% of amputees were less than 20 years old.32 Individuals with unilateral below-elbow amputation constitute the largest amputated group fitted with UL prostheses.33-35 Amputation surgery is per-formed to preserve the length and muscle balance of the residual limb for prosthetic fitting.35 Prosthetic fitting should start as soon there is no open wound because early fitting may be positively related to prosthetic ac-ceptance.17 Pain management is offered because many amputees experience different types of pain, such as phantom limb pain.36, 37 It was recently found that strong phantom limb pain is associated with decreased prosthesis use.38 In brief, prosthetic fitting for both groups (ULRD and AA) is a highly indi-vidual process. The patients are informed about different prosthetic options, such as cosmetic, body-powered, hybrid, and myoelectric-controlled prosthe-ses,39 because different prostheses have different strengths and limitations. Myoelectric control is the most commonly used control in commercial pros-

16 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
thetic hands.40 Although the media occasionally report ‘bionic’ hands that are controlled directly by the human mind, most currently used myoelectric pros-theses are controlled by voluntary muscle contractions that require a lot of practice and training.
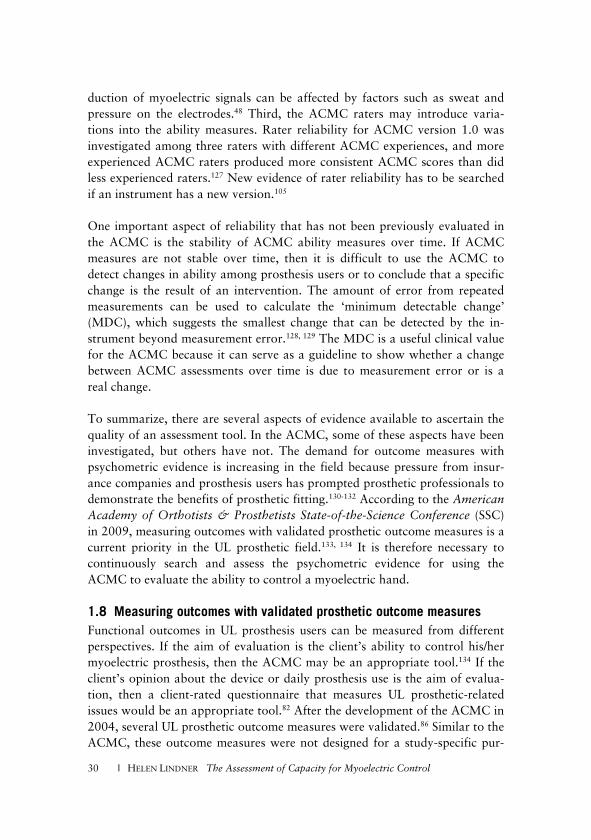
1.3 A myoelectric prosthetic hand – how to control it? Myoelectric prosthetic hands are controlled with voluntary muscle contrac-tion. Myoelectric signals generated during muscle contractions are detected by surface electrodes embedded in the prosthetic socket (Fig. 1, left). The signals are then amplified and sent to the appropriate prosthetic component to gen-erate the desired movement.41
Fig.1. left – two surface electrodes embedded inside a prosthetic socket; right – myoelectric signal examination (this image - courtesy from Advanced Arm Dynamics)
Surface electrodes are often placed over antagonistic muscles of a residual limb or muscles that can be voluntarily contracted in an isolated manner.12, 42 The best muscle sites for surface electrodes are selected during socket fabrica-tion (Fig. 1 right). A well-fitted socket, optimal muscle sites, good myoelectric signals, and good skin contact with surface electrodes are essential for the user to control a myoelectric prosthesis.42, 43
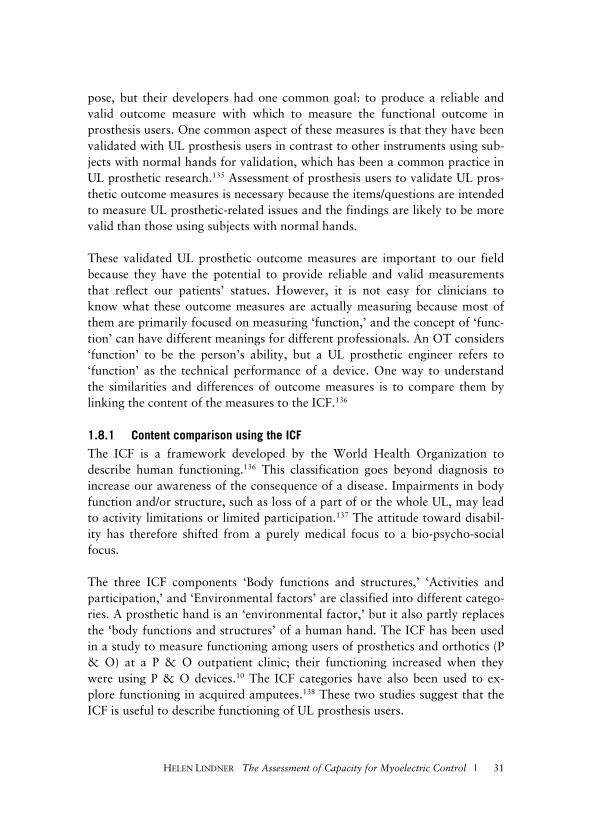
Fig.2. left – a below-elbow prosthesis; middle – an Otto Bock VariPlus Speed Hand for adults; right – an Otto Bock 2000 myoelectric prosthetic hand for children (cour-tesy from Otto Bock)

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 17
In a typical below-elbow (transradial) prosthesis with two surface electrodes (Fig. 1 left, Fig. 2 left), the hand opens when the surface electrode over fore-arm extensors picks up myoelectric signals that exceed the electrode thresh-old. Conversely, the hand closes when the surface electrode over forearm flexors picks up myoelectric signals that exceed the threshold. Different con-trol formats are offered in prosthetic hands, and one of them is an on/off format in which the hand speed is constant during both opening and closing.44 The on/off format is a common format for children’s prosthetic hands. Adult myoelectric hands offer several control formats. One common format is ‘proportional control,’ in which the hand speed and closing force are proportional to the amount of muscle contraction given by the user.45 Although commercial multifunctional hands with articulating fingers have been available since 2007, the majority of myoelectric prosthesis users are fitted with a prosthetic hand in which the motor drives the index and middle fingers synchronously with the thumb.46 The last two fingers are not articu-lated, but serve as support during grasping (Fig. 2 right). The thumb lines up with the tips of the two fingers (Fig. 2 middle), and the hand can thus per-form two grips: a cylindrical grip and a tripod pinch (Fig. 3 left, middle). Prosthetic hands come in different sizes and with different opening widths and grip forces that match the user’s growth.47
Fig.3. left –cylindrical grip (courtesy from Advanced Arm Dynamics); middle – tripod pinch (courtesy from Otto Bock); right – holding toothpaste (with permission)
Controlling a myoelectric prosthesis is different from controlling a human UL. One obvious reason is that the arm muscles were originally developed for physiological functions other than controlling a myoelectric prosthesis.48 The first challenge for novice users is to isolate muscle contraction.12, 49 Users must learn to contract one muscle site while relaxing the other muscles of the re-sidual limb. When the users try too hard, they co-contract the muscles used for opening and closing; hence, the hand will neither open nor close. The users may produce unwanted muscle contraction, which causes unintended movement.49 For example, the user may accidentally activate the ‘opening’

18 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
muscle and open the prosthetic hand when holding a cup (Fig. 3, left), which may cause the user to drop the cup. Alternatively, the user may produce too much muscle contraction during closing, such as grasping a toothpaste tube (Fig. 3 right), unintentionally squeezing out the toothpaste. When holding objects, the user must relax the arm muscles so that myoelectric signals are maintained below the electrode thresholds.
1.4 Aspects related to capacity for myoelectric control Compared with the number of studies on prosthetic components, literature on learning to control a myoelectric prosthetic hand is sparse. Some publications have an occupational therapy perspective,3, 42, 50-55 focusing on training from basic control to use training. A few articles have evaluated the effects of train-ing.56-58 A kinesiology team used motor learning to describe prosthetic move-ment.59-63 In addition, a movement science team recently used motor learning to understand skill acquisition in prosthesis users.48, 64-68 Different challenges related to capacity for myoelectric control can be found from these studies, and they can be summarized according to six different aspects.
(1) The need of external support Prosthesis users often have difficulty opening and closing the hand in space because of the weight of the prosthesis.51, 56, 58 The sudden increase in weight at the residual limb induces unintended muscle activity that interferes with the intended muscle activity,48, 60, 69 and the hand thus opens or closes involuntari-ly. Unintended muscle activity often disappears immediately when the user loads the prosthetic weight on a table or solid support.51 Novice prosthesis users must overcome this challenge because many activities require the users to perform reaching movements in space.53, 66 One way to overcome this is to acclimate the residual limb to the prosthetic weight by wearing the prosthesis on a daily basis. The interference from unintended muscle activity will gradu-ally diminish.51
(2) Grip force and opening width Another challenge for prosthesis users is accurate application of an appropri-ate prosthetic grip force during grasping.3, 61, 68 Novice users often produce too much contraction, and the object either slips out of the hand or is crushed by the hand. They must learn to regulate the grip force with an appropriate amount of contraction (in proportional control) or with an appropriate dura-tion of closing (in on/off control).45, 70 Another challenge for prosthesis users is the difficulty adjusting the opening width when releasing objects. Many users find it challenging to perceive the magnitude of hand opening.48

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 19
(3) Coordination of both hands It takes some practice for prosthesis users to coordinate the movements of the prosthetic hand and intact hand. The speed of a myoelectric prosthetic hand is determined by two features: (i) the time window during which the myoelec-tric signals must exceed the electrode threshold,48, 71 and (ii) the hand speed designed by the manufacturer. The speed of a prosthetic hand is obviously slower than that of a human hand50, 61; however, a user who is familiar with the speed of his/her own prosthetic hand can skillfully coordinate the hands, as demonstrated by the ability to remove the cap from a pen. The user begins to contract the ‘closing’ muscle early enough so that both hands can grasp objects in a coordinated manner.
(4) Different positions and in motion (timing) Another challenge is the use of a prosthetic hand in different positions. This may be difficult because when the arm is in different positions, unintended muscle activity may be produced, resulting in involuntary opening or closing.58, 72, 73 Another challenge is use of the hand with good timing when the hand or arm is in motion.66, 67 This ability can be observed when the user is passing objects between the hands or passing an object directly with the prosthetic hand to another person. The object may get stuck in the prosthetic hand if the user does not release the object quickly enough. In a similar way, it takes some practice to hold objects securely when the arm is in motion (Fig.4 left) because unintended muscle activity may activate the opening elec-trode and cause the object to be dropped.
Fig.4. Left – Holding object when the arm is in motion; middle, right – not looking at the prosthetic hand when holding objects (courtesy from Otto Bock)
(5) Repetitive grasp and release Switching quickly between opening and closing is a challenging movement.3, 51 This is an advanced skill of myoelectric control because the user must con-tract the pair of muscles in a swift manner. Repetitive grasping and releasing is useful for object manipulation, such as altering the object position. Prosthe-

20 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
sis users who are not capable of repetitively grasping and releasing objects often change the object positions with compensatory movements such as shoulder abduction and trunk deviation. It has been suggested that long-term performance of compensatory movements may cause shoulder pain.74, 75 Re-searchers have suggested that some compensatory movements can be avoided with certain prosthetic movements,75 such as repetitive grasping and releasing.
(6) The need of visual feedback Sensory feedback is an essential component for accurate dexterous actions.48,
54, 60 A myoelectric prosthesis does not provide direct sensory feedback; there-fore, the user cannot feel whether the hand is opened or closed or whether the object is being held securely. Many users find it challenging to perceive the magnitude of hand opening/closing or the strength of the grip force exerted on an object without direct feedback.48, 50, 60, 61 They often look at the hand during the operation68, and great concentration is needed.50 However, very experienced users reportedly do not look at the prosthetic hand during grasp-ing.68 Some users have claimed that they hear the hum of the motor76 or feel the motor vibration during muscle contraction.77 Sörbye reported a young blindfolded patient who grasped an object with her prosthesis without acous-tic feedback.78 Experienced users may be able to perceive vibration changes during the grasping and holding of objects, thus not requiring visual feedback (Fig.4 middle, right). The need for less visual feedback is an advanced level of myoelectric control that enables the user to use the device efficiently. In summary, the above six aspects are challenges that prosthesis users will experience while learning to control their prostheses. One study reported that younger children learn more quickly than older children do,52 and another study on adults suggested that different users may have different learning capacities.65 To evaluate the client’s progress in controlling the prosthetic hand, a reliable and valid instrument that evaluates the ability to control a myoelectric prosthetic hand is thus needed.
1.5 Prosthetic training – an occupational therapy perspective From an occupational therapy perspective, the ultimate goal of prosthetic training is to help the user to integrate the prosthesis into his/her daily life and achieve independence.42, 53 Prosthetic training often starts with control train-ing.3 The first step of control training is to help the user to discover how to open and close a prosthetic hand. For example, when the user extends the forearm to reach for an object, the hand grip opens because the extensors activate the ‘opening’ electrode. The training focuses on grasping and releas-ing objects of varying sizes, shapes, textures, and weights.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 21
When a prosthesis user has achieved basic control of his/her prosthesis, the training can shift to use training. Use training focuses on refinement and use of the prosthesis.3 Purposeful activities, such as playing with toys and every-day activities, are always used as tools in use training.42, 51, 52 The use of activi-ties during training not only enhances immediate performance, but promotes the learning of a prosthetic skill.54, 79 For example, during meal preparation, the user practices grasping different delicate food products with ‘appropriate grip force’ or practices using the prosthesis ‘in different positions’ when grasping bowls and plates from different shelves. During use training, the prosthetic hand is often used to stabilize objects while using the intact hand to manipulate objects during the activity.52 The occupational therapist (OT) also regularly identifies the user’s goals. For example, children may be preparing for school activities, whereas adults may aim to achieve self-dressing. Once the goals are identified, the OT provides training for the activities. Further-more, to help the users build habits of integrating the prosthesis into their daily lives,24 they are encouraged to wear their prostheses on a daily basis.51 Smurr53 uses the term ‘advanced prosthetic training’ to describe a more ad-vanced level of training. The idea is to teach the user the most efficient ap-proach to complete an activity using the prosthesis without causing too much stress or awkward body movements. The training goal is to help the user to incorporate the prosthesis efficiently and demonstrate a natural motor pat-tern. The length of prosthetic training depends on different factors, such as the complexity of the prosthetic components, learning capacity of the user, motivation, and family support.3, 53, 65
1.6 A tool is needed to assess capacity for myoelectric control Prosthetic training can be frustrating at times, especially during the first few months of training. The muscles may not contract as the user intends. The hand may open when the arm is moving. Failure to control the prosthesis may lead the patient to eventually stop using the prosthesis. It is therefore very important for the OT to monitor the user’s progress in controlling the pros-thesis because it helps the OT to adjust the training pace and direction and, most important, to help the prosthesis users achieve success with the right level and amount of training step by step. One way to monitor the user’s progress is to use an assessment tool that is able to capture different aspects related to the capacity for myoelectric control, because the assessment result can identify in which aspect the users need more training. Although monitor-ing the user’s progress is important, prosthetic clinics reportedly do not use any standardized assessment tests, but rely on their own tests in follow-up evaluations.24 One problem with clinic-owned tests is that the efficacy of

22 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
training cannot be compared among prosthetic services.80 Some clinics use human hand function tests to evaluate prosthetic function, but it has been suggested that hand function tests may not provide valid results because they do not address prosthetic-related issues and many compensatory movements may occur during the tests.81, 82 Although a variety of outcome measures have been used to measure outcomes among UL prosthesis users,83 none of those developed before the ACMC were designed to assess different aspects related to capacity for myoelectric control. In response to this demand, the ACMC was developed in 2000 and its first validation was published in 2004.4
1.7 The development of ACMC
The beginning of ACMC Just more than two decades ago, the Skills Index Ranking Scale (SIRS), a stepwise description of movement quality in myoelectric control, was devel-oped.51 This scale contains a series of steps that describe different ability levels in myoelectric control. However, one problem associated with the SIRS is that the differences in ability steps are unknown; thus, it cannot be used as an evaluation tool. However, the steps in the SIRS were selected to be the items in the ACMC. After two pilot trials and expert selection,15 extra items were added to ACMC, resulting in the ACMC version 1.0.
ACMC version 1.0 The ACMC version 1.0 comprises 30 items that assess 6 aspects related to the capacity for myoelectric control.4 (see also Results - ‘From version 1.0 to version 2.0’ for item list). The need for external support - 8 items Grip force and opening width - 3 items Coordination of both hands - 2 items In different positions and in motion (timing) - 8 items Repetitive grip and release - 2 items The need for visual feedback - 7 items Each item has a definition that guides the raters in identification of the movements.84 Items that assess ‘the need for external support’ are easily per-formed by users who can position their hands in space. Items that assess visu-al feedback are generally difficult for prosthesis users. The ACMC items are therefore not only different in terms of movement, but also in terms of diffi-culty.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 23
A 4-point rating scale (version 1.0) is used to rate the items. Category ‘0 - not capable’ is assigned when the user cannot or does not perform the item. Cate-gory ‘1 - sometimes capable’ is assigned when physical or verbal guidance from the OT is needed. Category ‘2 - capable on request’ is assigned if the user only performs the item when the rater asks the user to perform it. Cate-gory ‘3 - spontaneous and skillful control’ is given when the user performs the item spontaneously and skillfully. Because the activities are user-chosen dur-ing ACMC assessments, it is possible that one or two ACMC items are not required in the activities. For example, the item ‘holding without crushing’ will not be performed if no delicate object is involved in the activity. The item will then be rated as ‘missing.’
An ACMC assessment An ACMC assessment is administered by raters who have taken the training course.85 It can be carried out as soon as the user can open and close the pros-thetic hand. The prosthesis user is encouraged to choose an activity, and the ACMC rater assesses how the user controls his/her prosthetic hand during activity performance. For example, if the client chooses to set a table for af-ternoon tea, the activity steps are screw off a bottle cap, take things from the fridge, or place a tablecloth onto the table etc.
Fig.5. left: repetitive grasp and release – screw off the cap; middle: grasping objects at shoulder position; right: the timing in releasing objects (with permission)
During performance of the activity steps, the rater observes the six above-described aspects, such as how capable the user repetitively grasps and releas-es objects (Fig. 5, left), how well the user controls the prosthetic hand in dif-ferent positions (Fig.5, middle), and the timing of releasing objects (Fig.5, right). The rater scores the items and enters the ratings into the ACMC web-site,85 where the built-in Rasch model software calibrates an ACMC ability measure for the user (see ‘ACMC – a Rasch-built measure’ for Rasch analy-sis). Each ACMC assessment evaluates only one prosthetic hand; therefore, a bilateral user with two myoelectric hands can have two ACMC assessments (based on one activity performance) and obtain two ability measures.

24 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
Activities for ACMC assessment An ACMC assessment is often carried out during the client’s performance of a self-chosen activity. This means that the activity is selected according to the development and interest of the user.86 During the assessment, the user is encouraged to perform the activity in his/her usual way. The prosthetic hand is usually used to hold objects, while the intact hand is used to manipulate objects (Fig. 6 left).55, 57, 87 For unilateral users, the prosthetic hand is always used as the nonpreferred or nondominant hand, regardless of the side of dom-inance before amputation.57, 88, 89 Therefore, an ACMC assessment is per-formed to determine how the prosthetic hand is being used as an assistive device.
Fig.6. Left - holds apple with the prosthetic hand while the intact hand cuts it, Mid-dle– passive prosthesis use(courtesy from Otto Bock), Right – active prosthesis use (courtesy from Advanced Arm Dynamics)
Although the activity is chosen by prosthesis users, ACMC raters must con-sider two practical issues regarding activity objects. First, the activity objects must cause the hand to open. This means that the objects must be small enough to loosely fit inside the grip of the prosthetic hand. Adult prosthetic hands have large opening widths, but pediatric prosthetic hands have small opening widths (e.g. 33mm to 56mm for Otto Bock children 2000) and, the thumbs do not have an adduction function. Objects that are too large for the prosthetic hand will lead to passive prosthesis use (Fig. 6 middle). Since the ACMC assesses active prosthesis use, activities involving small objects or small handles are appropriate for ACMC assessment (Fig. 6 right). Further-more, small children can tolerate very little loading in their hands, and the objects must therefore be light. Second, the objects must be placed at different heights and in different locations to stimulate the user to stretch out the pros-thetic side in different positions. Accordingly, the activity must be able to stimulate the user to change prosthetic hand functions and UL movement so that the user’s ability to control his/her prosthesis can be assessed.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 25
1.7.1 ACMC – a Rasch-built measure The first validation of ACMC version 1.0 was carried out using Rasch analy-sis.4 Rasch analysis is an alternative to Classical Test Theory (CTT) for psy-chometric development of an instrument.90 With CTT, rank-ordered data are often summed to give a total score but it cannot be assumed that rank-ordered categories define equal intervals along the underlying construct.91 In Rasch analysis, rank-ordered categorical data are converted into interval logit measures and a change from 1 to 2 logits is the same as the change from 2 to 3 logits.92, 93 One useful function of Rasch analysis is that it orders items in terms of difficulty along an equal-interval unidimensional underlying con-struct. The sample of patients are also located along the same underlying construct which allows the developer to investigate whether the instrument has items to measure low, moderate and high levels of the underlying con-struct.90 This is important for the ACMC because the ACMC is expected to encompass the wide range of abilities encountered in clinical practice. Anoth-er useful function of Rasch analysis is the analysis of rating scale.91, 94, 95 A rating scale with rating categories that are confusing for its users, such as too wide or too narrow, would lead to inaccurate ratings.95 There is a family of Rasch models, such as ‘Rating Scale Model’ (RSM) and ‘Many-Facets Rasch Model’ (MFRM), available for different types of analyses. Although there are different Rasch models, the basic principle of Rasch model is that a person’s response to an item depends on the difference between the person’s ability and the item’s difficulty on a hypothetical underlying con-struct.96 Instead of using summed raw scores to represent a person’s ability directly, Rasch analysis converts raw scores into odds (which for dichoto-mous data is the probability of success on an item over the probability of failure on the item, and for rating scale data, odds are also used but the alge-braic expression is more complex). The natural logarithm of the odds con-verted from a person’s raw score gives a linear measure in logits (log-odds unit)92 that represents the person’s ability.97 An item’s difficulty is also esti-mated from its odds but now on the probability of failure over the probability of success. Both items and persons have the same logit units and therefore they can be placed side by side along a common logit scale (often displayed as a vertical scale), which visualizes the ability range of a group of persons and the diffi-culty range of a set of items (Fig. 7). In Fig. 7, the items are located along the logit scale according to their difficulty (commonly known as item difficulty hierarchy) and the persons are located along the logic scale according to their ability. Ideally, the item difficulty range and the person ability range should

26 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
target well on each other (so-called targeting) and their mean logits should be close to each other98 because this suggests that the set of items are appropriate to measure the ability of the sample99.
Fig.7. An illustrative example to show item difficulty hierarchy and targeting (each represents one person in a sam-ple and each item represents one item in an instrument)
The Rasch model constructs unidimensional linear measures from the data. The fit of the data to the model can be evaluated by comparing the observa-tions in the data with their Rasch expectations: ‘For person measure, a more able person must always have a better chance of success on an item than a less abled person. For item measure, any person must have a better chance of success on an easy item than on a more difficult item.91, 100 The Rasch model provides fit statistics for items and persons to determine how well the data fit this expectation.96, 101 If the item fit statistics are within an acceptable range, then the items contribute to a unidimensional construct96 or have good technical qualities.102 Depending on the type of outcome measures, different acceptable ranges for fit statistics have been suggested; for example, a wider range is suggested for clinical observational data than for survey data.103 In the first validation of ACMC version 1.0,4 item fit statistics were used to indicate unidimensionality, and fit statistics for all items met the model expec-tation of unidimensionality. Person fit statistics (96.2% of the sample) were also within the acceptable range, and the items targeted well at the ability of the sample. Instrument validation is an ongoing process, and the thesis con-tinued this process in terms of evaluating the validity and reliability evidence of the ACMC.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 27
1.7.2 Validity aspects of the ACMC In 1999, the Standards endorsed Messick’s view on validity104 and redefined validity as the degree to which evidence and theory support the interpretation of test scores entailed by proposed uses of tests.105 Messick emphasizes that validity is not a property of a test, but is the meaning of test scores for its proposed use.104 Instead of different types of validity, validity is viewed as a unitary concept that is established by accumulating evidence from different sources.104, 105 The Standards outlines five sources of evidence to guide devel-opers in the conduction of validation studies: test content, response processes, internal structure, relations to other variables, and the consequence of a test.105 The process of instrument validation therefore entails accumulation of evidence to provide a sound empirical foundation for the proposed interpreta-tion of test scores.106 This thesis continues this validation process of ACMC by conducting studies to search for evidence from the following sources:
Evidence based on content evidence According to Messick, content evidence includes content relevance, content representativeness, and technical quality.104 Different approaches have been suggested to collect content evidence, such as expert judgment on contents or the conduction of small pilot trials.105-107 In the beginning of the ACMC de-velopment, expert judgment and two pilot trials were used to select suitable items.15 The Rasch approach has been suggested to address content represent-ativeness by using item strata (statistically distinct regions of item difficulty that the persons have distinguished).108 The first ACMC validation shows that the prosthesis users separated ACMC items into 16 item strata,4 which is considered as excellent.109 Further content evidence is the technical quality of an item, for which Messick refers to technical quality as the ‘…unambiguous phrasing’ of items/questions.110 Rasch item fit statistics has been suggested to examine the technical quality of items102 because the misfit of an item (fit statistics outside the acceptable range) reflects the extent to which a signifi-cant portion of the sample responds inconsistently to that item.98 Item fit statistics can also identify redundant items that do not contribute much in-formation to the test score. An item with fit statistics that is above the ac-ceptable range should be investigated with further analyses because the item may contribute data that threaten the validity of the test score.103
Evidence based on response processes This source of evidence refers to the fit between the construct and the detailed nature of performance or responses actually engaged in by individuals.105 According to Messick, this evidence answers the question, ‘How well do the response processes demonstrate the construct?’104 Rasch approach has been

28 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
suggested to address this source of evidence using rating scale analysis, item difficulty hierarchy and person fit statistics.102, 108, 111 Person fit statistics was demonstrated earlier in the first validation of ACMC.4 A rating scale with rating categories that are confusing for its users, such
as too wide or too narrow, would lead to inaccurate ratings.95 The analy-sis of rating scale functioning enable us to examine how the rating scale categories function in relation to the underlying construct.102, 112 For ex-ample, a rating scale category with a narrow definition would occupy a narrow range along the construct.
The item difficulty hierarchy orders items from easiest to most difficult along the hierarchy. The responses to the items are used to estimate item difficulty; therefore, the ordering of item difficulty provides important ev-idence on how the ability of prosthesis users demonstrates the construct. Furthermore, the targeting of this hierarchy on the abilities of prosthesis users also provides evidence for this response process.
Evidence based on internal structure This source of evidence concerns the degree to which the relationships among test items conform to the construct on which the proposed test score interpre-tations are based.105 Validation examples are unidimensionality and differen-tial item functioning (DIF).105, 106, 113 Unidimensionality concerns whether all items measure one or more than
one attribute.93 If the items measure more than one attribute, then it is difficult for clinicians to distinguish which attribute the test score is pre-senting. Unidimensionality was previously demonstrated in the ACMC using item fit statistics.4 However, as suggested by later methodological studies,114, 115 item fit statistics should be supplement with other methods such as ‘principal components analysis’(PCA) to investigate unidimen-sionality.
DIF occurs in an item when two groups of persons with same ability have different chances to perform the item successfully for reasons unrelated to the construct being measured. The existence of DIF may suggest a flaw in the internal structure.116 If DIF exists in one or several items, the next question would be, ‘To what extent does the DIF affect the item location along the item difficulty hierarchy?’ In reality, it is not unusual for items with similar difficulty measures to swap locations along the item difficul-ty hierarchy. However, further analyses or actions must be taken if the DIF makes an easy item become difficult (or vice versa) for a certain per-son characteristic.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 29
Evidence based on relations to other variables This evidence concerns the relationship of test scores to variables external to the test.105 Validation examples are the correlation with other known varia-bles/instruments and known-group comparisons from widely used variables in the field.106, 117 The variable ‘prosthetic wearing time’ is a widely used variable that indicates prosthetic acceptance or daily prosthesis use.19, 45, 88, 118-121 Wear-ing the prosthesis on a daily basis helps the user to adjust to the prosthetic weight and provides the opportunity to use the prosthesis in different daily activities. Therefore, there is a possibility that ACMC ability measures would be higher in full-time users than non-full-time users. Another external variable is hand dominance. Hand dominance has been used as a variable that indi-cates prosthesis use,118, 119, 122 and dominant-sided users have been shown to have higher abilities than non-dominant-sided users.123
Construct-irrelevant variance While searching for evidence, Messick states that it is important to examine threats to test score validity.104 One threat is construct-irrelevant variance, which refers to the degree to which the scores are affected by processes that are extraneous to its intended construct.105 Construct-irrelevant variance is always present to some extent,124 and the question is how much the extent affects the test scores. In the ACMC, construct-irrelevant variance could arise from client-chosen activities. Although the purpose of using activities in ACMC assessment is to stimulate the users to change hand functions so their ability can be assessed, it is unknown how much the activities affect user abil-ity measures. One way to investigate this is to ask prosthesis users to perform different activities on one occasion and examine whether different activities give different ability measures. Furthermore, it is necessary to examine whether different activities favor a particular sex or prosthetic side.
1.7.3 Reliability aspects of the ACMC Reliability refers to the consistency of such measurement when a testing pro-cedure is repeated on a population of individuals or groups.105 Inconsistent assessment scores are difficult to interpret and therefore reduce validity evi-dence.125 Similar to validity, reliability is not viewed as a property of a test, but an interaction among the instrument, sample, and situation.126 Reliability of the ACMC ability measures can be influenced by various sources. First, variations among prosthesis users can play a role in the reliabil-ity of ACMC ability measures. Because great mental and physical effort may be required to control a myoelectric prosthesis, the ACMC ability measure may fluctuate randomly if the person is stressed or tired. Second, the trans-
30 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
duction of myoelectric signals can be affected by factors such as sweat and pressure on the electrodes.48 Third, the ACMC raters may introduce varia-tions into the ability measures. Rater reliability for ACMC version 1.0 was investigated among three raters with different ACMC experiences, and more experienced ACMC raters produced more consistent ACMC scores than did less experienced raters.127 New evidence of rater reliability has to be searched if an instrument has a new version.105 One important aspect of reliability that has not been previously evaluated in the ACMC is the stability of ACMC ability measures over time. If ACMC measures are not stable over time, then it is difficult to use the ACMC to detect changes in ability among prosthesis users or to conclude that a specific change is the result of an intervention. The amount of error from repeated measurements can be used to calculate the ‘minimum detectable change’ (MDC), which suggests the smallest change that can be detected by the in-strument beyond measurement error.128, 129 The MDC is a useful clinical value for the ACMC because it can serve as a guideline to show whether a change between ACMC assessments over time is due to measurement error or is a real change. To summarize, there are several aspects of evidence available to ascertain the quality of an assessment tool. In the ACMC, some of these aspects have been investigated, but others have not. The demand for outcome measures with psychometric evidence is increasing in the field because pressure from insur-ance companies and prosthesis users has prompted prosthetic professionals to demonstrate the benefits of prosthetic fitting.130-132 According to the American Academy of Orthotists & Prosthetists State-of-the-Science Conference (SSC) in 2009, measuring outcomes with validated prosthetic outcome measures is a current priority in the UL prosthetic field.133, 134 It is therefore necessary to continuously search and assess the psychometric evidence for using the ACMC to evaluate the ability to control a myoelectric hand.
1.8 Measuring outcomes with validated prosthetic outcome measures Functional outcomes in UL prosthesis users can be measured from different perspectives. If the aim of evaluation is the client’s ability to control his/her myoelectric prosthesis, then the ACMC may be an appropriate tool.134 If the client’s opinion about the device or daily prosthesis use is the aim of evalua-tion, then a client-rated questionnaire that measures UL prosthetic-related issues would be an appropriate tool.82 After the development of the ACMC in 2004, several UL prosthetic outcome measures were validated.86 Similar to the ACMC, these outcome measures were not designed for a study-specific pur-
HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 31
pose, but their developers had one common goal: to produce a reliable and valid outcome measure with which to measure the functional outcome in prosthesis users. One common aspect of these measures is that they have been validated with UL prosthesis users in contrast to other instruments using sub-jects with normal hands for validation, which has been a common practice in UL prosthetic research.135 Assessment of prosthesis users to validate UL pros-thetic outcome measures is necessary because the items/questions are intended to measure UL prosthetic-related issues and the findings are likely to be more valid than those using subjects with normal hands. These validated UL prosthetic outcome measures are important to our field because they have the potential to provide reliable and valid measurements that reflect our patients’ statues. However, it is not easy for clinicians to know what these outcome measures are actually measuring because most of them are primarily focused on measuring ‘function,’ and the concept of ‘func-tion’ can have different meanings for different professionals. An OT considers ‘function’ to be the person’s ability, but a UL prosthetic engineer refers to ‘function’ as the technical performance of a device. One way to understand the similarities and differences of outcome measures is to compare them by linking the content of the measures to the ICF.136
1.8.1 Content comparison using the ICF The ICF is a framework developed by the World Health Organization to describe human functioning.136 This classification goes beyond diagnosis to increase our awareness of the consequence of a disease. Impairments in body function and/or structure, such as loss of a part of or the whole UL, may lead to activity limitations or limited participation.137 The attitude toward disabil-ity has therefore shifted from a purely medical focus to a bio-psycho-social focus. The three ICF components ‘Body functions and structures,’ ‘Activities and participation,’ and ‘Environmental factors’ are classified into different catego-ries. A prosthetic hand is an ‘environmental factor,’ but it also partly replaces the ‘body functions and structures’ of a human hand. The ICF has been used in a study to measure functioning among users of prosthetics and orthotics (P & O) at a P & O outpatient clinic; their functioning increased when they were using P & O devices.10 The ICF categories have also been used to ex-plore functioning in acquired amputees.138 These two studies suggest that the ICF is useful to describe functioning of UL prosthesis users.

32 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
One useful aspect of the ICF is that it serves as a common language for differ-ent professionals to describe health-related status. This is particularly useful for our field, which comprises professionals from different disciplines. Be-cause the validated UL prosthetic outcome measures were developed by prac-titioners from different disciplines, they may use the same terminology, but with different meanings. Therefore, a content comparison of these UL pros-thetic outcome measures may provide a clear picture of their similarities and differences. The ICF has been proven to be useful for content comparison of similar measures in other fields.139-141 Researchers have commented that such comparison may help with the selection of an appropriate outcome measure and may identify the aspects of health that are lacking in the measures. To summarize, the newly validated UL prosthetic outcome measures have the potential to produce reliable and valid measurements that help us to make clinical decisions and demonstrate the benefits of prosthetic fitting. A content comparison of these outcome measures may therefore help professionals choose appropriate outcome measures for their clinical practice.
1.9 Rationale of the thesis Good control of UL myoelectric prostheses may ease users’ performance in their daily activities57, 88 but it may take a considerate amount of training and practice to achieve an adequate level of control. To monitor users’ progress in controlling their prostheses, a clinical tool that assesses how prosthesis users control their prostheses would be clinically useful. An assessment tool that can capture different aspects related to the capacity for myoelectric control can help the OT adjust the training pace and direction and, most importantly, help the prosthesis user achieve success in a step-by-step manner with the right level and amount of training. Although a variety of outcome measures have been used to measure outcomes among UL prosthesis users,83 none of them, before the ACMC, are designed to assess the capacity for myoelectric control. In response to this demand, the ACMC was developed, and two psy-chometric validations showed that this tool has the potential to produce reli-able and valid measurements. However, several important evidence related to the validity and reliability of ACMC are still lacking, such as the technical quality of ACMC items (content evidence), empirical item difficulty hierarchy (response processes evidence), DIF (internal structure), relations to external variables such as prosthetic wearing time and hand dominance, stability of the ACMC ability measures over time, and the influence of activity on the ACMC ability measures. Instrument validation is a continual process, and this thesis continued this process by searching and assessing the evidence re-

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 33
garding use of the ACMC to measure the ability to control a myoelectric prosthetic hand.
Measurement of the interaction between the UL prosthesis user and his/her prosthesis is challenging, and one outcome measure alone cannot fully grasp the whole picture of this interaction. The ACMC can only capture one part of this interaction; other outcome measures are needed to capture the other parts of this picture. Several UL prosthetic outcome measures have been developed in the last decade, including the ACMC. However, it is not always easy for clinicians to know what these new measures are actually measuring because quite a few of them are primarily focused on ‘function’ or ‘functional status,’ but their items/questions are different. Therefore, a content comparison of these outcome measures using the ICF may facilitate the selection of appro-priate outcome measures in clinical practice.

34 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
2 Aim The aim of the thesis is to search and assess the psychometric evidence regard-ing use of the ACMC to measure the ability to control a myoelectric prosthet-ic hand and to compare the contents of UL prosthetic outcome measures us-ing the ICF.
Specific aims: To evaluate the construct and rating scale of the ACMC (Study I) To evaluate the influence of standardized activities on the validity of
ACMC (Study II) To evaluate test-retest reliability and rater agreements of ACMC version
2.0 (Study III) To perform a content comparison of UL prosthetic outcome measures
using the ICF (Study IV)

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 35
3 Materials and Methods
3.1 Study Design For Studies I-III, a cross-sectional study design was chosen, and for Study IV, a systematic review was applied. Two ACMC versions have been used in this thesis; ACMC version 1.0 was used in Study I, and the results led to the de-velopment of version 2.0. Version 2.0 was then used in Studies II, III, and IV (see Results - ‘From version 1.0 to version 2.0’).
3.2 Participants in studies I, II and III The participants comprised individuals with either ULRD or AA of different ages, sexes, and prosthetic sides (Table 1). They were recruited from two clinics in Sweden: the ‘Limb Deficiency and Arm Prosthesis Centre’ (LDAPC) at Örebro University Hospital and the ‘Center for Arm Amputees’ (CAA) at Red Cross Hospital in Stockholm.
Table 1: Participant demographics in Studies I-III
STUDY I II III
Period Sep 00–Dec 04 Sep 09–Apr 11 Sep 09–Jun12
Clinic LDAPC LDAPC LDAPC/CAA
ULRD/AA 83/13 47/11 15/10
Age < 18 / age ≥ 18
81/15 35/23 10/15
Male/Female 55/41 31/27 13/12
Right /Left sided prosthesis users
39/57 19/36 (+3 bilateral)
8/16 (+1 bilateral)
Participants only in this study
72 24 7
Participants that took part in the other 2 studies
8 in II & III 16 in II
8 in I & III 16 in I 10 in III
8 in I & II 10 in II
Total no. of participants in this study
96 58 25

36 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
Prosthesis users who attend the LDAPC are from different counties in Swe-den, whereas prosthesis users who attend the CAA are mainly from the Stockholm region. The participants were fitted with one (unilateral) or two (bilateral) prosthetic hands of different sizes and models. Higher-level pros-thesis users were fitted with mechanical shoulder or elbow joints. A total of 103 UL prosthesis users took part in the 3 studies, and 34 of them took part in more than one study. Studies II and III were initiated at the same time; therefore 18 prosthesis users took part in both studies. In Study I, the sample comprised novice prosthesis users (n = 22) and users who had been wearing a myoelectric prosthesis for a period of 3 months to 19 years. All participants joined the study during their regular visits to the LDAPC. In Study II, to examine the influence of activity on different types of users, prosthesis users with different characteristics were included: (i) different pros-thetic levels (transhumeral, transradial, carpal); (ii) different years of prosthet-ic experience (0–40 years); and (iii) persons with ULRD, persons with AA, both sexes, both prosthetic sides, and persons of different ages (see Table 1). To assure that the sample was evenly distributed with regard to all activities, a ‘minimization’ sampling procedure was applied (see Data collection proce-dures for details). Study III aimed to examine the stability of the ACMC ability measures over time; therefore, we tried to recruit prosthesis users with stable control of their prostheses. A sample used for a test-retest study must be stable in terms of the attribute measured by the instrument so that errors from the instrument itself or the measurement procedure can be estimated.142 Prosthesis users excluded from recruitment were (i) novice prosthesis users or those just fitted with a new prosthesis, (ii) those who were unable to revisit the clinic within 5 weeks for the retest session, and (iii) those who underwent prosthetic training be-tween the test and retest sessions.
3.3 Materials in Study IV Published articles that used outcome measures to evaluate functional out-comes among UL prosthesis users were searched in the AMED, CINAHL, and MEDLINE databases. All English publications dated from 1985 onward, excluding conference proceedings, were considered. A total of 211 studies were found, and 68 studies remained after the removal of duplicates.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 37
3.4 Data collection procedures Procedures for data collection in Studies I, II and III are presented in Table 2. The ACMC assessments were performed either live (Study I) or with video-recording (Studies II, III). All raters in the studies had taken the ACMC train-ing course and were able to follow the manual to score the participants.
Table 2: Data collection procedures of Studies I-III
STUDY I II III
Activities Client-chosen Standardized Standardized
Activities per participant 1-2 3 1
No. of visits 1 1 2
Setting Live Recording Recording
ACMC Raters (n) 4 1 2
Clinical experience of ACMC raters (years)
2,10,15,20 5 5,15
Study I Self-chosen, non-standardized activities were used for Study I. Each partici-pant was assessed by his/her OT (ACMC rater), who was responsible for the participant’s visit. Six out of 96 ACMC assessments were collected by two OT students under OT supervision (the OT approved the student’s ratings). Client-chosen activities were used for the assessments, such as preparing a simple meal, making a bed, doing crafts, or playing with toys. The rater wrote down the scores on an ACMC 30-item scoring sheet. Missing ratings were allowed in data collection and therefore if an item was not performed during the activity, the item was then considered to be ‘missing.’
Study II Standardized activities were developed and used in Studies II. ACMC raters from different countries were asked to give three activity suggestions. From the suggestions, six bimanual activities were selected for standardization: ‘repotting a plant,’ ‘a ready-to-assemble project’ (e.g., build a structure with LEGO bricks or assemble a table lamp), ‘setting a table for four persons,’ ‘mixing a store-bought cake/pudding mix,’ ‘sorting bills or pictures,’ and ‘packing a suitcase for an overnight stay.’ The activity steps in each activity were then standardized with the ACMC items, such as opening a double door at shoulder level in all six activities so that the item ‘grasping and releasing in

38 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
different positions’ could be observed in all six activities. Activity materials were selected according to the size of the prosthetic hand so that the objects could fit well inside the prosthetic hand. The allocation method ‘minimization’143 was used to assign three of the six standardized activities to each participant so that each activity was performed by a group of prosthesis users with similar characteristics (age, sex, prosthetic side, and prosthetic experience). An OT (n = 3) gave instructions about the activity procedures. All three activities were performed during one clinical visit, and the performances were recorded. In the beginning of using ACMC version 2.0, the rater (Lindner HY) and the ACMC developer (Hermansson LM) assessed a number of participants together to ensure an understanding of the revised rating scale. Thereafter, the rater assessed the participants one activity at a time. A total of 30 ACMC assessments were collected for each activity (6 activities × 30 assessments = 180 assessments).
Study III Each participant performed one standardized activity approximately 2 to 5 weeks apart. The same OT (n = 6) placed the materials in the same locations and gave activity instructions in both sessions. All performances were record-ed. Rater 1 (doctoral student, 5 years of clinical experience) and Rater 2 (ACMC rater, 15 years of clinical experience) assessed each session separately using ACMC version 2.0. For the purpose of intrarater agreement, Rater 1 assessed the test session videos twice, 3 to 4 weeks apart.
Study IV Two criteria were used to select outcome measures: (i) outcome measure de-signed to evaluate UL prosthetic functional outcome, such as function, ac-ceptance, usage, satisfaction, adaptation, and ability; and (ii) outcome meas-ure that had been validated with UL prosthesis users. Outcome measures were excluded from consideration if their psychometric evaluations had not been performed with UL prosthesis users.
3.5 Data analyses Different statistical methods were used in Studies I, II and III (Table 3). The Rasch measurement approach was primarily used in Studies I and II, and the reliability statistical methods were primarily used in Study III. Two different Rasch models (RSM in Study I and MFRM in Studies II, III) were used for data analyses. Both RSM and MFRM are unidimensional models and are appropriate to analyze a set of items that share a common rating scale.111 The RSM analyzes two variables, such as item and person, whereas the MFRM

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 39
can analyze multiple variables (or facets) simultaneously (item/person/activity in Study II). Because two models and different parameters were used in Stud-ies I-III, the methods are described below separately.
Table 3: Statistical methods used in Studies I, II and III
STUDY I II III
Statistics Item fit statistics Rating scale analysis Item difficulty hierarchy PCA DIF and its effect on
item difficulty hierarchy
t-test Bias-interaction
analysis
Weighted κ PA ICC Bland-Altman
plot SEM MDC
Software Winsteps SPSS, Facets SPSS, Facets
The abbreviations in the table are explained in the following sections
3.5.1 Study I Using Winsteps144, the RSM calibrated two measures: participant ability measures and item difficulty measures. Each measure has a standard error (SE) that shows its precision. The size of the SE is most strongly influenced by the number of observations used to estimate the measure.145 The more data given to an item, the higher the precision and hence the lower the SE.
Technical quality of ACMC items (content) Item technical quality was examined using infit and outfit statistics. Infit is an information-weighted mean-square (MnSq) statistic, and outfit is an un-weighted MnSq statistic. MnSq fit statistics show the size of the randomness,146 and the significance of MnSq is reported by Z-standardized (Zstd) statistics.147 It has been recommended that an acceptable range to in-terpret item fit is MnSq of 0.5–1.5 and Zstd of <2.0.148 Therefore, these crite-ria were chosen to interpret item fit. An item was considered as a ‘misfit’ if its MnSq was <0.5, which indicates that the item could be redundant, or if its MnSq was >1.5, which indicates the item has been scored inconsistently and further investigation is therefore needed.
Rating scale functioning (response processes) The 4-point rating scale was analyzed using Linacre’s guidelines:94 ‘Frequency of Use’ of each rating category was used to indicate the num-
ber of participants rated in that particular category.

40 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
‘Observed Person Measures’ should increase from a category representing low ability to a category representing high ability.
‘Threshold Measure’ is the transition point between two adjacent catego-ries where there is a 50% chance to select either one of them. The thresh-old measure should also increase with increasing rating category number. This indicates that each rating category in turn is more likely to be ob-served than any other rating category as the person’s ability increases. Failure to demonstrate ordered thresholds indicates that the choices in the rating scale do not follow the expected hierarchical ordering.95
Outfit MnSq for each rating category was used to determine the presence of idiosyncratic use of the categories. A rating category with an outfit MnSq of >2.0 indicates that highly unexpected ratings in this category.
Item difficulty hierarchy (response processes) The difficulty measures of all ACMC items were plotted along a logit scale according to difficulty. In a similar way, the participants were also plotted along the same logit scale according to ability. This logit scale with both per-sons and items together was used to examine whether item difficulty hierar-chy matched clinical experience and whether the item difficulty range was well targeted to the ability range of the participants.
Unidimensionality (internal structure) The Rasch dimension was first removed from the data. Then, principal com-ponents analysis (PCA) examined the contrasts in the residuals. High contrast indicates the strength of many items, suggesting a second dimension.147 PCA also reports the variance explained by the Rasch measures and the variance explained by item difficulties.147 It is considered as good if variance explained by Rasch measures is > 60% and the first contrast is <5%.109
Differential item functioning (DIF) (internal structure) The existence of DIF was investigated in two person characteristics: sex and prosthetic side. A noticeable item DIF is present if the DIF size is >0.5 logits and is significant (t-statistic, p < 0.05).147, 149 The influence of DIF was further investigated in the item difficulty hierarchy. The two item difficulty hierar-chies in each subgroup (such as male against female) were compared.
3.5.2 Study II
Prosthetic wearing time and hand dominance (relations to other variables) Mean ability measures of full-time and non-full-time prosthesis users were calculated. Similarly, mean ability measures of dominant-sided/non-

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 41
dominant-sided prosthesis users were also calculated. Then independent t-test was used to test the differences between the means of full-time/non-full-time prosthesis users and dominant-sided/non-dominant-sided prosthesis users.
Influence of activities (construct-irrelevant variance) Using FACETS software,150 the MFRM calibrated three facets: participant ability measure, item difficulty measure, and activity difficulty measure. Two analyses were then performed: (i) investigation of the activities in relation to the user ability; and (ii) investigation of the sex and prosthetic side in relation to the activities. For the first investigation, the hypothesis was that partici-pants would perform similarly in their assigned activities and hence get simi-lar ability measures. The bias-interaction analysis produced a bias size that indicated whether any participant performed differently in any activity com-pared with the mean participant ability measure. For the second investigation, a bias size was generated for the interaction between each activity and each user characteristic. Separate analyses of persons with ULRD and with AA were performed. The magnitude of the bias size indicated whether an activity was harder or easier for any sex or prosthetic side compared with the activity difficulty measure based on the whole sample. The significance of each inter-action was tested with the t-statistic. As suggested by the MFRM, an interac-tion was considered significant when the magnitude of the bias size was ≥ ±0.5 logits and the interaction was statistically significant (p < 0.05).149, 151
3.5.3 Study III
Test-retest reliability Test-retest reliability was examined using three different statistics. Agreement at the item level was examined using the quadratic weighted kappa (weighted κ) and percentage agreement (PA). Participant ability measures for each ses-sion (estimated using FACETs software150) were used to calculate the intra-correlation coefficient (ICC2,1). The Bland-Altman method was used to exam-ine the agreement between participant ability measures in both sessions. The standard error of measurement (SEM) was calculated to show the amount of measurement error from both sessions. Three SEMs were calculated: one for Rater 1, one for Rater 2, and one for both raters together. The SEMs were then used to determine the MDC at the 95% confidence level (MDC95), again one for each rater and one for both raters together.
Rater reliability Inter-rater agreements of ACMC version 2.0 were examined for each session separately. At the item level, weighted κ and PA were used. Participant ability

42 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
measures from each rater were used to calculate two ICC2,1, one for each session. Intrarater agreement of Rater 1 was also examined using weighted κ, PA and ICC3,1.
3.5.4 Study IV Eight prosthetic outcome measures had been validated with UL prosthesis users at the time of this study. Apart from the University of New Brunswick (UNB) test, all identified outcome measures had at least one published psy-chometric study, giving a total of 14 published psychometric studies. The UNB test only briefly reports its rater reliability evaluation in its manual,152 and the information is not sufficient to assess its methodology. Methodology appraisal was therefore conducted on 14 studies separately by two reviewers (the doctoral student and the second author) using an appraisal form by MacDermid.153 The MacDermid appraisal form has been used to rate the qualities of psychometric studies in different recent systematic reviews in oth-er clinical fields.154-156 Any disagreement between the two reviewers was dis-cussed with the third author until a consensus was reached. The linking process was performed in several steps. (i) The items/questions in each outcome measure were entered into Excel. There were 438 items/questions in the 8 outcome measures, and some items were common in the different age or parent/child versions of the same measure. (ii) A total of 369 items/questions remained after the removal of duplicates of the same measure. (iii) Extraction of meaningful concepts from each item/question was then performed based on the ICF linking rules and advice from the ICF team leader Dr. Cieza. According to the ICF linking rules,136, 157, 158 more than one meaningful concept can be extracted from one item/question; e.g., two con-cepts were extracted from the ACMC item ‘coordinating both hands during grasping,’ namely ‘hand coordination’ and ‘grasping.’ (iv) Each meaningful concept was then linked to an ICF category based on the ICF category defini-tion. For example,
‘Grasping’ was linked to the ICF category ‘d4401 Grasping’ – which is defined as using one or both hands to seize and hold something, such as when grasping a tool or a door knob.159
(v) Excel was used to calculate the frequencies of concepts and ICF categories used for each component.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 43
4 Ethical Considerations Study I was approved by the Ethics Research Committee at Örebro County Council and Studies II-III was approved by Uppsala Ethical Committee. Study IV does not need ethical approval based on decision from the Regional Ethics Committee review board of Uppsala. All the participants and the parents for participants under 18 have received written and verbal information about the studies and about their rights to withdrawal and anonymity before participation. Parental written consent was obtained after parents had agreed to allow their child to participate in the studies. Although parents have decision-making power when their children are the object of research, the children should also have the right to decide when they are capable of understanding what consent to being researched means. Hence, both participants under 18 and their parents received written and verbal information but the parents were the ones who signed the consen-sus. Asking UL prosthesis users to perform activities is a normal routine at both clinics. In Study I, the assessments were taking place when the participants were performing activities of their own choices, such as playing with toys or cooking or performing other activities. However, standardized activities were used in Study II and III, that is, these activities were not client-chosen. We informed each participant about the activities they would have to perform so that they were able to consider if they would like to participate in Study II and III. For younger children, all the activities were adjusted to become a play activity, such as packing a doll outfit in a small colorful suitcase, setting table for a tea party, or opening envelopes with colorful stickers. One major ethical consideration is the use of video-recording for data collec-tion in Study II and III. Therefore, we explained carefully where the videos would be stored and no irrelevant person will have access to them. All infor-mation of the participants was kept confidential and it is not possible to iden-tify any participant from the data. It can happen that some participants may feel that their integrities are intruded after their performances were recorded. Therefore, it was strongly emphasized that they could retrieve from their participation at any time. During data collection, no participant had retrieved their participation and some of them even asked for copies of their videos.

44 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
5 Results
5.1 Content, response processes, internal structure evidence (Study I)
5.1.1 Technical quality of ACMC items Of 30 items, 27 were found to have MnSqs of 0.5 to 1.5. Two items were found to have an MnSq of >1.5 (with Z > 2.0). They were scored higher than expected according to the Rasch model in the three assessments, and their MnSqs were within 0.5 - 1.5 after removing the three assessments. This find-ing suggested that the item misfit was not systematic to the items. One item was found to have MnSq of <0.5 (with Z > 2.0); which suggested that this item could be redundant.
5.1.2 Rating scale functioning
Table 4. Summary statistics for the 4 rating-scale categories
Rating Category Frequency of Use (%)
Observed Person Measure
Threshold Measure
Outfit MnSq
0 - not capable 388 (19) -3.07 None 1.14
1 - sometimes capable 380 (18) -0.69 -1.72 1.00
2 - capable on request 366 (18) 1.10 0.31 0.50
3- spontaneously capable 949 (46) 3.90 1.41 1.09
Summary statistics for the four rating scale categories are shown in Table 4. The ‘frequency of use’ among categories 0, 1, and 2 was fairly even. Category ‘3 - spontaneously capable’ was used approximately three times more often than any of the other three categories. Both the observed person measures and threshold measures increased with the rating category value. Outfit MnSq for all categories was ≤1.14, indicating that there was no idiosyncratic use of the categories. All of these results suggest that the rating scale functioned in the expected manner. Outfit MnSq for Category ‘2 - capable on request’ was 0.50, however, indi-cating that the use of this category was somewhat redundant. Use of rating category 2 is clearly visualized in Fig. 8. The plot shows how the rating scale

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 45
categories relate to the underlying construct. Compared with the rating cate-gories 0, 1, and 3, the width of category 2 occupies a relatively small range along the x-axis, indicating that the use of category 2 was somewhat redun-dant (Fig. 8).
Fig.8. The probability curves of the 4 ACMC rating categories. The 0, 1, 2 and 3 category curves on the graph represent the 4 ACMC rating categories. The x-axis is participant ability minus item difficulty in logits.
5.1.3 Item difficulty hierarchy and targeting The item difficulty hierarchy and its relationship with the participants’ abili-ties are shown in Fig.9. Less capable persons/easier items are located at the lower end, while more capable persons/more difficult items are located at the upper end. Items that assess ‘the need for visual feedback’ during repetitive grip, repetitive release, and adjust force were the most difficult items. The items that assess timing were also difficult. Items that assess the need for ex-ternal support were the easiest items. Thus, the item difficulty matched the clinical experience in terms of the difficulty of items. The items targeted well the ability of the sample (By default, mean item difficulty = 0 logits; mean participant ability = +0.48 logits). However, several items that assessed visual feedback and timing had >50% missing ratings and slightly high SE (0.23–0.33).
5.1.4 Unidimensionality and presence of DIF Statistical decomposition of the variance in data indicates that the variance explained by the Rasch measures was 78% (not published), whereas 30.2% of the variance was explained by the item difficulties. The first factor in the residuals explained 2.3% of the variance in the data. The analysis of DIF showed that no item exhibited DIF between subjects with right or left pros-

46 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
thesis. Of the 30 items, 3 exhibited DIF between males and females. Further-more, two of the DIF items had >50% missing ratings. When comparing the male and female item hierarchies, these three items maintained similar loca-tions along the respective item difficulty hierarchies.
Figure 9.Persons’ ability measures in relation to item difficulty measures. X= participant, M=
mean for participant ability and item difficulty, S= 1 Standard deviation (SD) from the mean, T=
2 S.D. from mean, G= gripping, R= releasing, H= holding, C= co-ordinating, w/out= without
Logit scale
7 X +
|
|
X |
6 XX T +
|
X |
X |
5 +
X |
XX |
X |
4 +T
XXXX |
X |
XX S | G-repetitive grip, without visual feedback
3 XXX + G-adjust force, without visual feedback R-repetitive release, without visual feedback
XX | G-object towards hand
XXXXXX | G-feed hand forward
XXXX | G-without visual feedback
2 XX +S
XXXX |
XX | C-when gripping R-same time, arms in motion R-timing, arm is in forward/upward position
XXXX | R-timing, arm is in low position
1 XXXX + C-when releasing
X |
XXXX M |
XXX | R-adjust opening width
0 XX +M G-repetitive grip H-in motion, without visual feedback R-repetitive release
XX | R-without visual feedback
XXX | G-adjust force when gripping G,R-in any position H-w/out crushing H-w/out visual feedback
X |
-1 XXX +
XXX | H-in motion
XX | G-tripod pinch, without support R-without support
X |
-2 X +S G-whole hand, without support
XXX S | G-tripod pinch, with support
X | H-without support
XXX |
-3 XXX +
XX | H-with support
XXX | G-whole hand, with support
X | R-with support
-4 X +T
XX |
|
|
-5 XX +
T |
|
X |
-6 +
46 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
thesis. Of the 30 items, 3 exhibited DIF between males and females. Further-more, two of the DIF items had >50% missing ratings. When comparing the male and female item hierarchies, these three items maintained similar loca-tions along the respective item difficulty hierarchies.
Figure 9.Persons’ ability measures in relation to item difficulty measures. X= participant, M=
mean for participant ability and item difficulty, S= 1 Standard deviation (SD) from the mean, T=
2 S.D. from mean, G= gripping, R= releasing, H= holding, C= co-ordinating, w/out= without

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 47
5.2 From version 1.0 to version 2.0 Based on the findings in Study I, a revision of the ACMC was performed before Studies II-IV were initiated. The revision was intended to both improve the test in terms of evidence for validity and increase the usability of the test for clinicians. First, the findings on rating scale functioning were discussed with the Study I raters. Category ‘2 - capable on request’ was somewhat re-dundant because (i) some raters did not see the need to give a verbal request or (ii) the rater had missed the chance to give a verbal request. To improve the overall functioning of the rating scale, a decision was made to remove the verbal request and physical/verbal guidance from the middle categories. The category names and definitions were reworded to clearly indicate the increas-ing capacity level (Table 5).
Table 5: The ACMC rating scale Version 1.0 Category Version 2.0
Spontaneous and skillful control The item is performed smoothly and skillfully. The use of the prosthetic hand is immediate and spontaneous
3 Extremely capable Same as in version 1.0
Capable on request, spontaneity is not established The use of prosthetic hand is not spontaneous and verbal request is needed. The person is capable to perform the particular item but the control is delayed and not skillful
2 Generally capable Able to perform the item but the quality of movement is questionable. The use of the prosthetic hand can be slightly delayed
Sometimes capable, stability in the control is not established Physical or verbal guidance is needed. The control is slow, awkward and often fails
1 Somewhat capable The item is performed with difficulty or sometimes fails. The use of the prosthetic hand can be significantly delayed
Not capable Cannot perform the item even after several attempts or do not attempt to perform the item at all
0 Not capable Same as in version 1.0
Cannot rate the item The item is not observed
- Cannot rate the item Same as in version 1.0

48 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
Table 6. The ACMC items in version 1.0 and 2.0 Version 1.0 Version 2.0
The need for external support
G - whole hand, with support1
G - tripod pinch, with support1(redundant)
G - whole hand, without support
G - tripod pinch, without support
H - with support
H - without support
R - with support
R - without support
The need for external support
Grasping with support1
Power grip, without support
Precision grip, without support
Holding with support
Holding without support
Releasing with support
Releasing without support
Grip force and Opening width
Adjusting force when gripping
Holding without crushing
Adjust opening width
Grip force and Opening width
Appropriate grip force
Holding without crushing
Adjust opening width
Coordination of both hands
C - when gripping
C - when releasing2
Coordination of both hands
Coordinating both hands during grasping
Coordinating both hands during releasing2
Different positions and in motion(timing)
G - in any position
R - in any position
G - move hand forward3
G - object towards hand3
R - same time, arms in motion2
R - timing, arm in forward/upward position4
R - timing, arm in low position4
H - in motion
Different positions and in motion (timing)
Grasping in different positions
Releasing in different positions
Timing during grasping3
Timing during releasing4
Holding in motion
Repetitive grasp and release
Repetitive grip5
Repetitive release5
Repetitive grasp and release
Repetitive grasp and release5
The need for visual feedback
G – without visual feedback
G - Adjust force, without visual feedback
H - without visual feedback
H - in motion, without visual feedback
R - without visual feedback
G - repetitive grip, without visual feedback6
R - repetitive release, without visual feedback6
The need for visual feedback
Grasping without visual feedback
Appropriate grip force without visual feedback
Holding without visual feedback
Holding in motion, without visual feedback
Releasing, without visual feedback
Repetitive grasp and release, without visual
feedback6 G-gripping, H-holding, R-releasing, C-coordinating. Number in superscript - Items with the same number in version 1.0 are combined to become one item with the same number in version 2.0.
HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 49
Next, the high missing ratings in several items (visual feedback and timing items) were discussed with the raters. As also discussed in the first validity assessment of the ACMC,4 some raters were confused between the use of category ‘0 – not capable’ and ‘missing’ in certain difficult items, such as vis-ual feedback and timing. Therefore, a decision was made to combine these difficult, closely related items and redefine other items that were misinterpret-ed with the assumption that this would reduce the confusion. The redundant item ‘G - tripod pinch, with support’ was combined with ‘G - whole hand, with support.’ Many of the items were also renamed in version 2.0 (e.g., ‘G - tripod pinch, without support’ in version 1.0 and ‘Precision grip, without support’ in version 2.0 are the same items but with different names). This version 2.0 with 24 items was used in Study IV (Table 6). After using version 2.0 during the years 2009–2010, a slight revision was made. At that time, it was found that the item ‘adjust opening width’ was rated inconsistently. Another item, ‘holding without crushing,’ was consid-ered similar to ‘appropriate grip force.’ These two items had exactly the same difficulty measure in the analysis from Study I. Therefore, version 2.0 became a 22-item version and was used in Studies II and III.
5.3 Relations to other variables & construct-irrelevant variance(StudyII)
5.3.1 Relations to prosthetic wearing time & hand dominance For both groups (ULRD and AA), the mean ability measures of full-time pros-thesis users were significantly higher than that of non-full-time users (ULRD p = 0.04, AA p = 0.04). Participants with dominant-sided AA had higher ability measures than those with non-dominant-sided AA (p = 0.01), whereas no significant difference between sides was found in participants with ULRD.
5.3.2 Influence of standardized activities Of the 60 prosthetic hands from 58 users (the 2 bilateral users with 2 myoe-lectric hands gave 4 ACMC assessments), 57 showed no significant differ-ences among their 3 assessments, and their ability measures showed a differ-ence of <0.5 logits. Three non-full-time prosthetic users had different ability measures (>0.5 logits), and the differences were significant. The difficulty range of the six activities was between –0.67 and –1.08 logits; that is, they were similar in terms of difficulty. The analyses between the ac-tivities across sex and prosthetic side showed that the bias sizes of the activi-ties were all within ±0.5 logits and did not differ significantly between males

50 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
and females (p ≥ 0.17) or between dominant and non-dominant prosthesis users (ULRD p ≥ 0.59; AA p ≥ 0.33). This implies that the activities func-tioned similarly across both subgroups in terms of sex and prosthetic side.
5.4 Evidence on test-retest reliability and rater agreement (Study III) The mean ability measure was 0.97 logits (test session) and 0.96 logits (retest session) respectively. For test-retest reliability, The weighted κ of all items was 0.52 to 1.00 (PAs 66%–100%), and the test-retest ICC2,1 was 0.94. One item was scored with one rating category, and hence no weighted κ was calculated. The Bland-Altman method showed that all but one participant, a non-full-time prosthesis user, were within the 95% LOA. The MDC95 was 0.52 logits (Rater 1), 0.55 logits (Rater 2), and 0.69 logits (both raters). All MDC95 were <5% of the total ability logit range. For inter-rater agreement, three items were scored with one rating category only, and hence no weighted κ was calculated. The weighted κ at the item level in both sessions was 0.44 to 1.00 (PAs 56%–100%), and the ICC2,1 was 0.95 (test) and 0.92 (retest), respectively. Among all items, the two items ‘grasping’ and ‘releasing’ without visual feedback had the lowest PA and weighted κ. For the intrarater agreement of Rater 1, the weighted κ at the item level were all >0.80 and their PAs were ≥96%. The ICC3,1 for the test session of Rater 1 was 0.98.
5.5 Content comparison using ICF (Study IV) Eight outcome measures and 14 psychometric studies were found (in 2009): ACMC – all ages 4, 127, 160 Child Amputee Prosthetics Project - Functional Status Inventory (CAPP-
FSI) - age 1 to 17161-163 Child Amputee Prosthetics Project - Prosthesis Satisfaction Inventory
(CAPP-PSI) - age 1 to17164 Orthotics and Prosthetics Users’ Survey (OPUS) - all ages but only one
module has been validated with adult UL prosthesis users122 Prosthetic Upper Extremity Functional Index (PUFI) - age 3 to 1822, 165, 166 Trinity Amputation and Prosthesis Experience Scales (TAPES) - adults 167 Unilateral Below Elbow Test (UBET) - age 2 to 21166, 168 University of New Brunswick test (UNB) - age 2 to 21152(test manual) Three observational measures are clinician-used (ACMC, UBET, and UNB). The ACMC uses client-chosen activities for assessment, whereas the UBET and the UNB test assess prosthetic control with activities for different age

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 51
groups. The other five are client-rated questionnaires (CAPP-FSI, CAPP-PSI, OPUS, PUFI, and TAPES) that evaluate prosthesis use in daily life. Appraisal of the study methodologies showed that all studies received more than 60% of the ratings, and more than 80% of the ratings were given to the ACMC, OPUS, and TAPES. In terms of primary focus, the CAPP-FSI, CAPP-PSI, OPUS, PUFI, and UBET primarily focus on evaluation of function or functional status in prosthesis users, but their questions/items cover different areas. For example, the OPUS has questions on quality of life, the TAPES focus on psychosocial adjustment, and the CAPP-PSI has questions on prosthetic component functions. A total of 393 concepts were extracted from 369 items/questions. The con-cepts were linked to 54 ICF categories. The frequencies of the ICF categories used in ‘Body Functions,’ ‘Activity and Participation,’ and ‘Environmental Factors’ are presented in Tables 7, 8, and 9. The ACMC, OPUS, and TAPES have concepts that linked exclusively to the ‘Body Function’ categories, such as coordination and emotional functions (Table 7).
Table 7. Frequencies of ICF categories used in ‘Body functions’
Seven outcome measures, except the CAPP-PSI, were linked to the categories in ‘Activity and Participation’ (Table 8). As UL prosthesis is replacement of the missing hand, the categories ‘fine hand use’ and ´hand and arm use’ had the highest frequencies. The highest frequency is the UNB test because it has the highest number of activities. Although the TAPES is designed for both UL and lower limb users, it’s activities are related to more frequent to lower limb use than upper limb use. The CAPP-PSI questions are all focused on services and prosthetic components, and they are thus linked with the categories in the component ‘Environmental Factors.’ The OPUS and TAPES also have a spe-cific module that evaluates prosthesis services, and they were linked to cate-gories in ‘Environmental Factors’ (Table 9).

52 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
Table 8. Frequencies of ICF categories used in Activity and Participation
Table 9. Frequencies of ICF categories used in Environmental factors

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 53
6 Discussion
6.1 General discussion Instrument validation is a process that gathers evidence to support the mean-ing of test scores in relation to their intended use. The current view on validi-ty refers to ‘…evidence and theory in support of the interpretation of test scores…’105 The ACMC is designed to measure a theoretical construct that covers six aspects related to the capacity for myoelectric control, all of which have been described in the literature. However, it is possible that ACMC has missed some other aspects related to myoelectric control. Furthermore, ad-vances in prosthetic component design and control formats may lead to new aspects related to myoelectric control, and it is possible that the ACMC may include new aspects in the future. Nevertheless, the aim of this thesis was not to develop an instrument that covers all aspects of this capacity. Instead, the aim was to validate the ACMC and to assess whether any evidence exists in support of its use to assess the ability to control a myoelectric prosthetic hand. Instead of using different types of validity, different sources of evidence are used as a framework upon which to organize the validations and findings in this thesis. Different researchers have published different validation examples for each source of evidence based on their interpretations.106, 116, 117, 169-171 It is therefore possible that readers may also have different interpretations on how the validations are to be organized with respect to the different sources of evidence in this thesis. Nevertheless, the current view on validity is welcomed by researchers and authors in different clinical fields.106, 116, 117, 169, 172, 173
A minor but important part of this thesis is a content comparison of UL pros-thetic measures. While the comparison was performed to identify the similari-ties and differences between these outcome measures, the long-term goal of this comparison is to encourage the use of validated outcome measures in clinical practice. The discussion below starts with the findings concerning the psychometric evidence of the ACMC, which is followed by a discussion of the content comparison.
6.2 Validity Evidence of the ACMC (Study I and II) Evidence based on content evidence often focuses on content relevance and content representativeness, but rarely on technical quality of items such as ‘unambiguous phrasing.’ Examining the item technical quality using Rasch item fit statistics is a fairly new suggestion, but it has been used in a few psy-

54 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
chometric studies.174-176 Each ACMC item has a detailed definition that guides ACMC raters to rate the item; therefore, a poorly defined item that causes confusion in raters would lead to inconsistent ratings. The results showed that two items had MnSq > 1.5, but this was due to three assessments and was not systematic to the items. Interestingly, in the first validation of ACMC,4 in which a smaller MnSq was chosen (0.4–1.6), all items showed acceptable fit statistics. This further confirmed that the item misfit in Study I was likely due to sample or even rater error. Because the item misfit was not systematic to the items, and considering the findings from the first validation of the ACMC, we suggest that all items have sufficient technical qualities. Evidence based on response processes was searched using an item difficulty hierarchy, which provides evidence on how the abilities of prosthesis users demonstrate the construct. From clinical experience, we know that ‘the need for external support’ is the easiest aspect whereas ‘the need for visual feed-back’ is the most difficult aspect; therefore, the empirical item difficulty hier-archy is an important piece of evidence. This empirical item difficulty hierar-chy has two practical meanings. One is to provide us a sense of how much of the underlying construct or attribute is required to perform the item success-fully,90 and the other is to provide us a picture of how the items are related to one another along the construct. This means that the hierarchy may be used as a guideline to indicate how a typical new prosthesis user can be trained from the easiest aspect, ‘the need for external support,’ all the way up to the most difficulty aspect, ‘the need for visual feedback.’ Evidence based on response processes was also searched by analyzing the rating scale. The overall analysis of the rating scale suggested that the re-sponses to the rating scale behave in the expected manner. Category ‘2 – ca-pable on request’ occupies a shorter range on the construct ‘capacity for myo-electric control’ compared with adjacent categories. This is not a serious problem, but the functioning of this category should ideally be improved. Two suggestions have been raised to improve the functioning of Category 2: (i) collapse Categories 1 and 2 because studies have shown that the collapse of underused categories can improve rating scale functioning,122, 177-179 or (ii) revise the definition of Category 2. After a discussion with the raters, it seems that revising the definition is a better choice because the use of a rating cate-gory should not depend on whether a rater gives a verbal request or not, alt-hough verbal request are often used in prosthetic training. Therefore, the decision was made to revise the rating category definitions and to reword the category names to clearly indicate an increasing level of capacity.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 55
One important validation concerning evidence based on internal structure is the unidimensionality of an instrument. Unidimensionality is fundamental for invariant measurement, meaning that the rank order of item difficulty should not vary from one sample to another sample.91 The PCA results showed that the ACMC fulfils the requirement to be unidimensional. Together with the earlier evaluation,4 unidimensionality is demonstrated twice in the ACMC with two different methods (item fit and PCA). The evidence of unidimen-sionality thus provides an encouraging starting point for measuring the capac-ity for myoelectric control. However, DIF was present in three items for males and females. Two of these DIF items had more than 50% missing ratings, and missing ratings reduce item precision (large SE); therefore, it is too early to draw any conclusion regarding whether DIF exists in these items. Further-more, as suggested in other literature, the sample size for DIF analysis must be at least 100 per group.149, 151 Therefore, the current finding on DIF can only indicate the possibility of DIF in these items. Further research with a large sample is needed. Evidence based on relations with other variables is often searched by evaluat-ing the correlation of a given instrument with another similar instrument. Apart from the correlation with another instrument, Messick suggested that ‘other variables’ can be any external variables that are able to support the validity of the instrument.104 In this thesis, the prosthetic wearing time and hand dominance were chosen as external variables because they are widely used in the prosthetic field to indicate prosthetic acceptance or daily prosthet-ic use.19, 45, 88, 118-122 The results showed that full-time prosthesis users had higher ability measures than did non-full-time users among both persons with ULRD and persons with AA. This finding is in accordance with a study in which functionality among children with ULRD was evaluated.57 Adaptation to the prosthesis often encourages the users to increase their wearing time.57,
180 This may stimulate patients to use their prostheses in daily activities and hence achieve better myoelectric control; i.e., higher ability measures. For another variable, ‘hand dominance,’ persons with dominant-sided AA had higher ability measures than did those with non-dominant-sided AA. Alt-hough there were too few participants with AA in Study II to draw any defi-nite conclusions, dominant-sided prosthesis users are likely to use their pros-theses more actively than non-dominant-sided users, and hence a higher abil-ity measure is likely to be observed. Because the results are based on mean differences between groups but not on the correlations between the ACMC ability measures and these two variables, this evidence is not as strong as that based on correlations.
56 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
6.3 Influence of activities - construct-irrelevant variance (Study II) The question of whether activities have any influence on the ability measures has been raised in two ACMC validation studies: once in 2006127 and again in Study I.160 Therefore, six activities were standardized to answer this question. The results showed that in the majority of participants, there was no signifi-cant difference among their assessments, and their ability measures showed a difference of <0.5 logits. This confirms that construct-irrelevant variance is always present to some extent.124 The six standardized activities are similar in some ways but different in others. They are similar in that they all contain everyday objects such as clothing, glasses, kitchenware, table lamps, paper, pens, or LEGOs for children. They are also similar because every activity involves objects that require prosthesis users to use their prosthetic hands in different positions and to pass objects between their hands. However, the object shapes and textures are different enough to allow the evaluation of activity influence on the ACMC ability measures. The results showed that the majority of participants received similar ability measures in their assessments while performing different activities. This means that for a user who can con-trol his/her prosthetic hand without the need for external support, he/she is capable of grasping a LEGO piece (a ready-to-assemble project), a pen (sort-ing bills or pictures), and a t-shirt (packing a suitcase for an overnight stay) with no external support. However, three non-full-time users had a difference of >0.5 logits among their three activities, and the findings in Study II may not necessarily be generalizable in the same extent to non-full-time users.
6.4 Reliability evidence of the ACMC (Study III) Inconsistent scores reduce the validity evidence of the scores; therefore, it is important to evaluate the reliability of the ACMC ability measures in terms of both stability over time and rater agreements. The inter-rater agreement of version 1.0127 suggested that clinical experience helps to produce consistent ratings. This is logical because clinicians need to understand how a myoelec-tric prosthesis works and the challenges faced by prosthesis users when con-trolling their prostheses. This is also the main reason why experienced raters were used to evaluate version 2.0; the aim of this evaluation was to determine whether any item or rating scale definition is well understood. The rater agreements at the item level for version 2.0 were on average higher than those of version 1.0. One reason for this could be the revised rating scale because the rating scale in version 2.0 now clearly indicates an increasing level of capacity.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 57
The result of the test-retest ICC was excellent, and the MDC95 was <5% of the total ability range. The MDC95 is an important clinical value because the ACMC is intended to monitor the progress in prosthesis users, and the noise that is due to measurement error can mask changes that may, in fact, be at-tributable to the intervention. Furthermore, we know from clinical experience that the effect of prosthetic training is substantially smaller than that of hand surgery, which increases hand function considerably. To show the training effect, an instrument with a small MDC95 is necessary. The MDC95 for the same and different raters can be used as indicators to determine whether the change is due to variation or ability. However, this MDC95 is calculated from observations of two experienced raters, and it is likely larger in inexperienced raters.
6.5 Comparison of UL prosthetic outcome measures (Study IV) The purpose of performing this content comparison was to show in detail what the selected UL prosthetic outcome measures are actually measuring. The comparison therefore went beyond the aims of the selected UL prosthetic outcome measures and compared their items and questions using the ICF. Five out of eight outcome measures have primary focus on function or func-tional status in prosthesis users but their items/questions did not link the same ICF categories. This confirms that it cannot be assumed that outcome measures that have the same primary focus will provide similar kinds of clini-cal data. This comparison serves two purposes. One is to show the similarities and differences among the UL prosthetic outcome measures. The list of ICF cate-gories shows the areas intended to be measured by the outcome measures. The purpose of UL prosthesis is to provide a mean for the users to perform their activities and participated in different activities. Therefore, it is not sur-prising that the items and questions were linked most of the ICF categories come under the component ‘Activity and Participation’. For example, the CAPP-FSI, PUFI, UBET and UNB cover mostly the same categories and all are under the ICF component ‘Activity and participation’. Moreover, the ACMC, OPUS and TAPES cover more than one ICF component, indicating that these outcome measures cover a wider dimension than the other outcome measures identified in this comparison. The OPUS and TAPES cover stump pain, em-ployment, and social relationships, which are all relevant issues among upper limb amputees. The TAPES is the only outcome measure that covers ‘body image’, which is an important aspect in the acceptance and continued use of the device. However, the TAPES has items such as walking and climbing that are not so useful to evaluate UL prosthesis users.

58 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
Another purpose of this comparison is to suggest the aspects of health that are lacking in the outcome measures. Aspects such as emotional functions, psychosocial adjustment, body image and social interaction are important for both paediatric and adult prosthesis users, but only TAPES and OPUS cover these aspects. The TAPES is designed for adults and the validity of OPUS – health-related quality of life module has only been evaluated in lower limb prosthesis users. Since there is a need for such an outcome measure for paedi-atric users, further validation of the OPUS for paediatric upper limb prosthe-sis users is thus encouraged.
6.6 Methodological considerations
6.6.1 Study I, II and III The strength of psychometric evidence should always be interpreted in the light of the methods used to search for the evidence. Three major elements may have affected the evidence in this thesis: (i) samples, (ii) data collection procedures, and (iii) methods of data analysis.
Samples The ACMC has been examined across individuals with ULRD or AA, a wide age range, different sexes, different prosthetic sides, varying prosthetic experi-ences, and different wearing times. This is necessary because it covers the range of prosthesis users at which the ACMC aims. The use of samples from both individuals with ULRD and individuals with AA is common among the validations of UL prosthetic outcome measures.22, 161-163, 181 This is probably because these two groups often attend the same clinic, and the procedure of prosthesis fabrication is somewhat similar. One main limitation of the sam-ples in all three studies was that the participants were all self-selected. How-ever, the proportion of males/females in the samples represents the popula-tions of ULRD and AA in that more males than females have limb deficiencies or amputation.15, 29, 31, 182, 183 There were more left-sided than right-sided pros-thesis users in the samples because of the high number of ULRD in the sam-ples and because left below-elbow deficiency is the most common type of ULRD fitted with UL prostheses.18, 182 In Study I, there were more pediatric than adult prosthesis users because chil-dren change their prostheses more often than do adults and therefore attend-ed the LDAPC more often than did adults during the data collection period. The wide ability range of the sample in Study I is a strength, and the mean ability range was close to the mean item difficulty. This suggests that the sample in Study I was suitable for validation of the ACMC.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 59
In Study II, the sample was strategically recruited to meet the aim of the study. Different types of prosthesis users, such as those with different pros-thetic levels and prosthetic experiences, were recruited to examine the influ-ence of activity on their ability measures. The use of ‘minimization’ sampling to assign prosthesis users to different activities was a strength of Study II. This was necessary to perform a fair comparison of the influence of activities on groups with similar characteristics. However, there was a relatively small number of less-capable users in the sample. In Study III, the sample was also strategically recruited to meet the aim of the study. Prosthesis users with stable abilities were recruited so that errors from the ACMC itself or from the measurement procedure could be estimated. Therefore, the sample included a large number of users with more than 5 years of experience because they usually have a more stable ability than less experienced or new users. It was not easy to recruit participants that could take part in the retest session, and the recruitment therefore took quite some time. An even number of full-time and non-full-time users is a strength of the sample because it allowed us to see their variations between test-retest ses-sions. The sample size fulfilled the requirement of stable calibration for Rasch anal-yses (Studies I and II)184, 185 and test-retest reliability (Study III).186 However, the size of the subgroups for DIF analysis (Study I) was too small to draw a definite conclusion regarding whether DIF was present in the items. Similarly, each activity had only been performed by 30 prosthesis users in Study II; therefore, the findings must be confirmed with a larger sample.
Data collection procedures It was a conscious decision to include raters with different experiences to collect the data in Study I. This was because we aimed to determine how the ACMC worked with raters from no experience to those with many years of experience. Study I raters have various experiences and two of them were OT students; therefore, variation in the data was expected to be larger than in studies using only experienced raters. Rater influence on data is a known influential factor in clinical observational measures. Often, variation among the data is probably due to inexperienced raters. However, because the data were collected in a typical clinical setting by raters with different experiences, the validity evidence in Study I supported the use of the ACMC in a typical clinical setting.

60 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
However, in some cases, the use of multiple raters may not be suitable for the aim of the evaluation, such as the evaluation of the influence of activity on the ACMC ability measures. Sometimes, it is preferable that the same rater assesses the individuals to minimize unwanted variability in the ratings,187 as was the case in Study II. It was a challenge to evaluate 180 assessments, and any error would have affected the results. However, based on the intrarater reliability in Study III, it could be assumed that this consistency also existed in Study II. In addition, among all 180 assessments, 10 were the ‘test session’ assessments, which were also rated by Rater 2 in Study III. The fact that the inter-rater agreement of the test session was good indicated that ACMC ver-sion 2.0 was used well to rate the participants. The assessments were collected from either live (Study I) or video-recorded (Studies II and III) settings. The ACMC is always assessed in a live setting, and it was therefore important to validate its use in a live situation. Video recording was used in Studies II and III, and the advantage of using videos was that we were able to look at the performances repeatedly. However, as also described in the UBET study,168 sometimes the intact hand blocked the view of the prosthetic hand, which made it difficult to assess the use of the prosthetic hand. In the ACMC assessments, because the users walked around during the activities, it was not always clearly shown in the video whether the participants needed visual feedback or not. This made it difficult to score the items on ‘the need for visual feedback’ in Studies II and III when collecting ACMC assessments. From clinical experience, we know that it is always easi-er to assess visual feedback items in live assessments.
Methods of data analysis The Rasch measurement approach was mainly used to search for evidence in Studies I and II. Apart from the above-mentioned advantages of Rasch analy-sis, another advantage of Rasch analysis in Study I was its ability to handle missing data, because logit measures are not a sum of raw scores, but an es-timate of odds. However, one limitation of the Study I analysis was that the impact of raters was not taken into consideration. The Rasch RSM allows only the analysis of items and persons, whereas the MFRM allows the analy-sis of items, persons, and raters. The item difficulties and participant abilities likely would not have changed if the MFRM model had been used, but the MFRM allows for the analysis of rater severity and possible rater error. One debatable issue is the MnSq range (0.5–1.5) chosen to interpret item fit in Study I. This range is wider than the MnSq range of 0.6–1.4 in the first validation of the ACMC.4 An MnSq range of 0.5–1.7 has been recommended

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 61
for clinical observational data,103 and the following question has also arisen: ‘What kind of data variation do we expect?’ If clinical observational data are collected by experienced raters only, then a smaller variation in the data would be expected compared with data collected by raters with mixed experi-ence. Study I data were collected by raters with 0 to 20 years of experience; therefore, a larger variation was expected than that of the data collected by only experienced raters. It thus seemed logical to use a range of 0.5–1.5 to interpret item fit in Study I. In future studies of the ACMC involving raters that have gained an adequate level of consistency, a narrower MnSq range may be employed to interpret item fit. In Study III, the ICC was chosen as the reliability coefficient because it can be compared with other outcome measures in the prosthetic field. However, it is widely known that the ICC is sensitive to within-subject variance.188 There-fore, the Bland-Altman method was also used to examine the test-retest agreement because it is not affected by variance within a group.189, 190 The weighted κ was chosen to analyze agreements at the item level because we aimed to compare the weighted κ results with the previous rater agreement study of the ACMC, although the ICC is equivalent to the weighted κ.191
6.6.2 Study IV This content comparison was specifically focused on UL prosthetics. There-fore, outcome measures for musculoskeletal injuries in UL amputees were not included for comparison, although these measures are very useful in measur-ing physical body function in amputees and persons with ULRD. The selec-tion was also narrowed to include only the outcome measures that used UL prosthesis users as subjects in their psychometric evaluations; therefore, fewer instruments were present in this study than in the two reviews published around the same time.82, 83 One advantage of a more strict selection of out-come measures is that it is easier for clinicians to compare the outcome measures and to judge whether the outcome measures are able to provide information in line with the aims of their evaluations in clinical practice. Compared with the other three ICF components, the ‘Environmental Factors’ categories are very general. This has also been pointed out by researchers in assistive technology.192 193 Assistive devices, such as P & O devices, are in-cluded in one category ‘Assistive products and technology for personal use in daily living.’ If we had linked the items only to this category, then it would not have been possible to see their similarities and differences. Therefore, a decision was made to link the items according to their intended use in human functioning; for example, grasping using a prosthetic hand was linked to

62 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
grasping using a human hand. This way of viewing assistive devices according to their intended use has also been supported by assistive device researchers.193 The linking process was conducted according to the linking rules suggested by the ICF and Dr. Cieza.9, 157, 158 The communication with Dr. Cieza was also extremely valuable in applying the linking rules.
6.7 Further research on the ACMC Future research on the ACMC should continue to search for psychometric evidence for version 2.0. The Standards suggest a new process with which to gather evidence if the test has a new version.105 Evidence on the technical qualities of the 22 ACMC items must be searched, especially now that the ACMC is used by ACMC raters from different countries. In addition, evi-dence based on the response processes must be searched for the 22-item diffi-culty hierarchy, revised rating scale, and person fit statistics. One important question concerning the item difficulty hierarchy is whether it would remain unchanged for persons with ULRD and for persons with AA if a large enough sample is obtained to perform the analyses separately. Another question is whether the item difficulty hierarchy would remain unchanged if samples from different countries are used. Bond suggested that if the order of item difficulty stays the same in different samples, that would address the very essence of validity.194 Therefore, validation of the item difficulty hierarchy among different samples would provide valuable evidence for the ACMC. One important validation concerning evidence based on response processes involves the investigation of how test users reason their scores during scoring process.105 Every ACMC rater must complete a training course, and showing whether they clearly understand the items and rating scale use is an important piece of evidence. This evidence shows the effect of rater training.116 Evidence based on internal structure should be continued in searching for the existence of DIF in ACMC items if subgroup sizes can support the analyses. Different diagnoses (ULRD and AA), sex, prosthetic side (dominant and nondominant side), and samples from different countries are several person characteristics that can potentially show DIF in the ACMC. The combination of items in version 2.0 is not likely to make the ACMC multidimensional, but if new items are going to be added to the ACMC, such as finger movements or el-bow movements, then evidence for unidimensionality must be gathered again. In terms of evidence based on relations to other variables, a possible future validation might involve evaluation of how the ACMC ability measures corre-late with the UNB scores or client-rated questionnaires such as the PUFI or OPUS. Valuable evidence would be provided if the UNB test and the ACMC

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 63
are related to each other. Further validation with some widely used variables in the prosthetic field, such as the time between amputation and prosthetic fitting, amputation level, and amount of pain, would also be valuable.
In terms of the reliability aspects of the ACMC, the MDC95 value is now based on the assumption that measurement error or variation is uniform across the entire ability range. However, it seems that variation is larger in non-full-time users; therefore, it is possible that the MDC95 value would be different between new and experienced users or between full-time and non-full-time users. If it is possible to recruit large numbers of individuals within different subgroups, it would be valuable to investigate the MDC for different subgroups. A further validation would involve calculation of the ‘minimal clinical important difference’ (MCID),195, 196 which is a value important in interpreting the clinical relevance of observed change.197 The MCID is the threshold at which a person or group has just begun to experience an im-portant improvement195; namely, when prosthesis users have just begin to experience an improvement in controlling their prostheses. Evidence based on test consequence is a new source of evidence suggested by Messick.104 It concerns the possible impact of the test on both the test givers and test takers.105 Therefore, this evidence refers to the long-term goal of the use of a test. Although more evidence must be searched among other sources, one question concerning evidence based on the consequence of the ACMC is whether ACMC raters found it useful to evaluate their clients. This valuable evidence can be collected in the future, after the ACMC has been consistently used by raters in different prosthetic clinics. Further research on the activity influence on the ACMC ability measures should be carried out using a large sample of non-full-time users. Further-more, more activities are needed to investigate whether other activities would give different results.
6.8 Current status of the selected prosthetic outcome measures The ACMC, UBET, and UNB test are currently used in different prosthetic clinics.83 All client-rated questionnaires with the exception of the CAPP-FSI are also being used in different clinics. After the publication of this content comparison, new validations of the OPUS and TAPES have been published.198-201 The validation of the UNB test is also underway. No further validation has yet been published for the UBET or CAPP; however, in line with other researchers in the field,83 further evidence and development of the UBET and CAPP are recommended.

64 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
Although psychometric evidence is important, clinicians should also be con-cerned with issues such as the clinical usefulness of a new instrument.155 One question is how clinicians can apply the work from this thesis in their clinical practice. Therefore, it is important to understand the clinical implication of the findings in this thesis.
6.9 Clinical implications
6.9.1 Clinical use of the ACMC While the goal of prosthetic training is to help the user to integrate the pros-thesis into his/her daily life, good control of the prosthesis is a prerequisite. The evidence on unidimensionality indicates that all items work together to measure the six aspects related to the capacity for myoelectric control. One implication of the evidence on unidimensionality is that the ACMC can be used as a metric with which to measure capacity. The ACMC items range from low to high difficulty, which enables the ACMC to differentiate prosthe-sis users of different capacities. I propose the use of the item difficulty hierar-chy as a guideline for prosthetic training. For example, when a user is able to use their prosthetic hand in space, the training should proceed to other as-pects. The finding in Study II indirectly indicates what the ACMC is measuring (the ability to control a prosthesis) and is not measuring (e.g., the ability to per-form an activity independently). If the aim of a clinical evaluation is to assess the ability to control a myoelectric prosthetic hand, then the ACMC is an appropriate tool. If the aim of an evaluation is to assess whether a prosthesis user can perform daily activities independently regardless of whether the pros-thetic hand is being used, then other instruments that evaluate whether a user can perform an activity independently would probably be useful. However, it is widely known that unilateral users can perform many daily activities with their intact hands and their residual limbs or other body parts89; therefore, the fact that prosthesis users are able to perform daily activities independently does not mean that they have good control of their prostheses.
The results of Study II suggest that six standardized activities can be used interchangeably for ACMC assessments. Again, the ability measures may vary more for non-full-time users than for full-time users. If time allows, two standardized activities can be used in one ACMC assessment because this
64 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
Although psychometric evidence is important, clinicians should also be con-cerned with issues such as the clinical usefulness of a new instrument.155 One question is how clinicians can apply the work from this thesis in their clinical practice. Therefore, it is important to understand the clinical implication of the findings in this thesis.
6.9 Clinical implications
6.9.1 Clinical use of the ACMC While the goal of prosthetic training is to help the user to integrate the pros-thesis into his/her daily life, good control of the prosthesis is a prerequisite. The evidence on unidimensionality indicates that all items work together to measure the six aspects related to the capacity for myoelectric control. One implication of the evidence on unidimensionality is that the ACMC can be used as a metric with which to measure capacity. The ACMC items range from low to high difficulty, which enables the ACMC to differentiate prosthe-sis users of different capacities. I propose the use of the item difficulty hierar-chy as a guideline for prosthetic training. For example, when a user is able to use their prosthetic hand in space, the training should proceed to other as-pects. The finding in Study II indirectly indicates what the ACMC is measuring (the ability to control a prosthesis) and is not measuring (e.g., the ability to per-form an activity independently). If the aim of a clinical evaluation is to assess the ability to control a myoelectric prosthetic hand, then the ACMC is an appropriate tool. If the aim of an evaluation is to assess whether a prosthesis user can perform daily activities independently regardless of whether the pros-thetic hand is being used, then other instruments that evaluate whether a user can perform an activity independently would probably be useful. However, it is widely known that unilateral users can perform many daily activities with their intact hands and their residual limbs or other body parts89; therefore, the fact that prosthesis users are able to perform daily activities independently does not mean that they have good control of their prostheses.
The results of Study II suggest that six standardized activities can be used interchangeably for ACMC assessments. Again, the ability measures may vary more for non-full-time users than for full-time users. If time allows, two standardized activities can be used in one ACMC assessment because this

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 65
provides more opportunities for the rater to observe the items and rate them accurately.
The ACMC is designed to indicate changes between assessments. The MDC95 can serve as a guideline to indicate change. However, the results of test-retest reliability show that non-full-time users tend to demonstrate larger variation than do full-time users. This means that ACMC raters must consider the pros-thetic wearing time when interpreting changes between assessments because we know that prosthesis users may decrease or increase their wearing time for various reasons, such as skin rashes or motivation. Furthermore, the MDC95 is calculated based on ratings from experienced raters; therefore, a new rater should give himself/herself a wider margin.
6.9.2 Selection of an appropriate outcome measure Clinicians caring for patients with UL prosthetics often encounter individuals with various body function impairments, activity limitations, and participa-tion restrictions. Therefore, diverse outcome measures capable of addressing different areas are needed. The content comparison provides a clear picture of similarities and differences among the measures and can be used as a guide to select an appropriate outcome measure for clinical evaluations. The comparison highlights the use of a mixture of outcome measures to cover different aspects of health and functioning. Because of busy clinical routines, it is not always possible to use several tools during a single visit. One way to overcome this problem could be to ask the clients to fill in the questionnaire in advance (via post), and the clinicians then go through it with the clients during the visit. The clinician can then select one of the observational tool measures based on his/her evaluation aim. Although more work on all of the prosthetic outcome measures is required, as suggested by Hubbard132 at the SSC in 2009, now is the time to try out the newly developed validated outcome measures, use them in a consistent man-ner, and see if they are clinically useful. The instrument developer is responsi-ble for providing evidence for the instrument,105 but the test users (i.e., clini-cians and other prosthetic professionals) are responsible for judging whether the ACMC and other outcome measures are able to produce valid and relia-ble measurements that help them to make clinical decisions and demonstrate the effect of prosthetic fitting.

66 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
7 Conclusion Based on the evidence in this thesis, the ACMC can be recommended to measure the ability to control a myoelectric hand. Compared with 5 years ago, before this doctoral project, more evidence has been gathered to support the use of the ACMC to measure the ability to control a myoelectric hand. Of all evidence reported in this thesis, the strongest is the unidimensionality of the ACMC. The ACMC items have sufficient technical qualities, and the item difficulty hierarchy matches clinical experience. Reliability evidence also sup-ports the stability of the ACMC measures. Furthermore, the use of a mixture of outcome measures is recommended to cover different aspects of health.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 67
Summary in Swedish (Svensk sammanfattning) Instrumentet Assessment of Capacity for Myoelectric Control (ACMC) har tidigare utvecklats för att följa hur personer med handprotes utvecklar för-mågan att styra protesen. Bedömningen sker genom skattning av flera be-dömningspunkter på en 4-gradig skala. Trots att ACMC tidigare har visat god validitet och reliabilitet så behöver vidare psykometrisk evidens hos ACMC sökas. Under de senaste åren har även flera andra instrument inom handprotesfältet utvecklats. Frågan är vad dessa instrument mäter, vilka är deras likheter och skillnader? Det är viktigt att veta vad instrumenten fångar upp, dels för att kunna välja rätt metod för rätt fråga, och dels för att kunna studera flera aspekter av protesanvändningen. Ett sätt att studera detta är att jämföra instrumentens item/frågor genom att länka bedömningspunkterna till Klassifikation av funktionstillstånd, funktionshinder och hälsa (ICF). Syftet med denna avhandling var därför att söka psykometriska evidens för ACMC samt att jämföra de instrument som utvecklats för bedömning av handprotesanvändare. Bedömningar av personer i olika åldrar och med olika kön som använder myoelektrisk handprotes ingick i de tre första studierna. Rasch-analys och reliabilitetsstatistik användes för att analysera data och studera om i) ACMC är endimensionell, ii) om instrumentet fungerar olika för personer beroende på protessida, kön eller ålder, iii) om den 4-gradiga bedömningsskalan fungerar optimalt, iv) om protesanvändares ACMC-värde är lika oavsett vilken standardiserad aktivitet som utförs, samt för att studera v) stabilitet i upprepade mätningar. I studie IV gjordes en sökning i olika vetenskapliga databaser för att finna litteratur som beskriver instrument för bedömning av handprotes-användare. De instrument som validerats specifikt för dessa personer valdes ut för jämförelse. Genom att länka begreppen i varje bedömningspunkt till motsvarande ICF kategori kunde de områden som in-strumenten täcker kartläggas. Resultaten visar att ACMC är endimensionellt. Alla bedömningspunkter fun-gerar lika för personer oavsett protessida men tre bedömningspunkter funge-rar olika gällande kön. Den 4-gradiga bedömningsskalan fungerar överlag väl men ett skalsteg användes betydligt mindre än de tre andra. Som en följd av detta har en ny version av ACMC utvecklats. Tester av den nya versionen visade att ACMC-värdena är jämförbara oberoende av vilken av de standar-diserade aktiviteterna som används. Bedömar-reliabiliteten är hög och ICC för test-retest reliabilitet är excellent. Åtta instrument hittades i litteraturen och jämförelse mellan dem visar att de har liknande fokus. Bedömingspunk-

68 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
terna kopplades till ICF-kategorierna gällande ‘Kroppsfunktioner’, ‘Aktivitet och delaktighet’ och ‘Omgivningsfaktorer’. Konklusionen är att användning av flera instrument rekommenderas för att mäta olika aspekter av hälsa hos protesanvändare. Baserat på evidensen i den avhandling, kan ACMC rekommenderas för att mäta förmågan att styra en myoelektrisk handprotes.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 69
Acknowledgements As I reflect on the journey I have taken to get to this point, I can’t believe this day has finally arrived. There were certainly times when I didn’t think I could accomplish this task but when I look at the twinkling stars in cold Swedish winter and listen to singing birds in beautiful Swedish summer, I know that the Lord is always with me. A myriad of people have contributed their time and effort into this project and some of you have encouraged me in a personal way. I would like express my heartfelt gratitude to you. All the participants who took part in the studies. Without your effort and time, I would not be able to complete this task! My main supervisor Liselotte Hermansson, who invited me onboard this adventurous journey, introduced me to the prosthetic field, and allowed me to dissect the ACMC into pieces. I really appreciate your knowledge in UL pros-thetics and how to combine clinical work and research work together. One highlight for me was travelling with you to different prosthetic conferences. My co-supervisor Ann-Christin Eliasson, for your eagle eyes in finding flaws in my writing and your valuable advice on psychometrics and study II.
My co-supervisor Ann Langius Eklöf, for your understanding and encour-agement during tough times, for your valuable advice for study III and for the thesis. Mike Linacre, for sharing your Rasch knowledge so generously and for work-ing together with me in Study I. Birgitta Sjöqvist Nättelund, for sharing your knowledge on the ICF paper. Wendy Hill, for your advice in developing standardized activities and your tremendous help in my thesis writing. Ulrika Malm, Lis Sjöberg and Karin Eriksson, for your enormous help in data collection at the LDAPC; Anette Nilsson, for helping me with different de-tails; Eric Stenninger and Monica Åsberg, for your support of this project. Maria Nilseryd, Christina Ragnö and Anita Stockselius from the Red Cross Hospital. Thanks for all your help in data collection in Study III.

70 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
Marie Holmefur, Mats Eriksson, and Gustav Jarl, for your valuable advice on my thesis and Margareta Möller for your instant help! A special thanks to the Health Care Sciences Postgraduate School for the 4 years doctoral grant and the scholarship from Promobilia foundation. My lovely ‘HFC’ colleagues at the Centre for Rehabilitation Research. A spe-cial thanks to Lars-Olov Lundqvist for including me as part of the team. I have really enjoyed our time together, such as our serious seminars and our crayfish outing at Hjälmaren. A big hug to my roommate Christina, for your emotional support and life chats at our little corner. It has been really tough at the end of this journey and I especially want to thank Karin, Marie M, Siv and Rose-Marie for lending me your shoulders. Many of you who work in S-huset have encouraged me at different times during this journey and I am grateful to have met all of you. In particular, I want to thank Tabita Björk, for being my mentor and guiding me with your experience; Fredrik Holländare, for lending me your ears and encouraging me with your wise words; Carmen Strömberg (Katie), for always taking time to chat with me when I needed a break. Ayako Hiyoshi, for your friendship and help in finding flaws in the thesis. My international friends in my home group – especially Viendo, Joakim, Ida, Breezy, Kaddy, Jeena, Shalil, Sravanthi, Peter and thanks to David Kumar for finding flaws in the thesis. Thanks for being my extended family in Sweden and your enormous support for this journey. I truly love your FB stickers! My father Man Kit, the first doctor I met in my life, and my mother Sau Kuen, the best cook in the world. I am so lucky to have you as parents and you have taught me perseverance. Thanks to Sam, Stacey and especially An-nie, that has encouraged me throughout this journey. My in-laws Torgny and Eva, who encouraged me to step on this journey. Thanks for your support and prayers during this whole time. My cool David, my rock and my life companion. Thank you for being so supportive throughout this journey. My princess Hanna, thank you so much for taking care of your little brother when Daddy and Mommy are tired. My funny Josef, who came to this world after one year of my PhD study. It is not easy for you to understand why Mommy is so busy lately. Soon and very soon, I will have more time to play with you.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 71
References 1. Watve S, Dodd G, MacDonald R, Stoppard ER. Upper limb
prosthetic rehabilitation. Orthop Trauma 2011;25(2):135-42. 2. Plettenburg DH. Upper extremity prosthetics: current status and
evaluation. VSSD Delft, The Netherlands; 2006, P.19. 3. Hubbard S, Stocker D, Heger H. 'Training'. In: Powered Upper Limb
prostheses: Control, Implementation and Clinical Application. Ed. by Muzumdar. A: Springer-Verlag; 2004, P.147-174.
4. Hermansson LM, Fisher AG, Bernspang B, Eliasson AC. Assessment of capacity for myoelectric control: a new Rasch-built measure of prosthetic hand control. J Rehabil Med 2004;37(3):166-71.
5. Merriam-Webster Online: Dictionary and Thesaurus. 2013 [cited 2013 July 01]. Available from: www.merriam-webster.com.
6. World Health Organisation. Towards a Common Language for Functioning, Disability and Health: ICF The International Classification of Functioning, Disability and Health - ICF beginner guide; 2002.
7. Lovely DF. The origin and nature of myoelectric signal. In: Powered Upper Limb Prostheses: Control, Implementation and Clinical Application. Ed. by Muzumdar. A. Springer-Verlag; 2004. p. 17.
8. Soares AB, Berzin F, Andrade AO. Power spectrum estimation of EMG signals via Chirp-Z transform. Proceedings of the XIVth Congress of the International Society of Electrophysiology and Kinesiology; 2002, P.43.
9. World Health Organisation. International Classification of Functioning, Disability and Health (ICF). Geneva, Switzerland: World Health Organisation; 2001, P.15 and P.236.
10. Burger H. Can the International Classification of Functioning, Disability and Health (ICF) be used in a prosthetics and orthotics outpatient clinic? Prosthet Orthot Int 2011;35(3):302-9.
11. Parker K, Kirby RL, Adderson J, Thompson K. Ambulation of people with lower-limb amputations: relationship between capacity and performance measures. Arch Phys Med Rehabil 2010;91(4):543-9.
12. Dawson MR, Fahimi F, Carey JP. The development of a myoelectric training tool for above-elbow amputees. Open Biomed Eng J 2012;6:5-15.
13. Aucourt J, Budzik JF, Manouvrier-Hanu S, Mezel A, Cotten A, Boutry N. Congenital malformations of the hand and forearm in children: what radiologists should know. Semin Musculoskelet Radiol 2012;16(2):146-58.
14. Ephraim PL, Dillingham TR, Sector M, Pezzin LE, Mackenzie EJ. Epidemiology of limb loss and congenital limb deficiency: a review of the literature. Arch Phys Med Rehabil 2003;84(5):747-61.

72 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
15. Hermansson LM. Upper limb reduction deficiencies in Swedish children. Classification, prevalence and function with myoelectric prostheses (Doctoral Thesis). Stockholm: Karolinska Institutet; 2004, P.10-31.
16. Lake A. Hand therapy for children with congenital hand differences. Tech Hand Up Extrem Surg 2010;14(2):78-84.
17. Nelson VS, Flood KM, Bryant PR, Huang ME, Pasquina PF, Roberts TL. Limb Deficiency and Prosthetic Management. 1. Decision Making in Prosthetic Prescription and Management. Arch Phys Med Rehabil 2006;87(3, Supplement):3-9.
18. Scott RN, Parker PA. Myoelectric prostheses: state of the art. J Med Eng Technol 1988;12(4):143-51.
19. Davids JR, Wagner LV, Meyer LC, Blackhurst DW. Prosthetic management of children with unilateral congenital below-elbow deficiency. J Bone Joint Surg Am 2006; 88(6):1294-300.
20. Biddiss E, Andrysek J. 'Upper and lower extremity prosthetics for children and youth' In: Paediatric Rehabilitation Engineering: from Disability to Possibility. Ed. by Chau, T. and Fairley, J. CRC Press; 2011, P.189-239.
21. Meurs M, Maathuis CG, Lucas C, Hadders-Algra M, van der Sluis CK. Prescription of the first prosthesis and later use in children with congenital unilateral upper limb deficiency: A systematic review. Prosthet Orthot Int 2006;30(2):165-73.
22. Wright FV, Hubbard S, Naumann S, Jutai J. Evaluation of the validity of the prosthetic upper extremity functional index for children. Arch Phys Med Rehabil 2003;84(4):518-27.
23. Jain S. Rehabilitation in limb deficiency. 2. The pediatric amputee. Arch Phys Med Rehabil 1996;77(3, Supplement):S9-S13.
24. Shaperman JMOTR, Landsberger SES, Setoguchi YMD. Early Upper Limb Prosthesis Fitting: When and What Do We Fit. J Prosthet Orthot 2003;15(1):11-7.
25. Sorbye R. Myoelectric prosthetic fitting in young children. Clin Orthop Relat Res 1980(148):34-40.
26. Brugger P, Kollias SS, Muri RM, Crelier G, Hepp-Reymond MC, Regard M. Beyond re-membering: phantom sensations of congenitally absent limbs. Proc Natl Acad Sci U S A 2000;97(11):6167-72.
27. Reilly KT, Sirigu A. Motor cortex representation of the upper-limb in individuals born without a hand. PLoS One 2011;6(4):e18100.
28. Kohler F, Cieza A, Stucki G, Geertzen J, Burger H, Dillon MP, et al. Developing Core Sets for persons following amputation based on the International Classification of Functioning, Disability and Health as a way to specify functioning. Prosthet Orthot Int 2009;33(2):117-29.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 73
29. Anderson NJ, Bonauto DK, Adams D. Work-related amputations in Washington state, 1997-2005. Am J Ind Med 2010;53(7):693-705.
30. Krueger CA, Wenke JC, Ficke JR. Ten years at war: comprehensive analysis of amputation trends. J Trauma Acute Care Surg 2012;73(6 Suppl 5):S438-44.
31. Atroshi I, Rosberg HE. Epidemiology of amputations and severe injuries of the hand. Hand Clin 2001;17(3):343-50, vii.
32. Asplund M, Nilsson M, Jacobsson A, von Holst H. Incidence of traumatic peripheral nerve injuries and amputations in Sweden between 1998 and 2006. Neuroepidemiology 2009;32(3):217-28.
33. Bhaskaranand K, Bhat AK, Acharya KN. Prosthetic rehabilitation in traumatic upper limb amputees (an Indian perspective). Arch Orthop Trauma Surg 2003;123(7):363-6.
34. Dillingham TR, Pezzin LE, MacKenzie EJ. Limb amputation and limb deficiency: epidemiology and recent trends in the United States. South Med J 2002;95(8):875-83.
35. Esquenazi A. Amputation rehabilitation and prosthetic restoration. From surgery to community reintegration. Disabil Rehabil 2004;26(14-15):831-6.
36. Raichle KA, Hanley MA, Molton I, Kadel NJ, Campbell K, Phelps E, et al. Prosthesis use in persons with lower- and upper-limb amputation. J Rehabil Res Dev 2008;45(7):961-72.
37. Tintle SM, Baechler MF, Nanos GP, 3rd, Forsberg JA, Potter BK. Traumatic and trauma-related amputations: Part II: Upper extremity and future directions. J Bone Joint Surg Am 2010;92(18):2934-45.
38. Preissler S, Dietrich C, Blume KR, Hofmann GO, Miltner WH, Weiss T. Plasticity in the Visual System is Associated with Prosthesis Use in Phantom Limb Pain. Front Hum Neurosci 2013;7:311.
39. Lake C, Dodson R. Progressive upper limb prosthetics. Phys Med Rehabil Clin N Am 2006;17(1):49-72.
40. Clement RG, Bugler KE, Oliver CW. Bionic prosthetic hands: A review of present technology and future aspirations. Surgeon 2011;9(6):336-40.
41. Parker P, Englehart K, Hudgins B. Myoelectric signal processing for control of powered limb prostheses. J Electromyogr Kinesiol 2006;16(6):541-8.
42. Stubblefield KA, Miller LA, Lipschutz RD, Kuiken TA. Occupational therapy protocol for amputees with targeted muscle reinnervation. J Rehabil Res Dev 2009;46(4):481-8.
43. Lake C. The Evolution of Upper Limb Prosthetic Socket Design. J Prosthet Orthot 2008;20(3):85-92.
44. Fougner A, Stavdahl O, Kyberd PJ, Losier YG, Parker PA. Control of upper limb prostheses: terminology and proportional myoelectric

74 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
control-a review. IEEE Trans Neural Syst Rehabil Eng 2012;20(5):663-77.
45. Kyberd PJ. The influence of control format and hand design in single axis myoelectric hands: assessment of functionality of prosthetic hands using the Southampton Hand Assessment Procedure. Prosthet Orthot Int 2011;35(3):285-93.
46. Dosen S, Cipriani C, Kostic M, Controzzi M, Carrozza MC, Popovic DB. Cognitive vision system for control of dexterous prosthetic hands: experimental evaluation. J Neuroeng Rehabil 2010;7:42.
47. Hubbard S, Heim W, Naumann S, Glasford S, Montgomery G, Ramdial S. 'Powered Upper Limb Prosthetic Practice in Paediatrics'. In: Powered Upper Limb Prostheses Control, Implementation and Clinical Application. Ed. by Muzumdar, A: Springer-Verlag; 2004, P.85-115.
48. Bongers RMP, Kyberd PJP, Bouwsema HM, Kenney LPJP, Plettenburg DHP, Van der Sluis CKP. Bernstein's Levels of Construction of Movements Applied to Upper Limb Prosthetics. J Prosthet Orthot April 2012;24(2):67-76.
49. Dawson MR, Carey JP, Fahimi F. Myoelectric training systems. Expert Rev Med Devices 2011;8(5):581-9.
50. Ballance R, Wilson BN, Harder JA. Factors affecting myoelectric prosthetic use and wearing patterns in the junvenile unilateral below-elbow amputee. Can J Occup Ther 1989;56(No.3):132-7.
51. Hermansson LM. Structured training of children fitted with myoelectric prostheses. Prosthet Orthot Int 1991;15(2):88-92.
52. Hubbard S, Galway HR, Milner M. Myoelectric training methods for the preschool child with congenital below-elbow amputation. A comparison of two training programmes. J Bone Joint Surg Br 1985;67(2):273-7.
53. Smurr LM, Gulick K, Yancosek K, Ganz O. Managing the upper extremity amputee: a protocol for success. J Hand Ther 2008;21(2):160-75; quiz 76.
54. Yuen HK, Nelson DL, Peterson CQ, Dickinson A. Prosthesis training as a context for studying occupational forms and motoric adaptation. Am J Occup Ther 1994;48(1):55-61.
55. Meredith JM, Uellendahl JE, Keagy RD. Successful voluntary grasp and release using the cookie crusher myoelectric hand in 2-year-olds. Am J Occup Ther 1993;47(9):825-9.
56. Dromerick AW, Schabowsky CN, Holley RJ, Monroe B, Markotic A, Lum PS. Effect of training on upper-extremity prosthetic performance and motor learning: a single-case study. Arch Phys Med Rehabil 2008;89(6):1199-204.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 75
57. Korkmaz M, Erbahceci F, Ulger O, Topuz S. Evaluation of functionality in acquired and congenital upper extremity child amputees. Acta Orthop Traumatol Turc 2012;46(4):262-8.
58. Simon AM, Lock BA, Stubblefield KA. Patient training for functional use of pattern recognition-controlled prostheses. J Prosthet Orthot 2012;24(2):56-64.
59. Wallace S, Weeks DL, Foo P. A Dynamic Systems Approach to Understanding Reaching Movements with a Prosthetic Arm. Nonlinear Dynamics, Psychology, and Life Sciences 2000;4(4):311-38.
60. Wallace SA, Anderson DI, Hall P, Ryan G, McBride N, McGarry T, et al. Weight Discrimination Using an Upper-Extremity Prosthesis. J Prosthet Orthot 2002;14(3):127-33.
61. Wallace SA, Anderson DI, Trujillo M, Weeks DL. Upper Extremity Artificial Limb Control as an Issue Related to Movement and Mobility in Daily Living. Quest 2005;57(1):124-37.
62. Weeks DL, Anderson DI, Wallace SA. The Role of Variability in Practice Structure when Learning to Use an Upper-Extremity Prosthesis. J Prosthet Orthot 2003;15(3):84-92.
63. Weeks DL, Wallace SA, Anderson DI. Training with an upper-limb prosthetic simulator to enhance transfer of skill across limbs. Arch Phys Med Rehabil 2003;84(3):437-43.
64. Bouwsema H, van der Sluis CK, Bongers RM. The role of order of practice in learning to handle an upper-limb prosthesis. Arch Phys Med Rehabil 2008;89(9):1759-64.
65. Bouwsema H, van der Sluis CK, Bongers RM. Learning to control opening and closing a myoelectric hand. Arch Phys Med Rehabil 2010;91(9):1442-6.
66. Bouwsema H, van der Sluis CK, Bongers RM. Movement characteristics of upper extremity prostheses during basic goal-directed tasks. Clin Biomech (Bristol, Avon) 2010;25(6):523-9.
67. Romkema S, Bongers RM, van der Sluis CK. Intermanual transfer in training with an upper-limb myoelectric prosthesis simulator: a mechanistic, randomized, pretest-posttest study. Phys Ther 2013;93(1):22-31.
68. Bouwsema H, Kyberd PJ, Hill W, van der Sluis CK, Bongers RM. Determining skill level in myoelectric prosthesis use with multiple outcome measures. J Rehabil Res Dev 2012;49(9):1331-48.
69. Cipriani C, Sassu R, Controzzi M, Carrozza MC. Influence of the weight actions of the hand prosthesis on the performance of pattern recognition based myoelectric control: preliminary study. Conf Proc IEEE Eng Med Biol Soc 2011;2011:1620-3.
70. Sears HH, Shaperman J. Proportional myoelectric hand control: an evaluation. Am J Phys Med Rehabil 1991;70(1):20-8.

76 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
71. Peerdeman B, Boere D, Witteveen H, Veld RH, Hermens H, Stramigioli S, et al. Myoelectric forearm prostheses: State of the art from a user-centered perspective. J Rehabil Res Dev 2011;48(6):719-38.
72. Geng Y, Zhou P, Li G. Toward attenuating the impact of arm positions on electromyography pattern-recognition based motion classification in transradial amputees. J Neuroeng Rehabil 2012;9:74.
73. Jiang N, Muceli S, Graimann B, Farina D. Effect of arm position on the prediction of kinematics from EMG in amputees. Med Biol Eng Comput 2013;51(1-2):143-51.
74. Carey SL, Jason Highsmith M, Maitland ME, Dubey RV. Compensatory movements of transradial prosthesis users during common tasks. Clin Biomech (Bristol, Avon) 2008;23(9):1128-35.
75. Metzger AJ, Dromerick AW, Holley RJ, Lum PS. Characterization of Compensatory Trunk Movements During Prosthetic Upper Limb Reaching Tasks. Arch Phys Med Rehabil 2012;93(11):2029-34.
76. Silcox DH, 3rd, Rooks MD, Vogel RR, Fleming LL. Myoelectric prostheses. A long-term follow-up and a study of the use of alternate prostheses. J Bone Joint Surg Am 1993;75(12):1781-9.
77. Millstein SG, Heger H, Hunter GA. Prosthetic use in adult upper limb amputees: a comparison of the body powered and electrically powered prostheses. Prosthet Orthot Int 1986;10(1):27-34.
78. Sörbye R. What normality means to a girl called Aasa. New Scientist Mar 1978;1093:659.
79. Resnik L, Etter K, Klinger SL, Kambe C. Using virtual reality environment to facilitate training with advanced upper-limb prosthesis. J Rehabil Res Dev 2011;48(6):707-18.
80. Biddiss E, Chau T. The roles of predisposing characteristics, established need, and enabling resources on upper extremity prosthesis use and abandonment. Disabil Rehabil Assist Technol 2007;2(2):71-84.
81. Hebert JS, Lewicke J. Case report of modified Box and Blocks test with motion capture to measure prosthetic function. J Rehabil Res Dev 2012;49(8):1163-74.
82. Hill W, Kyberd P, Norling Hermansson L, Hubbard S, Stavdahl Ø, Swanson S. Upper Limb Prosthetic Outcome Measures (ULPOM): A Working Group and Their Findings. J Prosthet Orthot 2009;21 (9):69-82.
83. Wright FV. Proshtetic outcome measures for use with upper limb amputees: A systematic review of the peer-reviewed literature, 1970-2009. J Prosthet Orthot 2009;21(9):3-63.
84. Hermansson LM. Assessment of Capacity for Myoelectric Control - version 1.0. In. Örebro, Sweden; 2000.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 77
85. Hermansson L. The ACMC website. 2006 [cited 2013- 07-17]. Available from: http://www.acmc.se/.
86. Wright FV. Measurement of functional outcome with individuals who use upper extremity prosthetic devices: current and future directions. J Prosthet Orthot 2006;18(2):46-56.
87. Fraser CM. An evaluation of the use made of cosmetic and functional prostheses by unilateral upper limb amputees. Prosthet Orthot Int 1998;22(3):216-23.
88. Davidson J. A survey of the satisfaction of upper limb amputees with their prostheses, their lifestyles, and their abilities. J Hand Ther 2002;15(1):62-70.
89. Ostlie K, Lesjo IM, Franklin RJ, Garfelt B, Skjeldal OH, Magnus P. Prosthesis use in adult acquired major upper-limb amputees: patterns of wear, prosthetic skills and the actual use of prostheses in activities of daily life. Disabil Rehabil Assist Technol 2012.
90. DeVillis RF. Scale Development: Theory and Applications (Applied Social Research Methods) SAGE Publications, Inc.; 2012, P.159-183.
91. Engelhard GJ. Invariant Measurement: Using Rasch Models in the Social, Behavioral, and Health Sciences. New York: Routledge; 2013, P.3-23.
92. Linacre JM, Wright BD. The "Length" of a Logit. Rasch Measurement Transactions 1989;3(2):54-5.
93. Streiner DN, G. Health Measurement Scales: a practical guide to their development and use. 4th ed: Oxford University Press; 2008, P.299-330.
94. Linacre JM. Optimizing Rating Scale Category Effectiveness. J Appl Meas 2002;3:1:85-106.
95. Khadka J, Gothwal VK, McAlinden C, Lamoureux EL, Pesudovs K. The importance of rating scales in measuring patient-reported outcomes. Health Qual Life Outcomes 2012;10:80.
96. Bond TG, Fox CM. Applying the Rasch model: fundamental measurement in the human sciences. 2nd ed. Mahwah, N.J.: Lawrence Erlbaum Associates 2007, P.29-48.
97. Eckes T. Introduction to Many-Facet Rasch Measurement: Analyzing and Evaluating Rater-Mediated Assessments: Peter Lang Publishing Group; 2011, P.7-20.
98. Heinemann AW, Bode RK, O'Reilly C. Development and measurement properties of the Orthotics and Prosthetics Users' Survey (OPUS): a comprehensive set of clinical outcome instruments. Prosthet Orthot Int 2003;27(3):191-206.
99. da Rocha NS, Chachamovich E, de Almeida Fleck MP, Tennant A. An introduction to Rasch analysis for Psychiatric practice and research. J Psychiatr Res 2013;47(2):141-8.
100. Wright BD, Stone MH. Best test design. Chicago: MESA; 1979, P.69.

78 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
101. Linacre JM. Rasch Measures and Unidimensionality. Rasch Measurement Transactions 2011;24(4):1310.
102. Wolfe EW, Smith EV, Jr. Instrument development tools and activities for measure validation using Rasch models: part II--validation activities. J Appl Meas 2007;8(2):204-34.
103. Wright B, Linacre J. Reasonable mean-square fit values. Rasch Measurement Transactions 1994;8:3:370.
104. Messick S. Validity of psychological assessment: Validation of inferences from persons' responses and performances as scientific inquiry into score meaning. The American Psychologist 1995;50(9):741 - 9.
105. American Educational Research Association, American Psychological Association, National Council on Measurement in Education. Standards for educational and psychological testing: Washington, DC: American Psychological Association; 1999, P.9-36.
106. Brown T. Construct Validity: A Unitary Concept for Occupational Therapy Assessment and Measurement. Hong Kong J Occup Ther 2010;20(1):30-42.
107. Nielsen DG, Gotzsche O, Eika B. Objective structured assessment of technical competence in transthoracic echocardiography: a validity study in a standardised setting. BMC Med Educ 2013;13:47.
108. Smith EV, Jr. Evidence for the reliability of measures and validity of measure interpretation: a Rasch measurement perspective. J Appl Meas 2001;2(3):281-311.
109. Fisher WPJ. Rating Scale Instrument Quality Criteria. Rasch Measurement Transactions 2007;21:1 P. 1095.
110. Messick S. Validity and washback in language testing. Language Testing 1996;13(3):241-56.
111. Wolfe EW, Smith EV, Jr. Instrument development tools and activities for measure validation using Rasch models: part I - instrument development tools. J Appl Meas 2007;8(1):97-123.
112. Linacre JM. Predicting Responses from Rasch Measures. J Appl Meas 2010;11(1):1-11.
113. Goodwin LD. Changing conceptions of measurement validity: an update on the new standards. J Nurs Educ 2002;41(3):100-6.
114. Linacre JM. Detecting multidimensionality: which residual data-type works best? J Outcome Meas 1998;2(3):266-83.
115. Smith EV, Jr. Detecting and evaluating the impact of multidimensionality using item fit statistics and principal component analysis of residuals. J Appl Meas 2002;3(2):205-31.
116. Cook DA, Beckman TJ. Current concepts in validity and reliability for psychometric instruments: theory and application. Am J Med 2006;119(2):166 e7-16.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 79
117. Goodwin LD, Leech NL. The Meaning of Validity in the New "Standards for Educational and Psychological Testing": Implications for Measurement Courses. Measurement and Evaluation in Counselling and Development 2003;36(October):181-91.
118. Gaine WJ, Smart C, Bransby-Zachary M. Upper limb traumatic amputees. Review of prosthetic use. J Hand Surg Br 1997;22(1):73-6.
119. Jang CH, Yang HS, Yang HE, Lee SY, Kwon JW, Yun BD, et al. A survey on activities of daily living and occupations of upper extremity amputees. Ann Rehabil Med 2011;35(6):907-21.
120. Jones LE, Davidson JH. The long-term outcome of upper limb amputees treated at a rehabilitation centre in Sydney, Australia. Disabil Rehabil 1995;17(8):437-42.
121. Kejlaa GH. Consumer concerns and the functional value of prostheses to upper limb amputees. Prosthet Orthot Int 1993;17(3):157-63.
122. Burger H, Franchignoni F, Heinemann AW, Kotnik S, Giordano A. Validation of the orthotics and prosthetics user survey upper extremity functional status module in people with unilateral upper limb amputation. J Rehabil Med 2008;40(5):393-9.
123. Dudkiewicz I, Gabrielov R, Seiv-Ner I, Zelig G, Heim M. Evaluation of prosthetic usage in upper limb amputees. Disabil Rehabil 2004;26(1):60-3.
124. Hubley A, Zumbo B. Validity and the Consequences of Test Interpretation and Use. Social Indicators Research 2011;103(2):219-30.
125. Downing SM. Reliability: on the reproducibility of assessment data. Med Educ 2004;38(9):1006-12.
126. Streiner DN, G. Health measurement scales. A practical guide to their development and use. 4th ed: Oxford University Press; 2008, P.167-210.
127. Hermansson LM, Bodin L, Eliasson AC. Intra- and inter-rater reliability of the assessment of capacity for myoelectric control. J Rehabil Med 2006;38(2):118-23.
128. de Vet HC, Terwee CB. The minimal detectable change should not replace the minimal important difference. J Clin Epidemiol 2010;63(7):804-5; author reply 6.
129. de Vet HC, Terwee CB, Ostelo RW, Beckerman H, Knol DL, Bouter LM. Minimal changes in health status questionnaires: distinction between minimally detectable change and minimally important change. Health Qual Life Outcomes 2006;4:54.
130. Buffart LM, Roebroeck ME, Pesch-Batenburg JM, Janssen WG, Stam HJ. Assessment of arm/hand functioning in children with a congenital transverse or longitudinal reduction deficiency of the upper limb. Disabil Rehabil 2006;28(2):85-95.

80 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
131. Heinemann AW, Fisher WP, Gershon R. Improving Health Care Quality with Outcomes Management. Journal of Prosthetics and Orthotics 2006;18( 1S): 46-50.
132. Hubbard S. Pediatric Upper Limb Outcome Measurement. Journal of Prosthetics and Orthotics 2009;21(4S):64-8.
133. Miller LA, Swanson S. Introduction to the Academy's State of the Science Conference on Upper Limb Prosthetic Outcome Measures. J Prosthet Orthot 2009;21(nr 4S):P1-P2
134. Miller L, Swanson S. Summary and Recommendations of the Academy's State of the Science Conference on Upper Limb Prosthetic Outcome Measures. J Prosthet Orthot 2009;21(nr 4S):83-9.
135. Williams TW, 3rd. Progress on stabilizing and controlling powered upper-limb prostheses. J Rehabil Res Dev 2011;48(6):ix-xix.
136. World Health Organisation. International Classification of Functioning, Disability and Health (ICF). Geneva, Switzerland; 2001.
137. James MA, Bagley AM, Brasington K, Lutz C, McConnell S, Molitor F. Impact of prostheses on function and quality of life for children with unilateral congenital below-the-elbow deficiency. J Bone Joint Surg Am 2006;88(11):2356-65.
138. Gallagher P, O'Donovan MA, Doyle A, Desmond D. Environmental barriers, activity limitations and participation restrictions experienced by people with major limb amputation. Prosthet Orthot Int 2011;35(3):278-84.
139. Cieza A, Stucki G. Content comparison of health-related quality of life (HRQOL) instruments based on the international classification of functioning, disability and health (ICF). Qual Life Res 2005;14(5):1225-37.
140. Stucki A, Cieza A, Schuurmans MM, Ustun B, Stucki G, Gradinger F, et al. Content comparison of health-related quality of life instruments for obstructive sleep apnea. Sleep Med 2008;9(2):199-206.
141. Stucki G, Cieza A. The International Classification of Functioning, Disability and Health (ICF) Core Sets for rheumatoid arthritis: a way to specify functioning. Ann Rheum Dis 2004;63 Suppl 2:ii40-ii5.
142. Miller LA, McIntire SA, Lovler RL. Foundations of Psychological Testing: A Practical Approach. 4th ed: SAGE Publications; 2013, P.157-189.
143. Altman DG, Bland JM. Treatment allocation by minimisation. BMJ 2005;330(7495):843.
144. Linacre JM. Winsteps®Rasch measurement computer program. In. Winsteps Beaverton, Oregon: Winsteps.com; 2008.
145. Linacre JM. Winsteps Help for Rasch analysis: Standard error model and real [cited 2013-08-02]. Available from: http://www.winsteps.com/winman/index.htm?standarderrors.htm.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 81
146. Linacre JM. What do Infit and Outfit, Mean-square and Standardized mean? Rasch Measurement Transactions 2002;16(2):878.
147. Linacre JM. Winsteps® Rasch measurement computer program User's Guide In. Beaverton, Oregon: Winsteps.com; 2008.
148. Linacre JM, Wright BD. Reasonable mean-square fit values. Rasch Measurement Transactions 1994(8):370.
149. Linacre JM. Differential Item Functioning DIF Sample Size Nomogram. Rasch Measurement Transactions 2013;6:4 P. 1391
150. Linacre JM. Facets computer program for many-facet Rasch measurement version 3.7.1.0. . In. Beaverton, Oregon: Winsteps.com; 2013.
151. Tristan A. An adjustment for sample size in DIF analysis. Rasch Measurement Transactions 2006;20(3):1070-71.
152. Sanderson E, Scott R. UNB test of prosthetic function: a test for unilateral amputees (test manual). In: Fredericton, New Brunswick, Canada, University of New Brunswick; 1985.
153. Law M, MacDermid J. Evidence-Based Rehabilitation: a guide to practice. Hamilton, Ontario, Canada: Slack Incorporated; 2008, P.387-392.
154. Forhan M, Vrkljan B, MacDermid J. A systematic review of the quality of psychometric evidence supporting the use of an obesity-specific quality of life measure for use with persons who have class III obesity. Obes Rev 2010;11(3):222-8.
155. MacDermid JC, Walton DM, Avery S, Blanchard A, Etruw E, McAlpine C, et al. Measurement properties of the neck disability index: a systematic review. J Orthop Sports Phys Ther 2009;39(5):400-17.
156. Roy JS, MacDermid JC, Woodhouse LJ. Measuring shoulder function: a systematic review of four questionnaires. Arthritis Rheum 2009;61(5):623-32.
157. Cieza A, Brockow T, Ewert T, Amman E, Kollerits B, Chatterji S, et al. Linking health-status measurements to the international classification of functioning, disability and health. J Rehabil Med 2002;34(5):205-10.
158. Cieza A, Geyh S, Chatterji S, Kostanjsek N, Ustun B, Stucki G. ICF linking rules: an update based on lessons learned. J Rehabil Med 2005;37(4):212-8.
159. World HealthOrganisation. International Classification of Functioning, Disability and Health (ICF). Geneva, Switzerland World Health Organisation; 2001, P.142.
160. Lindner HYN, Linacre JM, Hermansson LM. Assessment of Capacity for Myoelectric Control: Evaluation of the construct and the rating scale. J Rehabil Med 2009;41(6):467-74.
82 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
161. Pruitt SD, Seid M, Varni JW, Setoguchi Y. Toddlers with limb deficiency: conceptual basis and initial application of a functional status outcome measure. Arch Phys Med Rehabil 1999;80(7):819-24.
162. Pruitt SD, Varni JW, Seid M, Setoguchi Y. Functional status in limb deficiency: development of an outcome measure for preschool children. Arch Phys Med Rehabil 1998;79(4):405-11.
163. Pruitt SD, Varni JW, Setoguchi Y. Functional status in children with limb deficiency: development and initial validation of an outcome measure. Arch Phys Med Rehabil 1996;77(12):1233-8.
164. Pruitt SD, Varni JW, Seid M, Setoguchi Y. Prosthesis satisfaction outcome measurement in pediatric limb deficiency. Arch Phys Med Rehabil 1997;78(7):750-4.
165. Wright FV, Hubbard S, Jutai J, Naumann S. The Prosthetic Upper Extremity Functional Index: development and reliability testing of a new functional status questionnaire for children who use upper extremity prostheses. J Hand Ther 2001;14(2):91-104.
166. Buffart LM, Roebroeck ME, van Heijningen VG, Pesch-Batenburg JM, Stam HJ. Evaluation of arm and prosthetic functioning in children with a congenital transverse reduction deficiency of the upper limb. J Rehabil Med 2007;39(5):379-86.
167. Desmond DM, MacLachlan M. Factor structure of the Trinity Amputation and Prosthesis Experience Scales (TAPES) with individuals with acquired upper limb amputations. Am J Phys Med Rehabil 2005;84(7):506-13.
168. Bagley AM, Molitor F, Wagner LV, Tomhave W, James MA. The Unilateral Below Elbow Test: a function test for children with unilateral congenital below elbow deficiency. Dev Med Child Neurol 2006;48(7):569-75.
169. Beckman TJ, Cook DA, Mandrekar JN. What is the validity evidence for assessments of clinical teaching? J Gen Intern Med 2005;20(12):1159-64.
170. Cook DA, Zendejas B, Hamstra SJ, Hatala R, Brydges R. What counts as validity evidence? Examples and prevalence in a systematic review of simulation-based assessment. Adv Health Sci Educ Theory Pract 2013.
171. Downing SM. Validity: on meaningful interpretation of assessment data. Med Educ 2003;37(9):830-7.
172. Morgan GA, Gliner JA, Harmon RJ. Understanding and evaluating research in applied and clinical settings: Psychology Press; 2006.
173. McDowell I, Newell C. Measuring Health: A guide to rating scales and questionnaires. Third ed: New York: Oxford University Press; 2006, P.10-46.
HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 83
174. Fendrich M, Smith EV, Jr., Pollack LM, Mackesy-Amiti ME. Measuring sexual risk for HIV: a Rasch scaling approach. Arch Sex Behav 2009;38(6):922-35.
175. Lamoureux EL, Pesudovs K, Thumboo J, Saw SM, Wong TY. An evaluation of the reliability and validity of the visual functioning questionnaire (VF-11) using Rasch analysis in an Asian population. Invest Ophthalmol Vis Sci 2009;50(6):2607-13.
176. Tesio L, Granger CV, Fiedler RC. A unidimensional pain/disability measure for low-back pain syndromes. Pain 1997;69(3):269-78.
177. Denny F, Marshall AH, Stevenson MR, Hart PM, Chakravarthy U. Rasch analysis of the daily living tasks dependent on vision (DLTV). Invest Ophthalmol Vis Sci 2007;48(5):1976-82.
178. Hsieh CL, Jang Y, Yu TY, Wang WC, Sheu CF, Wang YH. A Rasch analysis of the Frenchay Activities Index in patients with spinal cord injury. Spine 2007;32(4):437-42.
179. Page SJ, Shawaryn MA, Cernich AN, Linacre JM. Scaling of the revised Oswestry low back pain questionnaire. Arch Phys Med Rehabil 2002;83(11):1579-84.
180. Huizing K, Reinders-Messelink H, Maathuis C, Hadders-Algra M, van der Sluis CK. Age at first prosthetic fitting and later functional outcome in children and young adults with unilateral congenital below-elbow deficiency: a cross-sectional study. Prosthet Orthot Int 2010;34(2):166-74.
181. Resnik L, Adams L, Borgia M, Delikat J, Disla R, Ebner C, et al. Development and Evaluation of the Activities Measure for Upper Limb Amputees. Arch Phys Med Rehabil 2013;94(3):488-94.e4.
182. Rossi R, Alexander M, Cuccurullo S. Pediatric Limb Deficiencies. Physical Medicine and Rehabilitation Board Review. New York: Demos Medical Publishing; 2004 [cited 2013- 08-21]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK27239/.
183. Jain S, Lakhtakia PK. Profile of congenital transverse deficiencies among cases of congenital orthopaedic anomalies. J Orthop Surg (Hong Kong) 2002;10(1):45-52.
184. Linacre JM. Sample Size and Item Calibration Stability. Rasch Measurement Transactions 1994;7:4 328.
185. Linacre JM. A User's Guide to FACETs - Rasch-model computer programs. 2012.
186. Bonett DG. Sample size requirements for estimating intraclass correlations with desired precision. Stat Med 2002;21(9):1331-5.
187. Domholdt E. Rehabilitation Research: Principles and Applications. 3rd ed: Elsevier Saunders; 2005, P.245-264.
188. Weir JP. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res. 2005;19(1):231-40.

84 I HELEN LINDNER The Assessment of Capacity for Myoelectric Control
189. Bland JM, Altman DG. A note on the use of the intraclass correlation coefficient in the evaluation of agreement between two methods of measurement. Comput Biol Med 1990;20(5):337-40.
190. Bland JM, Altman DG. Applying the right statistics: analyses of measurement studies. Ultrasound Obstet Gynecol 2003;22(1):85-93.
191. Fleiss JL, Cohen J. The Equivalence of Weighted Kappa and the Intraclass Correlation Coefficient as Measures of Reliability. Educational and Psychological Measurement 1973;33(3):613-9.
192. Bernd T, Van Der Pijl D, De Witte LP. Existing models and instruments for the selection of assistive technology in rehabilitation practice. Scand J Occup Ther 2009;16(3):146-58.
193. Heerkens Y, Bougie T, Claus E. The use of the ICF in the process of supplying assistive products: discussion paper based on the experience using a general Dutch prescription guideline. Prosthet Orthot Int 2011;35(3):310-7.
194. Bond TG. Validity and assessment: a Rasch measurement perspective. Metodología de las Ciencias del Comportamiento 2003;5(2):179-94.
195. Beaton DE, Boers M, Wells GA. Many faces of the minimal clinically important difference (MCID): a literature review and directions for future research. Curr Opin Rheumatol 2002;14(2):109-14.
196. Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials 1989;10(4):407-15.
197. Lang CE, Edwards DF, Birkenmeier RL, Dromerick AW. Estimating minimal clinically important differences of upper-extremity measures early after stroke. Arch Phys Med Rehabil 2008;89(9):1693-700.
198. Gallagher P, Franchignoni F, Giordano A, MacLachlan M. Trinity amputation and prosthesis experience scales: a psychometric assessment using classical test theory and rasch analysis. Am J Phys Med Rehabil 2010;89(6):487-96.
199. Jarl GM, Heinemann AW, Norling Hermansson LM. Validity evidence for a modified version of the Orthotics and Prosthetics Users' Survey. Disabil Rehabil Assist Technol 2012;7(6):469-78.
200. Jarl GM, Hermansson LM. Translation and linguistic validation of the Swedish version of Orthotics and Prosthetics Users' Survey. Prosthet Orthot Int 2009;33(4):329-38.
201. Jarl G, Holmefur M, Hermansson LM. Test-retest reliability of the Swedish version of the Orthotics and Prosthetics Users' Survey. Prosthet Orthot Int 2013.

HELEN LINDNER The Assessment of Capacity for Myoelectric Control I 85
Errata Study I P.470, 3rd paragraph, line10: CI, should be 'confidence bands' P.470, Fig.2. ‘confidence intervals' and CI, should be ‘confidence bands’
Study IV P.122, Table IV – ‘Body Functions’, should be ‘Activity and Participation’


Publications in the series Örebro Studies in Care Sciences*
1. Gustafsson, Margareta (2003) Konsekvenser av en akut traumatisk handskada. En prospektiv studie av patientens situation under det första året efter olyckan. Doktorsavhandling/Doctoral thesis with focus on Nursing.
2. Jackson, Karin (2005) Att vara förälder till ett för tidigt fött barn – en prospektiv studie om upplevelsen av föräldraskap och möten med vården. Doktorsavhandling/Doctoral thesis with focus on Nursing.
3. Odencrants, Sigrid (2005) Måltidsrelaterade situationer och näringstillstånd ur patienters med kroniskt obstruktiv lungsjukdom och sjuksköterskors perspektiv. Vetenskaplig uppsats för licentiatexamen/Academic essay.
4. Göransson, Katarina (2005) Emergency department triage – a challenging task for Swedish emergency nurses. Vetenskaplig uppsats för licentiatexamen/Academic essay.
5. Eldh, Ann Catrine (2005) Patienters upplevelser av och uttryck för fenomenet delaktighet i hälso- och sjukvård. Vetenskaplig uppsats för licentiatexamen/Academic essay.
6. Florin, Jan (2005) Clinical judgement in nursing – a collaborative effort? Patient participation and nurses’ knowledge. Vetenskaplig uppsats för licentiatexamen/Academic essay.
7. Ekwall, Ewa (2006) Women’s Experiences of Primary and Recurrent Gynecological Cancer. Vetenskaplig uppsats för licentiatexamen/Academic essay.
8. Pettersson, Ingvor (2006) Significance of Assistive Devices in the Daily Life of Persons with Stroke and Their Spouses. Doktors avhandling/Doctoral thesis with focus on Occupational Therapy.
9. Carlsson, Eva (2006) Understanding persons with eating difficulties and communication impairment after stroke – patient experiences and methodological issues in qualitative interviews. Vetenskaplig uppsats för licentiatexamen/Academic essay.
* Seriens namn var tidigare (nr 1–24) ”Örebro Studies in Caring Sciences”.

10. Göransson, Katarina (2006) Registered nurse-led emergency department triage: organisation, allocation of acuity ratings and triage decision making. Doktorsavhandling/Doctoral thesis with focus on Nursing.
11. Eldh, Ann Catrine (2006) Patient participation – what it is and what it is not. Doktorsavhandling/Doctoral thesis with focus on Nursing.
12. Isaksson, Ann-Kristin (2007) Chronic sorrow and quality of life in patients with multiple sclerosis. Doktorsavhandling/Doctoral thesis with focus on Nursing.
13. Florin, Jan (2007) Patient participation in clinical decision making in nursing – a collaborative effort between patients and nurses. Doktorsavhandling/Doctoral thesis with focus on Nursing.
14. Johansson, Agneta (2007) Adolescents’ perspective on mental health and health-promoting dialogues. Vetenskaplig uppsats för licentiatexamen/Academic essay.
15. Frisk, Margot (2007) Asthma and respiratory symptoms related to the housing environment. Doktorsavhandling/Doctoral thesis with focus on Occupational Therapy.
16. Forslund, Kerstin (2007) Challenges in prehospital emergency care – patient, spouse and personnel perspectives. Doktorsavhandling/Doctoral thesis with focus on Nursing.
17. Odencrants, Sigrid (2008) The complexity of nutritional status for persons with chronic obstructive pulmonary disease – a nursing challenge. Doktorsavhandling/Doctoral thesis with focus on Nursing.
18. Tollén, Anita (2008) Vardagen och förväntningar på dagrehabilitering – en studie i äldre personers uppfattningar. Vetenskaplig uppsats för licentiat examen/Academic essay.
19. Dwyer, Lise-Lotte (2008) Dignity in the end of life care – what does it mean to older people and staff in nursing homes? Doktorsavhandling/Doctoral thesis with focus on Nursing.
20. Lidskog, Marie (2008) Learning with, from and about each other: Inter professional education on a training ward in municipal care for older persons. Doktorsavhandling/Doctoral thesis.
21. Tinnfält, Agneta (2008) Adolescents’ perspectives – on mental health, being at risk, and promoting initiatives. Doktorsavhandling/Doctoral thesis with focus on Public Health.
22. Carlsson, Eva (2009) Communication about eating difficulties after stroke – from the perspectives of patients and professionals in health care. Doktorsavhandling/Doctoral thesis with focus on Nursing.
23. Källström Karlsson, Inga-Lill (2009) Att leva nära döden. Patienters och vårdpersonals erfarenheter inom hospicevård. Doktorsavhandling/Doctoral thesis with focus on Nursing.
24. Österlind, Jane (2009) När livsrummet krymper. Doktorsavhandling/ Doctoral thesis with focus on Nursing.
25. Liedström, Elisabeth (2009) Experiences of Chronic Sorrow and Quality of Life in Next of Kin of Patients with Multiple Sclerosis. Vetenskaplig uppsats för licentiatexamen/Academic essay.
26. Petersson, Pia (2009) Att göra abstrakta begrepp och komplexa situationer konkreta. En avhandling om deltagarbaserad aktions- forskning i svensk vård och omsorg. Doktorsavhandling/ Doctoral thesis with focus on Nursing.
27. James, Inger (2010) Bakom rutinerna. Kunskap och omvårdnads- praxis i mänskliga gränssituationer. Doktorsavhandling/ Doctoral thesis with focus on Nursing.
28. Thoroddsen, Ásta (2010) The role of standardised nursing languages in representing nursing and supporting nurses as knowledge workers. Doktorsavhandling/ Doctoral thesis with focus on Nursing.
29. Pettersson, Camilla (2010) Parents’ Possibility to Prevent Underage Drinking. Studies of Parents, a Parental Support Program, and Adolescents in the Context of a National Program to Support NGOs. Doktorsavhandling/ Doctoral thesis with focus on Public Health.
30. Rydlo, Cecilia (2010) Fighting for the otherness. Student nurses’ lived experiences of growing in caring. Doktorsavhandling/Doctoral thesis.
31. Ek, Kristina (2010) Att leva med mycket svår kronisk obstruktiv lungsjukdom – ett liv i slowmotion. Doktorsavhandling/Doctoral thesis.

32. Fröding, Karin (2011) Public Health, Neighbourhood Development, and Participation. Research and Practice in four Swedish Partnership Cities. Doktorsavhandling/Doctoral thesis.
33. Kollén, Lena (2011) Dizziness, balance and rehabilitiation in vestibular disorders. Doktorsavhandling/Doctoral thesis.
34. Wallerstedt, Birgitta (2012) Utmaningar, utsatthet och stöd i palliativ vård utanför specialistenheter. Doktorsavhandling/Doctoral thesis.
35. Ewertzon, Mats (2012) Familjemedlem till person med psykossjukdom: bemötande och utanförskap i psykiatrisk vård. Doktorsavhandling/Doctoral thesis.
36. Fossum, Mariann (2012) Computerized Decision Support System in Nursing Homes. Doktorsavhandling/Doctoral thesis.
37. Henriksson, Anette (2012) A support group programme for family members: an intervention during ongoing palliative care. Doktorsavhandling/Doctoral thesis.
38. Hälleberg Nyman, Maria (2012) Urinary catheter policies for short-term bladder drainage in hip surgery patients. Doktorsavhandling/Doctoral thesis.
39. Thorstensson, Stina (2012) Professional support in childbearing, a challenging act of balance. Doktorsavhandling/Doctoral thesis.
40. Geidne, Susanna (2012) The Non-Governmental Organization as a Health promoting Setting. Examples from Alcohol Prevention Projects conducted in the Context of National Support to NGOs. Doktorsavhandling/Doctoral thesis.
41. Lidström Holmqvist, Kajsa (2012) Occupational therapy practice for clients with cognitive impairment following acquired brain injury – occupational therapists’ perspective. Doktorsavhandling/Doctoral thesis.
42. Tollén, Anita (2013): Äldre personers dagliga liv och betydelsen av dagrehabilitering. Doktorsavhandling/Doctoral thesis.
43. Pajalic, Zada (2013): Matdistribution till hemmaboende äldre personer ur flera perspektiv. Doktorsavhandling/Doctoral thesis.
44. Olsson, Annakarin (2013): Daily life of persons with dementia and their spouses supported by a passive positioning alarm. Doktorsavhandling/Doctoral thesis.

45. Norell Pejner, Margaretha (2013): The bright side of life. Support in municipal elderly home care. Doktorsavhandling/Doctoral thesis.
46. Karlsson, Ulf (2013): Arbetsterapeuters attityd till och uppfattning om forskningsanvändning samt professionen ur ett manligt perspektiv. Vetenskaplig uppsats för licentiatexamen/Academic essay.
47. Salzmann-Erikson, Martin (2013): Caring in intensive psychiatry. Rhythm and movements in a culture of stability. Doktorsavhandling/Doctoral thesis.
48. Lindner, Helen (2013): The Assessment of Capacity for Myoelectric Control. Psychometric evidence and comparison with upper limb prosthetic outcome measures. Doktorsavhandling/Doctoral thesis.



















