Stinging insect hypersensitivity: A practice parameter ...
86
Stinging insect hypersensitivity: 1 A practice parameter update 2016 2 3 4 5 6 7 8 Chief Editor: David B.K. Golden, MD 9 Practice Parameter Workgroup: Jeffrey Demain, MD; Theodore Freeman, MD; David Graft, 10 MD; Michael Tankersley, MD; James Tracy, DO; Joanne Blessing-Moore, MD 11 12 Members of the Joint Taskforce on Practice Parameters 13 David Bernstein, MD; Joann Blessing-Moore, MD; Matthew Greenhawt, MD; David Khan, 14 MD; David Lang, MD; Richard Nicklas, MD; John Oppenheimer, MD; Jay Portnoy, MD; 15 Christopher Randolph, MD; Diane Schuller, MD; Dana Wallace, MD 16 17 The American Academy of Allergy, Asthma and Immunology (AAAAI) and the 18 American College of Allergy, Asthma and Immunology (ACAAI) have jointly accepted 19 responsibility for establishing “Stinging Insect Hypersensitivity: a practice parameter 20 update 2016.” This is a complete and comprehensive document at the current time. The 21 medical environment is a changing environment, and not all recommendations will be 22 appropriate for all patients. Because this document incorporated the efforts of many 23 participants, no single individual, including those who served on the Joint Task force, is 24 authorized to provide an official AAAAI or ACAAI interpretation of these practice 25 parameters. Any request for information about or an interpretation of these practice 26 parameters by the AAAAI or ACAAI should be directed to the Executive Offices of the 27 AAAAI or the ACAAI. These parameters are not designed for use by pharmaceutical 28 companies in drug promotion. 29 30 All published practice parameters are available at http://www.allergyparameters.org 31 32 33 34 35 Authors (to be listed in this order for Pubmed) David B.K. Golden, MD; Jeffrey Demain, MD; Theodore Freeman, MD; David Graft, MD; Michael Tankersley, MD; James Tracy, DO; Joann Blessing-Moore, MD
Transcript of Stinging insect hypersensitivity: A practice parameter ...
Stinging insect hypersensitivity: 1
A practice parameter update 2016 2
3 4 5 6 7 8
Chief Editor: David B.K. Golden, MD 9 Practice Parameter Workgroup: Jeffrey Demain, MD; Theodore Freeman, MD; David Graft, 10
MD; Michael Tankersley, MD; James Tracy, DO; Joanne Blessing-Moore, MD 11 12
Members of the Joint Taskforce on Practice Parameters 13
David Bernstein, MD; Joann Blessing-Moore, MD; Matthew Greenhawt, MD; David Khan, 14 MD; David Lang, MD; Richard Nicklas, MD; John Oppenheimer, MD; Jay Portnoy, MD; 15 Christopher Randolph, MD; Diane Schuller, MD; Dana Wallace, MD 16
17
The American Academy of Allergy, Asthma and Immunology (AAAAI) and the 18 American College of Allergy, Asthma and Immunology (ACAAI) have jointly accepted 19 responsibility for establishing “Stinging Insect Hypersensitivity: a practice parameter 20 update 2016.” This is a complete and comprehensive document at the current time. The 21 medical environment is a changing environment, and not all recommendations will be 22 appropriate for all patients. Because this document incorporated the efforts of many 23 participants, no single individual, including those who served on the Joint Task force, is 24 authorized to provide an official AAAAI or ACAAI interpretation of these practice 25 parameters. Any request for information about or an interpretation of these practice 26 parameters by the AAAAI or ACAAI should be directed to the Executive Offices of the 27 AAAAI or the ACAAI. These parameters are not designed for use by pharmaceutical 28 companies in drug promotion. 29
30 All published practice parameters are available at http://www.allergyparameters.org 31
32 33 34 35
Authors (to be listed in this order for Pubmed) David B.K. Golden, MD; Jeffrey Demain, MD; Theodore Freeman, MD; David Graft, MD; Michael Tankersley, MD; James Tracy, DO; Joann Blessing-Moore, MD
CONTRIBUTORS 36 The Joint Task Force has made a concerted effort to acknowledge all contributors to 37 this parameter. If any contributors have been excluded inadvertently, the Task Force 38 will ensure that appropriate recognition of such contributions is made subsequently. 39
Workgroup Chair 40 David B.K. Golden, MD 41 Institution 42 Address 43 City, State, Country (if not USA) 44
Joint Taskforce Liaison 45 Joann Blessing-Moore, MD 46 Institution 47 Address 48 City, State, Country (if not USA) 49 50
PARAMETER WORKGROUP MEMBERS 51 Jeffrey Demain, MD 52 Institution 53 Address 54 City, State, Country (if not USA) 55 56 Theodore Freeman, MD 57 Institution 58 Address 59 City, State, Country (if not USA) 60 61 David Graft, MD 62 Institution 63 Address 64 City, State, Country (if not USA) 65 66 Michael Tankersley, MD 67 Institution 68 Address 69 City, State, Country (if not USA) 70 71
James Tracy, DO 72 Institution 73 Address 74 75
JOINT TASK FORCE MEMBERS 76 David I. Bernstein, MD 77 Professor of Clinical Medicine and Environmental Health 78 Division of Allergy/Immunology 79 University of Cincinnati College of Medicine 80 Cincinnati, Ohio 81 82 Joann Blessing-Moore, MD 83 Adjunct Professor of Medicine and Pediatrics 84 Stanford University Medical Center 85 Department of Immunology 86 Palo Alto, California 87 88 David A. Khan, MD 89 Associate Professor of Internal Medicine 90 University of Texas Southwestern Medical Center 91 Dallas, Texas 92 93 David M. Lang, MD 94 Head, Allergy/Immunology Section 95 Division of Medicine 96 Director, Allergy and Immunology Fellowship Training Program 97 Cleveland Clinic Foundation 98 Cleveland, Ohio 99 100 Richard A. Nicklas, MD 101 Clinical Professor of Medicine 102 George Washington Medical Center 103 Washington, DC 104 105 John Oppenheimer, MD 106 Department of Internal Medicine 107 New Jersey Medical School 108 Pulmonary and Allergy Associates 109
Morristown, New Jersey 110 111 Jay M. Portnoy, MD 112 Chief, Section of Allergy, Asthma & Immunology 113 The Children’s Mercy Hospital 114 Professor of Pediatrics 115 University of Missouri-Kansas City School of Medicine 116 Kansas City, Missouri 117 118 Christopher C. Randolph 119 Clinical Professor of Pediatrics 120 Yale Affiliated Hospitals 121 Center for Allergy, Asthma, & Immunology 122 Waterbury, Connecticut 123 124 Diane E. Schuller, MD 125 Professor of Pediatrics 126 Pennsylvania State University Milton S. Hershey Medical College 127 Hershey, Pennsylvania 128 129 Dana Wallace MD 130 Assistant Clinical Professor of Medicine 131 Nova Southeastern University College of Osteopathic Medicine 132 Davie, Florida 133 134 INVITED REVIEWERS (alphabetical order) 135
Invited reviewers are recognized and acknowledged if they have fulfilled their 136 responsibilities as reviewers 137
Name, Degree 138 City, State, Country (if not USA) 139 140 Name, Degree 141 City, State, Country (if not USA) 142 143 Name, Degree 144 City, State, Country (if not USA) 145 146
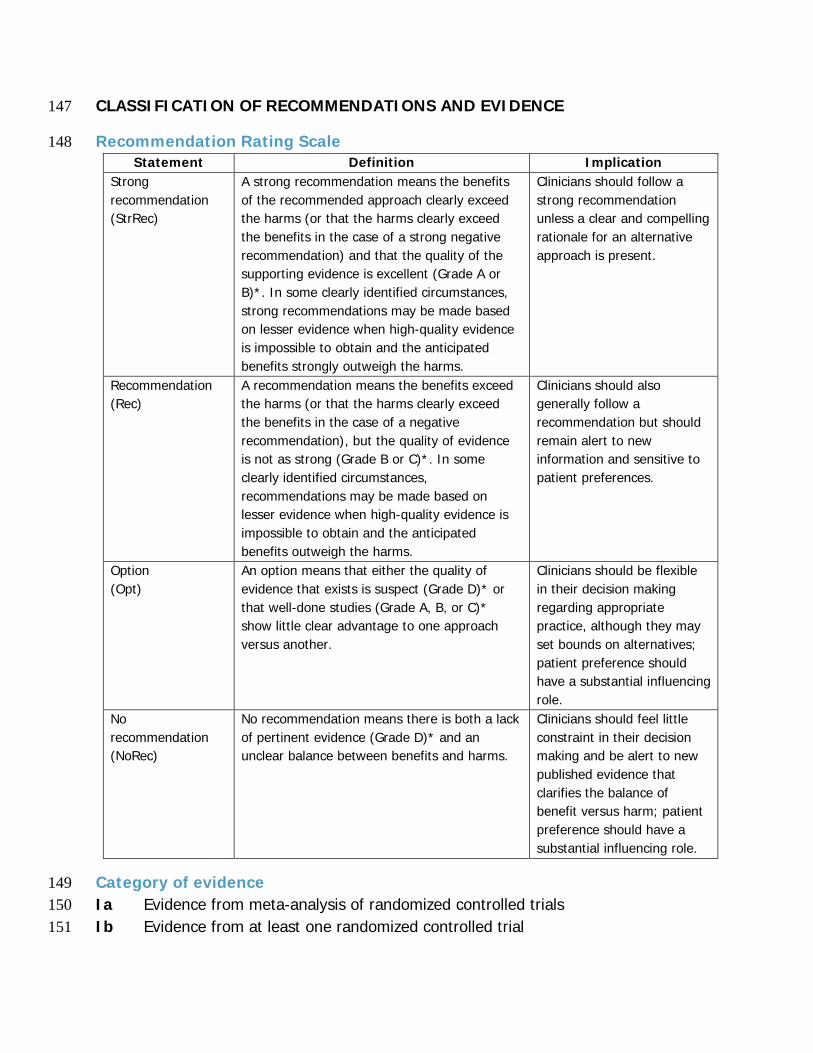
CLASSIFICATION OF RECOMMENDATIONS AND EVIDENCE 147
Recommendation Rating Scale 148 Statement Definition Implication
Strong recommendation (StrRec)
A strong recommendation means the benefits of the recommended approach clearly exceed the harms (or that the harms clearly exceed the benefits in the case of a strong negative recommendation) and that the quality of the supporting evidence is excellent (Grade A or B)*. In some clearly identified circumstances, strong recommendations may be made based on lesser evidence when high-quality evidence is impossible to obtain and the anticipated benefits strongly outweigh the harms.
Clinicians should follow a strong recommendation unless a clear and compelling rationale for an alternative approach is present.
Recommendation (Rec)
A recommendation means the benefits exceed the harms (or that the harms clearly exceed the benefits in the case of a negative recommendation), but the quality of evidence is not as strong (Grade B or C)*. In some clearly identified circumstances, recommendations may be made based on lesser evidence when high-quality evidence is impossible to obtain and the anticipated benefits outweigh the harms.
Clinicians should also generally follow a recommendation but should remain alert to new information and sensitive to patient preferences.
Option (Opt)
An option means that either the quality of evidence that exists is suspect (Grade D)* or that well-done studies (Grade A, B, or C)* show little clear advantage to one approach versus another.
Clinicians should be flexible in their decision making regarding appropriate practice, although they may set bounds on alternatives; patient preference should have a substantial influencing role.
No recommendation (NoRec)
No recommendation means there is both a lack of pertinent evidence (Grade D)* and an unclear balance between benefits and harms.
Clinicians should feel little constraint in their decision making and be alert to new published evidence that clarifies the balance of benefit versus harm; patient preference should have a substantial influencing role.
Category of evidence 149 Ia Evidence from meta-analysis of randomized controlled trials 150 Ib Evidence from at least one randomized controlled trial 151
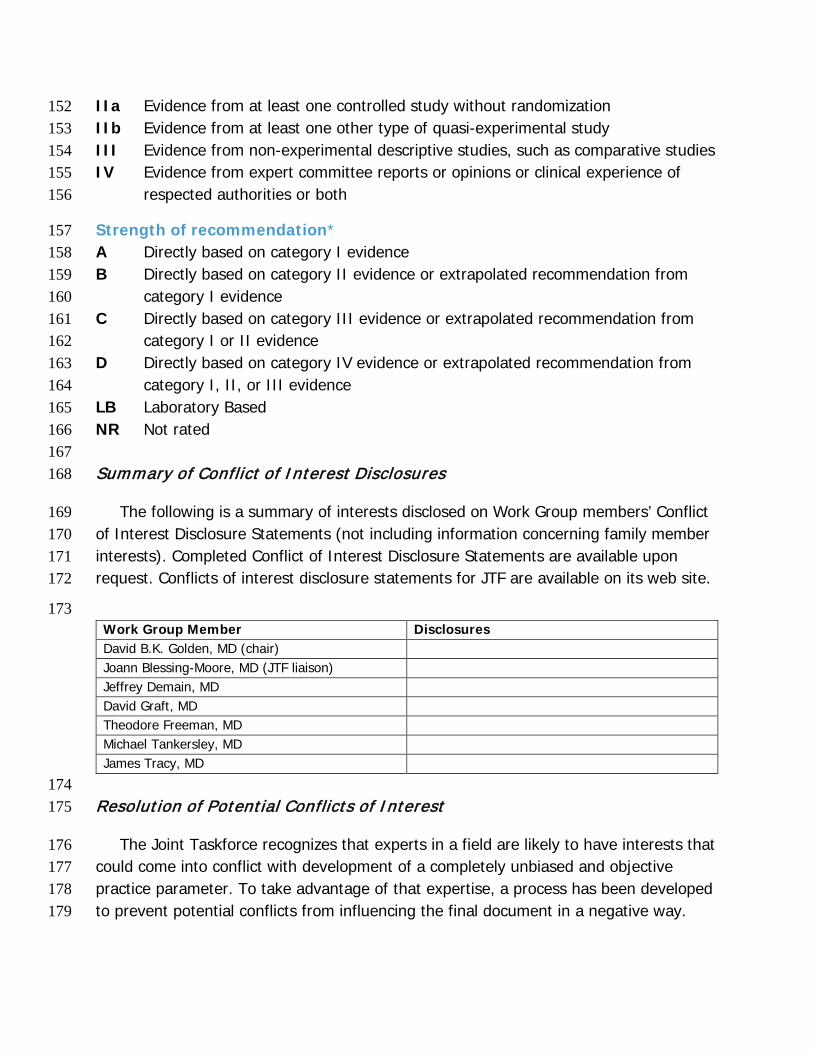
IIa Evidence from at least one controlled study without randomization 152 IIb Evidence from at least one other type of quasi-experimental study 153 III Evidence from non-experimental descriptive studies, such as comparative studies 154 IV Evidence from expert committee reports or opinions or clinical experience of 155
respected authorities or both 156
Strength of recommendation* 157 A Directly based on category I evidence 158 B Directly based on category II evidence or extrapolated recommendation from 159
category I evidence 160 C Directly based on category III evidence or extrapolated recommendation from 161
category I or II evidence 162 D Directly based on category IV evidence or extrapolated recommendation from 163
category I, II, or III evidence 164 LB Laboratory Based 165 NR Not rated 166 167 Summary of Conflict of Interest Disclosures 168
The following is a summary of interests disclosed on Work Group members’ Conflict 169 of Interest Disclosure Statements (not including information concerning family member 170 interests). Completed Conflict of Interest Disclosure Statements are available upon 171 request. Conflicts of interest disclosure statements for JTF are available on its web site. 172
173 Work Group Member Disclosures David B.K. Golden, MD (chair) Joann Blessing-Moore, MD (JTF liaison) Jeffrey Demain, MD David Graft, MD Theodore Freeman, MD Michael Tankersley, MD James Tracy, MD
174 Resolution of Potential Conflicts of Interest 175
The Joint Taskforce recognizes that experts in a field are likely to have interests that 176 could come into conflict with development of a completely unbiased and objective 177 practice parameter. To take advantage of that expertise, a process has been developed 178 to prevent potential conflicts from influencing the final document in a negative way. 179
At the workgroup level, members who have a potential conflict of interest either do 180 not participate in discussions concerning topics related to the potential conflict or if they 181 do write a section on that topic, the workgroup completely rewrites it without their 182 involvement to remove potential bias. In addition, the entire document is reviewed by 183 the Joint Taskforce and any apparent bias is removed at that level. Finally, the practice 184 parameter is sent for review both by invited reviewers and by anyone with an interest in 185 the topic by posting the document on the web sites of the ACAAI and the AAAAI. 186
How this practice parameter was developed 187
The Joint Taskforce on Practice Parameters (JTF) 188
The Joint Taskforce on Practice Parameters is a 12-member taskforce consisting of 189 six representatives assigned by the American Academy of Allergy, Asthma & 190 Immunology and six by the American College of Allergy, Asthma & Immunology. This 191 taskforce oversees the development of practice parameters; selects the workgroup 192 chair(s), reviews drafts of the parameters for accuracy, practicality, clarity and broad 193 utility of the recommendations for clinical practice. 194
The Stinging Insect Hypersensitivity Practice Parameter Workgroup 195
The Stinging Insect Hypersensitivity Practice Parameter Update 2016 workgroup was 196 commissioned by the JTF to develop practice parameters that address insect stings. The 197 Chair, David B.K. Golden, MD, invited workgroup members to participate in the 198 parameter development who are considered to be experts in the field. Workgroup 199 members have been vetted for financial conflicts of interest by the JTF and their COIs 200 have been listed in this document and are posted on the JTF web site at 201 http://www.allergyparameters.org . Where a potential COI is present, the potentially 202 conflicted workgroup member was excluded from discussing relevant issues. 203
The charge to the workgroup was to use a systematic literature review, in 204 conjunction with consensus expert opinion and workgroup-identified supplementary 205 documents to develop a Practice Parameter that provides a comprehensive approach for 206 Insect Hypersensitivity based on the current state of the science. 207
Protocol for Finding Evidence 208 209
A search of the medical literature was performed using a variety of terms that were 210 considered to be relevant for this practice parameter. Literature searches were performed on 211 PubMed, Medline, Medscape, Google Scholar, and the Cochrane Database of Systematic 212 Reviews. The time frame for most searches was 2011 to 2015, but some topics required 213
searches for an expanded timeframe from 1960 to present. The searches included only English 214 language articles. 215
Search terms included insect venom, Hymenoptera venom, insect sting, venom 216 immunotherapy, venom skin tests, venom diagnostic tests, serum tryptase, mastocytosis, ACE 217 inhibitors, beta-blockers, basophil activation tests, recombinant venom allergens, venom 218 component tests, fire ant, stinging ant, epinephrine, rush immunotherapy, Kounis syndrome, 219 and large local reactions. The search was narrowed by adding the terms allergy and 220 anaphylaxis. More focused searches were also used (eg, duration of VIT, discontinuing VIT). All 221 reference types were included in the results. Search results were screened for relevance, and 222 for the quality of the data and the analysis. 223
References identified as being relevant were searched for additional references and 224 these also were searched for citable references. In addition, members of the workgroup were 225 asked for references that were missed by this initial search. Initial search results yielded 1135 226 references, and additional references were suggested by work group members. Many of the 227 references were excluded because of poor study design or lack of relevance. The 215 228 references cited in this practice parameter represent the best quality and most relevant 229 evidence for the discussion and recommendations made herein. 230
While the ideal type of reference would consist of a randomized double-blind placebo-231 controlled study, the topic of this practice parameter is represented by very few such studies. 232 Consequently, it was necessary to use observational studies, case series, basic laboratory 233 reports, and expert review articles to develop a document that addresses most of the issues 234 included in this Practice Parameter. 235 236 Table of Contents 237 238 Preface 239 240 What’s New and What’s Different 241 242 Executive Summary 243 244 Algorithm and Annotations 245 246 Summary Statements 247 248 Stinging Insects and Venom Allergens 249
A. Classification 250 B. Cross Reactivity 251 252
The Clinical Spectrum of Venom Allergy 253 A. Categories of Adverse Sting Reactions 254 B. Definitions of Specific Venom Allergic Conditions 255
256 Prevalence, Natural History, Prevention 257
A. Epidemiology and Natural History 258 B. Prevention of Insect Sting Allergy 259 C. Indications for referral to an allergist 260 261
Diagnosis of Venom/Sting Allergy, Differential Diagnosis 262 A. Diagnosis of IgE-Mediated Venom Allergy 263
a. Skin tests 264 b. In vitro tests 265 c. New diagnostic methods 266
B. Mast cell disorders and Insect Sting Allergy 267 268
Management of Venom/Sting Allergy 269 A. Immediate Treatment 270 B. Venom Immunotherapy 271
a. Criteria for VIT 272 b. Large local reactors 273 c. Cutaneous systemic reactors 274 d. Selection of venoms for VIT 275
e. Dosage schedules for VIT 276 f. Problems during VIT 277 g. Duration of VIT 278
C. Fire Ant Immunotherapy 279 References 280
281
PREFACE 282 283
284 The objective of ‘‘Stinging insect hypersensitivity: a practice parameter update’’ is to improve 285
the care for patients with stinging insect hypersensitivity. This parameter is intended to refine 286 guidelines for the use and interpretation of diagnostic methods and for the institution and 287 implementation of measures to manage stinging insect hypersensitivity, with particular emphasis 288 on the appropriate use of immunotherapy with venoms (venom immunotherapy [VIT]) or whole-289 body extracts. 290
291 The document ‘‘Stinging insect hypersensitivity: a practice parameter update 2016’’ is the fourth 292 iteration of this parameter. The first was published in 1999 (Portnoy JM, Moffitt JE, Golden DB, 293 Bernstein IL, Dykewicz MS, Fineman SM, et al. Stinging insect hypersensitivity: a practice 294 parameter. J Allergy Clin Immunol 1999;103:963-80), and the first update was published in 2004 295 (Moffitt JE, Golden DB, Reisman RE, Lee R, Nicklas R, Freeman T, et al. Stinging insect 296 hypersensitivity: a practice parameter update. J Allergy Clin Immunol 2004;114:869-86, and there 297 was an update in 2011 highlighting advances in diagnosis and management of insect sting allergy 298 (Golden DBK, Moffitt J, Nicklas RA, AAAAI. Stinging insect hypersensitivity: A practice parameter 299 update 2011. J Allergy Clin Immunol 2011;127:852-4.). The working draft of this 2016 update 300 was prepared by a workgroup chaired by David B. K. Golden, MD, and was revised and edited by 301 the Joint Task Force on Practice Parameters. Preparation of this draft includes a review of the 302 recent medical literature using a variety of search engines, such as PubMed and Ovid. Published 303 clinical studies were rated as defined in the preamble by category of evidence and used to 304 establish the strength of the recommendations in the summary statements. It was then reviewed 305 by experts on insect sting allergy selected by the sponsoring organizations of the AAAAI and the 306 ACAAI, as well as being placed online for comments from the entire membership of both 307 organizations. Based on this process, this parameter represents an evidence-based document. 308 309
This document is similar in format to the previous iterations, but it has been considerably re-310 organized to make it easier for the reader to find the answers to specific questions and the 311 supportive evidence. It should be noted that with respect to diagnosis and treatment, the use of 312 the terms venom immunotherapy, VIT, venom testing, and venom refers to both venom and 313 imported fire ant whole-body extracts unless otherwise stated. The annotated algorithm in this 314 document summarizes the key decision points for the appropriate use of VIT (Fig E1). It has been 315 extensively revised to reflect changes in the recommended evaluation and treatment of insect-316 allergic patients. In this update, we introduce a new section on What’s New and What’s Different 317 in the field. There are some important changes in several areas of this document that address 318 techniques and interpretation of diagnostic tests, selection of patients for VIT, and risk factors for 319 severe anaphylaxis to stings. These new features of the 2016 update are summarized in a new 320 section on “What’s New”. As our experience with, and understanding of, VIT has evolved since it 321 was introduced in 1979, the recommendations made in the product package insert have become 322 out of sync with the published evidence base that is available for clinical guidance. For the 323
attention and consideration of the clinician, these are listed in a new section on “What’s 324 Different”. There remain important areas of uncertainty that must be addressed in focused 325 Practice Parameters when the evidence becomes available from future clinical observations and 326 research. 327
The Joint Task Force on Practice Parameters and the contributing authors wish to thank the 328 ACAAI and the AAAAI for their continued and/or past support of parameter development. The 329 Task Force would also like to thank the contributors to this parameter who have been so generous 330 with their time and effort. The members of the workgroup and the Task Force acknowledge the 331 contributions made by Dr. Robert Reisman and his dedication to this effort over many years, and 332 we dedicate this update to his memory. 333 334 335 336 WHAT’S NEW AND WHAT’S DIFFERENT 337 338 What’s New? 339 Every section of this Update contains new evidence with references and discussion. Many of 340 these are of great clinical importance and some of them warrant new sections for 341 comprehensive review. Some of these address new issues and observations, and some of them 342 simply add elements that have been missing from previous documents. Not all of these issues 343 have clear-cut answers, but guidance is provided based on the available evidence and the 344 experience of the experts in the field. 345 346 1. Updated discussion of indication for VIT in adults with cutaneous systemic reactions: 347
At least 2 prospective studies show <2% chance of progression and no severe reactions. 348 Retrospective 349 studies have major selection and recall bias. There is still the option for VIT when 350 considering high risk factors and quality of life concerns. (see Table 3). 351
352 2. New section on mast cell disorders and measurement of basal serum tryptase. 353
o Clinical significance of elevated basal serum tryptase? (increased risk of severe 354 anaphylaxis to stings before during and after VIT) 355
o When to measure tryptase? (patients with hypotension or severe anaphylaxis, and 356 consider in all patients who are candidates for VIT) 357
o What to do with abnormal results? (recognize increased risk, monitor for increasing level, 358 consider bone marrow biopsy, give VIT indefinitely) 359
o Mastocytosis in patients with insect sting allergy (estimated 2% frequency) 360 o Insect allergy in patients with mastocytosis (25% frequency; most common cause of 361
anaphylaxis 362 in mastocytosis patients; can be the presenting sign of indolent systemic mastocytosis) 363
o VIT in patients with mast cell disorders (significant benefit but higher than average 364 failure rate, and more than average systemic reactions to VIT) 365
366 3. New section on technique and interpretation of venom skin tests. 367
• Use the volume of injection (0.02 – 0.03 mL vs. 0.05 mL), or size of bleb (3-4 mm) 368 technique for intradermal skin tests? 369
• Is a positive test a wheal of 3 mm or 5 mm diameter? 370 371 4. New section on methods and materials for diagnostic tests for insect sting allergy. 372
• recombinant/component resolved diagnosis 373 • basophil activation test 374
375 5. New section on risk of cardiovascular medications in insect allergic patients. 376
Beta-blockers More risk to change medication than to not change 377 More risk to stop VIT than to continue 378
Less risk in patients on VIT than in untreated patients 379 ACEI Inconsistent literature 380 Less risk in patients on VIT than in untreated patients 381
6. New guidance on assessment and stratification of the risk of anaphylaxis to stings (when 382 considering 383 prescription of epinephrine injectors, or recommendation of venom skin tests or 384 immunotherapy): 385
High Risk Severe anaphylaxis, elevated basal serum tryptase, honeybee allergy, 386 frequent exposure, age/medical conditions 387
Low Risk children with cutaneous systemic reactions, large local reactors, 388 asymptomatic sensitization, on treatment with VIT, after discontinuing VIT 389
390 7. New content on VIT: Protocol, Procedures, Problems, and Special circumstances: 391
• Starting dose for skin tests and for VIT: reported safe at 1 mcg/mL for ST, 1 mcg for 392 VIT 393
• Up-dosing regimens and maintenance doses: semi-rush and rush are safe, ultra-rush 394 associated with more systemic reactions; 50 mcg dose in children, 100-200 dose mcg in 395 adults) 396
• VIT in Pregnancy: few data; no known problems; generally safer to continue than stop 397 • Maintenance interval gradually increased from 4 weeks to 8 weeks during the initial 398
years of treatment, and later up to12 weeks (3-4 months) 399 • Management of adverse reactions: minimal adjustment for large local reactions; for 400
repeated systemic reactions, try single venom with pre-medication, consider rush-VIT 401 and/or omalizumab 402
• Duration: 5 years is better than 3 years; longer treatment recommended in high-risk 403 patients; 3 years may be sufficient in children) 404
405 406 What’s Different? 407
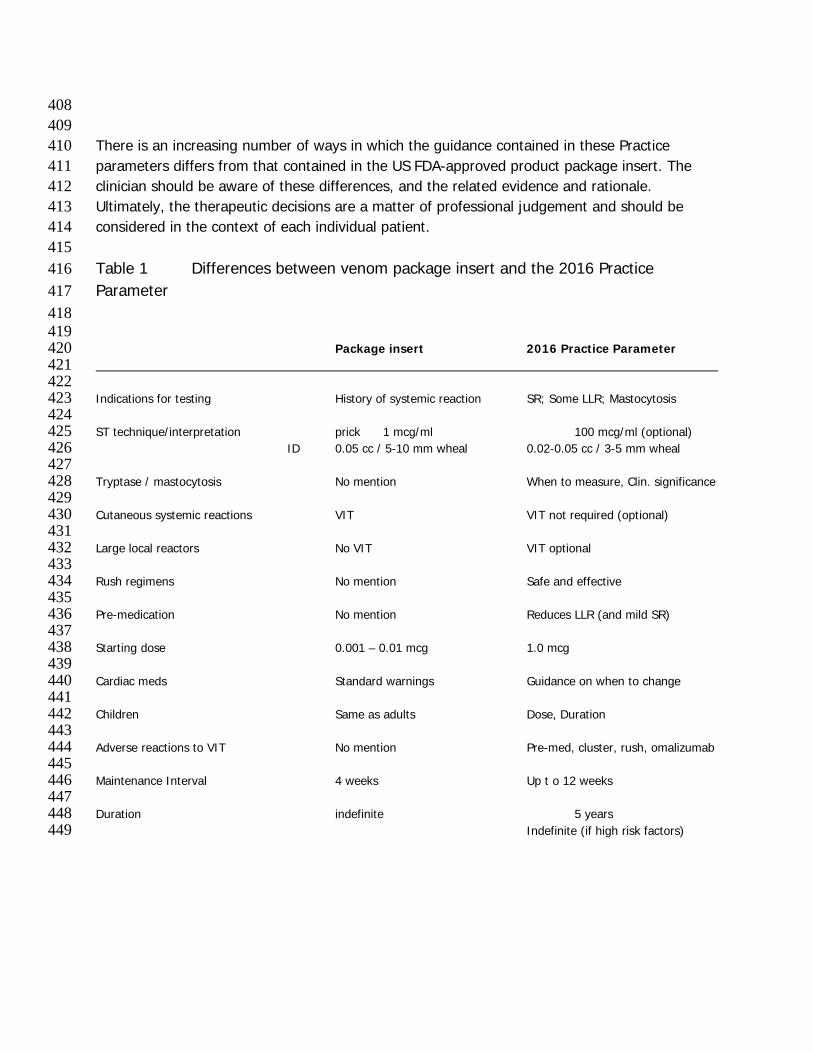
408 409 There is an increasing number of ways in which the guidance contained in these Practice 410 parameters differs from that contained in the US FDA-approved product package insert. The 411 clinician should be aware of these differences, and the related evidence and rationale. 412 Ultimately, the therapeutic decisions are a matter of professional judgement and should be 413 considered in the context of each individual patient. 414 415 Table 1 Differences between venom package insert and the 2016 Practice 416 Parameter 417 418 419 Package insert 2016 Practice Parameter 420 421 422 Indications for testing History of systemic reaction SR; Some LLR; Mastocytosis 423 424 ST technique/interpretation prick 1 mcg/ml 100 mcg/ml (optional) 425
ID 0.05 cc / 5-10 mm wheal 0.02-0.05 cc / 3-5 mm wheal 426 427 Tryptase / mastocytosis No mention When to measure, Clin. significance 428 429 Cutaneous systemic reactions VIT VIT not required (optional) 430 431 Large local reactors No VIT VIT optional 432 433 Rush regimens No mention Safe and effective 434 435 Pre-medication No mention Reduces LLR (and mild SR) 436 437 Starting dose 0.001 – 0.01 mcg 1.0 mcg 438 439 Cardiac meds Standard warnings Guidance on when to change 440 441 Children Same as adults Dose, Duration 442 443 Adverse reactions to VIT No mention Pre-med, cluster, rush, omalizumab 444 445 Maintenance Interval 4 weeks Up t o 12 weeks 446 447 Duration indefinite 5 years 448 Indefinite (if high risk factors) 449
450 451 EXECUTIVE SUMMARY 452 453 The primary focus of the Stinging Insect Practice Parameter over the years has been to provide 454 a working framework for the management of stinging insect hypersensitivity. Every effort has 455 been made to incorporate data driven and expert consensus recommendations. Since the most 456 recent iteration in 2011 many new, relevant and practical observations have occurred. This 457 parameter will attempt to address many of these observations and include contemporary 458 recommendations for this potentially lethal condition. Throughout this document, the use of 459 the terms venom immunotherapy, VIT, venom testing, and venom refers to both venom and 460 imported fire ant whole-body extracts unless otherwise stated. 461 While most insect stings produce a transient local reaction that can last up to several days and 462 generally resolves without treatment. Marked local swelling extending from the sting site is 463 usually an IgE-mediated late-phase reaction. The risk of a systemic reaction in patients who 464 experience large local reactions is no more than 5% to 10%. More serious anaphylactic sting 465 reactions account for at least 40 deaths each year in the United States.6 It is estimated that 466 potentially life-threatening systemic reactions to insect stings occur in 0.4% to 0.8% of children 467 and 3% of adults. 468 469 Systemic reactions are characterized by many different signs and symptoms, including any 470 combination of urticaria and angioedema, bronchospasm, edema of the large airway, 471 hypotension, or other clinical manifestations of anaphylaxis. The most serious anaphylactic 472 reactions involve the cardiovascular and respiratory systems and are potentially life-threatening. 473 The most common cardiovascular reaction is hypotension. Respiratory symptoms include 474 symptoms of upper or lower airway obstruction. Laryngeal edema and circulatory failure are the 475 most common causes of death from anaphylaxis. Patients who have a history of a systemic 476 reaction to an insect sting should: (1) be educated in avoidance of stinging insects, (2) carry 477 epinephrine for emergency self- administration and be instructed in its appropriate indications 478 and administration, (3) undergo testing for specific IgE antibodies to stinging insects, (4) be 479 considered for immunotherapy (with insect venom or fire ant whole-body extract) if test results 480 for specific IgE antibodies are positive, and (5) consider carrying medical identification for 481 stinging insect hypersensitivity. 482 483 The prevalence of a history of prior systemic reaction to a sting is about 3% in adults and less 484 than 1% in children. Large local reactions are reported by almost 10% of adults. Positive serum 485 or skin tests for venom IgE are present in more than 20% of normal adults, especially in the 486 months after a sting. However, only 5% to 15% of those with such asymptomatic sensitization 487 will have a systemic reaction to a subsequent sting, and most will lose the sensitivity over time. 488 In contrast, patients with a history of anaphylaxis to a sting have an average of almost 50% 489 frequency of systemic reaction to a sting. Patients with large local reactions have less than 10% 490
chance of a systemic reaction (and less than 5% chance of anaphylaxis). However, no test 491 predicts the severity of a sting reaction (other than basal serum tryptase). 492 493 Identification of the insect responsible for the sting reaction can be very useful in establishing 494 the diagnosis, prescribing treatment, and educating patients in avoidance measures. Different 495 insects have different nesting and behavioral characteristics and behaviors that can be distinct 496 and specific. For example, the most common species of in the U.S. build their nests in the 497 ground and therefore can be encountered during yard work, farming, and gardening. Hornets 498 are extremely aggressive and build large nests, usually in trees or shrubs, which, despite their 499 size, often go undetected. Wasps build honeycomb nests often in shrubs and under eaves of 500 houses or barns and, like yellow jackets and hornets, are scavengers, increasing the likelihood 501 of their presence at outdoor events where food and drink are being served. Domestic 502 honeybees are found in commercial hives, whereas wild honeybees might build their nests in 503 tree hollows or old logs. Africanized honeybees are hybrids developed from interbreeding of 504 domestic honeybees and African honeybees in South America and are much more aggressive 505 than domestic honeybees, often attacking in swarms. Usually honeybees, and occasionally other 506 stinging insects, leave a barbed stinger and attached venom sac in the skin after they sting. The 507 imported fire ant, which can be red or black, builds nests in mounds of fresh soil that can be 1 508 to 2 feet in diameter and elevated at least several inches. These ants are very aggressive, 509 particularly if their nests are disturbed, and often sting multiple times in a circular pattern, 510 producing sterile pseudo-pustules that have a distinctive appearance. 511 512 Patients who have experienced a systemic reaction to an insect sting should be referred to an 513 allergist-immunologist for evaluation including skin testing or in vitro testing for specific IgE 514 antibodies to insects. Extracts of honeybee, yellow jacket, white-faced hornet, yellow hornet, 515 and wasp venom are available for skin testing and VIT. Although there is no venom extract 516 available for commercial use in patients with suspected fire ant hypersensitivity, whole-body 517 extract is available and contains relevant venom allergens, the effectiveness of which is 518 supported by accumulating evidence. It is generally accepted that a positive intradermal skin 519 test response to insect venom at a concentration of less than or equal to 1.0 mcg/mL 520 demonstrates the presence of specific IgE antibodies. A survey (by the Joint Task Force on 521 Practice Parameters) of practicing allergists showed that there is variation in the reported 522 technique for the performance and interpretation of intradermal skin tests, so the clinician must 523 be consistent in the use of the test. When there is a clear history of sting anaphylaxis and skin 524 tests are negative, then serum IgE antibodies should be measured, and if necessary, skin tests 525 should be repeated after 3-6 months. Skin testing with fire ant whole-body extract is considered 526 indicative of specific IgE antibodies if a positive response occurs at a concentration of 1:100 527 wt/vol or less by using the skin prick method or 1:1,000 wt/vol or less by using the intradermal 528 method. There are tests in development that may improve the accuracy of diagnosis and 529 treatment of insect sting allergy. Component resolved IgE tests using recombinant venom 530 allergens may improve the specificity of diagnosis and treatment by distinguishing specific from 531 cross-reactive sensitivities (especially between honeybee and vespid venoms). The basophil 532
activation test may improve the sensitivity of diagnostic testing and prediction of which patients 533 are at risk for severe anaphylaxis. 534 535 Our understanding of the role of mast cell disease and its unique relationship to insect allergy 536 continues to evolve compared to other causes of life-threatening anaphylaxis. A growing body 537 of evidence shows that patients with severe insect sting reactions should be evaluated for mast 538 cell disorders. Some experts recommend a basal serum tryptase measurement as part of the 539 assessment of all patients with a systemic reaction to insect sting. Basal serum tryptase should 540 be measured when there is a history of severe insect sting anaphylaxis (especially with 541 hypotension and/or the absence of urticaria), and when skin and serum tests for venom-specific 542 IgE are negative. Tryptase measurement should be considered when patients have systemic 543 reactions during VIT, and when discontinuing VIT. Patients with mastocytosis should be tested 544 for Hymenoptera venom sensitivity because insect stings are the most common cause of 545 anaphylaxis in such patients, and their reactions are more likely to be severe. The cost and 546 burden of testing for basal tryptase should be considered. 547 548 There are patients who have negative skin test responses who give a convincing history of 549 anaphylaxis after an insect sting, some of whom experienced serious symptoms, such as upper 550 airway obstruction or hypotension. For such individuals, it is advisable to measure basal serum 551 tryptase, and to consider in vitro testing for IgE antibodies and/or repeat skin testing before 552 concluding that immunotherapy is not indicated. Either or both of the serum measurements of 553 specific IgE for insect venom/ fire ant whole- body extract and the skin test response might be 554 temporarily non- reactive within the first few weeks after a systemic reaction to an insect sting 555 and might require retesting in 6 weeks. Although one might want to wait for this period of time 556 before initial testing, it could be important to skin test patients without waiting, especially if 557 rapid initiation of VIT is required. Rarely (<1% of patients with a convincing history of systemic 558 reaction to a sting), patients can have an anaphylactic reaction from a subsequent sting despite 559 negative skin and in vitro test results. Some of these patients might have underlying systemic 560 mastocytosis. 561 562 Patients who have a history of an allergic reaction to an insect sting and have a positive skin or 563 in vitro test result for specific IgE antibodies to insects might be at risk for subsequent life-564 threatening reactions if re-stung. Therefore, venom immunotherapy should be considered in 565 such patients. Approximately 30% to 60% of patients with a history of systemic allergic reaction 566 to an insect sting who have specific IgE antibodies detectable by means of skin or in vitro 567 testing will experience a systemic reaction when re- stung. Because of this lower than optimal 568 positive predictive value, it has been suggested that patients can be better selected for 569 immunotherapy on the basis of the results of an intentional sting challenge. Sting challenges, 570 however, are not consistently reproducible and are associated with considerable risk. The 571 standard management of stinging insect hypersensitivity in the United States does not include a 572 sting challenge. 573 574
VIT is generally not necessary in children who have experienced isolated cutaneous systemic 575 reactions without other systemic manifestations after an insect sting. In a change from previous 576 recommendations, adults who have experienced only cutaneous manifestations of a systemic 577 reaction are also considered to be at low risk for a severe reaction and do not require VIT. VIT 578 is also generally not necessary for patients who have had only a large local reaction because 579 the risk of a systemic reaction to a subsequent sting is relatively low. In fact, the vast majority 580 of patients who have had a large local reaction do not need to be tested for specific IgE 581 antibodies to insect venom. VIT significantly reduces the size and duration of large local 582 reactions and thus might be useful in subjects who have unavoidable and/or frequent large 583 local reactions. VIT is extremely effective in reducing the risk of a subsequent systemic 584 reaction from an insect sting to less than 5%, and sting reactions that occur during VIT are 585 usually milder than those experienced before VIT. In patients at low risk for a severe reaction to 586 a sting, such as those with large local or cutaneous systemic reactions, there may be special 587 circumstances that would favor treatment, such as frequent exposure, impaired quality of life, 588 or underlying medical conditions. In these patients, the decision regarding initiation of VIT is 589 based upon a risk/benefit discussion with the patient. 590 591 Selection of venom and dose schedules is discussed in the main document. Adverse effects are 592 typically minor, though anaphylaxis may occur; therefore close monitoring is warranted. The full 593 dose of 100 mcg must be achieved to ensure optimal clinical protection (50 mcg in children). 594 Large local reactions are most common but can generally be tolerated. Antihistamines help to 595 limit the reaction. If systemic reactions recur, rush VIT (sometimes with omalizumab pre-596 treatment) is usually successful. Beta-blockers and ACE inhibitors may increase the risk of 597 anaphylaxis to VIT, but the published evidence is inconsistent. The benefits of VIT clearly 598 outweigh the potential risks associated with beta-blockers or ACE inhibitors in those patients 599 with anaphylaxis to stinging insects who also have cardiovascular disease requiring these 600 medications. Once initiated, VIT should usually be continued for at least 3 to 5 years. Evidence 601 suggests that despite the persistence of a positive skin test response, 80% to 90% of patients 602 will not have a systemic reaction to an insect sting if VIT is stopped after 3 to 5 years. There 603 are no specific tests that can distinguish which patients will relapse after stopping VIT, but 604 there is a higher risk in some patients than in others. Relapse is less likely with 5 years than 605 with 3 years of VIT. Although most patients can safely discontinue immunotherapy after this 606 period of time, some patients with a history of severe anaphylaxis with shock or loss of 607 consciousness still might be at continued risk for a systemic reaction if VIT is stopped, even 608 after 5 years of immunotherapy. For this reason, some experts recommend an extended 609 duration of immunotherapy, possibly indefinitely, in such patients. Other criteria suggested for 610 stopping VIT include a decrease in serum venom-specific IgE to insignificant levels or 611 conversion to a negative skin test response. Some patients have relapsed despite negative 612 venom skin test responses. Repeat skin (or venom-specific IgE serum) testing is not required 613 for consideration of discontinuing VIT. Measurements of venom-specific IgG antibodies have no 614 predictive value when discontinuing VIT. The decision on stopping VIT requires a context-615 sensitive flexibility based on the available evidence and the preference of the patient. 616
617 The optimal duration of fire ant immunotherapy is less well defined. Most allergists consider 618 stopping fire ant immunotherapy after a specified period (usually 3-5 years) either empirically or 619 only when skin or in vitro test results become negative. Until further data are available, a 620 definitive recommendation about the duration of immunotherapy for fire ant sting allergy 621 cannot be made. Less is known about the natural history of fire ant venom hypersensitivity and 622 the effectiveness of immunotherapy than is known about other stinging insects. Fire ant whole- 623 body extract has been shown to contain relevant venom allergens, and evidence continues to 624 accumulate, despite the lack of any placebo-controlled study, to support the effectiveness of 625 immunotherapy with fire ant whole-body extract. Recommendations for immunotherapy 626 with fire ant whole-body extract are generally the same as those for VIT. 627 628 Patients who have experienced a systemic reaction to an insect sting should be referred to an 629 allergist, and should be given a prescription for an injectable epinephrine device, be instructed 630 in its proper use, and be advised to carry it with them at all times. Some patients who 631 experience anaphylaxis might require more than one injection of epinephrine, so prescription 632 of more than 1 epinephrine injector should be considered. Patients and advocates who might 633 be administering epinephrine should be taught how to administer this drug and under what 634 circumstances this should be done. Although patients with coexisting conditions, such as 635 hypertension or cardiac arrhythmias, or concomitant medications, such as b-adrenergic blocking 636 agents, might require special attention, there is no contraindication to the use of epinephrine in 637 a life-threatening situation, such as anaphylaxis. In patients who have a relatively low risk of a 638 severe anaphylactic reaction from a sting, the decision on whether to carry injectable 639 epinephrine can be determined by discussion between the patient and physician. Patients with a 640 low risk of reaction are those with a history of only large local reactions to stings or of strictly 641 cutaneous systemic reactions, those receiving maintenance VIT, and those who have 642 discontinued VIT after more than 5 years of treatment. Factors associated with a higher risk 643 include a history of extreme or near-fatal reactions to stings, systemic reactions during VIT (to 644 an injection or a sting), severe honeybee allergy, underlying medical conditions, or frequent 645 unavoidable exposure. 646 647 There remain some unmet needs and unanswered questions in the diagnosis and treatment of 648 insect sting hypersensitivity. Managing the individual with a convincing history of insect related 649 anaphylaxis, but negative or inconclusive diagnostic testing remains a clinical dilemma. 650 Improved diagnostic sensitivity and specificity with better positive predictive value must await 651 studies to validate new tests, such as those using recombinant allergens or epitopes, or those 652 designed to detect basophil activation or basophil sensitivity. To better predict which patients 653 will have a systemic reaction to a sting after stopping VIT, there is a need for a test that can 654 identify when permanent tolerance has been achieved. There is a need for a study of 655 discontinuing VIT in low-risk patients after exactly 3 years of VIT (not a range of 3-7 years as in 656 previous studies). There is an increasing number of patients who have been on VIT for 657 extended periods because of high risk factors. Some patients have had systemic reactions up to 658
13 years after stopping VIT, even some who had negative skin tests. There is a need for a 659 controlled study of discontinuation after 15 to 30 years in ‘‘high-risk’’ patients with negative skin 660 test responses. One of the greatest concerns is that 50% of fatal sting reactions occur with the 661 first reaction, and therefore cannot be prevented by current standards of testing and treating 662 only those who have a history of reaction. Unfortunately measures of venom-specific IgE (skin 663 or serum tests) have poor positive predictive value, so there is a need for an effective screening 664 test to detect those who are at greatest risk for a severe reaction to a future sting so that VIT 665 can be recommended with greatest efficiency. 666 667
ALGORITHM 668
669
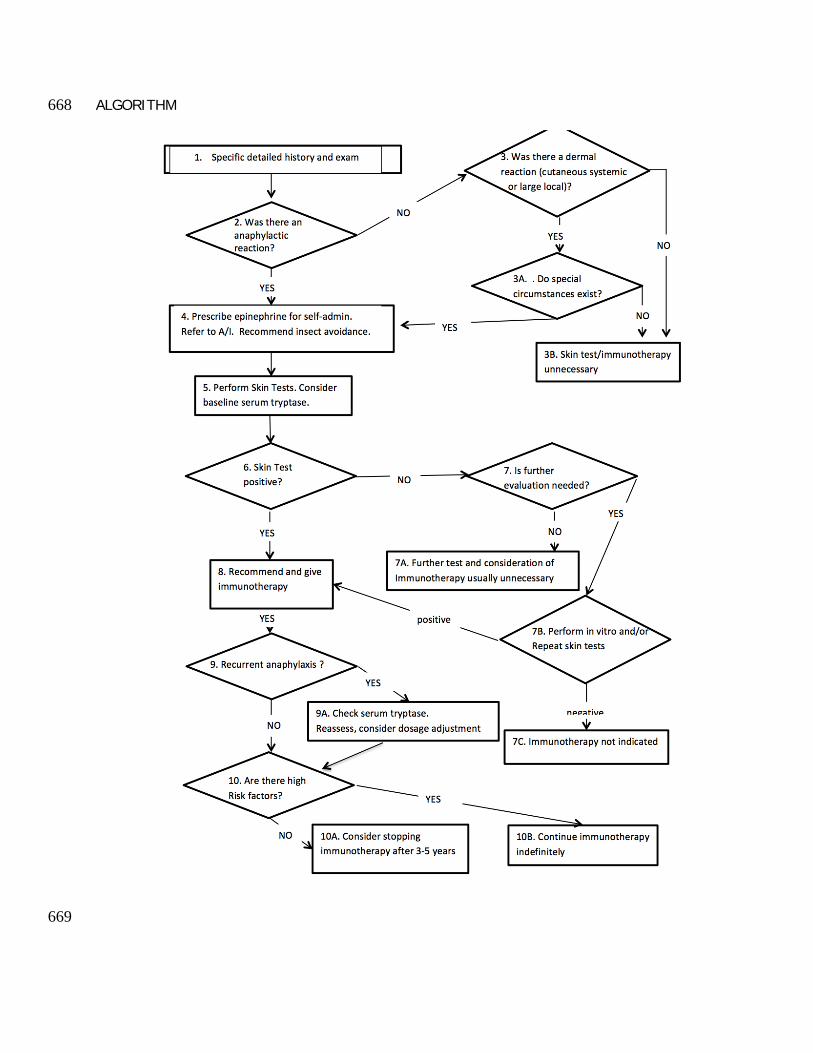
Annotations to Fig E1 670 671
Box 1: Specific detailed history and physical examination 672 Patient presents with a history of insect sting reaction. Although insects sting many 673
persons each year, most subjects do not have abnormal reactions and do not need medical 674 attention. Most who are stung have only local reactions and require only symptomatic, if 675 any, treatment. Persons who have a history of insect stings causing systemic reactions 676 require evaluation and usually preventative treatment. Reactions can range from large local 677 swelling to life-threatening systemic reactions. Delayed or toxic reactions can also occur. 678 Obtaining a careful history is important in making the diagnosis of insect sting reaction. 679
680 Identification of the responsible insect might be helpful in the diagnosis and treatment. 681
Patients should be encouraged to bring the offending insect, when available, to the 682 physician for identification. The physician should determine whether the patient was stung 683 once or multiple times. 684
Factors that might be helpful in identification include the following: 685 o the patient’s activity at the time of the sting (eg, cutting a hedge) 686 o the location of the person at the time of the sting (eg, close to nesting places for 687
stinging insects), the type of insect activity in the area where the patient was 688 stung, and 689
o visual identification of the insect. 690
Identification of stinging insects by patients is not always reliable. The presence of a 691 stinger, which is left most commonly by honeybees, or the presence of a pustule as a 692 result of an imported fire ant sting (up to 24 hours or longer) might help in insect 693 identification. 694
695 Box 2: Was there an anaphylactic reaction? 696
Most insect stings result in local reactions. These include the following: 697
o redness, 698 o swelling, and 699 o itching and pain. 700
Large local reactions usually include the following features: 701
o increase in size for 24 to 48 hours, 702 o swelling to more than 10 cm in diameter contiguous to the site of the sting, and 703 o 5 to 10 days to resolve. 704
Systemic reactions can include a spectrum of manifestations not contiguous with the site of 705 the sting, ranging from mild to life- threatening. Cutaneous systemic reactions are limited to 706 skin manifestations, whereas anaphylaxis includes hypotension or involvement of at least 2 707
organ systems. These may include the following: 708
o cutaneous (eg, urticaria, angioedema, itching, flushing), 709 o bronchospasm, 710 o upper airway obstruction (eg, tongue or throat swelling and laryngeal edema), 711 o cardiac (eg, arrhythmias and coronary artery spasm), 712 o hypotension and shock, 713 o gastrointestinal (eg, nausea, vomiting, diarrhea, and abdominal pain), and 714 o neurological (eg, seizures). 715
716 Box 3, 3A, 3B: Was there a dermal reaction (cutaneous systemic or large 717 local)? 718
Most insect stings cause mild local reactions for which no specific treatment is usually 719 required. Some local reactions are manifested by extensive swelling surrounding the sting 720 site that can persist for several days or more and might be accompanied by itching, pain, or 721 both. Cold compresses might help to reduce local pain and swelling. Oral antihistamines and 722 oral analgesics might also help to reduce the pain or itching associated with cutaneous 723 reactions. Many physicians use oral corticosteroids for large local reactions, although definitive 724 proof of efficacy through controlled studies is lacking. Swelling (and even lymphangitis) may 725 be caused by mast cell mediator release and not by infection, so antibiotics are not indicated 726 unless there is clear evidence of secondary infection (a common misdiagnosis). 727
Large local reactions are usually IgE mediated but are almost always self-limited and 728 rarely create serious health problems. Patients who have previously experienced large local 729 reactions often have large local reactions to subsequent stings, and up to 10% might eventually 730 have a systemic reaction. Some patients who have had large local reactions seek guidance on 731 insect avoidance measures. In patients who have had large local reactions, it is optional to 732 prescribe injectable epinephrine for use if the patient experiences a systemic reaction in the 733 future. The vast majority of patients with large local reactions need only symptomatic care and 734 are not candidates for testing for venom-specific IgE or for VIT. There is, however, growing 735 evidence that VIT significantly reduces the size and duration of large local reactions and thus 736 might be useful in affected subjects with a history of frequent unavoidable large local reactions 737 and detectable venom-specific IgE. The decision to give VIT for patients with large local 738 reactions must be weighed against the added cost and potential inconvenience. 739 740
The usual criteria for immunotherapy include a history of a systemic reaction to an insect sting 741 and demonstration of venom- specific IgE by means of either skin or in vitro testing. However, 742 immunotherapy is usually not required for patients who have experienced only cutaneous 743 systemic reactions after an insect sting. In a prospective field-sting study of children, there was 744 a 10% chance of having a systemic reaction if re-stung (usually milder than their previous 745 sting reactions), and <3% chance of a more severe reaction. Prospective sting challenge 746 studies in adults showed <3% chance of a more severe reaction in such patients. VIT is still an 747 acceptable option if there are special circumstances, such as frequent exposure, or lifestyle 748
considerations (potential impairment in quality of life) and must be weighed against added cost 749 and potential inconvenience. There is evidence that VIT improves the quality of the patient’s life 750 in patients with cutaneous reactions. 751 752 The need to carry epinephrine autoinjectors can be determined by the patient/caregiver and 753 physician after discussion of the relative risk of anaphylaxis and the anticipated effect on 754 quality of life. In addition, the cost of autoinjectors and the inconvenience of having to 755 carry them should be considered when recommending that a patient have them available. 756 Although VIT is considered to be almost completely effective in preventing life-threatening 757 reactions to stings, carrying self-injectable epinephrine might still be desired, even during VIT, 758 and is subject to discussion between the patient/caregiver and the physician. Although most 759 physicians generally apply the same criteria in selecting patients to receive immunotherapy for 760 fire ant allergy, it is not established that patients (children or adults) with only systemic 761 cutaneous reactions are not at risk for serious systemic reactions to subsequent stings. 762 Because the natural history of fire ant hypersensitivity in patients who have only cutaneous 763 manifestations has not been elucidated and there is increased risk of fire ant stings in those 764 who live in areas in which fire ants are prevalent, immunotherapy can be considered for such 765 individuals. 766 767
768 Box 4: Prescribe epinephrine for self- administration/refer to an 769 allergist-immunologist/recommend insect avoidance 770
Injectable epinephrine should be prescribed, and the patient should be instructed in its 771 proper administration and use. Patients should also consider obtaining and carrying a medical 772 identification bracelet or necklace. A patient with a history of severe reaction should have 773 injectable epinephrine prescribed because even if the test result for venom-specific IgE is 774 negative, there is a small risk of another systemic reaction. Referral to an allergist is 775 appropriate for any patient who has had an allergic reaction and is indicated for any patient 776 who is a potential candidate for immunotherapy, as outlined in Box 6. Preventive 777 management includes measures to prevent subsequent stings and to prevent subsequent 778 systemic reactions if the patient is stung. 779
780 Box 5: Perform skin or in-vitro testing and consider measuring basal 781 serum tryptase 782
Skin or in-vitro tests should be performed on patients for whom VIT might be indicated. Skin 783 tests with increasing concentrations of fire ant extract are also used (see text section on fire 784 ants). Positive and negative controls should be placed during skin testing. 785
Detection of all potentially relevant sensitivities requires testing with all of the commercially 786 available bee and vespid venoms and might include fire ant extracts when the patient has 787 exposure to fire ant stings. The insect that caused the sting often cannot be reliably identified, 788 but even if it is clearly identified, the possibility exists of future reactions to other venoms to 789 which there is existing sensitization. However, fire ant is only included under special 790
circumstances (see text). Venoms might contain shared antigenic components. Cross-791 sensitization and extensive immunologic cross-reactivity have been demonstrated between 792 hornet and yellow jacket venoms (vespids); cross-reactivity is less extensive between Polistes 793 wasp and other vespid venoms and is infrequent between honeybee and vespid venoms. Fire 794 ant venom (and therefore fire ant whole-body extract) has very limited cross- reactivity with 795 other stinging insect venoms. 796 797 Compared to other causes of anaphylaxis such as foods or medications, the prevalence of mast 798 cell disorders is higher in patients who have had anaphylaxis to an insect sting. Therefore, 799 measurement of basal serum tryptase should be considered in all patients who are candidates 800 for VIT. Elevated basal serum tryptase is closely correlated with the risk of severe anaphylaxis 801 to stings, and is most frequently found in patients with reactions including hypotensive shock. 802 The frequency of abnormal basal tryptase is much lower in patients with less severe systemic 803 reactions to stings, and the clinical significance in these patients is less clear. There is a cost 804 and burden associated with abnormal results of basal tryptase (eg: bone marrow biopsy, 805 consultation with other specialists, anxiety associated with an abnormal test result). However an 806 abnormal result is associated with severe anaphylaxis to stings, increased risk of systemic 807 reactions during VIT (to a sting or venom injection), and greater risk of sting anaphylaxis after 808 stopping VIT. With these considerations in mind, measurement of basal serum tryptase is highly 809 recommended in patients who had hypotensive reactions to a sting, and should be considered 810 in other patients with systemic reactions to stings. Additionally, elevated basal tryptase may 811 indicate the presence of an occult mast cell disorder and may be present in sting-allergic 812 patients with negative venom allergy tests as well. 813 814 815 Box 6: Positive skin or in-vitro test response? 816 VIT is recommended for patients who have had a systemic insect sting reaction, who have a 817 positive skin or in-vitro test response, and who meet the criteria outlined in the annotation for 818 Box 3 There is no absolute correlation between the skin test reactivity or the level of venom-819 specific IgE and the severity of the reaction to a sting. Near-fatal and fatal reactions have 820 occurred in patients with barely detectable venom IgE antibodies by means of skin or in 821 vitro testing. 822 823 Box 7, 7A, 7B: Is further evaluation needed? 824 Patients might have venom-specific IgE not detected by skin testing, even though skin testing 825 is the most reliable and preferred diagnostic method to identify venom-specific IgE. Therefore it 826 is recommended that further evaluation for detection of venom- specific IgE be performed if 827 the skin test response is negative. This would include serum IgE assays for venom-IgE, and 828 repeat skin tests, and may include new modalities in the future. Patients with a history of systemic 829 reaction but with no detectable venom allergy should be tested for basal serum tryptase (if not 830 already done). 831 832
For patients who have had a severe systemic reaction to an insect sting, as described in 833 the preceding annotation, and who have negative venom skin test responses, it would be 834 prudent to verify this result with repeat skin and in vitro testing before concluding that VIT is 835 not necessary. If the response of either such test is positive, VIT is indicated. If repeat test 836 responses fail to demonstrate the presence of IgE antibodies, there is no indication for VIT, 837 though basal serum tryptase levels should be measured to assess for an underlying mast cell 838 disorder. 839 840 Box 8: Recommend and give VIT 841
VIT greatly reduces the risk of systemic reactions in stinging insect–sensitive patients with 842 an efficacy of up to 98%. Patients who have had a systemic reaction from an insect sting 843 and evidence of venom-specific IgE should therefore be advised to receive VIT. The goal of 844 VIT is primarily to prevent life-threatening reactions. A secondary benefit is that it might 845 alleviate anxiety related to insect stings. VIT has been shown to improve the quality of life. 846
Candidates for VIT should be informed in writing or verbally with documentation in the 847 record about the potential benefits and risks related to the procedure. Patients should receive 848 a description of the procedure and be informed that although the risk of anaphylaxis is 849 small, they must wait for 30 minutes after each injection and follow any other specific 850 policies and rules of the provider of the VIT. 851
In the opinion of some experts, all venoms eliciting positive responses for venom-specific 852 IgE should be included in the immunotherapy regimen, whereas others contend that with 853 knowledge of venom cross-reactivity and insect identification, only a single venom may be 854 needed for VIT, even if skin or in vitro test results for other stinging insects are positive. 855 Immunotherapy for patients with fire ant hypersensitivity consists of injections with a whole-856 body extract and should be initiated in patients with a history of a systemic reaction to a fire 857 ant sting who have a positive skin test response to whole-body extract or a positive in vitro 858 assay result. 859
VIT injections are generally administered once a week, beginning with doses no greater 860 than 0.1 to 1.0 mcg and increasing to a maintenance dose of 100 mcg of each venom (eg, 861 1 mL of an extract containing 100 mcg/mL of 1 venom or 300 mcg of mixed vespid 862 venom). The dosing interval and increments can be adjusted at the discretion of the 863 prescribing physician to accommodate the preferences of the physician and the tolerance of 864 the patient. The dosage schedule for fire ant immunotherapy is less well defined in terms of 865 starting dose and rapidity of buildup. Although most experts recommend a maintenance dose 866 of 0.5 mL of a 1:100 wt/vol concentration—and there is increasing evidence that this dose is 867 protective—a 1:10 wt/vol maintenance concentration has been recommended by some. The 868 interval between maintenance dose injections can be increased to 4-week intervals during the 869 first year of VIT and eventually to every 6 to 8 weeks during subsequent years. Rush 870 immunotherapy protocols have been used successfully and safely to treat flying 871 Hymenoptera and fire ant sting allergy and can be considered for routine use. 872
Patients with insect venom allergy who are taking angiotensin-converting enzyme inhibitors 873 (ACEI) or beta-adrenergic blocking agents are at greater risk for more serious anaphylaxis to a 874
sting. Therefore patients who have stinging insect hypersensitivity should not be prescribed 875 ACEI or beta- blockers unless absolutely necessary. The risk appears to be less during VIT, so 876 if the patient who has stinging insect hypersensitivity cannot discontinue these medications, 877 the decision to administer immunotherapy should be made on an individual basis after analysis 878 of potential risks and benefits. In patients who have had life-threatening reactions to stings 879 and take beta-adrenergic blocking medications, the risk of VIT has been judged to be less than 880 the risk of a life-threatening reaction to a future sting. 881 882 Box 9, 9A: Recurrent anaphylaxis 883 VIT at the accepted maintenance dosage is very effective but does not protect all patients. 884 For patients who have allergic reactions to insect stings while receiving maintenance 885 immunotherapy, it is first necessary to identify the culprit insect. If the insect is the same as 886 that causing the initial reaction, an increase in venom dose of up to 200 mcg per injection 887 might provide protection. If the culprit is unknown, further testing might be needed to 888 determine whether there is a new or untreated venom sensitivity before considering an 889 increase in the venom dose. Consider measuring basal serum tryptase because failure of VIT 890 can be related to underlying mast cell disorders. 891 892 Box 10, 10A, 10B: Are there high risk factors? Consider stopping VIT 893 after 3 to 5 years. 894 The package insert for the Hymenoptera venom extracts recommends that VIT be continued 895 indefinitely. Research on the discontinuation of treatment have suggested several 896 possible criteria such as the duration of treatment (3 to 5 years), a decrease in serum 897 venom-specific IgE to insignificant levels, or conversion to a negative skin test response. These 898 studies suggest that even when skin or serum tests for venom-IgE remain positive, approximately 899 90% of patients will not have a systemic reaction to an insect sting if VIT is stopped after 3 to 900 5 years and that any reaction to a future sting is usually less severe than the pre-VIT reaction. 901 Most patients should consider discontinuing VIT after 3 to 5 years, except in certain high-risk 902 patients described in the text (and Table 5). However, there always remains a small risk that 903 future systemic sting reactions could occur. In addition, severe reactions have occurred 904 several years after stopping VIT in a small number of patients whose skin test responses 905 became negative while receiving VIT (although most still had positive in vitro test results). 906 Conversely, the persistence of skin test reactivity does not mean that all such patients are at 907 increased risk of having a systemic reaction if subsequently stung. There are no specific tests 908 to distinguish which patients will relapse after stopping VIT, but there is a higher risk in 909 some patients than in others. A decision about the duration of VIT is made individually after 910 discussion between the patient and physician and might involve consideration of lifestyle, 911 occupation, coexistent disease, medications, severity of sting reactions, and other factors. Repeat 912 skin (or venom-specific IgE serum) testing is not required when considering discontinuation of 913 VIT. Patients with a history of severe anaphylaxis (severe airway obstruction, shock, or loss 914 of consciousness), still might be at continued risk for a severe systemic reaction if VIT is stopped 915 even after 5 years of treatment. For this reason, some recommend that immunotherapy be 916
continued indefinitely in such patients (see text for details). There is also a higher chance of 917 relapse in patients with elevated basal serum tryptase, those who had systemic reactions during 918 VIT (to an injection or a sting), and those who are more frequently stung. 919 The optimal duration of imported fire ant immunotherapy has not been clearly established. 920 Skin reactivity appears to be a poor indicator of the risk for a systemic reaction to fire ant 921 venom after fire ant immunotherapy. As a result, there is a great deal of variation in 922 recommendations regarding the duration of immunotherapy for fire ant allergy, with some 923 allergists recommending indefinite treatment. Most allergists recommend stopping 924 immunotherapy after a specific period (usually 3-5 years), either empirically or when skin test 925 responses become negative. Until further data are available, a definitive recommendation 926 about the duration of immunotherapy for fire ants cannot be made. 927 928
SUMMARY STATEMENTS 929 930 1. Evaluate subjects with a history of a systemic reaction to an insect sting for 931 the presence of venom-specific IgE. If venom-IgE is present these patients are at 932 increased risk for subsequent sting anaphylaxis, which can be prevented by VIT. 933 (Strong Recommendation; A Evidence) 934
2. Evaluate the patient for details of the history of any reactions to insect stings. 935 (Strong Recommendation; B Evidence) 936
3. Recommend to patients who have a history of systemic reactions to insect 937 stings: 938
a. effective measures to avoid insect stings. (Recommendation; D evidence); 939 b. the need to always carry an epinephrine auto-injector, to be familiar with 940 its proper use and when to use it or not use it, and to carry medical 941 identification (Strong Recommendation; B evidence); and 942 c. referral for evaluation by an allergist/immunologist, the utility of specific 943 IgE testing for stinging insect sensitivity and the potential advantages of 944 venom immunotherapy (testing is not necessary for patients in whom VIT is 945 not required) (Strong Recommendation; D Evidence). 946
4. Perform immediate hypersensitivity skin tests and/or in-vitro tests with 947 stinging insect venoms on patients who are candidates for VIT. (Strong 948 Recommendation; A Evidence) 949
5. If initial test results are negative in a patient with a clear history of systemic 950 sting reaction, further testing (in vitro testing, repeat skin testing, or both) should 951 be performed, as well as basal serum tryptase measurement. (Strong 952 Recommendation; C Evidence) 953
6. Physicians and patients should not expect the degree of sensitivity found on 954 skin and serologic tests for venom-specific IgE to reliably predict the severity of a 955 reaction to a sting, but it is a good predictor for the likelihood of any systemic 956 reaction. (Recommendation; B Evidence) 957
7. Consider measuring basal serum tryptase in all patients who are candidates 958 for VIT. (Recommendation; B Evidence) 959
8. Use skin tests as the preferred test for initial measurement of venom-specific 960 IgE. In vitro measurement of serum IgE should be used as a complementary or 961 alternative test. Test for all 5 venoms, with the possible exception of individual 962 patients in whom a single culprit is definitively known. (Recommendation; C 963 Evidence) 964
9. Consider measuring basal serum tryptase in patients with anaphylaxis to a 965 sting, especially in those with severe or hypotensive reactions, and in all those with 966 negative tests for venom-IgE. (Strong Recommendation; B Evidence) 967
10. Counsel patients with elevated basal serum tryptase about the clinical 968 significance of potential underlying mast cell disorders. (Recommendation; B 969 Evidence) 970
11. Consider testing patients with mastocytosis for insect venom sensitivity, and 971 identify other high risk factors for severe anaphylaxis to stings (including 972 medications). (Recommendation; D Evidence) Discuss with the patient the benefits 973 and risks for testing and for VIT. 974
12. Advise the patient to treat acute systemic reactions to insect stings like any 975 anaphylactic reaction, with timely 976
12a. epinephrine injection (Strong Recommendation; A Evidence) 977
12b. supportive therapy(Strong Recommendation; A Evidence) 978
12c. transport to an emergency department. (Strong Recommendation; C 979 Evidence) 980
981
13. Treat large local reactions symptomatically, with antihistamines, cold 982 compresses, and analgesics as needed. In severe cases a short course of oral 983 corticosteroids may be useful. Antibiotics are usually not necessary and should be 984 prescribed only if specifically indicated. (Recommendation; D Evidence) 985
14. Recommend and initiate VIT in all patients who have experienced a systemic 986 allergic reaction to an insect sting and who have specific IgE to venom allergens 987 (Strong Recommendation; A Evidence), with the following special considerations 988 (Summary statements 17, 18, and 19): 989
15. Avoid VIT based solely on in-vivo and in-vitro testing for venom-IgE, without a 990 history of systemic reaction to a sting. (Strong Recommendation; A Evidence) 991
16. Counsel patients who have experienced only large local reactions to stings that 992 VIT is generally not necessary, but might be considered in those who have frequent 993 unavoidable exposure. (Recommmendation; B Evidence) 994
17. In a change from previous recommendations, advise both children and adults 995 who have experienced only cutaneous systemic reactions without other systemic 996 manifestations after an insect sting that VIT is generally not required, but may be 997 considered when there are special circumstances. This should be a shared decision 998 with consideration of high risk factors (frequent exposure, cardiovascular or 999 respiratory conditions, or selected medications) and the effects on quality of life. 1000 (Recommendation; C Evidence) 1001
18. Discuss with adults with cutaneous systemic reactions who are already receiving 1002 VIT the reasons for the change in recommendations, possible special circumstances, 1003 and the relative risks and benefits of discontinuing or completing the course of VIT. 1004
(Recommendation; D Evidence) 1005
19. Include in VIT all venoms for which the patient has demonstrated specific IgE. 1006 (Recommendation; C evidence) Treatment with some venoms may not be needed if 1007 cross-reactivity can be demonstrated by a RAST inhibition test. (Recommendation; C 1008 Evidence) 1009
20. Begin VIT with initial dose of up to 1 mcg, and increase to maintenance dose of 1010 at least 100 mcg of each venom. (Recommendation; B evidence) Children might be 1011 effectively treated with a maintenance dose of 50 mcg. (Recommendation; C 1012 Evidence) 1013
21. Choose a build-up dose schedule for optimal safety and convenience. 1014 Maintenance dose and protection can be achieved with equal safety using 1015 conventional (4 months) or modified rush (8 weeks) regimens. The risk of systemic 1016 reaction is similar using rush regimens (2-3 days), but may be slightly greater using 1017 ultra-rush regimens (4- 6 hours) . (Strong recommendation; B Evidence) 1018
22. Continue the maintenance dose monthly for at least 12-18 months, then 1019 consider extending the interval to 6 or 8 weeks during several years of treatment. 1020 For patients who continue VIT for longer than 4 years, a 12 week interval is safe and 1021 effective. (Strong Recommendation; C Evidence) 1022
23. Advise patients who start VIT to continue injections for 3 to 5 years (most 1023 experts recommend 5 years). (Strong Recommendation; B Evidence) 1024
24. Encourage continuation of VIT for an extended time, or indefinitely, in patients 1025 with high-risk factors, such as very severe reaction before VIT (syncope, 1026 hypotension, severe respiratory distress), systemic reaction during VIT, honeybee 1027 allergy, and increased basal serum tryptase levels. (Strong Recommendation; C 1028 Evidence) 1029
25. Consider continuation of VIT for more than 5 years in patients with other high 1030 risk factors for recurrent or severe sting reactions, such as underlying 1031 cardiovascular or respiratory conditions, select anti-hypertensive medications, 1032 frequent exposure, and limitation of activity due to anxiety about unexpected 1033 stings. (Strong Recommendation; A Evidence) 1034
26. Recommend immunotherapy with imported fire ant whole-body extracts to all 1035 patients who have experienced a systemic reaction to a fire ant sting and who have 1036 positive skin test responses or allergen- specific serologic test results with imported 1037 fire ant whole-body extract. (Strong Recommendation; B Evidence) 1038
27. Consider whole body extract immunotherapy in patients who have only 1039 cutaneous manifestations to fire ant stings, because the natural history of fire ant 1040 hypersensitivity has not been well elucidated and there is increased risk of fire ant 1041 stings in children who live in areas where fire ants are prevalent. (Recommendation; 1042 D Evidence) 1043
28. Consider continuation of imported fire ant whole-body extract for more than 5 1044 years in patients with imported fire ant allergy since the optimal duration of this 1045 therapy has been less well studied and the frequency of exposure is high. 1046 (Recommendation; C Evidence) 1047
1048 1049 1050 1051 Stinging insect hypersensitivity: A practice parameter update 1052 2016 1053 1054 1055 1056 Stinging Insects and Venom Allergens 1057 1058 1059
A. Classification 1060 1061
Identification of the culprit stinging insect by patients is difficult and unreliable. However, an 1062 understanding of its biology, behaviors, and geographic distribution may be very helpful in its 1063 identification. Changes in geographical distribution, range and prevalence have been noted as 1064 a result of climate change, as evidenced by increasing reports of yellow jacket sting reactions in 1065 Alaska.1,2 1066 1067 Domestic honeybees are found in commercial hives, while non-domestic honeybees nest in tree 1068 hollows, old logs, or in buildings. Hives usually contain hundreds or thousands of bees. 1069 Honeybees, except for Africanized honeybees, are usually non-aggressive away from their 1070 hives. Many honeybee stings occur on the feet when going barefoot in grass or clover. 1071 Honeybees usually leave a barbed stinger with attached venom sac in the skin after they sting. 1072 Other insects, particularly ground-nesting yellow jackets, also can leave stingers in the skin. 1073 Consequently, the presence of a stinger is not absolutely diagnostic of a honeybee sting. 1074 Bumblebees are very uncommon causes of sting reactions but have been reported to cause 1075 anaphylaxis during occupational exposure in greenhouse workers.3 Related to domestic 1076 honeybees, Africanized honeybees are hybrids that developed from interbreeding of domestic 1077 honeybees and African honeybees in South America. Their domain has now expanded 1078 northward and they can now be found in several states, including Texas, New Mexico, Arizona, 1079 Nevada, and California.4 They are far more aggressive than domestic honeybees and more likely 1080 to attack in swarms. Their venom has the same allergens as domestic honeybee venom.5 1081 1082 Yellow jackets, hornets, and wasps are in the vespid family and feed on human foods. They are 1083 especially attracted to sweet food. Consequently, they can be found around garbage cans, 1084
leftover food, or at outdoor events where food and soft drinks are served. Yellow jackets can be 1085 encountered during yard work, farming, gardening, or other outdoor activities. They may build 1086 large paper-enclosed nests underground, and can also be found in wall tunnels or crevices and 1087 in hollow logs or landscape ties. Yellow jackets are very aggressive and sting with minimum 1088 provocation. Subjects have been stung in the mouth, oropharynx, or esophagus while drinking a 1089 beverage from a container that contained a yellow jacket. There are many species of yellow 1090 jackets in North America, and they are the most common cause of sting reactions in most areas 1091 (see below). Hornets build large paper-enclosed nests that are usually found in shrubs and 1092 trees. Wasps build open-faced honeycomb nests that are several inches or more in diameter 1093 and are often visible on the outside of the nest. The nests can be found in shrubs, under the 1094 eaves of houses or barns, and occasionally in pipes on playgrounds or under patio furniture. 1095 Polistes species wasps are prevalent throughout North America, and are a more common 1096 causes of stings in Florida, Texas, and Louisiana. 1097 1098 The imported fire ant, can be red (S. invicta) or black (S. richterii), nests in mounds composed 1099 of freshly disturbed soil that can be at least several inches high and might extend 1 to 2 feet in 1100 diameter. Fire ants do not generally denude the area around their nest, and therefore 1101 vegetation might be found growing through the mounds. There can be multiple mounds a few 1102 feet apart. Fire ant mounds are very common along southeastern roadways and therefore are a 1103 danger to traveling motorists. In sandy areas, fire ant nests are flat. In addition, they are a 1104 major problem in residential neighborhoods, back yards, and public places. These ants are very 1105 aggressive, particularly if their nests are disturbed, and are often responsible for multiple stings. 1106 A sterile pseudo-pustule, which develops at the site of a sting in less than 24 hours, is 1107 pathognomonic of an imported fire ant sting. The distribution of Africanized honeybees and fire 1108 ants in the Southern United States is depicted in Fig E2. 1109 1110 1111
B. Cross-reactivity 1112 1113 Venoms contain some shared antigenic components. Cross sensitization and immunologic cross-1114 reactivity are extensive between hornet and yellow jacket venoms, somewhat less extensive for 1115 yellow jacket and hornet with wasp venoms, and less common between honeybee and the 1116 other venoms.6-10 Bumblebee venom contains unique allergens and has variable cross-reactivity 1117 with honeybee venom.11 Limited cross-reactivity exists between the antigens in fire ant venom 1118 and the antigens in venoms of other Hymenoptera.12,13 1119 1120 1121 1122 1123 1124 1125 1126
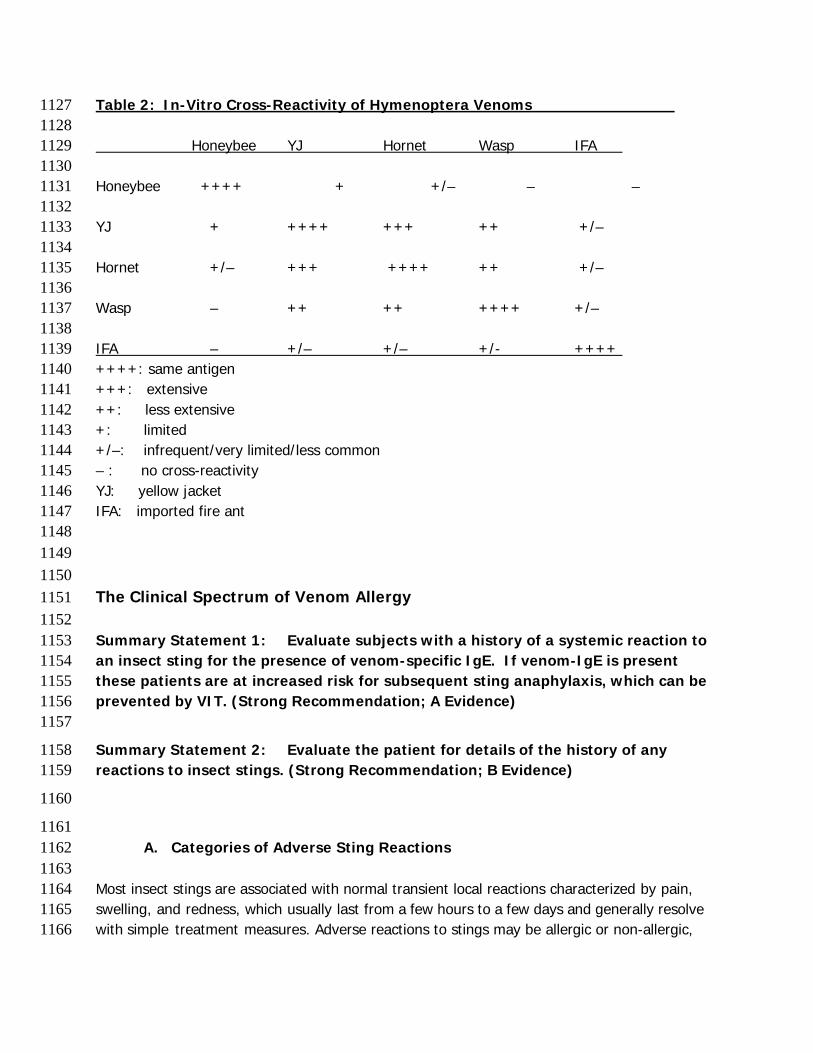
Table 2: In-Vitro Cross-Reactivity of Hymenoptera Venoms 1127 1128 Honeybee YJ Hornet Wasp IFA 1129 1130 Honeybee ++++ + +/– – – 1131 1132 YJ + ++++ +++ ++ +/– 1133 1134 Hornet +/– +++ ++++ ++ +/– 1135 1136 Wasp – ++ ++ ++++ +/– 1137 1138 IFA – +/– +/– +/- ++++ 1139 ++++: same antigen 1140 +++: extensive 1141 ++: less extensive 1142 +: limited 1143 +/–: infrequent/very limited/less common 1144 – : no cross-reactivity 1145 YJ: yellow jacket 1146 IFA: imported fire ant 1147 1148 1149 1150 The Clinical Spectrum of Venom Allergy 1151 1152 Summary Statement 1: Evaluate subjects with a history of a systemic reaction to 1153 an insect sting for the presence of venom-specific IgE. If venom-IgE is present 1154 these patients are at increased risk for subsequent sting anaphylaxis, which can be 1155 prevented by VIT. (Strong Recommendation; A Evidence) 1156 1157
Summary Statement 2: Evaluate the patient for details of the history of any 1158 reactions to insect stings. (Strong Recommendation; B Evidence) 1159
1160
1161 A. Categories of Adverse Sting Reactions 1162
1163 Most insect stings are associated with normal transient local reactions characterized by pain, 1164 swelling, and redness, which usually last from a few hours to a few days and generally resolve 1165 with simple treatment measures. Adverse reactions to stings may be allergic or non-allergic, 1166
with local or systemic manifestations. Some local reactions are IgE-mediated, with intense and 1167 prolonged local induration and swelling (large local reactions – see below). Systemic allergic 1168 reactions can cause the full spectrum of signs and symptoms of anaphylaxis, from the mildest 1169 (generalized erythema, pruritus and hives) to the most severe (hypotensive shock or respiratory 1170 obstruction and arrest). Cardiac anaphylaxis can cause myocardial ischemia (Kounis syndrome) 1171 or arrhythmias. Unusual reactions have been reported including neuropathies, seizures, renal 1172 failure (with rhabdomyolysis), and serum sickness. These reactions are mostly toxic in nature, 1173 and delayed in onset, but the mechanism of many of the unusual reactions is not known. 1174 1175 1176 B. Definitions of Specific Venom Allergy Conditions 1177 1178 Insect stings can trigger a range of immune and clinical responses. It is common for venom-specific 1179 IgE antibodies to be induced by an insect sting, although this is more often transient than persistent. 1180 Stings also induce production of IgG antibodies. 1181 1182 Large local reactions (LLR) are abnormally large localized reactions contiguous with the 1183 Hymenoptera sting site. Although occasionally rapid in onset, the swelling usually increases 6-1184 12 hours after the sting, progresses over 24-48 hours, and subsides after 3-10 days. LLR are 1185 usually larger than 10 cm in diameter, and can involve an entire extremity (crossing joint lines). 1186 These reactions represent late-phase IgE-dependent inflammatory responses to venom 1187 allergens. They do not represent cellulitis even though lymphangitic streaks may be present. 1188 They are generally not dangerous, but can occasionally cause a compartment syndrome in 1189 some anatomically constrained places, and could cause airway compromise if the sting occurs in 1190 the oropharynx (eg, after drinking from a straw or canned beverage).14,15 1191 1192 Systemic reactions (SR) are typically IgE mediated and may present with a variety of 1193 symptoms, involving multiple organ symptoms. Cutaneous symptoms may include pruritus, 1194 flushing, urticaria and angioedema. Respiratory symptoms may include stridor, wheezing and 1195 dyspnea. Gastrointestinal symptoms can include abdominal cramping, nausea, vomiting and 1196 diarrhea. Cardiovascular symptoms and signs are usually related to hypotension, and may 1197 include light-headedness, syncope, or cardiovascular shock. Cardiac anaphylaxis can cause 1198 arrhythmias, or the symptoms and signs of acute coronary insufficiency or myocardial 1199 infarction. This is due to the high concentration of mast cells in the vicinity of the coronary 1200 arteries and cardiac conduction fibers. Kounis syndrome, or “allergic angina” is the occurrence 1201 of the symptoms and signs of angina coincident with an acute allergic reaction, and has been 1202 reported following Hymenoptera sting.16 Systemic reactions to stings must be differentiated 1203 from toxic reactions or anxiety reactions (often subjective symptoms with no objective signs). 1204 The pattern and timing of symptoms, the presence of objective signs, and the response to 1205 treatment may help to clarify the nature of the reaction. Measurement of serum tryptase early 1206 in the reaction may provide evidence of anaphylaxis if it is elevated (at least 135% of baseline 1207 level).17 1208
1209 Serum sickness-like reactions to stings have occurred, and may be associated with the presence 1210 of venom-specific IgE, but the mechanism of the reactions and the risk of anaphylaxis are 1211 unknown.18 Cold urticaria and cold-induced anaphylaxis have been reported after insect stings, 1212 generally without anaphylaxis.19,20 1213 1214 1215 Prevalence, Natural History and Prevention 1216 1217
A. Epidemiology of Venom Allergy 1218 1219 The prevalence of LLR in the general population is about 10%, with estimates ranging from 1220 2.4% to 26.4%, and higher among beekeepers (14% to 43%).15,21 Skin testing and/or sIgE are 1221 reported to be positive in up to 80% of subjects with LLR. 1222 1223 The prevalence of SR ranges from 0.5% to 3.3% in U.S. reports, and from 0.3% to 7.5% in 1224 European reports. Systemic reaction rates among children are lower, ranging from 0.15% to 1225 0.8%.21 Fatality from insect sting anaphylaxis accounts for 20% of all cases of any cause fatal 1226 anaphylaxis, with an incidence of 0.03 to 0.48 fatalities per 1 million population. In the U.S., 1227 there are at least 40 deaths annually due to insect sting anaphylaxis, although this is felt to be 1228 under reported. Biphasic anaphylactic reactions, are associated with the most severe events, 1229 but may be less frequent in insect sting allergy than other causes of anaphylaxis. 1230 1231 Venom sensitization is common in the general population, estimated between 9.3% and 28.7%. 1232 In the months after a sting, transient sensitization occurs in up to 40% of adults. This high 1233 frequency of asymptomatic sensitization gives the tests a very limited positive predictive value 1234 in the absence of a clinical history of allergic reaction to a sting. For this reason, venom testing 1235 cannot be used to screen asymptomatic people.22 Atopy is associated with venom sensitization, 1236 but not with allergic reactions to stings. 1237 1238 The frequency of insect stings in the general population depends largely on climate and risk of 1239 exposure. Between 56% and 94% of the adult population report being stung at least 1240 once.21,23,24 The attack rate is estimated at 10% per year for yellow jackets and 50% for 1241 imported fire ants in endemic areas.25 1242 1243 1244
B. Natural History and Factors Influencing the Occurrence of Allergic Reaction 1245 1246
The clinical history is paramount in predicting the chance of future allergic reactions to stings. 1247 Asymptomatic sensitization is associated with a relatively low risk of systemic reaction to future 1248 stings, estimated at 5 to 15%. When systemic reactions do occur, they can range from the 1249 mildest to the most severe manifestations of anaphylaxis. Unfortunately, there is no test that 1250
can distinguish those who will react to future stings and those who will not, or how severe a 1251 reaction might be. 1252 1253 Patients with a history of LLR have about a 7% chance of systemic reaction to a future sting 1254 (range 4% to 15%), both in adults and children. Like the other “low-risk” sensitized individuals, 1255 some of these reactions will be severe, and many will be relatively mild (eg, cutaneous).26-30 1256 1257 The frequency of systemic reaction to a future sting in patients with a past history of systemic 1258 reactions to stings is about 50% (range 25% to 75%).31 The chance of reaction is in the lower 1259 end of this range for those with a history of mild-moderate systemic reactions, and is highest in 1260 those with a history of life-threatening anaphylaxis. Children or adults who had only cutaneous 1261 systemic reactions have about 10% chance of a future systemic reaction, but less than 3% 1262 chance of a more severe reaction.27,31,32 1263 1264 Systemic reactions may be more likely in response to multiple stings, or sequential stings 1265 (within weeks or months). The risk declines somewhat with time, but remains at 20% to 30% 1266 for decades.26,31,33 There is a significantly higher incidence of systemic reactions among 1267 beekeepers than the general population.34 The frequency and/or severity of allergic reactions to 1268 stings is also affected by factors other than the clinical history. The level of sensitivity (skin test 1269 or serum IgE) is correlated with the frequency but not the severity of the reaction. An elevated 1270 basal serum tryptase, the concomitant use of anti-hypertensive medications, and increasing age 1271 are associated with increased risk of more severe anaphylactic reactions to stings. 1272 1273 1274
C. Prevention of Insect Sting Allergy 1275 1276
Summary Statement 3: Recommend to patients who have a history of systemic 1277 reactions to insect stings: 1278
a. effective measures to avoid insect stings. (Recommendation; D Evidence); 1279 b. the need to always carry an epinephrine auto-injector, to be familiar with 1280 its proper use and when to use it or not use it, and to carry medical 1281 identification (Strong Recommendation; C Evidence); and 1282 c. referral for evaluation by an allergist/immunologist, the utility of specific 1283 IgE testing for stinging insect sensitivity and the potential advantages of 1284 venom immunotherapy (testing is not necessary for patients in whom VIT is 1285 not required) (Strong Recommendation; D Evidence). 1286
1287 Three tenets of treatment for patients at risk of systemic reactions to stings are: avoidance, 1288 availability of emergency medication, and VIT. Table 2 shows some of the effective and 1289 ineffective avoidance measures to reduce the likelihood of insect stings, including the following: 1290
• have known or suspected nests in the immediate vicinity of the patient’s home removed 1291 by trained professionals (periodic inspection by experts regarding the existence of nests 1292 should be considered).; 1293
• avoid walking outside barefoot or with open shoes (sandals); 1294 • wear long pants, long-sleeved shirts, socks, shoes, head covering, and work gloves 1295
when working outdoors; 1296 • be cautious near bushes, eaves, and attics and avoid garbage containers and picnic 1297
areas; 1298 • keep insecticides approved for use on stinging insects readily available to kill stinging 1299
insects from a distance if necessary (stinging insects are not affected by insect 1300 repellants, and fire ants require different specific insecticides); and 1301
• avoid eating or drinking outdoors and be cautious in situations outdoors in which food 1302 and beverages are being served (special care should be taken when drinking from 1303 opaque containers and straws). 1304
Current evidence does not support avoiding particular colors or patterns of clothing as insects 1305 do not recognize these as we do.35 1306 1307 The prescription of an epinephrine injector generally requires discussion about when and why it 1308 should be used (or not used). Although this seems prudent in patients with a potential risk of 1309 reaction to a sting, there is also a burden to the patient that accompanies the prescription.36 1310 Patients may be more fearful of being stung after they have been cautioned about the need to 1311 carry an epinephrine injector, and can experience a reduction in quality of life compared to 1312 similar patients who receive VIT and experience an improvement in quality of life.37 This 1313 contributes to uncertainty about whether there is a need to recommend an epinephrine injector 1314 to a patient whose risk of sting anaphylaxis is considered low enough that they do not require 1315 VIT. These considerations should be discussed with the patient and considered on an individual 1316 basis. 1317 1318 1319 Referral to an allergist-immunologist is recommended for patients who: 1320
• have experienced a systemic allergic reaction to an insect sting; 1321 • have experienced a systemic allergic reaction in which an insect sting could be the 1322
cause; 1323 • need education regarding their risk of reaction, and the need for stinging insect 1324
avoidance or emergency treatment; 1325 • might be candidates for VIT; 1326 • have a coexisting situation that might complicate treatment of anaphylaxis by making 1327
epinephrine injection less effective or more hazardous (eg, taking beta-blockers, 1328 hypertension, and cardiac arrhythmias), or might be unable to self-administer 1329 epinephrine, or 1330
• request consultation for more detailed information or specific testing. (D) 1331
DIAGNOSIS OF VENOM/STING ALLERGY, DIFFERENTIAL DIAGNOSIS 1332 1333
A. Diagnosis of IgE-mediated Venom Allergy 1334 1335 Summary Statement 4: Perform immediate hypersensitivity skin tests and/or in-1336 vitro tests with stinging insect venoms on patients who are candidates for VIT. 1337 (Strong Recommendation; A Evidence) 1338 1339
Skin testing for honeybee, wasps, hornets, and yellow jackets 1340 Diagnostic testing should be performed when the history is consistent with the indications for 1341 VIT (see below). Before ordering venom skin tests or venom-specific IgE level measurement, 1342 the clinician should discuss with the patient the likely recommendation depending on whether 1343 the test results are positive or negative and whether the potential benefit might exceed the 1344 potential harm (eg, anxiety, altered lifestyle, and decreased quality of life) from the results of 1345 diagnostic evaluation. Diagnostic testing is recommended based on the clinical history, even 1346 when the systemic reaction was many years or decades earlier, because the risk of reaction can 1347 persist for long periods of time. Even when there has been a sting without a reaction occurring 1348 after the systemic reaction, the risk of anaphylaxis can persist.31,38 1349 The presence of venom-specific IgE antibodies is usually confirmed by means of intracutaneous 1350 skin testing.26,39,40 Skin prick tests at concentrations up to 100 mcg/mL can be performed before 1351 intracutaneous tests but are not used by all allergists. Initial intradermal tests generally are 1352 done with venom concentrations no stronger than 0.001 to 0.01 mcg/mL. If intradermal (ID) 1353 test responses at these concentrations are negative, the concentration is increased by 10-fold 1354 increments until a positive skin test response occurs or a maximum concentration of 1.0 1355 mcg/mL is reached. By using appropriate positive and negative control tests, a positive skin test 1356 response at a concentration less than or equal to 1.0 mcg/mL demonstrates the presence of 1357 specific IgE antibodies. False positive results caused by nonspecific responses have been 1358 reported at concentrations greater than 1.0 mcg/ml.39 Several accelerated methods for 1359 performing venom skin testing has been described, including a one-step method using only the 1360 1.0 mcg/ml concentration.41-43 1361 1362
There has been some recent concern about what might be considered a positive ID skin 1363 test, because there is some inconsistency in the description of the technique and interpretation 1364 of venom skin tests. Some of the recommendations that have been used include the following: 1365
• In North America, Europe, and many countries, venom extract sufficient to produce a 1366 bleb of 3 mm is injected, which is usually a volume of 0.02 to 0.03 mL. A wheal 3 to 5 1367 mm greater than the negative control, with appropriate surrounding erythema at a 1368 concentration ≤1 mcg/mL, is considered positive44,45 1369
• In the United Kingdom, 0.03 mL of venom extract is injected to raise a bleb of 3 to 5 1370 mm. A wheal diameter of 3 mm greater than the negative control at 20 minutes is 1371 considered positive46 1372
• One manufacture's package insert suggests the injection of 0.05 mL of venom and 1373 defines a positive reaction as 5 to 10 mm wheal and 11 to 20 mm erythema (ALK 1374 Prescribing Information: Allergenic Extracts: Hymenoptera Venom/Venom Protein; ALK 1375 Abello A/S Horshhol, Denmark Revision C 12.01.2014.) This was the method used in the 1376 early clinical trials.40,47 1377
1378 There are no definitive studies to suggest any specific intradermal technique to be superior for 1379 determining specific IgE for venom. The original studies that validated venom skin tests as a 1380 diagnostic technique used an injection sufficient to raise a 3-4 mm bleb, and defined a positive 1381 test according to the method of Norman (at least 5 to 10 mm wheal and 11 to 20 mm 1382 erythema).40,47,48 1383 1384 In a recent survey of 5203 members of the AAAAI and ACAAI carried out by this task force in 1385 2015, there were 540 responses (10.4%). For ID tests, most of the respondents use a volume of 1386 injection of 0.02-0.03 ml (48.5%), or sufficient to raise a 3-4 mm bleb in the skin (29.5%). A 1387 volume of 0.05 ml was use by 22.8% of the respondents. The result of the ID skin test was 1388 considered positive by 65.6% of the respondents if the wheal was 3 mm greater than the 1389 negative control accompanied by surrounding erythema. The result was considered positive with 1390 a 5-10 mm wheal and >10 mm erythema (20.7% of respondents), with a 3 mm wheal regardless 1391 of erythema (8.1%), or with a 5 mm wheal regardless of erythema (5.6%) Currently, there are 1392 no data to suggest an inferior method of intradermal testing or interpretation. Consequently it is 1393 recommended that each practitioner use the technique they are most familiar with to determine a 1394 positive response. 1395 1396 Detection of all potentially relevant sensitivities requires testing with all of the commercially 1397 available bee and vespid venoms and might include fire ant extracts when the patient has 1398 exposure to fire ant stings. The insect that caused the sting often cannot be identified, but even 1399 if it is clearly identified, the possibility exists of future reactions to other venoms to which there 1400 is pre-existing sensitization. Some experts recommend testing with a single venom when the 1401 culprit is definitively known, particularly in the case of honeybee or fire ant stings. 1402 1403 Venoms contain some shared antigenic components. Cross sensitization and immunologic cross-1404 reactivity are extensive between hornet and yellow jacket venoms, somewhat less extensive for 1405 yellow jacket and hornet with wasp venoms, and less common between honeybee and the 1406 other venoms.6-10 (see Table above) It is therefore common for skin or serum tests for venom-1407 IgE to be positive to multiple vespid venoms, and many patients are positive to both honeybee 1408 and vespid venoms. 1409 1410 1411
Summary Statement 5: If initial test results are negative in a patient with a clear 1412 history of systemic sting reaction, further testing (in vitro testing, repeat skin 1413
testing, or both) should be performed, as well as basal serum tryptase 1414 measurement. (Strong Recommendation; C Evidence) 1415
1416 The diagnostic ability to detect all venoms to which each patient is sensitized might be limited 1417 by inherent variability in venom IgE test results in some patients, such that any one of the 1418 venoms tested could be negative on one occasion and positive at 1.0 mcg/mL on a later visit. In 1419 patients who have a history of a systemic allergic reaction to a sting and have positive 1420 diagnostic test results to some venoms and negative results to others, some experts 1421 recommend further evaluation for the negative venoms (by serum IgE tests and/or repeat skin 1422 tests) to identify all potentially relevant sensitivities before beginning VIT.49 1423 1424 Summary Statement 6: Physicians and patients should not expect the degree of 1425 sensitivity found on skin and serologic tests for venom-specific IgE to reliably 1426 predict the severity of a reaction to a sting, but it is a good predictor for the 1427 likelihood of any systemic reaction. (Recommendation; B Evidence) 1428
1429 There is no absolute correlation between the degree of skin test reactivity or levels of serum 1430 venom-specific IgE antibodies and the severity of clinical symptoms. There are patients who 1431 have had severe systemic reactions after an insect sting who have barely detectable venom IgE 1432 antibody levels determined by using skin or in vitro tests. In addition, there are occasional 1433 patients who have negative skin test responses but have increased levels of serum venom-1434 specific IgE antibodies.50-52 It is appropriate to perform in vitro venom testing in patients with 1435 negative skin test responses who would otherwise be potential candidates for VIT. Many 1436 physicians postpone testing for venom-specific IgE until 3 to 6 weeks after the sting reaction 1437 because of concerns about reduced sensitivity of testing modalities within the first few weeks 1438 after the reaction. One study found that 79% of patients with insect venom allergy could be 1439 identified at 1 week after the sting reaction when patients underwent both skin and in vitro 1440 tests; the additional 21% of patients whose test results were negative initially, had at least 1 1441 positive test result when tested again with both methods at 4 to 6 weeks after the reaction.53 1442 Negative test results for venom-specific IgE obtained within the first few weeks after a sting 1443 reaction might require cautious interpretation. 1444 1445 Summary Statement 7: Consider measuring basal serum tryptase in all patients 1446 who are candidates for VIT. (Recommendation; B Evidence) 1447
1448 A negative in vitro assay result in addition to a negative skin test response does not fully 1449 exclude the possibility of an anaphylactic reaction to a subsequent sting because rare 1450 occurrences have been reported.50 The pathogenesis of these rare reactions might involve a 1451 non-IgE mechanism. Basal serum tryptase levels have been found to be increased in some 1452 patients with insect sting allergy.54-56 Such patients might require evaluation for mastocytosis or 1453 disorders of mast cell function (discussed in more detail below). Some experts recommend 1454
measuring basal serum tryptase in all patients who are candidates for VIT because the result is 1455 abnormal in about 11% of all cases and is an important risk factor for severe reactions before, 1456 during, and after VIT.54,56-58 The likelihood of an elevated basal serum tryptase level is higher, 1457 and the test is therefore most useful, in patients with very severe reactions to stings 1458 (particularly when there is hypotension or the absence of urticaria), and those with no 1459 detectable venom IgE on both skin and serum tests, and should be considered in those with 1460 systemic reactions during VIT, and when considering discontinuation of VIT. (see below and 1461 Table 4) Full review of the available evidence and recommendations for this test will be the 1462 subject of a focused practice parameter in the near future. 1463 1464 Summary Statement 8: Use skin tests as the preferred test for initial 1465 measurement of venom-specific IgE. In vitro measurement of serum IgE should be 1466 used as a complementary or alternative test. Test for all 5 venoms, with the possible 1467 exception of individual patients in whom a single culprit is definitively known. 1468 (Recommendation; C Evidence) 1469
In vitro testing 1470 In vitro tests can also be used for detection of venom-specific IgE antibodies in those subjects, 1471 particularly in patients who cannot undergo skin testing or have negative venom skin tests. This 1472 includes patients with dermatographism or severe skin disease. Skin tests are generally the 1473 preferred initial testing method. Up to 20% of subjects with positive venom skin test responses 1474 have undetectable serum levels of specific IgE antibodies (negative in vitro test result). 1475 However, recent studies have demonstrated that about 10% of patients with negative skin test 1476 responses have positive in vitro test results when using assays capable of detecting low levels 1477 of venom-specific IgE antibodies.50-52 Whichever test is done first, a negative result to any of 1478 the venoms may justify repeating a test for that venom with the complementary diagnostic test 1479 method. The need for supplemental tests should be assessed for each individual patient based 1480 on the known risk factors for severe reactions and the results of the initial tests for venom IgE. 1481 This is also discussed in the preceding section on skin tests. The utility of laboratory methods is 1482 also dependent on the reliability of the methods used by clinical laboratories; the clinician is 1483 advised to become familiar with differences in results by using different assays and different 1484 laboratories.59,60 Clinicians should also be aware that although technical improvements permit 1485 reporting of serum IgE levels between 0.1 and 0.35 kU/L as positive, the clinical significance of 1486 these low levels has not been determined.61 1487 1488
1489 Skin testing for fire ant hypersensitivity 1490 1491 Imported fire ant whole-body extract is the only reagent currently available for diagnostic 1492 testing in patients with suspected fire ant hypersensitivity. If screening skin prick test responses 1493 are negative, intracutaneous testing should be performed, with initial concentrations of 1494 approximately 1 x 10-6 (1:1 million) wt/vol. The intracutaneous skin test concentration should be 1495 increased by increments until a positive response is elicited or a maximum concentration of 1 x 1496
10-3 (1:1,000) or 2 x 10-3 (1:500) wt/vol is reached.62-64 Limited cross-reactivity exists between 1497 the antigens in fire ant venom and the antigens in venoms of other Hymenoptera.12,65 If the 1498 patient is able to positively identify fire ant as the stinging insect, testing with other stinging 1499 insect venoms may not be necessary. The presence of a pseudo-pustule at the sting site at 24 1500 hours after the sting is diagnostic of an imported fire ant sting. This type of reaction should be 1501 looked for carefully in endemic areas if the identity of the culprit insect is uncertain. 1502 1503 1504 1505 New Diagnostic Methods 1506 1507
One of the issues that remain undefined for Hymenoptera allergy is the lack of a test 1508 that is 100% sensitive for assessing specific IgE. Some improvement in sensitivity can be 1509 gained by the use of skin tests with less irritating dialyzed venoms that can be used at 1510 concentrations up to 10 mg/mL with no irritant response.66 Dialyzed venom skin test 1511 preparations are not commercially available in the United States. 1512
1513 The basophil activation test (BAT) has been offered as a way to address this problem. Since 1514 basophils have high affinity IgE receptors on their surface, they will bind to specific IgE and be 1515 activated when exposed to an appropriate antigen. In the BAT, basophils from a patient with 1516 suspected hymenoptera allergy are exposed to defined concentrations of hymenoptera venom 1517 (usually 0.1 mcg/ml to 1.0 mcg/ml) and activation is measured based on the percentage of 1518 basophils that express activation markers (CD63) on their surface. BAT may be useful in 1519 patients with mastocytosis.67 In one study, BAT showed better sensitivity and specificity than 1520 ID testing in patients with negative prick and in vitro venom testing.68 Unfortunately this and 1521 other studies assessing BAT have compared determination of specific IgE to other testing 1522 methods and not to a gold standard of a sting challenge. Thus BAT has not been shown to 1523 improve diagnostic sensitivity with clinical relevance. 1524 1525 In addition, BAT has been used to determine whether VIT has been successful as determined 1526 by sting challenge.69 Lower values of BAT are associated with fewer systemic reactions after 1527 VIT.70 Higher expression of CD63 on basophils has been associated with a lack of response to 1528 VIT.71 A reduction in BAT has been associated with a protective immune response to honey 1529 bee VIT in children.72 1530 1531 Finally there are many technical challenges associated with the use of BAT. Included among 1532 these are a short half-life for viable basophils and a variable determination of what is 1533 considered a positive test.73-75 Consequently routine use of BAT in evaluating Hymenoptera 1534 sensitive patients is not recommended at this time. If technical issues can be addressed, BAT 1535 may be useful in diagnostic evaluation, and for monitoring the effectiveness of VIT. 1536 1537
Just as there are multiple components for aeroallergens and food allergens, there are multiple 1538 components for each of the Hymenoptera venoms. The clinical significance of diagnostic testing 1539 with recombinant venom allergens is not yet clear. Of interest is whether component testing 1540 allows better diagnosis than whole venom (ie, sensitivity), and/or more specific assignment of 1541 reactivity (ie, specificity)76 The data available so far are limited in that most studies are out of 1542 Europe, which limits applicability in the U.S. for 2 reasons. First, in Europe there are basically 1543 only two genera of concern (honeybee and yellow jacket). Second, most of the studies looking 1544 at sensitivity compare them only to the use of whole venom for the same in vitro IgE test, 1545 which makes it impossible to show improved sensitivity over current diagnostic testing. 1546 1547 For honeybee, studies show that rApi m 1 has a sensitivity of between 57% and 96% when 1548 compared to whole honeybee venom.77-79 For the lowest sensitivity study, use of the natural Api 1549 m 1 rather than recombinant led to an improved sensitivity of 91%.78 Similar studies for yellow 1550 jacket have shown sensitivities of 84-87% using Ves v 5 with an increase to 92% if Ves v 1 was 1551 determined as well.79,80 Until studies are done on patients with known hymenoptera sensitivity, 1552 but negative whole venom in vitro studies, it will be impossible to show an improved sensitivity 1553 with component testing.81,82 1554 1555 The attribution of specific sensitivity to individual species of hymenoptera seems more 1556 promising. A number of studies have reported the utility of recombinant venom allergens in 1557 differentiating honey bee from yellow jacket sensitivity in patient with double positivity.83-85 1558 One study using only Api m 1 and Ves v 1 found these were not sufficient to separate out 1559 species specific sensitivity.86 Measurement of IgE to multiple recombinant allergens may 1560 distinguish Vespula and Polistes sensitivity.87 The evaluation of clinical utility in the United 1561 States of component testing awaits studies done with components from all the species found in 1562 the US. 1563 1564 1565 1566
B. Mast cell disorders and Insect Sting Allergy, Basal serum tryptase 1567 1568
Summary Statement 9: Consider measuring basal serum tryptase in patients with 1569 anaphylaxis to a sting, especially in those with severe or hypotensive reactions, and 1570 in all those with negative tests for venom-IgE. (Strong Recommendation; B 1571 Evidence) 1572 1573
Mastocytosis, other mast cell diseases, and serum tryptase have assumed new importance in 1574 the management of allergic disease and anaphylaxis in recent years.56,88-90 This has been 1575 particularly important with venom allergic patients because mast cell disorders are associated 1576 more with sting anaphylaxis than with other common causes of anaphylaxis including foods and 1577 drugs.89,91 The importance of mast cell disease in venom allergic individuals has been an 1578 important factor during initial diagnosis and when assessing high risk individuals for future 1579
severe reactions, and may be a consideration in the duration of venom immunotherapy.55-57,88. 1580 Diagnostic criteria of systemic mastocytosis are discussed elsewhere.92 Measurement of serum 1581 tryptase, a marker for systemic mast cell disorders, is an important and readily available 1582 diagnostic tool for mast cell disorders. In most laboratories the upper limit of the normal range 1583 is 11.4 ng/ml. (Phadia AB. ImmunoCAP tryptase. Directions for use. Uppsala, Sweden: Phadia 1584 AB, 2008.) 1585
Management of patients who have a compelling history of insect-induced anaphylaxis, yet are 1586 negative to both skin and in vitro testing, remains a clinical challenge.51,52,93 Mastocytosis has 1587 emerged as a surprising link in this clinical quandary. A significant percentage of patients with 1588 severe systemic reactions following insect sting, who are demonstrated to have an elevated 1589 basal tryptase level, indeed, may have mastocytosis or monoclonal mast cell activation 1590 syndrome (MMAS).54,89,94 Additionally, in patients with mastocytosis, the most common cause 1591 of anaphylaxis is insect sting.89,95 Basal serum tryptase should be measured in patients with 1592 sting anaphylaxis who have no detectable venom-IgE. Clonal mast cell disorders can occur in 1593 patients with severe Hymenoptera venom allergy and normal serum tryptase levels.96 1594 1595 Summary Statement 10: Counsel patients with elevated basal serum tryptase 1596 about the clinical significance of potential underlying mast cell disorders. 1597 (Recommendation; B Evidence) 1598
1599 Serum tryptase has been described as a predictor of the severity of a systemic reaction to a 1600 sting. Rueff et al, in a multicenter retrospective study of Hymenoptera venom-sensitive 1601 patients, looked at predictors of severe systemic anaphylaxis following a sting.58 Of the 962 1602 patients, 202 (26%) had severe anaphylaxis (Mueller grade III or IV) following a field sting. The 1603 risk factors for severe anaphylaxis to stings or venom immunotherapy included basal serum 1604 mast cell tryptase levels above 5ng/ml; patients taking angiotensin converting enzyme 1605 inhibitors; vespid allergy; older age; and male sex.97 Bonadonna et al. reported a correlation 1606 between systemic reaction to Hymenoptera sting and mast cell tryptase.54 Of 379 patients with 1607 a history of systemic insect sting reactions, 11.6% had serum mast cell tryptase levels 1608 exceeding 11.4 ng/ml. Of this group, the rate of systemic (Muller grade IV) anaphylaxis was 1609 70.5%. In patients with hypotensive reactions to stings (Grade IV), 25% had elevated basal 1610 tryptase. Thirty-four of the patients with elevated mast cell tryptase level underwent bone 1611 marrow biopsy; of those, 61.8% were ultimately diagnosed with indolent systemic 1612 mastocytosis. Blum et al. confirmed these findings in a 5 year retrospective study of 868 1613 patients referred for the evaluation of severe reactions to Hymenoptera stings (758 had both 1614 total IgE and basal tryptase levels drawn).98 Elevated basal tryptase level (>11.4 ng/ml) was 1615 associated with severe systemic reactions (P = 0.026). Stoevesandt et al found a strong 1616 correlation between severity of sting anaphylaxis and elevated basal serum tryptase, and with 1617 the absence of urticaria.99 Finally, Guenova et al confirmed the correlation between severe 1618 systemic reaction to sting and elevated basal tryptase (P = 0.003), and also showed a 1619 correlation with increasing age (P = 0.001).95 Because of the dramatic increase in the severity 1620
of sting-related anaphylaxis in patients with mastocytosis, physicians should consider occult 1621 mast cell disease in anyone with unexplained anaphylaxis or severe sting-related anaphylaxis. 1622 1623 Rueff et al. reported that elevated basal tryptase level correlated with severe reactions 1624 occurring during the immunotherapy build-up phase (odds ratio of 1.56; P< 0.005).97 Generally, 1625 VIT in patients with clonal mast cell disorders has been shown to have reasonable safety and to 1626 significantly reduce the chance of sting anaphylaxis.100-102 Honeybee venom allergy correlated 1627 with higher risk of systemic reaction than vespid venom allergy. There was also a correlation of 1628 severe anaphylaxis to a sting with the use of anti-hypertensive medications (beta-blockers and 1629 angiotensin converting enzyme inhibitors). This has been reported in relation to immunotherapy 1630 and anaphylaxis in general. Patients with mastocytosis who are taking these antihypertensive 1631 medications should consult their physicians about the possibility of changing to an alternative 1632 medication (if it is safe and effective). Fatal anaphylaxis has been reported in patients with 1633 mastocytosis who discontinued VIT.103 1634 1635 When to discontinue venom immunotherapy remains controversial. However, the historical 1636 recommendation of 3-5-year duration of venom immunotherapy may not be optimal for venom 1637 allergic patients with mastocytosis. Patients with mastocytosis have lower probability of long-1638 term protection and consequently a greater risk for recurrent severe, even fatal anaphylaxis if 1639 they discontinue VIT.103 In a thorough review, Bonadonna et al. recommend venom 1640 immunotherapy for life in patients with mastocytosis and venom allergy.104 Since the efficacy of 1641 venom immunotherapy is less than optimal in mastocytosis patients, they should continue to 1642 carry two epinephrine injectors.102 1643 1644 Because there appears to be a high correlation with mastocytosis when the basal tryptase 1645 exceeds 11.4 ng/ml, this diagnosis should be entertained (and basal serum tryptase measured) 1646 in patients with severe anaphylaxis from Hymenoptera, especially when there was hypotension 1647 (and/or the absence of urticaria). The frequency of elevated basal serum tryptase is 25% in 1648 patients with grade IV sting anaphylaxis, but is about 5% in patients who had mild-to-moderate 1649 systemic reactions to stings (grade I, II, III), and the clinical significance is less clear in these 1650 patients.54 Some experts suggest that the evaluation of all patients with a history of a systemic 1651 reaction to hymenoptera should include measurement of the basal serum tryptase.46,104 If clonal 1652 mast cell disease is suspected, initial evaluation for venom specific IgE should begin using in 1653 vitro methods, with skin testing in those individuals who are negative using in vitro methods. If 1654 the serum tryptase is elevated (>11.4 ng/ml) bone marrow biopsy should be considered. 1655 Mastocytosis can occur with normal serum tryptase.96 There is a cost and burden associated 1656 with abnormal results of basal tryptase (eg: bone marrow biopsy, consultation with other 1657 specialists, anxiety associated with an abnormal test result). However an abnormal result is 1658 associated with severe anaphylaxis to stings, more chance of an increased chance of systemic 1659 reactions during VIT (to a sting or venom injection), and more chance of sting anaphylaxis after 1660 stopping VIT. The potential benefits and risks of ordering the test should be considered with 1661 each patient.. 1662
1663 Summary Statement 11: Consider testing patients with mastocytosis for insect 1664 venom sensitivity, and identify other high risk factors for severe anaphylaxis to 1665 stings (including medications). (Recommendation; D Evidence) Discuss with the 1666 patient the benefits and risks for testing and for VIT. 1667
1668 Individuals with known mastocytosis may warrant being tested for Hymenoptera venom 1669 sensitivity because insect stings are the most common cause of anaphylaxis in such patients. In 1670 patients with mastocytosis, sting anaphylaxis is more likely to occur, is more likely to be life-1671 threatening, and the risk can be significantly reduced with VIT. The frequency of sting 1672 anaphylaxis in patients with mastocytosis and positive skin or serum tests for venom IgE is not 1673 known. The positive predictive value of venom-IgE tests in asymptomatic normal individuals is 1674 poor. Nevertheless, it is the opinion of this work group that, when tests are positive for venom 1675 IgE in patients with mastocytosis, the clinician should discuss with the patient the potential 1676 benefits and risks of VIT. The presence of other high risk factors (see Table 3) would be likely 1677 to further increase the risk of severe anaphylaxis to a sting, and would add to the strength of 1678 recommendation for VIT. 1679 1680 It seems likely that dysregulation of other mediators of anaphylaxis will be found to correlate 1681 with the frequency or severity of reactions to stings. It has already been confirmed that levels 1682 of platelet activating factor (PAF) and PAF-acetylhydrolase correlate with the severity of sting 1683 anaphylaxis and with fatal anaphylaxis.105,106 1684 1685 1686 MANAGEMENT OF VENOM/INSECT ALLERGY 1687 1688 A. Treatment of acute sting reactions 1689
Summary Statements 12: Advise the patient to treat acute systemic reactions to 1690 insect stings like any anaphylactic reaction, with timely 1691
12a epinephrine injection (Strong Recommendation; A Evidence) 1692
12b supportive therapy(Strong Recommendation; A Evidence) 1693
12c transport to an emergency department. (Strong Recommendation; C 1694 Evidence) 1695
1696 1697 Epinephrine is the drug of choice for the treatment of anaphylaxis.107,108 The recommended 1698 dose is 0.01 mg/kg, up to 0.3 mg in children, and 0.3 to 0.5 mg in adults, depending on the 1699 severity of the reaction. Intramuscular injection in the anterolateral thigh will achieve a more 1700 rapid and higher plasma concentration than subcutaneous or intramuscular injection in the 1701 arm.109,110 Delayed use of epinephrine might be ineffective.111 Reports of fatal and near-fatal 1702
anaphylaxis show that fatal outcome is associated with delay or lack of administration of 1703 epinephrine.112-114 Patients allergic to insect venom should carry epinephrine at an appropriate 1704 dosage for administration in case of a sting. Patients and caregivers of children who have 1705 experienced a systemic reaction to an insect sting should be taught how to administer 1706 epinephrine and under what circumstances to do so. There is no contraindication to the use of 1707 epinephrine in a life-threatening situation, such as anaphylaxis. Repeat dosing might be 1708 required for persistent or recurrent symptoms. Patients who also have cardiovascular disease 1709 should be given epinephrine for use in the event of an allergic reaction, despite concern about 1710 epinephrine’s cardiac effects, because the risk of a life-threatening anaphylactic reaction is 1711 judged to exceed the risk of administering epinephrine in such patients (even in those using a 1712 beta-blocker medication). Antihistamines and corticosteroids should not be considered to be 1713 substitutes for epinephrine. In patients who have a relatively low risk of anaphylaxis from a 1714 sting, the need to carry injectable epinephrine can be determined by the patient and physician 1715 after discussion of the relative risk of reaction in addition to the cost and burden of having to 1716 carry epinephrine. Patients with a low risk of reaction include those with a history of only large 1717 local reactions to stings or of strictly cutaneous systemic reactions, those receiving maintenance 1718 VIT, and those who have discontinued VIT after more than 5 years of treatment. Factors 1719 associated with a higher risk include a history of extreme or near-fatal reactions to stings, 1720 systemic reactions during VIT (to an injection or a sting), a history of anaphylaxis to a 1721 honeybee sting, increased basal tryptase levels, underlying medical conditions or concomitant 1722 medications, or frequent unavoidable exposure to stinging insects. 1723 1724 Summary Statement 13: Treat large local reactions symptomatically, with 1725 antihistamines, cold compresses, and analgesics as needed. In severe cases a short 1726 course of oral corticosteroids may be useful. Antibiotics are usually not necessary. 1727 (Recommendation; D Evidence) 1728
1729 The vast majority of patients with large local reactions need only symptomatic care and are not 1730 candidates for testing for venom-specific IgE or for VIT. Cold compresses might help to reduce 1731 local pain and swelling. Oral antihistamines and oral analgesics might also help to reduce the 1732 pain or itching associated with cutaneous reactions. Many physicians use oral corticosteroids for 1733 large local reactions, although definitive proof of efficacy through controlled studies is lacking. 1734 Swelling (and even lymphangitis) may be caused by mast cell mediator release and not by 1735 infection, so antibiotics are not indicated unless there is clear evidence of secondary infection (a 1736 common misdiagnosis). 1737 1738 B. VENOM IMMUNOTHERAPY 1739
1740 Summary Statements 14: Recommend and initiate VIT in all patients who have 1741 experienced a systemic allergic reaction to an insect sting and who have specific IgE 1742 to venom allergens (Strong Recommendation; A Evidence) 1743 1744
Summary Statement 15: Avoid VIT based solely on in-vivo and in-vitro testing for 1745 venom-IgE, without a history of systemic reaction to a sting. (Strong 1746 Recommendation; A Evidence) 1747
1748 Venom immunotherapy (VIT) for honeybees, yellow jackets, hornets, and wasps is an extremely 1749 effective treatment for subjects at risk of insect sting anaphylaxis. VIT reduces the risk of a 1750 subsequent systemic sting reaction to as low as 5% compared with up to 60% in untreated 1751 patients.115-117 Moreover, those patients receiving VIT who do experience systemic reactions 1752 after an insect sting generally have milder reactions. Candidates for immunotherapy should 1753 receive informed consent with documentation in the medical record regarding the potential 1754 benefits and risks related to the procedure. There are individuals who seek treatment because 1755 of a fear of sting reactions, but have no history of abnormal reaction to previous stings. Testing 1756 for venom IgE is not recommended in those with no history of reaction to stings. This is 1757 because venom-IgE can be detected in more than 20% of adults who have no history of 1758 reaction to stings, and the tests have poor positive predictive value. For the same reasons, VIT 1759 is not recommended when there is no history of abnormal reaction to a sting, even if the 1760 venom-IgE tests are positive. 1761 1762 Criteria for immunotherapy 1763 1764 History of sting anaphylaxis 1765
Patients who have had an anaphylactic reaction from an insect sting and are found to 1766 have venom-specific IgE antibodies should receive VIT. The goals of VIT are to (1) prevent 1767 systemic reactions and (2) alleviate patients’ anxiety related to insect stings (with improved 1768 quality of life). An estimate of the risk (frequency and severity) of a recurrent sting-induced 1769 systemic reaction guides the selection of patients for VIT. The most serious anaphylactic 1770 reactions involve the cardiac and respiratory systems and are potentially life-threatening. The 1771 most common cardiovascular reaction is hypotension, which is usually associated with 1772 tachycardia. Other serious reactions include loss of consciousness, shock, airway compromise, 1773 and death. VIT is recommended for subjects with a history of these manifestations and the 1774 presence of venom-specific IgE antibodies. VIT is recommended as safe and effective, even in 1775 patients who have had cardiac anaphylaxis.118 VIT has also been effective in cases of delayed 1776 anaphylaxis after a sting.119 Some patients are at particularly high risk for severe anaphylactic 1777 reactions to future stings. Subjects who have experienced a very severe (near-fatal) 1778 anaphylactic reaction to a sting are more likely to have a similar event in the future.120-122 1779 Patients with mastocytosis, or an increased basal serum tryptase level, are also at higher risk 1780 for severe reactions to future stings.55,56,58,91,98,99 Such high-risk patients should have the 1781 greatest benefit from VIT. 1782 1783 Summary Statement 16: Counsel patients who have experienced only large local 1784 reactions to stings that VIT is generally not necessary, but might be considered in 1785 those who have frequent unavoidable exposure. (Recommmendation; B Evidence) 1786
1787 History of large local reaction 1788 A large local reaction or extreme swelling extending from the sting site, usually peaking at 48 to 1789 72 hours after a sting and lasting 1 week or more, is generally the result of an IgE-mediated 1790 late-phase reaction. The risk of a systemic reaction in patients with a history of large local 1791 reactions in most studies is 4% to 10%.27,29,30,123 Because of this relatively low risk, diagnostic 1792 testing and VIT are generally not required in such patients. Although their risk of anaphylaxis is 1793 barely more than that of the general population, large local reactors might be considered for 1794 VIT (and therefore diagnostic testing) for quality-of-life reasons and to reduce the morbidity of 1795 frequent or unavoidable sting reactions.14 1796 1797 Providing injectable epinephrine to patients who have a history of large local reactions for use 1798 if a subsequent systemic reaction occurs is usually not necessary but might be considered if it 1799 provides reassurance to the patient (with instructions on when or when not to use it). This 1800 decision and the physician’s judgment might be influenced by factors such as the potential risk 1801 of being stung, personal health issues (eg, the presence of cardiovascular disease), and the 1802 individual patient’s preference. There have been few studies examining the efficacy of VIT in 1803 preventing large local reactions to subsequent stings. Most patients with a history of large local 1804 reactions will experience similar reactions after subsequent stings, and those with frequent 1805 and/or severe reactions might benefit from VIT.14,124,125 Beekeepers, on the other hand, often 1806 have diminished large local reactions when they receive frequent stings.126,127 1807 1808 Summary Statement 17: In a change from previous recommendations, advise both 1809 children and adults who have experienced only cutaneous systemic reactions 1810 without other systemic manifestations after an insect sting that VIT is generally not 1811 required, but may be considered when there are special circumstances. This should 1812 be a shared decision with consideration of high risk factors (frequent exposure, 1813 cardiovascular or respiratory conditions, or selected medications) and the effects on 1814 quality of life. (Recommendation; C Evidence) 1815
1816 History of cutaneous systemic reaction 1817 Cutaneous systemic reactions, such as urticaria, angioedema, flushing and pruritus, can occur 1818 after an insect sting. While these can be extensive and intense, they not affect other systems 1819 (throat, breathing, light-headedness, hypotension). Prospective studies have shown that 1820 patients 16 years of age and younger who have experienced cutaneous systemic reactions 1821 without other allergic manifestations have approximately a 10% chance of having a systemic 1822 reaction if re-stung. If a systemic reaction does occur, it is likely to be limited to the skin, with 1823 less than a 3% risk of a more severe reaction and less than a 1% risk of life-threatening 1824 anaphylaxis.27,128 Therefore VIT is generally not necessary for patients 16 years of age and 1825 younger who have experienced only cutaneous systemic reactions; VIT is still an acceptable 1826 option in such patients if requested by the patient’s parents or if the child is likely to experience 1827
frequent or multiple stings. VIT gives improved quality of life in patients with cutaneous 1828 systemic reactions.129 1829 1830 VIT is generally not required for patients over 16 years of age who have experienced only 1831 cutaneous systemic reactions. This is a change from the recommendation in the previous 1832 updates of this Practice Parameter Although VIT has previously been recommended in the USA 1833 for patients older than 16 years with systemic reactions limited to the skin, this is not usually 1834 the case in other countries.46,130 There are no studies comparing outcomes in those patients 1835 receiving VIT vs. those not receiving VIT to guide this decision. However, sting challenge 1836 studies suggest that these patients are very unlikely to have severe anaphylactic reactions to 1837 subsequent stings, and may not require VIT.31,32 The risk/benefit ratio for VIT in such patients 1838 is uncertain. This should be a shared decision with consideration of potential high risk factors 1839 (eg, concomitant cardiovascular disease or specific medications, for example ACE inhibitors and 1840 beta blockers, elevated basal tryptase, a high likelihood of future stings, or detrimental effect 1841 on quality of life).46,130-132 It is also possible that younger adults and older adults should not 1842 have the same recommendations, especially since deaths from insect stings increase with age 1843 (for 1980-1999, USA data: 20-29yo, 41 deaths; 30-39yo, 112 deaths; 40-49yo, 196 deaths; 50-1844 59yo, 217 deaths; 60-69yo, 207 deaths; greater than 70yo, 131 deaths).133 1845 1846 Summary Statement 18: Discuss with adults with cutaneous systemic reactions who 1847 are already receiving VIT the reasons for the change in recommendations, possible 1848 special circumstances, and the relative risks and benefits of discontinuing or 1849 completing the course of VIT. (Recommendation; D Evidence) 1850
1851 This new recommendation that VIT is not required for adults with cutaneous systemic reactions 1852 will raise an important question for such patients who are already on VIT based on prior 1853 recommendations. The clinician may discuss with the patient the evidence base for the change 1854 of recommendation, the possible mitigating special circumstances (as above), and the option to 1855 discontinue VIT. The choice to discontinue VIT should be subject to a review of potential risk 1856 factors, as in all patients who are considering discontinuing VIT (systemic reactions during VIT, 1857 basal serum tryptase, cardiovascular or respiratory conditions, or selected medications, 1858 impairment of quality of life). The frequency of elevated basal serum tryptase in patients with 1859 cutaneous systemic reactions to stings is relatively low, and the clinical significance in these 1860 patients is unknown. The alternative choice, to complete the course of VIT, presents a slight 1861 risk (of systemic reaction to injections) and some potential benefit: the long-term outcome in 1862 children with cutaneous systemic reactions was better in those who received VIT than those 1863 who did not.27 1864 1865 Challenge stings 1866 Approximately 25% to 70% of patients with a history of anaphylaxis from an insect sting and 1867 detectable venom-specific IgE antibodies by means of skin or in vitro testing will experience a 1868 systemic reaction when re-stung.32,38,115-117,122,134,135 An intentional sting challenge has been 1869
recommended by some to better select those patients who need VIT.32,136 Patients allergic to 1870 honeybees are more likely to have positive sting challenge results than those allergic to yellow 1871 jackets.32 Sting challenges, however, are neither consistently reproducible nor without risk. 1872 About 20% of patients who do not react to a sting challenge will react after a second 1873 challenge.38 In addition, serious allergic reactions, such as anaphylaxis necessitating intensive 1874 care treatment, have occurred from these challenges. The use of sting challenges requires 1875 special centers because of the risk of serious reactions and is impractical as a general 1876 prerequisite for VIT in the United States.137,138 1877 1878 1879 Procedures for VIT 1880
Summary Statements 19: Include in VIT all venoms for which the patient has 1881 demonstrated specific IgE. .(Recommendation; C Evidence) Treatment with some 1882 venoms may not be needed if cross-reactivity can be demonstrated by a RAST 1883 inhibition test. (Recommendation; C Evidence) 1884 1885 (a) Selection of venoms for immunotherapy 1886 1887 Identification of the stinging insect responsible for a reaction can be aided by the geographic 1888 locality, the circumstances of the sting, and the appearance and location of the insect and nest. 1889 On the other hand, patient identification of stinging insects is notoriously unreliable.139 1890 Consensus data on which venoms to include for immunotherapy are not available. In the 1891 opinion of some authors, applying a knowledge of venom cross-reactivity and insect 1892 identification, the extract used for VIT need only contain a single venom if the culprit is 1893 definitively known, despite positive skin or in vitro test results for other stinging insects.10,140 1894 Other authors recommend that the treatment include venoms from all insects for which positive 1895 test results were obtained because of the potential for reaction to any venoms to which the 1896 patient is sensitized.138,141 1897 1898 Both of these approaches are valid and they are not mutually exclusive. In vitro RAST-inhibition 1899 tests (where available) can distinguish those yellow jacket allergic patients who are cross-1900 sensitized to Polistes wasp venom from those with true dual sensitivity, which would inform the 1901 choice of venoms for VIT.142 This approach has also been used for honeybee and yellow jacket 1902 double-positivity. More recently, the use of recombinant venom allergens has been able to 1903 resolve dual sensitivity to HB and YJ from cross-reactivity that may be due to cross-reacting 1904 carbohydrate determinants.83-87 1905 1906 Summary Statement 20: Begin VIT with initial dose of up to 1 mcg, and increase to 1907 maintenance dose of at least 100 mcg of each venom. (Recommendation; B 1908 evidence) Children might be effectively treated with a maintenance dose of 50 mcg. 1909 (Recommendation; C Evidence) 1910
Summary Statement 21: Choose a build-up dose schedule for optimal safety and 1911 convenience. Maintenance dose and protection can be achieved with equal safety 1912 using conventional (achieving 100 mcg maintenance dose in 4 months) or modified 1913 rush (8 weeks) regimens. The risk of systemic reaction is similar using rush 1914 regimens (2-3 days), but may be slightly greater using ultra-rush regimens (4- 8 1915 hours) . (Strong recommendation; B Evidence) 1916
1917 (b) Dosage schedules for VIT 1918 1919 The dose schedules approved by the US Food and Drug Administration are shown in Appendix 1920 E1. VIT injections are usually administered once or twice a week, usually beginning with a dose 1921 of 0.01 to 1.0 mcg and increasing to a maintenance dose of 100 mcg of each insect venom 1922 (300 mcg of mixed vespid venom).130,140,143 Treatment can be safely started at a dose of 1 mcg 1923 with no greater risk of reaction than regimens that begin with lower doses.144,145 The 100 mcg 1924 maintenance dose was selected in the early clinical trials because it was thought to be 1925 equivalent to 2 honeybee stings (50 mcg per sting). Subsequent studies showed variability in 1926 venom deposition from honeybee stings, and vespid stings have been shown to deliver 2 to 20 1927 mcg of venom protein per sting.116,146,147 The dosing interval and increments might be adjusted 1928 at the discretion of the prescribing physician to accommodate the preferences of the physician 1929 and the patient. The 100 mcg maintenance dose is achieved in 8 to 16 weeks using the FDA 1930 approved dose schedules. Safe and effective use of more accelerated schedules for VIT have 1931 been reported and some can be considered routine.130,148-150 Rush VIT schedules achieve the 1932 full dose in a matter of days instead of weeks. Some achieve the full dose in 2 to 3 days, and 1933 others in 3-5 days. Rush regimens have been shown to be as safe as weekly schedules and are 1934 used routinely in situations in which patients do not have ready access to specialists for 1935 treatment (in the US armed services and in most European countries). Such rush VIT schedules 1936 can be used when there is an urgent need for protection, when there have been repeated 1937 systemic reactions impeding progress of VIT, and are optional in all cases. Ultra-rush VIT is 1938 described using a build-up schedule over a period of hours instead of days. However, these 1939 regimens, like many rush regimens, do not achieve the maintenance dose until day 2. 1940 Comparison of the frequency of systemic reactions using rush and ultra-rush regimens is 1941 difficult because there are different definitions of rush and ultra-rush regimens, and they use 1942 different classification systems for the severity of systemic reactions. There are also different 1943 outcomes using honeybee or yellow jacket venoms. Rush regimens have been described giving 1944 a maximum dose between 0.4mcg and 20 mcg (cumulative dose 0.7 mcg to 58 mcg) on day 1. 1945 Ultra-rush regimens are reported giving a maximum dose of 40 to 50 mcg (cumulative dose 80 1946 to 111 mcg) on day 1. Certain rush regimens are quite similar to some ultra-rush regimens. The 1947 frequency of systemic reactions was 5% to 10% in most studies of rush regimens, and 0% to 1948 28% (median 11%) with ultra-rush regimens. In a study of jack jumper ant VIT, the reaction 1949 rate was 12% (none severe) using an 8 week schedule, and 65% (6% severe) using an ultra-1950 rush regimen.151 The physician and patient might consider a variety of factors, such as the 1951
characteristics and circumstances of the sting reaction and the patient’s lifestyle and 1952 preferences, in choosing a schedule. 1953 1954 There has been some controversy about the optimum maintenance dose. Initial studies used 1955 100 mcg as the maintenance dose.116,117 One investigator used the 50-mcg maintenance dose 1956 in patients with yellow jacket venom allergy successfully, although some believe that this dose 1957 offers a lesser degree of protection.140,143 Since the introduction of VIT, the same 100 mcg 1958 maintenance dose has been recommended to children as well as adults. In 2 recent studies 1959 children treated with a 50 mcg dose had a frequency of systemic reactions to stings during and 1960 after VIT that was similar to the experience with the 100 mcg dose.151,152 The children in these 1961 studies had a mean age of 9.5 (± 3.2) and 8 (range 2-14) years respectively. Although the 1962 numbers were relatively small, the outcome with 5 years of VIT was better than with 3 (range 1963 2-7) years. Increasing the maintenance dose up to 200 mcg per dose has been effective in 1964 achieving protection in patients who had sting reactions while receiving a 100-mcg maintenance 1965 dose of VIT.153 If the insect that caused the reaction during VIT is unknown, further testing 1966 might be needed to determine whether there is a new or untreated venom sensitivity before 1967 considering an increase in the venom dose. 1968 1969 Summary Statement 22: Continue the maintenance dose monthly for at least 12-18 1970 months, then consider extending the interval to 6 or 8 weeks during several years of 1971 treatment. For patients who continue VIT for longer than 4 years, a 12 week interval 1972 is safe and effective. (Strong Recommendation; C Evidence) 1973
1974 The interval between maintenance dose injections is usually increased to 4 weeks during the 1975 first year and then to every 6 to 8 weeks during subsequent years. A maintenance interval of 4 1976 weeks is recommended for indefinite treatment in the US Food and Drug Administration–1977 approved product package inserts. Experts in the field support the regimen of a 4-week 1978 maintenance interval for 12 to 18 months followed by a 6-week interval for 12 to 18 months 1979 and then 8-week intervals.130,154,155 Twelve week intervals have proven safe and effective for 1980 patients who have had several years of VIT at increasing intervals, but there is less evidence of 1981 efficacy for a 12 week interval in the first 1-2 years of VIT.156,157 A 6-month interval was not 1982 effective.158 1983 1984 The dosage schedule for fire ant whole-body extract immunotherapy is less well defined in 1985 terms of rapidity of buildup. However, most authors recommend a once- or twice-weekly 1986 buildup schedule until a maintenance dose is reached, and the interval between doses can then 1987 be increased. Two examples of dosage schedules are included in Appendix E2. Successful use 1988 of a rush immunotherapy protocol has been published.159,160 Most reports have recommended 1989 a maintenance dose of 0.5 mL of a 1:100 wt/vol vaccine/extract with either Solenopsis invicta 1990 or a mixture of S invicta and Solenopsis richteri extract, although there are some 1991 recommendations for a dose as high as 0.5 mL of a 1:10 wt/vol extract.160-163 A survey of 1992 practicing allergists found that 0.5 mL of a 1:200 wt/vol extract is the most widely prescribed 1993
maintenance dose.162 Evidence continues to accumulate to support the efficacy of this 1994 dose.160,161,163 Special dosing might need to be considered for treatment failures. 1995 1996 1997 (c) Problems During VIT (Adverse effects, Risk factors for severe reactions, Pregnancy, 1998 Medications) 1999 2000 Adverse Effects and Premedication 2001 Safety considerations related to administration of VIT injections are generally the same as those 2002 for other forms of allergen immunotherapy. The major risk of VIT, as with other types of 2003 allergen immunotherapy, is anaphylaxis. Early reports of the incidence of systemic reactions 2004 from VIT were in the range of 12% to 16%, although this incidence is higher than that 2005 experienced by most allergists.144,164,165 When a patient has repeated systemic reactions despite 2006 adjustment of dose and schedule, a rush regimen with pre-medication has been safe and 2007 effective.166 When this is not successful, pre-treatment with omalizumab has been reported to 2008 prevent reactions and enable treatment to the maintenance dose.167-169 2009 2010 Large local reactions to VIT are common but do not presage systemic reactions, and are 2011 generally tolerated if the induration does not exceed 3 to 4 inches in diameter. Premedication 2012 with antihistamines during build-up VIT has been shown to reduce the incidence of local 2013 reactions and mild systemic reactions.170,171 For appropriate interpretation of reactions, 2014 consistency in use or avoidance of antihistamines is suggested. There is evidence that 2015 antihistamine premedication can also improve the efficacy of VIT.172 There is also one report 2016 of reduced local reactions to VIT with montelukast premedication.173 2017 2018 There have been reports of patients who had serum sickness–like reactions from VIT.174,175 2019 Serum sickness has occurred as a sequel to insect stings, with or without an acute systemic 2020 reaction.18,176,177 Although these patients may be at greater risk of anaphylaxis if re-stung, 2021 recurrence of serum sickness has not been observed after initiation of VIT.176 VIT has been 2022 used successfully in this group of patients, but the safety and efficacy of this approach is 2023 unknown. 2024 2025 Practitioners have been uncertain about the safe procedure when beginning a new vial of 2026 venom, or changing from one manufacturer to another. There is no universal answer to these 2027 questions, and no data on which to base recommendations. Hymenoptera venoms are 2028 standardized extracts and should have minimal batch-to-batch variation. When changing to a 2029 different lot number, some physicians reduce the dose initially by 20% to 50% and others 2030 make no adjustment. When changing from one manufacturer to another, most physicians 2031 reduce the dose initially by 20% to 50%. There are known differences between manufacturers 2032 in the species included in the yellow jacket venom mix and the Polistes wasp venom mix, so 2033 appropriate caution is warranted when changing manufacturers. Fire ant whole body extracts 2034 are not standardized and each new vial should be started with caution, similar to the 2035
procedures for aeroallergen immunotherapy. 2036 2037 Risk Factors for Systemic Reactions to VIT 2038 Systemic reactions to VIT are more frequent in honeybee venom allergic patients, those with 2039 previous severe reactions to stings, during rush regimen initial treatment, and with greater time 2040 elapsed since the last sting reaction.97,178 The risk of systemic reactions to VIT injections is also 2041 increased in patients with elevated basal serum tryptase or mastocytosis.97,178-180 2042 2043 There is continued concern about the risk of anaphylaxis in patients taking anti-hypertensive 2044 medications. In patients with insect sting allergy, the risk of more severe systemic reactions to 2045 insect stings in patients not treated with VIT is increased by beta-blockers or ACE 2046 inhibitors.58,181 However, in patients receiving VIT, there is limited and conflicting evidence 2047 that these medications increase the risk of anaphylaxis.180,182,183 The incidence of systemic 2048 reactions to VIT is not significantly affected by these medications. The possibility that the 2049 severity of such reactions, should they occur, might be increased by the medications is 2050 supported by some studies and not by others.184,185 There is limited evidence that the risk 2051 associated with these medications is minimized by withholding the medication for 24 hours 2052 prior to VIT (if medically appropriate).186,187 2053 2054 The Practice Parameters on Anaphylaxis states that the benefits of AIT with Hymenoptera 2055 venoms clearly outweigh the potential risks associated with beta-blockers or ACE inhibitors in 2056 those patients with anaphylaxis to stinging insects who also have cardiovascular disease 2057 requiring these medications.108 Currently, the venom product package insert, and the Practice 2058 Parameter on the management of anaphylaxis suggest that consideration should be given to 2059 the discontinuation of any drug that may worsen an episode of anaphylaxis or complicate its 2060 treatment (eg, beta-adrenergic blockers, angiotensin inhibitors, alpha adrenergic blockers, some 2061 tricyclic antidepressants [e.g., amitriptyline], monoamine oxidase inhibitors, and possibly 2062 angiotensin receptor blockers and renin inhibitors). 2063 2064 Pregnancy 2065 There are scant data on VIT in pregnancy.188 As with other allergen immunotherapy, it is 2066 recommended to avoid beginning or building-up immunotherapy during pregnancy because of 2067 the higher chance of systemic reaction during up-dosing. The risk/benefit ratio must be 2068 considered, especially when the pregnancy overlaps the sting season. Strict avoidance of 2069 outdoor exposure is not always possible, and the risk of anaphylaxis in pregnancy must be 2070 considered. This should be a shared decision that might also consider other risk factors (eg, 2071 severity of previous reactions, frequency of exposure, basal serum tryptase). Also like other 2072 immunotherapy, maintenance dose treatment can be and probably should be continued during 2073 pregnancy. 2074 2075 2076 2077
Duration of VIT 2078 2079 Summary Statements 23: Advise patients who start VIT to continue injections for 5 2080 years. (Strong Recommendation; B Evidence) 2081 2082 Summary Statement 24: Encourage continuation of VIT for an extended time, or 2083 indefinitely, in patients with high-risk factors, such as very severe reaction before 2084 VIT (syncope, hypotension, severe respiratory distress), systemic reaction during 2085 VIT, honeybee allergy, and increased basal serum tryptase levels. (Strong 2086 Recommendation; C Evidence) 2087
Summary Statement 25: Consider continuation of VIT for more than 5 years in 2088 patients with other high risk factors for recurrent or severe sting reactions, such as 2089 underlying cardiovascular or respiratory conditions, select anti-hypertensive 2090 medications, frequent exposure, and limitation of activity due to anxiety about 2091 unexpected stings. (Strong Recommendation; A Evidence) 2092
2093 Guidelines for discontinuation of VIT have evolved since the products were approved in 2094 1979.120,130,189-191 The package insert for the venom extract has always recommended that VIT 2095 be continued indefinitely. Criteria that have been suggested for stopping VIT include treatment 2096 for a finite length of time (3-5 years), a decrease in serum venom-specific IgE antibodies to 2097 insignificant levels, or conversion to a negative skin test response. Some authors recommend 2098 repeat testing every 2 to 3 years, although negative results are uncommon until 5 years or 2099 longer. Repeat skin (or venom-specific IgE serum) testing is not required for consideration of 2100 discontinuing VIT. If both skin tests and serum tests are negative for venom-IgE there would 2101 seem to be no justification for continued treatment, although there is inadequate evidence on 2102 which to base any recommendation. An increasing body of evidence suggests that despite the 2103 persistence of a positive skin test response, 80% to 90% of patients will not have a systemic 2104 reaction to an insect sting if VIT is stopped after 3 to 5 years, and they can safely stop 2105 immunotherapy after that period of treatment.120,190,192-201 There are no specific tests to 2106 distinguish which patients will relapse after stopping VIT, but there is a higher risk in some 2107 patients than in others. Relapse is less likely with 5 years than with 3 years of VIT.190,197 2108 Relapse is less likely in younger children than in adolescents or adults.201 The small risk after 2109 discontinuation of VIT is a more significant concern for patients who have a history of severe 2110 anaphylaxis with shock or loss of consciousness, those who are allergic to honeybee stings 2111 (versus vespid stings), and those who had a systemic reaction during VIT (to a venom injection 2112 or a sting).120,190,197,200,202 A few patients who had previously experienced severe anaphylaxis 2113 with loss of consciousness and then, after more than 5 years of immunotherapy, had negative 2114 in vitro test or skin test responses, have later experienced systemic reactions to subsequent 2115 stings after stopping VIT.120,194,203 Fatal reactions to stings have occurred after stopping VIT in 2116 patients with mastocytosis.103 Although this occurrence is rare, some recommend continuation 2117 of immunotherapy indefinitely in patients with a history of severe anaphylaxis or with mast cell 2118
disorders. The decision to stop immunotherapy can involve consideration of several factors by 2119 the patient and physician, including (1) the severity of the initial reaction, (2) the basal serum 2120 tryptase, (3) the frequency of exposure, (4) the presence of concomitant disease and 2121 medications, (5) the effect of such action on work and leisure activities, and (6) the patient’s 2122 preferences. This decision requires a context-sensitive flexibility based on the available 2123 evidence. 2124 2125 2126 C. Fire ant immunotherapy 2127 2128 Summary Statements 26: Recommend immunotherapy with imported fire ant 2129 whole-body extracts to all patients who have experienced a systemic reaction to a 2130 fire ant sting and who have positive skin test responses or allergen- specific 2131 serologic test results with imported fire ant whole-body extract. (Strong 2132 Recommendation; B Evidence) 2133 2134
Summary Statement 27: Consider whole body extract immunotherapy in patients 2135 who have only cutaneous manifestations to fire ant stings, because the natural 2136 history of fire ant hypersensitivity has not been well elucidated and there is 2137 increased risk of fire ant stings in children who live in areas where fire ants are 2138 prevalent. (Recommendation; D Evidence) 2139
2140 2141 Compared with other stinging insects, less is known about the natural history of IFA 2142 hypersensitivity and the effectiveness of immunotherapy.25,62,161,163,204,205 IFA-WBE has been 2143 shown to contain relevant venom allergens, and evidence continues to accumulate, despite the 2144 absence of a placebo- controlled study, to support its efficacy for use as a diagnostic and 2145 therapeutic agent.62,64,65,160,161,192,206-209 The current criteria for immunotherapy for IFA allergy 2146 are similar to those for other Hymenoptera (i.e., a history of a systemic reaction and 2147 demonstration of IFA antigen–specific IgE antibodies by means of skin or in vitro testing). There 2148 is a high frequency of IFA re-stings in endemic areas, even in patients on IFA WBE IT, who it 2149 might be expected would actively practice avoidance techniques.25,210,211 Given the high 2150 frequency of IFA stings, both one and two day rush IT schedules have been reported in order 2151 to expedite the achievement of a therapeutic dose.159,160 Most systemic reactions occur from a 2152 single sting, and a systemic reaction to skin testing is a risk factor for a systemic reaction to IFA 2153 WBE IT.212 For stability, IFA WBE should be delivered alone and not mixed with other 2154 allergens.213,214 The most common maintenance dose, using a 1:20 w/v stock vial, is 0.5 mL 2155 1:200 w/v.215 Controversy exists regarding the management of patients who have systemic 2156 reactions that are confined to the skin. There has been no prospective study, but one 2157 retrospective survey suggests that cutaneous-only systemic reactions from IFA in children 2158 usually do not progress to more serious reactions.204
The majority of allergists, but not all, in 2159
IFA–endemic areas do not routinely recommend immunotherapy for children who have had only 2160 generalized cutaneous reactions.162 Thus immunotherapy in these patients is considered to be 2161 optional at the present time. Lifestyle consideration, parental preferences, and other factors 2162 might influence this decision. 2163
Summary Statement 28: Consider continuation of imported fire ant whole-body 2164 extract for more than 5 years in patients with imported fire ant allergy since the 2165 optimal duration of this therapy has been less well studied and the frequency of 2166 exposure is high. (Recommendation; C Evidence) 2167
The optimal duration of imported fire ant immunotherapy is less well defined. One retrospective 2168 survey suggests an equal risk of a sting reaction whether a patient received more than 3 years 2169 of immunotherapy or less than 3 years of immunotherapy, although the numbers were small.192 2170 A survey of allergists indicated a great deal of variation in recommendations regarding the 2171 duration of immunotherapy for fire ant allergy.4 Some allergists recommend indefinite 2172 treatment. Most allergists consider stopping immunotherapy after a specified period (usually 4-5 2173 years), either empirically or only when skin test responses become negative. Until further data 2174 are available, a definitive recommendation about the duration of immunotherapy for fire ants 2175 cannot be made. 2176
2177
2178 REFERENCES 2179 2180 2181 1. Demain JG, Gessner BD, McLaughlin JB, Sikes DS, Foote JT. Increasing insect 2182 reactions in Alaska: Is this related to changing climate? Asthma Allergy Proc 2183 2009;30:238-43. 2184 2. Freeman TM. Cold blooded. Curr Opin Allergy Clin Immunol 2008;8:308-9. 2185 3. deGroot H. Allergy to bumblebees. Curr Opin Allergy Clin Immunol 2006;6:294-7. 2186 4. Moffitt JE. Allergic reactions to insect stings and bites. South Med J 2187 2003;96:1073-9. 2188 5. Schumacher ML, Schmidt JO, Egen NB, Dillon KA. Biochemical variability of 2189 venoms from individual European and africanized honeybees (Apis mellifera). J Allergy 2190 Clin Immunol 1992;90:59-65. 2191 6. Hoffman DR. Allergens in Hymenoptera venom. XXV. The amino acid sequence 2192 of Antigen 5 molecules. The structural basis of antigenic crossreactivity. J Allergy Clin 2193 Immunol 1993;92:707-16. 2194 7. King T, Joslyn A, Kochoumian L. Antigenic cross-reactivity of venom proteins 2195 from hornets, wasps and yellow jackets. J Allergy Clin Immunol 1985;75:621-8. 2196
8. Reisman RE, Mueller U, Wypych J, Eliott W, Arbesman CE. Comparison of the 2197 allergenicity and antigenicity of yellow jacket and hornet venoms. J Allergy Clin 2198 Immunol 1982;69:268-74. 2199 9. Reisman RE, Wypych JI, Mueller UR, Grant JA. Comparison of the allergenicity 2200 and antigenicity of Polistes venom and other vespid venoms. J Allergy Clin Immunol 2201 1982;70:281-7. 2202 10. Reisman RE, Muller UR, Wypych JI, et a. Studies of coexisting honey bee and 2203 vespid venom sensitivity. J Allergy Clin Immunol 1984;73:246. 2204 11. Stapel SO, Waanders-LijsterdeRaadt J, vanToorenenbergen AW, DeGroot H. 2205 Allergy to bumble bee venom. II. IgE cross-reactivity between bumble bee and honey 2206 bee venom. Allergy 1998;53:769-77. 2207 12. Hoffman DR, Dove DE, Moffitt JE, Stafford CT. Allergens in Hymenptera venom. 2208 XXI. Cross-reactivity and multiple reactivity between fire ant venom and bee and wasp 2209 venoms. J Allergy Clin Immunol 1988;82:828-34. 2210 13. Rhoades RB, Kalof D, Bloom F, Wittig HJ. Cross reacting antigens between 2211 imported fire ant and other Hymenoptera species. Ann Allergy 1978;40:100-4. 2212 14. Golden DBK, Kelly D, Hamilton RG, Craig TJ. Venom immunotherapy reduces 2213 large local reactions to insect stings. J Allergy Clin Immunol 2009;123:1371-75. 2214 15. Severino M, Bonadonna P, Passalacqua G. Large local reactions from stinging 2215 insects: from epidemiology to management. Curr Opin Allergy Clin Immunol 2216 2009;9:334-7. 2217 16. Ridolo E, Olivieri E, Montagni M, Rolli A, Senna GE. Type I variant Kounis 2218 syndrome secondary to wasp sting. Ann Allergy Asthma Immunol 2012;109:79-81. 2219 17. Borer-Reinhold B, Haeberli G, Bitzenhofer M, et al. An increase in serum tryptase 2220 even below 11.4 ng/ml may indicate a mast cell-mediated hypersensitivity reaction: a 2221 prospective study in Hymenoptera venom allergic patients. Clin Exp Allergy 2222 2011;41:1777-83. 2223 18. Reisman RE, Livingston A. Late-onset allergic reactions, including serum 2224 sickness, after insect stings. J Allergy Clin Immunol 1989;84:331-7. 2225 19. Hogendijk S, Hauser C. Wasp sting-associated cold urticaria. Allergy 2226 1997;52:1145-6. 2227 20. Wong CC, Borici-Mazi R. Delayed-onset cold anaphylaxis after Hymenoptera 2228 sting. Ann Allergy Asthma Immunol 2012;109:77-8. 2229 21. Bilo MB, Bonifazi F. The natural history and epidemiology of insect venom 2230 allergy: clinical implications. Clin Exp Allergy 2009;39:1467-76. 2231 22. Sturm GJ, Kranzelbinder B, Schuster C, et al. Sensitization to Hymenoptera 2232 venoms is common, but systemic sting reactions are rare. J Allergy Clin Immunol 2233 2014;133:1635-43. 2234
23. Bilo BM, Bonifazi F. Epidemiology of insect-venom anaphylaxis. Curr Opin Allergy 2235 Clin Immunol 2008;8:330-7. 2236 24. Graif Y, Romano-Zelekha O, Livne I, Green MS, Shohat T. Allergic reactions to 2237 insect stings: results from a national survey of 10,000 junior high school children in 2238 Israel. J Allergy Clin Immunol 2006;117:1435-9. 2239 25. Tracy JM, Demain JG, Quinn JM, et a. The natural history of exposure to the 2240 imported fire ant. J Allergy Clin Immunol 1995;95:824-8. 2241 26. Bilo BM, Rueff F, Mosbech H, Bonifazi F, Oude-Elberink JNG, EAACI. Diagnosis of 2242 Hymenoptera venom allergy. Allergy 2005;60:1339-49. 2243 27. Golden DBK, Kagey-Sobotka A, Norman PS, Hamilton RG, Lichtenstein LM. 2244 Outcomes of allergy to insect stings in children with and without venom 2245 immunotherapy. N Engl J Med 2004;351:668-74. 2246 28. Golden DB. Large local reactions to insect stings. J Allergy Clin Immunol Prac 2247 2015;3:331-4. 2248 29. Graft DF, Schuberth KC, Kagey-Sobotka A, et al. A Prospective study of the 2249 natural history of large local reactions following Hymenoptera stings in children. J 2250 Pediatr 1984;104:664-8. 2251 30. Mauriello PM, Barde SH, Georgitis JW, Reisman RE. Natural history of large local 2252 reactions from stinging insects. J Allergy Clin Immunol 1984;74:494-8. 2253 31. Golden DBK, Breisch NL, Hamilton RG, et al. Clinical and entomological factors 2254 influence the outcome of sting challenge studies. J Allergy Clin Immunol 2006;117:670-2255 5. 2256 32. vanderLinden PG, Hack CE, Struyvenberg A, vanderZwan JK. Insect-sting 2257 challenge in 324 subjects with a previous anaphylactic reaction: Current criteria for 2258 insect-venom hypersensitivity do not predict the occurrence and the severity of 2259 anaphylaxis. J Allergy Clin Immunol 1994;94:151-9. 2260 33. Reisman RE, Dvorin DD, Randolph CC, Georgitis JW. Stinging insect 2261 allergy:natural history and modification with venom immunotherapy. J Allergy Clin 2262 Immunol 1985;75:735-40. 2263 34. Richter AG, Nightingale P, Huissoon AP, Krishna MT. Risk factors for systemic 2264 reactions to bee venom in British beekeepers. Ann Allergy Asthma Immunol 2265 2011;106:159-63. 2266 35. Greene A, Breisch NL. Avoidance of bee and wasp stings: an entomological 2267 perspective. Curr Opin Allergy Clin Immunol 2005;5:337-41. 2268 36. Oude-Elberink JN, vanderHeide S, Guyatt GH, Dubois A. Analysis of the burden of 2269 treatment in patients receiving an Epi-Pen for yellow jacket anaphylaxis. J Allergy Clin 2270 Immunol 2006;118:699--704. 2271
37. Oude-Elberink JNG, deMonchy JGR, vanderHeide S, Guyatt GH, Dubois AEJ. 2272 Venom immunotherapy improves health-related quality of life in yellow jacket allergic 2273 patients. J Allergy Clin Immunol 2002;110:174-82. 2274 38. Franken HH, Dubois AEJ, Minkema HJ, vanderHeide S, deMonchy JGR. Lack of 2275 reproducibility of a single negative sting challenge response in the assessment of 2276 anaphylactic risk in patients with suspected yellow jacket hypersensitivity. J Allergy Clin 2277 Immunol 1994;93:431-6. 2278 39. Georgitis J, Reisman R. Venom skin tests in insect-allergic and insect non-allergic 2279 populations. J Allergy Clin Immunol 1985;76:803-7. 2280 40. Hunt KJ, Valentine MD, Sobotka AK, Lichtenstein LM. Diagnosis of allergy to 2281 stinging insects by skin testing with Hymenoptera venoms. Ann Intern Med 1976;85:56-2282 9. 2283 41. Quirt JA, Wen X, Kim J, Herrero AJ, Kim HL. Venom allergy testing: is a graded 2284 approach necessary? Ann Allergy Asthma Immunol 2016;116:49-51. 2285 42. Strohmeier B, Aberer W, Bokanovic D, Komericki P, Sturm GJ. Simultaneous 2286 intradermal testing with Hymenoptera venoms is safe and more efficient than 2287 sequential testing. Allergy 2013;68:542-4. 2288 43. Yocum M, Gosselin v, Yungunger J. Safety and efficacy of an accelerated method 2289 for venom skin testing. J Allergy Clin Immunol 1996;97:1424-5. 2290 44. Bernstein IL, Li JT, Bernstein DI, et al. Allergy diagnostic testing: an updated 2291 practice parameter. Ann Allergy Asthma Immunol 2008;100:S1-S148. 2292 45. Oppenheimer J, Nelson HS. Skin testing. Ann Allergy Asthma Immunol 2006;96 2293 (Suppl 1):S6-12. 2294 46. Krishna MT, Ewan PW, Diwakar L, et al. Diagnosis and management of 2295 Hymenoptera venom allergy. British Society for Allergy and Clinical Immunology 2296 (BSACI) guidelnes. Clin Exp Allergy 2011;41:1201-20. 2297 47. Zeleznick LD, Hunt KJ, Sobotka AK, Valentine MD, Tippett LO, Lichtenstein LM. 2298 Diagnosis of Hymenoptera hypersensitivity by skin testing with Hymenoptera venoms. J 2299 Allergy Clin Immunol 1977;59:2-9. 2300 48. Norman PS. Skin testing. In: Rose NR, Friedman H, eds. Manual of Clinical 2301 Immunology. 3 ed. Washington D.C.: American Society of Microbiology; 1986:660-3. 2302 49. Graif Y, Confino-Cohen R, Goldberg A. Reproducibility of skin testing and serum 2303 venom-specific IgE in Hymenoptera venom allergy. Ann Allergy 2006;96:24-9. 2304 50. Golden DBK, Kagey-Sobotka A, Hamilton RG, Norman PS, Lichtenstein LM. Insect 2305 allergy with negative venom skin tests. J Allergy Clin Immunol 2001;107:897-901. 2306 51. Golden DBK, Tracy JM, Freeman TM, Hoffman DR, Insect CA. Negative venom 2307 skin test results in patients with histories of systemic reaction to a sting. (Rostrum 2308 article). J Allergy Clin Immunol 2003;112:495-8. 2309
52. Reisman RE. Insect sting allergy: The dilemma of the negative skin test reactor. 2310 J Allergy Clin Immunol 2001;107:781-2. 2311 53. Goldberg A, Confino-Cohen R. Timing of venom skin tests and IgE 2312 determinations after insect sting anaphylaxis. J Allergy Clin Immunol 1997;100:183-4. 2313 54. Bonadonna P, Perbellini O, Passalacqua G, et al. Clonal mast cell disorders in 2314 patients with systemic reactions to Hymenoptera stings and increased serum tryptase 2315 levels. J Allergy Clin Immunol 2009;123:680-6. 2316 55. Haeberli G, Bronnimann M, Hunziker T, Muller U. Elevated basal serum tryptase 2317 and hymenoptera venom allergy: relation to severity of sting reactions and to safety 2318 and efficacy of venom immunoltherapy. Clin Exp Allergy 2003;33:1216-20. 2319 56. Muller UR. Elevated baseline serum tryptase, mastocytosis and anaphylaxis. Clin 2320 Exp Allergy 2009;39:620-2. 2321 57. Niedoszytko M, Bonadonna P, Oude-Elberink JNG, Golden DBK. Epidemiology, 2322 diagnosis, and treatment of Hymenoptera venom allergy in mastocytosis patients. in 2323 Mastocytosis (Eds: Akin C, Alam R). Immunol Allergy Clin North Am 2014;34:365-81. 2324 58. Rueff F, Przybilla B, Bilo MB, et al. Predictors of severe systemic anaphylactic 2325 reactions in patients with Hymenoptera venom allergy: importance of baseline serum 2326 tryptase - a study of the EAACI Interest Group on Insect Venom Hypersensitivity. J 2327 Allergy Clin Immunol 2009;124:1047-54. 2328 59. Hamilton RG. Responsibility for quality IgE antibody results rests ultimately with 2329 the referring physician. Ann Allergy Asthma Immunol 2001;86:353-4. 2330 60. Hamilton RG. Diagnostic methods for insect sting allergy. Curr Opin Allergy Clin 2331 Immunol 2004;4:297-306. 2332 61. Hamilton RG. Clinical laboratories worldwide need to report IgE antibody results 2333 on clinical specimens as analytical results and not use differential positive thresholds. J 2334 Allergy Clin Immunol 2015;136:811-2. 2335 62. DeShazo RD, Butcher BT, Banks WA. Reactions to the stings of the imported fire 2336 ant. N Engl J Med 1990;323:462-6. 2337 63. Kemp SF, deShazo RD, Moffitt JE, et a. Expanding habitat of the imported fire 2338 ant: a public health concern. J Allergy Clin Immunol 2000;105:683-91. 2339 64. Triplett R. Sensitivity to the imported fire ant: successful treatment with 2340 immunotherapy. South Med J 1973;66:477-80. 2341 65. Rhoades RB, Schafer WL, Newman M, et al. Hypersensitivity to the imported fire 2342 ant in Florida. Report of 104 cases. J Fla Med Assoc 1977;64:247-54. 2343 66. Golden DBK, Kelly D, Hamilton RG, Wang NY, Kagey-Sobotka A. Dialyzed venom 2344 skin tests for identifying yellow jacket-allergic patients not detected using standard 2345 venom. Ann Allergy Asthma Immunol 2009;102:47-50. 2346
67. Bonadonna P, Zanotti R, Melioli G, et al. The role of basophil activation test in 2347 special populations with mastocytosis and reactions to Hymenoptera sting. Allergy 2348 2012;67:962-5. 2349 68. Korosec P, Erzen R, Silar M, Bajrovic N, Kopac P, Kosnik M. Basophil 2350 responsiveness in patients with insect sting allergies and negative venom-specific 2351 immunoglobulin E and skin prick test results. Clin Exp Allergy 2009;39:1730-7. 2352 69. Kucera P, Cvackova M, Hulikova K, Juzova O, Pachl J. Basophil activation can 2353 predict clinical sensitivity in patients after venom immunotherapy. J Investig Allergol 2354 Immunol 2010;20:110-16. 2355 70. Kosnik M, Silar M, Bajrovic N, Music E, Korosec P. High sensitivity of basophils 2356 predicts side effects in venom immunotherapy. Allergy 2005;60:1401-6. 2357 71. Peternelj A, Silar M, Erzen R, Kosnik M, Korosec P. Basophil sensitivity in patients 2358 not responding to venom immunotherapy. Int Arch Allergy Immunol 2008;146:248-54. 2359 72. Zitnik SE, Vesel T, Avcin T, Silar M, Kosnik M, Korosec P. Monitoring honeybee 2360 venom immunotherapy in children with the basophil activation test. Pediatr Allergy 2361 Immunol 2012;23:166-72. 2362 73. Kleine-Tebbe J, Erdmann S, Knol EF, MacGlashan DW, Poulsen LK, Gibbs BF. 2363 Diagnostic tests based on Human Basophils: Potentials, pitfalls and perspectives. Int 2364 Arch Allergy Immunol 2006;141:79-90. 2365 74. MacGlashan DWJ. Basophil activation testing. J Allergy Clin Immunol 2366 2013;132:777-87. 2367 75. Sturm GJ, Kranzelbinder B, Sturm EM, Heinemann A, Groselj-Strele A, Aberer W. 2368 The basophil activation test in the diagnosis of allergy: technical issues and critical 2369 factors. Allergy 2009;64:1319-26. 2370 76. Ollert M, Blank S. Anaphylaxis to insect venom allergens: role of molecular 2371 diagnostics. Curr Allergy Asthma Rep 2015;15:26 2372 77. Hofmann SC, Pfender N, Weskesser S, Huse-Marp J, Jakob T. Added value of IgE 2373 detection to rApi m 1 and r Ves v 5 in patients with Hymenoptera venom allergy. J 2374 Allergy Clin Immunol 2011;127:265-7. 2375 78. Korosec P, Valenta R, Mitterman I, et al. Low sensitivity of commercially available 2376 rApi m 1 for diagnosis of honeybee venom allergy. J Allergy Clin Immunol 2377 2011;128:671-3. 2378 79. Muller UR, Johansen N, Petersen AB, Fromberg-Nielsen J, Haeberli G. 2379 Hymenoptera venom allergy: analysis of double positivity to honey bee and Vespula 2380 venom by estimation of IgE antibodies to species-specific major allergens Api m1 and 2381 Ves v5. Allergy 2009;64:543-8. 2382 80. Korosec P, Valenta R, Mitterman I, et al. High sensitivity of CAP-FEIA rVes v 5 2383 and rVes v 1 for diagnosis of Vespula venom allergy. J Allergy Clin Immunol 2384 2012;129:1406-8. 2385
81. Cifuentes L, Vosseler S, Blank S, et al. Identification of Hymenoptera venom-2386 allergic patients with negative specific IgE to venom extract by using recombinant 2387 allergens. J Allergy Clin Immunol 2014;133:909-10. 2388 82. Rafei-Shamsabadi D, Muller S, Pfutzner W, Spillner E, Rueff F, Jakob T. 2389 Recombinant allergens rarely allow identification of Hymenoptera venom-allergic 2390 patients with negative specific IgE to whole venom preparations. J Allergy Clin Immunol 2391 2014;134:493-4. 2392 83. Eberlein B, Krischan L, Darsow U, Ollert M. Double positivity to bee and wasp 2393 venom: improved diagnostic procedure by recombinant allergen-based IgE testing and 2394 basophil activation test including data about cross-reactive carbohydrate determinants. 2395 J Allergy Clin Immunol 2012;130:155-61. 2396 84. Mitterman I, Zidarn M, Silar M, Markovic-Housley Z, Aberer W. Recombinant 2397 allergen based IgE testing to distinguish bee and wasp allergy. J Allergy Clin Immunol 2398 2010;125:1300-7. 2399 85. Muller UR, Schmid-Grendelmeier P, Hausmann O, Helbling A. IgE to recombinant 2400 allergens Api m 1, Ves v 1, and Ves v 5 distinguish double sesnitization from 2401 crossreaction in venom allergy. Allergy 2012;67:1069-73. 2402 86. Sturm GJ, Hemmer W, Hawranek T, et al. Detection of IgE to recombinant Api m 2403 1 and rVes v 5 is valuable but not sufficient to distinguish bee from wasp venom 2404 allergy. J Allergy Clin Immunol 2011;128:247-8. 2405 87. Monsalve RI, Vega A, Marques L, et al. Component-resolved diagnosis of vespid 2406 venom-allergic individuals: phospholipases and antigen 5s are necessary to identify 2407 Vespula or Polistes sensitization. Allergy 2012;67:528-36. 2408 88. Bonadonna P, Lombardo C, Zanotti R. Mastocytosis and allergic disease. J 2409 Investig Allergol Clin Immunol 2014;24:288-97. 2410 89. Brockow K, Jofer C, Behrendt H, Ring J. Anaphylaxis in patients with 2411 mastocytosis: a study on history, clinical features and risk factors in 120 patients. 2412 Allergy 2008;63:226-32. 2413 90. Castells M, Hornick J, Akin C. Anaphylaxis after Hymenioptera sting: Is it venom 2414 allergy, a clonal disorder, or both? J Allergy Clin Immunol Prac 2015;3:350-5. 2415 91. Bonadonna P, Zanotti R, Pagani M, et al. How much specific is the association 2416 between Hymenoptera venom allergy and mastocytosis? Allergy 2009;64:1379-82. 2417 92. Valent P, Akin C, Arock M, et al. Definitions, criteria, and glabal classification of 2418 mast cell disorders with special reference to mast cell activation syndromes: A 2419 consensus proposal. Int Arch Allergy Immunol 2012;157:215-25. 2420 93. Tracy J, Olsen J, Carlson J. A "difficult" insect allergy patient: Reliable history of a 2421 sting, but all testing negative. Curr Opin Allergy Clin Immunol 2015;15:358-63. 2422
94. Alvarez-Twose I, Zanotti R, Gonzalez-de-Olano D, et al. Nonaggressive systemic 2423 nastocytosis (SM) without skin lesions associated with insect-induced anaphylaxis shows 2424 unique features versus other indolent SM. J Allergy Clin Immunol 2014;133:520-8. 2425 95. Guenova E, Volz T, Echner M, et al. Basal serum tryptase as risk assessment for 2426 severe Hymenoptera sting reactions in elderly. Allergy 2010;65:919-23. 2427 96. Zanotti R, Lombardo C, Passalacqua G, et al. Clonal mast cell disorders in 2428 patients with severe Hymenoptera venom allergy and normal serum tryptase levels. J 2429 Allergy Clin Immunol 2015;136:135-9. 2430 97. Rueff F, Przybilla B, Bilo MB, et al. Predictors of side effects during the buildup 2431 phase of venom immunotherapy for Hymenoptera venom allergy: The importance of 2432 baseline serum tryptase. J Allergy Clin Immunol 2010;126:105-11. 2433 98. Blum S, Gunzinger A, Muller UR, Helbling A. Influence of total and specific IgE, 2434 serum tryptase, and age on severity of allergic reactions to Hymenoptera stings. Allergy 2435 2011;66:222-8. 2436 99. Stoevesandt J, Hain J, Kerstan A, Trautmann A. Over- and underestimated 2437 parameters in severe Hymenoptera venom-induced anaphylaxis: Cardiovascular 2438 medication and absence of urticaria/angioedema. J Allergy Clin Immunol 2012;130:698-2439 704. 2440 100. Bonadonna P, Gonzalez-de-Olano D, Zanotti R, et al. Venom immunotherapy in 2441 patients with clonal mast cell disorders: Efficacy, safety, and practical considerations. J 2442 Allergy Clin Immunol: In Practice 2013;1:474-8. 2443 101. Gonzalez-de-Olano D, Alvarez-Twose I, Esteban-Lopez MI, et al. Safety and 2444 effectiveness of immunotherapy in patients with indolent systemic mastocytosis 2445 presenting with Hymenoptera venom anaphylaxis. J Allergy Clin Immunol 2446 2008;121:519-26. 2447 102. Niedoszytko M, deMonchy J, vanDoormaal JJ, Jassem E, Oude-Elberink JNG. 2448 Mastocytosis and insect venom allergy: diagnosis, safety and efficacy of venom 2449 immunotherapy. Allergy 2009;64:1237-45. 2450 103. Oude-Elberink J, deMonchy J, Kors J, vanDoormaal J, Dubois A. Fatal anaphylaxis 2451 after a yellow jacket sting despite venom immunotherapy in two patients with 2452 mastocytosis. J Allergy Clin Immunol 1997;99:153-4. 2453 104. Bonadonna P, Zanotti R, Muller U. Mastocytosis and insect venom allergy. Curr 2454 Opin Allergy Clin Immunol 2010;10:347-53. 2455 105. Pravettoni V, Piantanida M, Primavesi L, Forti S, Pastorello EA. Basal platelet-2456 activating factor acetylhydrolase: Prognostic marker of severe Hymenoptera venom 2457 anaphylaxis. J Allergy Clin Immunol 2014;133:1218-20. 2458 106. Vadas P, Gold M, Perelman B, et al. Platelet-activating factor, PAF 2459 acetylhydrolase, and severe anaphylaxis. N Engl J Med 2008;358:28-35. 2460
107. Kemp SF, Lockey RF, Simons FE, WAO ahcoeia. Epinephrine: the drug of choice 2461 for anaphylaxis. A statement of the World Allergy Organization. Allergy 2008;63:1061-2462 70. 2463 108. Lieberman P, Nicklas RA, Randolph C, et al. Anaphylaxis – a practice parameter 2464 update 2015. Ann Allergy Asthma Immunol 2015;115:341-84. 2465 109. Simons FER, Roberts JR, Gu X, Simons KJ. Epinephrine absorption in children 2466 with a history of anaphylaxis. J Allergy Clin Immunol 1998;101:33-7. 2467 110. Simons FE. Epinephrine absorption in adults: Intramuscular versus subcutaneous 2468 injection. JAllergy Clin Immunol 2001;108:871-3. 2469 111. Bautista E, Simons FE, Simons KJ, et al. Epinephrine fails to hasten 2470 hemodynamic recovery in fully developed canine anaphylactic shock. Int Arch Allergy 2471 Immunol 2002;128:151-64. 2472 112. Bock SA, Munoz-Furlong A, Sampson HA. Further fatalities caused by 2473 anaphylactic reactions to food, 2001-2006. J Allergy Clin Immunol 2007;119:1016-8. 2474 113. Hoffman DR. Fatal reactions to Hymenoptera stings. Allergy Asthma Proc 2475 2003;24:123-7. 2476 114. Sampson HA, Mendelson L, Rosen JP. Fatal and near-fatal reactions to food in 2477 children and adolescents. N Engl J Med 1992;327:380-4. 2478 115. Brown SG, Wiese MD, Blackman KE, Heddle RJ. Ant venom immunotherapy: a 2479 double-blind placebo-controlled crossover trial. Lancet 2003;361:1001-6. 2480 116. Hunt KJ, Valentine MD, Sobotka AK, Benton AW, Amodio FJ, Lichtenstein LM. A 2481 controlled trial of immunotherapy in insect hypersensitivity. N Engl J Med 2482 1978;299:157-61. 2483 117. Muller U, Thurnheer U, Patrizzi R, Spiess J, Hoigne R. Immunotherapy in bee 2484 sting hypersensitivity: Bee venom versus wholebody extract. Allergy 1979;34:369-78. 2485 118. Muller UR. Cardiovascular disease and anaphylaxis. Curr Opin Allergy Clin 2486 Immunol 2007;7:337-41. 2487 119. Ghaffari G, Craig T, Golden D, Chegini S. Delayed and recurrent anaphylactic 2488 reaction to yellow jacket sting. (abstract). J Allergy Clin Immunol 2006;117:S309. 2489 120. Golden DBK, Kagey-Sobotka A, Lichtenstein LM. Survey of patients after 2490 discontinuing venom immunotherapy. J Allergy Clin Immunol 2000;105:385-90. 2491 121. Lantner R, Reisman RE. Clinical and immunologic features and subsequent 2492 course of patients with severe insect sting anaphylaxis. J Allergy Clin Immunol 2493 1989;84:900-6. 2494 122. Reisman RE. Natural history of insect sting allergy: Relationship of severity of 2495 symptoms of initial sting anaphylaxis to re-sting reactions. J Allergy Clin Immunol 2496 1992;90:335-9. 2497
123. Pucci S, Antonicelli L, Bilo MB, Garritani MS, Bonifazi F. The short interval 2498 between two stings as a risk factor for developing Hymenoptera venom allergy. Allergy 2499 1994;49:894-6. 2500 124. Severino M, Bonadonna P, Bilo MB, et al. Safety and efficacy of immunotherapy 2501 with Polistes dominulus venom: results from a large Italian database. Allergy 2502 2009;64:1229-30. 2503 125. Walker R, Jacobs J, Tankersly M, Hagan L, Freeman T. Rush immunotherapy for 2504 the prevention of large local reactions secondary to imported fire ant stings. J Allergy 2505 Clin Immunol 1999;103:S180. 2506 126. Bousquet J, Menardo J-L, Aznar R, Robinet-Levy M, Michel F-B. Clinical and 2507 immunologic survey in beekeepers in relation to their sensitization. J Allergy Clin 2508 Immunol 1984;73:332-40. 2509 127. Light WC, Reisman RE, Wypych JI, Arbesman CE. Clinical and immunologic 2510 studies of beekeepers. Clin Allergy 1975;5:389-95. 2511 128. Valentine MD, Schuberth KC, Kagey-Sobotka A, et al. The value of 2512 immunotherapy with venom in children with allergy to insect stings. N Engl J Med 2513 1990;323:1601-3. 2514 129. Oude-Elberink JNG, vanderHeide S, Guyatt GH, Dubois AEJ. Immunotherapy 2515 improves health-related quality of life in adult patients with dermal reactions following 2516 yellow jacket stings. Clin Exp Allergy 2009;39:883-9. 2517 130. Bonifazi F, Jutel M, Bilo BM, Birnbaum J, Muller U, EAACI. Prevention and 2518 treatment of Hymenoptera venom allergy: guidelines for clinical practice. Allergy 2519 2005;60:1459-70. 2520 131. Golden DB. Insect sting allergy and venom immunotherapy: A model and a 2521 mystery. J Allergy Clin Immunol 2005;115:439-47. 2522 132. Reisman RE. Insect stings. N Engl J Med 1994;331:523--7. 2523 133. Graft DF. Insect sting allergy. Med Clin N Am 2006;90:211-32. 2524 134. Golden DBK, Langlois J, Valentine MD. Treatment failures with whole body 2525 extract therapy of insect sting allergy. JAMA 1981;246:2460-63. 2526 135. Settipane GA, Chafee FH. Natural history of allergy to Hymenoptera. Clin Allergy 2527 1979;9:385-91. 2528 136. Blaauw PJ, Smithuis LOMJ. The evaluation of the common diagnostic methods of 2529 hypersensitivity for bee and yellow jacket venom by means of an in-hospital insect 2530 sting. J Allergy Clin Immunol 1985;75:556-62. 2531 137. Rueff F, Przybilla B, Muller U, Mosbech H. The sting challenge test in 2532 Hymenoptera venom allergy. Allergy 1996;51:216-25. 2533 138. Valentine MD. Insect sting anaphylaxis. Ann Intern Med 1993;118:225-6. 2534
139. Baker TW, Forester JP, Johnson ML, Stolfi A, Stahl MC. The HIT study: 2535 Hymenoptera identification test – how accurate are people at identifying flying insects? 2536 Ann Allergy Asthma Immunol 2014;113:267-70. 2537 140. Reisman RE, Livingston A. Venom immunotherapy: 10 years of experience with 2538 administration of single venoms and 50 micrograms maintenance dose. J Allergy Clin 2539 Immunol 1992;89:1189-95. 2540 141. Golden DBK. Insect Allergy. In: Adkinson NF YJ, Bochner BS, Busse WW, Holgate 2541 ST, Lemanske RF, Simons FER, ed. Middleton's Allergy: Principles and Practice, 8th 2542 edition. Philadephia: Elsevier; 2014:1260-73. 2543 142. Hamilton RH, Wisenauer JA, Golden DBK, Valentine MD, Jr NFA. Selection of 2544 Hymenoptera venoms for immunotherapy based on patients' IgE antibody cross-2545 reactivity. J Allergy Clin Immunol 1993;92:651-9. 2546 143. Golden DBK, Kagey-Sobotka A, Valentine MD, Lichtenstein LM. Dose dependence 2547 of Hymenoptera venom immunotherapy. J Allergy Clin Immunol 1981;67:370-4. 2548 144. Golden DBK, Valentine MD, Kagey-Sobotka A, Lichtenstein LM. Regimens of 2549 Hymenoptera venom immunotherapy. Ann Intern Med 1980;92:620-4. 2550 145. Roumana A, Pitsios C, S Vartholomaios EK, Kontou-Fili K. The safety of initiating 2551 Hymenoptera immunotherapy at 1 microgram of venom extract. J Allergy Clin Immunol 2552 2009;124:379-81. 2553 146. Hoffman DR, Jacobson RS. Allergens in Hymenoptera venom. XII. How much 2554 protein is in a sting? Ann Allergy 1984;52:276-8. 2555 147. Schumacher MJ, Tveten MS, Egen NB. Rate and quantity of delivery of venom 2556 from honeybee stings. J Allergy Clin Immunol 1994;93:831-5. 2557 148. Bernstein JA, Kagan SL, Bernstein DI, Bernstein IL. Rapid venom immunotherapy 2558 is safe for routine use in the treatment of patients with Hymenoptera anaphylaxis. Ann 2559 Allergy 1994;73:423-8. 2560 149. Birnbaum J, Charpin D, Vervloet D. Rapid Hymenoptera venom immunotherapy: 2561 comparative safety of three protocols. Clin Exp Allergy 1993;23:226-30. 2562 150. Birnbaum J, Ramadour M, Magnan A, Vervloet D. Hymenoptera ultra-rush venom 2563 immunotherapy (210 min): a safety study and risk factors. Clin Exp Allergy 2003;33:58-2564 64. 2565 151. Houliston L, Nolan R, Noble V, et al. Honeybee venom immunotherapy in children 2566 using a 50-mcg maintenance dose. J Allergy Clin Immunol 2011;127:98-9. 2567 152. Konstantinou GN, Manoussakis E, Douladiris N, et al. A 5-year venom 2568 immunotherapy protocol with 50 mcg maintenance dose: safety and efficacy in school 2569 children. Pediatr Allergy Immunol 2011;22:393-7. 2570 153. Rueff F, Wenderoth A, Przybilla B. Patients still reacting to a sting challenge while 2571 receiving conventional Hymenoptera venom immunotherapy are protected by increased 2572 venom doses. J Allergy Clin Immunol 2001;108:1027-32. 2573
154. Gadde J, Sobotka A, Valentine M, Lichtenstein L, Golden D. Intervals of six and 2574 eight weeks in maintenance venom immunotherapy. Ann Allergy 1985;54:348. 2575 155. Golden DBK, Kagey-Sobotka A, Valentine MD, Lichtenstein LM. Prolonged 2576 maintenance interval in Hymenoptera venom immunotherapy. J Allergy Clin Immunol 2577 1981;67:482-4. 2578 156. Cavalucci E, Ramondo S, Renzetti A, et al. Maintenance venom immunotherapy 2579 administered at a 3 month interval preserves safety and efficacy and improves 2580 adherence. J Investig Allergol Clin Immunol 2010;20:63-8. 2581 157. Goldberg A, Confino-Cohen R. Maintenance venom immunotherapy administered 2582 at 3-month intervals is both safe and efficacious. J Allergy Clin Immunol 2001;107:902-2583 6. 2584 158. Goldberg A, Confino-Cohen R. Effectiveness of maintenance bee venom 2585 immunotherapy administered at 6 month intervals. Ann Allergy Asthma Immunol 2586 2007;99:352-7. 2587 159. Arseneau A, Nesselroad TD, Dietrich JJ, et al. A 1-day imported fire ant rush 2588 immunotherapy schedule with and without premedication. Ann Allergy Asthma Immunol 2589 2013;111:562-6. 2590 160. Tankersley MS, Walker RL, Butler WK, Hagan LL, Napoli DC, Freeman TM. Safety 2591 and efficacy of an imported fire ant rush immunotherapy protocol with and without 2592 prophylactic treatment. J Allergy Clin Immunol 2002;109:556-62. 2593 161. Freeman TM, Hyghlander R, Ortiz A, Martin ME. Imported fire ant 2594 immunotherapy: effectiveness of whole body extracts. J Allergy Clin Immunol 2595 1992;90:210-5. 2596 162. Moffitt JE, Barker JR, Stafford CT. Management of imported fire ant allergy: 2597 results of a survey. Ann Allergy Asthma Immunol 1997;79:125-30. 2598 163. Steigelman DA, Freeman TM. Imported fire ant allergy: case presentation and 2599 review of incidence, prevalence, diagnosis and current treatment. Ann Allergy Asthma 2600 Immunol 2013;111:242-5. 2601 164. Lockey RF, Turkeltaub PC, Olive ES, Hubbard JM, Baird-Warren IA, Bukantz SC. 2602 The Hymenoptera venom study III: Safety of venom immunotherapy. J Allergy Clin 2603 Immunol 1990;86:775-80. 2604 165. Mosbech H, Muller U. Side effects of insect venom immunotherapy: results from 2605 an EAACI study. Allergy 2000;55:1005-10. 2606 166. Goldberg A, Confino-Cohen R. Rush venom immunotherapy in patients 2607 experiencing recurrent systemic reactions to conventional venom immunotherapy. Ann 2608 Allergy 2003;91:405-10. 2609 167. daSilva EN, Randall KL. Omailzumab mitigates anaphylaxis during ultra-rush 2610 honey bee venom immunotherapy in monoclonal mast cell activation syndrome. J 2611 Allergy Clin Immunol Prac 2013;1:687-8. 2612
168. Galera C, Soohun N, Zankar N, Caimmi S, Gallen C, Demoly P. Severe 2613 anaphylaxis to bee venom immunotherapy: Efficacy of pretreatment with omalizumab. J 2614 Investig Allergol Clin Immunol 2009;19:225-9. 2615 169. Kontou-Fili K. High omalizumab dose controls recurrent reactions to venom 2616 immunotherapy in indolent systemic mastocytosis. Allergy 2008;63:376-8. 2617 170. Brockow K, Kiehn M, Riethmuller C, Vieluf D, Berger J, Ring J. Efficacy of 2618 antihistamine pretreatment in the prevention of adverse reactions to Hymenoptera 2619 immunotherapy: A prospective, randomized, placebo-controlled trial. J Allergy Clin 2620 Immunol 1997;100:458-63. 2621 171. Muller U, Hari Y, Berchtold E. Premedication with antihistamines may enhance 2622 efficacy of specific allergen immunotherapy. J Allergy Clin Immunol 2001;107:81-6. 2623 172. Muller UR, Jutel M, Reimers A, et al. Clinical and immunologic effects of H1 2624 antihistamine preventive medication during honeybee venom immunotherapy. J Allergy 2625 Clin Immunol 2008;122:1001-7. 2626 173. Wohrl S, Gamper S, Hemmer W, Heinze G, Stingl G, Kinaciyan T. Premedication 2627 with montelukast reduces large local reactions of allergen immunotherapy. Int Arch 2628 Allergy Immunol 2007;144:137-42. 2629 174. Chabane MH, Leynadier MD, halpern GM, Dry J. Serum sickness with acquired 2630 precipitating antibodies during rush immunotherapy (2 cases). Ann Allergy 2631 1988;61:216-9. 2632 175. deBandt M, Atassi-Dumont M, Kahn M. Serum sickness after wasp venom 2633 immunotherapy; clinical and biological study. J Rheumatol 1997;24:1195-7. 2634 176. Lichtenstein LM, Golden DB. Postscript to bee stings: delayed "serum sickness". 2635 Hosp Pract 1983;18:36. 2636 177. Reisman RE. Unusual reactions to insect stings. Curr Opin Allergy Clin Immunol 2637 2005;5:355-8. 2638 178. Korosec P, Ziberna K, Silar M, et al. Immunological and clinical factors associated 2639 with adverse systemic reactions during the build-up phase of honey bee venom 2640 immunotherapy. Clin Exp Allergy 2015;45:1579-89. 2641 179. Brown SG, Wiese MD, vanEeden P, Stone SF, et a. Ultrarush versus semirush 2642 initiation of insect venom immunotherapy: A randomized controlled trial. J Allergy Clin 2643 Immunol 2012;130:162-8. 2644 180. Stoevesandt J, Hosp C, Kerstan A, Trautmann A. Hymenoptera venom 2645 immunotherapy while maintaining cardiovascular medication: safe and effective. Ann 2646 Allergy Asthma Immunol 2015;114:411-6. 2647 181. Nassiri M, Babina M, Dolle S, Edenharter G, Rueff F, Worm M. Ramipril and 2648 metoprolol intake aggravate human and murine anaphylaxis: Evidence for direct mast 2649 cell priming. J Allergy Clin Immunol 2015;135:491-9. 2650
182. Muller U, Haeberli G. Use of beta-blockers during immunotherapy for 2651 Hymenoptera venom allergy. J Allergy Clin Immunol 2005;115:606-10. 2652 183. Rueff F, Vos B, Oude-Elberink J, et al. Predictors of clinical effectiveness of 2653 Hymenoptera venom immunotherapy. Clin Exp Allergy 2014;44:736-46. 2654 184. Brown SG. Clinical features and severity grading of anaphylaxis. J Allergy Clin 2655 Immunol 2004;114:371-6. 2656 185. Lee S, HEss EP, Nestler DM, et al. Antihypertensive medication use is associated 2657 with increased organ system involvement and hospitalization in emergency department 2658 patients with anaphylaxis. J Allergy Clin Immunol 2013;131:1103-8. 2659 186. Ober AI, MacLean JA, Hannaway PJ. Life-threatening anaphylaxis to venom 2660 immunotherapy in a patient taking an angiotensin-converting enzyme inhibitor. J Allergy 2661 Clin Immunol 2003;112:1008-9. 2662 187. Tunon-de-Lara JM, Villanueva P, Marcos M, Taytard A. ACE inhibitors and 2663 anaphylactoid reactions during venom immunotherapy. Lancet 1992;340:908. 2664 188. Schwartz HJ, Golden DBK, Lockey RF. Venom immunotherapy in the 2665 Hymenoptera-allergic pregnant patient. J Allergy Clin Immunol 1990;85:709-. 2666 189. Graft DF, Golden D, Reisman R, Valentine M, Yunginger J. The discontinuation of 2667 Hymenoptera venom immunotherapy. Report from the Committee on Insects. J Allergy 2668 Clin Immunol 1998;101:573-5. 2669 190. Lerch E, Muller U. Long-term protection after stopping venom immunotherapy. J 2670 Allergy Clin Immunol 1998;101:606-12. 2671 191. Muller UR, Ring J. When can immunotherapy for insect allergy be stopped? J 2672 Allergy Clin Immunol Prac 2015;3:324-8. 2673 192. Forester JP, Johnson TL, Arora R, Quinn JM. Systemic reaction rates to field 2674 stings among imported fire ant sensitive patients receiving >3 years of immunotherapy 2675 versus <3 years of immunotherapy. Allergy Asthma Proc 2007;28:485-8. 2676 193. Golden DBK, Kwiterovich KA, Kagey-Sobotka A, Valentine MD, Lichtenstein LM. 2677 Discontinuing venom immunotherapy: Outcome after five years. J Allergy Clin Immunol 2678 1996;97:579-87. 2679 194. Golden DBK, Kwiterovich KA, Addison BA, Kagey-Sobotka A, Lichtenstein LM. 2680 Discontinuing venom immunotherapy: Extended observations. J Allergy Clin Immunol 2681 1998;101:298-305. 2682 195. Hafner T, Dubuske L, Kosnik M. Long-term efficacy of venom immunotherapy. 2683 Ann Allergy Asthma Immunol 2008;100:162-5. 2684 196. Haugaard L, Norregaard OFH, Dahl R. In-hospital sting challenge in insect 2685 venom-allergic patients after stopping venom immunotherapy. J Allergy Clin Immunol 2686 1991;87:699-702. 2687
197. Keating MU, Kagey-Sobotka A, Hamilton RG, Yunginger JW. Clinical and 2688 immunologic follow-up of patients who stop venom immunotherapy. J Allergy Clin 2689 Immunol 1991;88:339-48. 2690 198. Muller U, Berchtold E, Helbling A. Honeybee venom allergy: results of a sting 2691 challenge 1 year after stopping venom immunotherapy in 86 patients. J Allergy Clin 2692 Immunol 1991;87:702-9. 2693 199. Reisman RE. Venom immunotherapy: When is it reasonable to stop. J Allergy Clin 2694 Immunol 1991;87:618-20. 2695 200. Reisman RE. Duration of venom immunotherapy: Relationship to the severity of 2696 symptoms of initial insect sting anaphylaxis. J Allergy Clin Immunol 1993;92:831-6. 2697 201. Stritzke AI, Eng PA. Age-dependent sting recurrence and outcome in 2698 immunotherapy-treated children with anaphylaxis to Hymenoptera venom. Clin Exp 2699 Allergy 2013;43:950-5. 2700 202. Muller U, Helbling A, Berchtold E. Immunotherapy with honeybee venom and 2701 yellow jacket venom is different regarding efficacy and safety. J Allergy Clin Immunol 2702 1992;89:529-35. 2703 203. Light WC. Insect sting fatality 9 years after venom treatment. J Allergy Clin 2704 Immunol 2001;107:925. 2705 204. Nguyen SA, Napoli DC. Natural history of large local and generalized cutaneous 2706 reactions to imported fire ant stings in children. Ann Allergy Asthma Immunol 2707 2005;94:387-90. 2708 205. Stafford CT. Hypersensitivity to fire ant venom. Ann Allergy Asthma Immunol 2709 1996;77:87-95. 2710 206. Hoffman DR, Jacobson RS, Schmidt M, Smith AM. Allergens in Hymenoptera 2711 venoms. XXIII. Venom content of imported fire ant whole body extracts. Ann Allergy 2712 1991;66:29-31. 2713 207. Butcher B, deShazo R, Ortiz A, Reed M. RAST-inhibition studies of the imported 2714 fire ant, Solenopsis invicta, with whole body extracts and venom preparations. J Allergy 2715 Clin Immunol 1988;81:1096-100. 2716 208. Rhoades RB. Skin test reactivity to imported fire ant whole body extract - 2717 comparison of three commercial sources. J Allergy Clin Immunol 1993;91:282 2718 (abstract). 2719 209. Strom GB, Boswell MD, Jacobs RL. In vivo and in vitro comparison of fire ant 2720 venom and fire ant whole body extract. J Allergy Clin Immunol 1983;72:46-53. 2721 210. Letz LG, Quinn JM. Frequency of imported fire ant stings in patients receiving 2722 immunotherapy. Ann Allergy Asthma Immunol 2009;102:303-7. 2723 211. Patridge ME, Blackwood W, Hamiton RG, Ford J, Young P, Ownby DR. Prevalence 2724 of allergic sensitiazation to imported fireants in children living in endemic region of 2725 southeastern United States. Ann Allergy Asthma Immunol 2008;100:54-8. 2726
212. LaShell MS, Calabria CW, Quinn JM. Imported fire ant field reaction and 2727 immunotherapy safety characteristics: the IFACS study. J Allergy Clin Immunol 2728 2010;125:1294-9. 2729 213. Grier TJ, LeFevre DM, Duncan EA, Esch RE, Coyne TC. Allergen stabilities and 2730 compatibilities in mixtures of high protease fungal and insect extracts. Ann Allergy 2731 Asthma Immunol 2012;108:439-47. 2732 214. Rans TS, Hrabak TM, Whisman BA, et al. Compatibility of imported fire ant whole 2733 body extract with cat, ragweed, Dermatophagoides pteronyssinus, and timothy grass 2734 allergens. Ann Allergy Asthma Immunol 2009;102:57-61. 2735 215. Haymore BR, McCoy RL, Nelson MR. Imported fire ant immunotherapy 2736 prescribing patterns in a large health care system during a 17-year period. Ann Allergy 2737 Asthma Immunol 2009;102:422-5. 2738 2739 2740 2741 2742
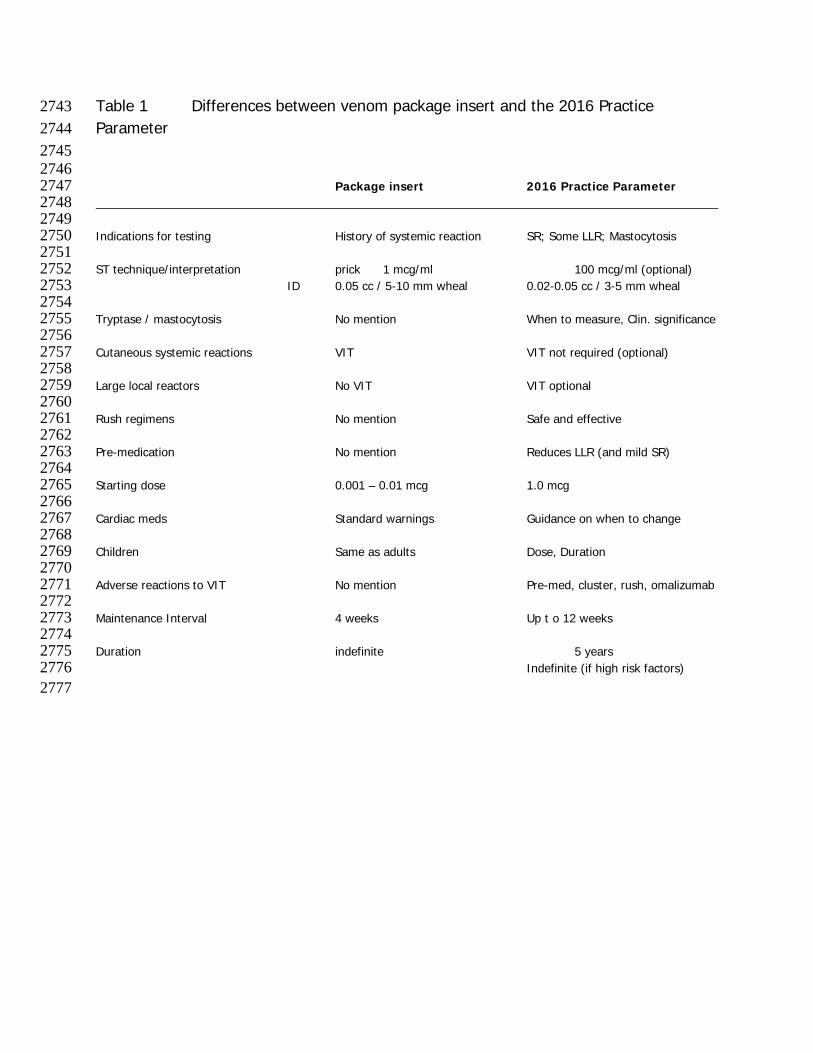
Table 1 Differences between venom package insert and the 2016 Practice 2743 Parameter 2744 2745 2746 Package insert 2016 Practice Parameter 2747 2748 2749 Indications for testing History of systemic reaction SR; Some LLR; Mastocytosis 2750 2751 ST technique/interpretation prick 1 mcg/ml 100 mcg/ml (optional) 2752
ID 0.05 cc / 5-10 mm wheal 0.02-0.05 cc / 3-5 mm wheal 2753 2754 Tryptase / mastocytosis No mention When to measure, Clin. significance 2755 2756 Cutaneous systemic reactions VIT VIT not required (optional) 2757 2758 Large local reactors No VIT VIT optional 2759 2760 Rush regimens No mention Safe and effective 2761 2762 Pre-medication No mention Reduces LLR (and mild SR) 2763 2764 Starting dose 0.001 – 0.01 mcg 1.0 mcg 2765 2766 Cardiac meds Standard warnings Guidance on when to change 2767 2768 Children Same as adults Dose, Duration 2769 2770 Adverse reactions to VIT No mention Pre-med, cluster, rush, omalizumab 2771 2772 Maintenance Interval 4 weeks Up t o 12 weeks 2773 2774 Duration indefinite 5 years 2775 Indefinite (if high risk factors) 2776 2777
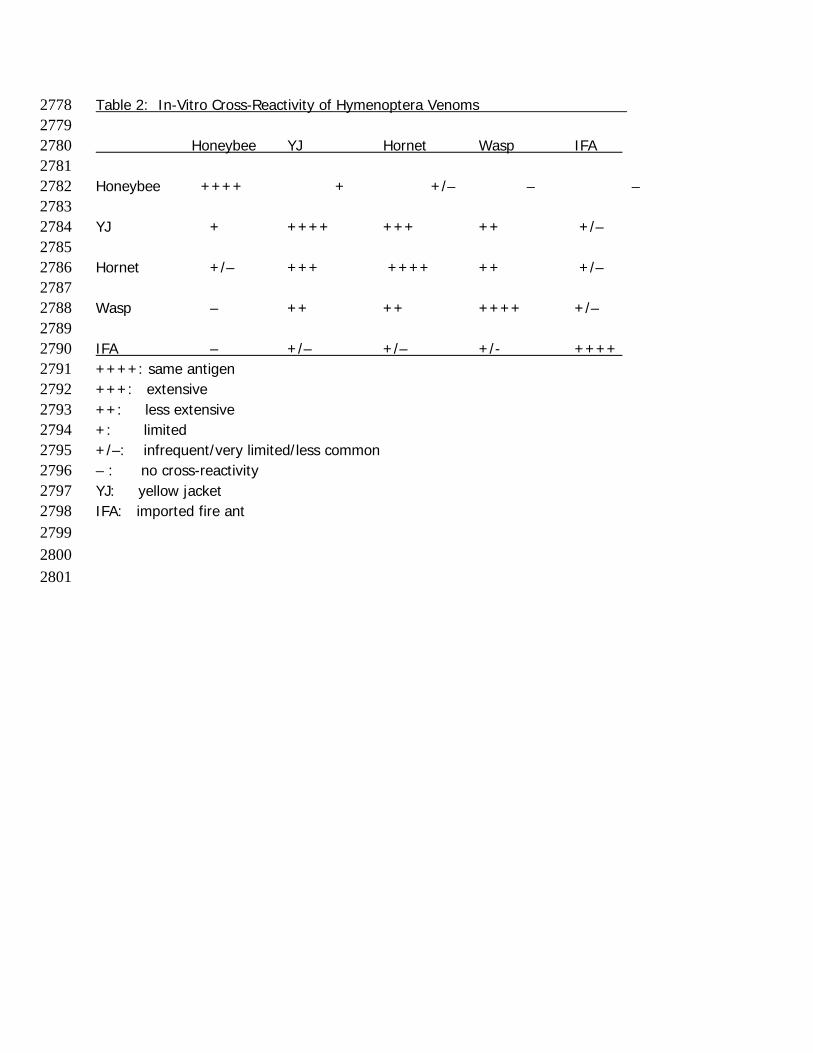
Table 2: In-Vitro Cross-Reactivity of Hymenoptera Venoms 2778 2779 Honeybee YJ Hornet Wasp IFA 2780 2781 Honeybee ++++ + +/– – – 2782 2783 YJ + ++++ +++ ++ +/– 2784 2785 Hornet +/– +++ ++++ ++ +/– 2786 2787 Wasp – ++ ++ ++++ +/– 2788 2789 IFA – +/– +/– +/- ++++ 2790 ++++: same antigen 2791 +++: extensive 2792 ++: less extensive 2793 +: limited 2794 +/–: infrequent/very limited/less common 2795 – : no cross-reactivity 2796 YJ: yellow jacket 2797 IFA: imported fire ant 2798 2799 2800 2801
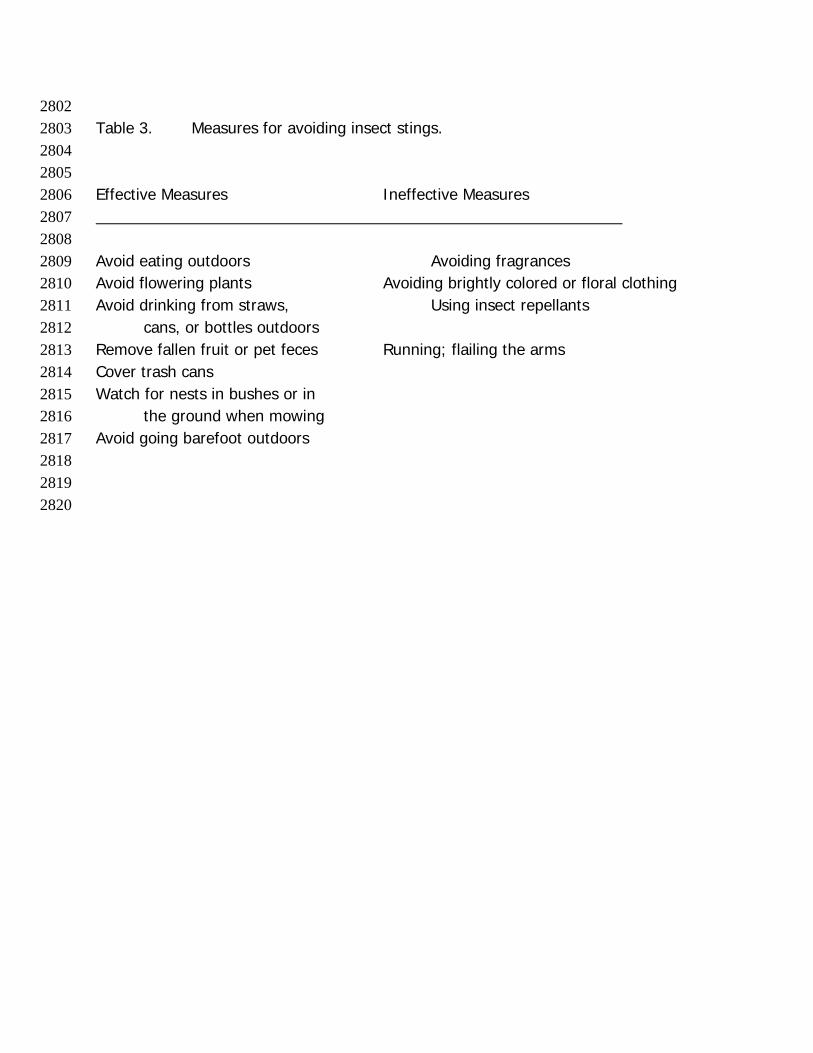
2802 Table 3. Measures for avoiding insect stings. 2803 2804 2805 Effective Measures Ineffective Measures 2806 2807 2808 Avoid eating outdoors Avoiding fragrances 2809 Avoid flowering plants Avoiding brightly colored or floral clothing 2810 Avoid drinking from straws, Using insect repellants 2811 cans, or bottles outdoors 2812 Remove fallen fruit or pet feces Running; flailing the arms 2813 Cover trash cans 2814 Watch for nests in bushes or in 2815
the ground when mowing 2816 Avoid going barefoot outdoors 2817 2818 2819 2820
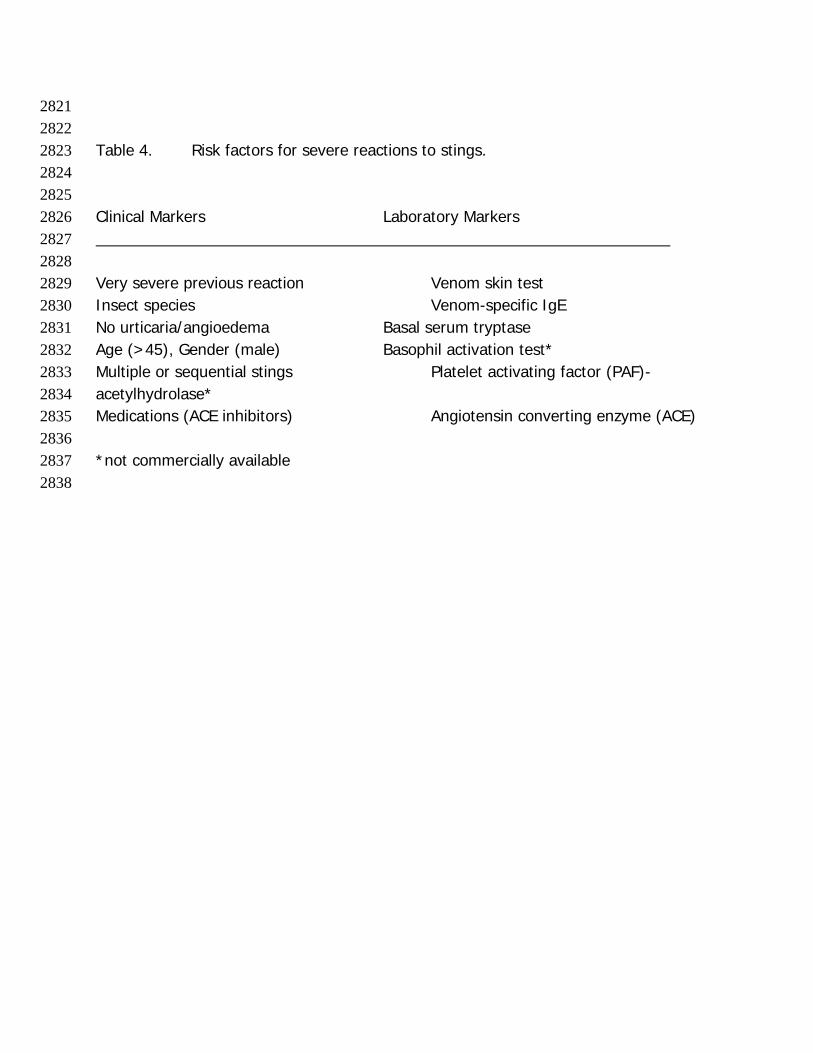
2821 2822 Table 4. Risk factors for severe reactions to stings. 2823 2824 2825 Clinical Markers Laboratory Markers 2826 2827 2828 Very severe previous reaction Venom skin test 2829 Insect species Venom-specific IgE 2830 No urticaria/angioedema Basal serum tryptase 2831 Age (>45), Gender (male) Basophil activation test* 2832 Multiple or sequential stings Platelet activating factor (PAF)-2833 acetylhydrolase* 2834 Medications (ACE inhibitors) Angiotensin converting enzyme (ACE) 2835 2836 *not commercially available 2837 2838
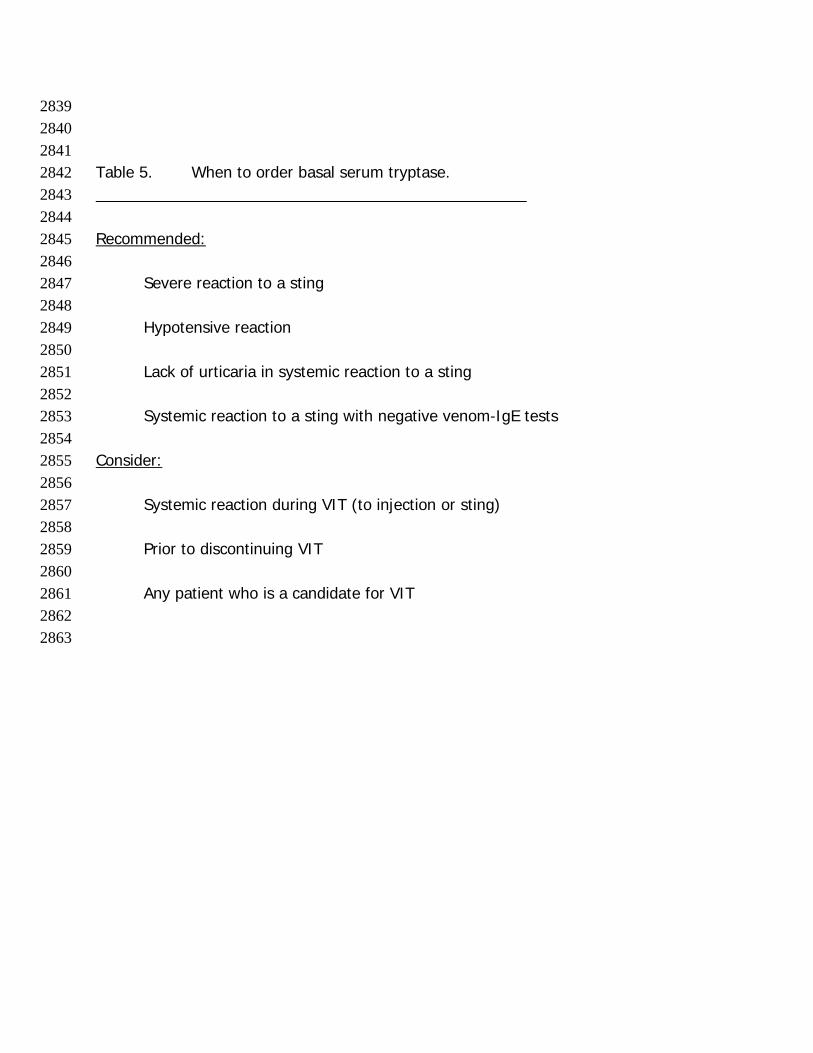
2839 2840 2841 Table 5. When to order basal serum tryptase. 2842 2843 2844 Recommended: 2845 2846
Severe reaction to a sting 2847 2848 Hypotensive reaction 2849 2850 Lack of urticaria in systemic reaction to a sting 2851 2852 Systemic reaction to a sting with negative venom-IgE tests 2853
2854 Consider: 2855 2856
Systemic reaction during VIT (to injection or sting) 2857 2858 Prior to discontinuing VIT 2859 2860 Any patient who is a candidate for VIT 2861
2862 2863
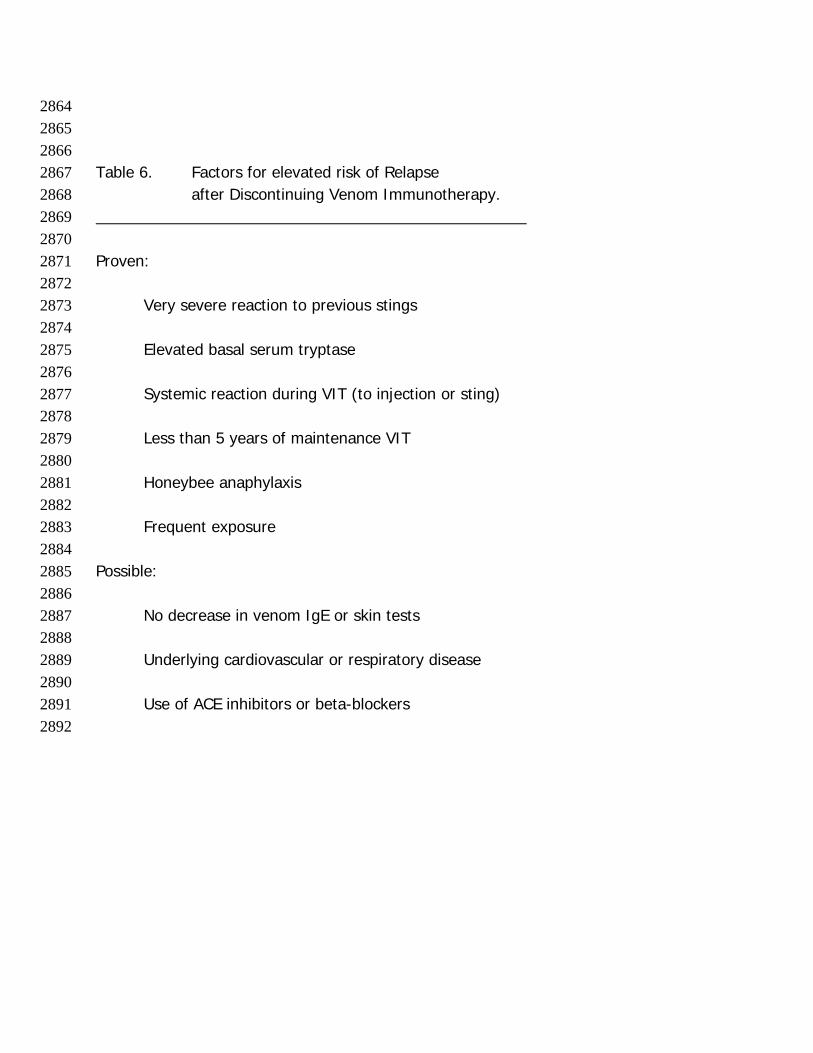
2864 2865 2866 Table 6. Factors for elevated risk of Relapse 2867
after Discontinuing Venom Immunotherapy. 2868 2869 2870 Proven: 2871 2872
Very severe reaction to previous stings 2873 2874 Elevated basal serum tryptase 2875 2876 Systemic reaction during VIT (to injection or sting) 2877 2878 Less than 5 years of maintenance VIT 2879 2880 Honeybee anaphylaxis 2881 2882 Frequent exposure 2883
2884 Possible: 2885 2886 No decrease in venom IgE or skin tests 2887 2888 Underlying cardiovascular or respiratory disease 2889 2890 Use of ACE inhibitors or beta-blockers 2891 2892
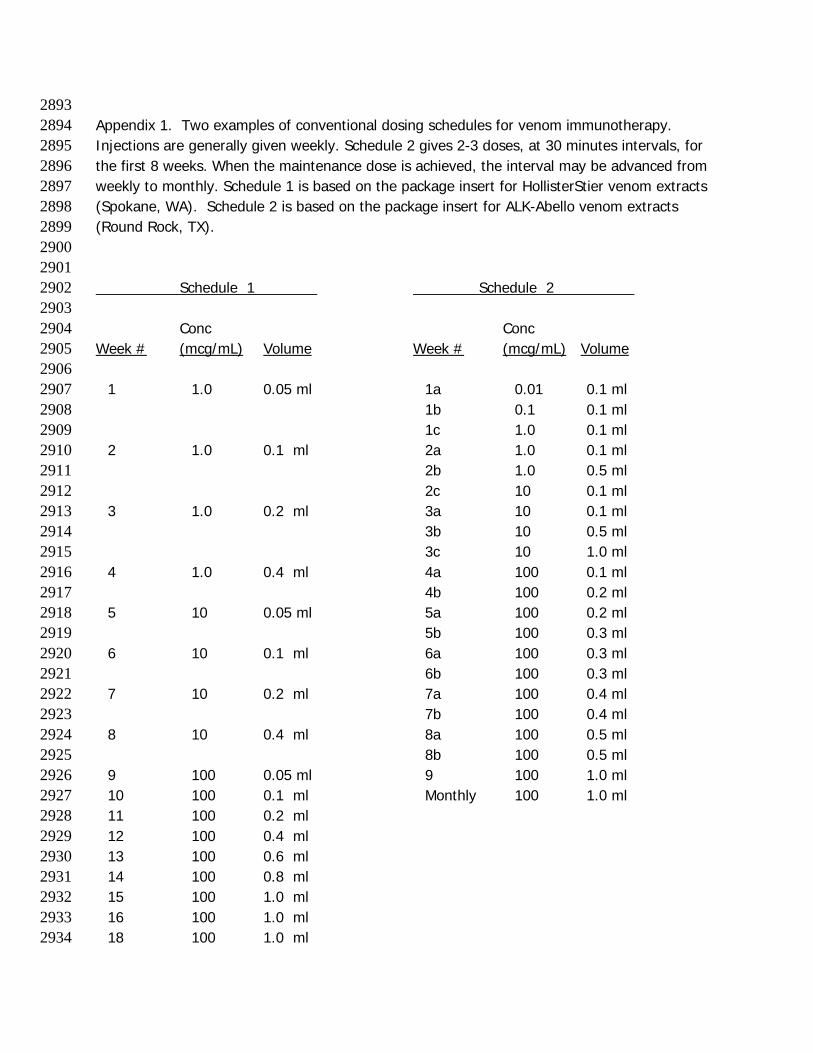
2893 Appendix 1. Two examples of conventional dosing schedules for venom immunotherapy. 2894 Injections are generally given weekly. Schedule 2 gives 2-3 doses, at 30 minutes intervals, for 2895 the first 8 weeks. When the maintenance dose is achieved, the interval may be advanced from 2896 weekly to monthly. Schedule 1 is based on the package insert for HollisterStier venom extracts 2897 (Spokane, WA). Schedule 2 is based on the package insert for ALK-Abello venom extracts 2898 (Round Rock, TX). 2899 2900 2901 Schedule 1 Schedule 2 2902 2903 Conc Conc 2904 Week # (mcg/mL) Volume Week # (mcg/mL) Volume 2905 2906
1 1.0 0.05 ml 1a 0.01 0.1 ml 2907 1b 0.1 0.1 ml 2908 1c 1.0 0.1 ml 2909 2 1.0 0.1 ml 2a 1.0 0.1 ml 2910 2b 1.0 0.5 ml 2911 2c 10 0.1 ml 2912 3 1.0 0.2 ml 3a 10 0.1 ml 2913 3b 10 0.5 ml 2914 3c 10 1.0 ml 2915 4 1.0 0.4 ml 4a 100 0.1 ml 2916 4b 100 0.2 ml 2917 5 10 0.05 ml 5a 100 0.2 ml 2918 5b 100 0.3 ml 2919 6 10 0.1 ml 6a 100 0.3 ml 2920 6b 100 0.3 ml 2921 7 10 0.2 ml 7a 100 0.4 ml 2922 7b 100 0.4 ml 2923 8 10 0.4 ml 8a 100 0.5 ml 2924 8b 100 0.5 ml 2925 9 100 0.05 ml 9 100 1.0 ml 2926 10 100 0.1 ml Monthly 100 1.0 ml 2927 11 100 0.2 ml 2928 12 100 0.4 ml 2929 13 100 0.6 ml 2930 14 100 0.8 ml 2931 15 100 1.0 ml 2932 16 100 1.0 ml 2933 18 100 1.0 ml 2934
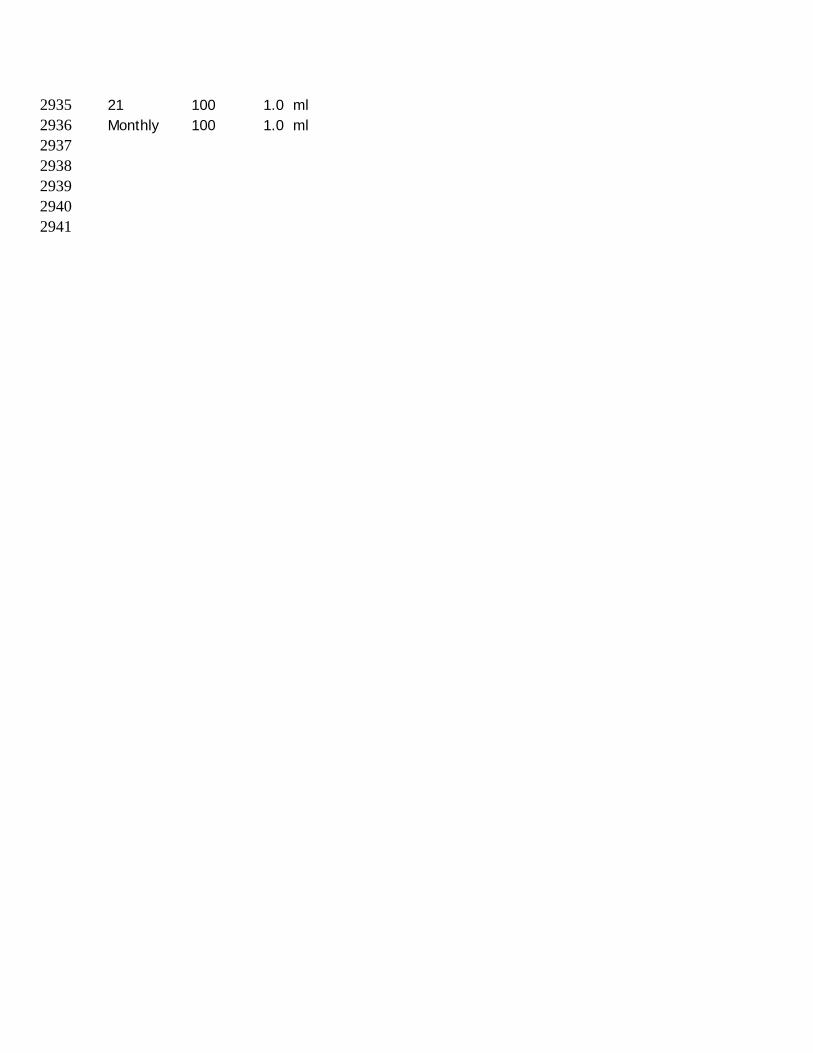
21 100 1.0 ml 2935 Monthly 100 1.0 ml 2936 2937 2938 2939
2940 2941
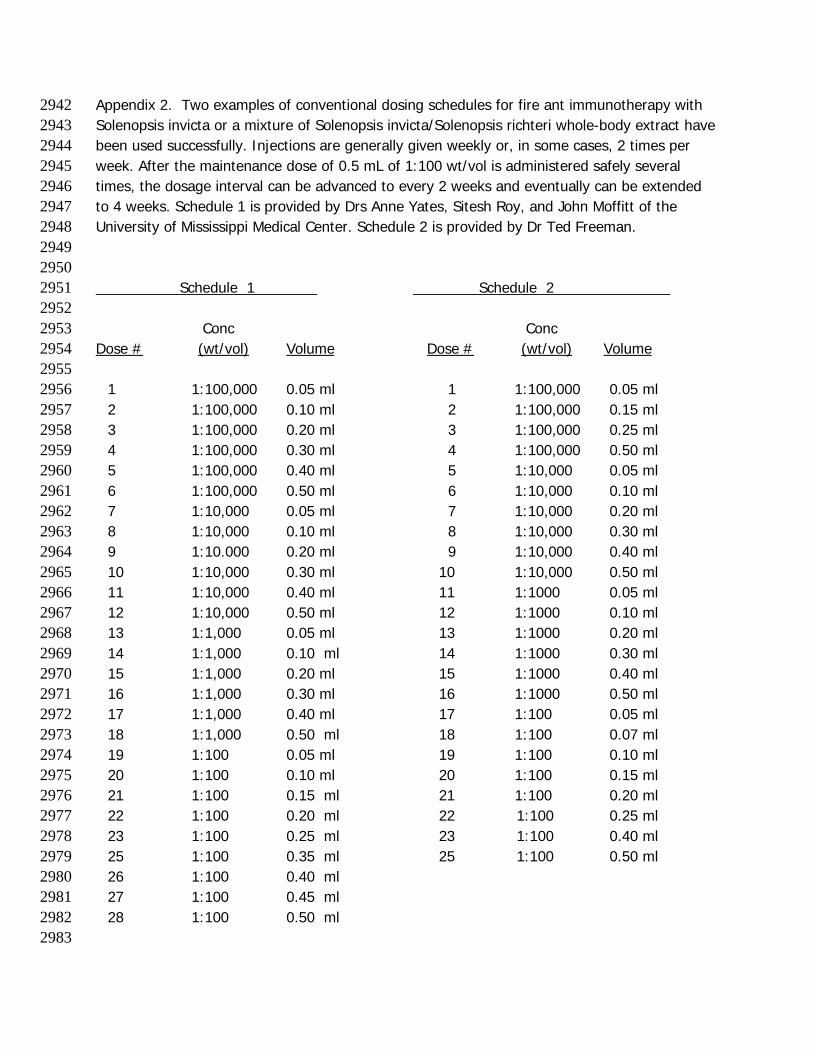
Appendix 2. Two examples of conventional dosing schedules for fire ant immunotherapy with 2942 Solenopsis invicta or a mixture of Solenopsis invicta/Solenopsis richteri whole-body extract have 2943 been used successfully. Injections are generally given weekly or, in some cases, 2 times per 2944 week. After the maintenance dose of 0.5 mL of 1:100 wt/vol is administered safely several 2945 times, the dosage interval can be advanced to every 2 weeks and eventually can be extended 2946 to 4 weeks. Schedule 1 is provided by Drs Anne Yates, Sitesh Roy, and John Moffitt of the 2947 University of Mississippi Medical Center. Schedule 2 is provided by Dr Ted Freeman. 2948 2949 2950 Schedule 1 Schedule 2 2951 2952 Conc Conc 2953 Dose # (wt/vol) Volume Dose # (wt/vol) Volume 2954 2955
1 1:100,000 0.05 ml 1 1:100,000 0.05 ml 2956 2 1:100,000 0.10 ml 2 1:100,000 0.15 ml 2957 3 1:100,000 0.20 ml 3 1:100,000 0.25 ml 2958 4 1:100,000 0.30 ml 4 1:100,000 0.50 ml 2959 5 1:100,000 0.40 ml 5 1:10,000 0.05 ml 2960 6 1:100,000 0.50 ml 6 1:10,000 0.10 ml 2961 7 1:10,000 0.05 ml 7 1:10,000 0.20 ml 2962 8 1:10,000 0.10 ml 8 1:10,000 0.30 ml 2963 9 1:10.000 0.20 ml 9 1:10,000 0.40 ml 2964 10 1:10,000 0.30 ml 10 1:10,000 0.50 ml 2965 11 1:10,000 0.40 ml 11 1:1000 0.05 ml 2966 12 1:10,000 0.50 ml 12 1:1000 0.10 ml 2967 13 1:1,000 0.05 ml 13 1:1000 0.20 ml 2968 14 1:1,000 0.10 ml 14 1:1000 0.30 ml 2969 15 1:1,000 0.20 ml 15 1:1000 0.40 ml 2970 16 1:1,000 0.30 ml 16 1:1000 0.50 ml 2971 17 1:1,000 0.40 ml 17 1:100 0.05 ml 2972 18 1:1,000 0.50 ml 18 1:100 0.07 ml 2973 19 1:100 0.05 ml 19 1:100 0.10 ml 2974 20 1:100 0.10 ml 20 1:100 0.15 ml 2975 21 1:100 0.15 ml 21 1:100 0.20 ml 2976 22 1:100 0.20 ml 22 1:100 0.25 ml 2977 23 1:100 0.25 ml 23 1:100 0.40 ml 2978 25 1:100 0.35 ml 25 1:100 0.50 ml 2979 26 1:100 0.40 ml 2980 27 1:100 0.45 ml 2981 28 1:100 0.50 ml 2982
2983
2984 2985
2986
Appendix 3. Examples of Rush and Ultra-rush Regimens 2987 2988 2989 2990 2991 2992
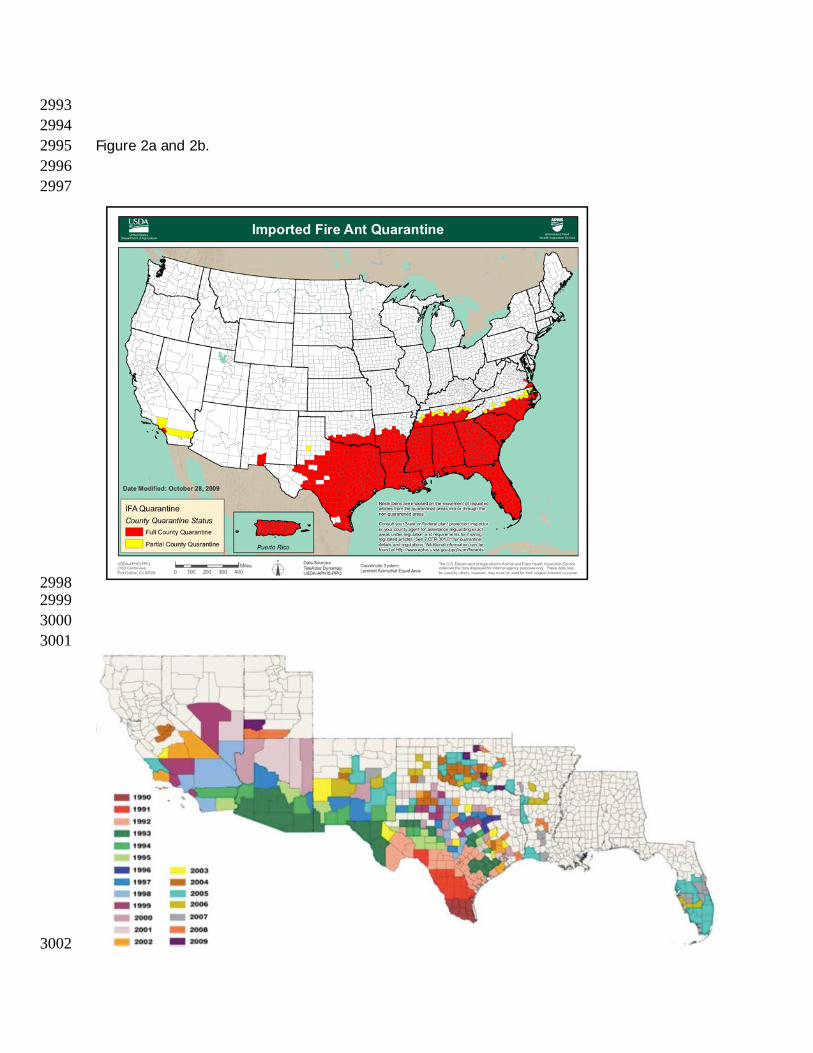
2993 2994 Figure 2a and 2b. 2995 2996 2997
2998 2999 3000 3001
3002
3003 3004 3005 3006 3007 Figure Legend. 3008 3009 Figure 2. Distribution of imported fire ants (Fig. 2a) and Africanized honeybees (Fig 3010 2b) in the United States, 2009 (USDA). 3011