
Can Meropenem Heteroresistance in OXA-48-Producing K. pneumoniae be Inferred from an E-test?

Available online at www.sciencedirect.com
Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426www.elsevier.com/locate/diagmicrobio
Summary trends for the Meropenem Yearly Susceptibility TestInformation Collection Program: a 10-year experience in the
United States (1999–2008)Paul R. Rhomberga, Ronald N. Jonesa,b,⁎
aJMI Laboratories, North Liberty, IA 52317, USAbTufts University School of Medicine, Boston, MA 02111, USA
Received 27 July 2009; accepted 28 August 2009
Abstract
The Meropenem Yearly Susceptibility Test Information Collection (MYSTIC) Program was a global, longitudinal antimicrobialresistance surveillance network of more than 100 medical centers worldwide monitoring the susceptibility of meropenem and selected otherbroad-spectrum comparator agents. In 1999, and from 2000 through 2008, a total of 10 or 15 United States (USA) medical centers eachforwarded 200 nonduplicate clinical isolates from serious infections to a central processing laboratory. Over the 10-year period of thissurveillance program, the activity of meropenem and an average of 11 other antimicrobial agents were assessed against a total of 27 289bacterial isolates using Clinical and Laboratory Standards Institute reference methods. Meropenem consistently demonstrated low resistancerates against Enterobacteriaceae species isolates through 2008 and did not exhibit a widespread change in resistance rates over the monitoredinterval. In fact, the incidence of emerging carbapenemase-producing (KPC-type) Klebsiella spp. showed a decline in 2008 compared to thesteeply increasing rates observed from 2004 to 2007. Moreover, the KPC serine carbapenemases have spread to other Enterobacteriaceaespecies monitored by the MYSTIC Program. Greatest increases in antimicrobial resistance rates were observed for the fluoroquinolones(ciprofloxacin, levofloxacin) among all species monitored by the MYSTIC Program. Current susceptibility rates for meropenem when testedagainst prevalent pathogens were Pseudomonas aeruginosa (439 strains, 85.4% susceptible), Enterobacteriaceae (1537 strains, 97.3%susceptible), methicillin-susceptible staphylococci (460 strains, 100.0% susceptible), Streptococcus pneumoniae (125 strains, 80.2% atmeningitis susceptibility breakpoints), other streptococci (159 strains, 90.0–100.0% susceptible), and Acinetobacter spp. (127 strains, 45.7%susceptible), the widest spectrum among β-lactams tested in 2008 and throughout the last decade. Continued local surveillance of broad-spectrum agents following the completion of the MYSTIC Program (USA) appears critical to detect emerging resistances among pathogenscausing the most serious infections requiring carbapenem agents.© 2009 Elsevier Inc. All rights reserved.
Keywords: MYSTIC Program; Meropenem; Carbapenems; Resistance
1. Introduction
The Meropenem Yearly Susceptibility Test InformationCollection (MYSTIC) Program was a longitudinal antimi-crobial resistance surveillance study initiated in 1997; theprogram expanded to include other geographic regions and,for its final year (2008), had greater than 100 participantmedical centers worldwide, located in Europe, North
⁎ Corresponding author. JMI Laboratories, North Liberty, IA 52317,USA. Tel.: +1-319-665-3370; fax: +1-319-665-3371.
E-mail address: [email protected] (R.N. Jones).
0732-8893/$ – see front matter © 2009 Elsevier Inc. All rights reserved.doi:10.1016/j.diagmicrobio.2009.08.020
America, South America, and Asia, to monitor for changesin the in vitro activity of meropenem and other broad-spectrum antimicrobial agents (Jones et al., 2005; Turner,2000, 2004, 2005, 2009; Turner et al., 1999). The UnitedStates (USA) portion of the MYSTIC Program (Jones et al.,2005; Pfaller and Jones, 2000; Pfaller et al., 2001; Rhombergand Jones, 2007; Rhomberg et al., 2004a, 2004b, 2005,2006a, 2006b, 2007) began in 1999 with 10 selected medicalcenters where meropenem was the primary treatmentcarbapenem on the formulary (Edwards, 1995; PackageInsert, 2007; Pfaller and Jones, 1997; Roberts et al., 2009;Wisemann et al., 1995). The program was expanded to 15

415P.R. Rhomberg, R.N. Jones / Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426
sites participating annually from 2000 through 2008 using acentral processing laboratory design (JMI Laboratories,North Liberty, IA), also employed in Brazil (Pfaller andJones, 2000) and special samplings in India (Jones et al.,2002; Mathai et al., 2002). Reference quality brothmicrodilution susceptibility testing was performed accordingto Clinical and Laboratory Standards Institute (CLSI, 2009b)(formerly National Committee for Clinical LaboratoryStandards) methods to detect antimicrobial resistance ratesand resistance trends for the carbapenems (meropenem andimipenem) and other comparator broad-spectrum agents.
Antimicrobial agents in the β-lactam class, especiallymeropenem (Wisemann et al., 1995), were initially veryeffective therapeutic agents in the treatment of seriousinfections caused by Gram-negative pathogens. The devel-opment and spread of β-lactamase resistance mechanismswithin Gram-negative bacilli have significantly reduced thevalue of early β-lactam agents and required newer morepotent and enzyme inhibitor protected extended-spectrumagents to be developed (Jones, 1996; Landman et al., 2002;Spellberg et al., 2008). To address the detection of emergingresistances, we have developed surveillance programs at alllevels (local, regional, and global), stimulated by discussionsin the United States and elsewhere (EARSS, 2007; Jones,1996). These programs vary widely in design, scope, appliedmethods, and monitored compound, thus, requiring carefulexamination of method/design to assure the value of results(Jones, 2000; Jones and Masterton, 2001; Masterton, 2000).Notable surveillance networks include EARSS (2007),Alexander Project (Felmingham et al., 2005), IntensiveCare Antimicrobial Resistance Epidemiology (Fridkin et al.,1999), PROTEKT (Harding and Felmingham, 2004), SEN-TRY Antimicrobial Surveillance Program (Jones, 2003), andthe MYSTIC Program (Turner et al., 1999). These programs,some with excellent molecular support for determiningmechanisms of β-lactam resistance, have discovered emerg-ing high rates of enzyme-mediated resistances.
The genes encoding most β-lactamases are on plasmids ortransposons, which can be easily transferred to other strainsand often carry additional genetic elements encodingresistances to other antimicrobial classes (Castanheiraet al., 2008). The most prevalent extended-spectrum β-lactamases (ESBLs) worldwide are the CTX-M type, foundin the community and hospital settings (Castanheira et al.,2008). Another β-lactam resistance mechanism that is on therise is plasmid-mediated AmpC enzymes. ChromosomalAmpC enzymes have become mobilized on plasmids andtransferred to commonly isolated Enterobacteriaceae, such asEscherichia coli and Klebsiella spp. (Castanheira et al.,2008). Fortunately, meropenem and other carbapenemsretain excellent antimicrobial activity against these ESBL-and AmpC-producing Enterobacteriaceae.
Historically, resistance to the carbapenems among Gram-negative bacilli has been secondary to hyperproduction ofAmpC β-lactamase associated with a loss of outer membraneproteins and/or overexpression of efflux pumps (Bradford
et al., 1997; Cao et al., 2000) or the presence of an intrinsicmetallo-β-lactamase (MβL) in some rarer nonfermentativeGram-negative species (Chryseobacterium spp., Stenotro-phomonas spp.). Recently, Enterobacteriaceae, Acinetobac-ter spp., and Pseudomonas spp. isolates have acquiredcarbapenemases (MβLs, oxacillinases, and serine carbape-nemases). Initially, IMP- and VIM-producing MβL isolateswere observed in Japan, Greece, and Italy, but MβLs remainrare in USA isolates. However, the USA MYSTIC andSENTRY Programs have documented MβL-producingPseudomonas aeruginosa strains (Aboufaycal et al., 2007;Deshpande et al., 2006; Toleman et al., 2004). Also, veryinfrequent in USA Enterobacteriaceae are the presence of theserine carbapenemase SME types with a handful of isolatesobserved (Deshpande et al., 2006; Gales et al., 2001;Queenan et al., 2000) during the entire monitored period(1999–2008). Of greater concern in the United States is thedetection and rapid spread of the KPC-type serine carbape-nemases. KPC-type enzymes were first detected inKlebsiellapneumoniae from North Carolina (Yigit et al., 2001), withKPC-2 and KPC-3 soon appearing in Maryland, Massachu-setts, New York, and Europe (Hossain et al., 2004; Miriagouet al., 2003;Woodford et al., 2004, 2007). The swift spread ofthe KPC-type carbapenemase among K. pneumoniae isolatesin New York medical centers prompted the Department ofHealth to issue an advisory for the detection and control ofthis pathogen. The KPC-type carbapenemases have nowspread to medical centers within and outside the New Yorkgeographic area and also have been reported among otherEnterobacteriaceae species (Bradford et al., 2004; Bratu et al.,2005; Castanheira et al., 2008; Deshpande et al., 2006).
This report summarizes the in vitro activity of meropenemand that of other broad-spectrum comparator agents testedagainst Enterobacteriaceae, Gram-negative nonfermentativebacilli, and Gram-positive cocci submitted from theMYSTIC Program (USA) medical centers in 2008 and the9 prior years. We observed the continued potent activity ofthe carbapenem class against Enterobacteriaceae except forthe known KPC-producing Enterobacteriaceae as part of anexpanding epidemic (Deshpande et al., 2006; Rhomberg andJones, 2007; Rhomberg et al., 2007). Increasing resistancerates for all agents against Acinetobacter spp. isolates hasbeen pronounced, and annual resistance rates have beendocumented for carbapenems, β-lactams, aminoglycosides,and fluoroquinolones against major pathogen groups, toestablish trends/changes and relationships to drug use(Mutnick et al., 2004) for organisms submitted for theMYSTIC Program (1999 and 2008). This is the summaryreport of the entire MYSTIC Program (USA) and relatedpharmacokinetic investigations (Kuti et al., 2004).
2. Materials and methods
The MYSTIC Program in the United States was initiatedin 1999 with 10 medical centers geographically dispersed
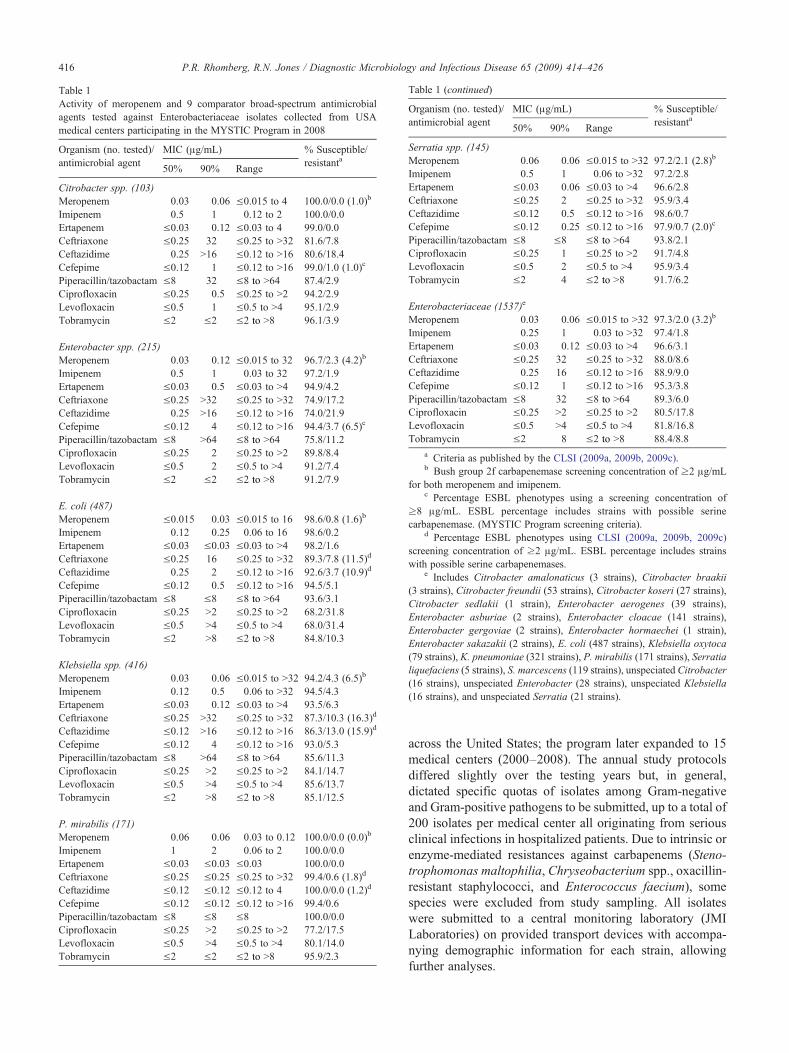
Table 1Activity of meropenem and 9 comparator broad-spectrum antimicrobialagents tested against Enterobacteriaceae isolates collected from USAmedical centers participating in the MYSTIC Program in 2008
Organism (no. tested)/antimicrobial agent
MIC (μg/mL) % Susceptible/resistanta
50% 90% Range
Citrobacter spp. (103)Meropenem 0.03 0.06 ≤0.015 to 4 100.0/0.0 (1.0)b
Imipenem 0.5 1 0.12 to 2 100.0/0.0Ertapenem ≤0.03 0.12 ≤0.03 to 4 99.0/0.0Ceftriaxone ≤0.25 32 ≤0.25 to N32 81.6/7.8Ceftazidime 0.25 N16 ≤0.12 to N16 80.6/18.4Cefepime ≤0.12 1 ≤0.12 to N16 99.0/1.0 (1.0)c
Piperacillin/tazobactam ≤8 32 ≤8.to N64 87.4/2.9Ciprofloxacin ≤0.25 0.5 ≤0.25 to N2 94.2/2.9Levofloxacin ≤0.5 1 ≤0.5 to N4 95.1/2.9Tobramycin ≤2 ≤2 ≤2.to N8 96.1/3.9
Enterobacter spp. (215)Meropenem 0.03 0.12 ≤0.015 to 32 96.7/2.3 (4.2)b
Imipenem 0.5 1 0.03 to 32 97.2/1.9Ertapenem ≤0.03 0.5 ≤0.03 to N4 94.9/4.2Ceftriaxone ≤0.25 N32 ≤0.25 to N32 74.9/17.2Ceftazidime 0.25 N16 ≤0.12 to N16 74.0/21.9Cefepime ≤0.12 4 ≤0.12 to N16 94.4/3.7 (6.5)c
Piperacillin/tazobactam ≤8 N64 ≤8.to N64 75.8/11.2Ciprofloxacin ≤0.25 2 ≤0.25 to N2 89.8/8.4Levofloxacin ≤0.5 2 ≤0.5 to N4 91.2/7.4Tobramycin ≤2 ≤2 ≤2.to N8 91.2/7.9
E. coli (487)Meropenem ≤0.015 0.03 ≤0.015 to 16 98.6/0.8 (1.6)b
Imipenem 0.12 0.25 0.06 to 16 98.6/0.2Ertapenem ≤0.03 ≤0.03 ≤0.03 to N4 98.2/1.6Ceftriaxone ≤0.25 16 ≤0.25 to N32 89.3/7.8 (11.5)d
Ceftazidime 0.25 2 ≤0.12 to N16 92.6/3.7 (10.9)d
Cefepime ≤0.12 0.5 ≤0.12 to N16 94.5/5.1Piperacillin/tazobactam ≤8 ≤8 ≤8.to N64 93.6/3.1Ciprofloxacin ≤0.25 N2 ≤0.25 to N2 68.2/31.8Levofloxacin ≤0.5 N4 ≤0.5 to N4 68.0/31.4Tobramycin ≤2 N8 ≤2.to N8 84.8/10.3
Klebsiella spp. (416)Meropenem 0.03 0.06 ≤0.015 to N32 94.2/4.3 (6.5)b
Imipenem 0.12 0.5 0.06 to N32 94.5/4.3Ertapenem ≤0.03 0.12 ≤0.03 to N4 93.5/6.3Ceftriaxone ≤0.25 N32 ≤0.25 to N32 87.3/10.3 (16.3)d
Ceftazidime ≤0.12 N16 ≤0.12 to N16 86.3/13.0 (15.9)d
Cefepime ≤0.12 4 ≤0.12 to N16 93.0/5.3Piperacillin/tazobactam ≤8 N64 ≤8.to N64 85.6/11.3Ciprofloxacin ≤0.25 N2 ≤0.25 to N2 84.1/14.7Levofloxacin ≤0.5 N4 ≤0.5 to N4 85.6/13.7Tobramycin ≤2 N8 ≤2.to N8 85.1/12.5
P. mirabilis (171)Meropenem 0.06 0.06 0.03 to 0.12 100.0/0.0 (0.0)b
Imipenem 1 2 0.06 to 2 100.0/0.0Ertapenem ≤0.03 ≤0.03 ≤0.03 100.0/0.0Ceftriaxone ≤0.25 ≤0.25 ≤0.25 to N32 99.4/0.6 (1.8)d
Ceftazidime ≤0.12 ≤0.12 ≤0.12 to 4 100.0/0.0 (1.2)d
Cefepime ≤0.12 ≤0.12 ≤0.12 to N16 99.4/0.6Piperacillin/tazobactam ≤8 ≤8 ≤8 100.0/0.0Ciprofloxacin ≤0.25 N2 ≤0.25 to N2 77.2/17.5Levofloxacin ≤0.5 N4 ≤0.5 to N4 80.1/14.0Tobramycin ≤2 ≤2 ≤2.to N8 95.9/2.3
able 1 (continued)
rganism (no. tested)/ntimicrobial agent
MIC (μg/mL) % Susceptible/resistanta
50% 90% Range
erratia spp. (145)eropenem 0.06 0.06 ≤0.015 to N32 97.2/2.1 (2.8)b
ipenem 0.5 1 0.06 to N32 97.2/2.8rtapenem ≤0.03 0.06 ≤0.03 to N4 96.6/2.8eftriaxone ≤0.25 2 ≤0.25 to N32 95.9/3.4eftazidime ≤0.12 0.5 ≤0.12 to N16 98.6/0.7efepime ≤0.12 0.25 ≤0.12 to N16 97.9/0.7 (2.0)c
iperacillin/tazobactam ≤8 ≤8 ≤8.to N64 93.8/2.1iprofloxacin ≤0.25 1 ≤0.25 to N2 91.7/4.8evofloxacin ≤0.5 2 ≤0.5 to N4 95.9/3.4obramycin ≤2 4 ≤2.to N8 91.7/6.2
nterobacteriaceae (1537)e
eropenem 0.03 0.06 ≤0.015 to N32 97.3/2.0 (3.2)b
ipenem 0.25 1 0.03 to N32 97.4/1.8rtapenem ≤0.03 0.12 ≤0.03 to N4 96.6/3.1eftriaxone ≤0.25 32 ≤0.25 to N32 88.0/8.6eftazidime 0.25 16 ≤0.12 to N16 88.9/9.0efepime ≤0.12 1 ≤0.12 to N16 95.3/3.8iperacillin/tazobactam ≤8 32 ≤8.to N64 89.3/6.0iprofloxacin ≤0.25 N2 ≤0.25 to N2 80.5/17.8evofloxacin ≤0.5 N4 ≤0.5 to N4 81.8/16.8obramycin ≤2 8 ≤2.to N8 88.4/8.8
a Criteria as published by the CLSI (2009a, 2009b, 2009c).b Bush group 2f carbapenemase screening concentration of ≥2 μg/mL
r both meropenem and imipenem.c Percentage ESBL phenotypes using a screening concentration of
8 μg/mL. ESBL percentage includes strains with possible serinearbapenemase. (MYSTIC Program screening criteria).
d Percentage ESBL phenotypes using CLSI (2009a, 2009b, 2009c)creening concentration of ≥2 μg/mL. ESBL percentage includes strainsith possible serine carbapenemases.
e Includes Citrobacter amalonaticus (3 strains), Citrobacter braakiistrains), Citrobacter freundii (53 strains), Citrobacter koseri (27 strains),itrobacter sedlakii (1 strain), Enterobacter aerogenes (39 strains),nterobacter asburiae (2 strains), Enterobacter cloacae (141 strains),nterobacter gergoviae (2 strains), Enterobacter hormaechei (1 strain),nterobacter sakazakii (2 strains), E. coli (487 strains), Klebsiella oxytoca9 strains), K. pneumoniae (321 strains), P. mirabilis (171 strains), Serratiaquefaciens (5 strains), S. marcescens (119 strains), unspeciated Citrobacter6 strains), unspeciated Enterobacter (28 strains), unspeciated Klebsiella6 strains), and unspeciated Serratia (21 strains).
416 P.R. Rhomberg, R.N. Jones / Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426
T
Oa
SMImECCCPCLT
EMImECCCPCLT
fo
≥c
sw
(3CEEE(7li(1(1
across the United States; the program later expanded to 15medical centers (2000–2008). The annual study protocolsdiffered slightly over the testing years but, in general,dictated specific quotas of isolates among Gram-negativeand Gram-positive pathogens to be submitted, up to a total of200 isolates per medical center all originating from seriousclinical infections in hospitalized patients. Due to intrinsic orenzyme-mediated resistances against carbapenems (Steno-trophomonas maltophilia, Chryseobacterium spp., oxacillin-resistant staphylococci, and Enterococcus faecium), somespecies were excluded from study sampling. All isolateswere submitted to a central monitoring laboratory (JMILaboratories) on provided transport devices with accompa-nying demographic information for each strain, allowingfurther analyses.

able 2ctivity of meropenem and 9 comparator broad-spectrum antimicrobialgents tested against nonfermentative Gram-negative bacilli isolatesollected from USA medical centers participating in the MYSTICrogram in 2008
rganism (no. tested)/ntimicrobial agent
MIC (μg/mL) %Susceptible/resistanta
50% 90% Range
. aeruginosa (439)eropenem 0.5 8 0.03 to N32 85.4/7.5ipenem 1 16 0.06 to 32 79.5/15.5rtapenem N4 N4 ≤0.03 to 4eftriaxone N32 N32 0.5 to N32 8.9/70.8eftazidime 4 16 ≤0.12 to N16 85.6/9.8efepime 4 16 ≤0.12 to N16 86.6/6.4iperacillin/tazobactam ≤8 64 ≤8.to N64 90.2/9.8iprofloxacin ≤0.25 N2 ≤0.25 to N2 77.0/17.3evofloxacin ≤0.5 N4 ≤0.5 to N4 72.7/19.1obramycin ≤2 8 ≤2.to N8 89.1/9.1
cinetobacter spp. (127)b
eropenem 8 N32 0.06 to N32 45.7/47.2ipenem 4 N32 0.06 to N32 52.0/38.6rtapenem N4 N4 0.5 to N4eftriaxone N32 N32 4.to N32 11.8/62.2eftazidime N16 N16 1.to N16 31.5/60.6efepime N16 N16 0.5 to N16 31.5/55.1iperacillin/tazobactam N64 N64 ≤8.to N64 34.6/60.6iprofloxacin N2 N2 ≤0.25 to N2 32.3/66.9evofloxacin N4 N4 ≤0.5 to N4 33.9/59.1obramycin ≤2 N8 ≤2.to N8 59.1/33.9
a Criteria as published by the CLSI (2009a, 2009b, 2009c).b Includes Acinetobacter baumannii (94 strains), Acinetobacter
alcoaceticus (1 strain), Acinetobacter lwoffii (12 strains), and unspeciatedcinetobacter (20 strains).
417P.R. Rhomberg, R.N. Jones / Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426
In 2008, a total of 2851 isolates (95.0% protocolcompliance) were processed, and over the 10-year periodof the USA MYSTIC Program, 27 289 isolates (94.1%compliance) were collected and tested. Bacterial strainidentifications were performed at the local laboratory, andidentifications were confirmed, as necessary, at the centralmonitoring laboratory using colony morphology, biochem-ical tests (Remel, Lenexa, KS), and/or the Vitek 2 Systemidentification cards (bioMerieux, Hazelwood, MO). Allisolates were stored at −70 °C.
Broth microdilution susceptibility testing was utilized onall bacterial strains by applying CLSI (2009b) referencemethods published in M07-A8 to determine MICs. Theantimicrobial agents tested in 2008 were meropenem,imipenem, ertapenem, cefepime, ceftazidime, ceftriaxone,piperacillin/tazobactam, tobramycin, ciprofloxacin, levo-floxacin, and penicillin. Additionally, oxacillin and cefoxitindisk susceptibility testing was performed on staphylococcalisolates using the CLSI (2009a) M02-A10 method to confirmmethicillin (oxacillin)-resistant strains. CLSI (2009c) inter-pretive breakpoint criteria published in M100-S19 wereapplied for determination of susceptibility rates. Concurrenttesting with American Type Culture Collection (ATCC)strains E. coli ATCC 25922, P. aeruginosa ATCC 27853,Enterococcus faecalis ATCC 29212, Staphylococcus aureusATCC 29213, and ATCC 25923 and Streptococcuspneumoniae ATCC 49619 assured the quality control (QC)of the susceptibility test methods (CLSI, 2009b, 2009c) . AllQC results were within published ranges (CLSI, 2009c).
The CLSI ESBL screening criteria (MIC, ≥2 μg/mL) forceftazidime or ceftriaxone were applied to the E. coli,Klebsiella spp., and Proteus mirabilis with isolates furthertested by a disk approximation or the Etest ESBL method(AB BIODISK, Solna, Sweden) to demonstrate an enhancedceftazidime or cefotaxime activity in the presence ofclavulanate. The CLSI (2009c) screening criteria of ≥2 μg/mL for both meropenem and imipenem was also utilized todetect possible KPC-type serine carbapenemase enzymes inEnterobacteriaceae isolates followed by multiplex polymer-ase chain reaction (PCR) confirmatory methods. Finally, allGram-negative bacilli matching the Senda et al. (1996a,1996b) criteria of resistance to meropenem (≥16 μg/mL),imipenem (≥16 μg/mL), and ceftazidime (≥32 μg/mL) weretested by PCR methods to determine the presence of a MβL.
Multidrug-resistant (MDR) isolates within a bacterialspecies or genus group were analyzed by antimicrobialresistance antibiogram patterns to screen for the presence oflocal epidemic clonality. Selected strains were then typed forgenotypic relatedness using automated ribotyping (Ribo-Printer™ Microbial Characterization System; Qualicon,Wilmington, DE) of genomic DNA after digestion usingappropriate restriction enzymes. The DNA fragments wereseparated by agarose gel electrophoresis resulting in bandingpatterns, which were then captured by image analysissoftware and compared to all previously tested isolates inthe riboprint library network (the United States, Brazil,
United Kingdom, and Australia) to assign a ribogroup. Whennecessary, further discrimination of a ribogroup wasperformed using CHEF-DRII pulsed-field gel electrophore-sis (BioRad Laboratories, Hercules, CA) on restrictiondigested DNA. Gels were stained with ethidium bromideto visually identify the banding patterns and determine clonalrelatedness (Tenover et al., 1995).
3. Results
3.1. Activity of meropenem in the 2008 MYSTIC Program
The susceptibility testing results for the sampled year2008 isolates, including the MIC50, MIC90, and percentagesusceptible and resistant, are summarized in Table 1 for 6Enterobacteriaceae species or genus groups, as well as for allEnterobacteriaceae isolates combined. The carbapenems(meropenem, imipenem, and ertapenem) all demonstrated ahigh level of antimicrobial activity against the Enterobacter-iaceae (1537 strains), with ≥96.6% susceptible rates. Whencomparing MIC50 and MIC90 results for all Enterobacter-iaceae isolates combined, meropenem was 8- to 16-fold morepotent than imipenem equal to or 2-fold more potent thanertapenem. Modest levels of carbapenem resistance was
TAacP
Oa
PMImECCCPCLT
AMImECCCPCLT
cA

Table 3Activity of meropenem and 9 comparator broad-spectrum antimicrobialagents tested against Gram-positive cocci isolates collected from USAmedical centers participating in the MYSTIC Surveillance Program in 2008
Organism (no. tested)/antimicrobial agent
MIC (μg/mL) % Susceptible/resistanta
50% 90% Range
S. aureus (317)Meropenem 0.12 0.12 0.03 to 0.25 100.0/0.0Imipenem 0.03 0.03 ≤0.015 to 0.06 100.0/0.0Ertapenem 0.12 0.25 0.06 to 0.5 100.0/0.0Ceftriaxone 4 4 0.5 to 16 99.7/0.0Ceftazidime 8 8 2.to 16 95.3/0.0Cefepime 2 4 0.5 to 8 100.0/0.0Piperacillin/tazobactam ≤8 ≤8 ≤8.to 16 99.7/0.3Ciprofloxacin 0.5 N2 ≤0.25 to N2 87.7/11.0Levofloxacin ≤0.5 4 ≤0.5 to N4 89.6/10.1Tobramycin ≤2 ≤2 ≤2.to N8 96.8/2.5
Coagulase-negative staphylococci (143)b
Meropenem 0.12 0.25 0.03 to 0.5 100.0/0.0Imipenem 0.03 0.03 ≤0.015 to 0.12 100.0/0.0Ertapenem 0.12 0.5 0.06 to 1 100.0/0.0Ceftriaxone 2 4 ≤0.25 to 16 99.3/0.0Ceftazidime 4 8 1.to 16 93.7/0.0Cefepime 0.5 2 ≤0.12 to 4 100.0/0.0Piperacillin/tazobactam ≤8 ≤8 ≤8 100.0/0.0Ciprofloxacin ≤0.25 N2 ≤0.25 to N2 77.6/21.7Levofloxacin ≤0.5 N4 ≤0.5 to N4 78.3/21.0Tobramycin ≤2 ≤2 ≤2.to N8 93.7/2.1
S. pneumoniae (125)Meropenem ≤0.015 1 ≤0.015 to 2 80.0/14.4Imipenem ≤0.015 1 ≤0.015 to 1 81.6/11.2Ertapenem ≤0.03 1 ≤0.03 to 2 94.4/0.0Ceftriaxone ≤0.25 1 ≤0.25 to 4 90.4/0.8Ceftazidime 0.25 16 ≤0.12 to N16Cefepime ≤0.12 1 ≤0.12 to 2 92.8/0.0Penicillin ≤0.06 4 ≤0.06 to 8 85.6/4.8
(60.0/20.0)c
Piperacillin/tazobactam ≤8 ≤8 ≤8.to 16Ciprofloxacin 1 2 0.5 to N2Levofloxacin 1 1 ≤0.5 to N4 99.2/0.8Tobramycin N8 N8 ≤2.to N8
β-Hemolytic streptococci (119)d
Meropenem ≤0.015 0.06 ≤0.015 to 0.12 100.0/–Imipenem ≤0.015 0.03 ≤0.015 to 0.06Ertapenem ≤0.03 0.06 ≤0.03 to 0.5 100.0/–Ceftriaxone ≤0.25 ≤0.25 ≤0.25 100.0/–Ceftazidime 0.25 1 ≤0.12 to 4Cefepime ≤0.12 ≤0.12 ≤0.12 to 0.5 100.0/–Penicillin ≤0.06 ≤0.06 ≤0.06 to 0.12 100.0/–Piperacillin/tazobactam ≤8 ≤8 ≤8Ciprofloxacin 0.5 1 0.5 to 2Levofloxacin ≤0.5 1 ≤0.5 to 2 100.0/0.0Tobramycin N8 N8 4.to N8
Viridans group streptococci (40)e
Meropenem 0.06 0.5 ≤0.015 to 4 90.0/–Imipenem 0.03 0.25 ≤0.015 to 4Ertapenem 0.12 1 ≤0.03 to 4Ceftriaxone ≤0.25 2 ≤0.25 to 8 87.5/7.5Ceftazidime 2 8 ≤0.12 to N16Cefepime 0.25 1 ≤0.12 to 8 90.0/5.0Penicillin ≤0.06 2 ≤0.06 to N8 67.5/7.5
able 3 (continued)
rganism (no. tested)/ntimicrobial agent
MIC (μg/mL) % Susceptible/resistanta
50% 90% Range
iperacillin/tazobactam ≤8 ≤8 ≤8.to N64iprofloxacin 1 N2 ≤0.25 to N2evofloxacin 1 N4 ≤0.5 to N4 85.0/15.0obramycin 8 N8 ≤2.to N8
a Criteria as published by the CLSI (2009a, 2009b, 2009c), β-lactamusceptibility should be directed by the oxacillin test results.
b Includes Staphylococcus capitis (6 strains), Staphylococcuspidermidis (26 strains), Staphylococcus haemolyticus (1 strain),taphylococcus hominis (3 strains), Staphylococcus lugdunensisstrains), Staphylococcus simulans (1 strain), Staphylococcus warneristrain), and unspeciated coagulase-negative staphylococci (99 strains).c Both parenteral and oral (in parenthesis) breakpoints provided.d Includes group A Streptococcus (45 strains), group B Streptococcus
4 strains), group C Streptococcus (2 strains), group F Streptococcusstrains), and group G Streptococcus (16 strains).e Includes Streptococcus anginosus (4 strains), Streptococcus
onstellatus (1 strain), Streptococcus milleri (2 strains), Streptococcusitis (4 strains), Streptococcus oralis (4 strains), Streptococcus sanguinisstrain), unspeciated α-hemolytic streptococci (1 strain), and unspeciated
iridians group streptococci (23 strains).
418 P.R. Rhomberg, R.N. Jones / Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426
T
Oa
PCLT
s
eS(6(1
(5(2
cm(1v
observed among E. coli (1.6%, 8 strains), Serratia spp.(2.8%, 4 strains), and Enterobacter spp. (4.2%, 9 strains) andwas most prevalent among Klebsiella spp. (6.3%; 26 strains).Only cefepime, among the comparator agents, had a similaroverall susceptibility rate (95.3%) against Enterobacteria-ceae with all other broad-spectrum agents having suscepti-bility rates ranging from 80.5% to 89.3% (Table 1). Lowestsusceptibility rates were observed for the fluoroquinolones(80.5–81.8%), especially prevalent among E. coli and P.mirabilis (14.0–31.8% resistant) isolates.
The MYSTIC Program (2008) results for the nonfermen-tative Gram-negative bacilli, P. aeruginosa and Acinetobac-ter spp., are found in Table 2. Against P. aeruginosa,piperacillin/tazobactam (90.2% at ≤64 μg/mL [CLSI]) andtobramycin (89.1%) had the highest coverage rates (%susceptible) followed by cefepime (86.6%), ceftazidime(85.6%), and meropenem (85.4%). The fluoroquinolonesagain had the lowest susceptibility rates (72.7–77.0%)among the agents recommended for antipseudomonaltherapy. Among carbapenem agents, meropenem was 2-fold more potent than imipenem (MIC90, 8 versus 16 μg/mL). Against Acinetobacter spp. isolates, tobramycin hadthe highest susceptibility rate (only 59.1%), and thecarbapenems were next at 52.0% (imipenem) and 45.7%(meropenem). All other so-called “broad-spectrum agents”had susceptible rates at less than 34.6%, confirming thispathogen group as the most difficult to treat using currentlymarketed agents.
Table 3 lists the susceptibility testing results for the Gram-positive cocci collected as part of the 2008 MYSTICProgram. The oxacillin-susceptible staphylococci werecompletely susceptible (100.0%) to the carbapenems andcefepime, in contrast to methicillin-resistant S. aureusisolates that are considered resistant to all currently available

419P.R. Rhomberg, R.N. Jones / Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426
β-lactams (CLSI, 2008, 2009b). Reduced susceptibility rateswere observed only for the fluoroquinolones, 77.6% to78.3% against coagulase-negative staphylococci and 87.7%to 89.6% against S. aureus. The β-hemolytic streptococciwere very susceptible to all agents tested, except tobramycin(MIC50, N8 μg/mL,) and susceptibility rates were 100.0% forall agents using published CLSI (2009c) breakpoints. Theviridans group streptococci and S. pneumoniae isolates wereless susceptible to the carbapenems than the β-hemolyticstreptococci, with meropenem susceptibility rates of 90.0%and 80.0%, respectively. The meropenem MIC90 values forviridans group streptococci (0.5 μg/mL) and S. pneumoniae(1 μg/mL) were greater than for the β-hemolytic streptococci(0.06 μg/mL).
3.2. Susceptibility rate trends in MYSTIC Program(1999–2008)
Table 4 shows the longitudinal resistance trends in theUSA MYSTIC Program for up to 10 monitored broad-spectrum antimicrobial agents over the 10-year studyinterval. Not all species groups were monitored in allyears; among Gram-negative bacilli, only E. coli andKlebsiella sp. isolates were collected in 2006, and noGram-positive cocci were collected in 2004.
Against the Citrobacter spp. isolates tested over the lastdecade, most agents showed stable resistance rates with onlysmall variations ±5% changes annually. Ceftazidime showeda dramatic increase in 2000 compared to the baseline year(1999) and a slight increasing trend over the 10-year period,mainly due to the spread of stably depressed AmpC enzyme-producing strains in this species group. Carbapenemresistance was rarely observed among Enterobacter spp.during the first 7 years; however, an increasing trend towardresistance was noted in the final 2 years studied due to thespread of KPC carbapenemase from the Klebsiella spp. intoEnterobacter spp. strains and secondary spread of thisresistance mechanism beyond the New York City geograph-ic area, where it has become endemic in MYSTIC Programmonitored hospitals.
The most interesting pathogen group with multipleantimicrobial agents showing increased resistance rates isthe E. coli (Table 4 and Fig. 1). Ciprofloxacin resistance wasonly 4.1% in the baseline year and has steadily increased to31.8% after 10 years (Table 4). The aminoglycosides alsoexhibited a slower, but still consistent, increase in resistancefrom 1999 (tobramycin, resistance at 1.5%) to 2007 (10.3%).Cefepime resistance in the E. coli strains first emerged in2004 (0.4%) and rapidly climbed to 5.1% in only 5 years(CTX-M ESBL- and KPC-producing isolates). Carbapenemresistance among E. coli isolates was first observed in the2008 sample, again, most likely due to the spread of KPCgenes from Klebsiella spp. Among the Klebsiella spp.isolates, carbapenem resistance was rarely observed prior to2003, but after the emergence, the resistance rates quicklyincreased to nearly 8% in 2007 before falling back to 4.3% in
2008 associated with local infection control interventions.Concurrent with the spread of KPC enzymes in theseKlebsiella spp. isolates was the rise in resistance among theother β-lactam and β-lactam/β-lactamase inhibitor combi-nation agents tested (Table 4 and Fig. 2). A rapid rise influoroquinolone and aminoglycoside resistance was noted in2005 compared to the stable rates observed in 1999 through2004. This was due to coresistances carried on KPC-harboring plasmids.
Most broad-spectrum agents showed stable resistancerates against the indole-positive Proteus spp. and P.mirabilis isolates except for the fluoroquinolones testedagainst P. mirabilis, which showed a dramatic 10-foldincrease from 2.1% (ciprofloxacin) in 1999 to nearly 20% in2007 to 2008 (target mutations and plasmidic qnr genes).Serratia spp. isolates also exhibited highly stable resistancerates over the 10-year study period except for some clonallyrelated SME carbapenemase-producing isolates in 1999 andKPC-producing Serratia marcescens in 2008.
Against the Acinetobacter spp. isolates, resistance ratesranged from 10.0% (imipenem) to 50.0% (gentamicin) in the1999 baseline year. Most agents showed increasing resistancerates over the 10-year study period with the highest rates in2008 for ciprofloxacin (73.4%), piperacillin/tazobactam(69.1%), and ceftriaxone and ceftazidime (68.1%). Lowestresistance rates observed were for tobramycin (40.4%),imipenem (47.9%), and meropenem (57.4%). Resistancerates varied up to ±7% annually among these agents testedagainst P. aeruginosa isolates tested between 1999 and 2008;however, the overall resistance rates generally remained stableor decreasing slightly for some agents (Table 4 and Fig. 3).
Among the methicillin-susceptible S. aureus and coagu-lase-negative Staphylococcus, resistance rates remained verystable for most agents tested, except for the fluoroquinoloneswhere the 1999 baseline rates of 4.2% and 9.2% increased to11.0% and 21.7% for ciprofloxacin against S. aureus andcoagulase-negative staphylococci, respectively (data notshown). Levofloxacin showed a rapidly increasing resistancerate from 0.0% in 2003 to 15.0% in 2008 for viridians groupstreptococci due to clonal spread of QRDR mutant strains inseveral institutions.
4. Discussion
Serious bacterial infections require prompt, appropriatetreatment to minimize the risk of morbidity andmortality, andcarbapenems have been strongly recommended as an initialempiric treatment followed by more directed therapy afterfollow-up susceptibility results are known from culture of thecausative pathogen. Meropenem is a very broad-spectrumcarbapenem approved by the USA Food and Drug Admin-istration for the treatment of complicated skin and skinstructure infections in adults and children, complicated intra-abdominal infections in adults and children, and pediatricbacterial meningitis infections in children ≥3 years old.
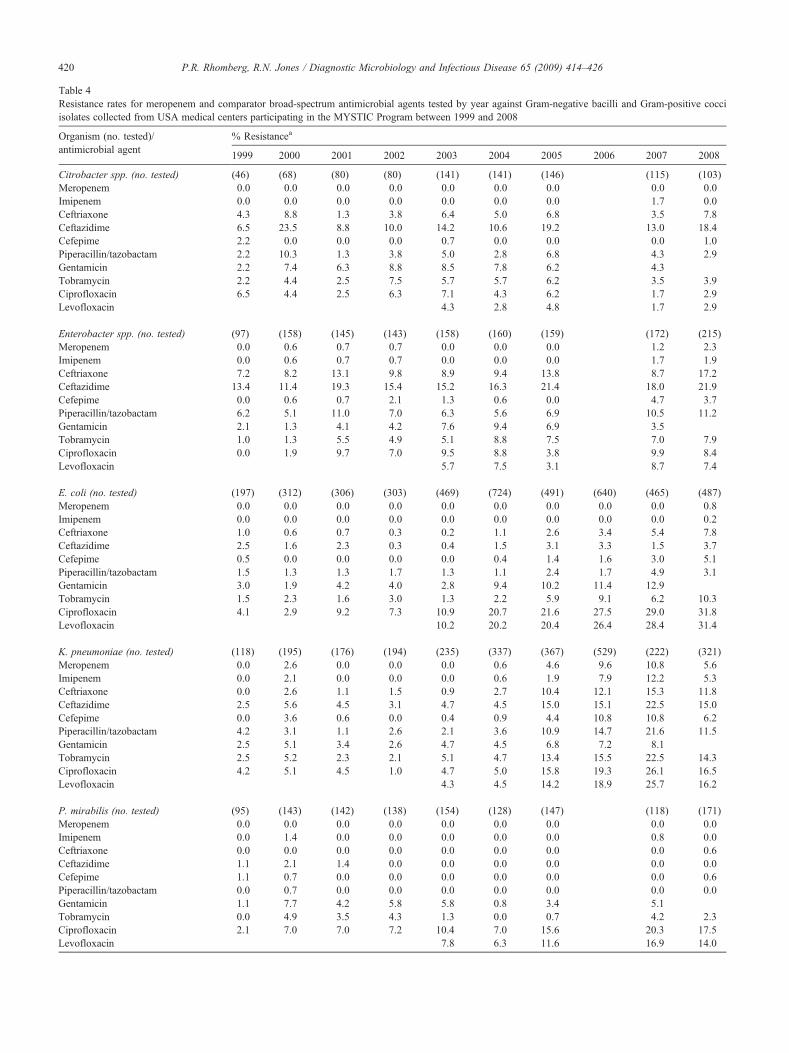
Table 4Resistance rates for meropenem and comparator broad-spectrum antimicrobial agents tested by year against Gram-negative bacilli and Gram-positive cocciisolates collected from USA medical centers participating in the MYSTIC Program between 1999 and 2008
Organism (no. tested)/antimicrobial agent
% Resistancea
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Citrobacter spp. (no. tested) (46) (68) (80) (80) (141) (141) (146) (115) (103)Meropenem 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0Imipenem 0.0 0.0 0.0 0.0 0.0 0.0 0.0 1.7 0.0Ceftriaxone 4.3 8.8 1.3 3.8 6.4 5.0 6.8 3.5 7.8Ceftazidime 6.5 23.5 8.8 10.0 14.2 10.6 19.2 13.0 18.4Cefepime 2.2 0.0 0.0 0.0 0.7 0.0 0.0 0.0 1.0Piperacillin/tazobactam 2.2 10.3 1.3 3.8 5.0 2.8 6.8 4.3 2.9Gentamicin 2.2 7.4 6.3 8.8 8.5 7.8 6.2 4.3Tobramycin 2.2 4.4 2.5 7.5 5.7 5.7 6.2 3.5 3.9Ciprofloxacin 6.5 4.4 2.5 6.3 7.1 4.3 6.2 1.7 2.9Levofloxacin 4.3 2.8 4.8 1.7 2.9
Enterobacter spp. (no. tested) (97) (158) (145) (143) (158) (160) (159) (172) (215)Meropenem 0.0 0.6 0.7 0.7 0.0 0.0 0.0 1.2 2.3Imipenem 0.0 0.6 0.7 0.7 0.0 0.0 0.0 1.7 1.9Ceftriaxone 7.2 8.2 13.1 9.8 8.9 9.4 13.8 8.7 17.2Ceftazidime 13.4 11.4 19.3 15.4 15.2 16.3 21.4 18.0 21.9Cefepime 0.0 0.6 0.7 2.1 1.3 0.6 0.0 4.7 3.7Piperacillin/tazobactam 6.2 5.1 11.0 7.0 6.3 5.6 6.9 10.5 11.2Gentamicin 2.1 1.3 4.1 4.2 7.6 9.4 6.9 3.5Tobramycin 1.0 1.3 5.5 4.9 5.1 8.8 7.5 7.0 7.9Ciprofloxacin 0.0 1.9 9.7 7.0 9.5 8.8 3.8 9.9 8.4Levofloxacin 5.7 7.5 3.1 8.7 7.4
E. coli (no. tested) (197) (312) (306) (303) (469) (724) (491) (640) (465) (487)Meropenem 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.8Imipenem 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.2Ceftriaxone 1.0 0.6 0.7 0.3 0.2 1.1 2.6 3.4 5.4 7.8Ceftazidime 2.5 1.6 2.3 0.3 0.4 1.5 3.1 3.3 1.5 3.7Cefepime 0.5 0.0 0.0 0.0 0.0 0.4 1.4 1.6 3.0 5.1Piperacillin/tazobactam 1.5 1.3 1.3 1.7 1.3 1.1 2.4 1.7 4.9 3.1Gentamicin 3.0 1.9 4.2 4.0 2.8 9.4 10.2 11.4 12.9Tobramycin 1.5 2.3 1.6 3.0 1.3 2.2 5.9 9.1 6.2 10.3Ciprofloxacin 4.1 2.9 9.2 7.3 10.9 20.7 21.6 27.5 29.0 31.8Levofloxacin 10.2 20.2 20.4 26.4 28.4 31.4
K. pneumoniae (no. tested) (118) (195) (176) (194) (235) (337) (367) (529) (222) (321)Meropenem 0.0 2.6 0.0 0.0 0.0 0.6 4.6 9.6 10.8 5.6Imipenem 0.0 2.1 0.0 0.0 0.0 0.6 1.9 7.9 12.2 5.3Ceftriaxone 0.0 2.6 1.1 1.5 0.9 2.7 10.4 12.1 15.3 11.8Ceftazidime 2.5 5.6 4.5 3.1 4.7 4.5 15.0 15.1 22.5 15.0Cefepime 0.0 3.6 0.6 0.0 0.4 0.9 4.4 10.8 10.8 6.2Piperacillin/tazobactam 4.2 3.1 1.1 2.6 2.1 3.6 10.9 14.7 21.6 11.5Gentamicin 2.5 5.1 3.4 2.6 4.7 4.5 6.8 7.2 8.1Tobramycin 2.5 5.2 2.3 2.1 5.1 4.7 13.4 15.5 22.5 14.3Ciprofloxacin 4.2 5.1 4.5 1.0 4.7 5.0 15.8 19.3 26.1 16.5Levofloxacin 4.3 4.5 14.2 18.9 25.7 16.2
P. mirabilis (no. tested) (95) (143) (142) (138) (154) (128) (147) (118) (171)Meropenem 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0Imipenem 0.0 1.4 0.0 0.0 0.0 0.0 0.0 0.8 0.0Ceftriaxone 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.6Ceftazidime 1.1 2.1 1.4 0.0 0.0 0.0 0.0 0.0 0.0Cefepime 1.1 0.7 0.0 0.0 0.0 0.0 0.0 0.0 0.6Piperacillin/tazobactam 0.0 0.7 0.0 0.0 0.0 0.0 0.0 0.0 0.0Gentamicin 1.1 7.7 4.2 5.8 5.8 0.8 3.4 5.1Tobramycin 0.0 4.9 3.5 4.3 1.3 0.0 0.7 4.2 2.3Ciprofloxacin 2.1 7.0 7.0 7.2 10.4 7.0 15.6 20.3 17.5Levofloxacin 7.8 6.3 11.6 16.9 14.0
420 P.R. Rhomberg, R.N. Jones / Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426

Table 4 (continued)
Organism (no. tested)/antimicrobial agent
% Resistancea
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Serratia spp. (no. tested) (53) (74) (74) (77) (133) (149) (134) (138) (145)Meropenem 3.8 0.0 0.0 0.0 0.0 0.0 0.7 0.0 2.1Imipenem 3.8 0.0 0.0 1.3 0.0 0.0 0.7 0.0 2.8Ceftriaxone 0.0 2.7 1.4 0.0 0.8 1.3 1.5 0.7 3.4Ceftazidime 0.0 2.7 1.4 2.6 0.8 2.7 2.2 0.7 0.7Cefepime 0.0 1.4 0.0 1.3 0.0 0.0 0.7 0.7 0.7Piperacillin/tazobactam 0.0 0.0 0.0 1.3 0.0 0.0 0.0 2.2 2.1Gentamicin 1.9 2.7 1.4 3.9 0.8 4.7 3.7 2.2Tobramycin 3.8 5.4 6.8 5.2 2.3 7.4 6.0 3.6 6.2Ciprofloxacin 3.8 8.1 8.1 1.3 3.8 1.3 1.5 4.3 4.8Levofloxacin 3.0 0.0 0.7 2.2 3.4
All Enterobacteriaceae (no. tested) (708) (1048) (1037) (1057) (1439) (1865) (1657) (1259) (1393) (1538)Meropenem 0.3 0.6 0.1 0.1 0.0 0.1 1.1 4.1 1.9 2.0Imipenem 0.3 0.7 0.1 0.2 0.1 0.1 0.5 3.3 2.4 1.8Ceftriaxone 1.7 2.9 2.6 2.1 1.9 2.4 5.2 6.8 5.7 8.6Ceftazidime 4.0 5.6 5.5 3.9 4.1 4.3 8.4 8.0 7.7 9.0Cefepime 0.4 1.0 0.3 0.4 0.3 0.4 1.4 5.3 3.4 3.8Piperacillin/tazobactam 2.3 2.7 2.5 2.8 2.2 2.0 5.0 7.8 8.0 6.0Gentamicin 2.7 4.0 3.8 4.6 4.6 6.8 7.4 8.9 7.5Tobramycin 1.7 3.3 2.9 4.2 3.1 4.0 6.9 11.2 7.8 8.8Ciprofloxacin 3.7 4.4 6.8 6.9 8.6 12.9 14.8 22.5 18.3 17.8Levofloxacin 7.0 11.7 13.2 21.7 17.3 16.8
A. baumannii (no. tested) (20) (34) (56) (55) (73) (111) (88) (86) (94)Meropenem 35.0 17.6 17.9 16.4 11.0 20.7 11.4 48.8 57.4Imipenem 10.0 8.8 10.7 14.5 2.7 10.8 4.5 37.2 47.9Ceftriaxone 40.0 32.4 35.7 40.0 39.7 45.9 48.9 68.6 68.1Ceftazidime 30.0 26.5 32.1 38.2 38.4 46.8 46.6 64.0 68.1Cefepime 20.0 23.5 30.4 32.7 26.0 38.7 31.8 59.3 62.8Piperacillin/tazobactam 30.0 20.6 21.4 21.8 24.7 46.8 39.8 66.3 69.1Gentamicin 50.0 32.4 33.9 34.5 34.2 39.6 36.4 55.8Tobramycin 30.0 17.6 26.8 21.8 9.6 13.5 8.0 43.0 40.4Ciprofloxacin 40.0 35.3 41.1 47.3 46.6 53.2 56.8 74.4 73.4Levofloxacin 41.1 46.8 42.0 73.3 64.9
P. aeruginosa (no. tested) (193) (299) (298) (301) (454) (689) (589) (606) (454) (439)Meropenem 16.1 10.0 8.4 4.7 7.3 6.0 6.8 6.4 8.6 7.5Imipenem 18.7 13.4 9.7 8.0 9.5 5.1 7.3 10.7 18.3 15.5Ceftriaxone 77.2 77.9 68.5 59.1 63.0 78.8 53.5 68.6 75.1 70.8Ceftazidime 10.9 13.0 10.1 10.3 10.8 13.4 9.8 12.9 10.8 9.8Cefepime 7.3 9.7 5.4 5.6 6.2 5.8 4.8 5.6 6.6 6.4Piperacillin/tazobactam 10.9 13.7 9.1 9.0 9.7 12.0 9.0 11.4 11.0 9.8Gentamicin 8.8 9.0 10.1 8.6 11.0 9.9 12.1 11.7 9.9Tobramycin 5.7 7.0 7.7 7.0 9.5 7.7 10.4 7.9 7.3 9.1Ciprofloxacin 11.9 20.4 22.1 23.9 25.3 21.2 22.4 20.6 19.6 17.3Levofloxacin 26.0 23.2 22.4 21.8 22.0 19.1
a Criteria as published by the CLSI (2008).
421P.R. Rhomberg, R.N. Jones / Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426
(Package Insert, 2007; Wisemann et al., 1995). Unlikeimipenem, meropenem does not require the coadministrationof the renal dehydropeptidase inhibitor cilastatin to preventrapid inactivation and toxicity. These risks are minimizedwith meropenem treatment, and it has been shown to be welltolerated in many clinical trials and at alternative dosingregimens to optimized PK/PD target attainments (Kuti et al.,2004; Package Insert, 2007; Roberts et al., 2009). Merope-nem is approved for meningitis because it penetrates well intomost body fluids and tissue, including the cerebral spinal
fluid. Bacterial meningitis infections caused by S. pneumo-niae,Haemophilus influenzae, andNeisseria meningitidis areall within the spectrum of meropenem treatment.
In the USA meropenem is not approved for antimicrobialtreatment of nosocomial pneumonia (including hospital-acquired bacterial pneumonia, ventilator-associated bacterialpneumonia, and health-care–associated bacterial pneumo-niae); however, it has demonstrated efficacy for theseindications in numerous clinical trials and is recommendedin the American Thoracic Society and Infectious Disease
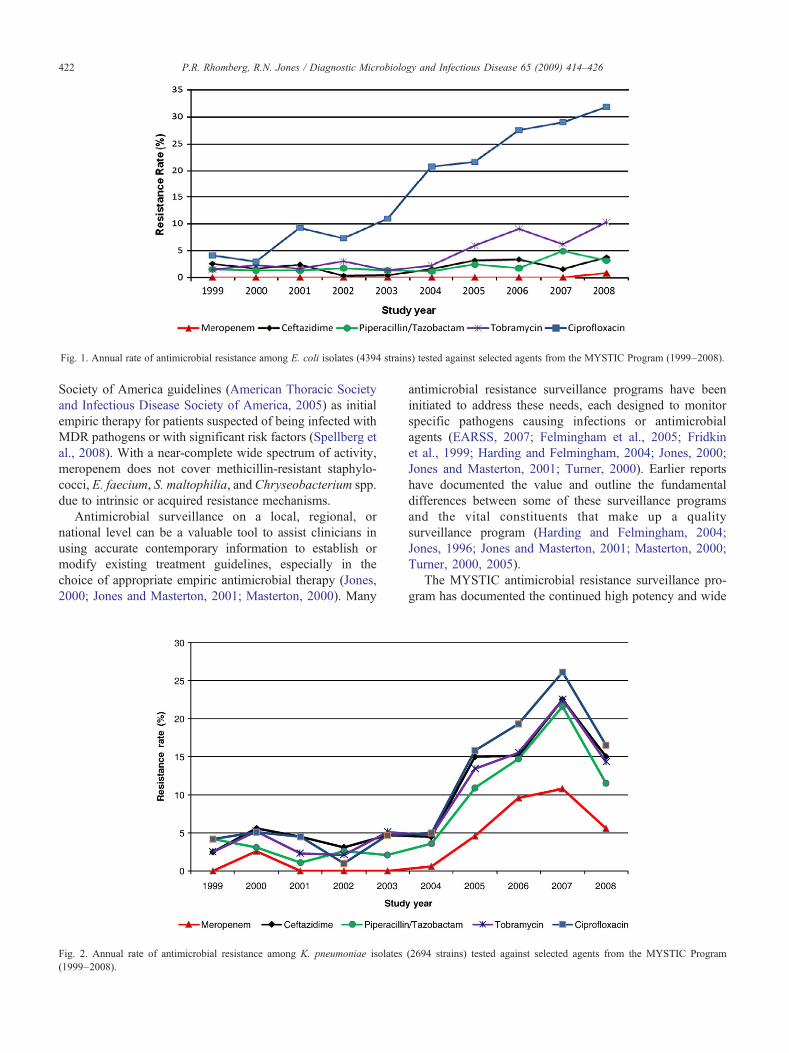
Fig. 1. Annual rate of antimicrobial resistance among E. coli isolates (4394 strains) tested against selected agents from the MYSTIC Program (1999–2008).
422 P.R. Rhomberg, R.N. Jones / Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426
Society of America guidelines (American Thoracic Societyand Infectious Disease Society of America, 2005) as initialempiric therapy for patients suspected of being infected withMDR pathogens or with significant risk factors (Spellberg etal., 2008). With a near-complete wide spectrum of activity,meropenem does not cover methicillin-resistant staphylo-cocci, E. faecium, S. maltophilia, and Chryseobacterium spp.due to intrinsic or acquired resistance mechanisms.
Antimicrobial surveillance on a local, regional, ornational level can be a valuable tool to assist clinicians inusing accurate contemporary information to establish ormodify existing treatment guidelines, especially in thechoice of appropriate empiric antimicrobial therapy (Jones,2000; Jones and Masterton, 2001; Masterton, 2000). Many
Fig. 2. Annual rate of antimicrobial resistance among K. pneumoniae isolates(1999–2008).
antimicrobial resistance surveillance programs have beeninitiated to address these needs, each designed to monitorspecific pathogens causing infections or antimicrobialagents (EARSS, 2007; Felmingham et al., 2005; Fridkinet al., 1999; Harding and Felmingham, 2004; Jones, 2000;Jones and Masterton, 2001; Turner, 2000). Earlier reportshave documented the value and outline the fundamentaldifferences between some of these surveillance programsand the vital constituents that make up a qualitysurveillance program (Harding and Felmingham, 2004;Jones, 1996; Jones and Masterton, 2001; Masterton, 2000;Turner, 2000, 2005).
The MYSTIC antimicrobial resistance surveillance pro-gram has documented the continued high potency and wide
(2694 strains) tested against selected agents from the MYSTIC Program
Fig. 3. Annual rate of antimicrobial resistance among P. aeruginosa isolates (4322 strains) tested against selected agents from the MYSTIC Program(1999–2008).
423P.R. Rhomberg, R.N. Jones / Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426
spectrum of activity of meropenem worldwide againstEnterobacteriaceae species isolates, including those withESBL- and AmpC-producing resistance mechanisms (Cas-tanheira et al., 2008; Jones et al., 2002, 2008; Mathai et al.,2002; Pfaller and Jones, 2000; Rhomberg and Jones, 2007;Turner, 2004). Recently, there has been a significant spreadof the Ambler class A serine carbapenemase KPC-typeendemic within the geographically distinct areas, primarilyamong K. pneumoniae isolates, but transmission to otherEnterobacteriaceae species has also been observed viamobile genetic elements (Hussein et al., 2009; Jones et al.,2008; Rhomberg et al., 2007). This KPC-type resistance
Fig. 4. Annual rate of antimicrobial resistance among all Enterobacteriaceae isolate(1999–2008).
mechanism has not yet been observed within the Europeanportion of the MYSTIC surveillance program through the2008 bacterial collection (Turner, 2009). The presence of theSME-type serine carbapenemase, identified in only 3 S.marcescens isolates in the USA MYSTIC Program over 10years, remains rare and does not seem to be as transmissibleor virulent as the KPC type (Deshpande et al., 2006; Galeset al., 2001; Queenan et al., 2000). Other clonal occurrencesof carbapenem resistances have also compromised therapyamong nonfermentative Gram-negative bacilli throughoutthe interval of the MYSTIC Program (USA) in someinstitutions (Jones et al., 2004).
s (13 001 strains) tested against selected agents from the MYSTIC Program

424 P.R. Rhomberg, R.N. Jones / Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426
The current CLSI MIC susceptibility breakpoints for thecarbapenems listed in the M100-S19 standard (e.g. ≤4, 8,≥16 meropenem against Enterobacteriaceae) are higherthan those in use by EUCAST for Europe (≤2, 4, ≥8),which has necessitated re-evaluation of breakpoints by theCLSI to achieve international harmonization. These to belowered CLSI carbapenem breakpoints will cause a shifttoward elevated resistance rates for some bacterial specieswith low level carbapenem resistance mechanisms (MICvalues 0.5–4 μg/ml).
While the carbapenem resistance rates have not variedsignificantly during the monitored interval of 1999 to 2008for the MYSTIC Program, other comparator broad-spectrum agents have shown increasing resistance rates,most notably the fluoroquinolone class (Adam et al., 2009;Jones, 2003; Jones and Pfaller, 2002; Rhomberg et al.,2003). The presence of endemic and epidemic dissemina-tion of fluoroquinolone-resistant clones among Enterobac-teriaceae species isolates has been observed with aresulting effect to drive up the overall fluoroquinoloneresistance rates. Increasing fluoroquinolone resistance rateshave been reported among many bacterial species wheresurveillance is performed (Figs. 1–4) and evidence of arelationship to use has been suggested (Adam et al., 2009;Mutnick et al., 2004). The genus groups showing thegreatest increases in fluoroquinolone resistance in theMYSTIC program are the indole-positive Proteae, E. coli,and Acinetobacter spp.
Clearly, the USA MYSTIC Program (1999–2008) hascontributed to the monitoring of antimicrobial resistances viause of molecular techniques to identify resistance mechan-isms, clonal spread, relationships to local hospital usestatistics, and ranking of the most broad-spectrum agentscurrently available for empiric treatment of serious hospital-associated infections. As documented initially in 1999, theMYSTIC Program for 2008 again confirms that carbape-nems (meropenem) have the widest coverage of nosocomialpathogens, and they remain excellent choices to apply invarious monotherapeutic or combination regimens tomaximize clinical outcomes. As newer and investigationalcarbapenems (doripenem, razopenem, etc.) become estab-lished in the antimicrobial market place, the class must befollowed by well-structured resistance surveillance studies toassure continued value across the United States (Edwards,1995; Paterson, 2000; Wisemann et al., 1995) and toestablish the advantages of alternative dosing and drugdelivery (Crandon et al., 2009; Kuti et al., 2003, 2004; Liet al., 2006; Roberts et al., 2009).
Acknowledgments
This 10-year surveillance study was supported by aneducational/research grant from AstraZeneca Pharmaceuti-cals. The USA MYSTIC Program sites and participantsbetween 1999 and 2008 were Arkansas Children's Hospital(T. Beavers-May/R. Jacobs/G. Schutze/S. Stovall); Chil-
dren's Hospital (J. Bradley); Children's Hospital of OrangeCounty (A. Arrieta/O. Vargas); Christiana Care (E. Foraker/L. Steele-Moore); Cleveland Clinic Foundation (G. Hall/D.Wilson/M. Tuohy); Clinical Laboratories of Hawaii (F. Pien/L. Ikei-Canter); Columbia Presbyterian Medical Center (P.Della-Latta/P. Pancholi/S. Whittier/S. Mittman); CreightonUniversity, St. Joseph Hospital (S. Cavalieri/M. Hostetter/A.Fleming); Denver Health Medical Center (M. Wilson/A.Graepler); Emory University (F. Nolte); Iowa MethodistMedical Center (A. Herring/L. Roller); Kaiser PermanenteMedical Group, Berkeley Regional Laboratory (J. Fusco/J.Konnig); New York University Medical Center, TischHospital (P. Tierno); Northwestern Memorial Hospital (L.Peterson); Ochsner Clinic Foundation (G. Pankey/D. Ash-craft); Penrose Hospital (M. Reynolds); Robert WoodJohnson Medical School (M. Weinstein/J. Rothberg);Spectrum Health (T. Capps); University Hospitals of Cleve-land (M. Jacobs/S. Bajaksouzian); University of ColoradoHospital (N. Madinger/J. Monahan); University of IowaHospitals and Clinics (J. Croco); University of KentuckyHospital (J. Ribes/S. Overman); University of MassachusettsMedical Center (M. Mitchell); MD Anderson Cancer Center,University of Texas (K. Rolston/R. Prince); ARUP Labora-tories, University of Utah, (M. Bale/A. Croft); University ofWashington (A. Limaye/S. Swanzy); Vanderbilt MedicalCenter (C. Stratton/R. Verrall); Portland Veterans AffairsMedical Center (D. Sewell); and Winthrop UniversityHospital (P. Schoch). The authors thank you for yourexcellent compliance to protocol design.
References
Aboufaycal H, Sader HS, Rolston K, Deshpande LM, TolemanM, Bodey G,Raad I, Jones RN (2007) blaVIM-2 and blaVIM-7 carbapenemase-producing Pseudomonas aeruginosa isolates detected in a tertiary caremedical center in the United States: report from the MYSTIC program. JClin Microbiol 45:614–615.
Adam HJ, Hoban DJ, Gin AS, Zhanel GG (2009) Association betweenfluoroquinolone usage and a dramatic rise in ciprofloxacin-resistantStreptococcus pneumoniae in Canada, 1997–2006. Int J AntimicrobAgents 34:82–85.
American Thoracic Society, Infectious Disease Society of America (2005)Guidelines for the management of adults with hospital-acquired,ventilator-associated, and healthcare-associated pneumonia. Am J RespirCrit Care Med 15:388–416.
Bradford PA, Urban C, Mariano N, Projan SJ, Rahal JJ, Bush K (1997)Imipenem resistance in Klebsiella pneumoniae is associated with thecombination of ACT-1, a plasmid-mediated AmpC beta-lactamase, andthe loss of an outer membrane protein. Antimicrob Agents Chemother41:563–569.
Bradford PA, Bratu S, Urban C, Visalli M, Mariano N, Landman D, RahalJJ, Brooks S, Cebular S, Quale J (2004) Emergence of carbapenem-resistant Klebsiella species possessing the class A carbapenem-hydrolyzing KPC-2 and inhibitor-resistant TEM-30 beta-lactamases inNew York City. Clin Infect Dis 39:55–60.
Bratu S, Landman D, Haag R, Recco R, Eramo A, Alam M, Quale J (2005)Rapid spread of carbapenem-resistant Klebsiella pneumoniae in NewYork City: a new threat to our antibiotic armamentarium. Arch InternMed 165:1430–1435.
Cao VT, Arlet G, Ericsson BM, Tammelin A, Courvalin P, Lambert T(2000) Emergence of imipenem resistance in Klebsiella pneumoniae

425P.R. Rhomberg, R.N. Jones / Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426
owing to combination of plasmid-mediated CMY-4 and permeabilityalteration. J Antimicrob Chemother 46:895–900.
Castanheira M, Mendes RE, Rhomberg PR, Jones RN (2008) Rapidemergence of blaCTX-M among Enterobacteriaceae in U.S. MedicalCenters: molecular evaluation from the MYSTIC Program (2007).Microb Drug Resist 14:211–216.
Clinical and Laboratory Standards Institute (CLSI) (2008) Development ofin vitro susceptibility testing criteria and quality control parameters—third edition, M23-A3. Wayne, PA: CLSI.
Clinical and Laboratory Standards Institute (CLSI) (2009a) Performancestandards for antimicrobial disk susceptibility tests; approved standard—10th edition, M02-A10. Wayne, PA: CLSI.
Clinical and Laboratory Standards Institute (CLSI) (2009b) Methods fordilution antimicrobial susceptibility tests for bacteria that growaerobically; approved standard—eighth edition, M07-A8. Wayne, PA:CLSI.
Clinical and Laboratory Standards Institute (CLSI) (2009c) Performancestandards for antimicrobial susceptibility testing: 19th informationalsupplement (M100-S19). Wayne, PA: CLSI.
Crandon JL, Kuti JL, Jones RN, Nicolau DP (2009) Comparison of 2002–2006 OPTAMA programs for US hospitals: focus on gram-negativeresistance. Ann Pharmacother 43:220–227.
Deshpande LM, Rhomberg PR, Sader HS, Jones RN (2006) Emergence ofserine carbapenemases (KPC and SME) among clinical strains ofEnterobacteriaceae isolated in the United States Medical Centers: reportfrom the MYSTIC Program (1999–2005). Diagn Microbiol Infect Dis56:367–372.
EARSS (2007) European Antimicrobial Surveillance System. Available athttp://www.rivm.nl/earss/about. Accessed October 25, 2007.
Edwards JR (1995) Meropenem: a microbiological overview. J AntimicrobChemother 36(Suppl A):1–17.
Felmingham D, White AR, Jacobs MR, Appelbaum PC, Poupard J,Miller LA, Gruneberg RN (2005) The Alexander Project: the benefitsfrom a decade of surveillance. J Antimicrob Chemother 56(Suppl 2):ii3–ii21.
Fridkin SK, Steward CD, Edwards JR, Pryor ER, McGowan Jr JE,Archibald LK, Gaynes RP, Tenover FC (1999) Surveillance ofantimicrobial use and antimicrobial resistance in United States hospitals:project ICARE phase 2. Project Intensive Care Antimicrobial ResistanceEpidemiology (ICARE) hospitals. Clin Infect Dis 29:245–252.
Gales AC, Biedenbach DJ, Winokur P, Hacek DM, Pfaller MA, Jones RN(2001) Carbapenem-resistant Serratia marcescens isolates producingBush group 2f beta-lactamase (SME-1) in the United States: results fromthe MYSTIC Programme. Diagn Microbiol Infect Dis 39:125–127.
Harding I, Felmingham D (2004) PROTEKT years 1–3 (1999–2002): studydesign and methodology. J Chemother 16(Suppl 6):9–18.
Hossain A, Ferraro MJ, Pino RM, Dew III RB, Moland ES, Lockhart TJ,Thomson KS, Goering RV, Hanson ND (2004) Plasmid-mediatedcarbapenem-hydrolyzing enzyme KPC-2 in an Enterobacter sp.Antimicrob Agents Chemother 48:4438–4440.
Hussein K, Sprecher H, Mashiach T, Oren I, Kassis I, Finkelstein R (2009)Carbapenem resistance among Klebsiella pneumoniae isolates: riskfactors, molecular characteristics, and susceptibility patterns. InfectControl Hosp Epidemiol 30:666–671.
Jones RN (1996) The emergent needs for basic research, education, andsurveillance of antimicrobial resistance. Problems facing the report fromthe American Society for Microbiology Task Force on AntibioticResistance. Diagn Microbiol Infect Dis 25:153–161.
Jones RN (2000) Detection of emerging resistance patterns withinlongitudinal surveillance systems: data sensitivity and microbialsusceptibility. MYSTIC Advisory Board. Meropenem Yearly Suscep-tibility Test Information Collection. J Antimicrob Chemother 46(Suppl T2):1–8.
Jones RN (2003) Global epidemiology of antimicrobial resistance amongcommunity-acquired and nosocomial pathogens: a five-year summaryfrom the SENTRY Antimicrobial Surveillance Program (1997–2001).Semin Respir Crit Care Med 24:121–134.
Jones RN, Masterton R (2001) Determining the value of antimicrobialsurveillance programs. Diagn Microbiol Infect Dis 41:171–175.
Jones RN, Pfaller MA (2002) Ciprofloxacin as broad-spectrum empirictherapy—are fluoroquinolones still viable monotherapeutic agentscompared with beta-lactams: data from the MYSTIC Program (US)?Diagn Microbiol Infect Dis 42:213–215.
Jones RN, Rhomberg PR, Varnam DJ, Mathai D (2002) A comparison of theantimicrobial activity of meropenem and selected broad-spectrumantimicrobials tested against multi-drug resistant Gram-negative bacilliincluding bacteraemic Salmonella spp.: initial studies for the MYSTICprogramme in India. Int J Antimicrob Agents 20:426–431.
Jones RN, Deshpande L, Fritsche TR, Sader HS (2004) Determination ofepidemic clonality among multidrug-resistant strains of Acinetobacterspp. and Pseudomonas aeruginosa in the MYSTIC Programme (USA,1999–2003). Diagn Microbiol Infect Dis 49:211–216.
Jones RN, Mendes C, Turner PJ, Masterton R (2005) An overview of theMeropenem Yearly Susceptibility Test Information Collection (MYS-TIC) Program: 1997–2004. Diagn Microbiol Infect Dis 53:247–256.
Jones RN, Kirby JT, Rhomberg PR (2008) Comparative activity ofmeropenem in US medical centers (2007): initiating the 2nd decade ofMYSTIC program surveillance.DiagnMicrobiol Infect Dis 61:203–213.
Kuti JL, Dandekar PK, Nightingale CH, Nicolau DP (2003) Use of MonteCarlo simulation to design an optimized pharmacodynamic dosingstrategy for meropenem. J Clin Pharmacol 43:1116–1123.
Kuti JL, Nightingale CH, Nicolau DP (2004) Optimizing pharmacodynamictarget attainment using the MYSTIC antibiogram: data collected inNorth America in 2002. Antimicrob Agents Chemother 48:2464–2470.
Landman D, Quale JM, Mayorga D, Adedeji A, Vangala K, Ravishankar J,Flores C, Brooks S (2002) Citywide clonal outbreak of multiresistantAcinetobacter baumannii and Pseudomonas aeruginosa in Brooklyn,NY: the preantibiotic era has returned. Arch Intern Med 162:1515–1520.
Li C, Kuti JL, Nightingale CH, Nicolau DP (2006) Population pharmaco-kinetic analysis and dosing regimen optimization of meropenem in adultpatients. J Clin Pharmacol 46:1171–1178.
Masterton RG (2000) Surveillance studies: how can they help themanagement of infection? J Antimicrob Chemother 46(Suppl T2):53–58.
Mathai D, Rhomberg PR, Biedenbach DJ, Jones RN (2002) Evaluation ofthe in vitro activity of six broad-spectrum beta-lactam antimicrobialagents tested against recent clinical isolates from India: a survey of tenmedical center laboratories. Diagn Microbiol Infect Dis 44:367–377.
Miriagou V, Tzouvelekis LS, Rossiter S, Tzelepi E, Angulo FJ, WhichardJM (2003) Imipenem resistance in a Salmonella clinical strain due toplasmid-mediated class A carbapenemase KPC-2. Antimicrob AgentsChemother 47:1297–1300.
Mutnick AH, Rhomberg PR, Sader HS, Jones RN (2004) Antimicrobialusage and resistance trend relationships from the MYSTIC Programmein North America (1999–2001). J Antimicrob Chemother 53:290–296.
Package Insert (2007) Merrem. Wilmington, DE: AstraZenecaPharmaceuticals.
Paterson DL (2000) Recommendation for treatment of severe infectionscaused by Enterobacteriaceae producing extended-spectrum beta-lactamases (ESBLs). Clin Microbiol Infect 6:460–463.
Pfaller MA, Jones RN (1997) A review of the in vitro activity of meropenemand comparative antimicrobial agents tested against 30,254 aerobic andanaerobic pathogens isolated world wide.DiagnMicrobiol Infect Dis 28:157–163.
Pfaller MA, Jones RN (2000) MYSTIC (Meropenem Yearly SusceptibilityTest Information Collection) results from the Americas: resistanceimplications in the treatment of serious infections. MYSTIC StudyGroup (Americas). J Antimicrob Chemother 46(Suppl T2):25–37.
Pfaller MA, Jones RN, Biedenbach DJ (2001) Antimicrobial resistancetrends in medical centers using carbapenems: report of 1999 and 2000results from the MYSTIC program (USA). Diagn Microbiol Infect Dis41:177–182.
Queenan AM, Torres-Viera C, Gold HS, Carmeli Y, Eliopoulos GM,Moellering Jr RC, Quinn JP, Hindler J, Medeiros AA, Bush K (2000)
426 P.R. Rhomberg, R.N. Jones / Diagnostic Microbiology and Infectious Disease 65 (2009) 414–426
SME-type carbapenem-hydrolyzing class A beta-lactamases fromgeographically diverse Serratia marcescens strains. Antimicrob AgentsChemother 44:3035–3039.
Rhomberg PR, Jones RN (2007) Contemporary activity of meropenem andcomparator broad-spectrum agents: MYSTIC Program report from theUnited States component (2005). Diagn Microbiol Infect Dis 57:207–215.
Rhomberg PR, Fritsche TR, Sader HS, Jones RN (2003) Antibioticresistance in hospitalized patients: MYSTIC Program (1999–2002).Antibiot Clin 7:2–7.
Rhomberg PR, Jones RN, Sader HS (2004a) Results from the MeropenemYearly Susceptibility Test Information Collection (MYSTIC)Programme: report of the 2001 data from 15 United States medicalcentres. Int J Antimicrob Agents 23:52–59.
Rhomberg PR, Jones RN, Sader HS, Fritsche TR (2004b) Antimicro-bial resistance rates and clonality results from the MeropenemYearly Susceptibility Test Information Collection (MYSTIC)programme: report of year five (2003). Diagn Microbiol InfectDis 49:273–281.
Rhomberg PR, Fritsche TR, Sader HS, Jones RN (2005) Comparativeantimicrobial potency of meropenem tested against Gram-negativebacilli: report from the MYSTIC surveillance program in the UnitedStates (2004). J Chemother 17:459–469.
Rhomberg PR, Fritsche TR, Sader HS, Jones RN (2006a) Antimicrobialsusceptibility pattern comparisons among intensive care unit and generalward Gram-negative isolates from the Meropenem Yearly SusceptibilityTest Information Collection Program (USA).Diagn Microbiol Infect Dis56:57–62.
Rhomberg PR, Fritsche TR, Sader HS, Jones RN (2006b) Clonaloccurrences of multidrug-resistant Gram-negative bacilli: report fromthe Meropenem Yearly Susceptibility Test Information CollectionSurveillance Program in the United States. Diagn Microbiol Infect Dis54:249–257.
Rhomberg PR, Deshpande LM, Kirby JT, Jones RN (2007) Activity ofmeropenem as serine carbapenemases evolve in US Medical Centers:monitoring report from the MYSTIC Program (2006). Diagn MicrobiolInfect Dis 59:425–432.
Roberts JA, Kirkpatrick CM, Roberts MS, Robertson TA, Dalley AJ,Lipman J (2009) Meropenem dosing in critically ill patients with sepsisand without renal dysfunction: intermittent bolus versus continuousadministration? Monte Carlo dosing simulations and subcutaneoustissue distribution. J Antimicrob Chemother 64:142–150.
Senda K, Arakawa Y, Ichiyama S, Nakashima K, Ito H, Ohsuka S,Shimokata K, Kato N, Ohta M (1996a) PCR detection of metallo-beta-lactamase gene (blaIMP) in gram-negative rods resistant to broad-spectrum beta-lactams. J Clin Microbiol 34:2909–2913.
Senda K, Arakawa Y, Nakashima K, Ito H, Ichiyama S, Shimokata K, KatoN, Ohta M (1996b) Multifocal outbreaks of metallo-beta-lactamase–
producing Pseudomonas aeruginosa resistant to broad-spectrum beta-lactams, including carbapenems. Antimicrob Agents Chemother 40:349–353.
Spellberg B, Guidos R, Gilbert D, Bradley J, Boucher HW, Scheld WM,Bartlett JG, Edwards Jr J (2008) The epidemic of antibiotic-resistantinfections: a call to action for the medical community from the InfectiousDiseases Society of America. Clin Infect Dis 46:155–164.
Tenover FC, Arbeit RD, Goering RV, Mickelsen PA, Murray BE, PersingDH, Swaminathan B (1995) Interpreting chromosomal DNA restrictionpatterns produced by pulsed-field gel electrophoresis: criteria forbacterial strain typing. J Clin Microbiol 33:2233–2239.
Toleman MA, Rolston K, Jones RN, Walsh TR (2004) blaVIM-7, anevolutionarily distinct metallo-beta-lactamase gene in a Pseudomonasaeruginosa isolate from the United States. Antimicrob Agents Che-mother 48:329–332.
Turner PJ (2000) MYSTIC (Meropenem Yearly Susceptibility TestInformation Collection): a global overview. J Antimicrob Chemother46(Suppl T2):9–23.
Turner PJ (2004) Susceptibility of meropenem and comparators testedagainst 30,634 Enterobacteriaceae isolated in the MYSTIC Programme(1997–2003). Diagn Microbiol Infect Dis 50:291–293.
Turner PJ (2005) Use of a program-specific website to disseminatesurveillance data obtained from the Meropenem Yearly SusceptibilityTest Information Collection (MYSTIC) Study. Diagn Microbiol InfectDis 53:273–279.
Turner PJ (2009) MYSTIC Europe 2007: activity of meropenem and otherbroad-spectrum agents against nosocomial isolates. Diagn MicrobiolInfect Dis 63:217–222.
Turner PJ, Greenhalgh JM, Edwards JR, McKellar J (1999) The MYSTIC(Meropenem Yearly Susceptibility Test Information Collection)programme. Int J Antimicrob Agents 13:117–125.
Wisemann LR, Wagstaff AJ, Brogden RN, Bryson HM (1995) Meropenem:a review of its antibacterial activity, pharmacokinetic properties andclinical efficacy. Drugs 50:73–101.
Woodford N, Tierno Jr PM, Young K, Tysall L, Palepou MF, Ward E,Painter RE, Suber DF, Shungu D, Silver LL, Inglima K, Kornblum J,Livermore DM (2004) Outbreak of Klebsiella pneumoniae producinga new carbapenem-hydrolyzing class A beta-lactamase, KPC-3, in aNew York Medical Center. Antimicrob Agents Chemother 48:4793–4799.
Woodford N, Hill RL, Livermore DM (2007) In vitro activity of tigecyclineagainst carbapenem-susceptible and -resistant isolates of Klebsiella spp.and Enterobacter spp. J Antimicrob Chemother 59:582–583.
Yigit H, Queenan AM, Anderson GJ, Domenech-Sanchez A, Biddle JW,Steward CD, Alberti S, Bush K, Tenover FC (2001) Novel carbapenem-hydrolyzing beta-lactamase, KPC-1, from a carbapenem-resistant strainof Klebsiella pneumoniae. Antimicrob Agents Chemother 45:1151–1161.














![Anti-Infectives - AscellaHealth hcl meropenem [inj] methenamine hippurate methenamine mandelate methylene blue ... EDROPHONIUM CHLORIDE entacapone ...](https://static.fdocuments.us/doc/165x107/5ab0bac97f8b9ac3348b8587/anti-infectives-ascellahealth-hcl-meropenem-inj-methenamine-hippurate-methenamine.jpg)



