
Standard Practice for the Occupational/Environmental...
21
Designation: E2473 - 05 (Reapproved 2011) An American National Standard Standard Practice for the Occupational/Environmental Health View of the Electronic Health Record 1 This standard is issued under the fixed designation E2473; the number immediately following the designation indicates the year of original adoption or, in the case of revision, the year of last revision. A number in parentheses indicates the year of last reapproval. A superscript epsilon (´) indicates an editorial change since the last revision or reapproval. 1. Scope 1.1 This Practice is intended to assemble a logical occupational/environmental health view of the already defined general structure and vocabulary for the Electronic Health Record (EHR) and to suggest the ways in which this view can be used to support employee health assessments and other healthcare delivered at the work site. This view is consistent with the ANSI/ADA Clinical Concept Data Model 2005, which identified the major data entities that will need to be involved. This view would complement other views addressed in other settings of care for the employee and could logically either request other EHR data or deliver to other practitioner request- er’s record systems portions of occupational/environmental health data that have been recorded at the work site. This practice does not deal with the specific implementation of the content and it also does not either suggest or recommend implementation techniques. Likewise, it does not suggest standards of care. These functions are dealt with in other domains. 2. Referenced Documents 2.1 ASTM Standards: 2 E1239 Practice for Description of Reservation/Registration- Admission, Discharge, Transfer (R-ADT) Systems for Electronic Health Record (EHR) Systems E1340 Guide for Rapid Prototyping of Information Systems E1384 Practice for Content and Structure of the Electronic Health Record (EHR) E1578 Guide for Laboratory Information Management Sys- tems (LIMS) E1633 Specification for Coded Values Used in the Electronic Health Record E1714 Guide for Properties of a Universal Healthcare Iden- tifier (UHID) E1715 Practice for An Object-Oriented Model for Registra- tion, Admitting, Discharge, and Transfer (RADT) Func- tions in Computer-Based Patient Record Systems E1744 Practice for View of Emergency Medical Care in the Electronic Health Record E1762 Guide for Electronic Authentication of Health Care Information E1869 Guide for Confidentiality, Privacy, Access, and Data Security Principles for Health Information Including Elec- tronic Health Records E1986 Guide for Information Access Privileges to Health Information E1987 Guide for Individual Rights Regarding Health Infor- mation (Withdrawn 2007) 3 E1988 Guide for Training of Persons who have Access to Health Information (Withdrawn 2007) 3 E2017 Guide for Amendments to Health Information E2066 Guide for Validation of Laboratory Information Man- agement Systems E2084 Specification for Authentication of Healthcare Infor- mation Using Digital Signatures (Withdrawn 2009) 3 E2085 Guide on Security Framework for Healthcare Infor- mation (Withdrawn 2009) 3 E2086 Guide for Internet and Intranet Healthcare Security (Withdrawn 2009) 3 E2145 Practice for Information Modeling E2147 Specification for Audit and Disclosure Logs for Use in Health Information Systems E2171 Practice for Rating-Scale Measures Relevant to the Electronic Health Record 2.2 ANSI/IEEE Standards: 4 ANSI/IEEE 610.2 Standard Glossary of Computer Applica- tions Terminology ANSI/IEEE 610.5 Standard Glossary of Information Man- agement Terminology 1 This practice is under the jurisdiction of ASTM Committee E31 on Healthcare Informatics and is the direct responsibility of Subcommittee E31.25 on Healthcare Data Management, Security, Confidentiality, and Privacy. Current edition approved May 1, 2011. Published May 2011. Originally approved in 2005. Last previous edition approved in 2005 as E2473 05. DOI: 10.1520/E2473-05R11. 2 For referenced ASTM standards, visit the ASTM website, www.astm.org, or contact ASTM Customer Service at [email protected]. For Annual Book of ASTM Standards volume information, refer to the standard’s Document Summary page on the ASTM website. 3 The last approved version of this historical standard is referenced on www.astm.org. 4 Available from American National Standards Institute (ANSI), 25 W. 43rd St., 4th Floor, New York, NY 10036, http://www.ansi.org. Copyright © ASTM International, 100 Barr Harbor Drive, PO Box C700, West Conshohocken, PA 19428-2959. United States 1
Transcript of Standard Practice for the Occupational/Environmental...

Designation: E2473 − 05 (Reapproved 2011) An American National Standard
Standard Practice for theOccupational/Environmental Health View of the ElectronicHealth Record1
This standard is issued under the fixed designation E2473; the number immediately following the designation indicates the year oforiginal adoption or, in the case of revision, the year of last revision. A number in parentheses indicates the year of last reapproval. Asuperscript epsilon (´) indicates an editorial change since the last revision or reapproval.
1. Scope
1.1 This Practice is intended to assemble a logicaloccupational/environmental health view of the already definedgeneral structure and vocabulary for the Electronic HealthRecord (EHR) and to suggest the ways in which this view canbe used to support employee health assessments and otherhealthcare delivered at the work site. This view is consistentwith the ANSI/ADA Clinical Concept Data Model 2005, whichidentified the major data entities that will need to be involved.This view would complement other views addressed in othersettings of care for the employee and could logically eitherrequest other EHR data or deliver to other practitioner request-er’s record systems portions of occupational/environmentalhealth data that have been recorded at the work site. Thispractice does not deal with the specific implementation of thecontent and it also does not either suggest or recommendimplementation techniques. Likewise, it does not suggeststandards of care. These functions are dealt with in otherdomains.
2. Referenced Documents
2.1 ASTM Standards:2
E1239 Practice for Description of Reservation/Registration-Admission, Discharge, Transfer (R-ADT) Systems forElectronic Health Record (EHR) Systems
E1340 Guide for Rapid Prototyping of Information SystemsE1384 Practice for Content and Structure of the Electronic
Health Record (EHR)E1578 Guide for Laboratory Information Management Sys-
tems (LIMS)E1633 Specification for Coded Values Used in the Electronic
Health Record
E1714 Guide for Properties of a Universal Healthcare Iden-tifier (UHID)
E1715 Practice for An Object-Oriented Model for Registra-tion, Admitting, Discharge, and Transfer (RADT) Func-tions in Computer-Based Patient Record Systems
E1744 Practice for View of Emergency Medical Care in theElectronic Health Record
E1762 Guide for Electronic Authentication of Health CareInformation
E1869 Guide for Confidentiality, Privacy, Access, and DataSecurity Principles for Health Information Including Elec-tronic Health Records
E1986 Guide for Information Access Privileges to HealthInformation
E1987 Guide for Individual Rights Regarding Health Infor-mation (Withdrawn 2007)3
E1988 Guide for Training of Persons who have Access toHealth Information (Withdrawn 2007)3
E2017 Guide for Amendments to Health InformationE2066 Guide for Validation of Laboratory Information Man-
agement SystemsE2084 Specification for Authentication of Healthcare Infor-
mation Using Digital Signatures (Withdrawn 2009)3
E2085 Guide on Security Framework for Healthcare Infor-mation (Withdrawn 2009)3
E2086 Guide for Internet and Intranet Healthcare Security(Withdrawn 2009)3
E2145 Practice for Information ModelingE2147 Specification for Audit and Disclosure Logs for Use
in Health Information SystemsE2171 Practice for Rating-Scale Measures Relevant to the
Electronic Health Record
2.2 ANSI/IEEE Standards:4
ANSI/IEEE 610.2 Standard Glossary of Computer Applica-tions Terminology
ANSI/IEEE 610.5 Standard Glossary of Information Man-agement Terminology
1 This practice is under the jurisdiction of ASTM Committee E31 on HealthcareInformatics and is the direct responsibility of Subcommittee E31.25 on HealthcareData Management, Security, Confidentiality, and Privacy.
Current edition approved May 1, 2011. Published May 2011. Originallyapproved in 2005. Last previous edition approved in 2005 as E2473 05. DOI:10.1520/E2473-05R11.
2 For referenced ASTM standards, visit the ASTM website, www.astm.org, orcontact ASTM Customer Service at [email protected]. For Annual Book of ASTMStandards volume information, refer to the standard’s Document Summary page onthe ASTM website.
3 The last approved version of this historical standard is referenced onwww.astm.org.
4 Available from American National Standards Institute (ANSI), 25 W. 43rd St.,4th Floor, New York, NY 10036, http://www.ansi.org.
Copyright © ASTM International, 100 Barr Harbor Drive, PO Box C700, West Conshohocken, PA 19428-2959. United States
1

ANSI/IEEE 610.12 Standard Glossary of Software Engi-neering Terminology
ANSI/IEEE 729 Fundamental Terms in Software Engineer-ing
ANSI/IEEE 830 Software Requirements SpecificationANSI/IEEE 1058 Software Project Management PlansANSI/IEEE 1062 Recommended Practice for Software Re-
quirementsANSI/IEEE 1063 Software User DocumentationANSI/IEEE 1073 Framework and OverviewANSI/IEEE 1073.2 Application Profile Framework and
OverviewANSI/IEEE 1073.3.1 Transport ProfileANSI/IEEE 1073.4.1 Physical Layer-Cable ConnectedANSI/IEEE 1074 Standard for Developing Life Cycle Pro-
cessesANSI/IEEE 1074.1 Guide for Developing Life Cycle Pro-
cessesANSI/IEEE 1220 Standard for Application and Management
of the System Engineering ProcessANSI/IEEE 1233 Guide to Preparing System Requirements
SpecificationsANSI/IEEE 1320.1 Standard for Conceptual Modeling
Language—Syntax and Semantics for IDEF0ANSI/IEEE 1320.2 Standard for Conceptual Modeling
Language—Syntax and Semantics for IDEF1X97 (IDEFObject)
ANSI/IEEE 1362 Guide for Information Technology—System Definition—Concept of Operations Document
ANSI/IEEE 1490 Guide to Project Management Body ofKnowledge
ANSI/IEEE 1498 Trial Use Standard for InformationTechnology—Software LifeCycle Processes—SoftwareDevelopment: Acquirer—Supplier Agreement
ANSI/IEEE 12207.0 Standard for InformationTechnology—Software Life Cycle Processes
ANSI/IEEE 12207.1 Guide for Information Technology—Software Life Cycle Processes—Life Cycle Data
ANSI/IEEE 12207.2 Guide for Information Technology—Software Life Cycle Processes—Implementation Consid-erations
IEEE P1157.1 Trial Use Standard for Healthcare DataInterchange—Information Model Methods
2.3 ANSI/HL7 Standards:4
ANSI/HL7 Interface Standard v2.4HL7 Message Development Framework v 3.0 Jan 1997
2.4 ISO Standards:4
ISO/IEC TR 9789 Information Technology—Guidelines forthe Organization and Representation of Data Elements forData Interchange—Coding Methods and Principles
ISO 12200 Computer Applications in Terminology—Machine-Readable Terminology Interchange Format(MARTIF)—Negotiated Interchange
ISO 12620 Computer Applications in Terminology—DataCategories
ISO IS 12207 Information Technology-Software Life CycleProcesses
ISO IS 15188 Project Management Guidelines for Terminol-ogy Standardization
ISO WD 15288 System Life Cycle ProcessesISO 15440 Guide for Life Cycle Processes
2.5 Other Standards:ANSI X3.172 American National Dictionary for Informa-
tion SystemsANSI/ADA TR 1039 2005 Clinical Content Data ModelANSI/ADA 1000.0 Introduction, Model Architecture, and
Specification FrameworkANSI/ADA 1000.1 Individual IdentificationANSI/ADA 1000.2 Codes and NomenclatureANSI/ADA 1000.3 Individual CharacteristicsANSI/ADA 1000.4 Population CharacteristicsANSI/ADA 1000.5 OrganizationANSI/ADA 1000.6 LocationANSI/ADA 1000.7 CommunicationANSI/ADA 1000.8 Healthcare EventANSI/ADA 1000.9 Health MaterielANSI/ADA 1000.10 Health ServicesANSI/ADA 1000.11 Health Service ResourcesANSI/ADA 1000.12 Population Health FactsANSI/ADA 1000.13 Patient Health FactsANSI/ADA 1000.14 Health Condition DiagnosisANSI/ADA 1000.15 Health Service PlanANSI/ADA 1000.16 Patient Health ServiceANSI/ADA 1000.17 Clinical InvestigationANSI/ADA 1000.18 Comments Subject AreaDICOM Supplement 15 Visible Light Image, Anatomic
Frame of Reference, Accession and Specimen for Endos-copy, Microscopy, and Photography
CEN ENV 1613 Medical Informatics—Messages for theExchange of Laboratory Information
CEN ENV 1614 Healthcare Informatics—Structure for No-menclature, Classification and Coding of Properties inClinical Laboratory Sciences
CEN EN 12017 Medical Informatics Vocabulary (MIVoc)CEN EN 12264 Categorical Structures of Systems of
Concepts—Model for Representation of Semantics(MOSE)
Internet RFC 1521 N. Borenstein, N Freed MIME [Multi-purpose Internet Mail Extensions] Purpose: Mechanismsfor Specifying and Designating the Format of InternetMessage Bodies Bellcore Innosoft Sep 1993
ANSI X12CLSI AUTO1-A Laboratory Automation: Specimen
Container/Specimen CarrierCLSI AUTO2-A Laboratory Automation: Bar codes for
Specimen Container IdentificationCLSI AUTO3-A Laboratory Automation: Communications
with Automated Clinical Laboratory Systems, Instru-ments, Devices and Information Systems
CLSI AUTO4-A Laboratory Automation: Systems Opera-tional Requirements, Characteristics and Information El-ements
CLSI AUTO5-A Laboratory Automation: ElectromechanicalInterfaces
E2473 − 05 (2011)
2

ANSI/ CLSI ASTP2 Point of Care In-vitro Diagnostic Test-ing
ANSI/CLSI GP19 Laboratory Instruments and Data Man-agement Systems: Design of Software User Interfaces andSoftware Systems Validation, Operations and Mainte-nance
CLSI LIS-3A (prior ASTM E792) Guide for Procurement ofa Clinical Laboratory Information Management System(CLIMS)
CLSI LIS-5A (prior ASTM E1238) Specification for Trans-ferring Clinical Observations Between Independent Com-puter Systems
CLSI LIS-1A (prior ASTM E1381) Specification for LowLevel Protocol to Transfer Messages Between ClinicalLaboratory Instruments and Computer Systems
CLSI LIS-2A (prior ASTM E1394) Specification for Trans-ferring Information Between Clinical Instruments andComputer Systems
CLSI LIS-7A (prior ASTM E1466) Specification for Use ofBar Codes on Specimen Tubes in the Clinical Laboratory
CLSI LIS-8A (prior ASTM E1639) Guide for FunctionalRequirements of Clinical Laboratory Information Man-agement Systems
CLSI LIS-9A (prior ASTM E2118) Guide for Coordinationof Clinical Laboratory Services Within the ElectronicHealth record Environment and Networked Architectures
IUPAC/IFCC Silver Book: Compendium of Terminologyand Nomenclature of Properties in Clinical LaboratorySciences
IUPAC/IFCC Properties and Units in Clinical LaboratorySciences X Properties and Units in General ClinicalChemistry
IUPAC/IFCC Properties and Units in Clinical LaboratorySciences XII Properties and Units in Clinical Pharmacol-ogy and Toxicology
3. Terminology
3.1 Definitions:3.1.1 case—an Occupational/Environmental Health event in
which one or more individuals and locations are found toexhibit measurements of environmental stressors that are atvariance with criteria that define normative states.
3.2 Acronyms:3.2.1 CAP—College of American Pathologists
3.2.2 CDC—Centers for Disease Control and Prevention,Dept. of Health and Human Services
3.2.3 CDSS—Clinical Decision Support Systems
3.2.4 CLIMS—Clinical Laboratory Information Manage-ment System
3.2.5 CLSI—Clinical and Laboratory Standards Institute
3.2.6 CPR—Computer-based Patient Record
3.2.7 DHHS—Department of Health and Human Services
3.2.8 EC—Electronic Commerce
3.2.9 EDI—Electronic Data Interchange
3.2.10 EHR—Electronic Health Record
3.2.11 EPA—Environmental Protection Agency
3.2.12 HIN—Health Information Network
3.2.13 IDS—Integrated Delivery Systems
3.2.14 ISA—Information Systems Architecture
3.2.15 LAS—Laboratory Automation System
3.2.16 LIMS—Laboratory Information Management System
3.2.17 MDSS—Management Decision Support System
3.2.18 MCO—Managed Care Organization
3.2.19 MPI—Master Person/Patient Index
3.2.20 NCVHS—National Committee on Vital and HealthStatistics
3.2.21 NIOSH—National Institute for Occupational Safetyand Health
3.2.22 NPF—National Provider File
3.2.23 NPI—National Provider Identifier
3.2.24 NPS—National Provider System
3.2.25 OSHA—Occupational Safety and Health Administra-tion
3.2.26 POC—Point-of-Care
3.2.27 POCT—Point-of-Care Testing
3.2.28 PPO—Preferred Provider Organization
3.2.29 SSAN—Social Security Account Number (also SSN)
3.2.30 UMLS—Unified Medical Language System
3.2.31 VHA—Veteran’s Health Administration
3.2.32 VistA—VHA Information Systems Technology Ar-chitecture
4. Significance and Use
4.1 This practice is directed at defining the application ofexisting conventions for the structure and content of EHRsystems used to support healthcare practitioners in a workplacesetting. In addition to supporting the capture of data onencounters and of periodic patient health assessments con-ducted during the time the employee is at work, this documentalso recognizes the interaction of care rendered over a lifetimeand when not at work with that due to the work environmentthat is delivered on the work site, either for care events thathave occupational significance or for surveillance of potentialhealth conditions that may result from the work or livingenvironment. This document recognizes not only the privacyand confidentiality of records that are kept in the work settingbut also the need to be able to interchange data from theworkplace record with health records in other settings in orderto fully support employee and environmental health.
4.2 Occupational Health Programs:4.2.1 Most occupational health programs are oriented, first,
to any regular surveillance for observations associated withpotentially adverse health conditions known to attend environ-mental stressors that may be present in either the workplace orthe living environment and, second, to care and documentationof any illness or injury incurred during the workday at the worksite or in other living environments. Each of these activitiesrequires recording data for the care record that is a subset ofthat regularly required for care in other more extensive
E2473 − 05 (2011)
3

ambulatory and inpatient care settings. It also requires relatingthe events occurring in either the work place or the livingenvironment to those observed healthcare data.
4.2.2 This practice is intended to identify the most fre-quently used of the general data elements which are morecompletely documented in Practice E1384 and SpecificationE1633. Thus, this description constitutes a “view” of the morecomprehensive set of data that might be captured in a generalambulatory care encounter. If the conventions given in thisdocument are adhered to, the data will ensure a record that isportable to any other setting and the record will be interoper-able with other standards conformant systems, regardless oftheir implementation techniques. Fig. 1 shows the inter-relationships of the basic information domains that supportOccupational/Environmental Health programs within health-care. The Care Record subdomain embraces the conceptualcontent and structure that have been documented in PracticeE1384 and associated standards. Resource Management andEpidemiology data analytic functions and subdomains are
documented elsewhere in descriptions of the requirements ofthe HIPAA legislation and the CDC Public Health InformationNetwork—PHIN(X). The Occupational Health Programs aregenerally organized in employing organizations, but healthcareenterprises need to also recognize that they too are “employ-ers” in the same sense as any other societal business organi-zation and that their employees, including all healthcarepractitioners, as well as their associate professional disciplinecolleagues, are entitled to management of their occupationalhealth information by the same principles. Thus, occupationalhealth information management is intrinsic to management ofall information in the healthcare enterprise and sets the stagefor the management of information of the enterprise’s “Patient”population. An occupational/environmental health “case” isdefined to be that informational record that identifies a specificinstance of an occupational/environmentally induced healthcondition and its associated attributes from the patient care andenvironmental assessment records that will enable resolution ofboth the health condition and the causal environmental factors
FIG. 1 Occupational/Environmental Health Information Subdomains
E2473 − 05 (2011)
4

associated with it. The handling of “cases” relating to adverseeffects of stressors in with general living environment issomewhat different since the adverse effects are usually firstdetected by the individual’s personal practitioner and then onlyindirectly related to environmental events. These cases are nottracked organizationally in the same way that is used for thosein the workplace. Even in workplaces for very small busi-nesses, the environmental effects of the workplace are usuallydetected in this latter unstructured fashion and these “cases”are not currently formally tracked, nor is environmental moni-toring performed.
4.3 Reportable Data—Certain data about care events arerequired to be regularly reported to public authorities, state orfederal. These include occupational illness or injury. Thesereportable data constellations are subsets of the occupationalhealth “view” described here and do not include all of theattributes of the “view.” Such “Reportable Data” are explicitlydefined. These data can be composed into electronic messagesfor transmission to reporting authorities. While this “view”does not deal with the format of such messages, its constituentdata elements provide the fields needed to compose suchmessages. For discussion of reportable data, consult Refs. (1,2).5
4.4 Health Surveillance Processes—Health Surveillanceprocesses supporting Occupational/Environmental Health be-gin with the Basic Patient Care Scenario given in PracticeE1384. In occupational/environmental healthcare, the “patient”must first be registered and have updated demographic dataavailable to the sites who give care for the illnesses and injuriesresulting from either the occupations or the general livingenvironment. Likewise, periodic environmental assessmentmeasurements must be posted to the susceptible individuals’patient record. When a health event occurs, provoking theindividual to visit a healthcare enterprise, the individualdemographic information must be easily accessible during theevent encounter’s Receipt Phase. Attributes of that phasedenote potential occupational or environmental involvement inthe health condition(s) assessed during the Activities Phase ofthe Encounter. The care data is captured during the encounterand is related to the individual’s recorded environmentalexposure measurements. These observations become thesource of reportable data that supports surveillance. Thoseencounter attributes also control the data that flows to all of thevarious other (for example, public health) information domainsat the completion of the encounter. For best followup, the datacaptured in the EHR need to identify either the living or thework locations and associated activities that produce theadverse health events that may potentially be related either tothe living or the work environment.
4.5 Occupational/Environmental Healthcare Processes—The individual’s “Employer,” if there is one that has ahealthcare facility and staff to service the health problems ofindividuals employed by the organization, will have a differentapproach than that for small businesses who rely on the
individual employee’s private practitioner, regardless of thehealthcare payer arrangements. “Workman’s Compensation”arrangements primarily address the financial managementfunctions rather than the health condition issues and thesituations that led to them, particularly if these illnesses orinjuries might have been caused by the work environment.Worker’s Compensation does not presently fully address thereasons for the inability to return to work due to the healthcondition, but rather provides limited stipends for a specifiedperiod. Particularly when the employer relies solely on theindividual’s practitioner, the mechanisms are not yet welldefined by which the employee can progressively return towork in an healthcare-supervised fashion and by which thework environment situations leading to the injury or illness areactively addressed in order to remedy their causes. Thesemechanisms should include such functions as steps to identifythe environmental causes of stressors in either general living orsmall business settings and the causes of injury in all settings.In industrial or large businesses, there may be specific staffresponsible for monitoring the work environment, but in smallbusinesses these capabilities should be also available via otherarrangements that are triggered by the nature of the docu-mented health conditions and a tracking of their source to thespecific work or living environment settings. The businessorganization structures, the functional responsibilities and theassociated data and data flows need documentation based uponcommon specific arrangements that can be made by theemployer organization. Other arrangements regarding environ-mental health conditions associated with the non-employedshould also be possible with respect to the individual’s privatepractitioner, and these arrangements should relate to patient-centered care issues. It is these processes that characterize whatmay be termed the “Occupational/Environmental HealthcareProcesses” as differentiated from the specific “Patient CareProcesses.”
4.6 Environmental Assessment Processes—The“Occupational/Environmental Healthcare Processes” arecomplemented by the “Environmental Assessment Processes,”which include the familiar monitoring of elements such as airand water for environmental contaminants. What is needed fora comprehensive treatment of occupational and environmentalhealth, either within the workplace or outside of it, is adescription of the flow of information among the environmen-tal and health care professional disciplines, such that each roleis clearly defined and the contribution of each role in specifiedsituations is recognized with regard to a healthy population inand out of the workplace. It is critical to define how informa-tion about the environment to which individuals are exposed,both during the workday and outside of it, is made available tothe documented healthcare practitioners serving those indi-vidual “patients” through being posted to appropriate patientrecords. The present kinds of environmental assessment infor-mation are well known, but how they are used to createintegrated multidisciplinary care process relationships that leadto “Patient-Centered Care” is not presently well documented.Section 5 will address this need.
5 The boldface numbers in parentheses refer to the list of references at the end ofthis standard.
E2473 − 05 (2011)
5
5. An Occupational/Environmental HealthInformation Model
5.1 Conceptual Model of Relationships of Occupational/Environmental Health within Healthcare—As noted in 4.2,looking at the overall four information subdomains, thesebreakdown into conceptual entities which must be related tothose data that are maintained in the Care Record now referredto as the Electronic Health Record (EHR), which has a muchmore specific structure than the commonly stated unspecific“Clinical Data Repository” term. The general implications ofthe points made in Section 4 are that the occupational/environmental health usages of the EHR data elements dependupon the particular needs of the individual work/living setting.If these data elements are used, then they are common to theirusage by other practitioners, such as the employees personalfamily practitioner(s). Thus they complement the data in the“Case Management” subdomain of Fig. 1 in the sense that the“Case” is a problem/health condition that results from anenvironmental situation in the workplace that must be concur-rently managed in order to ensure that the environment nolonger causes such problems/health conditions identified ineither the specific individual or in other individuals in thatwork/living environment setting. For that reason, the concep-tual objects involved in the individual enterprise informationarchitecture need to be approached in a unified way from an“Enterprise View.” Fig. 2 presents the key conceptual objectsthat should be considered. This diagram should also beconsidered in the context of the Model for the Registration,Admitting and Discharge core model that underpins not onlythe EHR but also all supporting ancillary services used inhealthcare, as documented in Practices E1239 and E1715, andextended for the clinical laboratory ancillary service domain byPractice CLSI LIS-8A. Fig. 2 also notes those conceptualobjects that deal with those attributes of the occupational/environmental health domains dealt with by the EnvironmentalHealth Laboratories which post information to EHR compo-nents within the healthcare enterprise information architecturethat support both the “Case Management” and the “Environ-mental Management” functions of the defined “Enterprise.”For healthcare providers that deliver healthcare services to avariety of “Employers,” careful definition of these informationsubdomains will be required if an effective information archi-tecture for supporting these functions is to be achieved. Boththe process and data models associated with these conceptualentities are dealt with below in 5.2 and 5.3 respectively. Thedata objects used for each function is given in Table 3.
5.2 Process Model for Occupational/Environmental HealthFunctions—The processes discussed in Section 4 can berepresented in the general model shown in Fig. 3. Thesefunctions, given in Table 1, reflect those given in the basic CoreEHR Functional Model given in Table 2 (see also PracticeE1239). The relationship of the processes to the EHR functionsgiven in the public health perspective and HL7 EHR functionalmodel described in Ref (1) is not yet clear because theconceptual linkages between the various public health agenciesinvolved in environmental issues and the patient care settingsfor occupational/environmental care has not yet been de-scribed. Such linkages will need to clearly depict how envi-
ronmental data would transparently aid in clinical decisionsupport of occupational/environmental care by practitioners, inaddition to its epidemiologic and environmental policy roles.
5.2.1 Functional Model Scenarios—Two key Scenarios,Occupational and Environmental, can be described to illustratehow these functions might be applied within these basicsituations. These will now be described.
5.2.1.1 Occupational—In occupational settings, the em-ployer would offer occupational care facilities and maintain anEHR to capture health data with respect to the workplace,including capturing stressor data for workplace locations; thesestressor exposure data would be located in the EHR asdescribed in Practice E1384 and would be accessible toappropriate occupational health practitioners. Such data wouldbe obtained as part of a designated environmental monitoringprotocol for identified work locations. At designated timesenvironmental samples would be taken and subsequentlyanalyzed by a designated environmental laboratory. The envi-ronmental measurement data for each date-time and locationwould be posted to a posting file. The occupational healthfacility for each employee (whose work location and appropri-ate dates would be known in the EHR) would, on a designatedschedule, access this posting file and copy the appropriatemeasurement entries to the employee stressor exposure seg-ment of the EHR. When the employee has an encounter (eitherscheduled or ad hoc), this updated segment is viewed by thepractitioner during the assessment phase, clued by entries inthe Health Condition/Problem List segment that the employeeis at risk for identified environmental stressors. These alertsmay stimulate requested clinical lab services for biomarkers inpatient specimens and specific examination observations po-tentially related to exhibited adverse effects of environmentalstressors. Presence or absence of appropriate observationswould trigger appropriate statements to be recorded in therecord of such encounters. These recorded encounter entrieswill provide clues to the occupational health service practitio-ners for early detection and characterization of adverse effectsof identified environmental stressors and, if such adverseeffects are detected, develop both a care treatment plan and anenvironmental remediation plan to deal with both the effectsand the cause respectively. In addition, identified reportabledata sets can be electronically prepared and sent from therecorded EHR data to designated public health agencies.Additional analytical data sets for the employer can also beabstracted from the EHR and used in the occupational healthmanagement process. If the care process requires coordinatedactivities by the employee’s private practitioner, appropriateEHR abstracts can be electronically forwarded (with appropri-ate privacy/confidentiality caveats) to that practitioner asdirected by the occupational health practitioner staff. Thesesteps should ensure patient-centered, multidisciplinary,evidences-based and quality care in the workplace.
5.2.1.2 Environmental—In general living settings where, forexample, there may be exposure by residents of a givencommunity to such stressors as arsenic, lead, selenium ororganic industrial pollutants that enter the air or drinking waterthat subsequently show up in exhibited health conditions that
E2473 − 05 (2011)
6

could be detected by the private practitioners of those resi-dents, if given sufficient clues about potential exposures. Thissituation will require appropriate health professional specialtyeducation and alerting that is supported by effective andconvenient data sources. The environmental informationneeded by the practitioners can be supplied by an appropriate
information architecture that contains components not only forthe EHR but also for collecting and posting to the EHR thosedata applicable to specific patients. This data posting mecha-nism will be more complex than that for occupational health-care settings because of the breadth and diversity of thegeographic and social settings; different regions may have
FIG. 2 Conceptual Occupational/Environmental Health Data Model
E2473 − 05 (2011)
7

different governmental or private organizational participants,but these will operate very similarly to the situation inoccupational settings. Thus the common conventions for envi-ronmental health business operations will parallel the informat-ics common conventions for the EHR and data exchange. Theindividual’s private practitioner would maintain an EHR tocapture health data with respect to the living environment,including capturing stressor data for community locations;these stressor exposure data would be located in the EHR asdescribed in Practice E1384 and would be accessible toappropriate private practitioners. Such data would be obtainedas part of a designated environmental monitoring protocol foridentified community locations. At designated times, environ-mental samples would be taken and subsequently analyzed bya designated environmental laboratory. The environmentalmeasurement data for each date-time and location would beposted to a posting file. The health facility for each patient(whose residential location and appropriate dates would beknown in the EHR) would, on a designated schedule, access
this posting file and copy the appropriate measurement entriesto the patient stressor exposure segment of the EHR. When thepatient has an encounter (either scheduled or ad hoc), thisupdated segment is viewed by the practitioner during theassessment phase, clued by entries in the Health Condition/Problem List segment that the patient is at risk for identifiedenvironmental stressors. These alerts may stimulate requestedclinical lab services for biomarkers in patient specimens andspecific examination observations potentially related to exhib-ited adverse effects of environmental stressors. Presence orabsence of appropriate observations would trigger appropriatestatements to be recorded in the record of such encounters.These recorded encounter entries will provide clues to theprivate practitioners for early detection and characterization ofadverse effects of identified environmental stressors and, ifsuch adverse effects are detected, develop both a care treatmentplan and help develop a community environmental remediationplan to deal with both the effects and the cause, respectively, ofcommunity environmental stressors. In addition, identifiedreportable data sets can be electronically prepared and sentfrom the recorded EHR data to designated public healthagencies. These steps should ensure patient-centered, multidis-ciplinary, evidences-based, and quality environmental healthcare in the community.
5.3 Data Model for Occupational/Environmental Health—The Core EHR Data model, given in Fig. 4, and the DataModel for the Occupational/Environmental Health View of theEHR, which is an extension of that core and is given in Fig. 5,represent how the data needed for integrated occupational/environmental patient care draw on the defined structure for thebasic EHR. The mapping of data objects to the functionalactivities given in 5.2 is given in Table 3. The attributes of thedata objects are given in 5.3.2.
TABLE 1 Functions Supporting the Occupational/EnvironmentalHealth View of the EHR
NOTE 1—Basic Core Functional Model Functions are in bold .
Occupational:
EmployerEmploy WorkersAssign WorkersManage Work ActivitiesPlan Surveillance ProtocolPost Occupational ActivitiesEvaluate Work Activities
Care:
PatientCategorize Living ActivitiesRegister Patients REGPost Patient Environmental AssignmentsPractitioner Assignment ASSGNConduct Encounter ENOTMake Assessment: Health History HISTMake Assessment: Examination EXMMake Assessment: Health Condition/Problem HCPLMake Clinical Laboratory Patient MeasurementsCoordinate Patient and Environmental MeasurementsEvaluate Occupational/Environmental FactorsInterpret Environmental MeasurementsPlan Treatment TPLIssue Clinical Orders CCOMake Disposition: Report Environmental Factors to Relevant Public
Health AgenciesMake Disposition: Develop Followup PlanReport Adverse Living/Workplace Factors
Healthcare ProviderMonitor List of EmployersMonitor List of Environmental LocationsMonitor List of Public Health Agencies
Public Health:
Plan Environmental SurveillancePlan Environmental MonitoringMonitor Environment with MeasurementsPost Environmental Data to Healthcare EnterprisesPlan Environmental RemediationInterpret Environmental Measurements
TABLE 2 EHR Core Model Patient Care Functions
Abbrev. Function Name
AdministrativeMPI Patient/Person Indexing [EHR03MPI]PRREG Register Practitioners/Staff [EHR031]REG Register Patient [EHR031]ASSGN Assign Practitioner [EHR032]PSAC Patient Screening/Acceptance[EHR03222]APPTS Create Patient Appointments [EHR032]
AssessmentENOT Enter Encounter Data [EHR03224]HIST Get Patient Health History [EHR03222]ESTR Document Exposure to Environmental Stressors [EHR03222]EXM Record Patient Examination[EHR03222]HSTAT Assess Patient Health Status[EHR03222]HCPL Input Health Condition/Problem List[EHR03222]
Treatment PlanningTPL Prepare Treatment Plans [EHR03223]CCO Create Clinical Orders [EHR03223]PEDC Patient Education/Communication Capability [EHR03223]RCON Request Patient Referral/Consult [EHR03223]
InfrastructureCHAUD Conduct Chart Audits [EHR01]CHTR Track Paper Charts [EHR01]PCQA Patient Care Quality Assurance [EHR02]REFDM Referential Data Maintenance [EHR01]PRT Patient Record Transfer [EHR01]
E2473 − 05 (2011)
8

5.3.1 Business Process Correlates of the Data Model—Thedata object relationships implied in Fig. 5 are that, by identi-fying the Work Operations and the Work/Environmental Loca-tions associated with the Employee/Patient and by document-ing the environmental sampling regimen associated with thatlocation, the specimens taken for analysis will yield environ-mental measurements for that work/living location. Theseenvironmental measurements can be posted to individualpatient records with sufficient identifying attributes for theanalyzing laboratory, and its associated environmental scien-tist, so that, should the Patient’s Healthcare Practitioner find an
association of the environmental measurement with a Patient’sHealth Condition and need further information about theWork/Environmental Location and its associated population,then an expeditious contact with the Environmental Scientistcan be made to arrive at an appropriate interpretation of theEnvironmental Measurement. The implemented specifichealthcare enterprise and regional information architectureswould determine how such specific communications wouldoccur but could be achieved by use of standards definedmessage formats.
TABLE 3 Function/Data Relationships
Function Data Objects
Employ Workers Organization, Employer, WorkerAssign Workers Location, Work LocationManage Work Activities Location, Work Location, Work OperationEvaluate Work Activities Location, Work Location, Work OperationPlan Surveillance Protocol Survey, LocationPost Occupational Activities Work OperationCategorize Living Activities Living ActivityRegister Patients Person, Patient, Healthcare EnterprisePost Patient/Environmental Assignments Health HistoryConduct Encounter Patient, EncounterMake Assessment: Health History Health HistoryMake Assessment: Examination Exam, Diagnostic TestsMake Assessment: Health Condition/Problem Health ConditionMake Clinical Laboratory Patient Measurements Diagnostic Test, Clinical Orders, Laboratory, Clinical
LaboratoryCoordinate Patient and Environmental Measurements Diagnostic Test, Environmental MeasurementEvaluate Occupational/Environmental Factors Health ConditionPlan Treatment Treatment PlanIssue Clinical Orders Clinical Order, PatientMake Disposition: Report Environmental Factors to Relevant
Public Health AgenciesPerson, Patient, Environmental Measurement,Environmental
LocationMake Disposition: Develop Followup Plan Patient, EncounterReport Adverse Living/Workplace Factors Environmental Location, Environmental MeasurementMonitor List of Employers EmployerMonitor List of Environmental Locations Location, Work Location, Environmental Location,
Instrument,Environmental Specimen
Monitor List of Public Health Agencies OrganizationPlan Environmental Monitoring Organization, Environmental MeasurementMonitor Environment with Measurements Environmental Measurement, Environmental
Laboratory, LaboratoryPost Environmental Data to Healthcare Enterprises Patient, Environmental SpecimenPlan Environmental Remediation OrganizationInterpret Environmental Measurements Environmental Measurement, Stressor
E2473 − 05 (2011)
9

FIG. 3 Occupational/Environmental Health Functional Model
E2473 − 05 (2011)
10
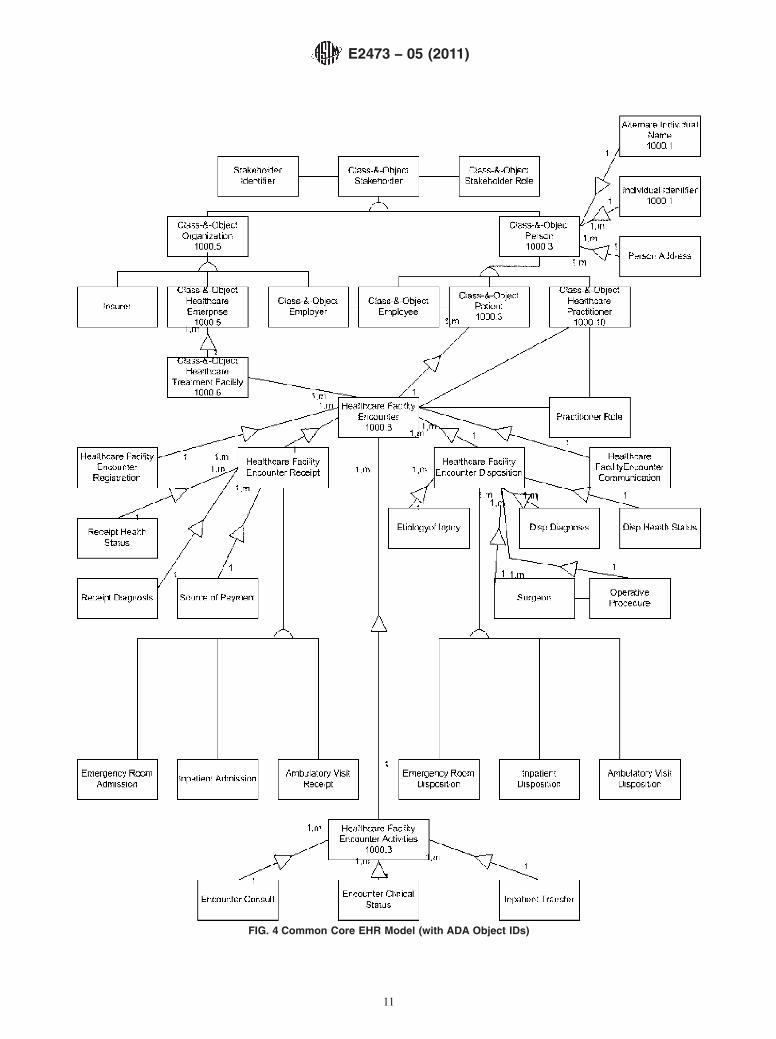
FIG. 4 Common Core EHR Model (with ADA Object IDs)
E2473 − 05 (2011)
11

FIG. 5 Common Core Occupational/Environmental Health EHR Model (with ADA Object IDs)
E2473 − 05 (2011)
12

5.3.2 Data Objects:
NOTE 1—National Committee Vital and Health Statistics Core Data Set are in italics.
NOTE 2—ASTM E1384 Minimal Data Set are underlined.
NOTE 3—HIPAA data elements are in bold.
NOTE 4—ADA 1000 series objects are so noted.
OrganizationORGANIZATION ADA 1000.5 ADA CONCEPT MODEL: ORGANIZATIONOrganization IdentifierOrganization NameAddressTelephone numberFAX NumberE-mail address
EmployerEMPLOYEREmployer ID---------------------------------------→ORGANIZATIONNumber of EmployeesCommercial Segment----------------------------→STANDARD INDUSTRIAL CODE
Healthcare EnterpriseHEALTHCARE ENTERPRISE ADA 1000.5Healthcare Enterprise Identifier -------------→ORGANIZATIONHealthcare Identifier (NPI)Healthcare Enterprise NameHealthcare Category-----------------------------→HEALTHCARE CATEGORY
Worker (Employee)EMPLOYEEEmployee Name----------------------------------→PERSONEmployee IdentifierEmployer------------------------------------------→EMPLOYERFunctional TitleCategoryRisk CodePay PlanJob IDJob TitleHire dateOccupation Code----------------------------------→OCCUPATIONSupervisor-----------→PERSONPrimary Worksite----------------------------------→WORK LOCATIONPrimary Work Operation-------------------------→WORK OPERATIONPersonal Protective Equipment------------------→STOCK ITEMApplicable Safety program (M)
Individual (Person)PERSON ADA 1000.3 ADA CONCEPT MODEL: INDIVIDUALPerson namePreviously Registered NameUniversal Patient IdentifierDate-time of BirthBirthplaceSex --------------------------------------------------→SEXRace ------------------------------------------------→RACEEthnic Group--------------------------------------→ETHNIC GROUPReligion ---------------------------------------------→RELIGIONMarital StatusEducation LevelOccupation -----------------------------------------→OCCUPATIONWork PhoneWork AddressCitizenship StatusHome AddressHome Address Location CodeHome Address County/Census tractTemporary AddressTemporary Address PhoneForeign Residence
PatientPATIENT ADA 1000.3Patient Name (Multiple) ------------------------→PERSON
E2473 − 05 (2011)
13

Adoption statusPatient NumberUniversal Patient Health NumberArchive DataLocation of ChartMultiple Birth MarkerBirth OrderSchool nameMilitary Service/Veteran StatusCurrent Work StatusCurrent Vocational StatusPrevious Occupations (M)----------------------→OCCUPATIONDate Completed OccupationNumber in HouseholdFamily Member Name (M) --------------------→FAMILY MEMBEREmergency Contact (relation/friend) NameEmergency Contact RelationshipEmergency Contact AddressEmergency Contact Home phoneEmergency Contact Business phonePatient Guardian Name--------------------------→PERSONPatient Guardian AddressPatient County/Census tractLNOK NameLNOK RelationshipLNOK AddressParental Marital StatusPatient’s LanguageInterpreter RequiredUsual Living Arrangement
Family MemberFAMILY MEMBER ADA 1000.3Family Member Name-------------------------→ PERSONFamily Member RelationshipFamily Member NameFamily Member SSANFamily Member Male ParentFamily Member Female ParentFamily Member SpouseFamily Member SexFamily Member DOBFamily Member Date of DeathFamily Member Head of Household StatusFamily Member Caregiver StatusFamily Member LocationFamily Member Occupation-------------------------------→OCCUPATIONFamily Member Major Diagnosis (M)
Segment II: Legal AgreementsConsent Signed/Admit AgreementPatient Rights AcknowledgementDirective to Physician
RECORD RELEASE INSTANCERelease of Information DatetimeType of Information ReleasedPerson Releasing
Segment III: FinancialPayment SourcePayer Group NoPayment SponsorAddress of Sponsor
Living Activity/OperationLIVING ACTIVITYLiving Activity NameLiving Activity Risk Assessment CodeAssociated Stressor (M)------------------------→STRESSORActivity Description
LocationLOCATION ADA CONCEPT MODEL: LOCATIONLocation IDLocation Name
Environmental Location ADA CONCEPT MODEL: ENVIRONMENT
E2473 − 05 (2011)
14
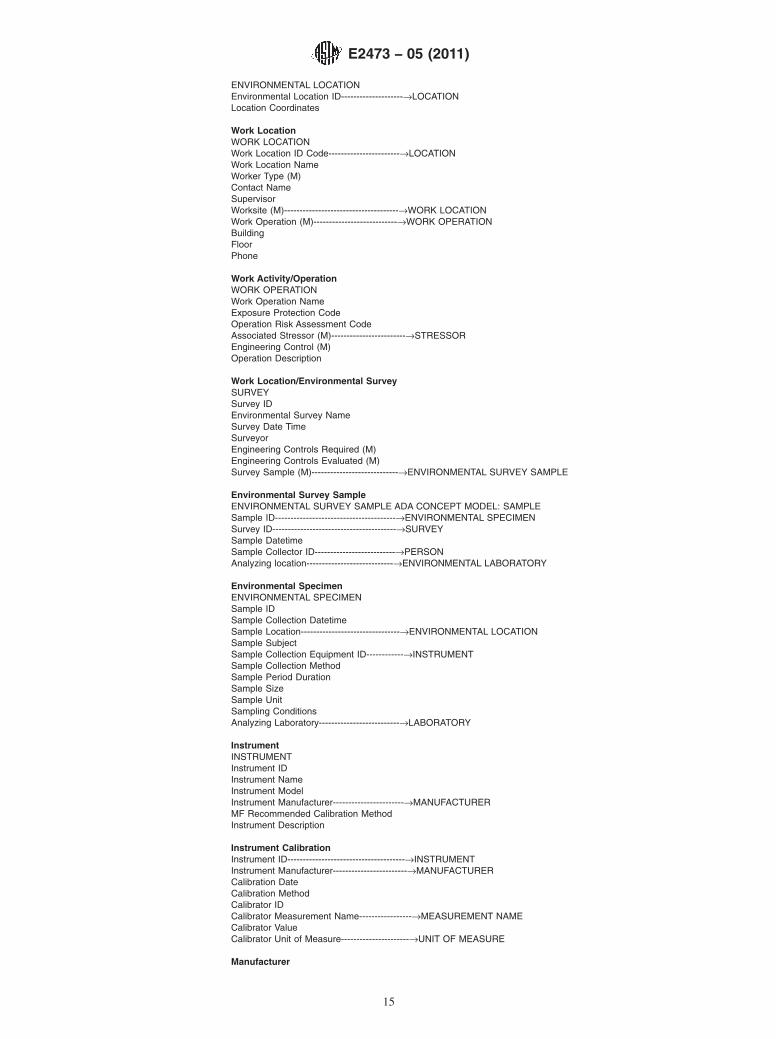
ENVIRONMENTAL LOCATIONEnvironmental Location ID--------------------→LOCATIONLocation Coordinates
Work LocationWORK LOCATIONWork Location ID Code-----------------------→LOCATIONWork Location NameWorker Type (M)Contact NameSupervisorWorksite (M)-------------------------------------→WORK LOCATIONWork Operation (M)---------------------------→WORK OPERATIONBuildingFloorPhone
Work Activity/OperationWORK OPERATIONWork Operation NameExposure Protection CodeOperation Risk Assessment CodeAssociated Stressor (M)------------------------→STRESSOREngineering Control (M)Operation Description
Work Location/Environmental SurveySURVEYSurvey IDEnvironmental Survey NameSurvey Date TimeSurveyorEngineering Controls Required (M)Engineering Controls Evaluated (M)Survey Sample (M)----------------------------→ENVIRONMENTAL SURVEY SAMPLE
Environmental Survey SampleENVIRONMENTAL SURVEY SAMPLE ADA CONCEPT MODEL: SAMPLESample ID---------------------------------------→ENVIRONMENTAL SPECIMENSurvey ID----------------------------------------→SURVEYSample DatetimeSample Collector ID--------------------------→PERSONAnalyzing location----------------------------→ENVIRONMENTAL LABORATORY
Environmental SpecimenENVIRONMENTAL SPECIMENSample IDSample Collection DatetimeSample Location--------------------------------→ENVIRONMENTAL LOCATIONSample SubjectSample Collection Equipment ID------------→INSTRUMENTSample Collection MethodSample Period DurationSample SizeSample UnitSampling ConditionsAnalyzing Laboratory--------------------------→LABORATORY
InstrumentINSTRUMENTInstrument IDInstrument NameInstrument ModelInstrument Manufacturer-----------------------→MANUFACTURERMF Recommended Calibration MethodInstrument Description
Instrument CalibrationInstrument ID--------------------------------------→INSTRUMENTInstrument Manufacturer------------------------→MANUFACTURERCalibration DateCalibration MethodCalibrator IDCalibrator Measurement Name-----------------→MEASUREMENT NAMECalibrator ValueCalibrator Unit of Measure----------------------→UNIT OF MEASURE
Manufacturer
E2473 − 05 (2011)
15
MANUFACTURERManufacturer Name-----------------------------→ORGANIZATIONManufacturer Industrial Classification
LaboratoryLABORATORYLaboratory ID--------------------------------------→ORGANIZATIONLab NameLaboratory CategoryLaboratory AddressLaboratory TelephoneLaboratory URL
Clinical LaboratoryCLINICAL LABORATORYClinical Lab ID-----------------------------------→LABORATORYHealthcare Enterprise----------------------------→HEALTH CARE ENTERPRISE
Environmental LaboratoryENVIRONMENTAL LABORATORYEnvironmental Lab ID---------------------------→LABORATORY
MeasurementMEASUREMENT NAMEMeasurement NameMeasurement IDMeasurement Usual Unit of Measure-------→UNIT OF MEASURE
Environmental MeasurementENVIRONMENTAL MEASUREMENTMeasurement Name-----------------------------→MEASUREMENT NAMEAnalyte Measured-------------------------------→STRESSORMeasured ValueTWAPeak ValueStandard Unit of Measure---------------------→UNIT OF MEASUREMeasurement DatetimeMeasurement Specimen DatetimeSpecimen ID------------------------------------→ENVIRONMENTAL SPECIMENEnvironmental Location-----------------------→ENVIRONMENTAL LOCATIONRelated Stressor---------------------------------→STRESSORMeasuring Laboratory-------------------------→ENVIRONMENTAL LABORATORYInterpretive Code
Patient Environmental StressorSTRESSOR EXPOSURE ADA CONCEPT MODEL: EXPOSUREStressor Type (M)--------------------------------→STRESSORStressor Total Lifetime ExposureStressor Unit of ExposureStressor Lifetime Milestone DateStressor Exposure Period (M)------------------→STRESSOR EXPOSURE PERIOD
Patient Environmental Stressor ExposureSTRESSOR EXPOSURE PERIODStressor Exposure begin date-timeStressor Exposure termination dateStressor Employer--------------------------------→EMPLOYERStressor Exposure SettingStressor Route of ExposureStressor Exposure Interval DoseStressor Plant Process CodeStressor Plant Location CodeStressor Work PerformedStressor Personal Protection used (M)
Patient Environmental Stressor MeasurementStressor Measurement DateStressor ID-------------------------------------→STRESSORForm of Measured AgentEnvironmental Specimen ID----------------→ENVIRONMENTAL SPECIMENUnits of Stressor Sample CollectedStressor Sample Unit of Measure-----------→UNIT OF MEASUREStressor Sample Collection DatetimeStressor Sample Collection DeviceStressor Test Sample MethodStressor Type of DeterminationStressor Peak Measurement ValueStressor Peak Measurement Unit
E2473 − 05 (2011)
16
StressorSTRESSORStressor IDStressor NameTrade Name (M)CAS NoRTECS CodeDescriptionMSDS Availability CodeSTELSTL Sampling DurationHazard Class
Occupational/Environmental CaseOCCUPATIONAL/ENVIRONMENTAL CASEOccupational/Environmental Case IDCase Patient ID------------------------------------→PATIENTHealthcare Enterprise-----------------------------→HEALTHCARE ENTERPRISECase Establishment DateCase DescriptionCase-related Health Conditions (M)----------→HEALTH CONDITIONAssociated Environmental Location---------→ENVIRONMENTAL LOCATIONInvolved Stressor(s) (M)------------------------→STRESSORAssociated Environmental Surveys (M)-----→ENVIRONMENTAL SURVEYAssociated Encounter Dates (M)---------------→ENCOUNTERCase StatusCase Resolution Date
AppointmentsSegment XIII: Appointments ADA 1000.15Date-time (M)Treatment FacilityExpected Duration 00868Clinic NamePrevious Encounter datetime--------------------------------→ENCOUNTERProvider ID-----------------------------------------------------→PRACTITIONERRequestor-------------------------------------------------------→PRACTITIONERPurpose/Chief Complaint 00866RemarksAppointment StatusExpected Services (M)Type 00867UrgencyCancellation ReasonCancellation DatetimeOverbook statusEncounter Disposition
EncounterENCOUNTER ADA CONCEPT MODEL: HEALTHCARE EVENTHEALTHCARE FACILITY ENCOUNTER ADA 1000.8Datetime of EncounterName of Facility of Encounter-------------------→HEALTHCARE ENTERPRISEEncounter statusCommentsType of EncounterPatient Chief ComplaintReason for Visit
HEALTHCARE ENCOUNTER RECEIPTSubSegment XIVA: Encounter ReceiptFacility TypeType of EncounterConfidentiality StatusEpisode IDMode of InjuryNature of InjuryChief ComplaintHealth Condition/Problem ID (M)-----------→HEALTH CONDITION/PROBLEMReceipt DiagnosisPractitioner ID
RECEIPT HEALTH STATUSReceipt Health Status Measure NameReceipt Health Status Measure Total ValueRECEIPT DIAGNOSISEncounter Receipt Diagnosis
E2473 − 05 (2011)
17

Encounter Receipt Health Status
SOURCE OF PAYMENTSource of Payment
HEALTHCARE ENCOUNTER ACTIVITIES
HEALTHCARE ENCOUNTER DISPOSITIONSubSegment XIVF/G: Encounter Disposition & ChargesDispositionDisposition Date timeDisposition DestinationPatient InstructionsDisposition NoteDisposition Note SignatureEncounter ChargesDisposition TypeFollowup ActionFollowup target date
DISPOSITION DIAGNOSIS: ADA CONCEPT MODEL: DIAGNOSISDisposition Diagnosis Name--→DIAGNOSISDiagnosis Type
DISPOSITION HEALTH STATUSDisposition Health Status Measure NameDisposition Health Status Measure Total Value
Health HistorySegment VIII: Health History ADA 1000.13Date of Health HistoryHistory Source Contact NameHistory Source RelationshipHistory Present Health TextPast History Social TextCurrent Habits TextHealth History Item (Multiple)
Segment VI: ImmunizationsImmunization Name (Multiple)Immunization Date (M)
ExamSegment IX: Examinations ADA 1000.12Date of ExaminationSource of History Present Illness/status Present HealthReview of SystemsExam Finding (Multiple)Exam Finding CommentExam Health Status Total Measure NameExam Health Status Total Measure ValueExam Summary
Patient/Environmental MeasurementSegment XI: Diagnostic Tests ADA 1000.13 ADA CONCEPT MODEL: HEALTH FACTDatetime of Test (Multiple)Clinical Order IDName of Requested Test-----------------------→MEASUREMENTTest Ordering FacilityTest Ordering PractitionerTest Performing FacilityTest PerformerDatetime Result ReportedTest Report Text (for Textual Reports)Analyte/Measurement/Observation Name (M)→MEASUREMENTAnalyte/Measurement/Observation ValueInterpretationMicroorganism Requested (M)Microorganism Attribute (M)Microorganism CommentsTest Comments
Health ConditionSegment V: Health Condition/Problem ADA 1000.14 ADA CONCEPT MODEL: HEALTH CONDITIONHealth Condition/Problem IDHealth Condition/Problem Name---------------→HEALTH CONDITIONHealth Condition/Problem Time of OnsetHealth Condition/Status
E2473 − 05 (2011)
18
Etiology--------------------------------------------→ETIOLOGY
Treatment PlanSegment X: Treatment Plans ADA 1000.15 ADA CONCEPT MODEL: TREATMENT PLANTreatment Plan IDTreatment Plan DescriptionHealth Condition/Problem ID------------------→HEALTH CONDITION/PROBLEMTreatment Plan Phase (M)
Clinical OrderSegment X: Clinical Orders ADA CONCEPT MODEL: COMMUNICATIONClinical Order IDClinical Order DatetimeClinical Order Full Text
ManufacturerManufacturer ID----------------------------------→ORGANIZATIONManufacturer NameProduct ID (M)
Public Health AgencyPublic Health Agency Organizational ID----→ORGANIZATION
Environmental Monitoring PlanEnvironmental Monitoring Plan IDEnvironmental Monitoring Plan NameEnvironmental Monitoring Plan Description
Environmental Remediation PlanEnvironmental Remediation Plan IDEnvironmental Remediation Plan NameEnvironmental Remediation Plan Description
Stock ItemStock Item Product IDStock Item Name
VOCABULARIES and REFERENTIAL CONTEXT-INSENSITIVE DATA: ADA 1000.2
Measurement NameMEASUREMENT NAMEMeasurement NameMeasurement LOINC IDMeasurement Payment Code
ObservationOBSERVATIONObservation IdentifierObservation Name
Unit of MeasureUNIT OF MEASURE [ADA 1000.14]Unit of Measure IDUnit of Measure Name/Unit of Measure TermUnit of Measure AbbreviationUnit of Measure CodeUnit of Measure System
OccupationOCCUPATION [ASTM/ADA]Occupation IDOccupation NameOccupation Identifier
RaceRACERace/Biologic Population IDRace/Biologic Population Name
ReligionRELIGION RELIGION [ADA 1000.3]Religion IDReligion NameReligion CodeSect Name
Sex CharacteristicSEX CHARACTERISTIC [ADA 1000.3]
E2473 − 05 (2011)
19
Sex Characteristic CodeSex Characteristic description
SexSEXSex IDSex Name
Ethnic GroupETHNIC GROUPEthnic Group IDEthnic Group Name
LanguageLANGUAGE [ADA 1000.3]Language CodeLanguage NameDialect Name
Marital (Pair-Bond) StatusMARITAL STATUS [ADA]Marital Status CodeMarital Status description
Healthcare CategoryHEALTHCARE CATEGORYHealthcare Category IDHealthcare Category Name
Health ConditionHEALTH CONDITION/PROBLEM [ADA 1000.10]Health Condition/Problem IdentifierHealth Condition/Problem Name
DiagnosisDIAGNOSIS [ADA 1000.10]Diagnosis IdentifierDiagnosis Term
ProcedurePROCEDURE [ADA 1000.10]Procedure IdentifierProcedure TermProcedure TypeProcedure mnemonicADA Procedure codeBase valueProcedure Description
MaterielMATERIEL [ADA 1000.9] ADA CONCEPT MODEL: MATERIELMateriel IdentifierMateriel Name
OutcomeOUTCOME [ADA 1000.10]Outcome IdentifierOutcome Term codeOutcome description
PopulationPOPULATION [ADA 1000.12]Population IdentifierPopulation Name
Quantitative MeasureQUANTITATIVE MEASURE [ADA 1000.14]Quantitative Measure TermQuantitative Measure Description
TaxonomyTAXONOMY [ADA 1000.3]Taxonmy IdentifierTaxonomy Name
Etiology ADA CONCEPT MODEL: ETIOLOGYETIOLOGY [ADA 1000.14]Etiology Code
E2473 − 05 (2011)
20
Etiology type
Service ADA CONCEPT MODEL: TREATMENTSERVICE [ADA 1000.16]Service IdentifierService TermService TypeService Description
LocationLOCATION [ADA 1000.6]Location IdentifierLocation Name
Anatomic Location ADA CONCEPT MODEL: ANATOMIC LOCATIONANATOMIC LOCATION [ADA ]Anatomic CodeAnatomic Location Type
Laboratory ProcedureLABORATORY PROCEDURE [ASTM]Laboratory Procedure IdentifierLaboratory Procedure NameICD-10 PCS Code
REFERENCES
(1) Public Health Data Standards Consortium: PHDSC Ad Hoc TaskForce on Electronic Health Records—Public Health “White PaperElectronic Health Records: Public Health Perspectives,” 8 March2004, Baltimore, MD.
(2) PHIN Standards Specification v1.2 (http://cdc.gov/phin/index.htm).
ASTM International takes no position respecting the validity of any patent rights asserted in connection with any item mentionedin this standard. Users of this standard are expressly advised that determination of the validity of any such patent rights, and the riskof infringement of such rights, are entirely their own responsibility.
This standard is subject to revision at any time by the responsible technical committee and must be reviewed every five years andif not revised, either reapproved or withdrawn. Your comments are invited either for revision of this standard or for additional standardsand should be addressed to ASTM International Headquarters. Your comments will receive careful consideration at a meeting of theresponsible technical committee, which you may attend. If you feel that your comments have not received a fair hearing you shouldmake your views known to the ASTM Committee on Standards, at the address shown below.
This standard is copyrighted by ASTM International, 100 Barr Harbor Drive, PO Box C700, West Conshohocken, PA 19428-2959,United States. Individual reprints (single or multiple copies) of this standard may be obtained by contacting ASTM at the aboveaddress or at 610-832-9585 (phone), 610-832-9555 (fax), or [email protected] (e-mail); or through the ASTM website(www.astm.org). Permission rights to photocopy the standard may also be secured from the ASTM website (www.astm.org/COPYRIGHT/).
E2473 − 05 (2011)
21

















![INDEX [assets.tequipment.net] · INDEX 491 A Abbreviations, ... ANSI B94.25 391 ANSI keyseat dimensions 262 ... ANSI/ASME B1.13M-1983 280, 396 ANSI/ASME B18.3 314](https://static.fdocuments.us/doc/165x107/5b6991367f8b9a68538e3fe0/index-index-491-a-abbreviations-ansi-b9425-391-ansi-keyseat-dimensions.jpg)
