Gastric surgery and NOTESsemmelweis.hu/sebeszet1/files/eloadasok/eng/gastricLP.pdfOesophageal...
26
Gastric surgery and NOTES Péter LUKOVICH M.D. Semmelweis University, Faculty of Medicine, 1 st Department of Surgery
Transcript of Gastric surgery and NOTESsemmelweis.hu/sebeszet1/files/eloadasok/eng/gastricLP.pdfOesophageal...

Gastric surgery and NOTES
Péter LUKOVICH M.D.
Semmelweis University, Faculty of Medicine, 1st Department of Surgery

Blood supply of the stomach
and the duodenum
Celiac trunk - a. gastrica sin.
- a hepatica comm. - a. gastroepiploica d.
- a. hepatica comm. - a. gastrica d.
- a. lienalis - a. gastroepiploica sin.
- a lienalis - a. gastricae breves

Anamnesis (familiar: ulcer,cancer)
Complains (vomitus, haematemesis, anaemia (iron deficiency) disgust of meat)
Physical examination (palpable mass, Wirchow lymph node)
Contrast X-ray
Endoscopy
Endoscopic Ultrasound (EUS)
CT
Virtual endoscopy
Capsule endoscopy
Helicobacter pylori test
Scintigraphy
Lab test: Gastrin level (Zollinger-Ellison syndrome) >50-100 pg/ml
Laparoscopy, laparotomy
Examination of the stomach

Congenital dieseases of the stomach
and the duodenum
Duodenum atresia Rare, double bubble sign : X-ray
Congenital pylorus stenosis
Pancreas annulare Frequency 1:6-7000
Meckel diverticulum
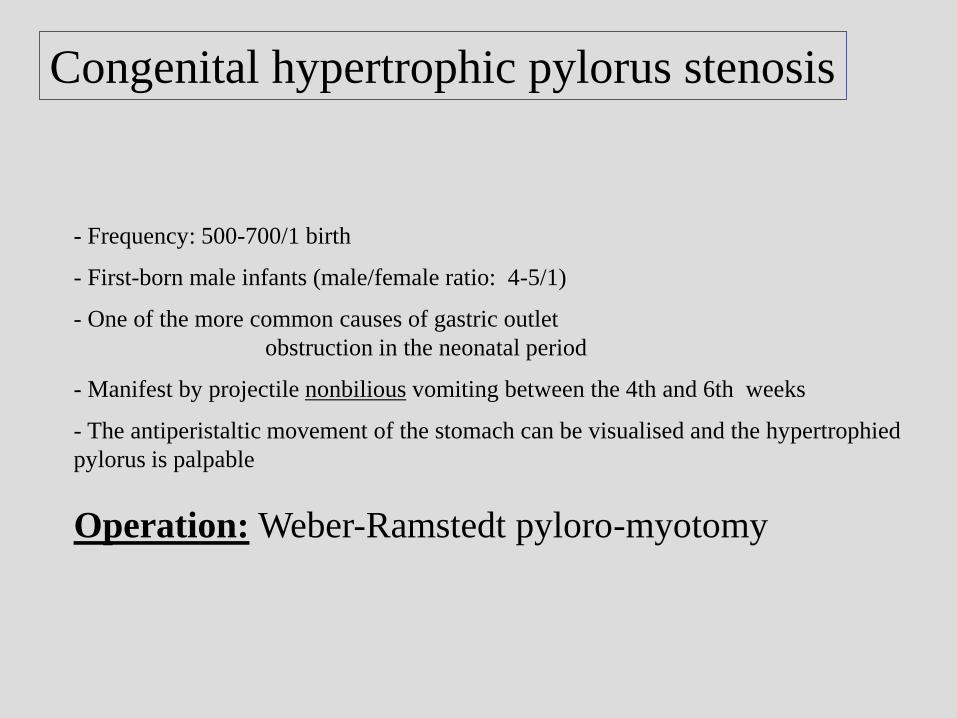
Congenital hypertrophic pylorus stenosis
- Frequency: 500-700/1 birth
- First-born male infants (male/female ratio: 4-5/1)
- One of the more common causes of gastric outlet
obstruction in the neonatal period
- Manifest by projectile nonbilious vomiting between the 4th and 6th weeks
- The antiperistaltic movement of the stomach can be visualised and the hypertrophied
pylorus is palpable
Operation: Weber-Ramstedt pyloro-myotomy

Pancreas anulare
1818 Tiedemann discribed at the first time
1862 Ecker gave the name: pancreas anulare
Drey classified: (neonatal, child age,
asymptomatic and symptomatic in the adult age
Rare disease: 20 000/3
(boncolt esetek)
Male/female ratio : 1/1

In 75% with other congenital diseaeses
Down syndrom
Tracheo-oesophageal fistula
Oesophageal atresia
Anus imperforatus
Hirchsprung disease
Duodenal atresia
Meckel diverticulum
Pancreas anulare

Ulcer of the stomach and the duodenum
Etiology
1., Familiar
2., Hyperacidity (Schwartz 1910 - "Ohne saure kein Ulcus”)
Peptic ulcer is not peptic, Zollinger-Ellison syndrome
3., Decreased level of the protective factors
(pepsin and bicarbonat, prostaglandin level)
4., Blood group - "O" blood group
5., Non steroid antiinflammatory drugs (aspirin)
6., Steroid therapy
7., Helicobacter pylori infection
8., Stress
9., Damage of the blood supply of the duodenum
10., Others Curling ulcer - after burning
Cushing ulcer - after trauma of the brain

Complication of the ulcer
of the stomach and the duodenum
Perforation
Pylorus stenosis
Bleeding

Perforation of the ulcer
Complains: Usually the ulcer on the anterior wall could perforate
Epigastrial pain like thrust of the knife -
later pain in the right lower quadrant (Moynihan tunnel)
Differential diagnosis: Appendicitis!!!
Examinations:
Physical examination: free air in the abdominal cavity,
loss of the blunt of the liver (Chilaiditi syndrome!)
defanse musculaire - peritonitis
no movement of the the bowels
Nativ abdominal X-ray:
air in the abdominal cavity (under the diaphragma)
Operation: suture of the perforation (+covering with omentum)
Neumann
resection of the stomach
Minimal invasiv technic: laparo-gastroscopy

P. Lukovich
Heinecke-Mikulicz
Finney
Jaboulay
Pyloromyotomy (Aust)
Pyloroplasty

Forrest classification of the ulcer
I. active bleeding Ia: spuring bleeding
Ib: oozing bleeding
II. signs of the previous bleeding
IIa: black surface
IIb: visible stump of vessel
IIc: coagulum
III. without any sign of bleeding
Bleeding of the ulcer

Surgery: vagotomy
1. Truncal vagotomy
2. Selectiv vagotomy
3. Superselectiv vagotomy
Now it is a history!

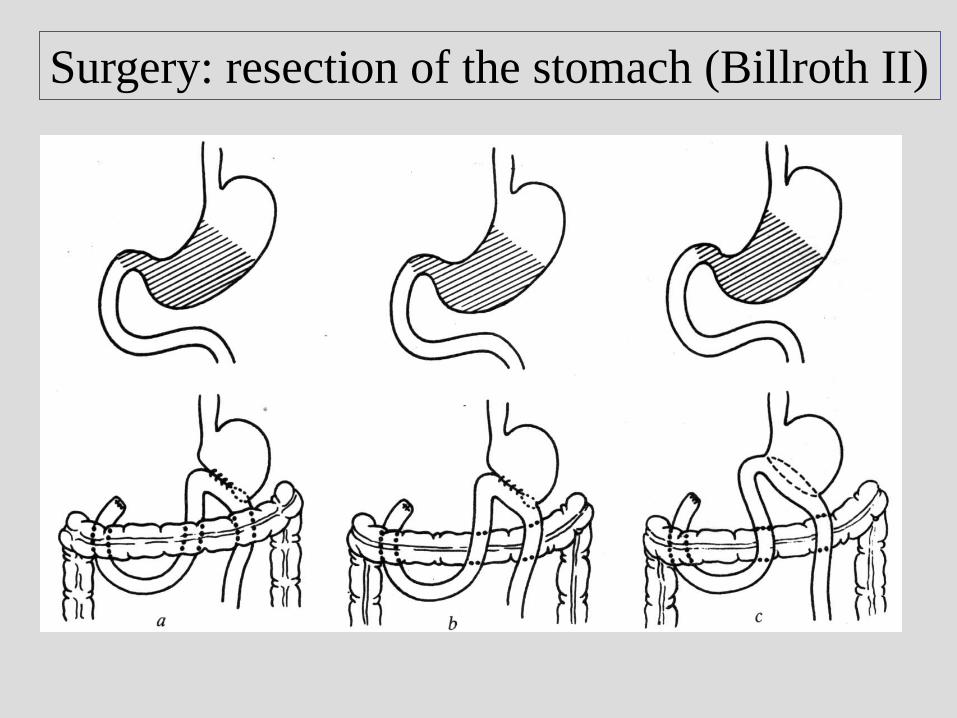
Surgery: resection of the stomach
Billroth-I resection Billroth-II resection

Surgery: resection of the stomach (Billroth-I)
of the stomach
and
the small bowel
Surgery: resection of the stomach (Billroth II)

Gastric cancer:
Incidence of the gastric cancer
decreased in USA
increase in Japan, Chile, Iceland
Peak of incidence in the 5th decade in the life
Male/female ratio: 2/1

Gastric cancer: epidemiology
Feeding: salt, qualitiy of the drinking water
Smoking
Precancerous diseases:
Polyps: hyperplastic adenomatous polyps
suggested:endoscopic polypectomy or surgical resection
Ulcus chronicum
Atrophic gastritis: Type A (anaemia perniciosa)
antibody against the parietal cells
localized into the fundus
Type B (local irratation of the foods)
localized into the fundus and the antrum
Dysplasia
Menetrier gastritis: suggested: preventiv gastrectomy
After Billroth II resection: bile reflux - after 15-20 yrs of the op

Gastric cancer: clinical presentation
Abdominal pain 66%
Weight loss more than 10% 50%
Nausea, vomiting 32%
GI bleeding 23%
Dysphagia 23%
Mass 36%
Tenderness 20%
Anaemia 42%
Hypoproteinaemia 26%

Gastric cancer: lymphnode metasteses
Kompartment I Kompartment II Kompartment III

Gastric cancer: pathology
Macroscopical appareance:
Bormann calssification
Histological classification:
adenocarcinoma
mucinous adenocarcinoma
round cell carcinoma
planocellular carcinoma
Localisation: antrum: 55%
corpus 35%
cardia 5%
linitis plastica 5%

Gastric cancer: TNM classification
T (primer tumor)T1 infiltration of the lamina propria
T2 infiltration of the subserosa
T3 involve the serosa
T4 involve the surronding organs (pancreas, colon, spleen, diaph)
N (regional lymph nodes)N0 no lymph node metastasis
N1 metastasis in the perigastric lymph nodes(distance <3 cm)
N2 metastasis in the perigastric lymph nodes(distance >3 cm)
Wirchow lymph node
M (distant metastases)Krukenberg tumor
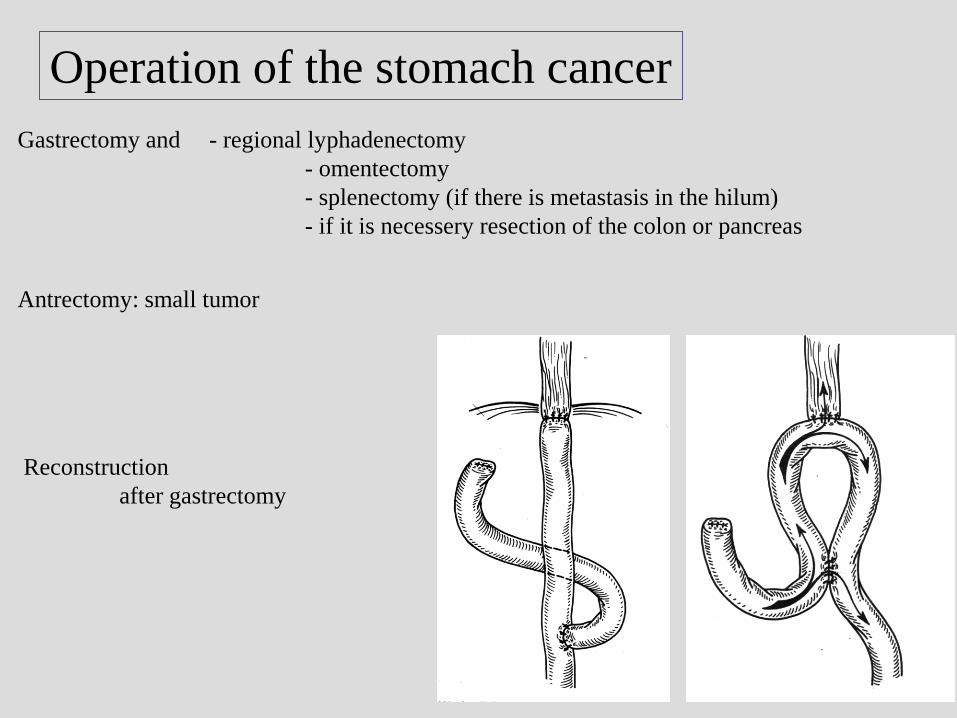
Operation of the stomach cancer
Gastrectomy and - regional lyphadenectomy
- omentectomy
- splenectomy (if there is metastasis in the hilum)
- if it is necessery resection of the colon or pancreas
Antrectomy: small tumor
Reconstruction
after gastrectomy

Gastric cancer: 5 year survival rates
Carcinoma in situ (2%) 100%
Stage I (6%) 43%
Stage II (9%) 42%
Stage III (17%) 6%
Stage IV (67%) 0%
Liver 35-40%
Colon 35-40%
Klatskin 20-30%
Oesophagus 10-20%
Pancreas 8-15%
Gallbladder 0-5%
Stomach 20-25%

Gastro-entero anastomosis (GEA)
Indication: Gastric outlet obstruction
Antecolic – retrocolic
Anterior – posterior
wall of the stomach

P. Lukovich
Indications:
- obstruction of the oesophagus
- feeding problem
(coma, muscle diseases)
Local anaesthesia (high risk patients!)
Surgical gastrostomy
Witzel (1891)
Kader (1896) (Stamm-Senn)
Percutan endoscopic gastrostomy (PEG)