Strategies in the Delivery Room and the first “Golden Minutes” · 2017. 11. 16. · the first...
54
Strategies in the Delivery Room and the first “Golden Minutes” Dr. Jeffrey Perlman Professor of Pediatrics Division Chief Newborn Medicine New York Presbyterian - Weill Cornell
Transcript of Strategies in the Delivery Room and the first “Golden Minutes” · 2017. 11. 16. · the first...

Strategies in the Delivery Room and the first “Golden Minutes”
Dr. Jeffrey PerlmanProfessor of Pediatrics
Division Chief Newborn MedicineNew York Presbyterian-Weill Cornell

Outline
• Situational awareness
• Basic concepts
• Ventilation and Changing Heart Rate
• Assessing Heart Rate
• Initial breaths following delivery in an apneic baby
• Oxygen delivery at birth
• Maintaining temperature at birth

Background
• Managing a newly born apneic premature infant is complex.
• Ventilation strategies to optimize the establishment of functional residual capacity, judicious oxygen management and avoidance of moderate hypothermia are critical initial steps to facilitate transition.
• Situational awareness and team work are essential to accomplish these goals

Situational Awareness
• Gestational Age
• Antenatal Corticosteroid Administration
• Placental Inflammation – Chorioamnionitis
• Intrauterine Growth Restriction
• Labor complications – e.g. FHRT abnormalities

Situational Awareness
• Team leader
• Checklists• Teamwork

0.1% Require
Intensive Resuscitation
~ 3-6% of BabiesRequire Basic Resuscitation
± Face Mask Ventilation ± Intubation
~ 10% of Babies Respond to Simple Stimulation (Drying and Rubbing) at
Birth to Facilitate Spontaneous Breathing
~ 85% of Babies only Require Immediate Assessment at Birth and Basic Newborn Care
(Assess Breathing, Dry, Maintain Warmth and Place Baby Skin-to-Skin with Mother)
How Common are DR Interventions?
Ersdal et al Resuscitation 2012
Perlman and Risser 1995
Barber et al 2006
Ersdal H Resuscitation 2012 Jul;83(7):869-73

Six Basic Concepts
• Is the Baby in Primary or Secondary Apnea ?
• Effective Ventilation is key to successful Resuscitation
• Heart rate is the best indicator of effective ventilation
• Establishing Functional Residual Capacity is key
• Minimizing Oxygen Exposure
• Maintaining temperature in a normal range is critical

Adapted from Dawes et al 1968
Primary vs Secondary Apnea

Six Basic Concepts
• Is the Baby in Primary or Secondary Apnea ?
• Effective Ventilation is key to successful Resuscitation
• Heart rate is the best indicator of effective ventilation
• Establishing Functional Residual Capacity is key
• Minimizing Oxygen Exposure
• Maintaining temperature in a normal range is critical

Changes in HR in Relation to Vco2 Changes
From Palme-Kilander Arch Dis Child 1993;68:1 1-6

Heart Rate Changes as a Function of Changing Tidal Volume
Linde JE, J. Schulz, Perlman JM et al Resuscitation, Volume 117, 2017, 80–86

Using the EKG to Assess HR in the Depressed Infant in the DR

Establishing Functional Residual Capacity (FRC)

Physiologic Pulmonary Measurements of Spontaneously Breathing Infants at Birth
Following Vaginal Delivery
• Mean inspiratory pressure = 52 cm H2O (range 25-105)
• Mean Inspiratory Volume = 37 ml (range 10-80)
• Functional Residual Capacity = 15 ml (range 8-30)
Following Cesarean Section
• Similar Inspiratory pressures and volumes
• Only 50% establish a FRC with the first breath
From Vyas et al Pediatr Pulm 787, 1981

Initial Expiratory Effort and Establishing FRC
Boon et al, J Pediatr 1979, 1031

Positive Pressure Ventilation in a Premature Infant
Requiring Resuscitation Using Two Inflations

Role of PPV Pre, During and Post Infants Own
Respiratory Effort
Murphy V et al European J Peds 2011

Pre- Active Inflation Active Inflation Post Inflation
Expired tidal
volume (ml/kg)
1.8
(0.7–7.3)
6.3
(1.9–18.4)
4.5
(0.5–18.3)
ETCO2
(kPa)
0.3
(0.1–2.1)
3.4
(0.4–11.5)
2.2
(0.3–9.3)
Inflation pressures
(cm H2O)
(Peak–PEEP)
20.0
(13.8–26.7)
19.6
(13.7–25.9)
20.2
(13.4–25.9)
Relationship of Expiratory Tidal Volume and ETCO2 Pre, During and Post Own Inspiratory Effort

From Palme-Kilander Arch Dis Child 1993;68:1 1-6
27-31 weeks
32-36 weeks
Term Infants
Ventilated- Open Symbols
Spontaneous- Closed Symbols
Comparison of VCO2 at Different Gestational Ages and Between
Spontaneous breathing and Ventilated Infants

Mechanisms Contributing to a Variable Response to Either Spontaneous Breathing and/or PPV
The inconsistent response to resuscitation in some infants in part reflects the infant’s response to initial mechanical breaths
• The most common is a REJECTION response with the production of high intrathoracic pressure, i.e. expiratory effort with no gas exchange
• A second response is the called “HEADS” paradoxical reflex with production of high negative intra-esophageal pressure and a marked improvement in the mechanical characteristics of the lung and the establishment of a functional residual capacity
• The third response is PASSIVE inflation with no change in esophageal pressure

Rejection Response “HEADS” Paradoxical Response
Passive Inflation From Boon, et al. Arch Dis Childh 1979, 492

Tidal Exchange
ml/kgReflex Present No Reflex Total #
<4.4 12 33 45
>4.4 14 4 18
Total 26 37 63
Endotracheal Resuscitation – Premature ResuscitationInfluence of Reflex Activity
Correlation between Tidal Exchange and Reflex response (p<0.001)15 Reflexes were Head’s Reflexes, 5 Rejection Responses, 6 Combined
Hoskyns EW, et al. Arch Dis Child 1987; 62:663-666

Face Mask Leak/Obstruction

Face Mask Leak and Expiratory Tidal Volumes

Airway obstruction during mask positive pressure ventilation
(PPV) in a very preterm infant with a self-inflating bag
Schmölzer G M et al. Arch Dis Child Fetal Neonatal Ed 2011;96:F254-F257

Summary
• Establishment of FRC at the time of birth is
complex dynamic and may involve several
reflex patterns.
• The presence or absence of these reflexes
and the type of induced reflex responses will
modulate lung volume recruitment.
• Mask leak and airway obstruction may in
addition complicate volume recruitment

Establishing FRC in Apneic Babies
• Prolonging Inspiratory time
• Role of PEEP

Pressure and Volume Characteristics in Infants requiring Resuscitation with Varying Inspiratory Times
Measurement Inspiratory Time
1 second 3 Seconds
Mean Volume Change (ml) 15.3 33.5
Functional Residual Capacity (ml) 1.0 15.9
From Vyas et al Pediatr Pulm 787, 1981

Te Pas et al Pediatric Research 2009;65:537
Changes in Lung Gas Volume From Birth in Anesthetized Ventilated Preterm Rabbit Pups Using
Plethysmography
SI(20s) + PEEP
PPV + PEEP
SI(20s) No PEEP
PPV No PEEP
FRC

• Some infants may require a SI to
establish FRC - duration is unclear
• CPAP/PEEP maybe more important
Summary

Oxygen Management at the Time of Delivery

What Constitutes Adequate Oxygenation
• Balance between O2 delivery and tissue demand.
• Neither PaO2 and O2 saturation can provide this
information.
• O2 transport from lung to tissues is almost
exclusively bound to Hb (97%) with ~ 3%
dissolved in plasma (determines PaO2)
• Minimal PaO2 contribution to O2 delivery.
• O2 toxicity correlates with PaO2 not saturation
(SaO2).

Air or Supplemental Oxygen for Resuscitation

Effect of Change in Practice on Starting FiO2 in the DR and Initial FiO2 on Admission Using the Target of 85-95%
0.70±0.03
0.38±0.02
0.28±0.07*
0.42±0.06
Period 2 (Sept-Nov)
*RA 14/53 (26%)
Stola et al Journal of Perinatology 2009;29:548
Period 1 (June-Aug)
Period 3 (Dec-Feb)
Period 4 (Mar-June)

Temperature Regulation

Temperature Regulation in the Newborn Infant
• A healthy term newborn tries to maintain temperature within the thermo-neutral range by constriction of peripheral blood vessels in response to a decrease in room temperature.
• This response is poorly developed in the preterm infant.
• The preterm baby has a narrow thermo-neutral range, thus it is critically important that effective steps are taken to reduce hypothermia and maintain body temperature from birth.

Temperature Loss at Birth
At birth, the infant’s body temperature can decrease rapidly in part due to evaporative losses from a wet body, a large surface area/body mass ratio and a cold delivery room environment.
Evaporative Losses Surface Area of the Newborn vs Adult

Important Clinical Fact
A naked, wet term infant in the delivery room placed
on an open table with a room temperature of 25°C
(77°F) will lose up to 4°C in skin temperature and 2°C
in core body temperature within 30 minutes
32
33
34
35
36
37
38
0 1 2 3 4 5
Tem
pe
ratu
re in
C°
Time In Minutes
With Intervention
Without Intervention

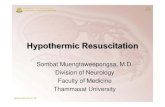
Early Hypothermia is Associated with
Increased Mortality

Budin- Paris 1896
Mortality
Weight (g)

Risk of Infant Death versus Admission Temperature
For every 1°C ↓ In Admission Temp < 36.5°C
there was a 28% ↑ Risk of Mortality
Adapted from Laptook AR et al, Pediatrics 2007;119:e643-e649

Arch Pediatr Adolesc Med. 2010;164(7):650-656. doi:10.1001/archpediatrics.2010.103
Risk of Mortality Associated With Neonatal Hypothermia in Southern Nepal

Preventing Heat Loss in the Premature Infant

Maternal Temperature
Delivery Room
Operating Room
Temperature
In Utero Environment
0.5°C > Mother
Radiant Warmer On
Skin to Skin
Occlusive wrap
Thermal Mattress
Dry
Cap
Events to be Monitored in the DR
Goal
21-23°C71-74°C

Background
• Audit of initial temperatures of infants admitted to our NICU, in 2010/2011 showed temperature <36°C in 45 - 55% of infants <35 weeks GA.
• Infants with an admitting temperature <36°C exhibited more severe early respiratory distress.
• These two observations led to a Quality Improvement Initiative.

Objective
To determine whether a multifaceted approach
(initiated prior to delivery and continued through
admission to the NICU) would reduce the number
of infants with an axillary temperature < 36°C by
50%, without increasing the number of infants
with a temperature >37.5°C.

Findings

<35 weeks Initial Temperature °C
TemperatureBaseline
n=66
Partial Implementation
n=102
Implementationn=193
DR Temperature °C 36.0 ±0.65 36.2±0.58 36.6±0.56*
NICU Temperature °C 36.0±0.81 36.3±0.58 36.7±0.50*
# Infants Temperature <36°C 36/66 (55%) 24/102 (23%) 12/193 (6%)*
Temperature >37.5°C 4/66 (6.0%) 4/102 (3.9%) 11/193 (5.6%)
DR and Initial NICU Axillary Temperatures and Number of Infants with Temperature
< 36°C and > 37.5°C
* P < 0.001

* p< 0.001
Number of Infants with a Temperature < 36°C at Baseline and at Full Implementation for the Cohort and by Gestational Age
% Occurrence
of Temp
< 36°C
55%
35%
44%
79%
6%9%
1%
9%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Cohort ≤28 Weeks 29-32 Weeks 33-34 Weeks
Baseline Implementation
*
* * *

CharacteristicBaseline
n=66Full Implementation
n=193
Intubated at 24 hours 26 (39%) 34 (17.6%)*
Infants Intubated at 24 hours at Baseline versus Full Implementation
* P <.001

Infants
Intubated
* p< 0.001
Infants Intubated at 24 hours at Baseline versus Full Implementation
39%
88%
22% 23%17,6%
55%
18%
7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Cohort ≤28 Weeks 29-32 Weeks 33-34 Weeks
Baseline Implementation
*

• Moderate hypothermia increases the risk of neonatal mortality
• Moderate hypothermia is associated with more severe respiratory distress
Summary

Summary of Current Practice of Resuscitating VLBW Infants at Cornell
• Situational awareness
• Team work
• Primary or secondary apnea
• Assessing HR – EKG - HR best indicator of effective ventilation
• Initial Respiratory support
- CPAP/PEEP, Prolonged Inspiratory time ( 3-5 seconds), PPV, Intubation
- Watch for Leak, Obstruction with BMV
• Pulse Oximeter, Blender – start with 30%
• CO2 detector
• Timing of Cord Clamping (30 to 60 seconds depending on breathing)
• Temperature maintenance
- Occlusive wrap, Heating Mattress, Cap, OR/DR temp
• Early Surfactant (if needed) within an hour
Golden Hour

Conclusions
• Managing the VLBW infant in the Delivery Room is complex and dynamic
• Requires situational awareness and team work
• Each patient should be treated on his/her own merit
• Ultimate marker of success is longterm outcome