Terapia ipocolesterolemizzante: linee guida e nuovi ... Marcello.pdf · Bisogni insoddisfatti nella...
30
Marcello Arca Dipartimento di Medicina Interna e Specialità Mediche UOS Centro Arteriosclerosi Sapienza Università di Rom a Terapia ipocolesterolemizzante: linee guida e nuovi approcci terapeutici. Il ruolo degli inibitori della PCSK9
Transcript of Terapia ipocolesterolemizzante: linee guida e nuovi ... Marcello.pdf · Bisogni insoddisfatti nella...

Marcello Arca
Dipartimento di Medicina Interna e
Specialità Mediche
UOS Centro Arteriosclerosi
Sapienza Università di Roma
Terapia ipocolesterolemizzante:
linee guida e nuovi approcci
terapeutici.
Il ruolo degli inibitori della
PCSK9
Presenter Disclosure Information
I have the following potential conflicts of interest to report:
☑ Consulting: Kowa, Regeneron, ISIS, Aegerion
☑ Speakers honoraria: AstraZeneca, MSD, Pfizer, Roche, Genzyme, Abbott, Sanofi, SigmaTau
☑ Research grants: MSD, Pfizer, Regeneron, Sanofi, Genzyme, Boheringer, Aegerion

Bisogni insoddisfatti nella terapia delle dislipidemie
• Parziale risposta nei pazienti condislipidemie genetiche (FH)
• Difficoltà a raggiungere il target neipazienti ad alto/altissimo rischio
• Presenza di pazienti che mostranouna intolleranza (muscolare) allestatine
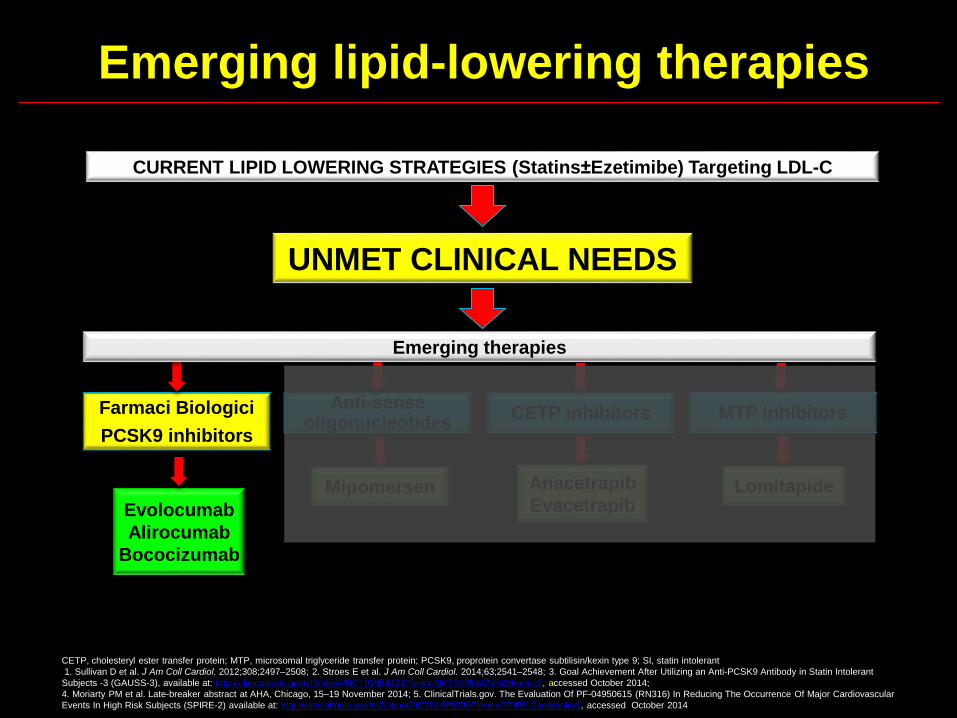
Emerging lipid-lowering therapies
CETP, cholesteryl ester transfer protein; MTP, microsomal triglyceride transfer protein; PCSK9, proprotein convertase subtilisin/kexin type 9; SI, statin intolerant
1. Sullivan D et al. J Am Coll Cardiol. 2012;308;2497–2508; 2. Stroes E et al. J Am Coll Cardiol. 2014;63;2541–2548; 3. Goal Achievement After Utilizing an Anti-PCSK9 Antibody in Statin Intolerant
Subjects -3 (GAUSS-3), available at: http://clinicaltrials.gov/ct2/show/NCT01984424?term=NCT01984424%26rank=1, accessed October 2014;
4. Moriarty PM et al. Late-breaker abstract at AHA, Chicago, 15–19 November 2014; 5. ClinicalTrials.gov. The Evaluation Of PF-04950615 (RN316) In Reducing The Occurrence Of Major Cardiovascular
Events In High Risk Subjects (SPIRE-2) available at: http://clinicaltrials.gov/ct2/show/NCT01975389?term=SPIRE-2andrank=1, accessed October 2014
PCSK9 inhibitorsFarmaci Biologici
PCSK9 inhibitors
Evolocumab
Alirocumab
Bococizumab
CURRENT LIPID LOWERING STRATEGIES (Statins±Ezetimibe) Targeting LDL-C
UNMET CLINICAL NEEDS
Emerging therapies
CETP inhibitors MTP inhibitors
Anacetrapib
EvacetrapibLomitapideMipomersen
Anti-senseoligonucleotides

Plasma LDL-C is controlled by hepatic low-density lipoprotein receptor (LDLR) levels
Brown et al. Proc Natl Acad Sci USA 1979;76:3330–3337.
Recycling of LDLR
Increased LDLR surface concentration
LDL particles
LDLR
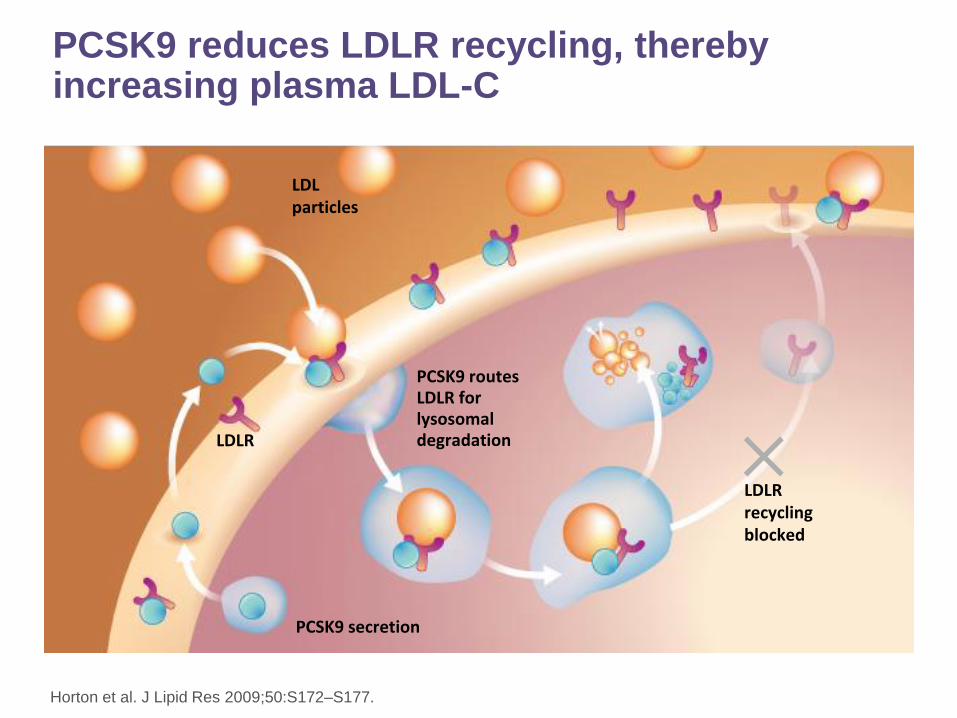
PCSK9 reduces LDLR recycling, thereby increasing plasma LDL-C
Horton et al. J Lipid Res 2009;50:S172–S177.
LDL particles
LDLR
PCSK9 secretion
PCSK9 routes LDLR for lysosomal degradation
LDLR recycling blocked

Impact of PCSK9 inhibition on LDL receptor
expression
11
For illustration purposes only
13
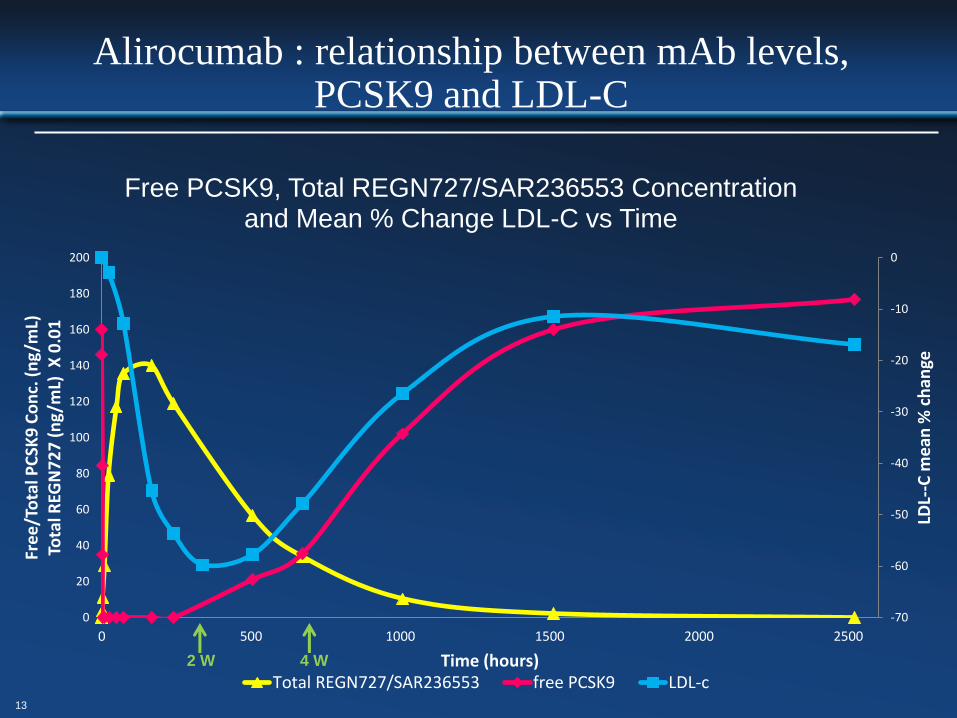
Alirocumab : relationship between mAb levels, PCSK9 and LDL-C
-70
-60
-50
-40
-30
-20
-10
0
0
20
40
60
80
100
120
140
160
180
200
0 500 1000 1500 2000 2500
LDL-
-C m
ean
% c
han
ge
Fre
e/T
ota
l PC
SK9
Co
nc.
(n
g/m
L)To
tal R
EGN
72
7 (
ng/
mL)
X 0
.01
Time (hours)
Free PCSK9, Total REGN727/SAR236553 Concentration and Mean % Change LDL-C vs Time
Total REGN727/SAR236553 free PCSK9 LDL-c2 W 4 W

Alirocumab is available in a pre-filled autoinjector pen
• 1mL solution in a single-use pre-filled
pen containing a syringe made from
type I glass with a stainless steel
27-gauge needle
• The needle cover of the pre-filled
pen is made from dry natural rubber
(a derivative of latex)
• The solution should be clear to
opalescent, colourless to yellowish,
and practically free from particles
• Pack sizes of one, two, three or
multipack of six (3 × 2) pre-filled
pens*
Yellow
(injection
complete)
Yellow
safety
guard
Orange
cap off
Grey start
button
Window
Medicine
Orange
cap on
Before
use
After
use

?Hypercholesterolemia in high
CV-risk population (NOT
controlled with max tolerated
dose of statins±Eze)
PCSK9 Inhibitors as Add-on to
max tolerated statin
(± other LLT)
PCSK9 inhibitorsFarmaci Biologici: PCSK9 inhibitors
Evolocumab, Alirocumab, Bococizumab
?????
?BASELINE LDL-C TO HIGH
TO REACH TARGETS!
I MONOCLONALI ANTI-PCSK9 NEI PAZIENTI
IPERCOLESTEROLEMICI SEVERI E/O INTOLLERANTI
ALLE STATINE
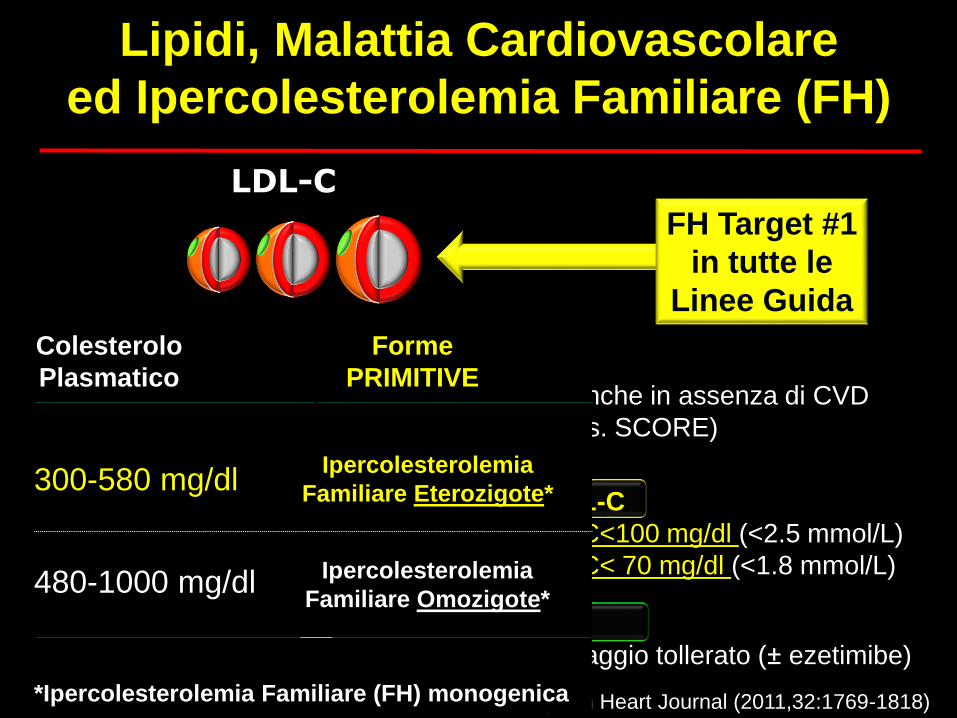
Lipidi, Malattia Cardiovascolare
ed Ipercolesterolemia Familiare (FH)
LDL-C
FH Target #1
in tutte le
Linee Guida
Terapia di scelta
Statine (ad elevata efficacia) al massimo dosaggio tollerato (± ezetimibe)
Livelli Target di LDL-C
FH senza CVD: rischio CV elevato: LDL-C<100 mg/dl (<2.5 mmol/L)
FH con CVD: rischio CV molto elevato: LDL-C< 70 mg/dl (<1.8 mmol/L)
ESC/EAS Guidelines - European Heart Journal (2011,32:1769-1818)
Pazienti con FH: rischio di eventi CV elevato anche in assenza di CVD
NON vanno utilizzate le carte del rischio CV (es. SCORE)
Colesterolo
Plasmatico
Ipercolesterolemia
Familiare Eterozigote*300-580 mg/dl
480-1000 mg/dl
Forme
PRIMITIVE
Ipercolesterolemia
Familiare Omozigote*
*Ipercolesterolemia Familiare (FH) monogenica
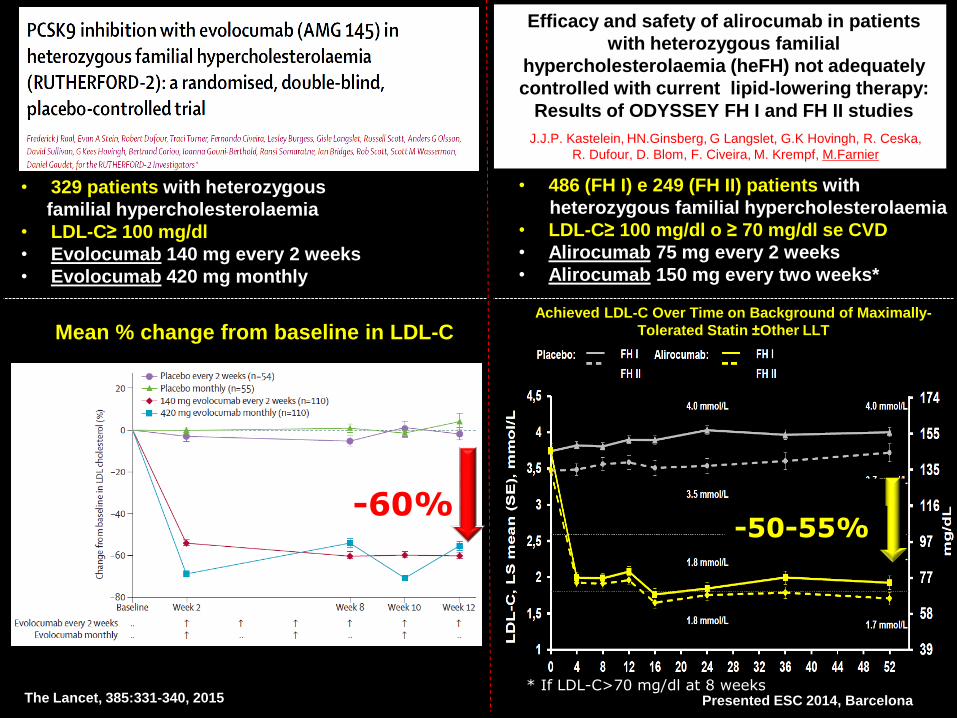
The Lancet, 385:331-340, 2015
Efficacy and safety of alirocumab in patients
with heterozygous familial
hypercholesterolaemia (heFH) not adequately
controlled with current lipid-lowering therapy:
Results of ODYSSEY FH I and FH II studies
J.J.P. Kastelein, HN.Ginsberg, G Langslet, G.K Hovingh, R. Ceska,
R. Dufour, D. Blom, F. Civeira, M. Krempf, M.Farnier
Presented ESC 2014, Barcelona
• 329 patients with heterozygous
familial hypercholesterolaemia
• LDL-C≥ 100 mg/dl
• Evolocumab 140 mg every 2 weeks
• Evolocumab 420 mg monthly
Mean % change from baseline in LDL-C
• 486 (FH I) e 249 (FH II) patients with
heterozygous familial hypercholesterolaemia
• LDL-C≥ 100 mg/dl o ≥ 70 mg/dl se CVD
• Alirocumab 75 mg every 2 weeks
• Alirocumab 150 mg every two weeks*
* If LDL-C>70 mg/dl at 8 weeks
Achieved LDL-C Over Time on Background of Maximally-
Tolerated Statin ±Other LLT
-50-55%-60%

The Lancet, 385:331-340, 2015
Efficacy and safety of alirocumab in patients
with heterozygous familial
hypercholesterolaemia (heFH) not adequately
controlled with current lipid-lowering therapy:
Results of ODYSSEY FH I and FH II studies
J.J.P. Kastelein, HN.Ginsberg, G Langslet, G.K Hovingh, R. Ceska,
R. Dufour, D. Blom, F. Civeira, M. Krempf, M.Farnier
Presented ESC 2014, Barcelona* If LDL-C>70 mg/dl at 8 weeks
LDL-C Goal Achievement < 70 mg/dL Weeks 10 and 12
2%
67%
2%
80%
78%*
65%*
Placebo Q2W (N = 54)
Placebo QM (N = 55)
Evolocumab 140 mg Q2W (N = 110)
Evolocumab 420 mg QM (N = 110)
*P<0.0001 evolocumab treatment difference vs placebo
Proportion of patients reaching LDL-C
goal† at Week 24
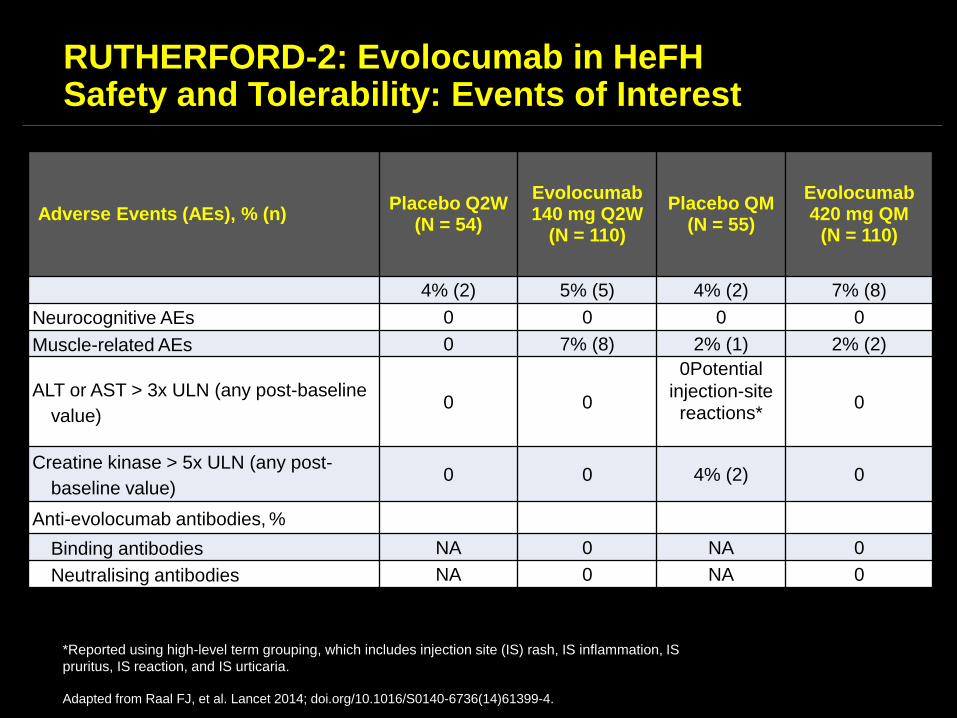
RUTHERFORD-2: Evolocumab in HeFHSafety and Tolerability: Events of Interest
*Reported using high-level term grouping, which includes injection site (IS) rash, IS inflammation, IS
pruritus, IS reaction, and IS urticaria.
Adapted from Raal FJ, et al. Lancet 2014; doi.org/10.1016/S0140-6736(14)61399-4.
Adverse Events (AEs), % (n)Placebo Q2W
(N = 54)
Evolocumab 140 mg Q2W
(N = 110)
Placebo QM (N = 55)
Evolocumab 420 mg QM
(N = 110)
4% (2) 5% (5) 4% (2) 7% (8)
Neurocognitive AEs 0 0 0 0
Muscle-related AEs 0 7% (8) 2% (1) 2% (2)
ALT or AST > 3x ULN (any post-baseline
value)0 0
0Potential
injection-site reactions*
0
Creatine kinase > 5x ULN (any post-
baseline value)0 0 4% (2) 0
Anti-evolocumab antibodies, %
Binding antibodies NA 0 NA 0
Neutralising antibodies NA 0 NA 0
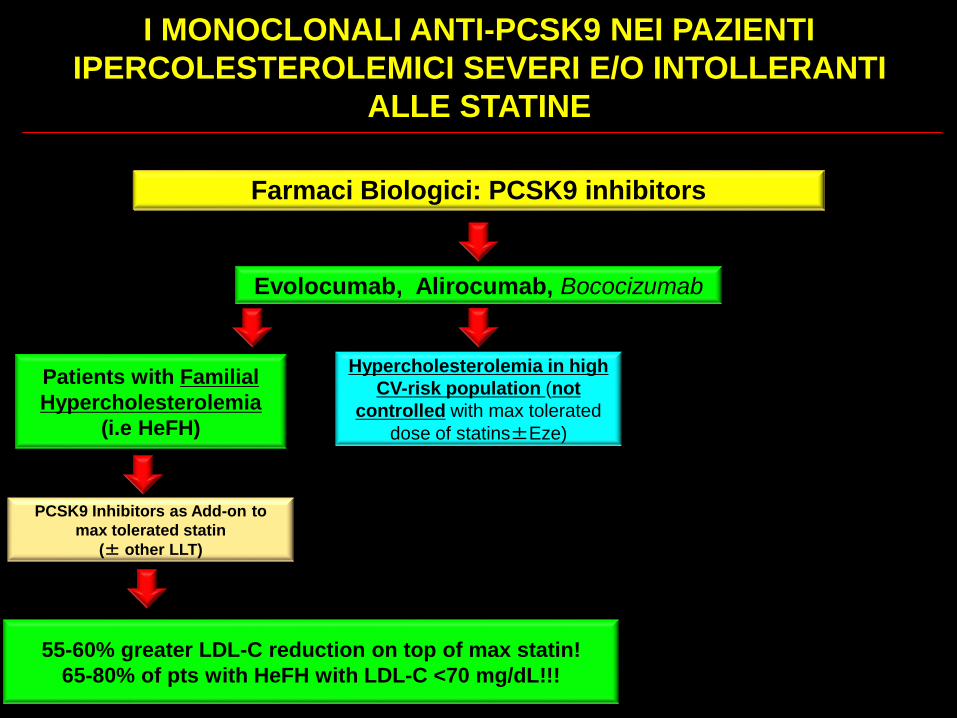
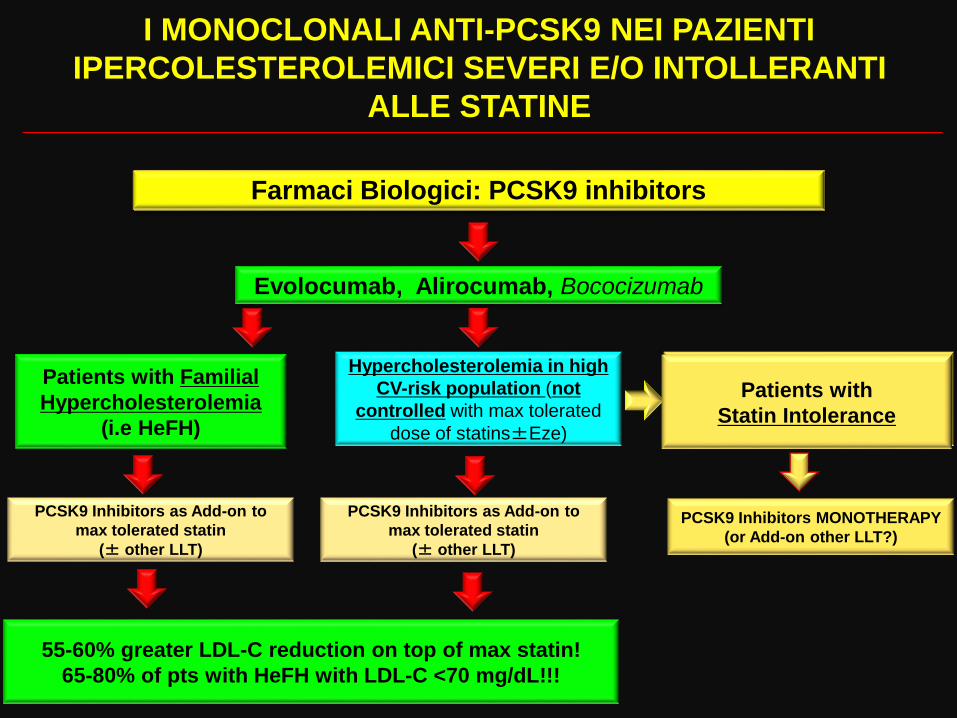
Hypercholesterolemia in high
CV-risk population (not
controlled with max tolerated
dose of statins±Eze)
PCSK9 inhibitorsFarmaci Biologici: PCSK9 inhibitors
Evolocumab, Alirocumab, Bococizumab
Patients with Familial
Hypercholesterolemia
(i.e HeFH)
PCSK9 Inhibitors as Add-on to
max tolerated statin
(± other LLT)
55-60% greater LDL-C reduction on top of max statin!
65-80% of pts with HeFH with LDL-C <70 mg/dL!!!
I MONOCLONALI ANTI-PCSK9 NEI PAZIENTI
IPERCOLESTEROLEMICI SEVERI E/O INTOLLERANTI
ALLE STATINE
PCSK9 inhibition in high risk patients
24
March 15, 2015
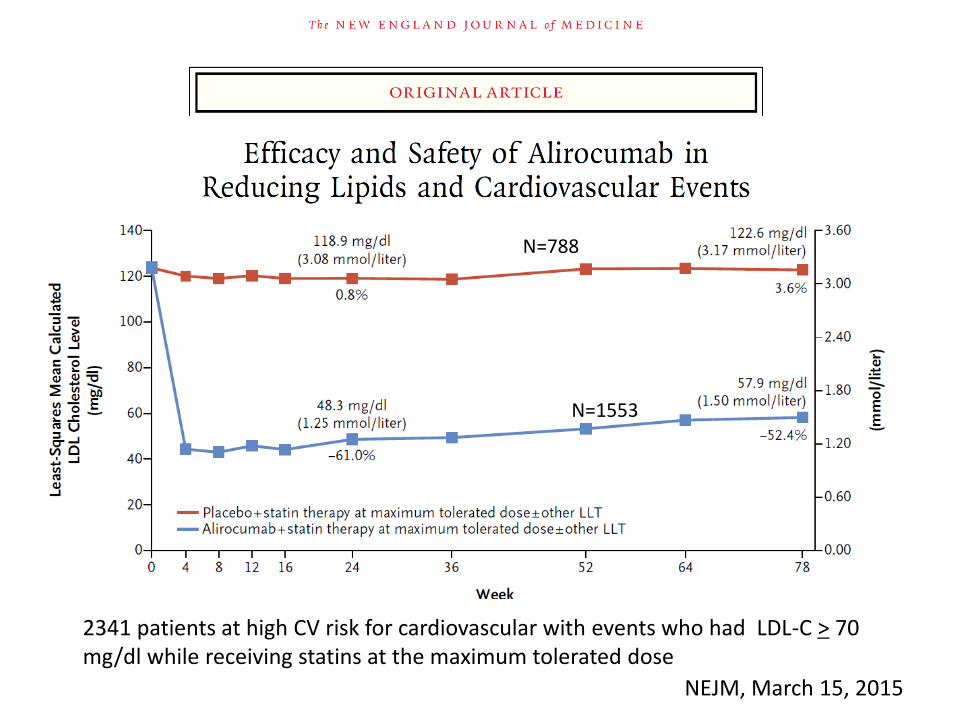
NEJM, March 15, 2015
N=1553
N=788
2341 patients at high CV risk for cardiovascular with events who had LDL-C > 70 mg/dl while receiving statins at the maximum tolerated dose
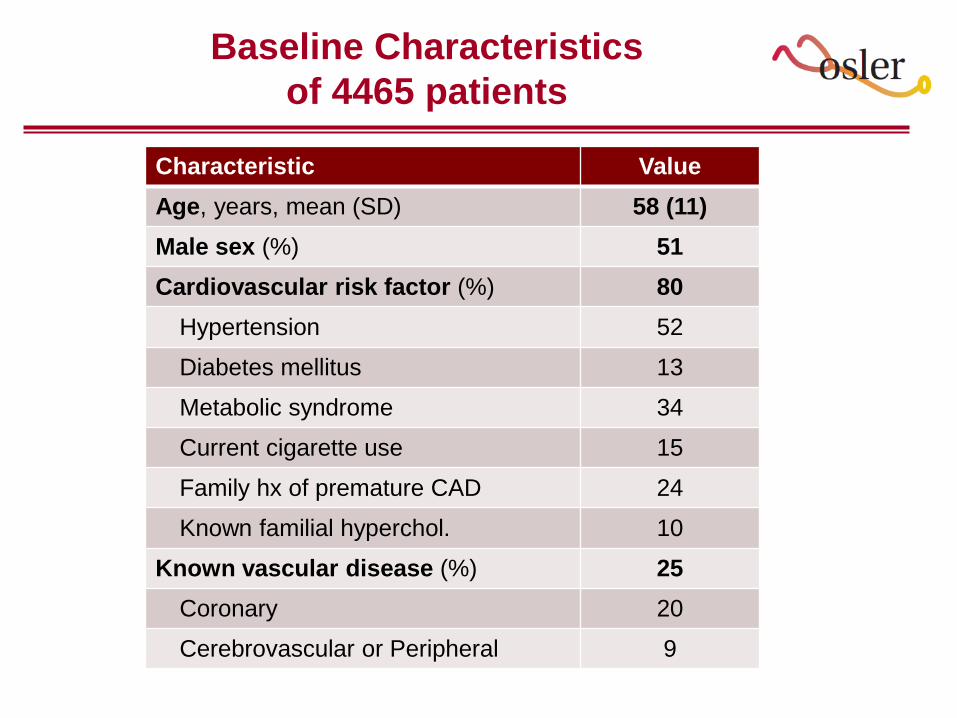
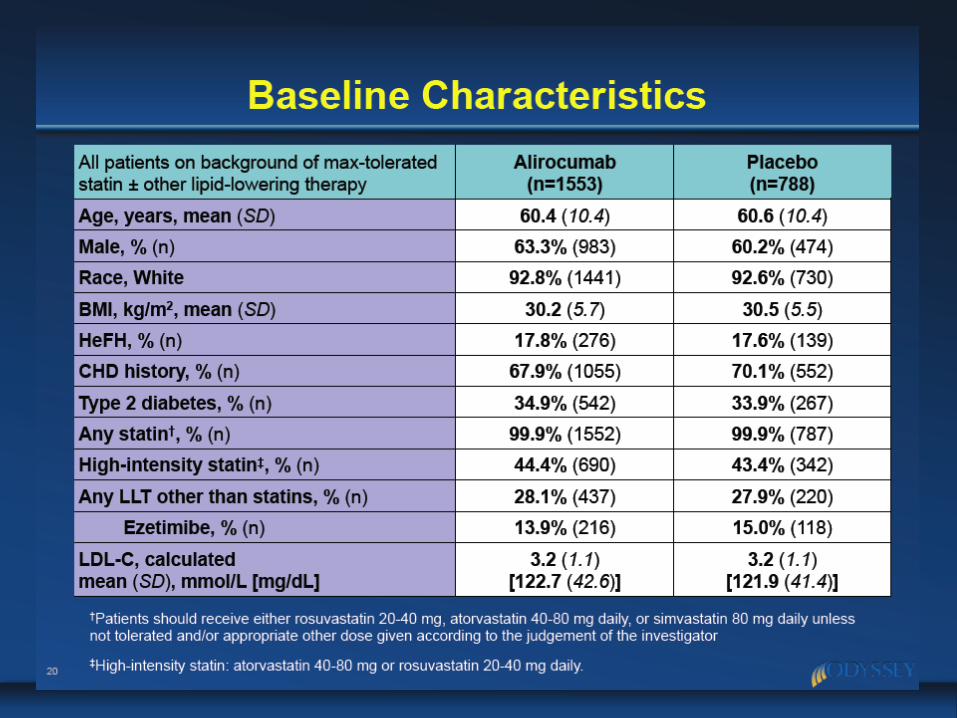
Baseline Characteristics
of 4465 patients
Characteristic Value
Age, years, mean (SD) 58 (11)
Male sex (%) 51
Cardiovascular risk factor (%) 80
Hypertension 52
Diabetes mellitus 13
Metabolic syndrome 34
Current cigarette use 15
Family hx of premature CAD 24
Known familial hyperchol. 10
Known vascular disease (%) 25
Coronary 20
Cerebrovascular or Peripheral 9
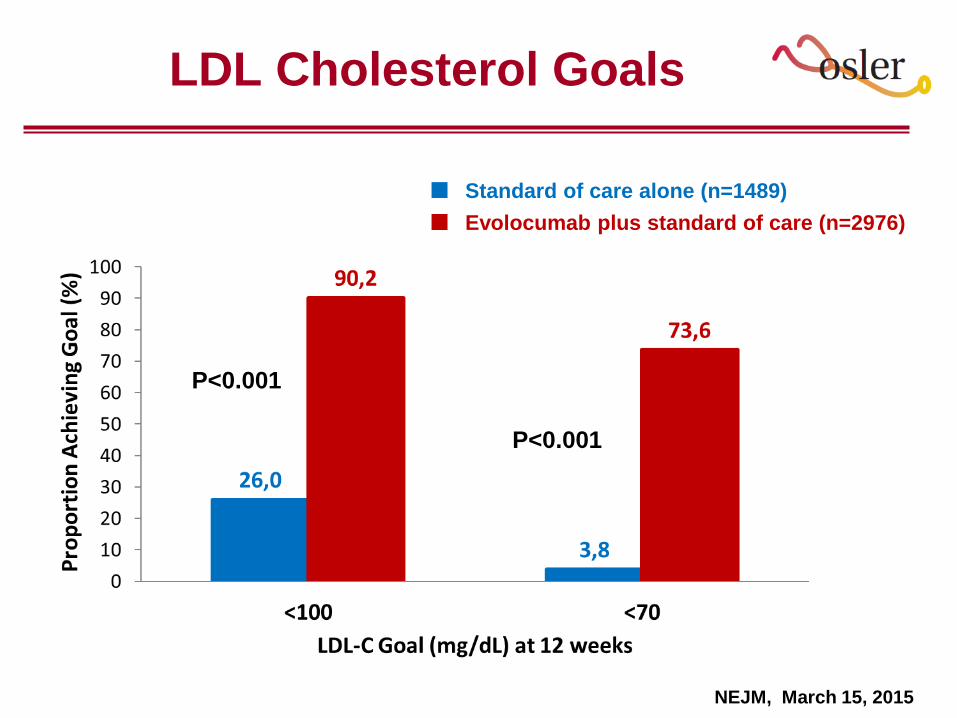
LDL Cholesterol Goals
P<0.001
P<0.001
Standard of care alone (n=1489)
Evolocumab plus standard of care (n=2976)
NEJM, March 15, 2015
Hypercholesterolemia in high
CV-risk population (not
controlled with max tolerated
dose of statins±Eze)
PCSK9 inhibitorsFarmaci Biologici: PCSK9 inhibitors
Evolocumab, Alirocumab, Bococizumab
Patients with Familial
Hypercholesterolemia
(i.e HeFH)
PCSK9 Inhibitors as Add-on to
max tolerated statin
(± other LLT)
?
55-60% greater LDL-C reduction on top of max statin!
65-80% of pts with HeFH with LDL-C <70 mg/dL!!!
I MONOCLONALI ANTI-PCSK9 NEI PAZIENTI
IPERCOLESTEROLEMICI SEVERI E/O INTOLLERANTI
ALLE STATINE
Patients with
Statin Intolerance
PCSK9 Inhibitors MONOTHERAPY
(or Add-on other LLT?)
PCSK9 Inhibitors as Add-on to
max tolerated statin
(± other LLT)
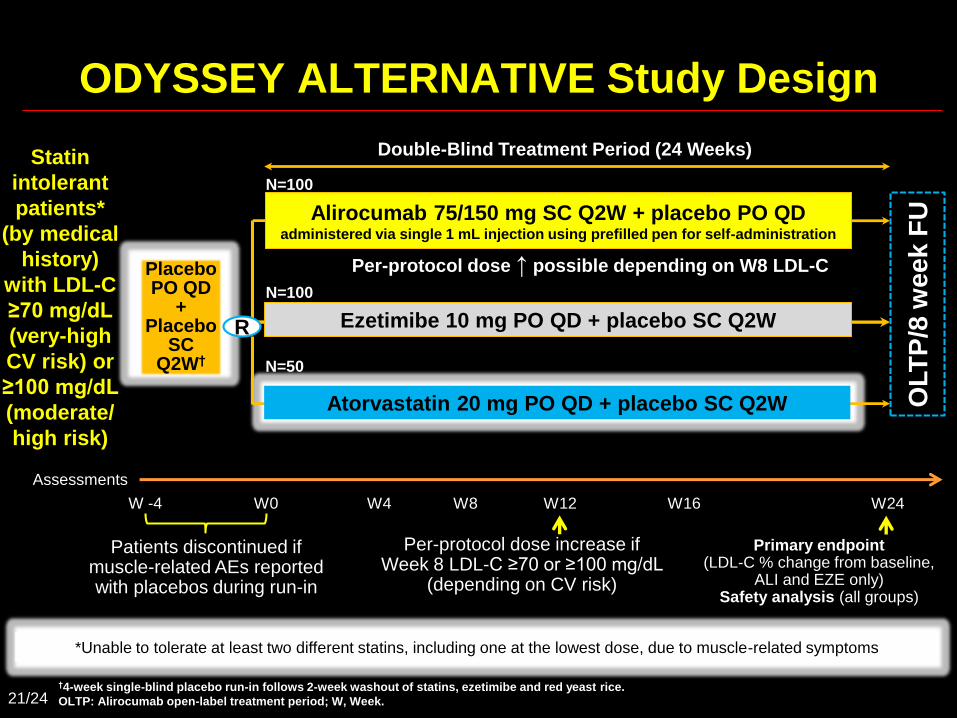
Double-Blind Treatment Period (24 Weeks)
Alirocumab 75/150 mg SC Q2W + placebo PO QDadministered via single 1 mL injection using prefilled pen for self-administration
Per-protocol dose ↑ possible depending on W8 LDL-C
N=100
Ezetimibe 10 mg PO QD + placebo SC Q2W
N=100
W8 W16
Primary endpoint (LDL-C % change from baseline,
ALI and EZE only) Safety analysis (all groups)
W4 W12 W24
Per-protocol dose increase if Week 8 LDL-C ≥70 or ≥100 mg/dL
(depending on CV risk)
*Unable to tolerate at least two different statins, including one at the lowest dose, due to muscle-related symptoms*Unable to tolerate at least two different statins, including one at the lowest dose, due to muscle-related symptoms
ODYSSEY ALTERNATIVE Study Design
Statin
intolerant
patients*
(by medical
history)
with LDL-C
≥70 mg/dL
(very-high
CV risk) or
≥100 mg/dL
(moderate/
high risk)
†4-week single-blind placebo run-in follows 2-week washout of statins, ezetimibe and red yeast rice.
OLTP: Alirocumab open-label treatment period; W, Week.
Assessments
W0W -4
Patients discontinued if muscle-related AEs reported with placebos during run-in
R
Placebo PO QD
+ Placebo
SC Q2W†
Atorvastatin 20 mg PO QD + placebo SC Q2W
N=50
OLT
P/8
we
ek
FU
21/24

Alirocumab Maintained
LDL-C Reductions Week 4–24
Week
156 mg/dL
97 mg/dL
157 mg/dL
92 mg/dL
EzetimibeAlirocumab
LD
L-C
, m
ean
(S
E),
mg
/dL
Achieved calculated LDL-C over time – on-treatment analysis
(modified ITT – observed data only)
49.5% received 150 mg Q2W at W12
Δ 59 mg/dLΔ 65 mg/dL
-52.2%
-17.1%
22/24
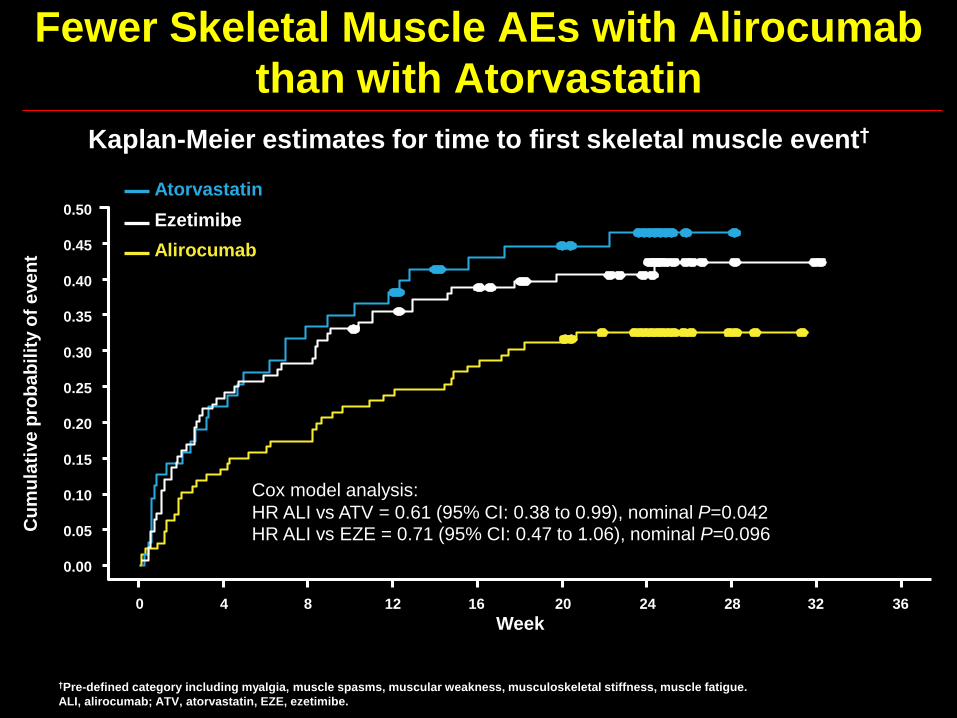
Fewer Skeletal Muscle AEs with Alirocumab
than with Atorvastatin
0.50
0.45
0.40
0.35
0.30
0.25
0.20
0.15
0.10
0.05
0.00
Cu
mu
lati
ve
pro
ba
bil
ity o
f e
ve
nt
Week
Atorvastatin
Alirocumab
0 4 8 12 16 20 24 28 32 36
Kaplan-Meier estimates for time to first skeletal muscle event†
†Pre-defined category including myalgia, muscle spasms, muscular weakness, musculoskeletal stiffness, muscle fatigue.
ALI, alirocumab; ATV, atorvastatin, EZE, ezetimibe.
Cox model analysis:
HR ALI vs ATV = 0.61 (95% CI: 0.38 to 0.99), nominal P=0.042
Ezetimibe
HR ALI vs EZE = 0.71 (95% CI: 0.47 to 1.06), nominal P=0.096

I MONOCLONALI ANTI-PCSK9 NEL CONTROLLO DEL
COLESTEROLO LDL
PCSK9 inhibitorsFarmaci Biologici: PCSK9 inhibitors
UNMET CLINICAL NEED WITH CURRENT THERAPY
REMARKABLE LDL-C REDUCTION BY 50-65% AS ADD-ON TO MAX LLT OR MONOTHERAPY
EXCELLENT SAFETY PROFILE, POTENTIALLY RELEVANT CLINICAL BENEFITS
POPULATION AT TOP COST/BENEFIT RATIO
1)Heterozygotes Familial Hypercholesterolemia2) Statin intolerant at very high CV risk
Hypercholesterolemia in high
CV-risk population (not
controlled with max tolerated
dose of statins±Eze)
Patients with Familial
Hypercholesterolemia
(i.e HeFH)
Patients with
Statin Intolerance
COST ($) CV BENEFITS
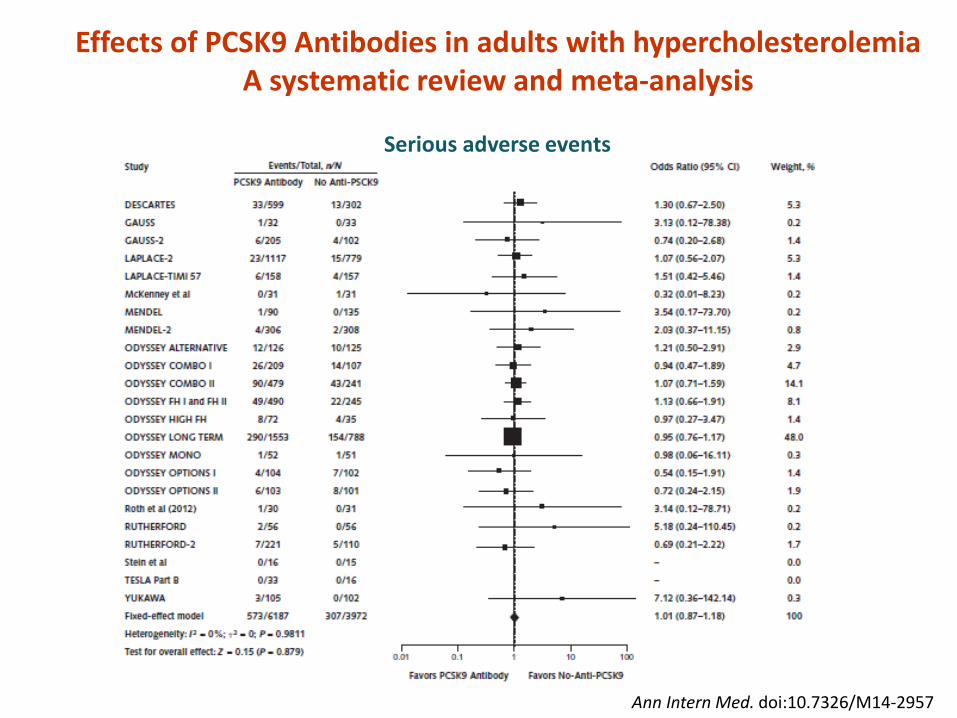
Ann Intern Med. doi:10.7326/M14-2957
Effects of PCSK9 Antibodies in adults with hypercholesterolemiaA systematic review and meta-analysis
Serious adverse events
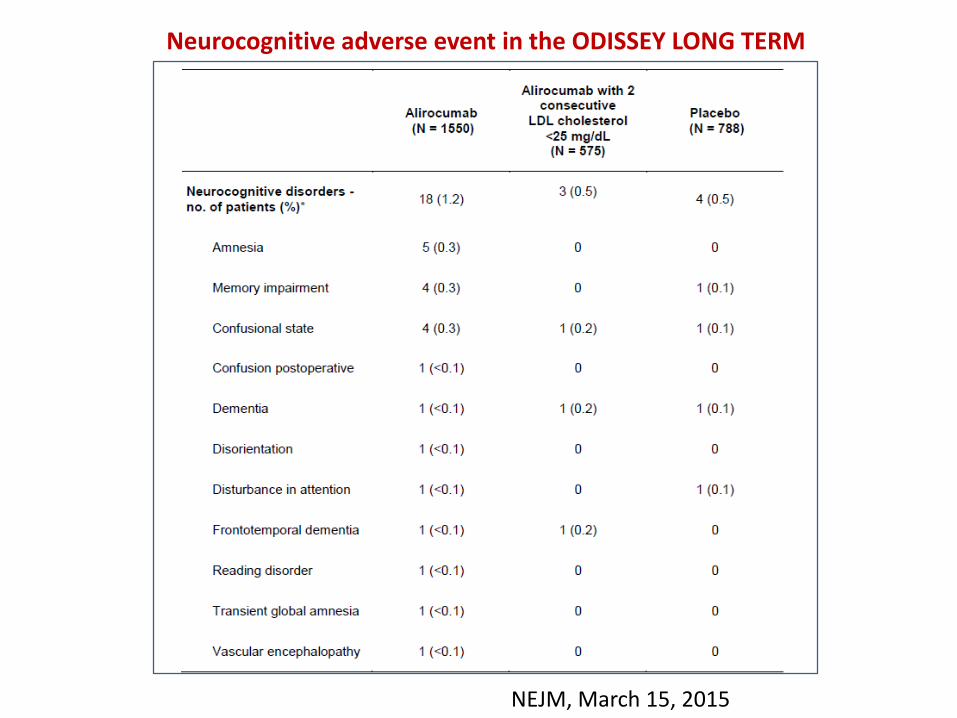
Neurocognitive adverse event in the ODISSEY LONG TERM
NEJM, March 15, 2015
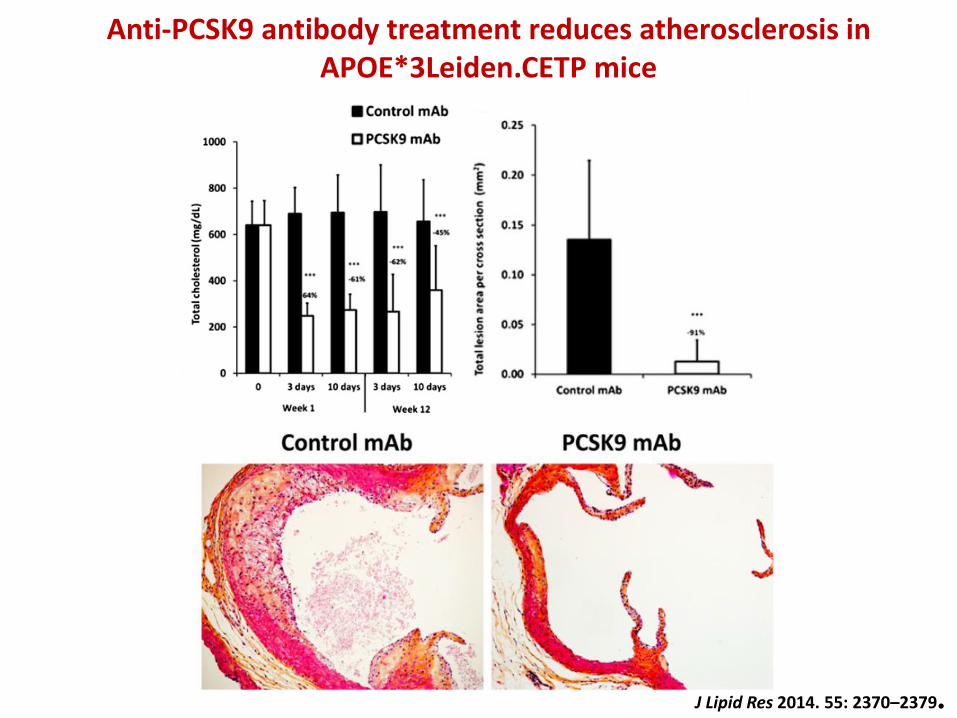
Anti-PCSK9 antibody treatment reduces atherosclerosis in APOE*3Leiden.CETP mice
J Lipid Res 2014. 55: 2370–2379.
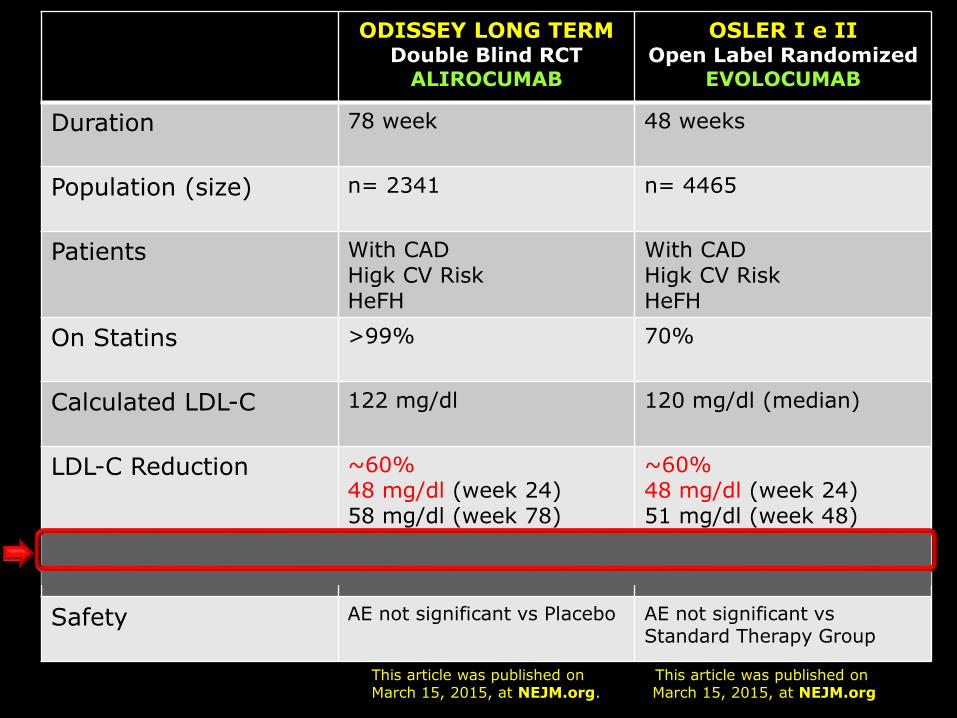
ODISSEY LONG TERMDouble Blind RCT
ALIROCUMAB
OSLER I e IIOpen Label Randomized
EVOLOCUMAB
Duration 78 week 48 weeks
Population (size) n= 2341 n= 4465
Patients With CADHigk CV RiskHeFH
With CADHigk CV RiskHeFH
On Statins >99% 70%
Calculated LDL-C 122 mg/dl 120 mg/dl (median)
LDL-C Reduction ~60%48 mg/dl (week 24)58 mg/dl (week 78)
~60%48 mg/dl (week 24)51 mg/dl (week 48)
CV Event Reduction ~50% ~50%
Safety AE not significant vs Placebo AE not significant vs Standard Therapy Group
This article was published onMarch 15, 2015, at NEJM.org
This article was published onMarch 15, 2015, at NEJM.org.
Conclusioni
La inibizione del PCSK9 attraverso l’uso dianticorpi monoclinali rappresenta una strategiamolto promettente per raggiungere il valoretarget di LDL-C nei pazienti a rischio CV
La somministrazione di Ab-anti-PCSK9 puòconsentire di ottenere una riduzione del LDL-Cdel 50-60%, in diverse tipologie di pazienti giàin trattamento con statine
Sebbene gli studi sono stati di breve durata,non sono stati osservati AE di particolare rilievoassociati all’uso di Ab- anti PCSK9