STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS V Report
41
STATUS OF THE ANTIMALARIA CAMPAIGN IN THE AMERICAS V Report PAN AMERICAN SANITARY BUREAU Regional Office of the World Health Organization Washington, D. C.
Transcript of STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS V Report

STATUS OF THE ANTIMALARIA CAMPAIGN
IN THE AMERICAS
V Report
PAN AMERICAN SANITARY BUREAU
Regional Office of the
World Health Organization
Washington, D. C.

STATUS OF THE ANTIMALARIA CAMPAIGN
IN THE AMERICAS
V Report
DR. CARLOS A. ALVARADO
WHO/PASB Regional lAfalaria Consultant
Scientific PublicationsNo. 27
PAN AMERICAN SANITARY BUREAU
Regional Office of theWorld Health Organization
1501 New Hampshire Avenue, N.W.
Washington 6, D. C.. U.S.A.
December, 1956

¡

TABLE OF CONTENTS
PROGRESS OF ANTIMALARIA WORK IN THE CONTINENT
Plage
Introduction ............................ ............................................. 1
Status and organization of National Malaria Services ...................................... 2
Technical professional personnel ........................................................ 5
Alaintenance of the antimalaria campaign and budget of the National Malaria Services...... 5
Legislation ...................................... O..............................9
Scope of the problem .................................................................. 10
Organization of the antimalaria campaign ................................................ 14
Antimalaria activities with imagocides ................................................... 16
Costs and productivity ................................................................ 20
Production of insecticides, solvents, emulsifiers, and equipment in the various countries ........ 22
Results of the campaign ............................................................... 22
Plans for the future ................................................................... 31
NEED FOR A COORDINATE PLAN FOR ERADICATION OF MIALARIA IN THE AMERICAS
At the national level .................................................................. 35
At the continental level ................................................................ 35
In the international organizations (WHO/PASB) ......................................... 35
iii

TABLES
Page1. Status of the national malaria service (or service responsible for the antimalaria campaign)
within the national public health organization of each country and territory ............. 22. Activities of the national malaria services in each country and territory ................... 43. Technical professional personnel in each country and territory ..................... 64. Participation in the maintenance of the antimalaria campaign in each country and territory.. 75. Budgets of the national malaria services in each country and territory, 1951-1954 ......... 86. Comparative antimalaria legislation in each country and territory ....................... 117. Total population, population in the malaria zones and percentage distribution in each coun-
try and territory ................................................................ 128. Exent of the malaria zones in each country and territory ............................... 139. Sanitary engineering works and antilarval campaigns in each country and territory ...... 14
10. Comparative results of malaria control with chloroquinated salt in two states of Brazil..... 1511. Imagocide campaign in each country and territory, 1950-1953 ..................... ...... 1612. Work with imagocides in each country and territory, 1950-1953 ......................... 17
Chart A. Antimalaria campaign schedule in Argentina ............................... 1813. Means of transportation available to the national malaria services in each country and terri-
tory ................... ................... .............................. 014. Unit costs and yield of the imagocide campaign in each country and territory ............. 2115. Malaria deaths in each country and territory, 1950-1953 ............................... 2416. Reported cases of malaria from all sources in each country and territory .................. 2517. Antimalaria drugs distributed as curatives and persons treated, in each country and terri-
tory, 1950-1953 ............................................................... 2718. Malariometric (parasitological) surveys in each country and territory, 1950-1953.......... 2819. Plans for the control of malaria in the future in each country and territory ................ 30
iv

STATUS OF THE ANTIMALARIA CAMPAIGN IN THE AMERICAS
V REPORT*
DRa. CARLOS A. ALVARADO
WHO/PASB Regional Malaria Consultant
To continue the tradition established atthe XI Pan American Sanitary Conference(Rio de Janeiro, 1942), the Pan AmericanSanitary Bureau requested the preparationof the V Report on the status of the anti-malaria campaign in the Americas. Like thelast report, presented to the XIII Con-ference (Ciudad Trujillo, 1950), the presentreport consists of two parts: the first con-tains an over-all comparative and analyticalstudy on the present status and the achieve-ments of antimalaria work in the WesternHemisphere; the second refers to the urgentneed for consolidating past gains through acoordinated plan on a continental scale forthe eradication of malaria in the Americas.In order to give as complete a picture aspossible, data were included on all politicaldivisions of the continent, including thosenot responsible for the conduct of theirinternational relations, these being referredto as "territories" for purposes of thisstudy.
To facilitate comparison with previousdata, the method of presentation used in theIV Report has, as far as possible, been fol-lowed in the present study.
PROGRESS OF ANTIMALARIA WORK INTHE CONTINENT
INTRODUCTION
The present status of the antimalariacampaign in the continent shows that sig-nificant qualitative and quantitative changeshave taken place since the preparation ofthe IV Report. Taken as a whole, the picturemay be considered favorable, although thevigorous impulse of the former period has
* Presented to the XIV Pan American Sani-tary Conference as Annex I of DocumentCSP14/36.
lagged somewhat during the last four years,and some countries have not taken fulladvantage of the splendid benefits obtainedthrough campaigns using imagocides.
A well-integrated antimalaria campaignshould proceed in two directions: (a) inbreadth, until all malarious zones of thecountry are covered, and (b) in depth, untiltotal eradication is achieved. Only fourcountries and two territories report thatthe first of these goals has been reached.The second objective has been achievedalmost completely by only one country;three other countries and two territorieshave achieved it in some areas.
Such factors as the spectacular reductionin the number of cases, the drastic loweringof parasitic indices, and the enthusiasmawakened by the collateral action of theimagocides against other arthropods, haveall exerted a negative influence on the plan-ning of antimalaria programs, on the struc-ture of the organizations concerned, and onthe policy of health authorities. Malariol-ogy, with its out-dated malariometry, basedon measures that were useful in the days ofantilarval campaigns and sanitary engineer-ing work, has not yet devised evaluationmethods to suit the strategy and fast actionof imagocides. As the results of campaignswere measured and evaluated with yard-sticks designed for other purposes, publichealth responsibility was considered fulfilledwhen indices dropped below a certain figureor when malaria no longer appeared in firstplace in mortality statistics. It was notrealized that this was comparable to detach-ing merely a segment of a tapeworm andthat any parasite index below 0.0, but notabsolute zero, meant the survival of the"head of the taenia." It is due to those last
1

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
vestiges of out-dated objectives and stand-ards that the four-year period 1950-53 hasfailed to keep pace and to exceed the levelreached during the previous period, thusthwarting the hopes expressed in the IVReport, which said:
If it were remembered that these results havebeen or are about to be achieved after a threeyear campaign only and in an area equivalentto two thirds of the malarious region of the conti-nent, one could appreciate the extent of the
progress made, as well as the well-founded hopethat the eradication of malaria can be achievedin the Americas within a relatively short time.
STATUS AND ORGANIZATION OF NATIONAL
MALARIA SERVICES
In this report, as in former ones, the term
"National Malaria Service" (NMS) will be
used to designate the service in charge ofthe antimalaria campaign. Table 1 showsthe administrative status and the specific
Table 1.-Status of the National Malaria Service (or Service Responsible for the AntimalariaCampaign) within the National Public Health Organization of each Country and Territory
Countries and Territories
Argentina ...............
Bolivia ..................Brazil ...................Colombia .................Costa Rica...............Cuba ....................
Dominican Republic......Ecuador ..................El Salvador .............
Guatemala ...............Haiti ....................Honduras ...............Mexico ..................
Nicaragua ................
Panama ..................
Paraguay .................
Peru .....................
United States............
Venezuela ...............
British Guiana...........French Guiana...........
Grenada ..................Jamaica ..................Puerto Rico..............Trinidad ................
Primary Division
Department of Malaria and YellowFever Control
Communicable Diseases DivisionNational Malaria ServiceSCISPDepartment of Insect ControlFinlay InstituteDivision of MalariologyNational Antimalaria ServiceDivision of Epidemiology
Insect Control SectionInsect Control CampaignSCISPDepartment of Epidemiology and
Public Health Campaigns
8th Division for the Control of In-sects and Metoxenous Diseases
Division of Public Health2
Asunción-Villarrica Area PublicHealth Program
Communicable Diseases DivisionSurveillance Section, Epidemiology
Branch (CDC-USPHS)Division of Malariology
Public Health DepartmentMalaria and Yellow Fever Control
ServiceMedical DepartmentInsect Control ServiceMalaria and Insect Control SectionMalaria Division
Secondary Division
National Malaria Department
National Malariology Division
Malaria Committee
Antimalaria ServiceVector Control ServiceDDT Campaign
Division of MalariologyNational Campaign against Ma-
laria and for the Prevention ofYellow Fever
Antimalaria Campaign'
Campaign against Malaria and Yel-low Fever
Division of Arthropod Control
Vector Control DepartmentNational Malaria Surveillance Pro-
gram
Mosquito Control Service
Insect Control Program
T In practice the antimalaria campaign is a primary service since it is the principal function of the8th Division.
2 The Public Health Division does not yet have a fully organized Central Office (Jefatura).
.
2

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
name of the NMS in each country or terri-tory.
The status of the NMS within the respec-tive National Public Health Service (NPHS)has changed somewhat since the last report.Argentina set up, in 1953, a primary serviceresponsible exclusively for malaria andyellow fever work, although the manage-ment and administration of the service con-tinue to be shared with the General HealthDepartment of the North. In Ecuador theNational Antimalaria Service is at presentalso a primary service, although it continuesto be under the direction and administrationof the Institute of Hygiene. In El Salvadorthere is no single service with complete re-sponsibility for this work, field operationsbeing under one service (Vector Control)and epidemiology and drug distributionunder another (Antimalaria Service), bothof which are coordinated within the Divisionof Epidemiology. In the United States,where all federal participation in the anti-malaria campaign has been suspended since1953, only a program of epidemiologicalsurveillance (National Malaria SurveillanceProgram) is being carried on under a sectionof the Epidemiology Branch, CommunicableDiseases Center (CDC), of the Public HealthService. In Guatemala, Haiti, and Nicaraguaprimary services were organized under thetitle of "Insect Control;" services wereorganized also in Paraguay, but these occupya secondary position. In Peru the old andwell-known Department of Malaria becamethe Vector Control Department. In thiscountry, as well as in two others (Guatemalaand Paraguay), the term "malaria" is nolonger used to designate sections of thepublic health services (even though malariacontinues to be a serious problem).
With regard to the territories, St. Luciahas no NMS, but the insect control programis a special service of the NPHS. There isno NMS in Dominica or in British Hon-duras, the antimalaria activities being in-cluded in the general functions of the PublicHealth Service. No data are available forGuadeloupe, Surinam, or the Canal Zone.
As to the internal organization of theNMS, some changes have occurred. Somehave been profitable and others not, butthe over-all picture continues to be favor-able. Argentina and Mexico have establishedinsecticide laboratories. The latter countrynow also has research and publications sec-tions. Brazil has organized a library in itsMalariology Institute, and Ecuador issuesregular publications on the activities of itsNMS. The Dominican Republic has set upsections for entomology and administration.Conversely, the NMS in Bolivia no longerhas its own administration, and in Peru theentomology, parasitology, statistics, andadministration sections have become part ofthe Division of Communicable Diseases.
Beyond analyzing the structure of theNMS, it is of even greater importance toconsider whether their work covers all as-pects of the malaria problem (anti-anophelescampaign, epidemiological evaluations, dis-tribution or application of treatments,registry of patients, parasitological confirma-tion of clinical cases, and epidemiologicalinvestigation of confirmed cases), or whetherit is limited to only a few of these activities;and also whether the NMS undertake otheractivities related to or coordinated withthe antimalaria campaign, or completelyunrelated. These activities are given indetail in table 2. Only Argentina and Vene-zuela approach the problem on a completeand over-all scale, since the United States(federal service) dropped from its programcertain activities that it had found no longernecessary. Next in line, as regards the scopeof activities, are Brazil, Ecuador, BritishGuiana, Puerto Rico, and St. Lucia. In othercountries and territories (excepting Cuba)the basic activity is anopheles control withimagocides, and decreasing emphasis isbeing placed on epidemiological evaluations,registry of patients, and parasitologic con-firmation of clinical cases. Only Argentina,the United States, and Venezuela, togetherwith British Guiana in part of its territory,make epidemiological investigations of eachconfirmed case of malaria.
3

Table 2.-Activities of the National Malaria Services in each Country and Territory
Countries and Territories
Argentina .........Bolivia ............Brazil .............Colombia ..........Costa Rica........Cuba ..............Dominican Rep....Ecuador ...........El Salvador.......Guatemala ........Haiti ..............Honduras .........Mexico ............Nicaragua .........Panama ...........Paraguay ..........Peru ..............United States.....Venezuela ........
British Guiana...British Honduras..Dominica .........French Guiana...Grenada ...........Jamaica ...........Puerto Rico.......St. Lucia..........Trinidad .........
Antimalaria
-·
XXXXX
XXXXXXXXXXX
X
X
XXXXX
X
X
X
X1~1--
_b
a;. m002
X
u
XXX
X
X
X
XXXc
XXXX
X
XX
X
X
XX.
5>0
0. 0
0*- E
X
XX
X
'Z d
XXXg
X
X
Xf
XXf
0g
Xef
XXg
X f
XXfXef
XfXfXfXf
Xf
X
XX
XX
XXX
sja
o0 ,-
X f
X
XiX'
x
XXf
XgXf
XfXf
Xd
X
X
X
XX
X
X
XX
Xf
-.0 >,
E >t1 Z
,uiW
X
XX
Xk
Not Antimalaria
Related or combined
YFh, AC
CD', FI, CSyFh
YFh, CD', FCMC
YFh-_i
YFh
YFh
YFh
YFh, AC, CSYFh
YFh, ACyFh
YFh, CD', VP
YFYFI, CD
i, FC, DD
YFhYFYF
YF, FIYFYF
YF, ACYF, ACYF, AC
-None.... Data not available.a Imagocides or larvicides not applied; only antimalaria engineeringb No federal activity. Some states conduct activities on their own ace Only in zones where measures were either not applied or were appliecd Reports that such work is done but does not give figures.o In official medical services only.f Data incomplete.g Only among personnel of the United Fruit Company.h Basically, Aédes aegypti eradication; occasionally, vaccination.
Principally control of Triatomidae.Imagocides applied solely as a measure against mosquitoes and flies.
k Only in those cases occurring along the coastal plains.N Activity in operation.YF Yellow fever. DD Diarrheal diseases.AC Anti-Culex campaign. SC Schistosomiasis.CD Chagas' disease. ET Epidemic typhus.FI Filiariasis. MT Murine typhus.CS Control of scorpions. RF Relapsing fever.FC House-fly control. PL Plague.MC Over-all antimosquito control. SC Street cleaning.VP Verruga peruana (bartonellosis). C:P Construction of sani
4
Totally different
SC
ET
PL
ET, MT, RF, PL, SC
SC, CP
projects.count.d irregularly.
tary privies.
I I

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
In fourteen countries and nine territories,the NMS have responsibility for Aedesaegypti eradication and thus, in an activityclosely related to their regular work, arecontributing toward the implementation ofthe important resolution adopted by theDirecting Council of the Pan AmericanSanitary Organization at its first meeting(Buenos Aires, 1947).
TECHNICAL PROFESSIONAL PERSONNEL
The tabulation of technical professionalpersonnel does not include part-timeworkers, who are few in number and of lessimportance. Table 3 shows the figures bycountry and by professional groups. TheUnited States reports a total of 30 medicalofficers with specialized training (as com-pared with 1 in 1950), but these participatealso in other activities of the CommunicableDiseases Center. Not counting this group,the total is the same as for 1950. For allcountries, the total number of non-spe-cialized physicians (but who have acereditedexperience) has doubled (41 as comparedwith 20).
The total for engineers is lower, but thisdecrease is due exclusively to their reductionin number in the United States and Argen-tina. There are also fewer entomologists (34as compared with 109 in 1950), but thissizeable reduction is accounted for by de-creases in only two countries, the UnitedStates and Brazil, which had 40 and 55,respectively, in 1950.
Five countries (Argentina, Brazil, Ecua-dor, the United States, and Venezuela) havetraining facilities for all categories of person-nel and these facilities can be extended topersonnel from other countries. In twocountries, Ecuador and Venezuela, fellow-ships are granted to include, in the former,room and board at the Leopoldo IzquietaPérez National Institute of Hygiene, and,in the latter, a sum of money to cover theseexpenses (500 bolivars per month). In theother countries travel and study fellowshipsmust be obtained from other sources.Colombia, Costa Rica, the Dominican Re-
public, El Salvador, Panama, Paraguay andPeru report that they have training facilitiesfor field personnel only.
Mention should be made of the debt owedby the countries of the Americas to theSchool of Malariology of Venezuela, whichhas trained the majority of professionalmalariologists and malariology engineersnow directing or working with the NMS ofall Latin American countries (with the ex-ception of Brazil).
MAINTENANCE OF THE ANTIMALARIA CAM-
PAIGN AND BUDGET OF THE NATIONAL
MALARIA SERVICES
In almost all countries of the Americasthe organization of antimalaria campaignscontinues to be the responsibility of thenational government. The most notable ex-ception is the United States, where the re-sponsibility rests with the states, whichhave the cooperation of the counties. From1951 on, federal support for antimalariaprograms in that country was graduallywithdrawn, leaving only an epidemiologicalservice to give supervision and to verify theresults (National Malaria Surveillance Pro-gram). In Braz'il, the state of Sao Paulocontinues to maintain an independent pro-gram, but no specific data could be obtainedon its activities.
The most significant facts for 1950 arethe above-mentioned withdrawal of federalsupport for antimalaria campaigns in theUnited States and the collaboration offeredby WHO/PASB and UNICEF in twelvecountries and six territories. Only Cuba andPuerto Rico have reported that their anti-malaria activities are supported exclusivelyby the National government. Elsewhere,either the states, provinces or departments,municipalities, private enterprises, or inter-national agencies (UNICEF and WHO/PASB, SCISP)1 collaborate in their opera-tion and mintenance.
Table 4 presents, in detail, all the informa-
1 Servicio Cooperativo Interamnericano de SaludPública (Inter-American Cooperative PublicHealth Service).
5

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
Table 3.-Technical Professional Personnel in each Country and Territory
Countries and Territories
Argentina .................Bolivia ......Brazil ...... ................
Colombia ..................Costa Rica ...................Cuba .........................Dominican Rep...............Ecuador ......................El Salvador .................Guatemala ...................Haiti .........................Honduras ..............Mexico .......................Nicaragua ....................Panama ......................Paraguay .....................Peru .........................United States ................Venezuela ....................
Countries Total............
British Guiana ...............British Honduras .............Dominica .....................French Guiana ...............Grenada ......................Jamaica .....................Puerto Rico ..................St. Lucia .....................Trinidad .....................
Territories Total...........
Continent Total............
General Total in 1950......
Malariologists Engineers
wwith ith wi withspecialized accredited specialized accredited
degrees experience degrees experience
23
613
16111
83
12
30,25
148
1
1
2
12
7
155
118
14
65
3
72
2
40
1
1
41
20
21111
1
65e9
27
27
36
2
3
3
8
11
111
5
13
17
Entomologistsa
2
51
1
25ld
11
7c1
27
2
212
7
34
109
EntomologicalTechniciansl'
133
52311
31
136
213
30
123
2
215
1896
43
166
e
a Understood to be persons capable of classifying any anopheles in the country.b Understood to be persons capable of classifying anopheles (larvae and adults) irl their own coun-
tries.* Participating in other activities of the CDC.d At present taking a specialized course in Brazil.
These data were not requested in 1950.Guadeloupe, Martinique, Surinam, and Panama Canal Zone did not send data.
tion obtained on the type and anmount ofthe contributions made toward the main-tenance of antimalaria campaigns.
Table 5 gives the annual budgets for thefour-year period 1951-1954, it being under-
stood that, where the fiscal year begins on1 July, the year referred to is that beginningwith the fiscal period. The budgets are givenin the national currency of each country, i
and the last column shows the 1954 budgets
6
e

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
Table 4.-Participation in the Maintenance of the Antimalaria Campaignin each Country and Territory
Countries and Territories
Argentina .........Bolivia ............Brazil .............Colombia ..........Costa Rica........Cuba .............Dominican Rep....Ecuador ...........El Salvador.......Guatemala ........Haiti .............Honduras ..........Mexico ............Nicaragua .........Panama ..........Paraguay ..........Peru ..............United States......Venezuela .........
British Guiana....British Honduras.Dominica .........French Guiana....Grenada ...........Jamaica ...........Puerto Rico.......St. Lucia ..........Trinidad ..........
b
d
e
f
g
h
i
k
z
nonononono
no
no
nono
nononononono
nono
no
>1l>e
o .,ca -
nonoyesyesnonono
nononononononononoyesno
Nation in Financial Collabora-tion with:
yes
yesyesnononoyes
nononoyesno
noyesyes
nonoyesyes
yes
no
.o1:
yes
noyesno
yesyesyesyesyes
yes ¡ yes
yes
yesyesnoyes
noyesno
nono
yes
no
yesnoyesyesnoyes
noyesno
yesyes
no
uD
maD3-)
no
nonono
noyes
nonoyesyesnoyes
yesnono
nono
no
yes ¡no
yes noyes -
no
yesno
yesyes
yesno
yesyesyesyesyes f
yesyesyesno
no
no
no
yesyes f
no
yesyes
yesyes
Amount of1951 and 1953
NMS budgets(in
thousands)1
18,460.522,845.6
640,798.47,073.7
730.0112.4a522.9
19,270.21,576.6
300.0131.6501.0
5,7 6 8.2k2,168.1
495.01,160.0
17,698.51,396.0
40,846.0
454.26.5 e
8.570,992.4
54.3155.6949.9
77.2864.1
Amount oflocal con-tributions
1951-53 (inthousands)'
2,424.0
9,400.0 h
390.0184 .5i
77.467.0
103.9
80.01,256.0
22.9
Percent-ageratio
13.1
1.55.5
0.44.2
34.6
SCISPcontri-
butions(in
thou-sands)'
962.3
16.0 601.021.0
4.6
5,780.2 414.6,817.5 16.7
d
d
d
d
d
d
d
8.7¡
WHO-PASB-UNICEF
contributions(in o
thousands)'
375.0i
58.6US$160.0
78.5
US$127.726.0
US$ 50.0c
Primary division of the country or territory.Secondary division.Vehicles and materials by WHO-UNICEF.No data given on amount contributed by states, municipalities, and/or private enterprise.1953 only.WHO-UNICEF to collaborate beginning October 1954.1951 budget not included.Private enterprise contribution not included.Local and international agencies' contributions combined.No data given.Other governmental agencies contribute approximately $2,000,000 (Mexican pesos) annually.Amounts are shown in each country's own currency unless otherwise specified.
converted into U.S. dollars at the free rate that, in spite of the fact that the majorityof exchange in effect in July of the same of the countries report an increase in fundsyear. allocated to antimalaria campaigns, the
In the study of the budgets, it is evident percentage of the total public health budget
7
c
c
c
C

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
allotted to this activity in the individualcountries has dropped in some countries toa considerable degree. In large part thisdecrease has been caused by the fact that,while other public health activities havebeen increasingly expanded, antimalariaprograms have remained the same. It would
operations. Several NMS have taken on newresponsibilities, making it necessary for thecosts of administrative-technical services tobe met with funds from antimalaria andother activities, with the result that thespecific budget for antimalaria work issometimes greatly reduced.
Table 5.-Budgets of the National Malaria Services in each Country and Territory, 1951-1954
Countries andTerritories
Argentina .........Bolivia ...........Brazil ...........Colombia .........Costa Rica........Cuba ............Dominican Rep...Ecuador ..........El Salvador........Guatemala ........Haiti .............Honduras ......Mexico .............Nicaragua .....Panama
a..........
Paraguay f ...Peru ...............United States......Venezuela ........
British Guina .....British Honduras..Dominica ..........French Guina....Grenada ...........Jamaica ......
Puerto Rico ......St. Lucia.........Trinidad .. ......
Currency
pesobolivianocruzeiropesocolonpc sopesosucrecolonquetzalgourdelempirapesocordobabalboaguaranisoldollarbolivar
BWI $BH dollarBWI sfrancBWI spound
sterlingdollarBWI $BwI $
National Malaria Services Budgets(in thousands)
1951
5,454.15,455.2
220,251.5954.3259.6
177.07,491. 6
527.8
100.032.4
e
120.01,445.2
359.4135.2120.0
3,743.8810.9
12,074.8
137.8
2.518,495.0
9.443.2
317.317.6
268.8
1952
5,933.25,920.4
206,471.73,085.4
323.159.2
205.75,441.6
586.7100.0
60.5e221.0
2,146.4968.4202.4360.0
4,375.5355.0
14,384.1
152.8
3.025,247.4
11.352.3
318.020.6"
289.5
1953
7,073.111,470.0
2141,075.33,034.0
147.3b
53.2140.2
6,337.0462.1100.038.5
e
160.02,176.5
840.3157.4680.0
9,579.1230.1
14,387.1
163.66.53.0
27,250.033.660.1
314.639.0"
305.8
1954
6,894.518,064.0
233,892.93,043.4
15 7 .8b53.2
161.54,400.0
657.050.079. le
220.02,780.31,256.0
150.5900.0
11,560.8104.5
14,287.5
149.412.03.0
17,281.043.565.8
300.052.6a
332.4
DoesSer-vicehaveits
ownbud-get?
d
noyesyesnoyesyesyesyesyesnoyesyesyesnonononoyes
yesnonoyesyesyes
yesyesyes
Percentageof Nat'l. 1954
Pub. indexHealth 1951 =budget 100
1954
1.63.5
11.37.4
0.33.0
20.917.4
1.32.5
14.11.4
16.82.22.63.00.048.9
3.8353.9
17.756.564.54
1.0419.044.14
126331106319
889159
12450
24418319234911175030913
118
108185e
12093
463152
95299124
a Includes other activities in addition to antimalaria work.b Salaries only; data on other costs not given.
c Base 1953 = 100.d Part is its own budget and part is included in other activities.e In dollars.f Estimate for 1952-1954.
seem that the increase in funds allotted forantimalaria work in many of the countriesis the result, not of actual expansion ofactivities, but rather of increases in the costof material and equipment and of salariesof personnel. In some cases the NMS budgethas really been decreased, as in the case ofArgentina, owing to changes in the structureof the service and a reduction in the area of
The figures in table 4 are designed to show,for a considerable number of countries, thefinancial collaboration of the various localagencies and international organizations. Itis apparent, from the extensive participationof states, municipalities, and private enter-prises, that community interest in the anti-malaria campaign has been kept alive. Aftermentioning the case of the United States,
8
Freedollar
exchange,rate as of
31-7-54
25
1,400572.56.65II
17.52.5152
12.56.6
6220
3.35
1.71.43
1.7
1.7
1.71.7
1954budget inthousandsof dollars
(freeexchange
rate)
275.812.9
4,103.41,217.3
23.753.2
161.5251.4262.850.015.8
110.0222.4190.3150.514.5
578.0
4,264.9
87.98.41.8
25.6
300.030.9
195.5
.e
,

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
where all activity is carried out on a localscale, it is fitting to point out that the statesof Venezuela contribute the equivalent of16.7% of the budget; the municipalities inHonduras contribute 16 %; private enter-prises in Guatemala contribute 34.6 %; andin Mexico and Argentina the total contribu-tion of these groups is 21% and 13.1 %, re-spectively. In Mexico, in addition, othergovernmental agencies contribute each yearamounts almost as large as the budget ofthe NMS itself. In Brazil, although the con-tribution of these groups represents only1.5% of the total budget of the NMS, thesum of 9,400,000 cruzeiros, contributed bythe states alone, is of considerable import-ance.
Undoubtedly, the most promising and sig-nificant development in the antimalariacampaign in the Continent is the expansionof the programs promoted by the WHO/PASB, with the financial support ofUNICEF. Five countries and one territoryreceived their assistance in 1950; the numberthat continued or began working with theequipment, transportation facilities, andtechnical assistance furnished by theseinternational organizations increased totwelve countries and six territories.
LEGISLATION
With the exception of Cuba, El Salvador,Haiti, Nicaragua, and Panama, all thecountries and territories mentioned in thisreport have legislation on malaria, and themajority of them deem it an obligation tocombat this disease. Ecuador, in referring tothe campaign against malaria, declares itseradication to be an urgent national enter-prise. Argentina, Panama, and Venezuelaalso classify the problem as one of nationalinterest, although not to the same extent asdoes Ecuador. The remaining countries donot put the same emphasis on the problem,but an analysis of the legislation in forceshows the importance given to the legalaspects of the antimalaria campaign through-out the Americas.
Argentina, Brazil, Panama, Peru and
Venezuela all have exhaustive legislation onthe subject, the most complete being theArgentinian law, complemented by its regu-latory decree. In the other countries, meas-ures concerning the antimalaria campaignare included in laws covering communicablediseases in general, in sanitary codes, or inlaws, decrees, or statutes aimed at combatingthe problem through united action againstnoxious or vector insects. However, in thesecases, all aspects of the antimalaria cam-paign are not covered. Unfortunately, there-fore, in the majority of the countries legisla-tion has not been adequately adapted tonew concepts of antimalaria strategy. As aresult of this fact, some of the indispensableactivities for the conduct and evaluation ofoperations (such as compulsory and immedi-ate reporting, and parasitological verificationof clinical cases occurring in regions undertreatment with imagocides or where malariais presumed to be eradicated) can be carriedout only with considerable effort, unless ahigh level of health education of the publicexists.
Declaration of "malaria zones" is notcompulsory in all countries and, where it is,such a declaration is made by the responsiblehealth authority upon advice of the agencyspecifically entrusted with the antimalariacampaign.
Environmental sanitation works designedto physically improve the environment,combat larvae, or protect communities bymechanical means, are in almost all nationsand territories under the responsibility, first,of the governments and second, of propertyholders, managers, tenants, etc. It is uponthat subject that the most emphasis hasbeen placed in the legal bodies concerned;steps taken have covered the most minutedetails. The use of imagocides in residencesis covered specifically only in the legislationof Argentina and of four territories (Grenada,British Guiana, French Guiana, and St.Lucia), although that of Peru, by referringto "other insecticides," leaves the way openfor the use of other types that have appearedrecently. The fact that only two countries
9

STATUS OF, ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
and four territories emphasized such respon-sibility is easily explained in that almost allthe legislation in force was passed before thediscovery of the modern insecticides. Theeffectiveness of environmental sanitation, inevery aspect, is based upon the obligationimposed by some laws to give public healthpersonnel access to any property or residencethat is to be covered.
In some countries the governrnent andvarious agencies have been made responsiblefor the supply of drugs. Only the laws ofArgentina refer to supervision of the dis-tributing and dispensing of such drugs, whichis an important measure since, when noti-fication is lacking, cases of malaria thathave not been reported in due time can berecognized and traced through this pro-cedure.
Only Brazil and Argentina have laws re-ferring to new or temporary dwellings andmaking it compulsory to report their in-stallation, so as to make the antimalariacampaign more effective.
Special importance is now placed on thereporting of malaria cases. The majority ofthe countries require such reporting; somefix definite time limits and specify whoshould have the responsibility for reporting,to whom the report should be made, in whatform and under what conditions, and if thereport should be accompanied by a bloodsample or any other evidence. Only Argen-tina, British Guiana, and Puerto Rico havemade it compulsory for blood tests to besent for parasitological confirmation. Inconnection with this requirement, somecountries make it the duty of the patient toseek treatment and to submit to a blood test.
In order to make the afore-mentionedstandards effective in practice, the majorityof the countries have established variouspenalties for failure to comply with any ofthe legal requirements. Argentina imposessevere fines on those who are responsible forreporting malaria cases and fail to do so, aswell as on persons who are required to sub-mit to blood tests and refuse.
The real importance of clearly defining in
legal statutes the measures for combatingand eliminating diseases is undeniable. Fromthis brief analysis can be seen the urgentneed for bringing present legislation up-to-date and for promoting such legislation inthose countries where it does not exist, soas to adapt the laws to the new methodsand requirements of the modern campaignto combat malaria, and, above all, to accom-plish the supreme objective of eradication.
Table 6 presents comparative malarialegislation in the Americas.
SCOPE OF THE PROBLEM
Under this same heading in Report IV(1950), the extent of the malaria problem inthe Americas was analyzed and discussed.The area of the malaria zone in each countryand the population in that zone, facts thatwere important as a starting point for theinitial evaluation of the problem, were takenas a basis for the discussions. In the future,the evaluation of the scope of the problemshould be based on a knowledge of currentconditions, and for this reason additionalfactors should be considered. In this reportfigures on inhabitants will be given for (a)"eradication zones," (b) "protected zones"(inhabitants directly or indirectly protected),and (c) "unprotected zones." These figurescover the "malarious zone." Table 7 presentsthis information. As a supplement, table 8shows the corresponding areas covered. Thecountries, now having a better knowledgeof the situation, apparently have made ad-justments in the total population figures forthe malaria zone, these figures being moreor less different from those in the IV Report.
Not including Guadeloupe, Surinam, andthe Canal Zone, which did not send data,the total population of the continent re-siding in the"malarious zone" is 135,000,000,of which 60,000,000 (44.4 %) live in the"eradication zones," 45,000,000 (33.3%) inthe "protected zones," and 30,000,000(22.2%) in the "unprotected zones." Thepresent extent of the problem can, then, beexpressed as 55.5 % of the original figure.
1q
.4
J
10

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT 11
Table 6.-Comparative Antimalaria Legislation in each Country and Territory
Countries and Territories 1. 2. 3. 4.1 4.2 4.3 5. 6. 7. 8. 9. 10. 10.1 10.2 11. 11.1 12.
Argentina ............. x x x x x x x x x x x x 1 x - x xBolivia............... x x x x x x - - x - - x 7 -- - x
Brazil ................. x x - x x x - x x - x x - - - - x
Colombia............. x x x x x x - -- - - x 7 - -
Costa Rica........... x x x x x- - - x
Cuba ................. -- x 1 - -Dominican Rep........ x x x x - x - x - - - x 8 - x x x
Ecuador .............. x - x d
El Salvador ...........- - - -
Guatemala............ x - x x x- x - - - x 1
Haiti ................. -- . .Honduras............. x - - - - x --
Mexico................x x x x - - -- - - - x 1 -
Nicaragua ............ -- - - - -
Panama ............... x x - x x x - - - - - x 7 - -
Paraguay .............- - - x - -- - -
Peru .................. x x x x x x x x x - - x 7 - - - xUnited States b...... x x - x x - - x - - - x 7 - - - x
Venezuelab............ x x x x x x - x - x 7 - x x x
British Guiana ....... x x - x x - x x - x d x - - X
British Honduras..... x x - x - - - - - - - x - - - - x
Dominica .......... x - x x- - - - - - x 30 - - - x
French Guiana ........ x x - x - - x x - - - - - - - - x
Grenada ............. x x - - x x - - - - - - - xJamaica ............. x - - - - - - - X d - -
Puerto Rico ........... x x - x x - - - - - - x 5 x - _ x
St. Lucia ......... x x - - x - x x - - - x 7 - - x
Trinidad ............. x x x x - - - - - - - - - - - - x
1. Has legislation.2. Obligation to combat malaria.3. Declaration of malaria zones.4. Obligation to carry out environmental sanitary activities:
4.1 of the physical environment;4.2 antilarval measures;4.3 mechanical protection.
5. Obligation to apply imagocides.6. Obligation to permit access to houses.7. Obligation to give drugs.8. Control of distribution and dispensing of drugs.9. Obligation to report the construction or renovation of dwellings.10. Compulsory case reporting:
10.1 time limit (No. of days);10.2 with blood sample.
11. Obligation of patient to take treatment:11.1 obligation of patient to permit blood extraction.
12. Sanctions.aState legislation only. bData taken from IV Report (1950). eDid not transmit legislation. dIm-
mediate reporting, but without indicating time limit.
Undoubtedly, the eradication of malaria fifths of the population are within the "pro-
> in the United States brought about this tected zones." With respect to the remaining
sharp change in the continental picture. two fifths, as yet unprotected, the responsi-
As to the present extent of the problem, three bility, in absolute and proportionate terms,

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
Table 7.-Total Population, Population in the Malaria Zones (in thousands), and PercentageDistribution in each Country and Territory
Countries and Territories
Argentina ...........Bolivia ..............Brazil ...............Colombia ...........Costa Rica..........Dominican Rep......Ecuador.............El Salvador.........Guatemala ..........Haiti ................Honduras ............Mexico ..............Nicaragua ...........Panama .............Paraguay ............Peru ................United States........Venezuela ...........
Br. Guiana..........Br. Honduras ........Dominica ............Fr. Guiana ..........Grenada .............Jamaica .............Puerto Rico.........St. Lucia............Trinidad and
Tobago ............
u
194719501950195119501950195019501950195019501950195019501950194019501950
19461946194619461946194319501946
1946
TotalPopulation
15,893.83,019.0
Populationof Malaria
Zones
Number centcent
1,855.0 100600.0 100
51,944.4126,800.0110011,545.4
800.92,135.93,202.81,855.92,788.13,097.31,368.6
25,791.01,057.0
756.61,405.66,208.0
150,697.4
6,999.9406.6
1,040.41,764.41,282.31,000.02,070.3
416.419,991.01,125.0
499.1422.8
3,773.157,790.5
100100100100100100100100100100100100100100
5,034.91 3,560.91100
369.859.247.628.572.4
1,237.12,210.7
70.1
558.0
465.475.858.030.4
120.0208.7
1,279.585.0
100100100100100100100100
508.01100
aIncluded in the population directly protected.bIncluded in the populations directly and indirectly protected.
rests with the following countries:
% of totalUnprotected populationpopulation unprotected in
Country (in thousands) the continent
Mexico .............Colombia ...........Brazil ..............Haiti .............Peru ...............El Salvador.........
Paraguay ...........12 other countries...
19,159.13,928.7
1,900.01,800.01,229.0
516.4397.0
1,050.6
63.713.16.3
6.04.11.71.33.8
A study of the areas involved (table 8)
reveals a close relationship between the fig-ures for unprotected population and thearea of unprotected zones:
% of totalArea of un- area un-
Country
Mexico .............Colombia ...........Peru ...............Brazil ..............British Guiana......Bolivia .............Paraguay ...........9 other countries....
protected protected inzones (km2) the continent
1,800,000
786,341613,582355,000180,556150,00069,50062,677
44.819.615.3
8.84.53.71.71.6
PopulationIndirectlyProterteted
Population inEradicated
AreaUnprotectedPopulation -s
PopulationDirectlyProtected
Number Pecel
750.0 4161.3 2
14,200.0 52,455.3 3
390.2 9800.0 7
1,213.5 6623.1 4235.8 2150.3256.4 6623.9
1,043.0 9199.9 425.8
1,264.9 3
2,248.0 6
150.9 344.8 56.1 1'
28.4 936.0 3,
208.7 10'643.7 5/50.8 6i
386.0 7,
Number cPen
O O200.0 33
1,900.0 73,928.7 56
16.4 4O O
124.0 7516.4 40210.3 21
1,800.0 87100.0 24
19,159.1 9675.0 6
187.2 37397.0 94
1,229.0 330 OO O
r t Numbernt
905.0238.7
10,700.0615.9
O240.4206.9142.8553.9120.060.0
208.07.0
112.9O
1,278.3O
1,312.0
311.530.0O2.0
36.0O
635.80.4
Percent
4940409O
231211556
1411
23O
34O
37
6740O7
30O
500.4
114.0122
Number
200.000O00
220.0Ooo00oooo0
0
0
57,790.5(1,538.4)a
(442.0)booOOoooo
0
Percent
11oOO00
12000O
00000
100
0000ooO
o
3.01.0
51.9o
48.0oo
33.8
8.0
11
90o
40Oo
40
2
'4
12
I

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
It can be seen, by the foregoing, thatMexico and Colombia hold first and secondplaces; Brazil and Peru maintain practically
St. Vincent, Grenadines, Barbados); otherislands had small endemic foci that havedisappeared in recent years (Antigua, Mar-
Table 8.-Extent of the Malaria Zones in each Country and Territory(in km2)
Countries and Territories
Argentina ...............Bolivia ..................Brazil ...................Colombia ................Costa Rica..............Cuba ....................Dominican Rep..........Ecuador.................El Salvador .............Guatemala ..............Haiti ....................Honduras ................Mexico ..................Nicaragua ...............Panama.................Paraguay ................Peru ....................United States............Venezuela ...............
British Guiana..........British Honduras........Dominica ................French Guiana..........Grenada .................Jamaica .................Puerto Rico.............St. Lucia ................Trinidad ................
Total Area of MalariaZone (as perReport IV)
270,000721,500
7,295,000760,00039,10030,00030,200
220,00021,20080,0005,600
80,0001,800,000
128,30066,600
172,300800,000
2,309,600600,000
22,300
86,000
3,630
Area of Zone ofEradication
60,000
3,016,548,180,000
5,000
Area of Operations
140,00061,000
6,337,271160,00029,738
96,10010,200
70040,00041,80020,00037,0002,400
252,667
600,000
83,000
83,60076
5,090
1,200
Area Occupied byUnprotected Population
O150,000355,000786,341
1,788
O
9,100
14,000b
20,0001,800,0000
17,00069,500
613,582O0
180,556
130O
74
O130455
Note.-Figures in Column 1 are 1950 estimates of area of endemic and epidemic malaria zones. (Re-port IV, Publication No. 261-Annex B, PASB-WHO). Figures in Columns 2, 3, and 4 are those for datagathered in 1954 and refer chiefly to endemic malaria zones; this explains the discrepancy betweenfigures in Column 1 and the sum total of Columns 2, 3, and 4.
. Data not available.a Data for 1954.b Malaria area recalculated in 1950.o Includes area of zone of eradication.
the same position; and Paraguay continuesin seventh place. But, in "unprotectedzones," British Guiana and Bolivia takethe places of Haiti and El Salvador.
Special mention should be made of theLesser Antilles. The majority of the areahas a history of malaria epidemics (Bahamas,
tinique, St. Kitts, Nevis, Anguilla). Theremaining areas have no record of malaria(Cayman, Turks, Caicos, Virgin Islands,Aruba, and Curaçao). Guadeloupe sent nodata.
Although Chile gives no data on malariacases, it reports an "eradication zone" cover-
13

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
ing an area of 15,000 square kilometers with10,000 inhabitants, and a total of 102,789persons protected with imagocides and anti-larval measures. Only Uruguay and Canadahave remained completely free from autoch-thonous malaria.
This chapter will discuss methods of malariacontrol based on engineering works and theuse of larvicides and drugs. Because of theirimportance, the imagocides will be taken upunder a separate heading.
Table 9 shows that four countries (Cuba,
Table 9.-Sanitary Engineering Works and Antilarval Campaigns in each Country and Territory
Countries and Territories
Argentina ...........Bolivia .............Brazil ...............Colombia ...........Costa Rica..........Cuba...............Dominican RepublicEcuador a ............El Salvador.........Guatemala ..........Haiti ...............Honduras ..........Mexico ..............Nicaragua .........Panama .............Paraguay ...........Peru ................United Statesb .....Venezuela ...........
British Guiana......British Honduras...Dominica ..........French Guiana......Grenada ...........Jamaica ............Puerto Rico.........St. Lucia...........Trinidad ............
Anti-malaria
engi-neering
projectsunderway
nononononoyesnoyesnonononoyesnonononoyesyes
noyesyesnoyesnoyesyesyes
Work projects under way
Lined canals; piped drains; fills
Fills and drainage maintenance
Lined canals; drainage
Antimalaria hydraulic control programsLined canals; piped drains;reforestation;
fills
DrainageLined canals; drainage
Lined canals; drainage
Conservation and small-scale drainageLined canals; drainageDrainage; fills
a SCISP projects. b Only the states and certain agencies.
ORGANIZATION OF THE ANTIMALARIA
CAMPAIGN
The manner in which the antimalariacampaign is conducted depends largely onthe organization of the NMS. Informationhas been given previously as to the way inwhich the different countries and territoriesdeal with the basic aspects of the problem.
Ecuador, Mexico, and Venezuela) and sixterritories (Dominica, Grenada, BritishHonduras, Puerto Rico, St. Lucia, and Trini-dad) continue carrying out the so-called"permanent control" works. In Ecuadorthey are carried out exclusively by SCISP.These works certainly contribute to thephysical improvement of the environment,
dE~C
r 5au ca
aH
40
40
100
1953
aB E1 w
. o._ M Q_
.. A_ _
t e * 5 -
2022
12000
14080
_- 408- 24000
.4
noyesnononononoyesnoyesnononoyesyesnonoyesno
nononononoyesnoyesyes
50
9
124
86
67
.A
22
50 52848
257046267
44r
14

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
but if the effort and investment made areweighed against the cost and effectivenessof the imagocides, it is clear that they areindeed a luxury in the antimalaria campaign.It is undoubtedly for this reason that theywere abandoned in Bolivia, Brazil, Colombia,the Dominican Republic, Peru, and FrenchGuiana, countries -which in 1950 reported
Brazil has begun a far-reaching experi-ment of malaria prophylaxis by means ofdrugs, combining chloroquine with tablesalt (Pinotti method), at the rate of 50 mg.of chloroquine diphosphate (30 mg. base)in each 10 g. of common salt. As the quantityof this salt consumed daily by man undernormal dietary conditions is from 10 to 15 g.,
Table 10.-Comparative Results of Malaria Control with Chloroquinated Salt in two States of Brazil
A-Two Adjoining Areas in the State of Maranhao
Treated zonea Control zone
Parasitemia
March 26th May 15th May 25th March 31st May 27th
Persons examined .............. 132 119 100 115 76' With positive blood ............ 13 2 1 12 10
Parasitic index % .............. 9.8 1.7 1.0 10.4 13.2P. vivaz ........................ 5 - - 11 7P. falciparum .................. 4 2 1 1 3P. malariae .................... 1 - -Mixed (P.v. and P.f.) .......... 3 ..
B-Two Adjoining Areas in the State of Para
Treated Zone (Rio Capim) Control Zone (Rio Guama)
Parasitemia
June 1952 Aug. 1952 Nov. 1952 Jan. 1953 May 1953 June 1952 Nov. 1952 Jan. 1953 May 1953
Persons examined ............. 389 331 641 477 616 204 299 247 350With positive blood............ 33 2b 0 0 lc 14 11 15 89Parasitic index % .............. 8.5 0.6 - _ - 0.2 6.9 3.7 6.1 25.4P. vivaz ........................ 15 - - - 1 13 4 9 45P. falciparum ................. 17 2 - - - 1 7 6 12P. malariae .................... - -- - - - 1Mixed (P.v. and P.f.).......... 1 - - - - - - 1
a Exclusive use of chloroquinated salt beginning 16 April 1953.b One newborn baby, breast-fed only, and one adult living in the area three days.
:j- 1e One year-old baby, breast-fed only.
that they were planning and carrying outworks of this kind. In the United Stateswater management programs continue inoperation, but only under the responsibilityof states and counties.
Table 9 also shows that six countries(Bolivia, Ecuador, Guatemala, Nicaragua,Panama, and the United States) and threeterritories (Jamaica, St. Lucia and Trinidad)apply antilarval measures, although on a
v very reduced scale as compared with thefour previous years.
an adult would absorb daily from 50 to 75mg. of chloroquine (30 to 45 mg. base) ifchloroquine salt were all that were consumed.First experiments seem to have demon-strated the efficacy and innocuousness ofthis method, which would have a large fieldof application in regions inaccessible toimagocide campaigns or where the low popu-lation density makes these campaigns costlyor uneconomical. The method might beuseful also to supplement or even to replaceinsecticides in special situations in which
15

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
the vector is found predominantly outsidedwellings. Table 10 shows the results ob-tained in Brazil in two localities in whichchloroquine salt was used, as compared with
malaria campaign in the Americas. The onlyexception to this is Cuba, which continuesto stress sanitary drainage work and anti-larval control. However, in the near future
Table 11-Imagocide Campaign* in each Country and Territory, 1950-1953
Countries and Territories
Argentina ................Bolivia ..................Brazil ....................Colombia ................Costa Rica...............Cuba....................Dominican Republic......Ecuador .................El Salvador..............Guatemala ...............Haiti ....................Honduras ................Mexico ...................Nicaragua ...............Panama ..................Paraguay ................Peru .....................United States............Venezuela ................
British Guiana...........British Honduras........Dominica ...............French Guiana...........Grenada .................Jamaica ..................Puerto Rico..............St. Lucia.................Trinidad .................
Totals ...................
DDTa
1950
73.17.6
1,430.015.28.6
16.767.816.434.5
21.624.825.6
6.1
48.3429.3314.3
13.73.2
2.80.10.4
39.20.28.6
2,618.0
1951
35.98.0
802.032.017.7
17.984.169.048.8
25.120.877.820.0
1.236.8
191.9407.9
12.13.1
2.80.51.9
44.70.29.1
1,971.3
1952
51.76.2
1,400.095.420.9
20.3102.785.321.6
18.911.978.320.73.6
45.373.6
408.9
10.16.1
3.90.53.8
42.90.1
10.9
2,543.6
1953
71.815.8
1,207.9202.423.9
51.594.7
109.130.6
1.124.272.928.328.61.6
76.7
383.0
9.66.20.012.42.9
11.432.0
1.824.7
2,170.4
BHCb 1953
0.3
0.3
8.2
20.1
0.5c
0.7 c
0.1
30.2
Chlord.' 1953 Dield.a 1953
_- 0.1
_- 0.7- 3.5
1.4
1.5
0.1
3.0
7.8
12.6
0.1
24.8
* Consumption in metric tons.a Reduced to pure products, technical grade.b Reduced to gamma isomer.e Consumption is not commensurate with surface sprayed, but the figures provided by the terri-
tories have been preserved.
data for two neighboring localities used forcontrol purposes.
ANTIMALARIA ACTIVITIES WITH
IMAGOCIDES
House spraying with imagocides is theprincipal and decisive factor in the anti-
Cuba plans to make use of imagocides inits campaign to eradicate malaria.
Table 11 shows that DDT is the mostwidely used imagocide. By reducing theother insecticides to a dose equivalent to2 grams of DDT per square meter, the fol-lowing distribution, by percentage of sprayed
4'
l
16

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
surfaces, is obtained with: has given excellent results from an economic
DDT ................... 91.0% and technical point of view.BHC ................... 5.1% Table 12 shows that there is a tendencyDieldrin............. 63.% toward reduction of sprayings to one a year.Chlordane............... 0.3% Only the smaller countries continue to spray
The DDT dose utilized averages about twice a year. It would seem that this practice
Table 12.-Work with Imagocides (figures in thousands) in each Country and Territory, 1950-1953
Countries and Territories
Argentina ................Bolivia ..................Brazil ....................Colombia ................Costa Rica..............Cuba ....................Dominican Republic.....Ecuador ................E1 Salvador .............Guatemala ...............Haiti ...................Honduras................Mexico ...................Nicaragua ...............Panama ..................Paraguay ................Peru .....................United States............Venezuela ................
British Guiana ...........British Honduras ......Dominica ...............French Guiana ...........Grenada .................Jamaica .................Puerto Rico..............St. Lucia ................Trinidad .................
Total No.of houses in
area ofoperations
371.0
2,840.0483.2
78.4
228.8222.3153.2112.326.075.0
43.095.0
541.153.0
631.0
76.8
1.28.0
12.041.7
255.918.684.6
Number ofhousessprayed
regularly
147.6
2,415.7389.675.7
168.4187.9128.047.226.049.6
126.131.744.12.3
269.753.0
516.7
34.59.71.2
7.2
41.7
128.811.084.6
Per-centageof total
40
858197
74858442
10066
7446
5010082
45
10090
1005059
100
Totalsprayed
1953
210.931.8
2,724.9408.875.7
168.4204.2215.147.926.051.8
126.163.488.2
5.4269.753.0
877.3
34.519.41.27.2
83.4128.811.0
100.1
Frequencyof
sprayingsper year
1 and 21 and 21 and 21 and 2
2
11 and 2
21 and 2
1111122211
1 and 2
211221
1 and 21
o
6-126
6-126-126
126-126
6-12128
1284Y2
612126-12
612
66
126-1212
Area Scheduletreatedb estab-
lished?
yesyesyesyesyes
yesyesyes
yesyesnoyesyesyesno
yes
yesyesnoyesyesyesyesyesyes
a Every 18 months along the coast; every 12 months in the river areas.b Area treated: T = total; P = partial.
Itineraryesta-
lished?
yesyesyesyesyes
yesyesyesyesyesyesnoyesyesyesnoyesyes
yesyes
yesyesyesyesyesyes
2 grams per square meter, which has beenused since the very beginning and which inpractice has offered a margin of safety inthis work. Preparations of 75% wettableDDT powder are now the most widely usedthroughout the continent. The NMS ofBrazil is producing and using an 80 % DDTemulsifiable paste, which in the first trials
is the result of operating difficulties in thefield rather than of technical considerations.Over-all house spraying is carried out in allcountries, except in some areas of Argentinaand Paraguay, where it is limited to sleepingrooms and living rooms.
Almost all the countries and territories,with the exception of Mexico, Peru, and
17

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
RURAL AREAS (o
TOWNS (b
ELEVATED AREAS(b
INDEX (c100
80
Ist. CYCLE -USE OF DDT ONLY 2nd.CYCLE- DDT orBHC RECESS
SPRAYING SEASON
DURATION OF RESIOUAL ACTION
AUc. 1 SEPT. ocrT. | NOV. I DEC. I JAN. I FEB. I MAR. I APR. I MAY I JUN. I JUL.
OUT-PATIENT TURNOVERAND MOSQUITO CAPTUREDURING DECADE PRIORTO THE USE OF DDT
-OUT-PATIENTTURNOVERIN CLINICS
MOSQUITO
603-
40 -
20 -
o
¡
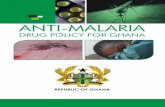
CHART A.-Antimalaria campaign schedule in Argentina
¡ AUG. SEPT. | OCT. | NOV. | DEC. | JAN. FE. MAR. | APR. | MAY | JUN. | JUL. ¡
18

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
Dominica, report that imagocide applica-tions follow a time schedule and an itinerary.Argentina submitted a table and an explana-tion of its time schedule, showing a strategicand economical method of field work; theseare considered of sufficient interest to bereproduced in this report (chart A). Thistime schedule reduces operating costs, sinceit is based on a practical approach that takesinto account the principal factors involved,i.e.:
(a) The epidemiology of malaria in north-western Argentina, where the outstanding char-acteristic is a period of non-transmission varyingaccording to latitude and elevation above sealevel. The chart shows the correlation betweenthe turn over of out-patients and capture ofadult anopheles, the curves having been plottedon the basis of data for the ten years prior to theuse of DDT.
(b) Availability of personnel and equipment.(c) Climate, since summer rains obstruct the
work in rural areas by making the roads impass-able.
transportation routes, and density of popula-tion. The number and type of vehicles avail-able in each country vary widely.
In almost all the countries, sanitary en-gineers participate in the field work, althoughtheir responsibility is not always the same.The countries in which they hold executivepositions are Argentina, Colombia, the Do-minican Republic, Peru, and Venezuela.
In countries where the malarious zone isextensive, the zone has been divided intodistricts, where various teams operate underthe direction of a chief. In the smaller zonesthe district coincides with the work area ofone team. The composition of the team isquite varied, depending principally on thetransportation facilities available. Motorizedteams comprise generally a chief, a driver,and a number of sprayers, varying accordingto whether the teams work in rural or urbanzones. The driver also acts as a sprayer, andin some cases the chief himself acts as driver.The composition of the motorized teams insome of the countries is as follows:
Assuming that in torrid zones the residualaction of DDT is of six months' durationand that of BHC three months' (250 mg.of gamma isomer per square meter), thefirst cycle is completed with DDT ex-clusively, starting with the lower and lessaccessible zones, where the population isfar away and widely scattered, and the entirehouse is treated. This is followed by partialtreatment of houses in villages and suburbanareas (sleeping rooms and living rooms),since the complementary action of partialtreatment of nearby houses is evident. Fi-nally, the higher and temperate zones aretreated, a return being made later to thefirst zones, but in this instance preferablyusing BHC, which is produced nationallyand permits a savings in foreign exchange;at the same time it acts also against theTriatomidae.
Table 13 shows the number and type ofvehicles available in each country.
The organization of field services, as statedin the previous report, depends on such localfactors as economic conditions, topography,
Country
Argentina ..........Bolivia .............Brazil ..............Colombia ...........Dominican Republic.Ecuador............El Salvador.........Honduras ..........Mexico .............Peru ..............Venezuela ..........
Chief
11111111111
i
Driv-er
11111
1
1
Auxi-liary
Sprayers staff
2 to 3 03 to 4 03 to 6 0
6 03 to 4 04 to 6 1
5 04 05 08 2
3 to 8 1
Besides the motor corps, there are otherteams that use several kinds of transporta-tion such as launches, beasts of burden,"trollies," etc., as well as those that travelsimply on foot. The number of sprayers,which is also very variable, ranges from 4to 11.
In Argentina, Bolivia, and Brazil thereare, in addition to the teams, so-called singlesprayers (the "zoning" method), who areassigned a fixed number of houses (varying
19

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
aceording to how widely scattered the housesare) which they cover systematically usingtheir own means of transportation, such asbeasts of burden, bicycles, etc. This work issupervised by special inspectors.
the characteristics common to the problemin all the countries, as well as the local con-ditions in each one, will it be possible todetermine what should be considered themost acceptable structure for the staff. This
Table 13.-Means of Transportation Available to the National Malaria Servicesin each Cosuntry and Territory
(According to data provided by those services)
Countries and Territories
Argentina ................Bolivia ...................Brazil .....................Colombia ..................Costa Rica ................Cuba.....................Dominican Republic.......Ecuador ...................El Salvador ...............Guatemala ................Haiti .....................Honduras ..................Mexico ...................Nicaragua .................Panama ...................Paraguay ..................Peru ......................United Statesb ............Venezuela .................
British Guiana.............British Honduras..........Dominica .................French Guiana.............Grenada...................Jamaica ...................Puerto Rico...............St. Lucia..................Trinidad ..................
Auto-mobiles
7
302
1
110011
1
1
Jeeps
185
16715
1
73
5
4
4
23
74
1
2
3
12
Station Pick-up Heavywagons trucks trucks
291
962461
208
20264
111739
17534
11
31725
451
1572
113
2
2
435
58
3
132638
Trailers
10
58
2
1
3
Laun- Air-ches planes
3312
3
1
241
17
1
1
11
4
Other
102 a
krTotal
11014
7105564
2622235
148
247
163
55293251
52184
13247
18
a Includes 2 tank trucks, 92 bicycles, 3 motorcycles with sidecars, and 5 canoes.b Many of these vehicles are loaned to the state public health services for insect-control programs.G 1 tank truck and 1 tractor.
It is impossible to present in this report acritical study on the organization of the staffthat carries out the field work, since theinformation requested allows only a descrip-tion of how such staff is constituted in thevarious countries. Taking into considerationthis description and the lack of uniformityin the composition of the teams, it is believedthat only by making special studies showing
aspect of the problem is undoubtedly one ofthe most important in the economie planningfor malaria eradication.
COSTS AND PRODUCTIVITY
Table 14 shows the direct costs of opera-tion that have been computed, taking intoconsideration the following four factors:(a) insecticides and solvents; (b) equipment
20
F
2e

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
and materials; (c) transportation; and (d) (quoted in dollars), is given below:field personnel.
Also appearing in this table is the per-centage ratio between the cost of field proj-ects and the budget of the service, a figurethat indicates the proportion of antimalariafunds invested directly in field work. Opera-tional costs are not "competitive" costs, tobe compared between countries, because of
s1 the intervention which in some cases is exer-cised by the State, for example, wvhen pur-
Country
Argentina ..........Colombia ...........Dominican Republic.Ecuador............E1 Salvador.........Honduras ..........Mexico .............Venezuela ..........Jamaica ............
Table 14.-Unit Costs and Yield of the Imagocide Campaign (figures in thousands)in each Country and Territory
Countries and Territories
Argentina ............Colombia ..............Dominican Republic...Ecuador ...............El Salvador...........Honduras ..............Mexico ................Nicaragua .............Panama ...............Perue..................Venezuela .............
British Guiana........Jamaica ...............Trinidad ..............
Total Operatingbudget of costs in
dthe NS nationalMS currency.
7,073.13,034.0
140.26,337.0
462.1160.0
2,176.5840.3157.4
3,743.814,387.1
163.660.1
305.8
5,485.51,887.3
118.13,162.2
607.2149.2
1,319.7826.5157.8
1,728.45,914.0
134.818.8
187.9
The countries and territories not appearing on this list failed to transmit data.Direct cost, excluding administrative personnel.
b The 60% includes material, equipment, and field teams.o Data for 1951.
chases of insecticides or equipment are madeat preferential exchange rates; because ofthe salary level established by the State;or because of the terms under which person-nel are contracted (permanent or temp-orary). Consequently, costs can be con-trasted only within a single country, bycomparing them in various years and places.
A comparison of the costs, per imagocideapplication, for the years 1949 and 1953
The above figures are only approximate,as the object has not been to make a studyof costs, but rather to promote interest inthe economic analysis of projects usingimagocides. The same comment may bemade with regard to unit productivity in
terms of man-hours per application, whichvaries greatly according to special circum-
stances in each country.
1949
1.714.000.921.20
1.580.950.822.450.53
1953
1.041.850.700.891.131.440.842.010.65
Percentageof Cost
o.
1314
94
Total d
spray-ing
210.9 1.04408.8 1.85168.4 0.70204.20.89215.1 1.1351.8 1.44
126.1 0.8463.40.9988.2 1.79
a
54111441537
54
,17
58i3
Per-cent-
age oftotal
budget
78628450
936098
1004641
823161
0
2738504356
402610
Operatingcosts indollars
219.4754.9118.1180.7242.9
74.6105.6125.2157.8115.3
1,765.3
79.352.7
110.5
DDTdose
per m2
and perapplica-
tion
2.122.092.002.002.001.983.202.002.602.102.00
1.502.002.00
o
o.2
pq
67633
13
135
911
GramsDDTper
appli-cation
353496306427538467578447335360606
358137320
Man/hoursper
applica-tion
1.851.661.041.75
0.95
1.86
1.30
1.52
Man/hours
perkilo-gram
ofDDT
5.23.33.44.2
1.7
5.5
2.1
5.5
60b15.5
3 34107.9 1.06137877.32.0137
11 3915 43
34.583.4
100.1
2.310.631.10
213756
14
5
566238
21
ii

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
PRODUCTION OF INSECTICIDES, SOLVENTS,
EMULSIFIERS, AND EQUIPMENT IN THE
VARIOUS COUNTRIES
In Argentina, a DDT plant that will havea basic annual production of 1,000 tons andwill use domestic raw material exclusively,is scheduled to start production late in Octo-ber 1954. With the opening of this plant,two countries of the Americas-Argentinaand the United States-will be producingthis insecticide.
Both Argentina and Brazil, in additionto the United States, produce benzene hex-achloride and lindane, without the need toimport any raw materials.
The NMS of Brazil, which has expandedits BHC factory, is now producing an ex-cellent 80% DDT emulsifiable paste, aswas previously mentioned, in addition toits already accredited emulsifier "B-13."
Argentina, Brazil, the United States, andTrinidad all produce emulsifiers, and all thecountries having petroleum industries pro-duce kerosene, which is used as a solventfor 5 % solutions.
At the present time, special sprayers areproduced only in Brazil and the UnitedStates.
RESULTS OF THE CAMPAIGN
The results of the antimalaria campaigncan be measured by: (a) partial or totaleradication of malaria in a country; (b)decrease or elimination of malaria mortality:(c) disappearance or reduction of morbidity(clinical cases); (d) reduction of antimalariadrug consumption; and (e) decrease in thesplenic and, above all, the parasite indices(concurrent surveys).
Eradication.-Four countries and twoterritories have reported that malaria hasbeen eradicated in some regions.
Argentina reports that it considers malariaeradicated as an endemic disease throughoutthe national territory. Nevertheless, in ac-cordance with the strict standard of theNational Malaria Society of the UnitedStates (namely, three consecutive years
without a single autochthonous case), ma-laria has been eradicated only in the prov-inces of La Rioja, San Luis, Córdoba, SanJuan, and Catamarca (with the exceptionof one department), in an area of 60,000square kilometers with a population of200,000 (this figure refers solely to the ma-larious departments of these provinces andnot to the total population). In accordancewith the same standard, Ecuador reportsthat malaria has been eradicated from themalarious regions in the inter-Andean prov-inces of Pichincha,, Imbabura, Carchi, andcertain parts of Guayas, with a populationof 220,000.
The United States indicates that endemicmalaria has been eradicated throughout thecountry, with the possible exception of Hi-dalgo and Cameron counties in Texas. Eradi-cation has been accomplished over an areaof 3,016,548 square kilometers with a popu-lation of 57,790,489.
Venezuela, also according to the standardof the National Malaria Society of theUnited States, reports that malaria has beeneradicated in 30 % of the malarious region,in the states of Anzoátegui (14 municipalitiesin the west), Aragua, Barinas (except forthe southern part of the three southeasternmunicipalities), Falcón (34 eastern munici-palities), Lara (20 eastern municipalities),Miranda, and the Federal District, in atotal area of 180,000 square kilometers anda net population of 1,538,449 (estimated onthe basis of the 1950 census).
With regard to the territories, BritishGuiana presents the most conspicuous ex-ample of eradication, not only of malaria butalso of its vector, A darlingi, in the threecoastal counties (Demerara, Berbice, andEsequibo), where 95 % of the population iscentered (442,000 inhabitants) in an ap-proximate area of 5,000 square kilometers.
Finally, Trinidad, although it gives nofigures or standard for evaluation, reportsthat malaria has disappeared in many dis-tricts.
French Guiana and Puerto Rico indicatethat, although they cannot as yet speak of
<4
22
"J

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
eradication, malaria is no longer endemic intheir territories.
Contrary to previous reports, Chile statesthat there is an eradication zone only in theprovince of Tarapacá, with an area of 15,000square kilometers and a population of 10,000,while it reports a population of 102,789protected by imagocides and antilarval meas-ures. It would thus appear that the A. pseu-dopunctipennis has not been totally eradi-cated in that country, as was indicated inthe IV Report.
Mortality.-Perhaps the least valuableof all the malariometric information avail-able is that obtained from mortality data,and there are various reasons to supportthis view.
In the first place, the malaria servicesnormally take no direct part in the registryof deaths, a function undertaken throughan independent system and, on occasion,without any direct connection with healthagencies. This situation gives rise to a start-ling paradox: malaria services are organizedto detect and verify cases of malaria, but notto verify the diagnosis in the case of death.When this occurs, the death is recorded asdue to malaria and, if the death certificateso records it, there is no further action. Sec-ond, it is well known that in countries wheremalaria was or is still endemic it is customaryto record many deaths of which the causeis undetermined as due to malaria. It is truethat during the past few years, because ofthe progress made in imagocide work, a
sr large number of well-informed physiciansno longer follow this practice, but even todayquite a few members of the profession stilldo so.
Another factor that tends to lessen thevalue of mortality data is the procedureestablished by some statistical offices ofclassifying as malaria deaths those causedby fevers in patients coming from malariousregions (International List of Causes ofDeath, Sixth Revision, 1948, No. 116), aprocedure that is no longer justifiable inadequately protected regions.
Finally, there is the fact that no country
has established an effective formula to de-termine whether deaths certified as due tomalaria are in reality due to that disease.
With the sole exceptions of French Guiana,which reported that the two deaths recordedas due to malaria in 1950 were confirmed,and of Mexico and Panama, which reported,without specifying how, that a part of thedeaths recorded had been confirmed, allother countries record death figures statingthat there was no confirmation of the diag-nosis for malaria. If the value of informationon deaths diagnosed as due to malaria isonly relative, of even less value is that wrhichcan be obtained from a study of the figuresfor deaths due to unknown causes, figuresthat are quite high in a majority of the coun-tries.
In spite of the difficulties mentioned, themortality figures for malaria bring out somequite important facts. Thus, in those coun-tries that provided information for 1952,out of a total of 1,013,815 deaths from allcauses in that year, 41,869 were presumablydue to malaria; that is, 4.1 of every 100deaths were caused by this disease. Of these41,869 deaths, 22,050 (52%) occurred inMexico. Countries that submitted mortalitydata are shown in table 15.
A study of the malaria mortality trendsin the countries that have given informationshows that in Argentina and British Guianathe rate reached zero. In Puerto Rico onlytwo deaths due to malaria occurred in 1953,and the figures for Costa Rica, El Salvador,Honduras, Nicaragua, Panama, Venezuelaand Trinidad show a sharp decline. Fromthe information provided by the remainderof the countries and territories, there is noclear evidence of a downward trend in thisspecific mortality rate.
As can be noted in table 15, there are stilla number of countries and territories inwhich from 5 % to 10 % of the total deathsfrom all causes are due to malaria.
Morbidity.-The record of patients is nobregularly kept in all countries and territories.Only Argentina, the United States, andPuerto Rico have submitted complete re-
23

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
ports; the rest have failed to include one ormore of the aspects covered by the question-naire.
With respect to autochthonous cases oc-curring in zones at present under treatmentwith imagocides, information has been sub-mitted by seven countries (Argentina, Co-lombia, Costa Rica, Mexico, Peru, the
reduction in 1953, as compared with thefigures for 1950; the same is true of BritishGuiana and Puerto Rico.
As to autochthonous cases occurring inregions where treatment with imagocideshas been suspended because it is consideredunnecessary, only the United States recordsthree cases in 1952 and three more in 1953.
Table 15.-Malaria Deaths in each Country and Territory, 1950-1953
Countries and Territories
Argentina ................Colombia ................Costa Rica ................Dominican Rep ...........Ecuador .................El Salvador ..............Guatemala .............Haiti ....................Honduras
b...............
Mexico ....................Nicaragua .................Panama ..................Paraguay .................United States............Venezuela .................
British Guiana............British Honduras..........Dominica .................French Guiana...........Grenada .................Jamaica .... ...... .........Puerto Rico...............St. Lucia ................Trinidad ..................
1950
Deaths Deathsall causesun-causes known
154,540160,378
9,76921,30314,39727,45461,2341,905
17,917418,43011,4667,169
7,5451,452,454
54,374
6,239
948465
1,05616,55621,917
1,1847,665
43,529356
5,412
6,9143,416
247
1,54224,959
452
2,14513,12924,247
445
75
8981,503
173
Deathsdueto
mala-ria
112,697
5712,1701,0251,7016,844
863,071
22,9662,961
2102976
219
6629152
45495
5748
141
1951
Deaths Deathsall causes
un-causes known
156,400 ...165,169 42,509
9,631 89221,731 5,14713,327 ..29,030 8,38156,550 1,4331,825 75
16,167 1,254458,238 27,53810,085 4466,652 ...8,278 1,851
1,482,099 13,38156,661 23,465
5,874 391801 ...870 ...422 ..
1,276 3117,233 96822,371 ...
1,3891 1297,8151 ...
Deathsdueto
mala-ria
93,091
4592,271
4821,5006,709
1063,900
24,681
1,58e200111
64145
317
20
61545
33116136
153,081153,738
9,90222,51516,20532,42371,9942,045
17,894402,54211,9566,774
57,085
6,037794
1,108466
1,25516,71720,504
1,2468,000
... No data available.a Deaths in hospitals only.b Data for fiscal year 1 July-30 June.e Provisional.
United States, and Venezuela) and fourterritories (British Guiana, French Guiana,Jamaica, and Puerto Rico). Others (Brazil,Ecuador, Guatemala, and British Hon-duras) report on the total number of hem-atological examinations made, without spe-cifying how many patients were subjectedto this test. The remainder give very frag-mentary information (see table 16). The onlycountry to record no autochthonous casefrom 1952 on is the United States. Argen-tina, Costa Rica and Venezuela show a sharp
With respect to autochthonous casesrecorded in areas that have never or onlyirregularly been treated, little informationhas been obtained. A decided reduction inthe number is observed in Argentina (epi-demic malaria zone), the United States andDominica. In the remaining countries thathave sent in reports, the extent of the prob-lem continues more or less unchanged.
On this occasion, information was re-quested also on non-autochthonous cases offoreign origin. Only Argentina, the United
24
1952 1953
"
Deaths DeathsDeathsal, causes
un-causes knownknown
Deaths Deathscauses due to
unknown malaria
Deathsdueto
mala-ria
02,873
2702,239
9711,3706,974
752,853
22,050976152
45
71
177
18
72415
10980
Deathsall
causes
160,450163,65310,31220,55116,05129,987
b
2,02418,859
11,3177,320
6,187
788413
1,08415,46517,9751,156
36,8731,3075,493
9,7662,229
102897
428
22,970
395
43671
1,83680
39, 112972
5,936
100866
409
22,476b
431
19
03,090
1891,709
717977
65
1,902
959130
34
60°
8
9O
45
29474
4
i

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT 25
Table 16.-Reported Cases of Malaria from all Sources in each Country' and TerritoryAccording to Type of Zone
-i~~~~~~~~ ~~~1950-1953
1950 1951 1952 1953
Counnries andTerrito ies Tot Total ttal Total Tsotal T Total ToT~~~~~~~otal % T, Total a/o
pi- ex al epati- x posi- patlci-
e- posi- efx- p. falci- . psents amina- tie p e amina tive ents tive ¡pa P amina P. pation ve tions erui tions ti rum e na . ...
Autochthonous cases occurring in zones being treated with imagocides
Argentina.......... 1,561 1,56 100.0 1.5 1,188 1,188 100.0 2.4 652 652 100.0 4.7 439 439 100.0 1.1Brazil ........... . . 104,677 6.6 26.4 . 15,786 2.7 17.4 165,033 3.1 21.0 .. 20,755 2.6 21.5Colombia ............ 73,057 64,78 75,513Costa Rica ......... 20,34 20,934 5.3 0 21,370 21,370 6.3 0 13,049 13,049 5.4 0 7,640 7,840 4.2 0
Dominican Rep...... . ... ... 6,626 23.9 66.6Ecuadorb .... .... 23,898 1. 47.3 34,598 1.9 61.2 ... 36,289 1.1 74.9 40,45 3.6 50.8Guatemala .......... ... 12,601 17.1 76.6 ... 10,088 10.0 58.0 .. 10,498 5.6 43.4 .. 11,552 4.0 52.4Mexico.............. 1,155 1,15 19.7 15.0 513 513 48.5 2.8 1,100 1,100 30.6 1.2 1,634 1,634 35.8 3.1
Paraguay ......... . ... . ... 876 ... ... 404 ... ... ...
Per ................ 12,262 . 11,763 ... . . 11,142 . . ... 11,448 .
United States ..... 1,810 1,000 0.6 16.4 13 13 62.0 12.5 0 0
Venezuela ........... 40,185 18,864 12.4 11.2 31,490 20,364 11.8 16.6 25,006 31,310 8.6 15.8 21,359 32,518 6.8 9.8
British Guiana ...... 3,183 6,360 1.6 84.0 1,854 5,709/ 5.8 85.6 1,135 4,2991 1.6 86.5 1,055 4,355 0.7 93.3British Honduras.... .. 2,758 10.4 0 ... 1,740 8.9 0 ... 823 4.2 65.7 ... 754 3.4 0French Guiana..... 1,20 1,920 8.6 71.0 4,004 4,004 1.0 89.0 2,866 2,866 0.5 85.0 997 977 1.1 90.0Jamaica ............. .. .. .. 6,592 809 15.6 86.6 9,943 2,562 28.6 96.0 16,161 10,674 31.0 94.9Puerto Rico ......... 7314,043 0.3 5.1 84 5,914 0.3 26.7 18 3,658 1.1 66.7 7 701 0.4 0
St. Lucia........... .. ... .. .. .. .. .. .. .. 3,225 1,658 4.6 77.9
Autochthonous cases occurring in zones where treatment was suspended because deemed unnecessary
United States . ...... ... ... ... ... ... ... ... ... 3 3 66.6 0 2 2 50.0 0
Autoclihthonous cases occurring in zones never or only irregularly treated
Argentina0
.......... 401 401 100.0 12.0 145 145 100.0 0 1 46 46 100.0 0 60 60 100.0 0
Colombia ... . 5,423 .. . .. 13,080 9.,195 .. 10,346. ...Haiti.............. 1,944 21,879 27.0 0 78,57 25,011 24.4 0 74,024 24,116 25.4 0 62,771 26,47 25.8 0Paraguay .......................Paraguay ............ 6,881 ... - . 13,717 ... 8,043 . 6,532 . .Peru....... 7,795 . .. 6,061 .. 6,596 . 5,61United States ....... 208 .... 0 . 7 7 100.0 0 48 48 66.6 0 30 28 100.0 4.0
British Guiana... . ....... .... . 49 49 100.0[ 69.5
Dominica ............ 1,8251 551 13.8 75.0 1,328 391 19.4 80.3 868 696 20.2 61.0 546 451 4.0 66.7Jamaica ............14,201 2,745 18.3 92.0 15,693 7,221 12.5 88.8 10,167 4,693 34.8 97.2 9,23 5,2 37.2 96.5St. Lucia............ 6,141 1,310 15.4 58.9 6,571 1,354 8.6 53.8 6,234 1,860 6.7 78.4
Trinidad........... ... 3,004 70.2 75.0 ... 2,064 18.8 83.6 ... 1,775 30.6 80.0
Non-autoclitbonous or imported cases
Argentina .. 5 5....... 100. 041 100.0 2.4 100.0 0 8 8 100.0 0.. 4 6 1000 ...18United States. 209 . 11. 0 12,970 . . . 10,000 ...... 1,36...
Puerto Rico ... 4 .... .. 110 ... ... 21 ...
... Data not available.a Percentage over total positive tests.b There is no case register; investigation for malaria in all febrile diseases.
. Only in zones of epidemie malaria.

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
States, and Puerto Rico have replied to thisquestion. In the United States and PuertoRico the majority of the cases were observedamong civilian or military personnel comingfrom the Far East. The United States alsorecorded cases of Mexican origin. In Ar-gentina the cases in question were traceableto Bolivia and Paraguay. Argentina statesthat the cases listed include only those forwhich unquestionable epidemiological docu-mentation is available, though it is esti-mated that the real number of such cases ismuch higher, some undoubtedly being in-cluded among those reported as autochthon-ous.
It is significant to point out, by way ofgeneral comment, the lack of developmentof the case registry systems in most of thecountries and territories, and the need forestablishing standards and methods to en-sure the effectiveness and uniformity ofsuch records with a view toward stricterevaluation of antimalaria campaigns, es-pecially if eradication is the objective.
Consumption and Distribution of Drugs.-Six countries (Argentina, Brazil, Colombia,Ecuador, Mexico, and Nicaragua) and fourterritories (British Guiana, Dominica, St.Lucia, and Trinidad) have replied to thequestionnaire with regard to the quantitiesof antimalaria drugs distributed as cura-tives.
From a study of the information given intable 17, it can be seen that there is no defi-nite tendency toward a specific type of medi-cation. In the past four years some quininehas still been used (especially in Mexico,Nicaragua, and St. Lucia), together withconsiderable quantities of atebrin (Colombiaand Mexico). There is no doubt that in re-cent years paludrine and, particularly, chlo-roquine have occupied a preferred placeamong the antimalaria drugs distributed bythe NMS.
The question of the drugs used in malariacontrol deserves special study, since theinformation obtained is too incomplete topermit a valid appraisal of the situation.Apparently, judging from the information
received, no reasonably adequate record ofthe use of these drugs is kept in the maj orityof the countries. Besides, it would seem that,in some, the policy followed before the intro-duction of imagocides still prevails, that ofindiscriminate distribution of curative anti-malaria drugs to unprotected populations,thereby obscuring or distorting the means ofevaluating the results of present-day cam-paigns. Moreover, the opportunity is lost forthese drugs to be of use as a means of de-tecting cases of malaria not reported at theproper time.
Parasite Surveys.-These surveys havebeen classified in this report according toconditions in the various zones with respectto malaria control, as follows: (a) zones inwhich anti-anopheles measures continue tobe applied regularly (concurrent evaluationsurveys); (b) zones where malaria is con-sidered eradicated; (c) zones where anti-malaria measures are not taken or have beentaken irregularly (exploratory surveys);and (d) zones where drugs are utilized asthe only regular method of control (not ascuratives).
Table 18 shows that Argentina, Bolivia,Brazil, Colombia, Costa Rica, the Domini-can Republic, Ecuador, El Salvador, Nica-ragua, Panama, Peru, Venezuela, FrenchGuiana, and Jamaica carry out evaluationsurveys regularly. Honduras began themin 1952.
Only Argentina, Ecuador, and BritishGuiana carry on surveys in zones wheremalaria is considered eradicated, and Vene-zuela, while furnishing no data, is known todo the same. Only three territories (Jamaica,St. Lucia and British Guiana) report sur-veys where no antimalaria measures aretaken.
Brazil is the only country that has madesurveys in zones where antimalaria drugshave been used, experimentally, as a controlmeasure (not as curatives).
It would appear, therefore, that Cuba,Guatemala, Haiti, Mexico, Paraguay, theUnited States, Dominica, Grenada, andTrinidad do not conduct surveys regularly,
26
,X

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
Table 17.-Antimalaria Drugs (in grams) Distributed as Curatives; and Persons Treatedin each Country and Territory, 1950-1953
Countries and Territoriesa
Argentina ...............
Brazilg ..................
Colombia ................
Ecuador .................
Mexico .................
Nicaragua ...............
British Guiana ...........
Dominica ...............St. Lucia ...............
Trinidad ................
Year
5051525350515253505152535051525350515253515253
50515253535051525350515253
Quinine
4,0641,397
544752
88,55074,090
153,30066,2501,9925,8164,372
14,84823,040
1,07551
Atabrineb PqUlasmo-quinob 1 Paludrine
6,1951,0901,709
914
57,30519,078
5,849
680
32,82420,54730,91326,607
9232,1663,650
1,4161,3461,432
867
1,7501,5001,300
950
9101711
1,00048,00025,000
180975
700
2,207710808207
1,224
2,058
1,2901,380
99,64296,492
137,80662,574
3,00028,50066,5004,000
1,0403169350
a Only reporting countries and territories.b Or synonyms.e Guanatol.d Guanatol and nivaquine.e Guanatol, nivaquine, and camoquin.' Camoquin.g Brazil reports, in addition, having distributed 14,464,708 treatments of chloroquine during the
four-year period, without indicating the amount of the drug.
while Puerto Rico did undertake them until age group, these are: Bolivia, the Dominican1951. Republic, Honduras, Peru, French Guiana,
Of the fifteen countries and territories and Jamaica, for the school-age group, 6-15that carry on evaluation surveys, seven con- years; and Costa Rica for ages 0-14 years.duct them through investigations in a single Only two nations use two age groups as the
Chloro-quineb
3,9411,102
1751,098
24,0812,839
18,994
7501,250
12,0177,9527,6127,700
4,200800
Personstreated
1,890939403624
1,025,063980,829
1,070,3691,027,529
181,283138,487235,467338,495
4,162362
7,1993,803
110,86896,29276,20575,784
1,1141,0161,141
577
6,1416,5746,2343,225
Othermedications
21,5880
27,972,63,891d
135,869,
14,880
8,520
44,700
99,7506,000
6
27

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
basis of the surveys: Argentina, which uses age groups: Brazil, Colombia, El Salvador,the age groups 0-2 and 6-15, and Ecuador, Nicaragua, and Panama, all of them takingwith those under 5 and over 16 years of age. the groups of under 5 years, from 6 to 15
There are five countries that take three years, and over 16 years of age. Finally,
Table 18.-Malariometric (Parasitological) Surveys in each Country andTerritory, According to Type of Zone
1950-1953
Countries and Territories
1950 1951 1952 1953
Persons %. % Pos o ne . . [ % Persons ¡
x Persons 1 95
ersons positive fal-sitie falci- e positive falci- edo st veeam- blood exam. bid a1 e 'dined Pa- ined s exam- blood p exam- blod
tesis ruc tests ruman tests rma tests
In zones where regular anti-anopheles measures continue to be applied
Under 5 yearsArgentina ..........Brazil ...............Colombia ...........Costa Ricab .........Ecuador .............El Salvador..........Nicaragua ..........Panama .............Venezuela c ...........6-15 yearsArgentina ..........Bolivia .............Brazil ...............Colombia ............Dominican Rep......El Salvador.........Honduras ............Nicaragua ..........Panama .............Peru ...............British Guiana.......French Guiana.......Jamaica ............16 years and overBrazil ..............Colombia ............Ecuador..............El Salvador .........Nicaragua ..........Panama ............
10,53414,8031,889
10,619540
3611,078
18,008
57,30613,65636,1544,0406,221
10,308
3,7878,895
17,117
3,6631,125
3,4341,488
23,298659
1,6331,273
In zones where malaria is considered eradicated
Under 5 yearsBritish Guiana ....... 1,8906-15 yearsArgentina .......... 16,823British Guiana ....... 6,24316 years and overEcuador ............ 956
0.1
O0.3
6.7
100.0
100.0
16.9
3,0612,799
1,011
o0.6
2.0
90.0
4.7
3,7791,484
526
0 1- 4,4220.5 100.0 1,404
1.1 453
falci-pa-
rum3
10,2185,720
36210,4284,096
909538
1,30429,184
66,1056,106
19,6022,7901,4151,6434,5781,5147,7792,751
O0.59.42.10.542.64O1.59.0
0.013.020.48.97.73.410.980.130.70.73
01.11.8
12.30.74
7.200.8
11.4
0.043.60.92.64.503.30
5.680.50.05
0.327.1
1.34.81.82
40.85.140.9
11,2865,839
20527,5204,7947,201
4761,642
31,469
60,0846,629
17,9381,8671,1083,375
9401,059
10,14626,544
02.53.44.30.251.6(
2.67.1
0.024.51.61.23.42.010.3101.60.79
13.638.231.075.0
3.833.312.2
12.310.647.675.473.0
1.942. 322.22
9192.6
22.752.847.7552.0
2.458.3
8,91911,146
27512,6883,756
762629
22,090
56,80412,08235,1303,3382,1974,582
3,1666,720
18,477702130
3,256
7,44913
30,8424,046
1,5181,006
O0.68.76.60.13
2.602.2
10.0
0.014.60.53.65.63.58
3.750.60.103.0
23.9
1.1
15.42.08
25.18.11.0
23.912.532.320.0
057.117.7
26.225.620.273.553.0
O52.533.3395.0O
85.4
33.350.062.3045.90
45.4
26.528.263.6462.5O
45.016.6
13.034.520.275.248.242.30
27.225.00
95.2
26.116.075.7644.250.044.4
59.111.141.141.6728.7O
34.810.4
24.217.64.5
63.114.733.3o
38.432.70
094.7
39.6
50.9623.90
30.0
1,0021 18.73,389 0
893 17. 1
2,910360
32,1935,984
156869
0.86.91.23
17.52.561.0
5,278158
35,66511,000
5771,307
4.11.94.106.7O1.5
0
0.6
28
I
?·

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
Table 18.-Continued
1950 1951 1952 1953
Countries and Territories Persons Perss eronosive % esOp Persons % eoiveexam- os itivef f alci-e falci- ea ostv falc- eam positive
ined blood upa- exm ood pa- p ned es ra- P blood"ed tests a in tests ruW, tests run e tests"/ I~~~~~~tet
falci-pa-
ruma
In zones where antimalaria measures are not applied or are applied irregularly
4-10 yearsSt. Lucia ............ 2,603 75.36-15 yearsBritish Guiana....... - - - 156 9.0 86.0 47 0 112 41.0Jamaica ............ 74 6.7 100.0 2,271 20.8 83.3 3,199 38.31 95.0 4,171 20.2
a Of the total positive blood tests.b Age group 0-14 years.a All ages.
Venezuela uses all ages as the basis of thesurveys, without preference for any one.
The number of persons examined in 1953(all ages and all zones), the relations of thisnumber to the population of the malariouszone, and the parasite indices are as follows:
Countries andterritories
Argentina ..........Ecuador ............Venezuela ..........Brazil ..............Costa Rica.........Peru ...............El Salvador.........Panama............Bolivia ............Jamaica............French Guiana......Colombia ...........St. Lucia...........Nicaragua..........British Guiana......Dominican Republic.Honduras ..........
Proportionper
thousandof popu-
lation in thePersons malariousexamined zone
75,79240,91231,46929,05527,52026,54021,87613,095
6,6295,0643,3892,2312,6032,1121,5121,108
940
40.823.18.71.19.28.0
17.126.012.02.4
100.00.3
30.01.83.21.02.2
Per-cent-age
posi-tive
0.013.67.22.34.30.84.21.77.01.9o3.07.5o3.03.40.3
From the above it will be noted thatArgentina, Ecuador, and Venezuela occupy
the first three places in number of personsexamined, but in the ratio of this number tothe population of the malarious zone thefirst places go to French Guiana (100 perthousand), Argentina (40.8 per thousand),and St. Lucia (30.6 per thousand).
From a study of the parasite indices shownby the surveys, it can be seen that the coun-tries achieving the best results are FrenchGuiana (0 %), Nicaragua (0 %), Argentina(0.01 %), Honduras (0.3 %), and Peru(0.8 %). In previous years the indices forBrazil were lower than for 1953, the ex-planation being that, instead of repeatingthe surveys in the same localities, it waspreferred to carry them out in regions wherecases of malaria were reported.
The percentages of infection with Plas-modium falciparum, among the total positivehematological examinations, were the follow-ing in 1953: (a) in zones where regular anti-anopheles measures are applied: Jamaica,94.7; Dominican Republic, 63.1; Ecuador,49.8; Costa Rica, 41.1; Panama, 37.1;Bolivia, 34.2; Honduras, 33.3; Peru, 32.7;Brazil, 29.9; El Salvador, 24.6; Venezuela,10.4; Colombia, 5.1; Argentina, 0; Nicara-gua, 0; and French Guiana, 0; (b) in areaswhere no antimalaria measures are applied:Jamaica, 90.8; British Guiana, 85.0; andSt. Lucia, 72.4.
72.4
85.090.8
29

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
Table 19.-Plans for the Control of Malaria in the Future in each Country and Territory
(Information from the National Malaria Services)
Countries and Territories
Argentina ..............
Bolivia ...............
Brazil ..................
Colombia ..............
Costa Rica.............Dominican Republic...
Ecuador ..............El Salvador............
Plans for the Future
Reorganize the service toachieve total malariaeradication.
Extend malaria control tothe major part of malariaareas in the country.
Extend DDT application.Chloroquine distributionin sparsely settled areas.Malaria eradication in cer-tain areas.
Eradication. Spraying600,000 more dwellings inuntreated regions.
Eradication.Continue present campaign
covering entire malariazone in the country.
EradicationExtend treatment to entire
malaria zone.
Guatemala ............ Eradication.Haiti ................. Increase areas under
Honduras ..........
Mexico .............
Nicaragua .........
Panama ............
Paraguay ..........
Peru ...............
treat-ment.
Extend treatment areas untilentire malaria zone iscovered.
Malaria control throughoutthe country. Yellow feverprevention.
Training of personnel (espe-cially microscope techni-cians) and purchase ofequipment for laboratorydiagnosis.
Extend DDT applicationzones and construction ofdrains in important towns.
Extend DDT applicationzones. Organization of en-tomologic laboratory.Study of malaria situationin the country.
Extend area treated withimagocides. Eradication invalleys bordering withChile.
Advisabil-ity of
Coordinat-ing Activi-ties with
NeighboringCountries
yes
yes
yes
yes
yesyes
yesyes
yesyes
yes
yes
yes
yes
yes
Is Economic (E) or Technical (T) Aid orCooperation Desired?
E
yes
yes
yes
yes
yesyes
yes
yes
yes
T
yes
yes
yes
yesyes
yesyes
yesyes
yes
yes
yes 1 yes
yes
yes
yes
Remarks
Information on malariasituation in neighbor-ing countries.
Collaboration of an en-tomologist. Provisionof equipment andvehicles.
Fellowships for trainingkey scientific person-nel.
Coordination.
One malariologist andone entomologist.Material and equip-ment.
Provision of materials.
Personnel trained inmicroscopy and ento-mologists.
Equipment and mate-rials.
Equipment and insecti-cides.
Transportation equip-ment and insecti-cides.
30

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: Y REPORT
Table 19.-Continued
Countries and Territories
United States..........
Venezuela ..............
British Guiana.........British Honduras......
Dominica .............
French Guiana ........
Grenada ..............Jamaica ...............Puerto Rico............
Santa Lucia............
Trinidad ...............
Plans for the Future
None.
Control of other vectors, es-pecially flies.
None.Drainage work in town of
Belize.Insect-control program in
collaboration with WHO.Treatment of immigrants in-
fected with Plasmodium.
Epidemiological studies.Increase of bilharziasis con-
trol and eradication ofAedes aegypti.
Continuation of DDT spray-ing work.
Land fills and leveling op-erations in Piarco and con-struction of seaheads.
Advisabil-ity of
Coordinat-ing Activi-ties with
NeighboringCountries
yes
yes
yesyes
no
yes
yesno
yes
yes
Is Economic (E) or Technical (T) Aid orCooperation Desired?
E
yesyes
yes
yes
T
yes
yes
yes
yes
yes
yes
yes
Remarks
Continued informationon malaria situationin the continent.
Training fellowships forpersonnel and visitsby experts.
Not immediately.Loan of technical per-
sonnel.
Facilities for trainingpersonnel.
Visits by experts. Fel-lowships.
PLANS FOR THE FUTURE
A study of the replies from each countryon their plans for the future, which appearin table 19, is highly interesting.
Argentina, Brazil, Colombia, Costa Rica,Ecuador, Guatemala, and Peru report over-all or partial programs for the eradication ofmalaria. In a supplementary report, Cubaalso mentions an eradication program.
Bolivia, Brazil, El Salvador, Haiti, Hon-duras, Mexico, Panama, and Paraguay de-scribe plans to expand the control and treat-ment zones.
Mexico, Venezuela, Dominica, and PuertoRico state specific plans to intensify thecontrol of other vectors, particularly thehouse fly and the Aedes aegypti.
French Guiana, as a step forward, stressesthe treatment of immigrants infected withPlasmodium. This objective should be given
emphasis as an initial step toward consider-ing malaria in the future as a quarantinabledisease in those countries that have alreadyeradicated the causal agent.
Concerning the advisability of coordinat-ing activities with neighboring countries,seventeen countries and six territories re-plied in the affirmative. Two territories,Dominica and Jamaica, replied in the nega-tive; Mexico and Puerto Rico failed to replyto the question.
Twelve countries and four territories de-sire economic aid or collaboration. Fifteencountries and five territories indicate a de-sire to receive technical aid or collaboration.
The types of assistance the countriesconsider most necessary are: equipment andmaterials; fellowships and other facilitiesfor training personnel; loans of technicalpersonnel, particularly entomologists; andvisits by experts.
31

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
Two countries (Argentina and the United
States) requested collaboration in the formof information on the status of malaria inthe continent, a request that emphasizes theimportance now given to the malaria situa-tion in other countries.
The following conclusions were derivedfrom a study of the information obtained onthe plans of the various countries:
(1) A number of countries are alreadyplanning programs for the eradication ofmalaria.
(2) Several countries feel that they haveovercome the problem to the point wherethey are planning an expansion of activitiesto include other phases of control measuresagainst other insect vectors.
(3) The other countries and territoriesin the hemisphere, with two exceptions,favor the coordination of activities, a factthat points to the general conviction thatthe malaria problem in one country can becontrolled but not entirely eliminated unlessjoint action is carried out among neighboringcountries, to eliminate the possibility ofreinfection.
(4) Collaboration or aid provided to thedifferent countries to enable them to pursuetheir own antimalaria programs, or to inte-grate them in a continental program, shouldbe divided into four well-defined forms: (a)information and coordination; (b) facilitiesfor training personnel; (c) provision of equip-ment and materials; and (d) assignment oftechnical personnel and visits by experts.
NEED FOR A COORDINATED PLAN FORERADICATION OF MALARIA IN
THE AMERICAS
The latter part of the IV Report on thestatus of the antimalaria campaign, pre-
sented four years ago, discussed the technicaland economic possibilities of coordinating aplan for the eradication of malaria in theAmericas. In considering these possibilities,various aspects-epidemiology, organiza-
tion, technical assistance, and cost of an
over-all program--were analyzed and finallysummarized as follows: five years after the
introduction of DDT, two countries (Ar-gentina and the United States) had almostsolved their endemic malaria problem; twoothers (Brazil and Venezuela) were on theway to an early solution; and a fifth country(Ecuador) was vigorously pursuing the samegoal. These five countries accounted for75 % of the dwellings in the malarious regionof the continent; and the programs startedin Central America and other countries withthe aid of the WHO/PASB and UNICEFwould reduce the remaining figure to only20% by the beginning of 1951. There wastherefore a well-founded hope that the bal-ance could be covered in the ensuing fiveyears.
Shortly before the end of the five-yearperiod, a new estimate showed that 22 % ofthe inhabitants of the malarious zones arestill without protection. It is therefore evi-dent that the rate of progress achieved inthe five-year period, 1945-1949, has slack-ened.
There are four apparent factors to beconsidered in this situation:
(1) The decline of interest and concernas regards malaria, because this disease hasceased to be the public health, economic,and social scourge it once was.
(2) The lack of financial support to ex-pand the programs, and, in some countries,even the curtailment of funds previouslyallotted for this purpose.
(3) The weakening of the intellectual"drive" to solve the problem, on the partof experts responsible for the campaign,which began after the unexpected successof the first operations had been confirmedand, especially, when field work became amonotonous and uninteresting routine.
(4) The assumption of additional respon-sibilities by the NMS, particularly hetero-geneous activities, which led to a dispersionof efforts and a lowering of the quality ofantimalaria work.
If these four negative factors meant nomore than a delay in the program to extendthe antimalaria campaign to the whole con-tinent, there would be, perhaps, no sub-
32

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
stantial reason to alter the policy of "pa-tience and perseverance." However, twoother extremely serious factors have ap-peared during the period in question: a re-sistance to DDT in some anopheline vectors,in different parts of the world, and another-no less serious-the reluctance of officialsresponsible for the disbursement of publicfunds, who seem less and less inclined toincrease or even to maintain allotments fora campaign that, both socially and politi-cally, would seem to have lost in timeliness.
The appearance of resistance in the ano-pheles was foreseeable, in view of what hap-pened to the house fly and to other insectsharmful to agriculture. It wvas merely a ques-tion of determining under what circum-stances and when this phenomenon wouldoccur under natural conditions. The studieson the A. sacharovi in Greece unmistakablydemonstrated the capacity of this species toacquire, after several years of exposure toDDT, a physiological resistance abetted bythe concurrent application of the same prod-uct as a larvicide. The same situation hasoccurred with the A. quadrimaculatus insome regions of the United States. The ex-pectation of neutralizing this resistance byalternating imagocides provides only a truce.Since all these substances (those of prolongedresidual action) belong to the same chemicalfamily (chlorinated hydrocarbons), it isreasonable to suppose that the same resultwill be obtained with the anopheles as withother insects which, on acquiring resistanceto any member of the family (DDT, BHC,chlordane, dieldrin, etc.) develop at the sametime a capacity to acquire resistance againstthe rest of the family much more quickly.
Observations on the A. albimanus in Pan-ama show a yet more serious type of resist-ance; namely, that of changes in behavior(behavioristic resistance) which make theinsect capable of eluding to some extent thesurfaces on which the imagocide has beenapplied. Although no specific studies havebeen made on this subject, four countriesand three territories have reported observingthe presence or increase of anopheline vectors
in houses that have been sprayed, or somechanges in the vectors' behavior. If there areno other confirmations of well-establishedresistance, it is probably not because suchresistance does not exist to some degree,but rather because no precise investigationshave been carried out, or because in mostcountries the time period required beforesuch symptoms start to appear has not yetelapsed.
Very little imagination is necessary, then,to determine the prognosis of malaria in thecontinent in future years, when DDT andother insecticides begin to lose their "vir-tue," unless the sources of infection areeliminated by that time. To support thisview, it is appropriate to quote a paragraphfrom the 1953 Annual Report of the Direc-tor-General of WHO:
... the fact that in some countries in 1953 thelocal malaria vectors had developed DDT re-sistance after several years of spraying cam-paigns suggests that programmes of malariacontrol for a country or group of countries shouldbe planned so that the application of the insecti-cides could be withheld before the time whenresistance might develop (never less than fiveyears, so far as has been reported). Obviously,when malaria transmission has ceased, this doesnot imply that the anopheline vector species hasbeen eradicated; indeed, the anopheles densitymay even be nearly as high as before control. Ifsubjects carrying malaria parasites come intothe country, the transmission may be startedagain, but the danger would decrease in directproportion to the number of neighbouring coun-tries from which malaria was also eradicated.When active malaria control is interrupted, itwill have to be replaced by a policy of defenceagainst the reintroduction of malaria, and theprevention-or immnediate suppression-of trans-mission. For this purpose, it will be necessary toensure the adequate and immediate notificationof new cases of malaria and the decentralizationof facilities for diagnosis and for epidemiologicalresearch; and, in case of an epidemic it may benecessary to resume the insecticide spraying(which is why the campaign should be withlheldwhen the insecticide is still active on the vectorspecies) and the use of chemotherapeutics.
33

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
The other resistance mentioned pre-viously, that of those administering publicfunds, has already begun to appear in sev-eral countries in which malaria has lost thepower to attract the attention it previouslyevoked when it produced such disastrouseffects. Thus, it is also of the greatest im-portance to eradicate all sources of infectionbefore this type of resistance has becomedeeply rooted.
As a bright side to the dark picture givenabove, some events have taken place thatshould be pointed out and discussed.
(1) Four countries and two territorieshave demonstrated that malaria can beeradicated and that this possibility impliesimmense public health, social, and economicbenefits, the latter being all the more ob-vious when the point is reached where opera-tions can be suspended or discontinued.
(2) Seven other countries indicate asgoals for the future the development of totalor partial eradication programs, a fact thatdemonstrates the mature and widespreadawareness of the need for eradication nowexisting in the Americas. This is in sharpcontrast to the aspirations of little less thanten years ago, when the NMS still spokeof the "sanitation" of given localities, whichrepresented mere pinpoints of conqueredterritory on the malaria map of the country.
(3) A revolutionary change has beenbrought about in the position of malaria inthe field of international health. Until lessthan a decade ago, the assumption was thatmalaria constituted a local problem, one ofpurely local importance that should be ap-proached and solved by means of local for-mulae. At present, this problem and itsrepercussions, now beyond the sphere ofnational concern, have become a problem ofinternational proportions. Two countrieshave already shown their interest by keepingup-to-date with the epidemiological situationof the rest, a trend observable in the caseof plague, cholera, or smallpox at; the be-ginning of this century. And one territoryhas announced its intention of keeping aparasitological check on immigrants. The
word "imported" already figures in malaria.terminology, and it is logical to foresee thatcountries that have eradicated the disease,or are in process of doing so, will find thatthey are obliged to protect themselves bydemanding from persons entering the coun-try certificates attesting that they comefrom immune regions, or by imposing com-pulsory treatment.
(4) New residual-action insecticides havebeen discovered, improved knowledge ofthe qualities and failures of those in use hasbeen obtained; and it is possible to determinewhich insecticide is most suitable and inwhat manner it should be applied in accord-ance with the bionomics of the vector, theenvironmental conditions under which trans-mission takes place, and the economic factorspresent.
(5) New drugs have appeared and nevwmethods of treatment and of chemical pro-phylaxis (chloroquinated salt) have beentested, by means of which not only a radicalcure is possible but also the prevention ofnew infections in communities covered bymass prophylaxis programs.
(6) New and more accurate knowledge ofthe epidemiological situation of malaria inthe various countries and territories hasbeen acquired, and tactical and strategicalmethods of achieving eradication have beenperfected. It can therefore be asserted thatan "eradication technique" is now available.
(7) Seventeen countries and six territorieshave declared themselves in favor of thecoordination of activities in the antimalariacampaign.
To summarize: There is noNws an awarenessof the need for malaria eradication in theAmericas, as well as a general desire to co-ordinate activities on the regional or zonelevels; and better means of waging the cam-paign and improved working techniques havebeen discovered. Yet with all this, there isthe risk of losing all these gains if we do nottake advantage and make adequate use ofthem now. This is a serious responsibilityfor the present generation.
Should a decision be taken to coordinate
34

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
a continental plan for the eradication ofmalaria in the Americas, the folloNwing sug-gestions are formulated:
1. At the national level:
(a) To reorganize the NMS, entrustingthem with the entire responsibility for theantimalaria campaign and equipping themwith technical and administrative personnelto carry out nation-wide eradication pro-grams.
(b) To ensure the necessary financialresources to permit coverage of the entirecountry.
(c) To promote adequate coordination ofactivities among all the medical care andpublic health services, to ensure accuraterecording and identification of malaria casesand direct reporting to the NMS.
(d) To enact up-to-date antimalaria legis-lation, establishing as basic provisions: au-thorization to the public health service tospray imagocides inside dwellings; immediatereporting to the NMS of deaths due to ma-laria; immediate reporting of clinical casesand their parasitological confirmation onthe basis of compulsory blood tests; andadequate treatment (radical cure) of thepatient or carrier.
(e) To make it possible for the personnelof the NMS to attend advanced trainingcourses and international meetings of theheads of NMS.
(f) To provide training facilities for tech-nical, auxiliary, and field personnel comingfrom neighboring countries.
2. At the continental level:
To embody the decision of the countriesin the form of an agreement, with definitepronouncements on:
(a) Objectives: over-all campaign; eradi-cation; prevention of the exportation ofmalaria.
(b) Means of achieving these objectives:coordination; cooperation; information;technical and economic assistance.
(c) Responsibility of the Pan American
Sanitary Bureau for the preparation, pro-motion, and supervision of a coordinatedplan for the eradication of malaria in thecontinent.
3. In the international organizations (WHO/-PASB):
(a) To provide, to those countries thatrequire it, technical assistance for the or-ganization of their NMS and for the prepa-ration of operational plans, over-all or pro-gFessive, to permit effective action as regardsboth area covered (breath) and exhaustive-ness of the coverage (depth).
(b) To promote collaboration at the re-gional level by means of agreements betweenbordering countries or groups of countrieshaving common interests.
(c) To encourage economic participationby other international organizations inter-ested in similar or related objectives.
(d) To standardize and distribute, on apermanent and periodic basis, comprehensivereports on the malaria situation in eachcountry or territory, and on operationaldevelopments and the results obtained interms of public health.
(e) To select and distribute on a perma-nent basis, technical and scientific informa-tion on activities and developments of prac-tical interest in the antimalaria campaign.
(f) To organize regional meetings of thoseofficers responsible for the antimalaria cam-paign, in areas of the continent where thePan American Sanitary Bureau considersit appropriate, to discuss uniformity of tech-niques, coordination of border activities orimprovement of the strategy of antimalariawork.
(g) To promote, ini collaboration withsuch schools as offer facilities, refreshercourses for administrative personnel, plannedto cover eradication techniques.
Since the International Sanitary Con-ference of the American Republics, held inWashington in 1902, fifty-two years ago,the countries of this continent have con-tinued to display at all Pan American publichealth meetings a united interest in the
35

STATUS OF ANTIMALARIA CAMPAIGN IN THE AMERICAS: V REPORT
problem of malaria. With the first report ofthe Pan American Malaria Committee, sub-mitted at the XI Pan American SanitaryConference in Rio de Janeiro, in 1942, therehave been periodic appraisals of the statusof the antimalaria campaign in the hemi-sphere. The present report, No. V, is thelatest in the series.
No group of nations in the world hasshown, for more than half a century, such aconstant interest in malaria nor can it pre-
sent, over a period of twelve years, so com-plete and current a history of the status ofthe disease and the campaign to combat it.Neither is there any other group that hasbeen advocating, over the years, coordinatedaction and the exchange of information ashave the peoples of this hemisphere.
At the present time, the coordination ofa plan to eradicate malaria in the Americasis not merely a technical, public health, andeconomic need but also a mandate of history.
36