STEMI (Andi Fauziah a, C 111 07 070)
31
STEMI EXTENSIVE ANTERIOR ONSET 4 HOURS KILLIP I By: Andi Fauziah Armayani (C111 07 070) Supervisor: dr. Khalid Saleh, Sp.PD- KKV, FINASIM CARDIOLOGY DEPARTMENT FACULTY OF MEDICINE HASANUDDIN UNIVERSITY WAHIDIN SUDIROHUSODO HOSPITAL 2013
-
Upload
jefrizalzain -
Category
Documents
-
view
10 -
download
1
Transcript of STEMI (Andi Fauziah a, C 111 07 070)

STEMI EXTENSIVE ANTERIOR ONSET 4 HOURS KILLIP I
By:
Andi Fauziah Armayani
(C111 07 070)
Supervisor:
dr. Khalid Saleh, Sp.PD- KKV, FINASIM
CARDIOLOGY DEPARTMENT
FACULTY OF MEDICINE HASANUDDIN UNIVERSITY
WAHIDIN SUDIROHUSODO HOSPITAL
2013

PATIENT’S IDENTITY
Name : Mr. KGender : Male Age : June 16, 1986Registration no : 601336Date of Admission : March 28, 2013

HISTORY TAKING
Chief Complain :• Chest Pain
Present illness history:• Chest pain was felt since 4 hours
before admitted to the hospital. This pain was felt continue and described as a squeezing sensation. Pain was felt on the left side of chest and radiated to the neck, shoulder, his left arm and the back.

• Cold Sweat (+) while chest pain occurred• Palpitation (+)• Nausea (+), vomiting (-) , epigastric pain (-)• Short of breathness (-), history of short of
breathness (-)• Cough (-) ,mucus (-)• Dizziness (-), headache (-) .• Urination = normal• Defecation = normal

PREVIOUS ILLNESS HISTORY
History of hypertension (-) History of Diabetes mellitus (-) History of heart disease (-) History of smoking (+) 2 packs/day since 10 years
ago

RISK FACTOR
Modified Risk Factor
• Smoking 2 packs/day
Non-modified risk factor:• Gender : man

PHYSICAL EXAMINATION
• moderate illness/well-nourished/conscious
General appearan
ce • BP : 120/80 mmHg• P : 72 x/min• R : 20 x/min• T :36.8oC
Vital Sign
• Anemi (-) , icterus (-)Head
• JVP R - 2 cm H20Neck

CONT…• I : symmetric R=L, normochest
• P : mass (-), tenderness (-), VF R=L
• P : sonor• A : breath
sound :bronchovesicular additional sound : ronchi -/- , wh -/-
Chest Examinati
on
• I : ictus cordis unseen• P : ictus cordis
unpalpable• P : dull, left heart border
left midclavicular line ICS V.
• A : HS I/II pure regular, murmur(-)
Cor

CONT…
Abdomen :• Inspection : flat and correspond with
breathing movement• Auscultation : peristaltic sound (+) ,
normal• Palpation : liver and spleen unpalpable• Percussion: tympani, ascites (-)
Extremitas :• edem -/-

ELECTROCARDIOGRAPHY FINDINGS
ECG Interpretation Sinus Rhythm Heart Rate :60
x/IP Wave : 0.06 ’PR interval : 0.12
’QRS
complex :0.08 ’Axis :
normoaxis ST-elevated : V1-
V6, L1 & aVL

CONCLUSIONSinus Rhythm, heart rate :60 x/minute, normoaxis,
ST elevated at V1, V2, V3, V4, V5, V6 + L1 and AVL
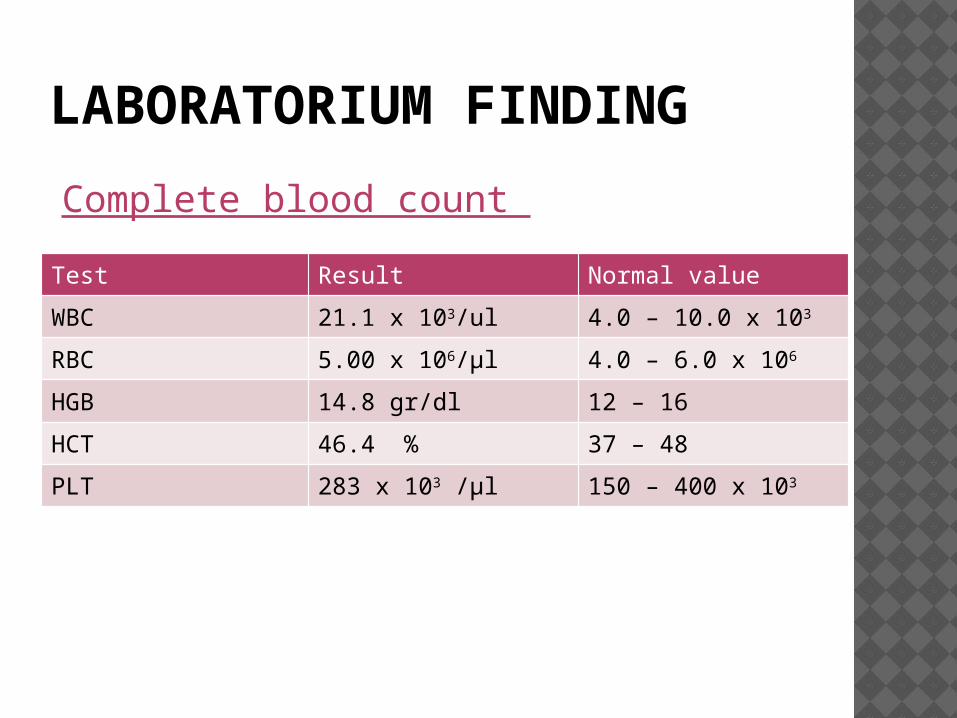
LABORATORIUM FINDING
Test Result Normal value
WBC 21.1 x 103/ul 4.0 – 10.0 x 103
RBC 5.00 x 106/µl 4.0 – 6.0 x 106
HGB 14.8 gr/dl 12 – 16
HCT 46.4 % 37 – 48
PLT 283 x 103 /µl 150 – 400 x 103
Complete blood count

Blood ChemistryTest Result Normal value
GDS 112 mg/dl <140
Ureum 25 mg/dl 10 – 50
Creatinine 1.0 mgr/dl < 1.3
SGOT 24 u/l <38
SGPT 15 u/l <41
Total CholHDL CholLDL Chol
129 mg/dl 37 mg/dl54 mg/dl
<200> 55 < 130
TG 91 mg/dl <200
Test Result Normal value
CK 419 U/L <167
CK-MB 16 U/L <25
Troponin-T >2.0 Negative
Cardiac Enzymes

Electrolyte
Test Result Normal value
Na 145 mmol/l 136-145
K 3.9 mmol/l 3.5-5.1
Cl 109 mmol/l 97-111

DIAGNOSIS
ST Elevation Myocardial Infarction
(STEMI)Extensive Anterior 4
Hours KILLIP I

MANAGEMENT O2 2-4 lpm IVFD NaCl 0,9% 500cc/12h Anti platelet Aspilet 80mg 1x1 Anti platelet Clopidogrel 1 x 75mg Anti Thrombolytic Streptokinase 1.5 million IU
in 60 minutes Anti coagulant Fondaparinux Sodium 2.5
mg/24 h/ S ACE Inhibitor Captopril 12.5 mg ½-0- ½ Statin simvastatin 20 mg 0-0-1 Lactulosa Laxadyn syr Benzodiazepine Alprazolam 0.5 mg 0-0-1

PLANNING Echocardiography Angiography

ST ELEVATION MYOCARDIAL INFARCTION

Occurs when coronary blood flow decreases abruptly after a thrombotic occlusion of a coronary artery previously affected by atherosclerosis.
In most cases, infarction occurs when an atherosclerotic plaque fissures, ruptures, or ulcerates.
PATHOPHYSIOLOGY

ACS describe a group of conditions resulting from acute myocardial
ischemia (insufficient blood flow to heart muscle) ranging from
unstable angina to myocardial infarction.
CLASSIFICATION

RISK FACTOR
Modifiable
• Smoking• Hypertension• Obesity• Diabetes
Mellitus• Dyslipidemia• Low HDL < 40• Elevated LDL /
TG
Non-modifiable
• Gender and age:• male after
age 45 y.o• woman after
age 55 y.o
• Family History in first degree relative > 55 y.o for male/ 65 y.o for woman

WHO DIAGNOSTIC CRITERIA
Clinical history of ischaemic type chest pain lasting >20 minutes
Changes in serial ECG tracings
Rise of serum cardiac biomarkers such as creatinine kinase-MB fraction and troponin-T

CLINICAL FEATURES
Substernal chest pain / chest discomfort radiated to the left arm, shoulder, neck, jaw. Penetrated to the back.
The chest discomfort may also be described as a dull pain ,‘pressure’, ‘squeezing’ or ‘crushing sensation’ or burning sensation
Duration more than 20 minutes. more intense and persistent.
Not fully relieved by rest or nitroglycerine
Often accompanied by systemic symptoms: nausea, vomiting, SOB, palpitation, fatigue, cold sweat, light headness

ECG IN AMI
• Non Specific ST-Elevation• T taller and wider
Hyperacute Phase
• Specific ST-Elevation• T inverted• Q – Phatologic
Complete Evolution
• Q- Phatologic• ST segmen isoelectric• T normal or inverted
Old Infarct
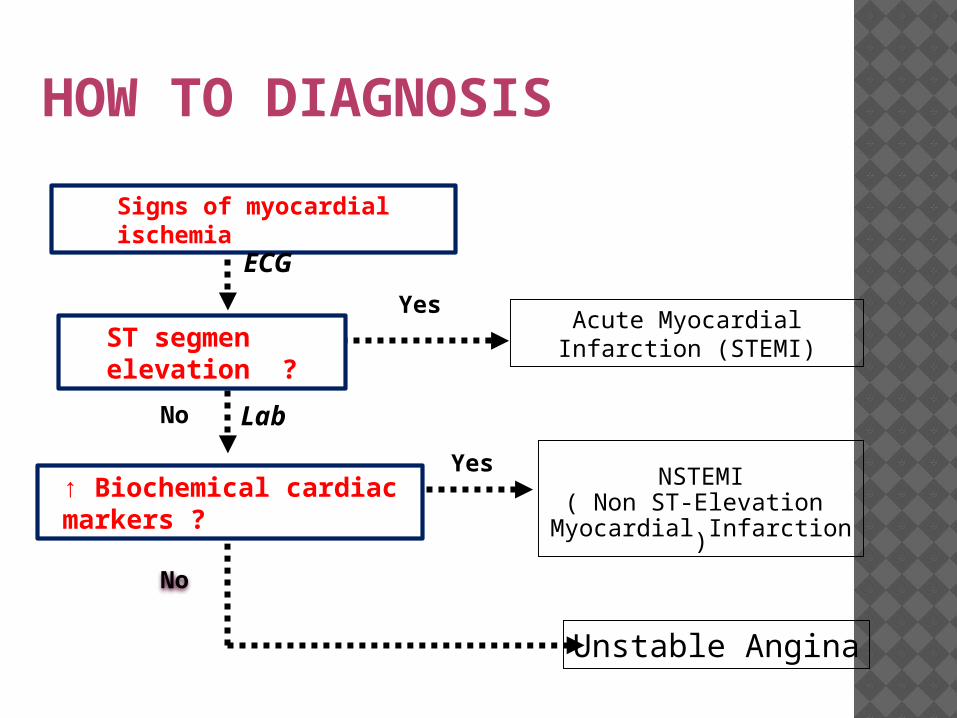
HOW TO DIAGNOSIS
No
Yes
Yes
No
Acute Myocardial Infarction (STEMI)
NSTEMI( Non ST-Elevation
Myocardial Infarction )
Unstable Angina
Signs of myocardial ischemia
↑ Biochemical cardiac markers ?
ECG
Lab
ST segmen elevation ?
MANAGEMENT
Fixing the chest pain and fearness• Bed rest• Heart Diet • O2 • Nitrat sublingual/oral/IV• Antiplatelet : aspirin and clopidogrel• Morfin/petidine• Diazepam

Stabilizing the hemodynamic ( blood pressure and pheripheral pulse controlβ-blockerCalcium chanel blocker (CCB)ACE-InhibitorReperfusion of the myocard

TIMI PROGNOSIS IN STEMI
Risk Factor Score
Age > 65 years old 2
Age > 75 years old 3
History of angina/hypertension/D
M1/1/1
Systolic BP <100 3
Heart rate > 100 2
Killip II-IV 2
Weight > 67kg 1
Anterior MI or LBBB 1
Delay treatment >4hours
1

Total Score Risk of Death in 30 days
0 0.8%1 1.6%2 2.2%3 4.4%4 7.3%5 12.4%6 16.1%7 23.4%8 26.8%
9-16 35.9%

PROGNOSIS KILLIP CLASSIFICATION
Class Description Mortality Rate (%)
I no clinical signs of heart failure
6
II rales or crackles in the lungs, an S3, and elevated jugular venous pressure
17
III acute pulmonary edema 30 - 40
IV cardiogenic shock or hypotension (systolic BP < 90 mmHg), and evidence of peripheral vasoconstriction
60 – 80

Thank you