Summary of psychiatric disorders during pregnancy & lactation
27
Psychiatric Disorders in Pregnant & Lactating women Dr\ Hosam Hassan PR Director National Mental Health Council
-
Upload
hosam-hassan -
Category
Health & Medicine
-
view
91 -
download
5
Transcript of Summary of psychiatric disorders during pregnancy & lactation

Psychiatric Disorders
in
Pregnant & Lactating women
Dr\ Hosam Hassan
PR Director
National Mental Health Council

Agenda
1) Detection , Prediction, Prevention of
Mental Disorders Before & during
pregnancy .
2) Managements of Mental Disorders
during Pregnancy & Lactation .
3 ) Consent & Mental Capacity .
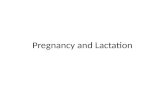
Introduction
PsychiatryObstetric & Gynecology
Already Diagnosed as a Psychiatric
Patient
Psychiatric Disorders Related To
Menstruation, Pregnancy & Labor
Detection
Prediction
Management
Prevention

Detection - Prediction
of Mental Disorder
Current Mental Disorder Potential Risk
Previous Treatments
Admission Consultations Medications
Past History of Mental illness
( previous deliveries ?)
Examination
Mental State( Thinking / Mood )
Psychological Tests
( EPDS )
Regular Check Up
Past Family History
( previous deliveries ?)
Screening Questions
Loss of interest
Feeling down
Need Help

Prevention
High Risk Mild
SymptomsPrevious Episodes
Psychosocial Intervention
Brief psychotherapy Social Support
Referral

Management
Treating Current Mental Disorder
Planning for pregnancy
PregnancyAfter
Delivery
Already
Diagnosed
Mental
Disorder
Developing
during any
Stage

Management of Psychiatric
DisorderInvestigation
Psychometry – Further Assessment
PsychotherapySupportive – CBT – Interpersonal
Psychopharmacotherapy
ECT( Electro – Convulsive Therapy )
Mild
Moderate
Severe

Overview of Psychiatric
Disorders
Neurotic Disorders
GAD PD OCD PTSD Phobia
Mood Disorders
Depression Mania Bipolar
Psychotic Disorders
Delusions + Hallucinations Schizophrenia Brief Psychotic Episode
Substance Abuse
Benzodiazepine Opiates Cannabis Nicotine Alcohol

Overview of Psychiatric
Disorders
Eating DisordersAnorexia Nervosa
Bulimia Nervosa
Pica
Sleep Disorders
Insomnia Restless Leg Syndrome

Postpartum Psychiatric Illness
Characteristic SymptomsOnsetIncidence
Mood lability
Tearfulness
Insomnia
Anxiety
Within first
week
50 to 75%Postpartum
Blues
Depressed Mood
Excessive Anxiety
Insomnia
Usually
insidious, within
first two to
three months
10 to 15%Postpartum
Depression
Agitation and Irritability
Depressed Mood or
Euphoria
Delusions
Depersonalization
Disorganized Behavior
Usually within
first two to four
weeks
0.1 to
0.2%
Postpartum
Psychosis

Psychopharmacotherapy During
PregnancyGeneral Rules
Written Plan of Management
Informed Consent
Medications
Switch to The safest Drug Monotherapy Minimal Effective doseGradual withdrawal before
delivery (BDZ, SSRIs )
Try to Avoid Medications in 1st Trimester
Follow Up Psychotherapy
Discuss with the patient
Risks Benefits
ContinuationDiscontinuation
TeratogenicityRelapse

Psychopharmacotherapy During
LactationGeneral Rules
Medications
Switch to The safest Drug Monotherapy Minimal Effective doseSingle dose before infant
longest sleep period
You shouldn’t discourage breast feeding
Schedule Feedings according to half life of the drug & its serum levels
Try to use non pharmacological interventions
Follow Up Psychotherapy
Discuss with the patient
Risks Benefits
ContinuationDiscontinuation
Possible effects of drugs on babyRelapse

Antipsychotics( Neuroleptics / Major Tranquilizers )
Mode of Action
↓Dopamine
Major Indications
Psychosis
Bipolar Mood Disorder
Agitation
Types
Typical 1st Generation Conventional
Chlorpromazine Haloperidol Pimozide
Atypical 2nd Generation
RisperidoneOlanzapineQuietiapineClozapine
Side Effects
Extra Pyramidal Dystonia
pseudo parkinsonism
NeurolepticMalignant Syndrome
Hyperprolactinemia
Metabolic Syndrome

Antipsychotics
Generally Antipsychotics are categorized as cluster C drugs
Except Clozapine is Cluster B
Better Avoid :
Depot injections for◦ possible extra pyramidal effect on the baby
◦ may produce severe withdrawal symptoms after delivery
Anti - cholinergic :
◦ Possible side effects on the baby
◦ Better adjust dose of antipsychotics

Antipsychotics
WhylactationWhypregnancy
If the baby has
hepatic impairment
Risk of
Agranulocytosis
ClozapineContra-indicated
Weight Gain (Mother)
Gestational
Diabetes
AtypicalBetter Avoid
Haloperidol
Chlorpromazine
Haloperidol
Chlorpromazine
Use but with
caution
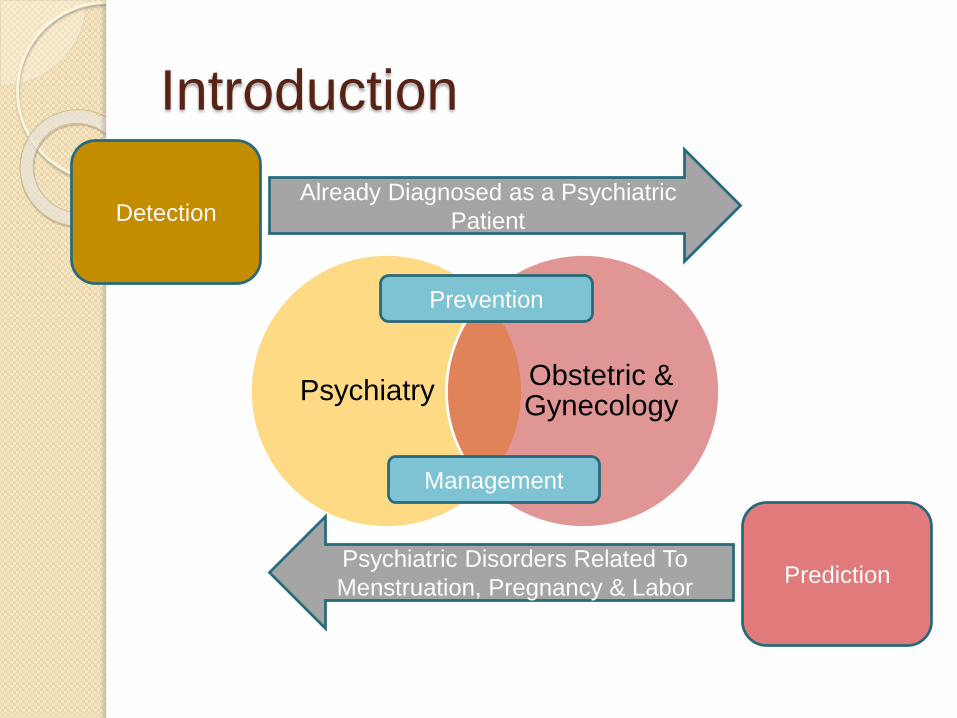
Antidepressants
Types
TCAs - Tricyclic Antidepressants
AmitriptylineClomipramine
imipramine
SSRIs - Selective Serotonin
Reuptake Inhibitors Fluoxetine
paroxetine SertralineCipalopram
MAOIs –Monoamine
Oxidase Inhibitors
Hydrazines
Mode of Action
↑Serotonin↑Noradrenaline↑Dopamine↓Histamine↓Ach
↑Serotonin
↑Tyramine
Major Indications
Depression
Anxiety
Side Effects
Dry Mouth Blurring of Vision Urine retention
Cardiotoxic
NauseaVomiting
DiscontinuationSerotonin Syndrome
Hypertensive Crisis with Tyramine
Containing Food

Antidepressants
Generally Antidepressants are categorized as cluster C drugs
Except Nortriptyline (TCA ) & Paroxetine( SSRI ) D
It is better to prescribe TCAs rather than SSRIs during pregnancy:
◦ for SSRIs are newer & less studied regarding effect on pregnancy & lactation
◦ A study in 2006 showed that using SSRIs after 20 week gestation increase risk of persistent pulmonary hypertension in neonates .
Neonates may show Discontinuation symptoms ( neonatal toxicity ) of antidepressants taken in pregnancy :
Feeding Difficulties, irritability , Rigidity , Respiratory Distress ( for SSRIs) , Diarrhea , Jitterness , Muscle weakness ( for TCAs ) usually mild & self limiting ( 1-2 weeks ) , Less frequent signs of excessive crying , Sleep disturbance , Seizures could occur , the infant should be monitored .

Antidepressants
WhylactationWhypregnancy
Present in breast
milk at relatively
high levels
Citalopram
Fluoxetine
Congenital
Cardiac
Malformations
ParoxetineBetter Avoid
HypertentionVenlafaxine
Present in breast
milk at relatively
low levels
Imipramine
Setraline
Imipramine
Fluoxetine
Use but with
caution

Mood Stabilizers
Types
AnticonvulsantsValproate
carbamezapineLamotrigine
Lithium
Mode of Action
↑GABA
Modulate Cell membrane excitability
Major Indications
Epilepsy
Bipolar
Serious Side
Effects
Bone marrow depression
Skin Rashes
Toxicityrenal failure
hypothyroidism

Mood Stabilizers
Generally Mood Stabilizers are categorized ascluster D drugs
Except Lamotrigine C
Careful Choice of drug should be considered for any female in her child bearing period .
Try switching gradually to antipsychotics
Should the patient continue taking mood stabilizers , special care should be offered :
◦ Generally :offer appropriate screening & counseling regarding continuation of pregnancy , the need for additional monitoring & risks to the fetus .
full pediatric assessment of the newborn infant , & monitor for the 1st few weeks .
◦ lithium : Monitor serum level every 4 weeks 36th week weekly .
Adequate fluid intake .
Hospital delivery with monitoring specially fluid balance
◦ Valproate : Max dose 1 gm daily in divided dose & slow release form .
Add Folic Acid 5 mg/day .

Mood Stabilizers
WhylactationWhypregnancy
Present in breast
milk at high levels
Hypotonia -
lethargy
Lithium•Fetal Heart defects
60 in 1000
•Ebstein anomaly
10 in 20,000
LithiumBetter
Avoid
Steven-johnson
syndrome in the
infant
Lamotrigine• Neural tube defect
(spina bifida)
100 – 200 in 10,000
Valproate
Single dose
/day
Carbamezapine•Neural tube defect
20 – 50 in 10,000
CarbamezapineUse but
with
caution
Valproate•Oral cleft
9 in 1000
Lamotrigine
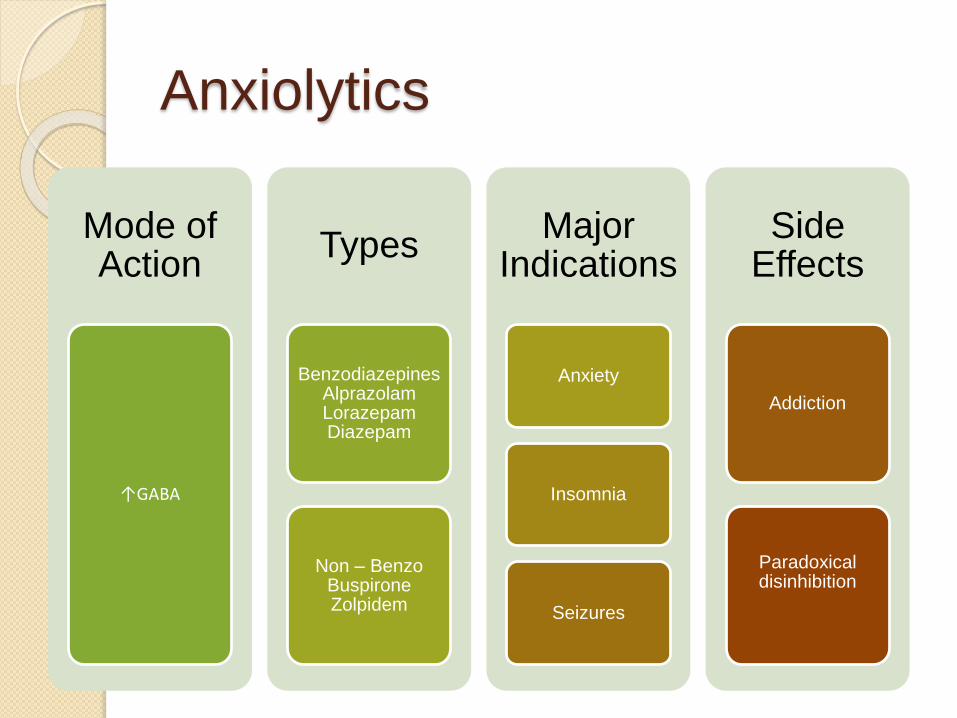
Anxiolytics
Mode of Action
↑GABA
Types
BenzodiazepinesAlprazolamLorazepamDiazepam
Non – BenzoBuspironeZolpidem
Major Indications
Anxiety
Insomnia
Seizures
Side Effects
Addiction
Paradoxical disinhibition
Anxiolytics
Generally Anxiolytics are categorized ascluster D drugs
Except : Flurazepam X / Zolpidem C / Buspirone B
Better Avoided during pregnancy :
◦ Fetus Cleft palate
◦ Neonate Floppy baby Syndrome ( Hypotonia , Hypothermia , Respiratory Depression )
If used :
◦ Short period .
◦ Minimal dose .

The organization of services
Clinical Network
MultiDisciplinary
Service
Clear Referral Protocol
Access to Specialized
Experts

References
NICE clinical guidelines for Antenatal & Postnatal Mental
Health .
National Institute for Health & Clinical Excellence
Oxford Handbook of Psychiatry . 2nd Edition .
David Semple & Roger Smyth
Management of Mood Disorders During Pregnancy .
Dr Magda Fahmy

Discussion