
Systems Science to Guide Implementation of Whole-of...
85
Systems Science to Guide Implementation of Whole-of-community Childhood Obesity Interventions Matthew W. Gillman, MD, SM EN Power of Programming March 2014 Note: for non-commercial purposes only
Transcript of Systems Science to Guide Implementation of Whole-of...

Systems Science to Guide Implementation of
Whole-of-community Childhood Obesity Interventions
Matthew W. Gillman, MD, SM EN Power of Programming
March 2014
Note: for non-commercial purposes only
Thanks to…
Faculty, Trainees, & Staff
Obesity Prevention Program Department of Population Medicine
Harvard Medical School/Harvard Pilgrim Health Care Institute

Questions about Obesity
• Population trends – What caused/is causing the epidemic? – How can we reverse it?
• Not necessarily the same as what caused it • Individual (between-person) variability
– Why do some people develop obesity and others not?
– How can we use that information to tailor, and evaluate, prevention and treatment
• What works, for whom, & under what circumstances

• Population trends – What caused/is causing the epidemic? – How can we reverse it?
• Individual (between-person) variability – Why do some people develop obesity and
others not? – How can we use that information to tailor, and
evaluate, prevention and treatment
Questions about Obesity

• Population trends – What caused/is causing the epidemic? – How can we reverse it?
• Individual (between-person) variability – Why do some people develop obesity and
others not? – How can we use that—and other—information
to tailor, and evaluate, prevention and treatment
Questions about Obesity

• Population trends – What caused/is causing the epidemic? – How can we reverse it?
• Individual (between-person) variability – Why do some people develop obesity and
others not? – How can we use that information to tailor, and
evaluate, prevention and treatment
Questions about Obesity

It’s because of what happened to them in utero and in early childhood
• Early (developmental) origins of obesity – [Motivation, Evidence] – How systems science may help
• Untangle the complex webs of etiology • Help drive design of prevention
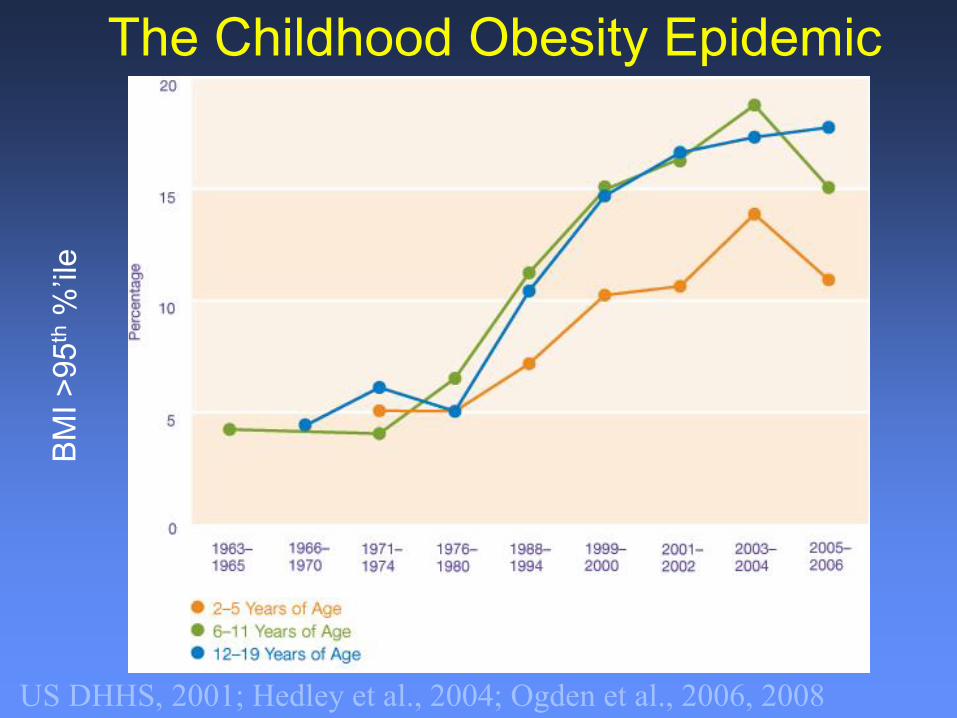
The Childhood Obesity Epidemic
US DHHS, 2001; Hedley et al., 2004; Ogden et al., 2006, 2008

0
5
10
15
Pre
va
len
ce o
f O
ver
wei
gh
t
Year
24-71 months
0-11 months
12-23 months
1980 1985 1990 1995 2000
…in Younger Children Too Including Infants
Kim et al., Obesity 2006; ~500,000 well child visits in Mass. HMO

a
Standardized for age, race/ethnicity, and HVMA site, using the year 1999-2000 as reference
13.7
8.1
10.6
14.2
11.9
13.3 13.3 13.5
13.8
12.3
13.0
12.1
12.7 12.6
13.1 12.9
9.1
9.8 10.0
9.0
8.1
7.4
9.9 9.8 9.6 9.3
9.8 10.2
4
5
6
7
8
9
10
11
12
13
14
15
16
1980-1982
1983-1984
1985-1986
1987-1988
1989-1990
1991-1992
1993-1994
1995-1996
1997-1998
1999-2000
2001-2002
2003-2004
2005-2006
2007-2008
Year
Pre
va
len
ce
Overweight (standardized) Obesity (standardized)
Boys
X. Wen et al. Pediatrics 2012;129:823-831
Downward trend in BMI since 2004 in 0-6-year-olds

Girls
X. Wen et al. Pediatrics 2012;129:823-831
a
Standardized for age, race/ethnicity, and HVMA site, using the year 1999-2000 as reference
12.3
13.3
11.7
12.6
11.7
6.5 6.3
7.0
8.5 8.4
6.8
11.4 11.1 10.9
11.3
11.9 12.1 11.7
12.3 12.6
5.8
7.4 7.8
7.5 8.0
8.5 8.6
7.3
4
5
6
7
8
9
10
11
12
13
14
15
16
1980-1982
1983-1984
1985-1986
1987-1988
1989-1990
1991-1992
1993-1994
1995-1996
1997-1998
1999-2000
2001-2002
2003-2004
2005-2006
2007-2008
Year
Pre
va
len
ce
Overweight (standardized) Obesity (standardized)


Curious trends in SGA & LGA, U.S. 1990-2005 N = 502,716 low-risk mothers: 37-41 wk, age 25-29 y, white, >13 y educ, married,
1st trim prenatal care, non-smoker, no complications, NSVD, had U/S, GWG 26-35 lb
Donahue et al., Obstet Gynecol 2010; 115:357

Curious trends in SGA & LGA, U.S. 1990-2005 N = 502,716 low-risk mothers: 37-41 wk, age 25-29 y, white, >13 y educ, married,
1st trim prenatal care, non-smoker, no complications, NSVD, had U/S, GWG 26-35 lb
Donahue et al., Obstet Gynecol 2010; 115:357

Message
• The obesity epidemic has spared no age group, not even our youngest children
• Once present, obesity tenaciously resists treatment
• Prevention must start early

• Usual etiologic epidemiology – 1 determinant at a time – Independent of others
• Moving toward systems approach – More than 1 determinant
Developmental Origins of Obesity

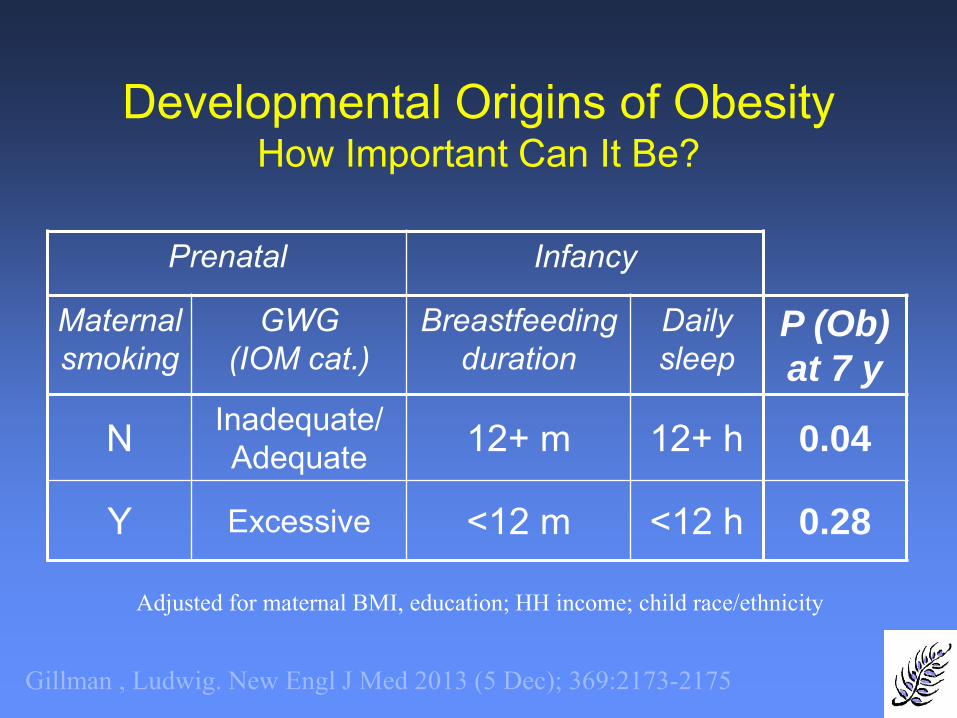
Developmental Origins of Obesity How Important Can It Be?
Prenatal Infancy
Maternal smoking
GWG (IOM cat.)
Breastfeeding duration
Daily sleep
P (Ob)
at 7 y
N Inadequate/ Adequate 12+ m 12+ h 0.04
Y Excessive <12 m <12 h 0.28
Gillman , Ludwig. New Engl J Med 2013 (5 Dec); 369:2173-2175
Adjusted for maternal BMI, education; HH income; child race/ethnicity

Risk of obesity at age 7-10 y according to combinations of 4 pre/post-natal risk factors
Smoking – – – + – – + – + – + + – + + +Gest. weight gain – + – – – + + + – – – + + + – +Breastfeeding – – + – – + – – + + – + + – + +Sleep – – – – + – – + – + + – + + + +Prob. obesity 0.04 0.06 0.07 0.07 0.08 0.10 0.10 0.11 0.11 0.13 0.13 0.16 0.18 0.18 0.20 0.28
Pred. BMI-z 0.07 0.24 0.22 0.23 0.31 0.39 0.40 0.48 0.38 0.46 0.47 0.55 0.63 0.64 0.62 0.79
Pred. DXA % fat 23.2 23.0 24.5 24.1 24.4 24.4 24.0 24.2 25.4 25.7 25.3 25.3 25.5 25.2 26.6 26.5
Prevalence in this cohort6.9% 10.4% 20.3% 0.2% 5.2% 26.6% 0.2% 5.6% 1.1% 7.2% 0.1% 3.5% 9.2% 0.3% 1.5% 1.9%
Combinations of 4 risk factors
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16Combinations of 4 risk factors
Pro
bab
ility
of
ob
esi
ty
Gillman , Ludwig. New Engl J Med 2013 (5 Dec); 369:2173-2175

Smoking – – – + – – + – + – + + – + + +Gest. weight gain – + – – – + + + – – – + + + – +Breastfeeding – – + – – + – – + + – + + – + +Sleep – – – – + – – + – + + – + + + +Prob. obesity 0.04 0.06 0.07 0.07 0.08 0.10 0.10 0.11 0.11 0.13 0.13 0.16 0.18 0.18 0.20 0.28
Pred. BMI-z 0.07 0.24 0.22 0.23 0.31 0.39 0.40 0.48 0.38 0.46 0.47 0.55 0.63 0.64 0.62 0.79
Pred. DXA % fat 23.2 23.0 24.5 24.1 24.4 24.4 24.0 24.2 25.4 25.7 25.3 25.3 25.5 25.2 26.6 26.5
Prevalence in this cohort6.9% 10.4% 20.3% 0.2% 5.2% 26.6% 0.2% 5.6% 1.1% 7.2% 0.1% 3.5% 9.2% 0.3% 1.5% 1.9%
Combinations of 4 risk factors
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16Combinations of 4 risk factors
Pro
bab
ility
of
ob
esi
ty
PAR% ~ 20-50%
Risk of obesity at age 7-10 y according to combinations of 4 pre/post-natal risk factors

More risk factors • Prenatal
– Smoking, GWG, GDM • Perinatal
– C-section, leptin • Infancy
– Type of feeding, sleep duration, rapid adiposity gain, early intro solids

More risk factors • Prenatal
– Smoking, GWG, GDM • Perinatal
– C-section, leptin • Infancy
– Type of feeding, sleep duration, rapid adiposity gain, early intro solids
• Emerging – Epigenetics, toxic environment, microbiota….

• More than 1 determinant • Interacting with each other
Developmental Origins of Obesity

• More than 1 determinant • Interacting with each other • Over time (age)
– Life course approach
Developmental Origins of Obesity

• More than 1 determinant • Interacting with each other • Over time (age) • At multiple levels of influence
– Different influences at different developmental periods
Developmental Origins of Obesity

• More than 1 determinant • Interacting with each other • Over time (age) • At multiple levels of influence *********************************************** • Dynamic
– Feedback loops
Developmental Origins of Obesity
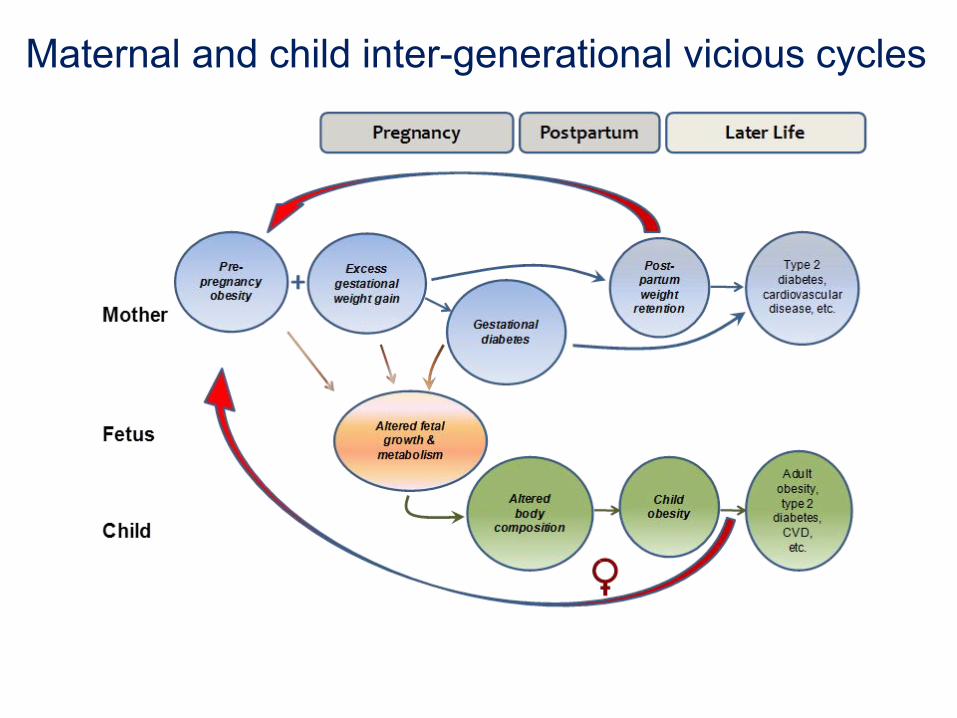
Maternal and child inter-generational vicious cycles

• More than 1 determinant • Interacting with each other • Over time (age) • At multiple levels of influence *********************************************** • Dynamic
– Feedback loops • That may operate in different directions at different
stages of the life course
Developmental Origins of Obesity

Hormone feedback loops in older
children and adults
Tend to impede weight loss

Cord blood leptin predicts slower WFL gain in 1st 6 mo, lower 3 & 7-y BMI,
but ...3-y leptin predicts higher 7-y BMI early sensitive period of leptin action, then tolerance
Boeke et al, Obesity 2013;21:1430-7

Body Composition Whole Body Total Energy Expenditure Thermic Effect of Feeding Adaptive Thermogenesis Physical Activity Energy Expenditure Resting Metabolic Rate Daily Average Lipolysis Rate Ketone Oxidation Rate Daily Average Ketogenesis Rate Daily Average Ketone Excretion Rate Daily Average Glycogenolysis Rate Glycerol 3-Phosphate Production Rate Gluconeogenesis From Amino Acids De Novo Lipogenesis Rate Macronutrient Oxidation Rates Respiratory Gas Exchange Nutrient Balance Parameter Constraints Carbohydrate Perturbation Constraint Protein Perturbation Constraint Physical Inactivity Constraint
Model Parameter Values
Predicting metabolic adaptation, body weight
change, and energy intake
KD Hall
• More than 1 determinant • Interacting with each other • Over time (age) • At multiple levels of influence *********************************************** • Dynamic
– Feedback loops • At multiple levels of influence
Developmental Origins of Obesity

Health
outcomes
d
Pre- and peri-
natal factors
Micro
Macro
Time Axis
Hierarchical Axis
Weight
gain
Energy in (diet)
Energy out
(physical activity)
Health Behaviors
Genes
Appetite Metabolism
Mood HPA axis
Built environments (e.g., connectivity, walkability)
Commercial messaging (e.g., TV ads to kids)
Psychosocial hazards (e.g., crime)
Local food environment (e.g., presence of fast food)
Area deprivation (e.g., poverty)
Cultural norms (e.g., body image)
Laws, regulations, policies (e.g., farm subsidies)
Social, built, natural environment
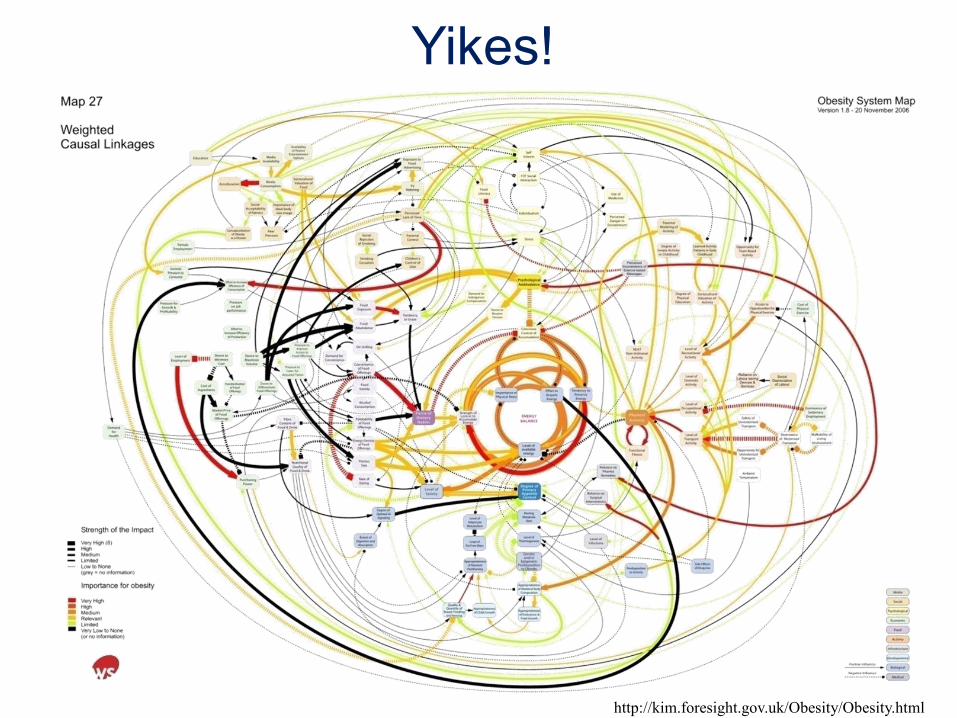
http://kim.foresight.gov.uk/Obesity/Obesity.html
Yikes!

Complex System
• “…one whose properties are not fully explained by an understanding of its component parts”
• Whole is greater than sum of parts
Gallagher & Appenzeller, quoted in Luke and Stamatakis, Annu Rev Public Health 2012; 33:357-76

Complex System
• Elements – Large number – Heterogeneous, within and between – Interact with each other
• Interactions produce emergent properties
• Effects – Persist over time – Adapt to changing circumstances
Luke and Stamatakis, Annu Rev Public Health 2012; 33:357-76

Complex System Need to understand drivers
• Leverage for most powerful and efficient
effects on health outcomes – Seemingly unimportant elements with large
downstream effects? – Combinations of elements? – Unforeseen adverse effects (unintended
consequences)?
Luke and Stamatakis, Annu Rev Public Health 2012; 33:357-76

System Dynamics “top down”
Stocks & flows
Agent-based Modeling “bottom up”
Actors & rules
Network Analysis Nodes & ties among them

Systems Science
• Systems science approaches have the potential to – Identify the most potent early drivers of the
development of obesity and its complications

Systems Science
• Systems science approaches have the potential to – Identify the most potent early drivers of the
development of obesity and its complications – Use for developing (and evaluating) multi-
setting, mutli-component life course interventions
• Address “what works, for whom, and under what circumstances”
Implementation of Interventions How can systems science help?
• Like etiology, implementation is complex – Informed by SNPs, methylated CpG sites,
16s speciation, dopamine reward pathways, insulin resistance…
– But primarily involves stakeholders, interactions, processes

Stakeholders, Processes

But too simple—lacks interactions, feedback, etc
Implementation of Interventions How can systems science help?
• Stakeholders, interactions, processes – Whole of community interventions try to
change them all – Need to study mechanisms (same as ‘omics)
to understand “what works, for whom, and under what circumstances?”

R01 Funded by NIH (NHLBI, OBSSR) 2013-2018
Systems Science to Drive Whole-of-community Childhood Obesity Prevention Interventions
Investigator Institution Role Expertise
Gillman Harvard Univ PI Obesity etiology and prevention
Hammond Brookings Inst PI Agent-based modeling
Economos Tufts Univ Co-I CPBR, obesity whole community interventions
Hovmand Washington Univ Co-I Participatory group model building
Allender Deakin Univ Co-I Systems intervention approaches
Swinburn Deakin Univ, Univ Auckland Co-I Community/policy
approaches to obesity

Systems Science to Drive Whole-of-community Childhood Obesity Prevention Interventions
Logic: •Start with 2 completed interventions •Relevant literature •Build initial computational model

Systems Science to Drive Whole-of-community Childhood Obesity Prevention Interventions
Logic: •Start with 2 completed interventions •Relevant literature •Build initial computational model •Refine models with ongoing intervention

Victorian Trial
• Cluster RCT • 12 intervention, 12 control communities • Funded by Victoria state and Australia
federal government ($160m) • Consortium of state government,
academia, NGO evaluation unit

Systems Science to Drive Whole-of-community Childhood Obesity Prevention Interventions
Logic: •Start with 2 completed interventions •Relevant literature •Build initial computational model •Refine models with ongoing intervention •Use to design new intervention

Departure from:
Linear thinking
Multiple causation
Independent levels of influence
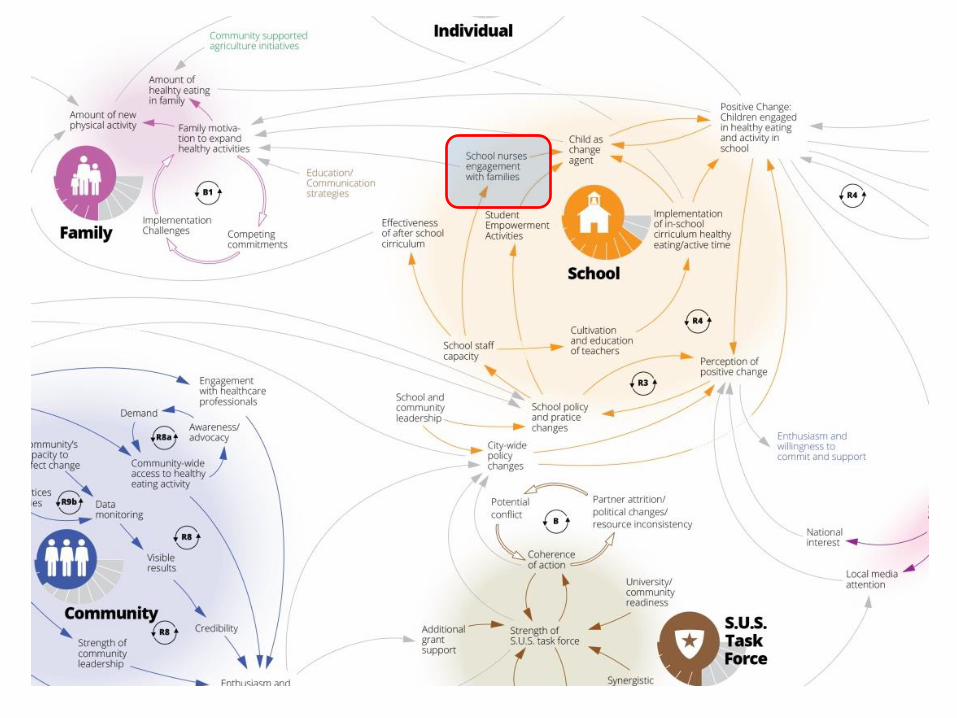
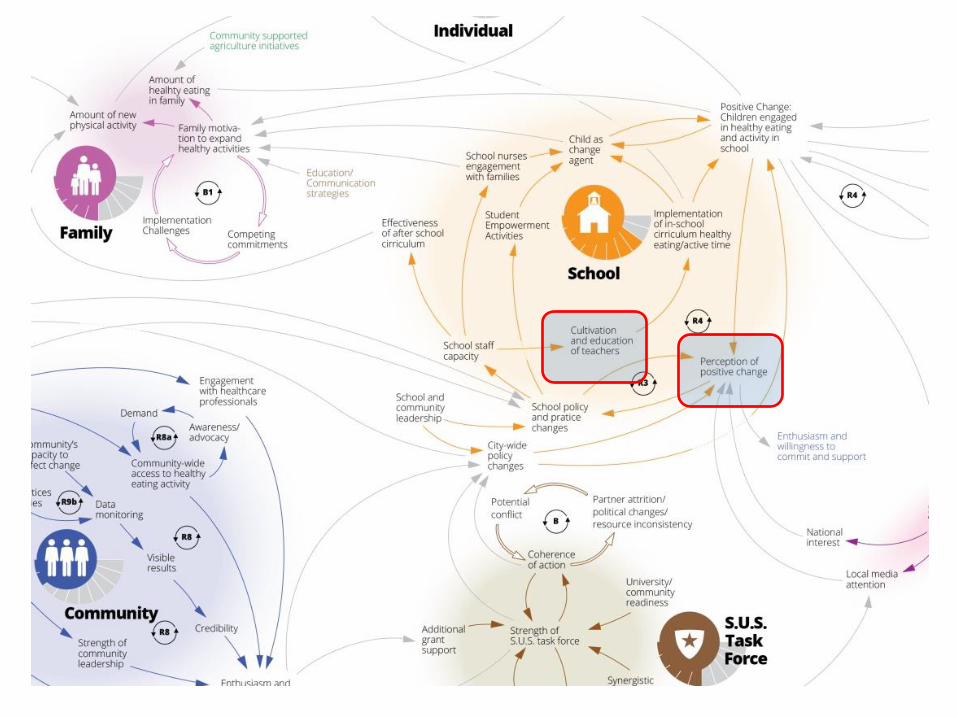
Systems Approach to Obesity Prevention: “Whole of community”
Courtesy Christina Economos

Creating a Causal Loop Map: The Shape Up Somerville Experience
• Develop understanding of whole system – Describes key dynamics of social change
within Somerville over time (10 y) – Based on CBPR – Informed by qualitative individual and group
interviews with key SUS stakeholders and researchers
– Illustrated through integration of complex, reciprocal, interdependent, and interactive relationships among individuals and their environments
• Highlights importance of context

X
Economos et al., submitted

X

X



SUS Model
• Based on deep qualitative knowledge • But
– Retrospective – Not quantitative – School age, not younger – Replicable? Refinable? Predictive?

ABM = Agent-based modeling GMB = Participatory group model building
Systems Science to Drive Whole-of-community Childhood Obesity Prevention Interventions

Participatory Group Model Building
• Involves participants and other stakeholders in iterative process of developing system dynamics (and, now, agent-based) models – Problem conceptualization – Formulation – Policy analysis – Implementation
• Reasons for using GMB
– Sharing of insights – Developing consensus – Design for implementation
Hovmand

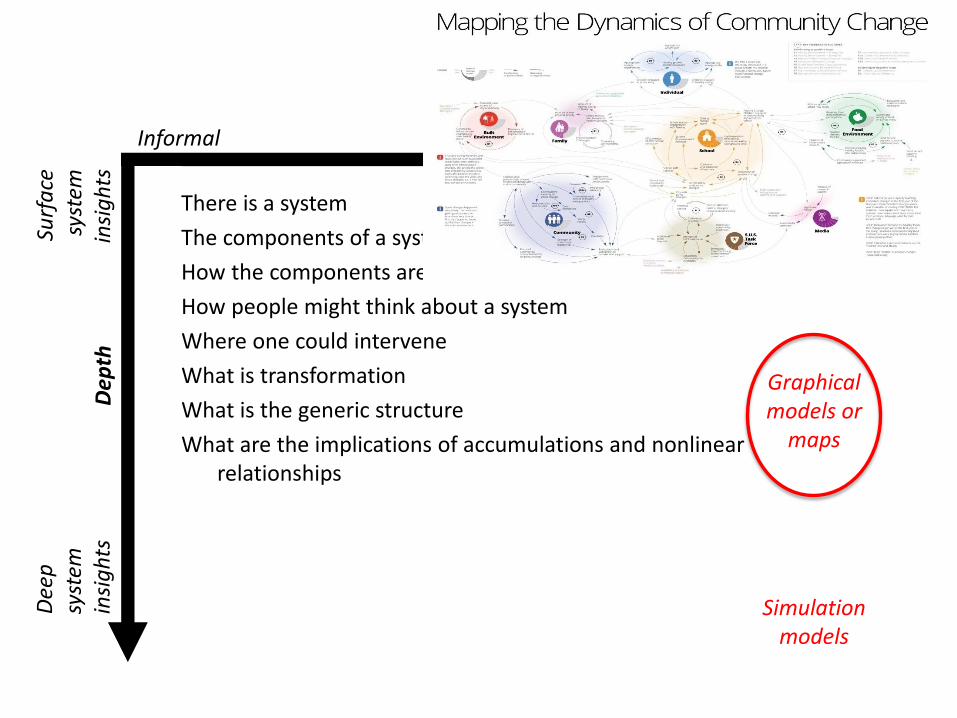
Levels of System Insights
There is a system
The components of a system
How the components are related through feedback
How people might think about a system
Where one could intervene
What is transformation
What is the generic structure
What are the implications of accumulations and nonlinear relationships
What systems can generate the dynamic behavior
Where are the leverage points
When do boundary conditions determine behavior
Why do things happen Dee
p
syst
em
insi
gh
ts
Surf
ace
sy
stem
in
sig
hts
Graphical models or
maps
Simulation models
Dep
th
Informal Formal Modeling
System pictures or diagrams
Hovmand

Levels of System Insights
There is a system
The components of a system
How the components are related through feedback
How people might think about a system
Where one could intervene
What is transformation
What is the generic structure
What are the implications of accumulations and nonlinear relationships
What systems can generate the dynamic behavior
Where are the leverage points
When do boundary conditions determine behavior
Why do things happen Dee
p
syst
em
insi
gh
ts
Surf
ace
sy
stem
in
sig
hts
Graphical models or
maps
Simulation models
Dep
th
Informal Formal Modeling
System pictures or diagrams
October 5, 2012
There is a system
The components of a system
How the components are related through feedback
How people might think about a system
Where one could intervene
What is transformation
What is the generic structure
What are the implications of accumulations and nonlinear relationships
What systems can generate the dynamic behavior
Where are the leverage points
When do boundary conditions determine behavior
Why do things happen Dee
p
syst
em
insi
gh
ts
Surf
ace
sy
stem
in
sig
hts
Graphical models or
maps
Simulation models
Dep
th
Informal Formal Modeling
System pictures or diagrams
X
X X x

Levels of System Insights
There is a system
The components of a system
How the components are related through feedback
How people might think about a system
Where one could intervene
What is transformation
What is the generic structure
What are the implications of accumulations and nonlinear relationships
What systems can generate the dynamic behavior
Where are the leverage points
When do boundary conditions determine behavior
Why do things happen Dee
p
syst
em
insi
gh
ts
Surf
ace
sy
stem
in
sig
hts
Simulation models
Dep
th
Informal Formal Modeling
System pictures or diagrams
Hovmand

Conclusions
• Systems science approaches have the potential to – Identify the most potent early drivers of the
development of obesity and its complications – Use for developing multi-setting, mutli-
component life course interventions • Address what works, for whom, and under what
circumstances
Questions
• In general…What do system science approaches offer over and above …
• More specifically – Initial steps often qualitative – Inputs are often quantitative – Pros and cons of ABM, SD for different
circumstances. Other approaches?

Questions
• In general…What do system science approaches offer over and above …
• More specifically – Initial steps often qualitative – Inputs are often quantitative – Pros and cons of ABM, SD – When do we have enough data?
• Right balance of too little/too much • Face, construct, criterion validity?

Questions
• In general…What do system science approaches offer over and above …
• More specifically – Initial steps often qualitative – Inputs are often quantitative – Pros and cons of ABM, SD – When do we have enough data? – Generalizability (as usual)

Agent-based Model

Finucane et al., Lancet 2011; 377: 557–67
Worldwide increases in adult obesity 1980-2008
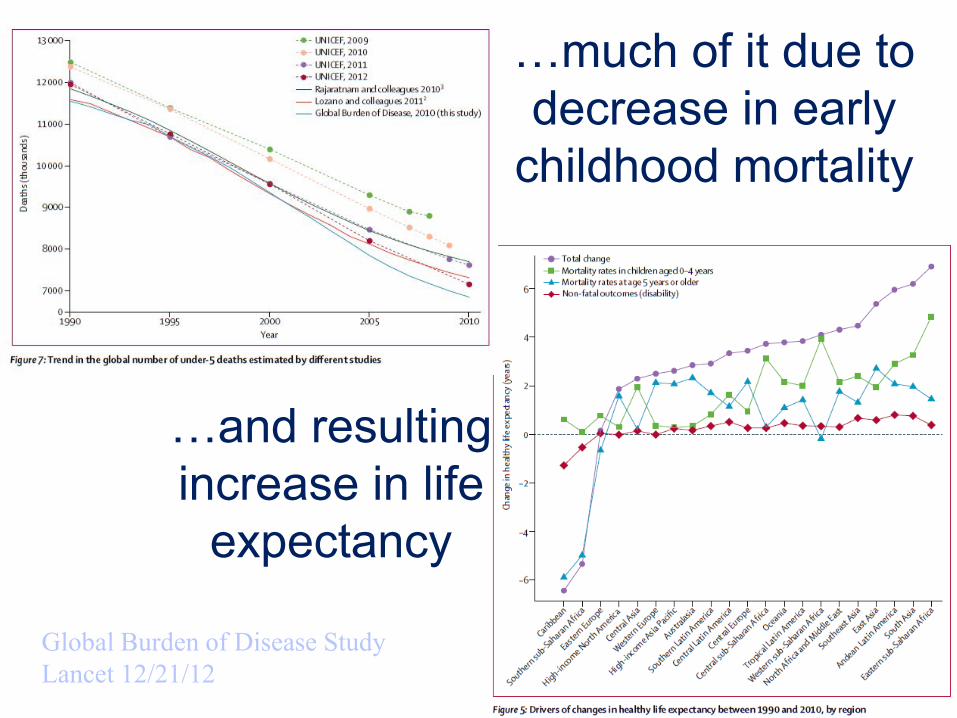
Global Burden of Disease Study Lancet 12/21/12
…much of it due to decrease in early
childhood mortality
…and resulting increase in life
expectancy
Developmental Origins of Health and Disease
• DOHaD emphasizes prenatal period and early childhood as important periods for development of chronic disease throughout life

Developmental Origins of Obesity
• Together pre- and post-natal risk factors predict a substantial fraction of childhood obesity
• Prevention interventions starting in pregnancy and infancy have potential to – Reduce these risk factors – Thus obesity-related disorders – And interrupt intergenerational vicious cycles



Developmental Origins Research
• In animal models, perinatal programming of adult health outcomes well known
• Programming – Perturbation at a critical period of
development causes alterations with lifelong, sometimes irreversible consequences

Zygote
Adult
Neonate 45 Divisions
55 Divisions
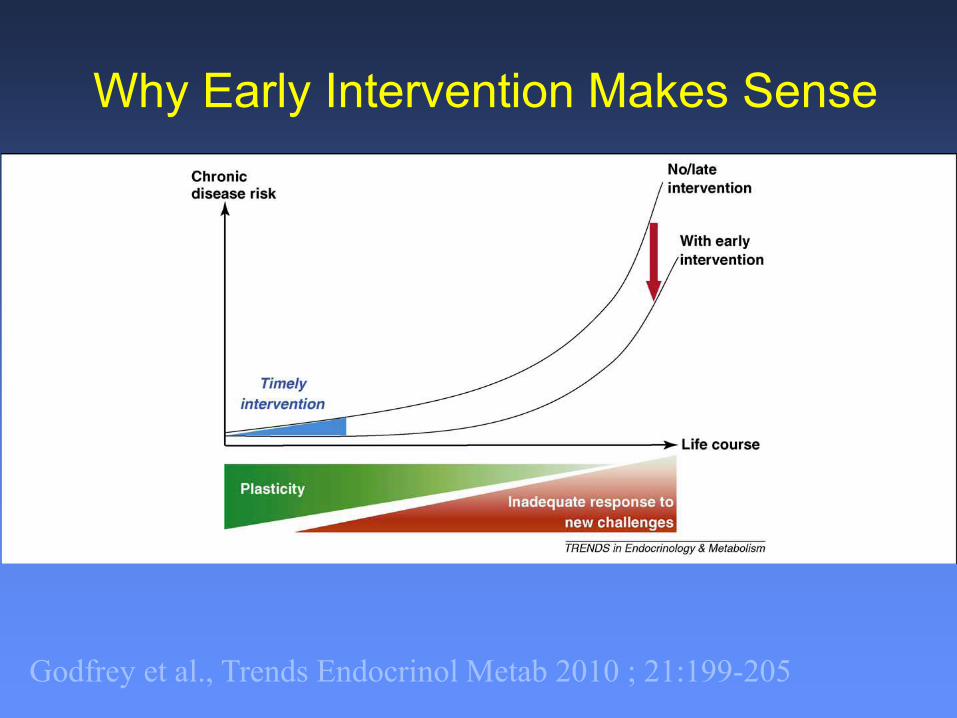
Godfrey et al., Trends Endocrinol Metab 2010 ; 21:199-205
Why Early Intervention Makes Sense

Conclusions
• Together pre- and post-natal risk factors predict a substantial fraction of childhood obesity
• Prevention interventions starting in pregnancy and infancy have potential to – Reduce these risk factors – Thus obesity-related disorders – And interrupt intergenerational vicious cycles

Luke and Stamatakis, Annu Rev Public Health 2012; 33:357-76.


















