Surgical Management of Ulcerative ColitisB. Severe\ഠulcerative colitis. Mucosal ulceration and...
41
Surgical Management of Ulcerative Colitis Kiyanda Baldwin SUNY Downstate Grand Rounds Kings County Hospital 3/10/11 www.downstatesurgery.org
Transcript of Surgical Management of Ulcerative ColitisB. Severe\ഠulcerative colitis. Mucosal ulceration and...

Surgical Management of Ulcerative Colitis
Kiyanda BaldwinSUNY Downstate Grand Rounds
Kings County Hospital3/10/11
www.downstatesurgery.org

Patient Presentation 54 y/o M h/o UC x16yrs last c-scope low
grade dysplasia PMH UC PSH appendectomy All nkda Meds: prednisone, asacol, 6MP FH NC SH denies x3
www.downstatesurgery.org

H/H 12/36.8
Alb 3.9
CXR wnl
CT minimal thickening of ascending & descending colon w/ pericolonic lymphadenopathy consistent w/ chronic inflammation
UGI series WNL
C-scope pan colitis random Bx chronic inflam, cryptitis, low grade dysplasia
Patient Presentationwww.downstatesurgery.org

Ex-lap, proctocolectomy, double-staple ileal J pouch anal anastomosis, intraopcolonoscopy, diverting loop ileostomy
Path: pancolitis, low grade dysplasia
Now 1 month postop doing well
Patient Presentationwww.downstatesurgery.org

Surgical Management of
Ulcerative Colitis
www.downstatesurgery.org
Presenter
Presentation Notes
40%

Epiemiology Incidence: 8-15/100,000
Incidence lower in Asia, Africa, S. America,
& nonwhite Americans
Peaks in 3rd & 7th decades
Schwartz 9th ed, Maingot 11thed
www.downstatesurgery.org
Presenter
Presentation Notes
Crohn’s 1-5/100,000 incidence & peaks 15-30, 55-60 Smoking protects, ex smokers more likely to have & more severe Appendectomy possibly protective

Etiology Geographic differences suggest
environmental (diet/infection)
Smoking, etoh, OCPs implicated
Genetic? 10-30% have + FH
autoimmune
Schwartz 9th ed, Maingot 11th ed
www.downstatesurgery.org
Presenter
Presentation Notes
-smokers have less incidence, ex smokers higher incidence and more severe -Autoimmune based on extraintestinal manifestations similar to rheumatological disorders

Pathophysiology Poorly understood
Intestinal mucosa continually exposed to
environmental challenge
chronic dysregulation of mucosal immunity
uncontrolled inflammatory response
IL-1B, 6, 8, TNF, prostaglandin (E2), leukotriene B4
exacerbate mucosal inflammation
IL-4, 10 suppress intestinal inflammationMaingot 11thed
www.downstatesurgery.org

Sydney Australia; Neurogastroenterology Motility
Tachykinins, like substance P & neurokinin,
hemokinin
Role in motility, secretion, and immune functions
Tachykinin receptor gene expression was 10-fold
more abundant in colon mucosa of pts w/ UC
compared to Control (p<0.01)
Liu et al, Feb 2011www.downstatesurgery.org

Pathology Colonic mucosa & submucosa infiltrated w/
inflammatory cells
Mucosal edema is the earliest manifestation
Ulcers are linear & knifelike
Atrophic mucosa & crypt abscesses common
mucosa is friable & may have inflammatory pseudopolyps
TI may demonstrate inflammatory changes (backwash ileitis)
Schwartz 9th edition
www.downstatesurgery.org
Presenter
Presentation Notes
Pseudopolyps: as the mucosa erodes, only small islands of mucosa resembling polyps r left Crohns: transmural, mucosal ulcers, noncaseating granulomas, fibrosis, strictures, fistulas, cobblestone on c-scope

Gross Pathology
Mild Colitis
Severe Colitis
www.downstatesurgery.org
Presenter
Presentation Notes
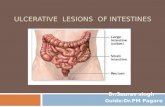
A. Resected rectosigmoid from a patient with mildly active disease showing swollen, congested, and ulcerated mucosa. B. Severe ulcerative colitis. Mucosal ulceration and inflammation is characteristically diffuse and uninterrupted, often extending from the rectum proximally. Chronic ulcerative colitis is frequently associated with the appearance of small pseudopolyps, which represent areas of regenerating mucosa among diffuse mucosal destruction. While the risk of colon cancer is higher in patients with ulcerative colitis, pseudopolyps themselves have no malignant potential.�

Microscopic Pathologywww.downstatesurgery.org
Presenter
Presentation Notes
A. Typical hematoxylin-eosin (H&E)–stained whole mount section of a colon from a patient with severe ulcerative colitis showing broad-based undermined ulcers. Inflammation is limited to the mucosa with no evidence of transmural inflammation or fibrosis, and that might be indicative of Crohn's disease. B. A higher-magnification H&E-stained histological section of an ulcer edge showing overhanging inflamed mucosa. C. High-magnification H&E-stained section of inflamed mucosa showing diffuse acute and chronic inflammation with architectural distortion and destruction of some glands, loss of goblet cells and depletion of mucin from the remaining goblet cells, crypt abscesses, and basal plasmacytosis. The glands show hyperchromatic nuclei with inflammatory atypia.�

Lead Pipe Colonwww.downstatesurgery.org
Presenter
Presentation Notes
If chronic, colon may be foreshortened, mucosa replaced by scar, & lack of haustral markings (lead pipe) Single-contrast barium enema showing chronic ulcerative colitis characterized by shortening and straightening of the colon with loss of haustrations, resulting in the appearance of a featureless tube. No ulcerations are seen.��

Symptoms Bloody diarrhea Abdominal cramping Tenesmus (proctitis) Fulminant colitis
Bloody diarrhea, severe abd pain, dehydration, high fever
Schwartz 9th edition
www.downstatesurgery.org

Diagnosis
Colonoscopy
Mucosal biopsy
Schwartz 9th edition
www.downstatesurgery.org
Presenter
Presentation Notes
Since rectum involved 90-95% of cases flex sig is 1st step

Endoscopy Mild
Moderate
Severe
www.downstatesurgery.org
Presenter
Presentation Notes
A. Endoscopic appearance of the rectum in a patient with mild ulcerative colitis, showing mucosal granularity, diffuse erythema, and loss of the normal vascular pattern. The mucosa is friable and often bleeds on contact. B. Endoscopic appearance of the rectum in a patient with moderate ulcerative colitis, with pitted mucosa and spontaneous hemorrhage. The mucosa is diffusely erythematous, edematous, and granular, with areas of submucosal hemorrhage. A mucopurulent exudate is evident. C. Severe ulcerative colitis showing extensive ulceration with irregular, inflamed, ulcerated mucosa and a patchy exudate.�

Indications for Emergent Surgery
Life threatening hemorrhage (1%) Toxic megacolon (2.5%) Fulminant colitis (15%)*pts who fail to respond to medical therapy*deterioration or failure to improve w/in 24-
48hrs Acute perforation Obstruction due to stricture (11%) Abdominal colectomy w/ ileostomy
Schwartz 9th ed, Maingot 11th ed
www.downstatesurgery.org
Presenter
Presentation Notes
-toxic megacolon = transverse or L colon >5.5cm -Abdominal colectomy w/ ileostomy prevents pelvic dissection in critically ill pt and residual rectum usually isn't much of a prob -if pt really sick, Turnbull’s blow-hole colostomy w/ loop ileostomy -rectal hemorrhage may require proctocolectomy w/ ileostomy or ileal pouch anastomosis

Intractability despite maximal medical
therapy
High risk of complications from medical
therapy
Significant risk of developing colorectal Ca
Indications for Elective Surgery
Schwartz 9th ed, Maingot 11th ed
www.downstatesurgery.org
Presenter
Presentation Notes
-in children extreme growth/developmental retardation, joint, eye, skin respond to colectomy -pyoderma gangrenosum responds 50% & hemolytic anemia (usually +splenectomy) -ankylosing spondylosis & liver dysfunction (primary sclerosing cholangitis) don’t respond

Risk for Colorectal Ca Increased w/ early age at Dx, increased
duration, extent of Dz
Increased w/ duration
2% after 10yrs & increases 0.5-1% annually
afterward
8% after 20yrs
18% after 30yrs
Schwartz 9th edition, Maingot 11th ed, Cameron 10th ed
www.downstatesurgery.org
Presenter
Presentation Notes
Mucosal proctectomy with ileal-anal anastomosis is contraindicated for rectal tumors located in the middle and lower thirds of the rectum. In these patients, a standard proctocolectomy and permanent Brooke ileostomy is recommended

More likely to arise from areas of flat dysplasia making early Dx more difficult
=> pts undergo (40-50) random Bx during colonoscopy
Annual surveillance after 8yrs for pts w/ pancolitis, 15 yrs for pts w/ L. colitis
Ca may be present in up to 20% of pts w/ low grade dysplasia
Risk for Colorectal Ca
Schwartz 9th edition, Maingot 11th ed, Cameron 10th ed
www.downstatesurgery.org

Proctocolectomy & Ileostomy
Single stage
Curative
Incontinent
Use of collecting device
20% morbidity:
Hemorrhage, sepsis, neural injuryMaingot 11th ed
www.downstatesurgery.org
Presenter
Presentation Notes
Bladder & sexual dysfunction due to parasympathetic N injury -1940’s cure was coloproctectomy, 50’s brooke ileostomy

Subtotal Colectomy & Ileal-rectal Anastomosis No need for stoma
Pelvic autonomic nerves are undisturbed
Not curative, 20% proctectomy
Contraindicated in pts w/
Anal sphincter dysfunction, severe rectal Dz,
rectal dysplasia, or malignancyMaingot 11th ed
www.downstatesurgery.org

Continent Ileostomy/ Koch Pouchwww.downstatesurgery.org
Presenter
Presentation Notes
1960’s

Continent Ileostomy/ Koch Pouch
45-50cm of terminal ileum is used
The proximal 30-35cm is fashioned into a pouch
The outflow tract is intussuscepted & sutured/stapled
creating a nipple valve
The reservoir is sutured to the peritoneum & fascia
The efferent limb is externalized as a flush stoma
Passing a soft plastic tube through the nipple valve
empties the pouchMaingot 11th ed
www.downstatesurgery.org

Offered a curative resection and continence
Complicated by Nipple valve failure requiring revision 60%
Enteritis, pouchitis, nonspecific ileitis
Fat & B12 malabsorption
Neural and perineal wound problems similar to that of standard proctocolectomy
Still 2/3 are satisfied after 30 yrs
Continent Ileostomy/ Koch Pouch
Maingot 11th ed, Lepisto et al 2003
www.downstatesurgery.org
Presenter
Presentation Notes
-nipple valve failure: dislodgement incontinence, or difficulty emptying the pouch -fistulas btw pouch & skin -stagnant loop syndrome -probly best 4 pts w/ existing ileostomy who want a continent restoring procedure or failed IPAA

Total Proctocolectomy w/ Ileal Pouch-Anal Anastomosis
End to end ileal-anal anastomosis at the dentate line
Benefits Preserve parasympathetics
Preservation of the anorectal sphincter
Elimination of the perineal proctectomy
Permanent ileostomy not required, maintains continence
High stool frequency
Diverting loop ileostomyMaingot 11th ed
www.downstatesurgery.org
Presenter
Presentation Notes
-1st ileal-anal anastomosis by nissen in germany in ’30’s but mark ravitch & david sabiston proposed anal sphincter preservation -also procedure of choice for familial adenomatous polyposis & hereditary nonployposis colorectal ca -age is not a contraindication -associated w decreased fertility for woman -Taylor et al 1983 pouch associated w/ less diarrhea, better continence, & improved quality of life

R/O Crohn’s or other pathology preop
Colonoscopy & biopsy
UGI series
Intraoperative palpation of SB
Total Proctocolectomy w/ Ileal Pouch-Anal Anastomosis
www.downstatesurgery.org

Operative Technique of IPAA
Lithotomy
Midline incision
Colon mobilization
Transect ileum ~1-2cm proximal to ICV
Ileocolic A & colonic mesentery serially clamped, divided, & ligated
Rectal mobilization to the levator ani sling
Transect rectum 1-2cm above dentate line
Maingot 11th ed
www.downstatesurgery.org

Ileal Pouch Construction
A. J-pouch, B. S-pouch, C. Side-to-side isoperistaltic pouch, and D. W-pouch
www.downstatesurgery.org

Ileal J-Pouch
www.downstatesurgery.org
Presenter
Presentation Notes
-faster, less tedious, less ileum, similar or better functional results Pouch is filled w saline to check staple line (should hold 2-300cc) -2 help pouch reach: mobilize SB mesentery including division of attachments of the 3rd portion of the duodenum, score peritoneum of mesentery 1-2cm more

Ileal J-Pouch 15-20cm of the stapled off TI is folded onto itself in the
shape of a J
The distal/efferent limb is secured to the afferent limb
The pouch is formed using sequential firings of a 75-mm
mechanical stapler applied through an enterotomy in the
apex of the pouch
Pouch is filled w saline to check staple line (should hold 2-
300cc)
Mobilize the SB mesentery so the pouch can reach the pelvis
w/ no tensionMaingot 11th ed
www.downstatesurgery.org

Hand Sewn Ileal-anal Anastomosiswww.downstatesurgery.org
Presenter
Presentation Notes
Transperineal mucosal proctectomy: infiltrate submucosa w epi, circumferential incision at dentate line, dissect rectal mucosa from anal sphincter & rectal muscularis -The ileal J-pouch is secured to the sphincter in each quadrant with a suture. The purse-string stitch closing the enterotomy is cut to allow the apex of the pouch to open. An anastomosis is then created between the apex of the pouch and the anoderm with interrupted absorbable sutures.

Double-Staple
Ileal-anal Anastomosis
www.downstatesurgery.org
Presenter
Presentation Notes
Double-staple technique for ileal pouch–anal anastomosis using an end-to-end anastomosing (EEA) stapler. After the pouch is constructed, the head of an EEA stapler is secured in the apex of the pouch and connected to the pin of the stapler, which was placed upward through the anus

Mucosectomy vs Double Staple
Double Staple = retained rectal mucosa => potential for proctitis & Ca
Double staple Increased anal resting pressure
Preservation of the rectoanal inhibitory reflex
Improved continence
Fewer septic complications
Other studies have shown no difference
=> surgeon’s preferenceMaingot 11th ed, Hallgren et al 1995
www.downstatesurgery.org

Salient Points Pathophysiology still poorly understood Emergent surgery
Hemorrhage, Toxic megacolon, Fulminant colitis, Perforation, Obstruction
Subtotal colectomy w/ ileostomy
Elective surgery Intractability of symptoms, complications from
medications, risk of Ca Total proctocolectomy w/ IPAA
Total proctocolectomy w/ Ileal J pouch AA R/O other pathology preoperatively Provides curative surgery w/ continence
www.downstatesurgery.org

References Schwartz’s Principles of Surgery, 9th Edition 2010 Current Surgical Therapy, 9th Edition Cameron 2008 Maingot’s Abdominal Operations, 11th Edition 2007 Liu L, Markus I, Saghire HE, et al. Distinct differences in tachykinin gene expression in
ulcerative colitis, Crohn’s disease, and diverticular disease: a role for hemokinin-1? Neurogastroenterology Motility. no. doi: 10.1111/j.1365-2982.2011.01685.x
Larson DW, Pemberton JH. Current concepts and controversies in surgery for IBD. Gastroenterology 2004;126:1611–1619
Cheung O, Regueiro MD. Inflammatory bowel disease emergencies. Gastroenterol Clin North Am 2003;32:1269–1288 Lepisto AH, Jarvinen HJ. Durability of Kock continent ileostomy. Dis Colon Rectum 2003;46:925–928
Lepisto AH, Jarvinen HJ. Durability of Kock continent ileostomy. Dis Colon Rectum2003;46:925–928
Borjesson L, Oresland T, Hulten L. The failed pelvic pouch: conversion to a continent ileostomy. Tech Coloproctol 2004;8:102–105
Heppell J, Kelly KA, Phillips SF et al. Physiologic aspects of continence after colectomy, mucosal proctectomy, and endorectal ileal-anal anastomosis. Ann Surg 1982;195:435–443
Parks AG, Nicholls RJ. Proctocolectomy without ileostomy for ulcerative colitis. BMJ1978;2:85–88
Utsunomiya J, Iwama T, Imajo M et al. Total colectomy, mucosal proctectomy, and ileal-anal anastomosis. Dis Colon Rectum 1980;23:459–466
Taylor BM, Cranley B, Kelly KA et al. A clinico-physiological comparison of ileal pouch-anal and straight ileoanal anastomoses. Ann Surg 1983;198:462–468
Hallgren TA, Fasth SB, Oresland TO, Hulten LA. Ileal pouch anal function after endoanal mucosectomy and hand sewn ileoanal anastomosis compared with stapled anastomosis without mucosectomy. Eur J Surg. 1995 Dec; 161(12):915-21
Farouk R, Pemberton JH, Wolff BG et al. Functional outcomes after ileal pouch-anal anastomosis for chronic ulcerative colitis. Ann Surg 2000;231:919–926
www.downstatesurgery.org

Medical Management - Salicylates
Sulfasalazine Inhibition of cyclooxygenase & 5-lipoxygenase in gut
mucosa & => decrease inflammation Pentasa(mesalamine), asacol, rowasa, canasa remission 80% @3g/day Sulfapyradine attached to 5-ASA which is cleaved by
enteric bacteria inflammatory side effex Oral, topical, or combo Drug of choice for mild to moderate disease
www.downstatesurgery.org

Steroids Moderate to severe HTN, hyperglycemia, cataracts, osteoporosis,
osteomalacia Budesonide, beclomethasone undergo rapid
hepatic degradation to limit systemic toxicity
Medical Management
www.downstatesurgery.org

Medical Management Immunosuppressive Agents
Azathioprine, 6-MCP Interfere w/ nucleic acid synthesis Good for those who failed salicylate Tx or are dependent on
steroids (6-12 wk onset of axn) Cyclosporine
Interferes w/ T cell funxn Helps acute flares 80%
Methotrexate Folate antagonist
Infliximab (Remicade) Monoclonal Ab against TNF alpha >50% w/ moderate to severe Dz respond
www.downstatesurgery.org

Extraintestinal Manifestations
Liver most common: fatty liver 40-50% reverse by med or Sx, cirrhosis (2-5%) irreversible
Primary sclerosing cholangitis strixrs of intra & extrahepatic ducts (40-60% have UC) only effective therapy is liver transplant
Cholangiocarcinoma rare but pts r ~20yrs younger than typical pts w/ it
Arthritis improves w/ meds or Sx but sacroiliitis or ankylosing spondylitis does not
Erythema nodosum 5-15%, W:M 3-4:1, raised red & on lower legs & pyoderma grangenosum some may improve w/ Sx
www.downstatesurgery.org

Post-IPAA
Barium enema & flex sig Evaluate anal sphincter tone Loop ileostomy reversed
www.downstatesurgery.org