Statistical Analysis of Clustered Binary Response in Oral Health Research
40
Statistical Analysis of Clustered Binary Response in Oral Health Research Ronen Ofec*, DMD ; David M. Steinberg, PhD ; Devorah Schwartz-Arad, DND, PhD * M.Sc. program in Biostatistics, School of Mathematical sciences, Tel-Aviv university * Praviate dental practice, Tel-Aviv, Israel The 4 th International Meeting on Methodological Issues In Oral Health Research, Istanbul , Turkey
-
Upload
ronen-ofec -
Category
Health & Medicine
-
view
269 -
download
0
Transcript of Statistical Analysis of Clustered Binary Response in Oral Health Research

Statistical Analysis of Clustered Binary Response in Oral Health Research
Ronen Ofec*, DMD ; David M. Steinberg, PhD ; Devorah Schwartz-Arad, DND, PhD
* M.Sc. program in Biostatistics, School of Mathematical sciences, Tel-Aviv university
* Praviate dental practice, Tel-Aviv, Israel
The 4th International Meeting on Methodological Issues In Oral Health Research, Istanbul , Turkey

Dental implants treatment

Dental implants treatment

Dental implants treatment

Dental implants treatment

Dental implants treatment

Dental implants treatment

Dental implants treatment

Dental implants treatment

Dental implants treatment

The durability of Dental implants treatment
Failures (removal of an implant) do occur
Marginal bone loss (MBL) can be an early sign for a failure
MBL: The amount of bone an implant loses during function time

What are the risk factors for MBL?
Are some patients more prone to MBL?
Are implants within patients correlated to each other?
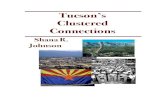
Marginal bone loss (MBL)
Fransson et al.(2005)

What are the risk factors for MBL?
Are some patients more prone to MBL?
Are implants within patients correlated to each other?
Marginal bone loss (MBL)
Fransson et al.(2005)

What are the risk factors for MBL?
Are some patients more prone to MBL?
Are implants within patients correlated to each other?
Marginal bone loss (MBL)
Fransson et al.(2005)

Main question of interest and Objectives of the study
To identify risk factors for MBL in a long term follow up study
To estimate the Intra patient correlation with regard to MBL
To compare results from a naïve analysis to one that includes intra patient correlation
1
2
3
What will be the consequences of a naïve analysis that doesn't recognize correlation within a patient?

Main question of interest and Objectives of the study
To identify risk factors for MBL in a long term follow up study
To estimate the Intra patient correlation with regard to MBL
To compare results from a naïve analysis to one that includes intra patient correlation
1
2
3
What will be the consequences of a naïve analysis that doesn't recognize correlation within a patient?

Main question of interest and Objectives of the study
To identify risk factors for MBL in a long term follow up study
To estimate the Intra patient correlation with regard to MBL
To compare results from a naïve analysis to one that includes intra patient correlation
1
2
3
What will be the consequences of a naïve analysis that doesn't recognize correlation within a patient?

Main question of interest and Objectives of the study
To identify risk factors for MBL in a long term follow up study
To estimate the Intra patient correlation with regard to MBL
To compare results from a naïve analysis to one that includes intra patient correlation
1
2
3
What will be the consequences of a naïve analysis that doesn't recognize correlation within a patient?

Study design and participants
Historical prospective cohort study design
Schwartz-Arad Surgical center, between January1996, and July 1998 by a single surgeon (DSA)
Follow-up time was up to 147 months with a meanof 70 months

The exposures, Binary response and data set
The exposures: Patient-specific and implant-specific
Clustered response: MBL measurement at implant level
Binary response: Acceptable vs. advanced bone loss
Cut point at MBL=0.2 mm/year
The data set: Multilevel data set
195 Patients as the primary sample units (clusters)
721 Implants as the Elementary units
No. of implants per patient [1,16], mode=3

1 Way Random Effect ANOVA
Patient effect
Implant effect
Patient and implant effect are independent
The Intra Class Correlation (ICC)
The Intra Patient Correlation

Kappa type estimator proposed by Fleiss and Cuzick (1979)
Confidence Intervals for the estimator formulatedby Zou and Donner (2004)
Simulation results: empirical coverage is close to nominal with C.I for the kappa type
In our study:
The estimator and the estimatefor ICC

Population average (Marginal) model Liang and Zeger (1986)
1. The mean model:
2. Working variance structure:
3. Working correlation structure:
The empirical/sandwich estimator for the precision of estimates
The Generalized Estimating Equations (GEE)

Robustness of the Sandwich estimator
The estimator is robust to misspecification of the variance and correlation structures
Our estimates are still valid (consistent) if we use a structure which is not reflecting reality
Mancl and Leroux (1996): Gain of precision for the “right” correlation structure

The prevalence of advanced bone loss by GEE

Interaction between function time and risk factors
For smoker:
The odds for MBL for smokers is 4.22 times greater than for non smokers
The effect of HA & TPS turns from protective to risk
Risk factors for MBL by GEE
Function time≥3 yearsFunction time<3 yearsExposure
PV.S.EBetaPV.S.EBeta
***0.411.44Smoker
***0.391.34**0.76-2.22Coating (HA &TPS)
**0.290.85Early spontaneous exposure
***0.40-1.39Diameter
0 *** 0.001 ** 0.01 * 0.05

Interaction between function time and risk factors
For smoker:
The odds for MBL for smokers is 4.22 times greater than for non smokers
The effect of HA & TPS turns from protective to risk
Risk factors for MBL by GEE
Function time≥3 yearsFunction time<3 yearsExposure
PV.S.EBetaPV.S.EBeta
***0.411.44Smoker
***0.391.34**0.76-2.22Coating (HA &TPS)
**0.290.85Early spontaneous exposure
***0.40-1.39Diameter
0 *** 0.001 ** 0.01 * 0.05

Interaction between function time and risk factors
For smoker:
The odds for MBL for smokers is 4.22 times greater than for non smokers
The effect of HA & TPS turns from protective to risk
Risk factors for MBL by GEE
Function time≥3 yearsFunction time<3 yearsExposure
PV.S.EBetaPV.S.EBeta
***0.411.44Smoker
***0.391.34**0.76-2.22Coating (HA &TPS)
**0.290.85Early spontaneous exposure
***0.40-1.39Diameter
0 *** 0.001 ** 0.01 * 0.05

Function time >= 3 years
The naïve estimation and GEE
Estimates for exposure effects – it is not bad to be naïve
Correlation doesn’t induce bias to an unbiased estimator
Standard errors of estimates- a naïve analysis leads to bias
Underestimation or overestimation of standard errors
Risk for invalid inference concerning the estimated effect
GEENaïve
PV.S.EBetaPV.S.EBetaExposure
***0.411.44***0.291.50Smoker
***0.391.34***0.271.31Coating (HA &TPS)
**0.290.85**0.260.85Early exposure
***0.40-1.39***0.35-1.57Diameter

Function time >= 3 years
The naïve estimation and GEE
Estimates for exposure effects – it is not bad to be naïve
Correlation doesn’t induce bias to an unbiased estimator
Standard errors of estimates- a naïve analysis leads to bias
Underestimation or overestimation of standard errors
Risk for invalid inference concerning the estimated effect
GEENaïve
PV.S.EBetaPV.S.EBetaExposure
***0.411.44***0.291.50Smoker
***0.391.34***0.271.31Coating (HA &TPS)
**0.290.85**0.260.85Early exposure
***0.40-1.39***0.35-1.57Diameter

GEENaïve
PV.S.EBetaPV.S.EBetaExposure
0.300.43-0.430.320.41-0.41Smoker
**0.76-2.20.041.09-2.2Coating (HA &TPS)
0.350.390.350.400.420.35Early exposure
0.210.47-0.600.130.42-0.63Diameter
The naïve estimation and GEE
Estimates for exposure effects – it is not bad to be naïve
Correlation doesn’t induce bias to an unbiased estimator
Standard errors of estimates- a naïve analysis leads to bias
Underestimation or overestimation of standard errors
Risk for invalid inference concerning the estimated effect
Function time < 3 years

Patient specific exposure: variation between patient
Similar to treatment effect in Between cluster design
Implant specific exposure: variation within and between patient
Might be similar to treatment effect in Within/Between cluster design
Depends on the source of variation of Implant specific exposure
The source of exposures variation
Within
patient/cluster
Between
patient/cluster
Source of exposure/treatment variation

Deff<1
Variance attenuation factor (VAF)
Therefore, a naïve analysis is conservative (overestimate)
Deff >1
Variance inflation factor (VIF)
Therefore, a naïve analysis is anti-conservative (underestimate)
The Design Effect (Deff)
Within
cluster design
Between
cluster design

Deff<1
Variance attenuation factor (VAF)
Therefore, a naïve analysis is conservative (overestimate)
Deff >1
Variance inflation factor (VIF)
Therefore, a naïve analysis is anti-conservative (underestimate)
The Design Effect (Deff)
Within
cluster design
Between
cluster design

Deff >1
Variance inflation factor (VIF)
Therefore, a naïve analysis is anti-conservative (underestimate)
Deff<1
Variance attenuation factor (VAF)
Therefore, a naïve analysis is conservative (overestimate)
The Design Effect (Deff)
Within
cluster design
Between
cluster design

No problem with the estimated effect
For a patient specific exposure: underestimation of standard errors
For an implant specific exposure: underestimation if variance is from between patients
But, overestimation if variance of exposure is from within patient
Mancl, Leroux, DeRouen (2000) recommended to separate the effect of a site specific exposure, into within and between effect
The answer to the main question of interest
What will be the consequences of a naïve analysis that doesn't recognize correlation within a patient?

Conclusions
Intra patient correlation for advanced MBL exists
The effect of some exposures isn’t constant during function time
Ignoring ICC might bias the precision of estimated effect. Simulation
studies should confirm the direction of the bias
1
2
3

Conclusions
Intra patient correlation for advanced MBL exists
The effect of some exposures isn’t constant during function time
Ignoring ICC might bias the precision of estimated effect. Simulation
studies should confirm the direction of the bias
1
2
3

Conclusions
Intra patient correlation for advanced MBL exists
The effect of some exposures isn’t constant during function time
Ignoring ICC might bias the precision of estimated effect. Simulation
studies should confirm the direction of the bias
1
2
3

Thanks ! [email protected]