Medications in Pregnancy and Lactation - University of … in pregnancy 1.pdf · Medications in...
23
Clinical Expert Series Continuing medical education is available online at www.greenjournal.org Medications in Pregnancy and Lactation Part 1. Teratology Catalin S. Buhimschi, MD, and Carl P. Weiner, MD, MBA One of the least-developed areas of clinical pharmacology and drug research is the use of medication during pregnancy and lactation. This article is the first in a two-part series designed to familiarize physicians with many aspects of the drugs they commonly prescribe for pregnant and breast-feeding women. Almost every pregnant woman is exposed to some type of medication during pregnancy. Although the majority of pregnant and breast-feeding women consume clinically indicated or over-the- counter drug preparation regularly, only few medications have specifically been tested for safety and efficacy during pregnancy. There is scant information on the effect of common pregnancy complications on drug clearance and efficacy. Often, the safety of a drug for mothers, their fetuses, and nursing infants cannot be determined until it has been widely used. Absent this crucial information, many women are either refused medically important agents or experience potentially harmful delays in receiving drug treatment. Conversely, many drugs deemed “safe” are prescribed despite evidence of possible terato- genicity. Novel research and diagnostic applications evolving from the opportunities presented by the advances in genomics and proteomics are now beginning to affect clinical diagnosis, vaccine develop- ment, drug discovery, and unique therapies in a modern diagnostic–therapeutic framework—part of the new scientific field of theranostics. This review critically explores a number of recently raised issues in regard to the use of several classes of medications during gestation and seeks to provide a general and concise resource on drugs commonly used during pregnancy and lactation. It also seeks to make clinicians more aware of the controversies surrounding some drugs in an effort to encourage safer prescribing practices through consultation with a maternal–fetal medicine specialist and through references and Web sites that list up-to-date information. (Obstet Gynecol 2009;113:166–88) D rug therapy is an integral part of the health care system. Almost every pregnant woman is ex- posed to some type of medication during pregnancy. When prescribed to pregnant and breast-feeding women, many drugs can exercise a teratogenic effect on fetuses and nursing infants; therefore, rigorous investigation into commonly prescribed drugs is es- sential. Although the majority of pregnant and breast- feeding women consume clinically indicated or over- the-counter drug preparation regularly, only few medications have specifically been tested for safety and efficacy during pregnancy. Current methods to assess teratogenicity consist mainly of pregnancy reg- istries and case– control surveillance studies; how- ever, these practices have proven insufficient to de- termine drug safety accurately. This insufficiency is due, in part, to shortcomings in the design of the studies. Physicians are therefore typically dependent on inaccurate or outdated information in prescribing medication. Even the U. S. Food and Drug Adminis- From the Department of Obstetrics, Gynecology and Reproductive Science, Yale University School of Medicine, New Haven, Connecticut; and Department of Obstetrics and Gynecology, University of Kansas School of Medicine, Kansas City, Kansas. The authors thank Kelly Horvath, MA, for her assistance with the writing and editing of the manuscript. Corresponding author: Catalin S. Buhimschi, MD, Director, Perinatal Re- search, Department of Obstetrics, Gynecology and Reproductive Sciences, Yale University School of Medicine, 333 Cedar Street, LLCI 804, New Haven, CT 06520; e-mail: [email protected]. Financial Disclosure The authors did not report any potential conflicts of interest. © 2008 by The American College of Obstetricians and Gynecologists. Published by Lippincott Williams & Wilkins. ISSN: 0029-7844/08 166 VOL. 113, NO. 1, JANUARY 2009 OBSTETRICS & GYNECOLOGY
-
Upload
phungtuyen -
Category
Documents
-
view
220 -
download
0
Transcript of Medications in Pregnancy and Lactation - University of … in pregnancy 1.pdf · Medications in...

Clinical Expert Series
Continuing medical education is available online at www.greenjournal.org
Medications in Pregnancy and LactationPart 1. Teratology
Catalin S. Buhimschi, MD, and Carl P. Weiner, MD, MBA
One of the least-developed areas of clinical pharmacology and drug research is the use of medicationduring pregnancy and lactation. This article is the first in a two-part series designed to familiarizephysicians with many aspects of the drugs they commonly prescribe for pregnant and breast-feedingwomen. Almost every pregnant woman is exposed to some type of medication during pregnancy.Although the majority of pregnant and breast-feeding women consume clinically indicated or over-the-counter drug preparation regularly, only few medications have specifically been tested for safety andefficacy during pregnancy. There is scant information on the effect of common pregnancy complicationson drug clearance and efficacy. Often, the safety of a drug for mothers, their fetuses, and nursing infantscannot be determined until it has been widely used. Absent this crucial information, many women areeither refused medically important agents or experience potentially harmful delays in receiving drugtreatment. Conversely, many drugs deemed “safe” are prescribed despite evidence of possible terato-genicity. Novel research and diagnostic applications evolving from the opportunities presented by theadvances in genomics and proteomics are now beginning to affect clinical diagnosis, vaccine develop-ment, drug discovery, and unique therapies in a modern diagnostic–therapeutic framework—part of thenew scientific field of theranostics. This review critically explores a number of recently raised issues inregard to the use of several classes of medications during gestation and seeks to provide a general andconcise resource on drugs commonly used during pregnancy and lactation. It also seeks to make cliniciansmore aware of the controversies surrounding some drugs in an effort to encourage safer prescribingpractices through consultation with a maternal–fetal medicine specialist and through references and Websites that list up-to-date information.(Obstet Gynecol 2009;113:166–88)
Drug therapy is an integral part of the health caresystem. Almost every pregnant woman is ex-
posed to some type of medication during pregnancy.
When prescribed to pregnant and breast-feedingwomen, many drugs can exercise a teratogenic effecton fetuses and nursing infants; therefore, rigorousinvestigation into commonly prescribed drugs is es-sential. Although the majority of pregnant and breast-feeding women consume clinically indicated or over-the-counter drug preparation regularly, only fewmedications have specifically been tested for safetyand efficacy during pregnancy. Current methods toassess teratogenicity consist mainly of pregnancy reg-istries and case–control surveillance studies; how-ever, these practices have proven insufficient to de-termine drug safety accurately. This insufficiency isdue, in part, to shortcomings in the design of thestudies. Physicians are therefore typically dependenton inaccurate or outdated information in prescribingmedication. Even the U. S. Food and Drug Adminis-
From the Department of Obstetrics, Gynecology and Reproductive Science, YaleUniversity School of Medicine, New Haven, Connecticut; and Department of Obstetricsand Gynecology, University of Kansas School of Medicine, Kansas City, Kansas.
The authors thank Kelly Horvath, MA, for her assistance with the writing andediting of the manuscript.
Corresponding author: Catalin S. Buhimschi, MD, Director, Perinatal Re-search, Department of Obstetrics, Gynecology and Reproductive Sciences, YaleUniversity School of Medicine, 333 Cedar Street, LLCI 804, New Haven, CT06520; e-mail: [email protected].
Financial DisclosureThe authors did not report any potential conflicts of interest.
© 2008 by The American College of Obstetricians and Gynecologists. Publishedby Lippincott Williams & Wilkins.ISSN: 0029-7844/08
166 VOL. 113, NO. 1, JANUARY 2009 OBSTETRICS & GYNECOLOGY

tration (FDA) drug classifications suffer from inaccura-cies and inconsistencies. Detailed supplemental druginformation and new strategies for testing and research,such as those being developed in the new field oftheranostics, are critical to safe drug practices. Investiga-tions into how and why current drug information and, inturn, prescribing practices are inadequate are presentedhere in addition to a summary of the existing evi-dence—or lack thereof—on many potentially teratogenicdrugs commonly prescribed for pregnant and breast-feeding women.
TERATOGENSTeratogens are agents that act to irreversibly altergrowth, structure, or function of the developing em-bryo or fetus. Recognized teratogens include viruses(eg, rubella, cytomegalovirus, congenital lymphocyticchoriomeningitis virus), environmental factors (eg,hyperthermia, irradiation), chemicals (eg, mercury,alcohol), and therapeutic drugs (eg, inhibitors of therenin–angiotensin system, thalidomide, isotretinoin,warfarin, valproic acid, carbamazepine).1
Most drugs reach the fetus by the maternalbloodstream; thus embryonic and fetal exposure de-pends on several critical factors, such as gestationalage, route of administration, absorption of the drug,the dose of the drug medication, maternal serumlevels, and the maternal and placental clearancesystem. Placental passage to the embryo or fetus isnecessary for a drug medication to exercise its specificteratogenic effect. In turn, placental transfer dependsgreatly on maternal metabolism, gestational age, pro-tein binding and storage, charge, liposolubility of thedrug, and molecular size.2 Molecular weight of asubstance is an important regulator of its transplacen-tal passage. Previous studies have shown that mostsubstances with mass below 500 Da diffuse rapidlyacross the placental barrier, whereas agents of highermolecular weight demonstrate more variable trans-placental migration rates. Ionization and high fatsolubility (eg, in anesthetic gases) assures rapid trans-fer of these drugs by simple diffusion.3 Lastly, varia-tions in pH gradients between maternal and conceptalcompartments play an important role as well (Fig. 1).
CRITICAL DEVELOPMENTAL PERIODAn agent is recognized as a human teratogen if itmeets certain criteria. A comprehensive review of theconditions necessary to prove teratogenicity of anagent is in the most recent work of Shepard andRonald.4 The criteria include 1) proven exposure atcritical times during human development; 2) consis-tent dysmorphic findings recognized in well-con-
ducted epidemiologic studies; 3) specific defects orsyndromes associated consistently with specific ter-atogens; 4) rare anatomic defects associated withenvironmental exposure (eg, facial dysmorphologismand nail hypoplasia with carbamazepine); 5) proventeratogenicity in experimental animal models.
To cause a birth defect, a teratogen acts duringcritical periods of embryonic or fetal development;thus, teratogenic drug medications can either induceembryopathy or fetopathy. From the perspective of tera-togenesis, human gestation is divided into three peri-
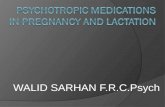
Fig. 1. Representative pictures of a fetus with methotrexateembryopathy. A. Postmortem examination of the fetusshowed craniofacial abnormalities, including a wide ante-rior fontanelle, low-set and poorly formed ears, absentauditory canals, flat nose, cleft lip, and micrognathia. B.Examination of the body showed shortened forearms, hyp-oplastic thumbs, clinodactyly, brachydactyly of the fifthdigit, and pelvic and lower limb abnormalities.Buhimschi. Medications in Pregnancy and Lactation. ObstetGynecol 2009.
VOL. 113, NO. 1, JANUARY 2009 Buhimschi and Weiner Medications in Pregnancy and Lactation 167

ods: preimplantation (fertilization to implantation), em-bryonic (second through ninth week), and fetal (ninthweek to term). The preimplantation period is tradi-tionally viewed as a gestational window characterizedby an “all or nothing” phenomenon: During earlymammalian embryo development, injury to a largenumber of cells will predictably cause an embryonicloss. If only a small number of cells are disrupted, aphenomenon called compensation can protect the em-bryo and facilitate survival without malformation.5
A teratogenic agent can cause malformation dur-ing organogenesis (2 to 8 weeks postconception), wheneach system has a period of maximum vulnerability (eg,the heart is mostly affected if the teratogen acts between6.5 weeks to 8 weeks of gestation). However, the fetuscan also be affected by alterations in structure andfunction of the organs that have initially developednormally during embryogenesis. For example, spinabifida, anencephaly, and encephalocele arise due to thefailure of closure of the neural tube during the process ofneurulation (17th through 30th postfertilization days).Still, neural tube defects (eg, encephaloceles) may alsooccur postclosure during the fetal period.6
Many potent human teratogens act during veryspecific developmental stages. For instance, it was longbelieved that angiotensin-converting enzyme (ACE) in-hibitors (eg, captopril, enalapril) had no adverse effectsduring the first trimester and that only a late exposure(second or third trimester) was associated with renal andcardiac malformations.7 However, a more recent analy-sis of a large cohort of neonates exposed to ACEinhibitors during gestation disputes the safety of first-trimester exposure to this class of medication, indicatingthat ACE inhibitors can induce malformations through-out gestation.8 Likewise, nonsteroidal antiinflammatorydrugs (NSAIDs) (eg, indomethacin, ibuprofen) are asso-ciated with gastroschisis and other fetal sequelae if theembryo is exposed during early gestation, whereas irre-versible closure of the ductus and kidney failure can occurif the fetus is exposed to NSAIDs after 32 weeks.
ASSESSMENT OF DRUG TERATOGENICITYTeratology is the study of the biologic mechanismsand causes of abnormal human development and theadvancement of preventive strategies.1 The finding ofa birth defect should always raise the question ofwhether it was the consequence of a genetic defector if it was the result of prenatal exposure to ateratogen. Recognition of a teratogenic drug afterwidespread use always causes worry about “failures ofthe system.”9 Unfortunately, scientists, physicians,patients, and policy-makers are commonly reassuredthat the most serious short-term adverse effects of a
drug are identified in premarketing studies. Regretta-bly, although approval of a drug requires comprehen-sive animal studies, such models are seriously limitedin their ability to predict human teratogenesis becauseof variations in species-specific effects even betweenmammalian species.2 The unfortunate reality is thatwe learn about virtually all human teratogenic effectsonly after a drug has received marketing approval bythe FDA. Teratogens commonly go undetected in thehuman trials conducted before FDA approval be-cause most studies are small and routinely excludepregnant women, particularly if there is any suspicionthat a drug might be teratogenic.
PREGNANCY REGISTRIES ANDCASE–CONTROL SURVEILLANCE STUDIESPregnancy registries and case–control surveillancestudies are currently the two main methods used toidentify teratogens.9 Pregnancy registries are routinelydeveloped to permit identification of drugs that arehigh-risk teratogens. Because pregnancy registries aretypically operated by drug manufacturers and be-cause patients receive multiple drugs or are recruitedinto multiple, uncoordinated registries, however, con-cerns have been raised with regard to their accuracy.Inclusion of an adequate number of exposed pregnan-cies, thorough long-term follow-up, and complete andaccurate ascertainment of pregnancy outcome arecritical attributes of a well-designed registry.10 Physi-cians can access the most up-to-date list of pregnancyexposure registries by consulting the FDA Web site(http://www.fda.gov/womens/registries/).
Case–control surveillance studies provide an-other tool to identify serious illnesses caused bymedications used in an outpatient population.11 Byincluding information on infants with a wide range ofbirth defects and interviews with mothers focusing ondetails of their antenatal exposure to all prescriptionand over-the-counter medications (including herbalproducts), case–control surveillance studies can pro-vide the required opportunity to examine large num-bers of specific defects in relation to the wide range ofmedications taken by pregnant women.1
BREAST-FEEDINGBreast-feeding is beneficial for the health of mother andchild.12 However, many therapeutic and environmentalsubstances can be transferred into breast milk, com-monly causing the risk of breast-feeding to exceed itsbenefit to the infant, mother, or both.13 Very few med-ications are as yet contraindicated for breast-feeding.14
There is still scant information on the risk of mostmedications used in human pregnancy and lactation at
168 Buhimschi and Weiner Medications in Pregnancy and Lactation OBSTETRICS & GYNECOLOGY

the time they receive their FDA approval and are initiallymarketed.15 The dose of a drug an infant receives duringbreast-feeding depends on the amount excreted into thebreast milk, the daily volume of milk ingested, and theaverage plasma concentration of the mother. The milk-to-plasma concentration ratio has large intersubject andintrasubject variability. The transfer of medications acrossthe basal membrane of the mammary gland alveolidepends on lipophilicity and protein binding and on thedegree of substance ionization.
Very few studies have investigated drug concen-trations in breast milk.16 To determine exposure of thebreast-fed neonate to a specific drug, the weight-corrected percent of the maternal dose ingested by anunsupplemented newborn and the resulting neonatalblood levels is used. Unfortunately, these data arereported for few agents. The milk:maternal plasmaratio conveyed to the clinician can be misleadingbecause it commonly disregards the quantity ingestedand its oral bioavailability.
Research into environmentally related chemicalcontaminants in breast milk is an increasingly impor-tant field of research.17 These pollutants can remain inthe human body for decades and thus pose a risk forboth mother and her unborn child even in theabsence of recent exposure. For example, diet is onemajor factor influencing breast milk levels of organicpollutants (eg, mercury in fish).18 Furthermore, the
types of and extent to which medications (eg, moodstabilizers) are used by breast-feeding women havenot been thoroughly investigated.19 Existing literatureconsists essentially of case reports with few attempts atlongitudinal investigation.20 Findings are often diffi-cult to compare because of discrepant research meth-odologies or the lack of key pharmacologic or phar-macokinetic information. The most data available arefor the tricyclic antidepressants, but reports includefewer than 100 mother–infant pairs even for this group.
Dilemmas about whether to prohibit breast-feedingwhen the mother is undergoing drug therapy regularlyarise. Because the relationship between medication useduring pregnancy and lactation has been insufficientlyinvestigated, acute attention should be paid to any drugwhich is recommended postpartum.21 Studies designedto quantify the amount of drug passed to the neonateand provide clinically reliable recommendations basedon infant clearance, which is itself dependent on theontogeny of elimination pathways and pharmacogenet-ics, are critically needed.
U.S. FOOD AND DRUG ADMINISTRATIONDRUG RISK CLASSIFICATION INPREGNANCYPhysicians routinely rely almost exclusively on FDAclassification (A, B, C, D, or X) (Table 1) to make a
Table 1. U.S. Food and Drug Administration Drug Classification System
FDA Category* Pregnancy Category Definition
A Controlled studies showed no risk to humansAdequate, well-controlled studies in pregnant women have not shown an increased risk of fetal abnormalities
B No evidence of risk in humansAnimal studies have revealed no evidence of harm to the fetus. However, there are no adequate and well-
controlled studies in pregnant womenorAnimal studies have shown an adverse effect, but adequate and well-controlled studies in pregnant women
have failed to demonstrate a risk to the fetus
C Risks cannot be ruled out in humansAnimal studies have shown an adverse effect and there are no adequate and well-controlled studies in
pregnant womenorNo animal studies have been conducted and there are no adequate and well-controlled studies in pregnant
women
D Clear evidence of risk in humansStudies, adequate well-controlled or observational, in pregnant women have demonstrated a risk to the fetus.
However, the benefits of therapy may outweigh the potential risk
X Drugs contraindicated in human pregnancyStudies, adequate well-controlled or observational, in animals or pregnant women have demonstrated positive
evidence of fetal abnormalities. The use of the product is contraindicated in women who are or maybecome pregnant
FDA, U.S. Food and Drug Administration.* Please verify the FDA categorization for each drug.
VOL. 113, NO. 1, JANUARY 2009 Buhimschi and Weiner Medications in Pregnancy and Lactation 169

decision to initiate, continue, discontinue, or replace amedication. This reliance is, unfortunately, mis-placed. Although only few drugs are known orstrongly suspected to be teratogens, the majority of alldrugs marketed in the U.S. are classified CategoryC—risks cannot be ruled out in humans but thebenefits of the medication may outweigh the potentialrisks—and less than 1% are Category A—no risk tohumans. And although major congenital abnormali-ties complicate 2–3% of all pregnancies, fewer than10% of these can be associated with a particular drugexposure, possibly due in part to the lack of reliabledrug information. Inexplicably, some Category Xdrugs—clear evidence that the medication causes ab-normalities in the fetus—are not absolutely contrain-dicated during pregnancy, and several Category C orD drugs are either known human teratogens or com-monly have serious adverse fetal effects.14
Out of 2,150 products searched in the 2002 Physi-cians’ Desk Reference (Thomson Healthcare, Montvale,NJ), a widely used source of drug information by U.S.clinicians and patients, only 124 drugs were classified aspregnancy Category X.22 Yet, about one in every fivewomen uses FDA C, D, and X drugs at least once duringpregnancy. The most common prescription drugs inpregnancy are antiasthmatics, antibiotics, NSAIDs, anx-iolytics, antidepressants, and oral contraceptives.23 Table2 shows a list of the most common drugs or drug groups(in alphabetical order) known or strongly suspected tocause developmental defects. Because of the extensive-ness of the subject, only the drug medications believedto be most commonly encountered in routine clinicalpractice are presented.
After review of the label/package insert for eachCategory X drug to identify risk management strate-gies for pregnancy prevention, it was concluded that1) the majority of the labels included only a black boxwarning and/or a contraindication for use in womenwho are or may become pregnant; 2) only 13 drugscontained specific pregnancy prevention risk-man-agement strategies in the label to direct the clinicianand/or patient (eg, on frequency of pregnancy testingand number and type of contraception methods); 3)only three drugs (isotretinoin, acitretin, and thalido-mide) had formal pregnancy prevention risk-manage-ment programs. This analysis demonstrates an urgentneed both for consistency in the classification ofpregnancy Category X products and for the recom-mendation of pregnancy prevention risk-manage-ment strategies included in their classification andlabels. Pregnancy risk categories have currentlyproven suboptimal, outdated, and too superficial toaccount for the physiology and health care needs of
pregnant and breast-feeding women. They arerarely or too hastily revised as new informationbecomes available. The common result is confusionamong clinicians about whether to prescribe certaindrugs.
To ensure that the information included in thissummary of teratogenic medication commonly pre-scribed to pregnant and breast-feeding women isevidence-based, the research strategy included com-puterized bibliographic searches of MEDLINE(1966–2008), PubMed (1966–2008), and referencesof published articles. Meta-analysis studies were in-cluded only if the guidelines of the Meta-analysis ofObservational Studies in Epidemiology Group wereappropriately applied. Additionally, the AmericanCollege of Obstetrics and Gynecology CommitteeOpinion and Practice Bulletins were used as a refer-ence when relevant. For clinical relevance, tradenames for commonly used drugs are also included.See Table 3.
Table 2. Commonly Prescribed TeratogenicDrugs*
DrugFDA
Classification†
Agents acting on renin–angiotensinsystem (captopril, lisinopril,enalapril)
C (first trimester)D (second andthirdtrimesters)
Antidepressants (paroxetine) DAntiepileptic drugs (valproic acid,
carbamazepine, phenytoin)D
Anxiolytics (diazepam) DAlkylating agents (cyclophosphamide) DAndrogens (danazol) XAntimetabolites (methotrexate) D, XCarbimazole DCoumarin derivatives (warfarin) XEstrogens (diethylstilbestrol) XFluconazole CLithium DMisoprostol XOral contraceptives XPenicillamine DRetinoids (isotretinoin) XRadioactive iodine (sodium iodide-
128)X
Thalidomide X
FDA, U.S. Food and Drug Administration.Data from Buhimschi CS, Weiner CP. Medications in pregnancy
and lactation. In: Queenan JT, Spong CY, Lockwood CJ,editors. Management of high-risk pregnancy: an evidence-based approach. 5th ed. Malden (MA): Blackwell PublishingLtd.; 2007. p. 38–58.
* Drugs or drug groups known or strongly suspected to causedevelopmental defects and their pregnancy safety categoriza-tion (see Table 1 for an explanation of the safety categories).
† Please verify the FDA categorization for each drug.
170 Buhimschi and Weiner Medications in Pregnancy and Lactation OBSTETRICS & GYNECOLOGY

Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
ACE inhibitorsEnalapril (Vasotec) Captopril
(Capoten, Lopurin)Lisinopril (Prinivil, Zestril)
• Contraindicated inpregnancy.
• No adequate reports or well-controlled studies of thesedrugs in pregnant women.
• May be indicated for thecontrol of severehypertension in extremelyrare cases when the patientis refractory to othermedications.24,25
• If mothers must take thesedrugs, close consultationwith a cardiologist or anephrologist and serialmonitoring of amniotic fluidand fetal well-being isrecommended.26
• Should be discontinuedimmediately ifoligohydramnios is detected,unless lifesaving for themother.
• Recent information reveals ateratogenic risk for theseagents.27
• Crosses humanplacenta.28,29,30
• Formerly believed thatexposure in the firsttrimester was safe; exposurein the 2nd and 3rdtrimesters was associatedwith oligohydramnios,hypocalvaria, anuria, renalfailure, patent ductusarteriosus, aortic archobstructive malformations,and death.31,32,33
• More recent studies showthat even in the firsttrimester, the fetus has anincreased risk formalformations of thecardiovascular (atrial septaldefect, pulmonic stenosis,atrial and ventricular defect)and the CNS (microcephaly,eye anomaly, spina bifida,coloboma) systems.
• Accuracy of recent studies islimited by the relativelysmall number of fetusesincluded in the final analysisand their retrospectivedesign.
• Extreme caution andavoidance of ACE inhibitorsin the first trimester, ifpossible, is recommended.
• Antenatal surveillanceshould be initiated ifinadvertent exposure occurs.
• Oligohydramnios may notappear until afterirreversible renal injury.
• Neonates exposed in uteroshould be observed closelyfor hypotension, oliguria,and hyperkalemia.
• Considered compatiblewith breast-feeding.
• Enalapril and captoprilfound in breast milk,although the kineticsremain to be clarified.34,35
• Still unknown if lisinoprilenters breast milk soinfants should bemonitored for possibleadverse effects, the lowesteffective dose should berecommended to themother, and breast-feeding avoided at timesof peak maternal druglevels.
AntidepressantsWhole category (fluoxetine,
sertraline, paroxetine)• Because depression is
prevalent and commonlyunrecognized, universalscreening is recommendedat the time of first prenatalvisit, each trimester, andpostpartum.36,37
• SSRIs cross the humanplacenta.40,41,42,43
• Not contraindicated.49
(continued)
VOL. 113, NO. 1, JANUARY 2009 Buhimschi and Weiner Medications in Pregnancy and Lactation 171

Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen (continued)
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
Whole category (fluoxetine,sertraline, paroxetine)(continued )
• Pregnancy is not necessarilya reason to discontinuepsychotropic drugs.38
• Discontinuation ofmedication exchanges therisks of embryopathy orfetopathy for the risks ofuntreated illness: pretermbirth, IUGR, and STDs dueto potential for engagementin high-risk sexual behavior.
• In general, women takingSSRIs during pregnancyrequire an increased dose tomaintain euthymia.39
• Team comprisingpsychiatrist and obstetricianshould decide on necessityof continuing treatment anddiscuss all risks withmother.36,.37
• Evidence ofteratogenicity40,41,42,43;appraisal of risk is notunanimous.44
• Not considered majorteratogens.
• Exposure to SSRIs duringearly pregnancy is likelyassociated with an increasedrisk of cardiac defects(especially after paroxetineexposure).
• The absolute risk is smalland generally not greaterthan 2/1,000 births butcaution should be used,especially with paroxetine.
• Possible association betweenSSRIs use during gestationand newborn persistentpulmonary hypertension.45
• Late exposure is linked withtransient neonatalcomplications includingjitteriness, mild respiratorydistress, transient tachypnea ofthe newborn, weak cry, poortone, and neonatal intensivecare unit admission.46,47,48
• Infant should bemonitored for possibleadverse effects, the druggiven at the lowesteffective dose, and breast-feeding avoided at timesof peak drug levels.
• Most psychotropicmedications aretransferred to breast milkin varying amounts, andthus potentially passedon to the nursing infant.
• Discarding breast milkobtained at the time ofpeak drug concentrationcould allow the motherto reduce the infant’sexposure to hermedication; however, thisis often impractical todo.49
Fluoxetine (Prozac,Sarafem)
• Effective for postpartumdepression.50
• Fluoxetine crosses thehuman placenta.
• Not considered a teratogen.
• Maternal serum and peakbreast milkconcentrations predictnursing infant serumconcentrations.
Sertraline (Zoloft, Lustral) • Lacks adequate reports orwell-controlled studies ofpregnant women.
• There is growing experiencewith its use for the treatmentof postpartum depression.50
• Associated with omphaloceleand atrial and ventricularseptum defects.51
• Present in the humanmilk.
• The neonate should bemonitored for possibleadverse effects, the druggiven at the lowesteffective dose, and breast-feeding avoided at timesof peak drug levels.
Paroxetine (Paxil) • Recent investigations suggestan increased risk of congenitalmalformations after exposurein the first trimester:52
1) Number of subjects wassmall and the conclusionsderived subsequent to alarge number of statisticalanalyses.
2) Manufacturer changedFDA classification from Cto D (see Table 1).
• 1.5-fold to twofold increasedrisk of congenital cardiacmalformations (atrial andventricular septal defects)after first trimesterexposure. 40,41,42,43
• Associated with rightventricular outflow defects.51
• Associated withanencephaly,craniosynostosis, andomphalocele.44
• Limited data suggest thatparoxetine is notdetectable in theneonates who areexclusively breast-fed.53
(continued)
172 Buhimschi and Weiner Medications in Pregnancy and Lactation OBSTETRICS & GYNECOLOGY

Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen (continued)
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
Paroxetine (Paxil)(continued )
• Should be avoided duringgestation and in womenplanning pregnancy.37
AnticonvulsantsWhole category (valproic
acid, carbamazepine,phenytoin,lamotrigine)
• Approximately 500,000 U.S.women require psychiatriccare, commonly involvingthese drugs.37
• Recommended to switch to30–35 micrograms estrogenoral contraception if takinganticonvulsants and wish toavoid pregnancy.37
• Negatively affect reliabilityof oral contraceptives,especially carbamazepineand phenytoin54 but withpossible exception ofvalproic acid.55
• Patients planningpregnancy should becounseled on the risks andthe importance ofpericonceptual folate.supplementation (4 mg/d).56
• Goal to avoid generalizedtonic-clonic seizures withminimized risk to fetus.
• Monotherapy (at a higherdose if necessary) is preferableto multidrug regimen.37
• Results indicate that the riskof congenital abnormalitiesin children exposed in uterois reduced but noteliminated by folic acidsupplementation at 5–12 wkfrom the last menstrualperiod.57
• Breast-feeding infantsshould be monitored forpossible adverse effectsand the drug given at thelowest effective dose.
• Breast-feeding should beavoided at times of peakdrug levels.
Valproic acid (Depakene) • No adequate or well-controlled studies.
• Known human teratogen.58,59
• Rapidly transported acrosshuman placenta reaching afetal:maternal ratio greaterthan double.60
• Risk to fetus is dose-dependentand compounded by lowserum folate.57
• Enters breast milk.• Neonatal serum
concentration levels reachless than 10% of maternallevels.64
• “Valproate syndrome”includes distinct craniofacialappearance, limbabnormalities, heart defects,a cluster of minor and majoranomalies, and CNSdysfunction.61,62
• Impairments may bediagnosed in utero with anincreased nuchaltranslucency measurement.63
• After delivery, 10% diein infancy; 1/4 hasdevelopmental deficits ormental retardation.
(continued)
VOL. 113, NO. 1, JANUARY 2009 Buhimschi and Weiner Medications in Pregnancy and Lactation 173

Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen (continued)
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
Carbamazepine (Tegretol,Atretol, Convuline,Epitol)
• Used for epilepsy andbipolar disorders.
• Well-known teratogen.65
• Crosses human placenta.• “Carbamazepine syndrome”
includes facial dysmorphism,developmental delay, spinabifida, and distal phalangeand fingernailhypoplasia.66,67
• Excreted in breast milk.• Limited data suggests that
breast-feeding whiletaking this drug isgenerally safe.
• Rarely, neonatalcholestatic hepatitis hasbeen reported.68
Phenytoin (Dilantin,Aladdin, Dantoin)
• Stable serum levelsachievable duringpregnancy69:1) Low levels could be due
to patient noncomplianceor to hypermetabolism.
2) High levels can resultfrom hepatic disease,congenital enzymedeficiency, or other drugsthat interfere with itsmetabolism.
3) To reduce the risk ofseizure, dose adjustmentsshould be based onclinical symptoms ratherthan on serum drugconcentrations.
• May impair effect ofcorticosteroids, coumarin,digitoxin, doxycycline,estrogens, furosemide, oralcontraceptives, quinidine,rifampin, theophylline, andvitamin D.70
• Specifically associated withcongenital heart defects andcleft palate.71
• Monotherapy and the lowesteffective quantity given individed doses to lower thepeaks can theoreticallyminimize the risks.72
• Transfer to breast milk islow.
• Considered safe forbreast-feeding.73
Lamotrigine (Lamictal) • No adequate or well-controlled studies.
• Used for epilepsy andbipolar disorders.74
• May experience increasedrisk of seizures in absence oflevel monitoring.75,76
• Crosses human placenta.• Fetal exposure has not been
documented to increase therisk of major anomalies.77
• Transfer to breast milk islow.
• Considered safe forbreast-feeding.73
Anxiolytics (benzodiazepines)Diazepam (Valium) • No adequate or well-
controlled studies.• Drug prescribed for anxiety
disorders including a varietyof psychiatric conditions:panic disorders, generalizedanxiety disorders,posttraumatic stress disorder,social anxiety, and phobias:Collectively, anxiety disorderscomprise the most commonpsychiatric conditions with aprevalence of approximately18% in the U.S.78
• No evidence of significantrisk of teratogenicity.
• Rapidly crosses humanplacenta.85
• Overall results arereassuring, revealing noadverse effects onneurodevelopment.
• Some studies show increasedrisk of oral clefts with firsttrimester exposure.†
• Excreted in breast milk.• Maximum neonatal
exposure is estimated atonly 3% of maternaldose.87
(continued)
174 Buhimschi and Weiner Medications in Pregnancy and Lactation OBSTETRICS & GYNECOLOGY

Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen (continued)
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
Anxiolytics (benzodiazepines)Diazepam (Valium)
(continued )• May be beneficial adjunct to
IV fluids and vitamins fortreating hyperemesisgravidarum.79
• Useful anxiolytic for womenundergoing fetal therapyprocedures because it causesdecreased fetal movement.
• Used for prophylaxis andtreatment of eclampticconvulsions.
• Clinical efficacy was provenless than that of magnesiumsulfate, and thus it is notcurrently recommended asfirst line therapy.80,81,82
• Initial findings have not beenconfirmed by long-termfollow-up studies.83,84
• Shortest course and lowestdose should be used whenindicated.
• Prolonged CNS depressioncan occur, with symptomsincluding mild sedation,hypotonia, reluctance tosuck, apneic spells, cyanosis,impaired metabolicresponses to stress, “floppyinfant” syndrome, andmarked neonatal withdrawalthat can persist for hours tomonths after birth.86
• Special attentionshould be paid to thepremature neonate orif the maternal dose isparticularly high.
Alkylating agentsCyclophosphamide
(Cytoxan)• Integral part of the multi-
agent regimens used totreat cancer of the ovary,breast, blood and lymphsystems.
• Transient sterility andsecondary malignancy arethe most commoncomplications of treatment.
• Case reports suggest thatthis drug can be used withgood pregnancyoutcome.88,89
• Crosses human placenta.• Neonatal hematologic
suppression and secondarymalignancies have beenreported.90,91
• In utero exposure findingsinclude growth deficiency,high-arched palate,microcephaly, flat nasalbridge, syndactyly, andfinger hypoplasia.92,93
• Not compatible withbreast-feeding.
• Enters breast milk inhigh concentrations.
• Commonly causesneonatalneutropenia.94,95
Hormones/androgensWhole category
(methyltestosterone,medroxyprogesteroneacetate, danazol)
• Insufficient data to quantifyrisk in humans; however,some reports reveal thatsynthetic progestins causemild virilization of femaleexternal genitalia.96,97
• First trimester exposure isan indication for a detailedanatomic ultrasoundbetween 18–22 wk ofgestation.
—
Methyltestosterone(Adoral, Testred)
• Recommended forendometriosis and palliationwith inoperable breastcancer.
• Unknown if crosses humanplacenta.
• In animal studies,pseudohermaphroditismresults in female fetuses; inmales, an increased risk ofhypospadias.99,‡
• Unknown if entersbreast milk.
• Excreted in breastmilk in smallamounts.
Medroxyprogesteroneacetate (Depo-Provera,Med-Pro, Provera)
• Some recommend incombination with estrogensfor libido enhancement.98
• No evidence of significantrisk of teratogenicity.
• Does not suppresslactation or adverselyaffect neonate.100,101
(continued)
VOL. 113, NO. 1, JANUARY 2009 Buhimschi and Weiner Medications in Pregnancy and Lactation 175

Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen (continued)
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
Medroxyprogesteroneacetate (Depo-Provera,Med-Pro, Provera)(continued )
• Prescribed to prevent firsttrimester spontaneousabortion:1) No well-conducted
studies to substantiatethis claim.
2) No demonstrableincrease in ectopicpregnancy aftertreatment.
• In utero exposure of malefetuses to progestationalagents apparently doublesthe risk of hypospadias.
• Typically given forcontraception 3 d afterdelivery sinceprogesteronewithdrawal may beone stimulus for theinitiation oflactogenesis.
Danazol (Danocrine,Danatrol)
• Considered effective forendometriosis.102
• Not an effectivecontraceptive and should bediscontinued immediately ifpatient becomes pregnant.
• No indications duringpregnancy.
• Unknown if crosses humanplacenta.
• Classified as Category X.• Not always necessary to
terminate an exposed fetus.• Can have androgenic effect
on female fetuses, includingvaginal atresia, clitoralhypertrophy, labial fusion,and ambiguousgenitalia.103,104
• Unknown if entersbreast milk.
• Contraindicated duringbreast-feeding.
AntimetabolitesMethotrexate (Folex,
Mexate, Rheumatrex,Tremetex)
• Commonly recommendedto treat ectopic pregnancy,neoplastic disease,autoimmune disorders, andinflammatory conditions(Crohn’s disease,rheumatoid arthritis).105
• Considered an efficientmedical abortifacient ofintrauterine pregnancy whencombined withmisoprostol.106,107
• Ectopic pregnancy: Afteradministration, women mustbe clinically tested untilthere is completenormalization of their serum�-hCG titers.108,109
• First trimester exposureresults in an increased riskof fetal malformations,including craniofacial, axialskeletal, cardio-pulmonary,and gastrointestinalabnormalities (Fig. 1) anddevelopmental delay.110,111
• Most pregnancies exposed tolow doses are not adverselyaffected.110,111
• Even single doses used inmedical termination ofpregnancy are associatedwith multiple congenitalanomalies.112
• Exposure later in pregnancyseems to be safe.94
• Unknown if entersbreast milk.
• Views vary on safetybut the drug isgenerallycontraindicated innursing mothers.113
• Women with rheumatoidarthritis commonly experiencea disease flare within 3 mo ofdelivery and drug treatment isrequired.
AntithyroidsWhole category
(propylthiouracil,methimazole)
• During gestation, womenwith hyperthyroidismshould have their thyroidfunction checked every 3–4wk.
• Graves’ disease represents themost common cause ofmaternal hyperthyroidismduring pregnancy.
• Fetal reaction is oftenunpredictable and differentthan the maternal response.
• No deleterious effectson neonatal thyroidfunction or on physicaland intellectualdevelopment of breast-fed infants have beendescribed.118,119
(continued)
176 Buhimschi and Weiner Medications in Pregnancy and Lactation OBSTETRICS & GYNECOLOGY

Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen (continued)
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
AntithyroidsWhole category
(propylthiouracil,methimazole)(continued)
•There is general consensusamong clinicians that thelowest dose needed tokeep T3 and T4 within theupper normal range forthese women should beused.114,115
• Because women previouslyablated with eitherradioactive iodine orthyroidectomy may stillbe producing thyroid-stimulating antibodies(even though they arethemselves euthyroid), thefetus remains at risk andshould be monitored withserial ultrasonography forgrowth and early detection ofgoiter.116,117
Propylthiouracil • First-line treatment forGraves’ disease inpregnancy due tolower risks thanmethimazole.120,121,122
• Crosses the humanplacenta.
• Associated with fetalhypothyroidism and, rarely,aplasia cutis.
• Cordocentesis sometimesrecommended to test fetalthyroid function.
• Does not readily crossmembranes.
• Milk concentrationsare quite low.
Methimazole(Thiamazole,Mercazole, Tapazole)
Second-line treatment forGraves’ disease.
• Crosses the human placenta. • Excreted in breastmilk.• Can induce fetal goiter and
even cretinism in a dose-dependent fashion.
• Also commonly associatedwith fetal anomalies suchas aplasia cutis, esophagealatresia, and choanalatresia.120,121,122
• Long-term follow-upstudies of exposed childrenreveal no deleterious effectson either thyroid functionor physical and intellectualdevelopment with doses upto 20 mg/d.123
Coumarin derivativesWarfarin (Coumadin) • Contraindicated in
pregnancy.• No adequate reports or
well-controlled studies.• Because the risk of a
bleeding complicationduring pregnancyapproximates 18%, specialattention should be paidwhen used duringpregnancy.
• Despite significantpreventive effort,thromboembolic diseaseremains one of the majorcauses of maternalmorbidity and mortalityduring pregnancy.
• Recognized teratogen.• Exposure from 6–10 wk of
gestation is associated withan embryopathy (possiblysecondarily from vitamin Kdeficiency), and subsequentexposure with a fetopathy(possibly secondarily frommicrohemorrhages).
• “Warfarin syndrome”includes nasal hypoplasia,microphthalmia, hypoplasiaof the extremities, IUGR,heart disease, scoliosis,deafness, and mentalretardation.130
• Compatible withbreast-feeding becauseit does not enterhuman breastmilk.132,133
(continued)
VOL. 113, NO. 1, JANUARY 2009 Buhimschi and Weiner Medications in Pregnancy and Lactation 177

Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen (continued)
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
Coumarin derivativesWarfarin (Coumadin)(continued)
• A dose higher than 5 mg/d isreported to be associated witha greater risk of an adverseoutcome.
• In women with mechanicalheart valves, an INR of2.3–3.0 is recommendedfor either prophylaxis ortreatment of venousthromboembolism:1) Believed that this INR
level minimizes the riskof hemorrhage which isfrequently associatedwith higher doses.124
2) Safe approach: womenreceiving therapeuticdose anticoagulationwith the drug beforepregnancy for ahereditary or acquiredcondition should betransitioned totherapeutic doses ofunfractionated heparinor low molecular weightheparin before or within6 wk of gestation.125
• Previous studies advise thatthe maternal morbidity ishigher in women withbioprosthetic valves:
• In a large series of womentreated the duration ofpregnancy for a prostheticvalve, the incidence of fetal“warfarin syndrome” was5.6%, the pregnancy loss ratewas 32%, and the stillbirth rate10% of pregnancies achievingat least 20 wk.131
• Agenesis of the corpuscallosum, Dandy-Walkermalformation, and opticatrophy are the most commonCNS malformations.131
• Long-term follow-up studiesreported that school-agechildren exposed in utero havean increased incidence of mildneurologic dysfunction and anIQ�80.131
• Compatible withbreast-feeding becauseit does not enterhuman breastmilk.132,133
1) Coumarin derivativeswere safe and effectiveand did not lead toembryopathy.126
2) In such cases therapeuticheparin may not beeffective prophylaxis; itmay be safest to continuewarfarin, although inmost instances physiciansrecommend replacementwith heparin or lowmolecular weight heparinbetween 6–12 wk.127
• If the mother’s conditionrequires anticoagulation withwarfarin, it should besubstituted with heparin at36 wk to decrease the risk ofepidural/spinal anesthesia(subdural hematoma) andwarfarin treatment should beresumed postpartum.128, 129
(continued)
178 Buhimschi and Weiner Medications in Pregnancy and Lactation OBSTETRICS & GYNECOLOGY

Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen (continued)
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
LithiumLithium (Calith,
Lithocarb, Lithonate)• Used for the treatment of
psychiatric disorders(prevention of recurrent maniaand bipolar depression and inreducing risk of suicidalbehavior); typically not usedfor the rapid control of acutemania.134
• The decision to discontinuedrug therapy in pregnancybecause of fetal risks should bebalanced against the maternalrisks of exacerbation ofillness.37
• Physicians should be awarethat pregnancy and especiallythe puerperium are high-risktimes for recurrence of bipolardisease and likewise thatsudden discontinuation of thedrug can be associated with ahigh rate of disease relapse.135
• ACOG recommendations(2008):1) In women who experience
mild and infrequentepisodes of illness,treatment should begradually tapered beforeconception.
2) In women who have moresevere episodes but areonly at moderate risk forrelapse, treatment shouldbe tapered beforeconception but reinstitutedafter organogenesis.
3) In women who haveespecially severe andfrequent episodes of illness,treatment should becontinued throughoutgestation and the patientcounseled regarding therisks.37,136
• A special concern is theuse of lithium prior todelivery:1) Many recommend that the
drug be tapered graduallyover the month prior todelivery, maintainingserum levels between0.5–1.2 mEq/L.137
• Crosses the placenta andmay be a weak humanteratogen (small increase incongenital cardiacmalformations reported).138
• Associated with fetal andneonatal cardiacarrhythmias, hypoglycemia,nephrogenic diabetesinsipidus, polyhydramnios,changes in thyroid function,premature delivery, LGAinfant, and “floppy infant”syndrome.37,139
• Several studies noted anincreased prevalence ofEbstein’s anomaly, althoughthis finding was notconfirmed in a prospective,multicenter study.140
• The risk ratio for cardiacmalformations isapproximately 1.2–7.7 andthe risk ratio for overallcongenital malformations is1.5–3.141
• Fetal echocardiography isrecommended in womenexposed during the firsttrimester.142
• Excreted in breast milkand detectable levels canbe measured in thenursing newborn.143
• Whether nursing mothersshould continue drugtherapy while breast-feeding is subject ofcontroversy.144
• Neonatal clearance rate isslower than in the adult;thus, in the neonate thelevel of circulating drugmight be much higherthan expected.
• If lithium must becontinued during breast-feeding, its levels shouldbe measured in theneonatal blood to noteany adverse effects.
(continued)
VOL. 113, NO. 1, JANUARY 2009 Buhimschi and Weiner Medications in Pregnancy and Lactation 179

Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen (continued)
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
LithiumLithium (Calith,
Lithocarb, Lithonate)(continued)
2) Levels should bemonitored weekly after35 wk of gestation, andtherapy eitherdiscontinued ordecreased by one quarter2–3 d before delivery.
MisoprostolMisoprostol (Cytotec) • Not FDA-approved for any
indications in pregnancy.• Currently, FDA-approved
only for the treatment andprevention of intestinalulcer disease resulting fromNSAID use.
• Well-studied andextensively used for bothcervical ripening andinduction of labor duringthe second and thirdtrimesters.145,146
• Combined withmifepristone, the drug issafe and effective formedical termination ofearly pregnancy.147
• In 2000, the manufacturer(Pfizer) issued a warningletter to U.S. health careproviders, cautioningagainst the use ofmisoprostol in pregnantwomen secondary to thelack of safety data for itsuse in obstetric practice.
• In 2002, ACOG concludedthat the risk of uterinerupture during vaginalbirth after cesareandelivery is substantiallyincreased by the use of thedrugs as well as otherprostaglandin cervicalripening agents.148
• ACOG recommendations(2003):1) If used for cervical ripening
or labor induction in thethird trimester, 25micrograms should beconsidered for the firstdose.
2) Higher doses (50micrograms every 6 h) canbe used in some situations.
• Associated with a higherrate of fetal variabledecelerations, and, as aresult, a higher prevalenceof meconium.149
• Although suchcomplications occur morefrequently with the use ofthis drug compared tooxytocin, there is noincrease in the incidence ofcesarean delivery for fetaldistress or umbilicalacidemia.
• Congenital defects afterunsuccessful first trimestermedical abortions havebeen reported, includingskull defects, cranial nervepalsies, facialmalformations, and limbdefects.150
• Excreted in breastmilk.
• Milk levels rise anddecline rapidly(essentiallyundetectable in 5 h),significantly loweringinfant exposure.151
(continued)
180 Buhimschi and Weiner Medications in Pregnancy and Lactation OBSTETRICS & GYNECOLOGY

Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen (continued)
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
MisoprostolMisoprostol (Cytotec)(continued)
3) Uterine hyperstimulation,and meconium stainingof amniotic fluid arerecognizedcomplications.
4) The drug should not beadministered morefrequently than every3–6 h.
5) Oxytocin should not beadministered less than4 h after the lastmisoprostol dose.
6) When used for laborinduction, fetal heart rateand uterine activitymonitoring should beinitiated in a hospitalsetting.
7) Contraindicated inwomen with prior uterinescar.148
Oral contraceptivesOral contraceptives • Numerous studies have
addressed the safety andeffectiveness of hormonalcontraceptive use in healthywomen:1) Data are far less
complete for womenwith underlying medicalproblems.152
2) Decisions regardingcontraception, especiallyfor women with medicalproblems may becomplicated.
3) Age, smoking,hypertension, diabetes,dyslipidemia, andmigraines are importantrisk factors to beconsidered prior torecommending anyform of hormonalcontraception.
4) In some cases,medications takenfor certain chronicconditions mayalter the effectivenessof hormonalcontraception.
• Risk for major congenitalmalformations probablyrelated to the drugsused to control aparticular medicalcondition and not to theoral contraceptive (seeAnticonvulsants).
• About 1% of pregnantwomen use oralcontraceptives duringthe first part of theirpregnancy and therebyexpose their fetuses toestrogens; however,exposure to specificestrogens orprogestogens seemsto be unrelated to theoccurrence ofmalformations.
• Causal relationshipbetween a syndrome ofmultiple congenitalanomalies (vertebral, anal,cardiac, tracheoesophageal,renal, and limb) andmaternalprogesterone/estrogenexposure has possibly beenestablished.154
• Postpartum womenremain in ahypercoagulable statefor weeks afterchildbirth.
• Product labeling forcombination oralcontraceptivesrecommends theiruse only after 4 wkpostpartum in non-breast-feedingwomen.
• Because progestin-only oralcontraceptives anddepotmedroxyprogesteroneacetate do notcontain estrogen,these methods maybe safely initiatedimmediatelypostpartum.
(continued)
VOL. 113, NO. 1, JANUARY 2009 Buhimschi and Weiner Medications in Pregnancy and Lactation 181

Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen (continued)
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
Oral contraceptivesOral contraceptives
(continued)
5) Pregnancy in these casesmay pose substantialrisks to the mother andher fetus.
• For more information,refer to the most recentACOG Practice Bulletin(2006) on which this topicis extensively covered.152
• Contraceptive failure withconcomitant antibioticsreported; however,evidence exists only forrifampin.153
• Studies have demonstratedreduced serum levels oforal contraceptives inwomen takinganticonvulsants; however,ovulation and accidentalpregnancy were notobserved.
• Higher risk ofcontraceptive failure inobese women; however,use should not necessarilybe discontinued.
• A study providing evidencebetween oral contraceptivesand birth defects (limbanomalies) found onlymales affected; however,this link remains weak andit was suggested that if oralcontraceptives areteratogenic, it is withpeople who arepredisposed.
• Apparently the likelihoodto deliver a malformedinfant in women whoused oral contraceptivesat the beginning ofpregnancy is increased bysmoking.155
• One study concludedthat early, high-dose inutero exposures to Depo-Provera may affect fetalgrowth.156
• Others suggested thatmedroxyprogesteroneacetate cannot bedemonstrated to have ameasurable teratogenic riskand certainly does notpresent a risk forcongenital heart diseaseand limb reductiondefects.157
• Several studies addressedthe issue related to fetalexposure to levonorgestrelin women who seekemergency contraception:
—If hormonal emergencycontraception isinadvertently taken in earlypregnancy, neither thewoman nor the fetus willbe harmed.
RetinoidsIsotretinoin (Accutane) • Contraindicated during
pregnancy.• Before prescribing,
physicians must be sure thatpatients are capable ofcomplying with mandatorycontraceptive measures.(Only manufacturer-approved physicians mayprescribe it.158)
• This drug and its activemetabolites cross thehuman placenta and areknown human teratogens.
• Multiple organ systems areaffected including CNS,cardiovascular, andendocrine and thus damagecan be severe.160
• Unknown if entershuman breast milk.
• Considering its potentialadverse impact on thefetus, breast-feeding iscontraindicated.
(continued)
182 Buhimschi and Weiner Medications in Pregnancy and Lactation OBSTETRICS & GYNECOLOGY

CONCLUSIONWhether to prescribe a drug to a pregnant or breast-feeding woman is a decision that must be made inconsideration of many factors, including, but notlimited to, gestational age of the embryo or fetus,route of drug administration, absorption rate of thedrug, whether the drug crosses the placenta or isexcreted in breast milk, the necessary effective dose ofthe drug, molecular weight of the drug, whethermonotherapy is sufficient or if multiple drugs arenecessary to be effective, and even the mother’sgenotype. Potential harm to the fetus or nursing infantis paramount among these factors. Equally importantis assessment of the potential harm to the mother thatwithholding a drug can cause. The decision, then,typically comes down to, “Does the benefit of thedrug outweigh its risks?”
However, accurately weighing benefit against riskrequires a thorough understanding of those benefitsand risks. Current methods to assess and classify drugrisk are spotty at best. Pharmaceutical companies gainapproval to market drugs before follow-up studieshave been conducted on their long-term effects.Moreover, pregnant and breast-feeding women arenot appropriate test subjects precisely because of therisk of drug teratogenicity.
Novel approaches in the field of theranostics arebeing developed to address this research shortfall.Theranostics involves a diagnostic test to classifydisease subtypes or stages to select and qualify aspecific course of treatment and to monitor patientresponse to the specific targeted therapy. In contrastto current inadequate research methods, theranosticscan potentially address several important questions:
Table 3. Considerations for Teratogenic Drugs Commonly Prescribed in Pregnant and Breast-feedingWomen (continued)
Drug Maternal Considerations Fetal ConsiderationsBreast-feedingConsiderations
RetinoidsIsotretinoin (Accutane)(continued)
• The most recent and moststringent system aimed toavoid exposure is anInternet-based, performance-linked system callediPLEDGE.*159
• Two reliable forms of birthcontrol must be used at thesame time (unless abstinenceis the chosen method ofbirth control) for 1 mobefore starting treatment,during treatment, and for atleast 1 mo after the end ofthe treatment.
• Mental retardation withoutmalformations has also beenreported.
• Unknown if entershuman breast milk.
• Considering itspotential adverseimpact on the fetus,breast-feeding iscontraindicated
Radioactive iodine (iodine-131)Iodine-131 (I-131) • Contraindicated in pregnant
women.• Cost-effective, safe, and
reliable treatment forhyperthyroidism in non-pregnant women.161
• Although excreted from thebody within 1 mo, thecurrent ACOGrecommendation is thatwomen should avoidpregnancy for 4–6 mofollowing treatment.113
• No adequate reports or well-controlled studies in humanfetuses.
• Detrimental effects on thethyroid of the developingfetus as a result of I-131
treatment for thyrotoxicosisof the mother in the firsttrimester of pregnancy arereported.162
• Breast-feeding shouldbe avoided for at least120 d aftertreatment.163
ACE, angiotensin-converting enzyme; CNS, central nervous system; SSRI, selective serotonin reuptake inhibitor; IUGR, intrauterine growthrestriction; STD, sexually transmitted disease; IV, intravenous; INR, international normalized ratio; IQ, intelligence quotient; LGA, large forgestational age; ACOG, American College of Obstetricians and Gynecologists; FDA, U.S. Food and Drug Administration; NSAID, nonsteroidalantiinflammatory drug.
* Available at http://www.fda.gov/cder/drug/infopage/accutane /iPLEDGEupdate.† Saxen I. Cleft palate and maternal diphenhydramine intake [letter]. Lancet 1974;1:407–8.‡ Tuffli GA. Testosterone and micropenis [letter]. J Pediatr 1974;84:927.
VOL. 113, NO. 1, JANUARY 2009 Buhimschi and Weiner Medications in Pregnancy and Lactation 183

Why do pregnant women present with different signsand symptoms and of varying degrees? Why dopregnant women respond differently to treatments?Why do they require different medication doses?
Bioinformatics, genomics, and functional pro-teomics are molecular biology tools essential for theprogress of “molecular theranostics.” The increasingavailability of rapid and sensitive diagnostic toolsalready allows personalized treatment, which ad-dresses the heterogeneity of both the disease and thesubject. Theranostics offers the opportunity of build-ing bridges between research and clinical develop-ment (translational medicine). Although theranosticsis still in its infancy, it is expected to grow rapidly. InMarch 2004, the FDA released a white paper entitled,“Innovation or Stagnation?—Challenge and Opportu-nity on the Critical Path to New Medical Products.”164
This report describes the inefficiencies in the transla-tion of novel research from the bench to bedside, witha focus on drug discovery and development pro-cesses. This “critical path” initiative has already dem-onstrated success in several areas. For example, tras-tuzumab (Herceptin, Genentech, S. San Francisco,CA) targets the her2/neu receptor, which is a biomar-ker for an aggressive subset (25%) of breast cancer.Molecular diagnostics can detect HER2/neu frombiopsy samples of breast tumor tissue.165 Trastuzumabis not indicated for the general population of breastcancer patients, because it does not have a beneficialeffect on patients whose tumors do not express theher2/neu receptor. However, treatment with trastu-zumab in the her2/neu–expressing breast cancersubpopulation cuts the 4-year recurrence rate by 50%and thus extends the life of appropriate breast cancer
patients. An example of a “theranostic strategy” herewould be the development of rapid genotyping assaysfor pregnant women that are predictive of phenotypeexpression in the mother and fetus.166 As more muta-tions are identified and clinical, pharmacologic, biologic,and pharmacokinetic relationships are established, rapidgenotyping may soon become a clinical reality for thetargeted treatment of maternal and fetal disease.
Meanwhile, physicians should look more criti-cally at a drug’s classification and at evidence of itsteratogenicity before prescribing it. Information aboutthe effect of exposure to a large number of medica-tions during pregnancy can be obtained in electronicformat through consultation of several Web sites(Table 4). In particular, the Reprotox resource wasdeveloped to provide summary information to healthcare providers on the effects of chemical and physicalagents on fertility, pregnancy, and lactation. Agentsinclude industrial and environmental chemicals aswell as over-the-counter, prescription, and recre-ational drugs. There are summaries for more than4,000 agents included, along with references for thedata.
REFERENCES1. Buhimschi CS, Weiner CP. Medications in pregnancy and
lactation. In: Queenan JT, Spong CY, Lockwood CJ, editors.Management of high-risk pregnancy: an evidence-basedapproach. 5th ed. Malden (MA): Blackwell Publishing Ltd;2007. p. 38–58.
2. Carney EW, Scialli AR, Watson RE, DeSesso JM. Mecha-nisms regulating toxicant disposition to the embryo duringearly pregnancy: an interspecies comparison. Birth DefectsRes C Embryo Today 2004;72:345–60.
3. Giroux M, Teixera MG, Dumas JC, Desprats R, GrandjeanH, Houin G. Influence of maternal blood flow on theplacental transfer of three opioids–fentanyl, alfentanil, sufen-tanil. Biol Neonate 1997;72:133–41.
4. Shepard TH, Lemire RJ. Catalog of teratogenic agents. 12thed. Baltimore (MD): John Hopkins University Press; 2007.
5. Clayton-Smith J, Donnai D. Human malformations. In:Rimoin DL, Connor JM, Pyeritz RE, editors. Emery andRimoin’s principles and practice of medical genetics. 3rd ed.New York (NY): Churchill Livingstone; 1997. p. 383–94.
6. Cabrera RM, Hill DS, Etheredge AJ, Finnell RH. Investiga-tions into the etiology of neural tube defects. Birth DefectsRes C Embryo Today 2004;72:330–44.
7. Steffensen FH, Nielsen GL, Sørensen HT, Olesen C, Olsen J.Pregnancy outcome with ACE-inhibitor use in early preg-nancy. Lancet 1998;351:596.
8. Cooper WO, Hernandez-Diaz S, Arbogast PG, Dudley JA,Dyer S, Gideon PS, et al. Major congenital malformationsafter first-trimester exposure to ACE inhibitors. N Engl J Med2006;354:2443–51.
9. Mitchell AA. Systematic identification of drugs that causebirth defects–a new opportunity. N Engl J Med 2003;349:2556–9.
10. Kennedy DL, Uhl K, Kweder SL. Pregnancy exposure regis-tries. Drug Saf 2004;27:215–28.
Table 4. Resources for Drug Effects in Pregnancy*
ResourceName
Web Site
Reprotox http://www.reprotox.orgTeris http://depts.washington.edu/teriswebFDA http://www.fda.gov/womens/registries/Paroxetine http://www.gskus.com/news/paroxetine/
paxil_letter_e3.pdfIsotretinoin http://www.fda.gov/cder/drug/infopage/
accutane/iPLEDGEupdateSTD http://www.cdc.gov/std/treatment/2006/
updated-regimens.htm
FDA, U.S. Food and Drug Administration; STD, sexually transmit-ted diseases.
* Web sites listed and recommended for relevant information inregard to the effect of exposure to a large number of drugmedications during pregnancy (Reprotox, Teris), U.S. Food andDrug Administration, paroxetine and isotretinoin exposure duringpregnancy, and the most up-to-date recommendations for treat-ment of sexually transmitted diseases during pregnancy.
184 Buhimschi and Weiner Medications in Pregnancy and Lactation OBSTETRICS & GYNECOLOGY

11. Slone D, Shapiro S, Miettinen OS. Case-control surveillanceof serious illnesses attributable to ambulatory drug use. In:Colombo, F, Shapiro S, Slone D, Tognoni G, editors. Epide-miological evaluation of drugs. Amsterdam (the Netherlands):Elsevier/North Holland Biomedical Press; 1977. p. 59–70.
12. Buhimschi CS. Endocrinology of lactation. Obstet GynecolClin North Am 2004;31:963–79.
13. Berlin CM, Briggs GG. Drugs and chemicals in human milk.Semin Fetal Neonatal Med 2005;10:149–59.
14. Weiner CP. Introduction. In: Weiner CP, Buhimschi C,editors. Drugs for pregnant and lactating women. New York(NY): Churchill Livingston; 2004. p. XII–XV.
15. Lagoy CT, Joshi N, Cragan JD, Rasmussen SA. Medicationuse during pregnancy and lactation: an urgent call for publichealth action. J Womens Health (Larchmt) 2005;14:104–9.
16. McNamara PJ, Abbassi M. Neonatal exposure to drugs inbreast milk. Pharm Res 2004;21:555–66.
17. Solomon GM, Weiss PM. Chemical contaminants in breastmilk: time trends and regional variability. Environ HealthPerspect 2002;110:A339–47.
18. Dorea JG. Exposure to mercury during the first six monthsvia human milk and vaccines: modifying risk factors. AmJ Perinatol 2007;24:387–400.
19. Stowe ZN. The use of mood stabilizers during breastfeeding.J Clin Psychiatry 2007;68 suppl:22–8.
20. Yoshida K, Smith B, Kumar R. Psychotropic drugs in moth-ers’ milk: a comprehensive review of assay methods, phar-macokinetics and of safety of breast-feeding. J Psychophar-macol 1999;13:64–80.
21. Stultz EE, Stokes JL, Shaffer ML, Paul IM, Berlin CM. Extentof medication use in breastfeeding women. Breastfeed Med2007;2:145–51.
22. Uhl K, Kennedy DL, Kweder SL. Risk management strategiesin the Physicians’ Desk Reference product labels for preg-nancy category X drugs. Drug Saf 2002;25:885–92.
23. Wen SW, Yang T, Krewski D, Yang Q, Nimrod C, Garner P,et al. Patterns of pregnancy exposure to prescription FDA C,D and X drugs in a Canadian population. J Perinatol 2008;28:324–9.
24. Tomlinson AJ, Campbell J, Walker JJ, Morgan C. Malignantprimary hypertension in pregnancy treated with lisinopril.Ann Pharmacother 2000;34:180–2.
25. August P, Mueller FB, Sealey JE, Edersheim TG. Role ofrenin-angiotensin system in blood pressure regulation inpregnancy. Lancet 1995;345:896–7.
26. Easterling TR, Carr DB, Davis C, Diederichs C, Brateng DA,Schmucker B. Low-dose, short-acting, angiotensin-convertingenzyme inhibitors as rescue therapy in pregnancy. ObstetGynecol 2000;96:956–61.
27. Landon MB. Diabetic nephropathy and pregnancy. ClinObstet Gynecol 2007;50:998–1006.
28. Tabacova SA, Kimmel CA. Enalapril: pharmacokinetic/dy-namic inferences for comparative developmental toxicity. Areview. Reprod Toxicol 2001;15:467–78.
29. Miller RK, Jessee L, Barrish A, Gilbert J, Manson JM.Pharmacokinetic studies of enalaprilat in the in vitro perfusedhuman placental lobule system. Teratology 1998;58:76–81.
30. Burrows RF, Burrows EA. Assessing the teratogenic potentialof angiotensin-converting enzyme inhibitors in pregnancy.Aust N Z J Obstet Gynaecol 1998;38:306–11.
31. Centers for Disease Control and Prevention (CDC). Postmar-keting surveillance for angiotensin-converting enzyme inhib-itor use during the first trimester of pregnancy–United States,
Canada, and Israel, 1987–1995. MMWR Morb Mortal WklyRep 1997;46:240–2.
32. Maliheh K, Abdorrazagh K, Armen K, Reza S. Angiotensinconverting enzyme inhibitors and aortic arch obstructivemalformations. Indian J Med Sci 2006;60:417–20.
33. Boix E, Zapater P, Pico A, Moreno O. Teratogenicity withangiotensin II receptor antagonists in pregnancy. J Endocri-nol Invest 2005;28:1029–31.
34. Redman CW, Kelly JG, Cooper WD. The excretion ofenalapril and enalaprilat in human breast milk. Eur J ClinPharmacol 1990;38:99.
35. Devlin RG, Fleiss PM. Captopril in human blood and breastmilk. J Clin Pharmacol 1981;21:110–3.
36. ACOG Committee on Obstetric Practice. ACOG CommitteeOpinion No. 354: Treatment with selective serotonin reuptakeinhibitors during pregnancy. Obstet Gynecol 2006;108:1601–3.
37. ACOG Committee on Practice Bulletins—Obstetrics. ACOGPractice Bulletin: Clinical management guidelines for obste-trician-gynecologists number 92, April 2008 (replaces practicebulletin number 87, November 2007). Use of psychiatricmedications during pregnancy and lactation. Obstet Gynecol2008;111:1001–20.
38. Cohen LS, Altshuler LL, Harlow BL, Nonacs R, Newport DJ,Viguera AC, et al. Relapse of major depression duringpregnancy in women who maintain or discontinue antide-pressant treatment [published erratum appears in JAMA2006;296:170]. JAMA 2006;295:499–507.
39. Heikkinen T, Ekblad U, Palo P, Laine K. Pharmacokinetics offluoxetine and norfluoxetine in pregnancy and lactation. ClinPharmacol Ther 2003;73:330–7.
40. Wen SW, Yang Q, Garner P, Fraser W, Olatunbosun O,Nimrod C, et al. Selective serotonin reuptake inhibitors andadverse pregnancy outcomes. Am J Obstet Gynecol 2006;194:961–6.
41. Malm H, Klaukka T, Neuvonen PJ. Risks associated withselective serotonin reuptake inhibitors in pregnancy. ObstetGynecol 2005;106:1289–96.
42. Einarson TR, Einarson A. Newer antidepressants in preg-nancy and rates of major malformations: a meta-analysis ofprospective comparative studies. Pharmacoepidemiol DrugSaf 2005;14:823–7.
43. Hendrick V, Stowe ZN, Altshuler LL, Hwang S, Lee E,Haynes D. Placental passage of antidepressant medications.Am J Psychiatry 2003;160:993–6.
44. Alwan S, Reefhuis J, Rasmussen SA, Olney RS, Friedman JM,National Birth Defects Prevention Study. Use of selectiveserotonin-reuptake inhibitors in pregnancy and the risk ofbirth defects. N Engl J Med 2007;356:2684–92.
45. Chambers CD, Hernandez-Diaz S, Van Marter LJ, WerlerMM, Louik C, Jones KL, et al. Selective serotonin-reuptakeinhibitors and risk of persistent pulmonary hypertension ofthe newborn. N Engl J Med 2006;354:579–87.
46. Chambers CD, Johnson KA, Dick LM, Felix RJ, Jones KL.Birth outcomes in pregnant women taking fluoxetine. N EnglJ Med 1996;335:1010–5.
47. Costei AM, Kozer E, Ho T, Ito S, Koren G. Perinatal outcomefollowing third trimester exposure to paroxetine. Arch PediatrAdolesc Med 2002;156:1129–32.
48. Zeskind PS, Stephens LE. Maternal selective serotoninreuptake inhibitor use during pregnancy and newborn neu-robehavior. Pediatrics 2004;113:368–75.
49. Stowe ZN, Hostetter AL, Owens MJ, Ritchie JC, Sternberg K,Cohen LS, et al. The pharmacokinetics of sertraline excretion
VOL. 113, NO. 1, JANUARY 2009 Buhimschi and Weiner Medications in Pregnancy and Lactation 185

into human breast milk: determinants of infant serum con-centrations. J Clin Psychiatry 2003;64:73–80.
50. Howard LM, Hoffbrand S, Henshaw C, Boath L, Bradley E.Antidepressant prevention of postnatal depression. TheCochrane Database of Systematic Reviews 2005, Issue 2.Art.No.: CD004363. DOI: 10.1002/14651858.CD004363.
51. Louik C, Lin AE, Werler MM, Hernandez-Diaz S, Mitchell AA.First-trimester use of selective serotonin-reuptake inhibitors andthe risk of birth defects. N Engl J Med 2007;356:2675–83.
52. Hallberg P, Odlind V, Sjöblom V. Selective serotonin-reuptake inhibitors and persistent pulmonary hypertension ofthe newborn. N Engl J Med 2006;354:2188–90.
53. Hendrick V, Fukuchi A, Altshuler L, Widawski M, WertheimerA, Brunhuber MV.. Use of sertraline, paroxetine and fluvox-amine by nursing women. Br J Psychiatry 2001;179:163–6.
54. Back DJ, Bates M, Bowden A, Breckenridge AM, Hall MJ,Jones H, et al. The interaction of phenobarbital and otheranticonvulsants with oral contraceptive steroid therapy. Con-traception 1980;22:495–503.
55. Crawford P, Chadwick D, Cleland P, Tjia J, Cowie A, BackDJ, et al. The lack of effect of sodium valproate on thepharmacokinetics of oral contraceptive steroids. Contracep-tion 1986;33:23–9.
56. Crawford P. Interactions between antiepileptic drugs andhormonal contraception. CNS Drugs 2002;16:263–72.
57. Kjaer D, Horvath-Puho E, Christensen J, Vestergaard M,Czeizel AE, Sørensen HT, et al. Antiepileptic drug use, folicacid supplementation, and congenital abnormalities: a popu-lation-based case–control study. BJOG 2008;115:98–103.
58. Azarbayjani F, Danielsson BR. Embryonic arrhythmia byinhibition of HERG channels: a common hypoxia-relatedteratogenic mechanism for antiepileptic drugs? Epilepsia2002;43:457–68.
59. Jager-Roman E, Deichl A, Jakob S, Hartmann AM, Koch S,Rating D, et al. Fetal growth, major malformations, and minoranomalies in infants born to women receiving valproic acid.J Pediatr 1986;108:997–1004.
60. Nakamura H, Ushigome F, Koyabu N, Satoh S, Tsukimori K,Nakano H, et al. Proton gradient-dependent transport ofvalproic acid in human placental brush-border membranevesicles. Pharm Res 2002;19:154–61.
61. Lindhout D, Omtzigt JG, Cornel MC. Spectrum of neural-tube defects in 34 infants prenatally exposed to antiepilepticdrugs. Neurology 1992;42 suppl:111–8.
62. Kozma C. Valproic acid embryopathy: report of two siblingswith further expansion of the phenotypic abnormalities and areview of the literature. Am J Med Genet 2001;98:168–75.
63. Witters I, Van Assche F, Fryns JP. Nuchal edema as the first signof fetal valproate syndrome. Prenat Diagn 2002;22:834–5.
64. Chaudron LH. When and how to use mood stabilizers duringbreastfeeding. Prim Care Update Ob Gyns 2000;7:113–7.
65. Pynnönen S, Kanto J, Sillanpaa Erkkola R. Carbamazepine:placental transport, tissue concentrations in foetus and new-born, and level in milk. Acta Pharmacol Toxicol (Copenh)1977;41:244–53.
66. Matalon S, Schechtman S, Goldzweig G, Ornoy A. Theteratogenic effect of carbamazepine: a meta-analysis of 1255exposures. Reprod Toxicol 2002;16:9–17.
67. Moore SJ, Turnpenny P, Quinn A, Glover S, Lloyd DJ,Montgomery T, et al. A clinical study of 57 children with fetalanticonvulsant syndromes. J Med Genet 2000;37:489–97.
68. Frey B, Schubiger G, Musy JP. Transient cholestatic hepatitisin a neonate associated with carbamazepine exposure duringpregnancy and breast-feeding. Eur J Pediatr 1990;150:136–8.
69. McAuley JW, Anderson GD. Treatment of epilepsy inwomen of reproductive age: pharmacokinetic considerations.Clin Pharmacokinet 2002;41:559–79.
70. Leppik IE, Rask CA. Pharmacokinetics of antiepileptic drugsduring pregnancy. Semin Neurol 1988;8:240–6.
71. Webster WS, Howe AM, Abela D, Oakes DJ. The relation-ship between cleft lip, maxillary hypoplasia, hypoxia andphenytoin. Curr Pharm Des 2006;12:1431–48.
72. Iqbal MM, Sohhan T, Mahmud SZ. The effects of lithium,valproic acid, and carbamazepine during pregnancy andlactation. J Toxicol Clin Toxicol 2001;39:381–92.
73. Shimoyama R, Ohkubo T, Sugawara K, Ogasawara T, Ozaki T,Kagiya A, et al. Monitoring of phenytoin in human breast milk,maternal plasma and cord blood plasma by solid-phase extractionand liquid chromatography. J Pharm Biomed Anal 1998;17:863–9.
74. Eberhard-Gran M, Eskild A, Opjordsmoen S. Treating mooddisorders during pregnancy: safety considerations. Drug Saf2005;28:695–706.
75. Petrenaite V, Sabers A, Hansen-Schwartz J. Individualchanges in lamotrigine plasma concentrations during preg-nancy. Epilepsy Res 2005;65:185–8.
76. Battino D, Tomson T. Management of epilepsy during preg-nancy. Drugs 2007;67:2727–46.
77. Cunnington M, Ferber S, Quartey G, International Lam-otrigine Pregnancy Registry Scientific Advisory Committee.Effect of dose on the frequency of major birth defectsfollowing fetal exposure to lamotrigine monotherapy in aninternational observational study. Epilepsia 2007;48:1207–10.
78. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR,Walters EE. Lifetime prevalence and age-of-onset distributions ofDSM-IV disorders in the National Comorbidity Survey Replica-tion [published erratum appears in Arch Gen Psychiatry 2005;62:768]. Arch Gen Psychiatry 2005;62:593–602.
79. American College of Obstetrics and Gynecology. ACOG(American College of Obstetrics and Gynecology) PracticeBulletin: nausea and vomiting of pregnancy. Obstet Gynecol2004;103:803–14.
80. Belfort MA, Anthony J, Saade GR. Prevention of eclampsia.Semin Perinatol 1999;23:65–78.
81. Duley L, Gulmezoglu AM. Magnesium sulphate versus lyticcocktail for eclampsia. The Cochrane Database of SystematicReviews 2001, Issue 1. Art No.: CD002960. DOI: 10.1002/14651858.CD002960.
82. Duley L, Henderson-Smart D. Magnesium sulphate versusdiazepam for eclampsia. The Cochrane Database of System-atic Reviews 2003, Issue 4. Art No.: CD000127. DOI:10.1002/14651858.CD000127.
83. Rosenberg L, Mitchell AA, Parsells JL, Pashayan H, Louik C,Shapiro S. Lack of relation of oral clefts to diazepam useduring pregnancy. N Engl J Med 1983;309:1282–5.
84. Eros E, Czeizel AE, Rockenbauer M, Sorensen HT, Olsen J.A population-based case–control teratologic study of nitraz-epam, medazepam, tofisopam, alprazolum and clonazepamtreatment during pregnancy. Eur J Obstet Gynecol ReprodBiol 2002;101:147–54.
85. Kanto J, Erkkola R. The feto-maternal distribution of diaze-pam in early human pregnancy. Ann Chir Gynaecol Fenn1974;63:489–91.
86. Gonzalez de Dios J, Moya-Benavent M, Carratala-Marco F.“Floppy infant” syndrome in twins secondary to the use ofbenzodiazepines during pregnancy [in Spanish]. Rev Neurol1999;29:121–3.
186 Buhimschi and Weiner Medications in Pregnancy and Lactation OBSTETRICS & GYNECOLOGY

87. McElhatton PR. The effects of benzodiazepine use duringpregnancy and lactation. Reprod Toxicol 1994;8:461–75.
88. Kart Koseoglu H, Yucel AE, Kunefeci G, Ozdemir FN,Duran H. Cyclophosphamide therapy in a serious case oflupus nephritis during pregnancy. Lupus 2001;10:818–20.
89. Ozalp SS, Yalcin OT, Tanir HM. A hospital-based multicen-tric study results on gestational trophoblastic disease manage-ment status in a developing country. Eur J Gynaecol Oncol2001;22:221–2.
90. Peters BG, Bray JJ, Masidonski P, Mahon SM. Issues sur-rounding adjuvant chemotherapy for breast cancer duringpregnancy. Oncol Nurs Forum 2001;28:639–42.
91. Enns GM, Roeder E, Chan RT, Ali-Khan Catts Z, Cox VA,Golabi M. Apparent cyclophosphamide (cytoxan) embryop-athy: a distinct phenotype? Am J Med Genet 1999;86:237–41.
92. Meirow D, Epstein M, Lewis H, Nugent D, Gosden RG.Administration of cyclophosphamide at different stages offollicular maturation in mice: effects on reproductive perfor-mance and fetal malformations. Hum Reprod 2001;16:632–7.
93. Paskulin GA, Gazzola Zen PR, de Camargo Pinto LL, Rosa R,Graziadio C. Combined chemotherapy and teratogenicity.Birth Defects Res A Clin Mol Teratol 2005;73:634–7.
94. Ostensen M. Treatment with immunosuppressive and diseasemodifying drugs during pregnancy and lactation. AmJ Reprod Immunol 1992;28:148–52.
95. Amato D, Niblett JS. Neutropenia from cyclophosphamide inbreast milk. Med J Aust 1977;1:383–4.
96. Duck SC, Katayama KP. Danazol may cause femalepseudohermaphroditism. Fertil Steril 1981;35:230–1.
97. Minh HN, Belaisch J, Smadja A. Female pseudohermaphro-ditism [in French]. Presse Med 1993;22:1735–40.
98. Hammond MG, Hammond CB, Parker RT. Conservativetreatment of endometriosis externa: the effects of methyltes-tosterone therapy. Fertil Steril 1978;29:651–4.
99. Grote K, Stahlschmidt B, Talsness CE, Gericke C, Appel KE,Chahoud I. Effects of organotin compounds on pubertal malerats. Toxicology 2004;202:145–58.
100. Baheiraei A, Ardsetani N, Ghazizadeh S. Effects of progesto-gen-only contraceptives on breast-feeding and infant growth.Int J Gynaecol Obstet 2001;74:203–5.
101. Ratchanon S, Taneepanichskul S. Depot medroxyprogester-one acetate and basal serum prolactin levels in lactatingwomen. Obstet Gynecol 2000;96:926–8.
102. Bianchi S, Busacca M, Agnoli B, Candiani M, Calia C,Vignali M. Effects of 3 month therapy with danazol afterlaparoscopic surgery for stage III/IV endometriosis: a ran-domized study. Hum Reprod 1999;14:1335–7.
103. Kingsbury AC. Danazol and fetal masculinization: a warning.Med J Aust 1985;143:410–1.
104. Rosa FW. Virilization of the female fetus with maternaldanazol exposure. Am J Obstet Gynecol 1984;149:99–100.
105. Kaya H, Babar Y, Ozmen S, Ozkaya O, Karci M, Aydin AR,et al. Intratubal methotrexate for prevention of persistentectopic pregnancy after salpingotomy. J Am Assoc GynecolLaparosc 2002;9:464–7.
106. Kulier R, Gulmezoglu AM, Hofmeyr GJ, Cheng LN, Cam-pana A. Medical methods for first trimester abortion. TheCochrane Database of Systematic Reviews 2004, Issue 2. ArtNo.: CD002855. DOI: 10.1002/14651858.CD002855.
107. Creinin MD, Wiebe E, Gold M. Methotrexate and misopros-tol for early abortion in adolescent women. J Pediatr AdolescGynecol 1999;12:71–7.
108. Gracia CR, Brown HA, Barnhart KT. Prophylactic metho-trexate after linear salpingostomy: a decision analysis. FertilSteril 2001;76:1191–5.
109. Dilbaz S, Caliskan E, Dilbaz B, Degirmenci O, Haberal A.Predictors of methotrexate treatment failure in ectopic preg-nancy. J Reprod Med 2006;51:87–93.
110. Yedlinsky NT, Morgan FC, Whitecar PW. Anomalies associ-ated with failed methotrexate and misoprostol termination.Obstet Gynecol 2005;105:1203–5.
111. Del Campo M, Kosaki K, Bennett FC, Jones KL. Develop-mental delay in fetal aminopterin/methotrexate syndrome.Teratology 1999;60:10–2.
112. Yedlinsky NT, Morgan FC, Whitecar PW. Anomalies associ-ated with failed methotrexate and misoprostol termination.Obstet Gynecol 2005;105:1203–5.
113. Sorosky JI, Sood AK, Buekers TE. The use of chemothera-peutic agents during pregnancy. Obstet Gynecol Clin NorthAm 1997;24:591–9.
114. Mestman JH. Diagnosis and management of maternal and fetalthyroid disorders. Curr Opin Obstet Gynecol 1999;11:167–75.
115. American College of Obstetrics and Gynecology. ACOGpractice bulletin. Thyroid disease in pregnancy. Number 37,August 2002. American College of Obstetrics and Gynecol-ogy. Int J Gynaecol Obstet 2002;79:171–80.
116. Nachum Z, Rakover Y, Weiner E, Shalev E. Graves’ diseasein pregnancy: prospective evaluation of a selective invasivetreatment protocol. Am J Obstet Gynecol 2003;189:159–65.
117. Luton D, Le Gac I, Vuillard E, Castanet M, GuibourdencheJ, Noel M, et al. Management of Graves’ disease duringpregnancy: the key role of fetal thyroid gland monitoring.J Clin Endocrinol Metab 2005;90:6093–8.
118. Azizi F, Bahrainian M, Khamseh ME, Khoshniat M. Intellec-tual development and thyroid function in children who werebreast-fed by thyrotoxic mothers taking methimazole. J Pedi-atr Endocrinol Metab 2003;16:1239–43.
119. Shepard TH, Brent RL, Friedman JM, Jones KL, Miller RK,Moore CA, et al. Update on new developments in the studyof human teratogens. Teratology 2002;65:153–61.
120. Nakamura S, Nishikawa T, Isaji M, Ishimori M, Shimizu N,Iwamura M, et al. Aplasia cutis congenita and skull defects afterexposure to methimazole in utero. Intern Med 2005;44:1202–3.
121. Karg E, Bereg E, Gaspar L, Katona M, Turi S. Aplasia cutiscongenita after methimazole exposure in utero. Pediatr Der-matol 2004;21:491–4.
122. Chattaway JM, Klepser TB. Propylthiouracil versus methim-azole in treatment of Graves’ disease during pregnancy. AnnPharmacother 2007;41:1018–22.
123. Messer PM, Hauffa BP, Olbricht T, Benker G, Kotulla P,Reinwein D. Antithyroid drug treatment of Graves’ disease inpregnancy: long-term effects on somatic growth, intellectualdevelopment and thyroid function of the offspring. ActaEndocrinol (Copenh) 1990;123:311–6.
124. Vitale N, De Feo M, De Santo LS, Pollice A, Tedesco N,Cotrufo M. Dose-dependent fetal complications of warfarin inpregnant women with mechanical heart valves. J Am CollCardiol 1999;33:1637–41.
125. Marks PW. Management of thromboembolism in pregnancy.Semin Perinatol 2007;31:227–31.
126. Suri V, Sawhney H, Vasishta K, Renuka T, Grover A.Pregnancy following cardiac valve replacement surgery. IntJ Gynaecol Obstet 1999;64:239–46.
127. Vitale N, De Feo M, Cotrufo M. Anticoagulation for prostheticheart valves during pregnancy: the importance of warfarin dailydose. Eur J Cardiothorac Surg 2002;22:656.
VOL. 113, NO. 1, JANUARY 2009 Buhimschi and Weiner Medications in Pregnancy and Lactation 187

128. Hall JG, Pauli RM, Wilson KM. Maternal and fetal sequelae ofanticoagulation during pregnancy. Am J Med 1980;68:122–40.
129. Tyagi A, Bhattacharya A. Central neuraxial blocks andanticoagulation: a review of current trends. Eur J Anaesthesiol2002;19:317–29.
130. Zakzouk MS. The congenital warfarin syndrome. J LaryngolOtol 1986;100:215–9.
131. Wesseling J, Van Driel D, Smrkovsky M, Van der Veer E,Geven-Boere LM, Sauer PJ, Touwen BC. Neurological out-come in school-age children after in utero exposure tocoumarins. Early Hum Dev 2001;63:83–95.
132. Dardick KR. Warfarin during lactation. Conn Med 1980;44:693.133. Orme ML, Lewis PJ, de Swiet M, Serlin MJ, Sibeon R, Baty
JD, et al. May mothers given warfarin breast-feed theirinfants? Br Med J 1977;1:1564–5.
134. Carney SM, Goodwin GM. Lithium - a continuing story inthe treatment of bipolar disorder. Acta Psychiatr Scand Suppl2005;suppl:7–12.
135. Viguera AC, Nonacs R, Cohen LS, Tondo L, Murray A,Baldessarini RJ. Risk of recurrence of bipolar disorder inpregnant and nonpregnant women after discontinuing lithiummaintenance. Am J Psychiatry 2000;157:179–84.
136. Gelenberg AJ. Lithium efficacy and adverse effects. J ClinPsychiatry 1988;49 suppl:8–11.
137. Teixeira NA, Lopes RC, Secoli SR. Developmental toxicity oflithium treatment at prophylactic levels. Braz J Med Biol Res1995;28:230–9.
138. Giles JJ, Bannigan JG. Teratogenic and developmental effectsof lithium. Curr Pharm Des 2006;12:1531–41.
139. Pinelli JM, Symington AJ, Cunningham KA, Paes BA. Casereport and review of the perinatal implications of maternallithium use. Am J Obstet Gynecol 2002;187:245–9.
140. Jacobson SJ, Jones K, Johnson K, Ceolin L, Kaur P, Sahn D, et al.Prospective multicentre study of pregnancy outcome after lithiumexposure during first trimester. Lancet 1992;339:530–3.
141. Cohen LS, Friedman JM, Jefferson JW, Johnson EM, WeinerML.. A reevaluation of risk of in utero exposure to lithium[published erratum appears in JAMA 1994;271:1485]. JAMA1994;271:146–50.
142. van Gent EM, Verhoeven WM. Bipolar illness, lithium prophy-laxis, and pregnancy. Pharmacopsychiatry 1992;25:187–91.
143. Arnon J, Shechtman S, Ornoy A. The use of psychiatric drugs inpregnancy and lactation. Isr J Psychiatry Relat Sci 2000;37:205–22.
144. Schou M, Amdisen A. Lithium and pregnancy. 3. Lithiumingestion by children breast-fed by women on lithium treat-ment. Br Med J 1973;2:138.
145. Dodd JM, Crowther CA, Robinson JS. Oral misoprostol forinduction of labour at term: randomised controlled trial. BMJ2006;332:509–13.
146. Eroglu D, Oktem M, Yanik F, Kuscu E. Labor induction at term:a comparison of the effects of 50 microg and 25 microg vaginalmisoprostol. Clin Exp Obstet Gynecol 2007;34:102–5.
147. Zikopoulos KA, Papanikolaou EG, Kalantaridou SN, TsanadisGD, Plachouras NI, Dalkalitsis NA, et al. Early pregnancytermination with vaginal misoprostol before and after 42 daysgestation. Hum Reprod 2002;17:3079–83.
148. ACOG Committee Opinion. American College of Obstetri-cians and Gynecologists. ACOG Committee Opinion. Num-ber 283, May 2003. New US. Food and Drug Administrationlabeling on Cytotec (misoprostol) use and pregnancy. ObstetGynecol 2003;101:1049–50.
149. Alfirevic Z, Weeks A. Oral misoprostol for induction of labour.The Cochrane Database of Systematic Reviews 2006, Issue 2. ArtNo.: CD001338. DOI: 10.1002/14651858.CD001338.
150. Yedlinsky NT, Morgan FC, Whitecar PW. Anomalies associ-ated with failed methotrexate and misoprostol termination.Obstet Gynecol 2005;105:1203–5.
151. Vogel D, Burkhardt T, Rentsch K, Schweer H, Watzer B,Zimmermann R, et al. Misoprostol versus methyler-gometrine: pharmacokinetics in human milk. Am J ObstetGynecol 2004;191:2168–73.
152. ACOG Committee on Practice Bulletins-Gynecology.ACOG practice bulletin. No. 73: Use of hormonal contracep-tion in women with coexisting medical conditions. ObstetGynecol 2006;107:1453–72.
153. Back DJ, Breckenridge AM, Crawford F, MacIver M,Orme ML, Park BK, et al. The effect of rifampicin onnorethisterone pharmacokinetics. Eur J Clin Pharmacol1979;15:193–7.
154. Nora JJ, Nora AH. Editorial: Can the pill cause birth defects?N Engl J Med 1974;291:731–2.
155. Jellesen R, Andersen AM. Prenatal exposure to birth controlpills: risk of fetal death and congenital malformations [inDanish]. Ugeskr Laeger 2006;168:2437–42.
156. Pardthaisong T, Gray RH. In utero exposure to steroidcontraceptives and outcome of pregnancy. Am J Epidemiol1991;134:795–803.
157. Yovich JL, Turner SR, Draper R. Medroxyprogesteroneacetate therapy in early pregnancy has no apparent fetaleffects. Teratology 1988;38:135–44.
158. Brinker A, Kornegay C, Nourjah P. Trends in adherence to arevised risk management program designed to decrease oreliminate isotretinoin-exposed pregnancies: evaluation of theaccutane SMART program. Arch Dermatol 2005;141:563–9.
159. Abroms L, Maibach E, Lyon-Daniel K, Feldman SR. What isthe best approach to reducing birth defects associated withisotretinoin? PLoS Med 2006;3:e483.
160. Charakida A, Mouser PE, Chu AC. Safety and side effects ofthe acne drug, oral isotretinoin. Expert Opin Drug Saf2004;3:119–29.
161. Iagaru A, McDougall IR. Treatment of thyrotoxicosis [pub-lished erratum appears in J Nucl Med 2007;48:872]. J NuclMed 2007;48:379–89.
162. Pauwels EK, Thomson WH, Blokland JA, Schmidt ME,Bourguignon M, El-Maghraby TA, et al. Aspects of fetalthyroid dose following iodine-131 administration during earlystages of pregnancy in patients suffering from benign thyroiddisorders. Eur J Nucl Med 1999;26:1453–7.
163. McClellan DR, Francis GL. Thyroid cancer in children,pregnant women, and patients with Graves’ disease. Endocri-nol Metab Clin North Am 1996;25:27–48.
164. Food and Drug Administration. Innovation or stagnation?—Challenge and opportunity on the critical path to new med-ical products. Rockville (MD): U.S. Department of Healthand Human Services; 2004.
165. Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V,Bajamonde A, et al. Use of chemotherapy plus a monoclo-nal antibody against HER2 for metastatic breast cancer thatoverexpresses HER2. N Engl J Med 2001;344:783–92.
166. Buhimschi CS, Rosenberg VA, Dulay AT, Thung S,Sfakianaki AK, Bahtiyar MO, et al. Multidimensional systembiology: genetic markers and proteomic biomarkers ofadverse pregnancy outcome in preterm birth. Am J Perinatol2008;25:175–87. Catalin S. Buhimschi, Carl P. Weiner,
188 Buhimschi and Weiner Medications in Pregnancy and Lactation OBSTETRICS & GYNECOLOGY