
Surgical treatment of a gastric diverticulum in an adolescent
3
Surgical treatment of a gastric diverticulum in an adolescent Steven Elliott, Anthony D. Sandler, John J. Meehan, John P. Lawrence * Division of Pediatric Surgery, The University of Iowa Hospitals and Clinics, Iowa City, IA 52242, USA Abstract Gastric diverticula are uncommonly seen in childhood. They typically emanate from the posterior wall of the stomach near the gastroesophageal junction. The authors report on a 15-year-old adolescent boy who presented with a symptomatic gastric diverticulum that was surgically resected. Potential pitfalls in diagnosis and treatment are discussed. D 2006 Elsevier Inc. All rights reserved. Gastric diverticula are unusual malformations assumed to be of congenital origin when seen in the pediatric population. The symptoms associated with a gastric diverticulum are often vague and nonspecific. We present a case of an adolescent treated for a gastric diverticulum that highlights useful diagnostic modalities and an approach helpful for surgical treatment. 1. Case report A 15-year-old adolescent boy was referred to our facility for evaluation of symptoms of left-sided abdominal pres- sure. The patient had experienced a bfull feelingQ intermit- tently for about 4 months in the left flank region. He described the sensation of pressure to be worse with eating and when lying on his left side. He denied vomiting or any abnormal bowel function. His past medical history was remarkable for mononucleosis the previous year. Both his mother and maternal grandfather had a history of peptic ulcer disease. Physical examination revealed him to be a well-developed adolescent boy in no acute distress. His abdominal exam revealed no tenderness, masses, or other abnormalities. Examination of his left flank and back was also unremarkable. The patient’s local physician had instituted empiric therapy for gastroesophageal reflux with a proton pump inhibitor several months previously; this failed to relieve his symptoms. One week before referral, an abdominal ultra- sound was performed, demonstrating a left suprarenal lesion (Fig. 1). This was subsequently followed by a computed tomography (CT) scan of the abdomen that indicated a possible gastric diverticulum situated in the left suprarenal region (Fig. 2). To confirm the diagnosis, an upper gastrointestinal (GI) series was obtained, demonstrating a diverticulum directed posteriorly off the fundus of the stomach (Fig. 3). Because of the strong family history of ulcer disease and the possibility of gastroesophageal reflux, an upper endoscopy was performed. A gastric diverticulum was visualized in the fundus of the stomach (Fig. 4); the gastric mucosa was mildly erythematous and the lower esophageal sphincter was felt to be somewhat patulous. The patient was taken to surgery and the operation was performed through a left subcostal incision. After division 0022-3468/$ – see front matter D 2006 Elsevier Inc. All rights reserved. doi:10.1016/j.jpedsurg.2006.04.010 * Corresponding author. Tel.: +1 319 356 1766; fax: +1 319 356 8378. E-mail address: [email protected] (J.P. Lawrence). Index words: Gastric diverticulum; Congenital; Surgery Journal of Pediatric Surgery (2006) 41, 1467 – 1469 www.elsevier.com/locate/jpedsurg
-
Upload
steven-elliott -
Category
Documents
-
view
213 -
download
1
Transcript of Surgical treatment of a gastric diverticulum in an adolescent

www.elsevier.com/locate/jpedsurg
Surgical treatment of a gastric diverticulumin an adolescent
Steven Elliott, Anthony D. Sandler, John J. Meehan, John P. Lawrence*
Division of Pediatric Surgery, The University of Iowa Hospitals and Clinics, Iowa City, IA 52242, USA
0022-3468/$ – see front matter D 2006
doi:10.1016/j.jpedsurg.2006.04.010
* Corresponding author. Tel.: +1 319
E-mail address: john-lawrence@uio
Index words:Gastric diverticulum;
Congenital;
Surgery
Abstract Gastric diverticula are uncommonly seen in childhood. They typically emanate from the
posterior wall of the stomach near the gastroesophageal junction. The authors report on a 15-year-old
adolescent boy who presented with a symptomatic gastric diverticulum that was surgically resected.
Potential pitfalls in diagnosis and treatment are discussed.
D 2006 Elsevier Inc. All rights reserved.
Gastric diverticula are unusual malformations assumed to
be of congenital origin when seen in the pediatric
population. The symptoms associated with a gastric
diverticulum are often vague and nonspecific. We present
a case of an adolescent treated for a gastric diverticulum that
highlights useful diagnostic modalities and an approach
helpful for surgical treatment.
1. Case report
A 15-year-old adolescent boy was referred to our facility
for evaluation of symptoms of left-sided abdominal pres-
sure. The patient had experienced a bfull feelingQ intermit-
tently for about 4 months in the left flank region. He
described the sensation of pressure to be worse with eating
and when lying on his left side. He denied vomiting or any
abnormal bowel function. His past medical history was
remarkable for mononucleosis the previous year. Both his
mother and maternal grandfather had a history of peptic
Elsevier Inc. All rights reserved.
356 1766; fax: +1 319 356 8378.
wa.edu (J.P. Lawrence).
ulcer disease. Physical examination revealed him to be a
well-developed adolescent boy in no acute distress. His
abdominal exam revealed no tenderness, masses, or other
abnormalities. Examination of his left flank and back was
also unremarkable.
The patient’s local physician had instituted empiric
therapy for gastroesophageal reflux with a proton pump
inhibitor several months previously; this failed to relieve his
symptoms. One week before referral, an abdominal ultra-
sound was performed, demonstrating a left suprarenal lesion
(Fig. 1). This was subsequen tly followed by a compu ted
tomography (CT) scan of the abdomen that indicated a
possible gastric diverticulum situated in the left suprarenal
region (Fig. 2). To confirm t he diagnosis, an upper
gastrointestinal (GI) series was obtained, demonstrating a
diverticulum directed posteriorly off the fundus of the
stomach (Fig. 3). Bec ause of the stro ng fami ly hist ory of
ulcer d isease and the possi bility of gastr oesopha geal reflux,
an upper endoscopy was performed. A gastric diverticulum
was visua lized in the fundus of the stomach (Fig. 4); the
gastric mucosa was mildly erythematous and the lower
esophageal sphincter was felt to be somewhat patulous.
The patient was taken to surgery and the operation was
performed through a left subcostal incision. After division
Journal of Pediatric Surgery (2006) 41, 1467–1469
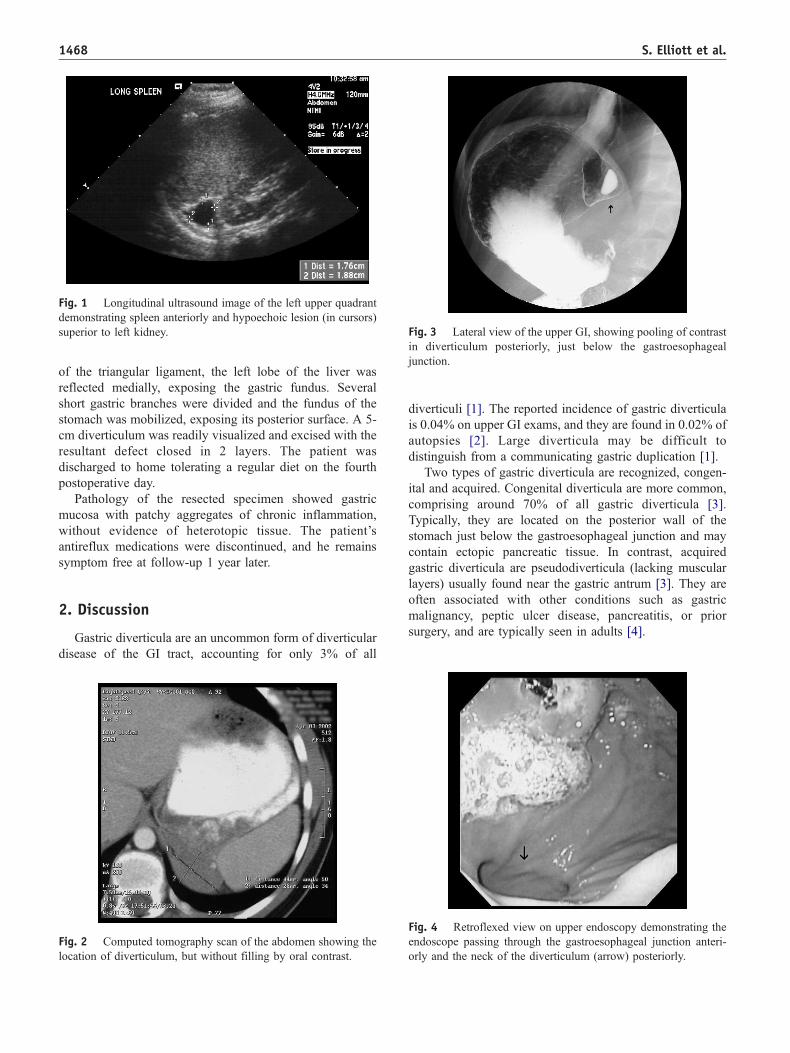
Fig. 1 Longitudinal ultrasound image of the left upper quadrant
demonstrating spleen anteriorly and hypoechoic lesion (in cursors)
superior to left kidney. ig. 3 Lateral view of the upper GI, showing pooling of contrast
diverticulum posteriorly, just below the gastroesophageal
nction.
S. Elliott et al.1468
of the triangular ligament, the left lobe of the liver was
reflected medially, exposing the gastric fundus. Several
short gastric branches were divided and the fundus of the
stomach was mobilized, exposing its posterior surface. A 5-
cm diverticulum was readily visualized and excised with the
resultant defect closed in 2 layers. The patient was
discharged to home tolerating a regular diet on the fourth
postoperative day.
Pathology of the resected specimen showed gastric
mucosa with patchy aggregates of chronic inflammation,
without evidence of heterotopic tissue. The patient’s
antireflux medications were discontinued, and he remains
symptom free at follow-up 1 year later.
2. Discussion
Gastric diverticula are an uncommon form of diverticular
disease of the GI tract, accounting for only 3% of all
Fig. 2 Computed tomography scan of the abdomen showing the
location of diverticulum, but without filling by oral contrast.
Fin
ju
diverticu li [1]. The report ed incidence of gastr ic diver ticula
is 0.04% o n upper GI exams, an d they are found in 0.02% of
autopsies [ 2] . Large di ve rticula may be diff icult t o
distingu ish from a comm unicating gastric du plication [1].
Two types of gastric diverticula are recognized, congen-
ital and acquired. Congenital diverticula are more common,
co mprising around 70% of a ll gastric diver ticula [3].
Typically, they are located on the posterior wall of the
stomach just below the gastroesophageal junction and may
contain ectopic pancreatic tissue. In contrast, acquired
gastric diverticula are pseudodiverticula (lacking muscular
layers) usual ly found near the gastr ic antru m [3]. They are
often associated with other conditions such as gastric
malignancy, peptic ulcer disease, pancreatitis, or prior
surge ry, and are typi cally seen in adu lts [4].
Fig. 4 Retroflexed view on upper endoscopy demonstrating the
endoscope passing through the gastroesophageal junction anteri-
orly and the neck of the diverticulum (arrow) posteriorly.

Surgical treatment of a gastric diverticulum in an adolescent 1469
Patients with gastric diverticula may remain asymptom-
atic throughout life. When symptoms do arise, they most
commonly are upper abdominal pain, nausea, and emesis
[3]. Occasiona lly, patients with gastr ic d iverticula can have
dramatic presentations related to massive bleeding or
perforation. Not unexpectedly, given the posterior location,
physical exam in most children with this disorder is
unremarkable.
The ability to definitively diagnose a gastric diverticulum
can be difficult. Ultrasound or CT scans are commonly the
first studi es radiographi cally performed to evalua te abdom -
inal symptoms in children; either can suggest the diagnosis
of a gastric diverticulum, but may not be specific. Confusion
with adrenal masses, splenic abnormalities, or pancreatic tail
lesions may occur [5]. Ora lly adminis tered contr ast shoul d
be given to facilitate diagnosing gastric diverticula during
CT scanning. More certain diagnosis is often made by upper
endoscopy or an upper GI series, although both modalities
can sti ll miss the lesi on if it has a narrow neck [3]. To
optimize yield, a right anterior oblique view should be used
in an upper GI seri es [3,6]. Uppe r endosco py can rule out
associated pathology and may be able to reproduce
symptom s with distention of the diverticu lum [6].
Surgical resection is the recommended treatment for
symptomatic gastric diverticula. The standard approach is to
open the gastrocolic omentum to visualize the posterior
gastric wal l [3,6]. Difficulty is encount ered in locat ing
known diverticula through this technique, and anterior
gastrostomy to identify the neck of the lesion is reported
[6]. Alternativel y, we would propose that gi ven the
propensity for gastric diverticula to be located near the
gastroesophageal junction, superior mobilization of the
fundus (as might be performed for a fundoplication) gives
a more direct approach to the anticipated location of these
lesions. Laparoscopic resection is also a viable surgical
modalit y for treatmen t [7].
References
[1] Simstein N. Congenital gastric anomalies. Am Surg 1986;52(5):264-8.
[2] Palmer ED. Gastric diverticula. Surg Obstet Gynecol 1951;92:417 -28.
[3] Rodeberg DA, Zaheer S, Moir CR, et al. Gastric diverticulum: a
series of four pediatric patients. J Pediatr Gastroenterol Nutr 2002;
34(5):564-7.
[4] Eras P, Berenbaum S. Gastric diverticula: congenital and acquired. Am
J Gastreoenterol 1972;57:120-32.
[5] Chasse E, Buggenhout A, Zalcman M, et al. Gastric diverticulum
simulating a left adrenal tumor. Surgery 2003;133(4):447 -8.
[6] Anaise D, Brand DL, Smith NL, et al. Pitfalls in diagnosis and
treatment of a symptomatic gastric diverticulum. Gastrointest Endosc
1984;30(1):28 -30.
[7] Fine A. Laparoscopic resection of a large proximal gastric diverticu-
lum. Gastrointest Endosc 1998;48(1):93 -5.


















