Spontaneous Esophageal Rupture 修改后
59
SPONTANEOUS SPONTANEOUS ESOPHAGEAL RUPTURE ESOPHAGEAL RUPTURE Su HaiY an DEPARTMENT OF EMERGENCY MEDICINE, THE FIRST CLINICAL COLLEGE OF TIANJIN MEDICAL UNIVERSITY
-
Upload
deep-deep -
Category
Health & Medicine
-
view
2.245 -
download
4
description
spontaneous esophageal rupture
Transcript of Spontaneous Esophageal Rupture 修改后

SPONTANEOUS SPONTANEOUS ESOPHAGEAL ESOPHAGEAL
RUPTURERUPTURE
Su HaiYan
DEPARTMENT OF EMERGENCY MEDICINE,
THE FIRST CLINICAL COLLEGE OF TIANJIN MEDICAL UNIVERSITY

AnatomyGeneral considerationsPathophysiologyDiagnosisTreatmentPrognosis

Anatomy of Esophagus

Anatomy of EsophagusAnatomy of Esophagus
The wall of the digestive tube from the mouth to the anus is composed of four basic layers or tunics.

Anatomy of EsophagusAnatomy of Esophagus
Tunica serosa is the outermost covering of the digestive tube. In most of the digestive tract (stomach and intestines) it consists of a thin layer of loose connective tissue covered by mesothelium (a type of squamous epithelium that lines body cavities); within the peritoneal cavity, this structure is also referred to as visceral peritoneum.

Anatomy of EsophagusAnatomy of Esophagus
In the abdominal cavity, the serosa on each side of the tube fuses together to form a suspensory structure called mesentery, which houses vascular and nervous supplies to the digestive tract and is continuous with the lining of the cavity.

Anatomy of EsophagusAnatomy of Esophagus
In regions outside of the abdominal cavity where the digestive tube is essentially affixed to adjacent structures via its outer layer of connective tissue (esophagus and rectum), this tunic is referred to as tunica adventitia instead of tunica serosa.

Anatomy of EsophagusAnatomy of Esophagus
Tunica adventitia : irregular dense connective tissue (ct) blends with surrounding ct.

Anatomy of EsophagusAnatomy of Esophagus
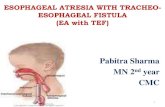
The esophagus extends from the pharynx in the neck through the posterior mediastina and pierces the diaphragm at the level of the tenth thoracic vertebra.

Anatomy of EsophagusAnatomy of Esophagus
Complicated muscular tube
Skeletal in upper third; mixed with smooth mus
cle in middle third; smooth in lower third;

Anatomy of EsophagusAnatomy of Esophagus
The oesophagus (or gullet) is a complicated muscular tube that carries food and fluid from the throat to the stomach passing through the chest. There is a muscular sphincter (opening) at each end to prevent the stomach contents from refluxing back up the oesophagus.

Anatomy of EsophagusAnatomy of Esophagus
The lowest of these sphincters is positioned at the junction between the oesophagus and the stomach (level with the diaphragm).

Anatomy of EsophagusAnatomy of Esophagus
Three narrow points:
Cricoid cartilageBifurcation of the t
racheaDiaphragmatic hia
tus

Anatomy of EsophagusAnatomy of Esophagus
Length of esophagus is about 20-24cm.
Divide three portions :CervicalThoracicAbdominal

General Consideration

General ConsiderationGeneral Consideration
The abbreviation of Spontaneous Esoph
ageal Rupture is SER.SER is also termed as Boerhaav
e’s syndrome.

General ConsiderationGeneral Consideration
SER is first reported by Boerhaave. He described the death of a Dutch after
he overindulged in wine and subsequently vomited.
The autopsy revealed a ruptured esophagus and gastric contents polluted the pleural space.

General ConsiderationGeneral Consideration
The etiology is overindulgent ingestion of food and alcohol and subsequently nausea , vomit.
Other causes such as blunt trauma , childbirth,laughing and so on.

General ConsiderationGeneral Consideration
It often occurs in middle-aged males. Female and neonatal cases have also
been reported. The diagnosis relies on history ,physical
examination and laboratory data. Diagnosis and operative treatment at an
early stage is crucial to the prognosis.

Pathophysiology

PathophysiologyPathophysiology
Spontaneous rupture may occur just above the diaphragm in the left posterior lateral wall of the esophagus.
This intrinsic weakness has been demonstrated in the esophagus of cadavers.
Perforations are usually longitudinal (0.6-8.9 cm long), with the left side more commonly affected than the right (90%).

PathophysiologyPathophysiology Vomiting is
forcing the contents of the stomach up through the esophagus and out of the mouth.

PathophysiologyPathophysiology Vomiting is a forceful
action accomplished by a fierce, downward contraction of the diaphragm. At the same time, the abdominal muscles tighten suddenly against a relaxed upper stomach with an open sphincter. The contents of the stomach are propelled up and out.

PathophysiologyPathophysiology
A disorganized vomiting reflex in which the upper esophageal sphincter fails to relax during vomiting leads to increase in esophageal pressure. The pressure of pleural space is lower than the intra-esophageal pressure. When intra-esophageal pressure is increased, the lack of striated muscle and the vertical arrangement of longitudinal muscles in lower esophagus make it weak and amenable to rupture.

PathophysiologyPathophysiology
Other areas have rarely been reported to rupture and create an emetic in
jury like that of Boehaave,s syndrom
e:CervicalMidthoracicInfradiaphragmatic sites

PathophysiologyPathophysiology
More than 80% of these injuries occur in middle-aged males following the overindulgent ingestion of food and alcohol.

PathophysiologyPathophysiology
A tear similar to that seen in cases of B
oehaave,s syndrome requires a force of
3 to 6 lb/in ,which may be generated in vivo by gastric pressure caused by emesis.

PathophysiologyPathophysiology
Increasing intraabdominal pressure cause this injury:Blunt traumaSeizuresChildbirthLaughingStraining at stoolHeavy lifting

Diagnosis

Diagnosis Diagnosis
HistoryPhysical examinationLaboratory

Diagnosis Diagnosis
1.Symptoms The most reliable symptom of an esoph
ageal injury is pain localized along the course of the esophagus.The pain usually is pleuritic. It may be exacerbated by swallowing and by neck flexion. It may be located in the epigastrium, substernal area, or the back.

DiagnosisDiagnosis
As the process advances, the pain worsens over time and moves from the abdomen into the chest, the patient may experience dyspnea and shock.

DiagnosisDiagnosis
2.Signs The early physical signs of esophageal
perforation are sparse. As air and caustic contaminated materia
l move through the esophageal tear into the mediastinum and pleural space, the true gravity of the condition becomes manifest. This mediastinal air may surround the heart and produce a systolic crunching.

DiagnosisDiagnosis
When air and fluid move into the pleural space, it may result in the signs of hydropneumothorax and empyema.
When air travels into subcutaneous tissues, subcutaneous emphysema may become evident. This classic sign is present in only about 60% of these patients.

DiagnosisDiagnosis
As the infective and inflammatory process advances, the patients may manifest the signs of cardiopulmonary collapse and sepsis with fever, cyanosis, hypotention, anuria,and eventually death.

DiagnosisDiagnosis
3. Laboratory Examination
3.1 The pleural effusion liquid examinationVery low PHHigh level of salivary amylase

DiagnosisDiagnosis
3.2 Radiographic ExaminationMediastinal air with or without subcutaneous e
mphysemaLeft-side pleural effusion PneumothoraxWidened mediastinum

DiagnosisDiagnosis
At an early stage the radiographic examination may be normal.1~2 hours later it may take on mediastinal air with or without subcutaneous emphysema. Several hours later it may take on widened mediastinum. Left-side pleural effusion ,PneumothoraxAnd hydropneumothorax may also occur.

DiagnosisDiagnosis
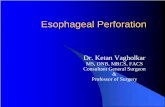
Esophagram is a useful procedure in diagnosing esophageal injuries.
The esophagus is barium-filled. Barium flow from esophagus through the perforation.

DiagnosisDiagnosis
It is, however, up to 25% of these studies have false-negative results. It is generally recommended that the initial study employ a water-soluble agent, and then if no gross leak is demonstrated, a barium study may be undertaken to better define the mucosal detail.

DiagnosisDiagnosis
3.3 Endoscopy Examination:Endoscopy is not an infallible aid
in establishing the presence or absence of an esophageal perforation.

DiagnosisDiagnosis

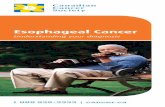
This 36-year-old man presented with hematemesis after an alcoholic binge. Endoscopy shows oozing blood from a base of a clot overlying a Mallory-Weiss tear (arrow).

Posteroanterior chest radiograph shows a right-sided hydropneumothorax after an esophageal rupture.

Nonenhanced CT scan through the mid esophagus in a patient with esophageal perforation after upper GI endoscopy shows a false tract emanating from the esophagus (arrow).

DiagnosisDiagnosis
The diagnosis of any esophageal perforation rests primarily on the clinician
,s hig
h index of suspicion for this injury. In patients with the classic Boehaave
,s syndr
ome with overindulgence and emesis followed by severe chest pain, subcutaneous emphysema, and cardiopulmonary collapse, the diagnosis is readily confirmed.

DiagnosisDiagnosis
Up to one third of cases of a perforated esophagus, however, are atypical.
About 25% of patients with Boehaave,s
syndrome have no history of emesis. In almost 50% of those who do vomit, th
e relationship between the vomiting and the onset of pain does not suggest an emetic injury.

DiagnosisDiagnosis
Only a careful history and physical examination supplemented with appropriate laboratory and x-ray studies enable the clinician to diagnose a subtle case at an early stage.

Differential diagnosis

Different diagnosisDifferent diagnosis
Pulmonary embolusAcute myocardial infarction (AMI)PancreatitisPerforated peptic ulcerCholecystitisAortic aneurysm

Different diagnosisDifferent diagnosis
1. Pulmonary embolus: Pulmonary embolism can be defined as the
occlusion of one or more vessels in the pulmonary arterial tree by matter from a source extrinsic to the lung. The process is almost invariably acute but may on occasion be chronic. The diagnosis should be based on the presence risk factors, symptoms,chest radiograph, ventilation/perfusion lung scanning, pulmonary angiography etc.

Different diagnosisDifferent diagnosis
2. Acute myocardial infarction (AMI) :
AMI results from prolonged myocardial ischemia. The diagnosis depends on history, changes of ECG, and characteristic cardiac enzymes.

Different diagnosisDifferent diagnosis
3. Pancreatitis: Acute pancreatitis is an acute infla
mmatory disorder with abdominal pain associated with elevations of pancreatic enzymes, and it is a common disorder that may vary in severity from mild to fulminant.

Treatment

TreatmentTreatment
1. Non-operative treatment: Given nothing by mouth; Broad-spectrum intravenous antibiotics. Volume replacement and other support as ne
eded; A nasogastric tube should be carefully passe
d to decompress the stomach. Patients should be given parenteral nutrition
(PN) for at least 10d while they are given nothing by mouth.

TreatmentTreatment
2. Operative treatment:If the patient’s condition fails to
improve or deteriorates within 24h of initiation of non-operative treatment, strong consideration should be given to operative management.

Prognosis

PrognosisPrognosis
Predicting a poor prognosis:Poor general medical consideration, most notably the presence of esophageal cancer;Spontaneous perforation; Greater than 24h delay prior to diagnosis and initiation of treatment.

THANK YOU!