Smoking related interstitial lung diseases
112
Smoking-related Interstitial Lung Diseases The Never-Ending Story of Smoke and Disease
-
Upload
elshazly -
Category
Health & Medicine
-
view
149 -
download
1
Transcript of Smoking related interstitial lung diseases

Smoking-related Interstitial Lung Diseases
The Never-Ending Story of Smoke
and Disease

Smoking-related Interstitial Lung Diseases
Mostafa ElshazlyMD, FCCP,ERSD,
Professor of Pulmonary MedicineChairman of PVRU
Kasr ElAini School Of Medicine Cairo University

Smoking-related Interstitial Lung Diseases
Mostafa ElshazlyMD, FCCP,ERSD,
Professor of Pulmonary MedicineChairman of PVRU
Kasr ElAini School Of Medicine Cairo University

Smoking-related Interstitial Lung Diseases
Cigarette smoke is a complex mixture of more
than 6,000 compounds and causes a variety of
pulmonary and systemic effects in humans .
Smoking remains the most preventable cause of
premature death and morbidity in the United
States and throughout the developed world .
Cigarette smoking is the major cause of lung
cancer, which in turn is the leading cause of
cancer deaths in both males and females in the
United States .

Smoking-related Interstitial Lung Diseases
Cigarette smoke is a complex mixture of more
than 6,000 compounds and causes a variety of
pulmonary and systemic effects in humans .
Smoking remains the most preventable cause of
premature death and morbidity in the United
States and throughout the developed world .
Cigarette smoking is the major cause of lung
cancer, which in turn is the leading cause of cancer
deaths in both males and females in the United
States .

Smoking-related Interstitial Lung Diseases
Cigarette smoke is a complex mixture of more
than 6,000 compounds and causes a variety of
pulmonary and systemic effects in humans .
Smoking remains the most preventable cause of
premature death and morbidity in the United
States and throughout the developed world .
Cigarette smoking is the major cause of lung
cancer, which in turn is the leading cause of
cancer deaths in both males and females in the
United States .

Smoking-related Interstitial Lung Diseases

Smoking-related Interstitial Lung Diseases
• Smoking-induced lung diseases constitute
a complex group of disorders, varying from
the well- known entity of chronic
obstructive pulmonary disease (COPD) to
the more recently described interstitial
lung diseases (ILDs) 1,2
1. Baumgarten Kbet al., Cigarette smoking: a risk factor for idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 1997;155:242–248.2. Heynemann LE, et al., RB,RB_ILD,and DIP : different entities or part of the spectrum of the same disease process? AJR Am J Roentgenol 1999;173:1617–1622.

• Smoking-related ILD is a term used to describe the relationship between
– RB-associated ILD (RB-ILD),
– Desquamative interstitial pneumonia (DIP), and
– Pulmonary Langerhans’ cell histiocytosis
(PLCH)
• as interstitial disorders that are
etiologically linked to cigarette smoking 1 .
Smoking-related Interstitial Lung Diseases
Moon J, du Bois RM, Colby TV, Hansell DM, Nicholson AG. Clinical significance of respiratory bronchiolitis on open lung biopsy and its relationship to smoking related interstitial lung disease. Thorax 1999; 54:1009–1014.

Copyright © American College of Chest Physicians. All rights reserved.
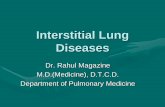
The Overlap Between Respiratory Bronchiolitis and Desquamative Interstitial Pneumonia in Pulmonary Langerhans Cell Histiocytosis*: High-Resolution CT, Histologic, and Functional Correlations
Chest. 2003;124(4):1199-1205. doi:10.1378/chest.124.4.1199
Nonproportional Venn diagram illustrating the spectrum of airways and interstitial injury associated with cigarette smoking. The larger outer circle represents the virtually universal occurrence of RB in smokers. Emphysema will develop in approximately 20% of these smokers during their lifetime. ILD will develop in a small proportion of smokers due to DIP or PLCH. In a significant proportion of those in whom DIP or PLCH develops (or overlaps of both), there is accompanying emphysema (as in the current series). which provides evidence that RBILD, DIP and PLCH form a spectrum of interstitial patterns of lung injury related to cigarette smoke .

• This direct causative role for smoking in the pathogenesis of these disorders is based on significant epidemiological data:– Consistent preponderance of smokers within
this population– Potential of disease remission upon smoking
cessation– the existence of similar lesions, namely
respiratory bronchiolitis, in healthy smokers without ILD, and
– the presence of a combination of these lesions in some affected smokers 1,2 .
Smoking-related Interstitial Lung Diseases
1.Ryu JH, Colby TV, Hartman TE, et al. Smoking-related interstitial lung diseases: a concise review. Eur Respir J 2001; 17: 122–132. 20.Vassalo R, Ryu JH. Tobacco smoke-related diffuse lung diseases. Semin Respir Crit Care Med 2008; 29: 643–650.

• This direct causative role for smoking in the pathogenesis of these disorders is based on significant epidemiological data:– Consistent preponderance of smokers within
this population– Potential of disease remission upon smoking
cessation– Existence of similar lesions, Respiratory
Bronchiolitis, in healthy smokers without ILD, and
– The presence of a combination of these lesions in some affected smokers 1,2 .
Smoking-related Interstitial Lung Diseases
1.Ryu JH, Colby TV, Hartman TE, et al. Smoking-related interstitial lung diseases: a concise review. Eur Respir J 2001; 17: 122–132. 20.Vassalo R, Ryu JH. Tobacco smoke-related diffuse lung diseases. Semin Respir Crit Care Med 2008; 29: 643–650.

• Pathogenesis
Smoking-related Interstitial Lung Diseases

Smoking-related Interstitial Lung Diseases

Smoking-related Interstitial Lung Diseases
• Pathogenesis• Cigarette smoke can injure the
endothelial and the alveolar
epithelial cells by increasing
oxidative stress and enhancing
virus induced parenchymal
inflammation.
• Such injury could lead to
abnormal wound healing and
parenchymal fibrosis in
susceptible individualsSmoking-related Interstitial Lung
Diseases

Smoking-related Interstitial Lung Diseases
• Pathogenesis• Cigarette smoke can injure the
endothelial and the alveolar
epithelial cells by increasing
oxidative stress and enhancing
virus induced parenchymal
inflammation.
• Such injury could lead to
abnormal wound healing and
parenchymal fibrosis in
susceptible individuals

Smoking-related Interstitial Lung Diseases

Smoking-related Interstitial Lung Diseases


Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)
• Is a rare, mild inflammatory pulmonary disorder
that occurs almost exclusively in current or
former heavy smokers, usually between the third
and sixth decades, most likely with no gender
predilection.
Sieminska and Kuziemski: Respiratory bronchiolitisinterstitial lung disease. Orphanet Journal of Rare Diseases 2014 9:106.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)
• Epidemiology
• The prevalence and incidence of RB-ILD is
unknown and has remained difficult to assess for
many years.
• In several earlier case series, the incidence of RB-
ILD & DIP, 10%–17% of the study samples 1,2 .
• RB-ILD was recorded separately in only two of
these case series, and accounted for 2% and 13%
of cases 3.
1. Bjoraker JA, et al., Prognostic significance of histopathologic subsets in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 1998, 157:199–203. 2.Nicholson AG, et al.,: The prognostic significance of the histologic pattern of interstitial pneumonia in patients presenting with the clinical entity of cryptogenic fibrosing alveolitis. Am J Respir Crit Care Med 2000, 162:2213–2217. 3. Flaherty KR, et al., Clinical significance of histological classification of idiopathic interstitial pneumonia. Eur Respir J 2002, 19:275–83.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)
• Epidemiology
• In KSA register of newly diagnosed ILD cases, RB-
ILD cases accounted for 5.5% of all types of IIPs 1
.
• A German pathology review of ILD cases revealed
9.5% of RB-ILD cases among all types of IIPs 2 .
1.Alhamad EH: Interstitial lung diseases in Saudi Arabia: a single-center study. Ann Thorac Med 2013, 8:33–7.2. Theegarten D, Müller HM, Bonella F, Wohlschlaeger J, Costabel U: Diagnostic approach to interstitial pneumonias in a single centre: report on 88 cases. Diagn Pathol 2012, 7:160–171.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• Clinical description
• Insidious onset of
– Exertional dyspnea,
– Symptomatic wheezing, and
– Persistent cough, which may be non-productive.
• Bibasilar end-inspiratory crackles are the most
common signs.
Portnoy J, Veraldi KL, Schwarz MI, Cool CD, Curran-Everett D, Cherniack RM, King TE Jr, Brown KK: Respiratory bronchiolitis-interstitial lung disease:long-term outcome. Chest 2007, 131:664–671.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• Physiologic changes
• Obstructive pattern was the most common
pulmonary function defect (47%)
• Pure restriction or mixed defects were less
common (31% and 9%, respectively)
• 13% of patients had normal spirometry data .
Portnoy J, Veraldi KL, Schwarz MI, Cool CD, Curran-Everett D, Cherniack RM, King TE Jr, Brown KK: Respiratory bronchiolitis-interstitial lung disease:long-term outcome. Chest 2007, 131:664–671.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• Physiologic changes
• Patients with minimal symptoms usually
reveal a mild to moderate decrease in DLco.
• Patients with more severe symptoms, both
airway obstruction and restriction or
occasionally an isolated increase in RV may
be found .Myers JL, Veal CF Jr, Shin MS, Katzenstein AL: Respiratory bronchiolitis causing interstitial lung disease: a clinicopathological study of six cases. Am Rev Respir Dis 1987, 135:880–4.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• Radiographic findings
• Radiographic findings are usually relatively
subtle.
• Normal chest radiographs ( 20% to 28%) .
• Fine reticulonodular interstitial opacities, which
are diffuse or are predominant in basal lung
areas . 1, 2
Park JS, et al.,: Respiratory bronchiolitis-associated interstitial lung disease: radiologic features with clinical and pathologic correlation. J Comput Assist Tomogr 2002, 26:13–20.Heyneman LE, et al.,: RB,RB-ILD,DIP different entities or part of the spectrum of the same disease process. Am J Roentgenol 1999, 173:1617–22.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• High-Resolution CT Findings of RB-ILD
– Centrilobular nodular opacities– Patchy ground-glass opacity– Bronchial wall thickening– Upper lobe predominance– Associated centrilobular emphysema– Air trapping at expiration– Findings of fibrosis absent
Park JS, et al.,: Respiratory bronchiolitis-associated interstitial lung disease: radiologic features with clinical and pathologic correlation. J Comput Assist Tomogr 2002, 26:13–20.Anil K. Attili, et al., Smoking-related Interstitial Lung Disease: Radiologic-Clinical-Pathologic Correlation. RadioGraphics 2008; 28:1383–1398

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• High-Resolution CT Findings of RB-ILD
– Centrilobular nodular opacities– Patchy ground-glass opacity– Bronchial wall thickening– Upper lobe predominance– Associated centrilobular emphysema– Air trapping at expiration– Findings of fibrosis absent

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• High-Resolution CT Findings of RB-ILD
– Centrilobular nodular opacities– Patchy ground-glass opacity– Bronchial wall thickening– Upper lobe predominance– Associated centrilobular emphysema– Air trapping at expiration– Findings of fibrosis absent

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• High-Resolution CT Findings of RB-ILD
– Patchy ground-glass opacity– Bronchial wall thickening

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• High-Resolution CT Findings of RB-ILD
– Upper lobe predominance

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• High-Resolution CT Findings of RB-ILD
– Associated centrilobular emphysema

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• High-Resolution CT Findings of RB-ILD
– Associated centrilobular emphysema
HRCT image of the upper lung lobes shows centrilobular nodules (white arrows), patchy ground-glass opacities (black arrow), and mild coexisting centrilobular emphysema (arrowhead).

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)Histopathologic Findings Pigmented
macrophages in a terminal bronchiole and the adjacent alveoli (arrows), and
Moderate Peribronchiolar inflammation and fibrosis (arrowhead) are present.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• Bronchoalveolar lavage
– An increased total number of cells with a
normal cellular differential analysis .
– or an increase in the percentage of
macrophages.
– A modest increase in neutrophils may also be
present.
Hunninghake GW, Crystal RG: Cigarette smoking and lung destruction: accumulation of neutrophils in the lungs of cigarette smokers. Am Rev Respir Dis 1983, 128:833–838.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• Diagnosis
• It is increasingly accepted that a diagnosis of RB-
ILD is secure when based upon
– Typical HRCT findings (ground-glass opacities and
centrilobular nodules)
– In a current smoker, especially when
– BAL findings (the presence of smokers’ macrophages
and the absence of lymphocytosis) are also compatible.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• Management and disease course
• Smoking cessation is considered the most
important factor in the management of RB-ILD.
• It is also unclear whether patients with RB-ILD
benefit from corticosteroid therapy with regard to
the natural history of the disease.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• Management and disease course• The course of RB-ILD is heterogeneous, often with
no functional improvement and with disease progression despite smoking cessation and treatment 1,2,3 .
• Clinical worsening was common, as well as worsening of spirometry results and gas exchange, regardless of smoking status and treatment ordered, including corticosteroids 3.
• RB-ILD is now less commonly regarded as a benign entity.
Moon J, et al.,: Clinical significance of respiratory bronchiolitis on open lung biopsy and its relationship to smoking related interstitial lung disease. Thorax 1999, 54:1009–14. 2. Ryu JH, et al.,:Desquamative interstitial pneumonia and respiratory bronchiolitis–associated interstitial lung disease. Chest 2005, 127:178–184.3. Portnoy J, Veraldi KL, Schwarz MI, Cool CD, Curran-Everett D, Cherniack RM, King TE Jr, Brown KK: Respiratory bronchiolitis-interstitial lung disease: long-term outcome. Chest 2007, 131:664–671.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• Management and disease course• The course of RB-ILD is heterogeneous, often with
no functional improvement and with disease progression despite smoking cessation and treatment 1,2,3 .
• Clinical worsening was common, as well as worsening of spirometry results and gas exchange, regardless of smoking status and treatment ordered, including corticosteroids 3.
• RB-ILD is now less commonly regarded as a benign entity.
Moon J, et al.,: Clinical significance of respiratory bronchiolitis on open lung biopsy and its relationship to smoking related interstitial lung disease. Thorax 1999, 54:1009–14. 2. Ryu JH, et al.,:Desquamative interstitial pneumonia and respiratory bronchiolitis–associated interstitial lung disease. Chest 2005, 127:178–184.3. Portnoy J, Veraldi KL, Schwarz MI, Cool CD, Curran-Everett D, Cherniack RM, King TE Jr, Brown KK: Respiratory bronchiolitis-interstitial lung disease: long-term outcome. Chest 2007, 131:664–671.

Respiratory Bronchiolitis Associated
Interstitial Lung Disease (RB-ILD)• Management and disease course• The course of RB-ILD is heterogeneous, often with
no functional improvement and with disease progression despite smoking cessation and treatment 1,2,3 .
• Clinical worsening was common, as well as worsening of spirometry results and gas exchange, regardless of smoking status and treatment ordered, including corticosteroids 3.
• RB-ILD is now less commonly regarded as a benign entity.
Moon J, et al.,: Clinical significance of respiratory bronchiolitis on open lung biopsy and its relationship to smoking related interstitial lung disease. Thorax 1999, 54:1009–14. 2. Ryu JH, et al.,:Desquamative interstitial pneumonia and respiratory bronchiolitis–associated interstitial lung disease. Chest 2005, 127:178–184.3. Portnoy J, Veraldi KL, Schwarz MI, Cool CD, Curran-Everett D, Cherniack RM, King TE Jr, Brown KK: Respiratory bronchiolitis-interstitial lung disease: long-term outcome. Chest 2007, 131:664–671.


Desquamative Interstitial Pneumonia (DIP)

Desquamative Interstitial Pneumonia (DIP)
It was originally defined by Liebow et al. in 1965 1.
In the following 2 decades it was considered as the
putative early stage of the usual interstitial
pneumonia (UIP) 2
Initially, it was believed that its histological feature
was the desquamation of epithelial cells, but then it
was recognized that the presence of intra-alveolar
macrophages was due to an alveolar filling process 3.1.Liebow AA, et al.,. Desquamative interstitial pneumonia. Am J Med 1965; 39: 369–404. 2.Tubbs RR, et al. Desquamative interstitial pneumonitis. Cellular phase of fibrosing alveolitis. Chest 1977; 72: 159–165.3. Ryu JH, et al. Desquamative interstitial pneumonia and respiratory bronchiolitis-associated interstitial lung disease. Chest 2005; 127: 178–184.

Desquamative Interstitial Pneumonia (DIP)
DIP is associated to tobacco in nearly 80–90% of patients 1 but, could also be associated to many drugs 2
systemic disorders 3
environmental exposures 4
and infections 4
In addition, it also has been described in children .
1.ATS-ERS. International multidisciplinary consensus. Classification of the IIPs. Am J Respir Crit Care Med 2002;165: 277–30. 2. Corrin B, Price AB. Electron microscopic studies in desquamative interstitial pneumonia associated with asbestos. Thorax 1972; 27:324–331. 3.Abraham JL, Hertzberg MA. Inorganic particles associated with desquamative interstitial pneumonia. Chest 1981; 80: 67–70. 4. Craig JP, Wells AU, Doffman S, et al. Desquamative interstitial pneumonia, respiratory bronchiolitis and their relationship to smoking. Histopathol 2004; 45: 275–282

Desquamative Interstitial Pneumonia (DIP)
The average age at the onset of symptoms is about 40 years 1
Male-Female ratio of 2 : 1 2
Clinical presentation of DIP is Insidious and is characterized by Progressive dyspnea and dry cough. Inspiratory crackles are present in 60% and Digital clubbing in 50% of patients 3.
1.ATS-ERS. International multidisciplinary consensus. Classification of the IIPs. Am J Respir Crit Care Med 2002;165: 277–30. 2. Corrin B, Price AB. Electron microscopic studies in desquamative interstitial pneumonia associated with asbestos. Thorax 1972; 27:324–331. 3.Abraham JL, Hertzberg MA. Inorganic particles associated with desquamative interstitial pneumonia. Chest 1981; 80: 67–70.

Desquamative Interstitial Pneumonia (DIP)
Physiologic changes
The most common and striking PFT abnormality is
marked reduction in diffusing capacity, with
reductions of 50% or more being common 1 .
Restrictive defects are also common.
Patients with advanced disease may have
hypoxemia at rest or with exertion.
Ryu JH, Myers JL, Capizzi SA, Douglas WW, Vassallo R, Decker PA. Desquamative interstitial pneumonia and respiratory bronchiolitisassociated interstitial lung disease. Chest 2005;127:178–184.

Desquamative Interstitial Pneumonia (DIP)
Radiologic Findings
Chest radiographs are insensitive for detection
of DIP and are reported to be normal in 3%–
22% of biopsy-proved cases 1 .
The radiologic patterns are nonspecific and
include patchy ground glass opacities with a
lower lung and peripheral predominance.
Hartman TE, Primack SL, Swensen SJ, Hansell D, McGuinness G,Mu¨ ller NL. Desquamative interstitial pneumonia: thin-section CT findings in 22 patients. Radiology 1993;187:787–790.

Desquamative Interstitial Pneumonia (DIP)
Radiologic Findings
Chest radiographs are insensitive for detection
of DIP and are reported to be normal in 3%–
22% of biopsy-proved cases 1 .
The radiologic patterns are nonspecific and
include patchy ground glass opacities with a
lower lung and peripheral predominance.
Hartman TE, Primack SL, Swensen SJ, Hansell D, McGuinness G,Mu¨ ller NL. Desquamative interstitial pneumonia: thin-section CT findings in 22 patients. Radiology 1993;187:787–790.

Desquamative Interstitial Pneumonia (DIP)
Radiologic Findings

Chest radiograph of a patient with desquamative interstitial pneumonia (DIP) showing bilateral
interstitial infiltrates involving mainly the lower lung zones. Mild, localized areas of fibrosis cause
a reticular pattern.

Desquamative Interstitial Pneumonia (DIP)
High-Resolution CT Findings
Bilateral patchy ground-glass opacity
Reticular opacities
Subpleural and basal predominance
Honeycombing uncommon
Associated centrilobular emphysema
Anil K. Attili, et al., Smoking-related Interstitial Lung Disease: Radiologic-Clinical-Pathologic Correlation. RadioGraphics 2008; 28:1383–1398

Desquamative Interstitial Pneumonia (DIP)
High-Resolution CT Findings
Bilateral patcReticular opacities
Subpleural and basal predominance
Honeycombing uncommon
Associated centrilobular emphysema
hy ground-glass opacity

Desquamative Interstitial Pneumonia (DIP)
High-Resolution CT Findings
Bilateral patchy ground-glass opacity

Desquamative Interstitial Pneumonia (DIP)
High-Resolution CT Findings
Bilateral patchy ground-glass opacity
Subpleural and basal predominance
Honeycombing uncommon
Associated centrilobular emphysema

Desquamative Interstitial Pneumonia (DIP)
HistologicallyThe main characteristic of DIP is the presence
of pigmented macrophages within the alveolar spaces that stain in a nonspecific fashion with PAS-diastase [8].
Minimal to moderate alveolar septal widening usually accompanies the air-spaces changes.
Honeycombing is rare [16, 32].

Desquamative Interstitial Pneumonia (DIP)
Macrophage accumulations within most of the distal air spaces. The alveolar septa are thickened by a sparse inflammatory infiltrate.The intraluminal macrophages in DIP frequently contain dusty brown pigment

Desquamative Interstitial Pneumonia (DIP)
• Treatment and Outcome– Smoking cessation is the primary treatment
for DIP and may lead to disease regression– Oral corticosteroids is generally
recommended for patients with• Significant symptoms,• PFT abnormalities, and• Progressive disease.
– The response to corticosteroids is not uniform

Desquamative Interstitial Pneumonia (DIP)
• Treatment and Outcome– Smoking cessation is the primary treatment
for DIP and may lead to disease regression– Oral corticosteroids is generally
recommended for patients with• Significant symptoms,• PFT abnormalities, and• Progressive disease.
– The response to corticosteroids is not uniform

Desquamative Interstitial Pneumonia (DIP)
• Treatment and Outcome– Smoking cessation is the primary treatment
for DIP and may lead to disease regression– Oral corticosteroids is generally
recommended for patients with• Significant symptoms,• PFT abnormalities, and• Progressive disease.
– The response to corticosteroids is not uniform

Desquamative Interstitial Pneumonia (DIP)
• Treatment and Outcome• The 5- and 10-yr survival rates are 95.2 and
69.6%, respectively, for patients with DIP 1 . • Nevertheless, DIP progresses in some cases and a
small number of patients have a poor outcome 2 .• Lung transplantation has been performed
successfully in patients with end-stage disease; however, disease recurrence in the transplanted lung has been reported 3 .
1.Carrington CB et al., . Natural history and treated course of usual and desquamative interstitial pneumonia. N Engl J Med 1978;298:801–809. 2. Hartman TE,et al., Disease progression in usual interstitial pneumonia compared with desquamative interstitial pneumonia: assessment with serial CT. Chest 1996;110:378–382. 3. Barberis M, Harari S, Tironi A, Lambertico P. Recurrence of primary disease in a single lung transplant recipient. Transplant Proc 1992;24: 2660–2662.

Desquamative Interstitial Pneumonia (DIP)
• Treatment and Outcome• The 5- and 10-yr survival rates are 95.2 and
69.6%, respectively, for patients with DIP 1 . • Nevertheless, DIP progresses in some cases and a
small number of patients have a poor outcome 2 .• Lung transplantation has been performed
successfully in patients with end-stage disease; however, disease recurrence in the transplanted lung has been reported 3 .
1.Carrington CB et al., . Natural history and treated course of usual and desquamative interstitial pneumonia. N Engl J Med 1978;298:801–809. 2. Hartman TE,et al., Disease progression in usual interstitial pneumonia compared with desquamative interstitial pneumonia: assessment with serial CT. Chest 1996;110:378–382. 3. Barberis M, Harari S, Tironi A, Lambertico P. Recurrence of primary disease in a single lung transplant recipient. Transplant Proc 1992;24: 2660–2662.

Desquamative Interstitial Pneumonia (DIP)
• Treatment and Outcome• The 5- and 10-yr survival rates are 95.2 and
69.6%, respectively, for patients with DIP 1 . • Nevertheless, DIP progresses in some cases and a
small number of patients have a poor outcome 2 .• Lung transplantation has been performed
successfully in patients with end-stage disease; however, disease recurrence in the transplanted lung has been reported 3 .
1.Carrington CB et al., . Natural history and treated course of usual and desquamative interstitial pneumonia. N Engl J Med 1978;298:801–809. 2. Hartman TE,et al., Disease progression in usual interstitial pneumonia compared with desquamative interstitial pneumonia: assessment with serial CT. Chest 1996;110:378–382. 3. Barberis M, Harari S, Tironi A, Lambertico P. Recurrence of primary disease in a single lung transplant recipient. Transplant Proc 1992;24: 2660–2662.


Pulmonary langerhans cell histiocytosis
The histiocytic disorders are rare diseases characterized by abnormal infiltration of certain organs by cells derived from monocyte/macrophage or dendritic cell lineage .
Langerhans Cell Histocytosis (LCH) is a specific type of histocytic syndrome characterized by infiltration of tissues with a specific dendritic cell, the Langerhans cell .
Favara BE, et al: Contemporary classification of histiocytic disorders. The WHO Committee On Histiocytic/Reticulum Cell Proliferations. Reclassification Working Group of the Histiocyte Society. Med Pediatr Oncol 1997, 29(3):157-166.

Pulmonary langerhans cell histiocytosis
The histiocytic disorders are rare diseases characterized by abnormal infiltration of certain organs by cells derived from monocyte/macrophage or dendritic cell lineage .
Langerhans Cell Histocytosis (LCH) is a specific type of histocytic syndrome characterized by infiltration of tissues with a specific dendritic cell, the Langerhans cell .
Favara BE, et al: Contemporary classification of histiocytic disorders. The WHO Committee On Histiocytic/Reticulum Cell Proliferations. Reclassification Working Group of the Histiocyte Society. Med Pediatr Oncol 1997, 29(3):157-166.

Pulmonary langerhans cell histiocytosis
Pulmonary Langerhans cell
histiocytosis refers to disease in adults
that affects the lung, usually in isolation
and less commonly in addition to other
organ systems .
Vassallo R, Ryu JH, Colby TV, Hartman T, Limper AH. Pulmonary Langerhans’-cell histiocytosis. N Engl J Med 2000;342:1969–1978.

Pulmonary langerhans cell histiocytosis
Epidemiology and demographic characteristicsPLCH is a rare disease which occurs almost
exclusively in smokers 1,2 .Estimated incidence 4-5% of all DLD biopsies
3 .Affects young adults between the ages of 20 to
40 years1. No gender predilection 1,4.
1.Vassallo R, et al.,: Clinical outcomes of pulmonary Langerhans’-cell histiocytosis in adults. N Engl J Med 2002, 346(7):484-490. 2. Arico M, et al.,: Langerhans cell histiocytosis in adults. Report from the International Registry of the Histiocyte Society. Eur J Cancer 2003, 39(16):2341-2348. 3. Gaensler EA, Carrington CB: Open biopsy for chronic diffuse infiltrative lung disease: clinical, roentgenographic, and physiological correlations in 502 patients. Ann Thorac Surg 1980, 30(5):411-426. 4. Travis WD, et al.,: Pulmonary Langerhans cell granulomatosis (histiocytosis X). A clinicopathologic study of 48 cases. Am J Surg Pathol 1993, 17(10):971-986

Pathogenesis
• It is possible that smokers with PLCH develop
an amplified inflammatory response induced by
tobacco smoke (and possibly other factors) that
induces activation of multiple cell types in the
lung, including epithelial and immune cells,
resulting in a vicious cycle of inflammation,
tissue injury and tissue remodeling

Pathogenesis
• Whether failure of endogenous anti-
inflammatory mechanisms or additional
exogenous insults like viral infections have
a role in promoting smoking induced PLCH
is unknown, and continues to be an
important area of investigation.

The primary event in the pathogenesis probably involves cigarette smoke-induced recruitment and activation of LCs to the small airways, a process that may result from a variety of potential mechanisms.
Pathogenesis

Cigarette smoke activates epithelial cells and macrophages toproduce cytokines and chemokines Cigarette smoke may also directly activateLCs.Langerhans cells conditioned by cigarette smokemay inappropriately recognize autontigens in the lungs and activate adaptive T cell responses that secondarily mediate injury in airway tissues
Pathogenesis

Chronic inflammation and cytokine production(particularly TGF-b) may promote local fibroblast activation and airway-centered fibrosis.
The combination of airway centered inflammation and tissue remodeling promote dilatation of structures distal to the inflamed small airways and cystic formation.
Pathogenesis

Pulmonary langerhans cell histiocytosis
Clinical Features
Ninety percent to 100% of adults with PLCH
are current or former smokers 1.
Prevalence of 3.4%.
Peak occurrence is at 20–40 years of age.
Men and women are equally affected 2.
1.Braier J, et al.,: Outcome in children with pulmonary Langerhans cell Histiocytosis. Pediatric blood & cancer 2004, 43(7):765-769. 2. Seely JM, et al.,: Pulmonary Langerhans Cell Histiocytosis: A Comparative Study of Computed Tomography in Children and Adults. Journal of thoracic imaging 2010.

Pulmonary langerhans cell histiocytosis
Clinical Features
– Up to 25% of patients are asymptomatic.
– Nonproductive cough and dyspnea.
– Weight loss, fever, night sweats, and anorexia,
(33%).
– Spontaneous pneumothorax (10%)
– Crackles and wheezes may occasionally be heard,
and in advanced cases breath sounds are decreased.1.Braier J, et al.,: Outcome in children with pulmonary Langerhans cell Histiocytosis. Pediatric blood & cancer 2004, 43(7):765-769. 2. Seely JM, et al.,: Pulmonary Langerhans Cell Histiocytosis: A Comparative Study of Computed Tomography in Children and Adults. Journal of thoracic imaging 2010.

Pulmonary langerhans cell histiocytosis
Pulmonary function and echocardiographic findings
PFT findings are variable depending upon the course of the disease and prevalent anatomical lesions .
Up to 20% of patients have normal PFT. 70% of patients have low DLCO, which is the most
common physiologic abnormality observed. A restrictive pattern (earlier stages) Obstructive pattern (predominant as disease
progresses) . Pulmonary Hypertension in advanced PLCH are much
greater than in other chronic lung diseases.
Vassallo R, Ryu JH, Schroeder DR, Decker PA, Limper AH: Clinical outcomes of pulmonary Langerhans’-cell histiocytosis in adults. N Engl J Med 2002, 346(7):484-490.

Pulmonary langerhans cell histiocytosis
Pulmonary function and echocardiographic findings
PFT findings are variable depending upon the course of the disease and prevalent anatomical lesions .
Up to 20% of patients have normal PFT. 70% of patients have low DLCO, which is the most
common physiologic abnormality observed. A restrictive pattern (earlier stages) Obstructive pattern (predominant as disease
progresses) . Pulmonary Hypertension in advanced PLCH are much
greater than in other chronic lung diseases.

Pulmonary langerhans cell histiocytosis
Pulmonary function and echocardiographic findings
PFT findings are variable depending upon the course of the disease and prevalent anatomical lesions .
Up to 20% of patients have normal PFT. 70% of patients have low DLCO, which is the most
common physiologic abnormality observed. A restrictive pattern (earlier stages) Obstructive pattern (predominant as disease
progresses) . Pulmonary Hypertension in advanced PLCH are much
greater than in other chronic lung diseases.

Pulmonary langerhans cell histiocytosis
Pulmonary function and echocardiographic findings
PFT findings are variable depending upon the course of the disease and prevalent anatomical lesions .
Up to 20% of patients have normal PFT. 70% of patients have low DLCO, which is the most
common physiologic abnormality observed. A restrictive pattern (earlier stages) Obstructive pattern (predominant as disease
progresses) . Pulmonary Hypertension in advanced PLCH are much
greater than in other chronic lung diseases.

Pulmonary langerhans cell histiocytosis
Pulmonary function and echocardiographic findings
PFT findings are variable depending upon the course of the disease and prevalent anatomical lesions .
Up to 20% of patients have normal PFT. 70% of patients have low DLCO, which is the most
common physiologic abnormality observed. A restrictive pattern (earlier stages) Obstructive pattern (predominant as disease
progresses) . Pulmonary Hypertension in advanced PLCH are much
greater than in other chronic lung diseases.
Vassallo R, Ryu JH, Schroeder DR, Decker PA, Limper AH: Clinical outcomes of pulmonary Langerhans’-cell histiocytosis in adults. N Engl J Med 2002, 346(7):484-490.

Pulmonary langerhans cell histiocytosis
Radiographic findings
• CXR is almost always abnormal, although the
findings may be subtle and easy to overlook .
• Reticulonodular infiltrates are predominant in
early disease whereas cystic lesions are more
dominant in advanced disease
• Predominantly involving upper and middle lobes
with relative sparing of lung bases.

Pulmonary langerhans cell histiocytosis
Radiographic findings
• CXR is almost always abnormal, although the
findings may be subtle and easy to overlook .
• Reticulonodular infiltrates are predominant in
early disease whereas cystic lesions are more
dominant in advanced disease
• Predominantly involving upper and middle lobes
with relative sparing of lung bases.

Pulmonary langerhans cell histiocytosis
Radiographic findings
• CXR is almost always abnormal, although the
findings may be subtle and easy to overlook .
• Reticulonodular infiltrates are predominant in
early disease whereas cystic lesions are more
dominant in advanced disease
• Predominantly involving upper and middle lobes
with relative sparing of lung bases.

Pulmonary langerhans cell histiocytosis

Pulmonary langerhans cell histiocytosis
Radiographic findings

Pulmonary langerhans cell histiocytosis
Radiographic findings

Pulmonary langerhans cell histiocytosis
Radiographic findings

Pulmonary langerhans cell histiocytosis
HRCT Findings of PLCH• Thin-walled cysts, some confluent or with bizarre
shapes.• Thick-walled cysts.• Nodules, usually 1–5 mm, centrilobular or
peribronchial, may be cavitary, and seen in association with cysts.
• Progression from three to two to one .• Upper lobe predominance of nodules and cysts,
costophrenic angles spared.• Fine reticular opacities.• Ground-glass opacities.

Pulmonary langerhans cell histiocytosis
HRCT Findings of PLCH• Thin-walled cysts, some confluent or with bizarre
shapes

Pulmonary langerhans cell histiocytosis
HRCT Findings of PLCH• Thin-walled cysts, some confluent or with bizarre
shapes

Pulmonary langerhans cell histiocytosis
HRCT Findings of PLCH• Thick-walled cysts.

Pulmonary langerhans cell histiocytosis
HRCT Findings of PLCH• Thick-walled cysts.

Pulmonary langerhans cell histiocytosis
HRCT Findings of PLCH• Nodules, usually 1–5 mm, centrilobular or
peribronchial, may be cavitary, and seen in association with cysts

Pulmonary langerhans cell histiocytosis
HRCT Findings of PLCH• Nodules, usually 1–5 mm, centrilobular or
peribronchial, may be cavitary, and seen in association with cysts

Pulmonary langerhans cell histiocytosis
HRCT Findings of PLCH• Upper lobe predominance of nodules and cysts,
costophrenic angles spared.• Fine reticular opacities.• Ground-glass opacities.

Pulmonary langerhans cell histiocytosis
HRCT Findings of PLCH
• Upper lobe predominance of nodules and cysts, costophrenic angles spared.
• Fine reticular opacities.• Ground-glass opacities.

Pulmonary langerhans cell histiocytosis
Bronchoalveolar lavage (BAL)
BAL should be performed in all patients as the
detection of > 3% CD1a-positive cells
(Langerhans’ cells) in the appropriate clinical
context (supported by consistent chest HRCT
findings) is highly suggestive of PLCH 1,2 .
1.Auerswald U, Barth J, Magnussen H: Value of CD-1-positive cells in bronchoalveolar lavage fluid for the diagnosis of pulmonary histiocytosis X. Lung 1991, 169(6):305-309.2. Chollet S, Soler P, Dournovo P, Richard MS, Ferrans VJ, Basset F: Diagnosis of pulmonary histiocytosis × by immunodetection of Langerhans cells in bronchoalveolar lavage fluid. Am J Pathol 1984, 115(2):225-232.

Pulmonary langerhans cell histiocytosis
Histopathologic Findings Lung biopsy is necessary for a definitive
diagnosis
• A key histologic feature is the presence of cellular
peribronchiolar nodules containing Langerhans
cells and inflammatory cells in the early stages
(15).
• LCs stain positive for S100, CD1a, and HLA–DR at
immunohistochemical analysis.

Pulmonary langerhans cell histiocytosis
Histopathologic Findings Lung biopsy is necessary for a definitive
diagnosis
• A key histologic feature is the presence of cellular
peribronchiolar nodules containing Langerhans
cells and inflammatory cells in the early stages 1.
• LCs stain positive for S100, CD1a, and HLA–DR at
immunohistochemical analysis.
Suri et al.: Pulmonary langerhans cell histiocytosis. Orphanet Journal of Rare Diseases 2012 7:16.

Pulmonary langerhans cell histiocytosis
Histopathologic Findings Lung biopsy is necessary for a definitive
diagnosis
• A key histologic feature is the presence of cellular
peribronchiolar nodules containing Langerhans
cells and inflammatory cells in the early stages 1.
• LCs stain positive for S100, CD1a, and HLA–DR at
immunohistochemical analysis.
Suri et al.: Pulmonary langerhans cell histiocytosis. Orphanet Journal of Rare Diseases 2012 7:16.

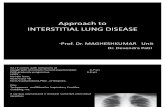
a low-power microscopic picture with nodular airway-centered lesions
showing microcystic change

High-power shows diffuse infiltration of lung tissue with Langerhans cells showing vesicular nuclear chromatin, irregular nuclear contour and moderate amount of pale cytoplasm devoid of phagocytosed material. Many eosinophils are also intermixed among Langerhans cells

High-power photomicrographs of a surgical lung biopsy specimen Staining is both
nuclear and cytoplasmic with S100.

Pulmonary langerhans cell histiocytosis
Treatment and Outcome– Smoking cessation is essential and leads to
stabilization of symptoms in most patients.
– Corticosteroids are the mainstay of medical therapy for PLCH.
– Lung transplantation is considered for patients with advanced PLCH associated with severe respiratory impairment and limited life expectancy.

Treatment and Outcome– Smoking cessation is essential and leads to
stabilization of symptoms in most patients.
– Corticosteroids are the mainstay of medical therapy for PLCH.
– Lung transplantation is considered for patients with advanced PLCH associated with severe respiratory impairment and limited life expectancy.

Pulmonary langerhans cell histiocytosis
Treatment and Outcome– Smoking cessation is essential and leads to
stabilization of symptoms in most patients.
– Corticosteroids are the mainstay of medical therapy for PLCH.
– Lung transplantation is considered for patients with advanced PLCH associated with severe respiratory impairment and limited life expectancy.

Pulmonary langerhans cell histiocytosis
Treatment and Outcome– Smoking cessation is essential and leads to
stabilization of symptoms in most patients.
– Pharmacotherapy with immunosuppressive medication should be considered for • Patients with severe disease, or
• Patients in whom progressive decline in lung function occurs.
– Lung transplantation is considered for patients with advanced PLCH associated with severe respiratory impairment and limited life expectancy.

Pulmonary langerhans cell histiocytosis
Outcomes and prognosis– The course of PLCH in adults is variable and
unpredictable, ranging from asymptomatic to progressive debilitating disease that leads to respiratory failure and death over a period of few years.
– Several factors have been associated with poor outcome including • Extremes of age, Prolonged constitutional symptoms,• Multi-organ involvement,• Extensive cysts and honeycombing on the radiograph,• Severely DLCO & obstructive physiology• prolong treatment with steroid therapy and• associated pulmonary hypertension

Pulmonary langerhans cell histiocytosis
Outcomes and prognosis– The course of PLCH in adults is variable and
unpredictable, ranging from asymptomatic to progressive debilitating disease that leads to respiratory failure and death over a period of few years.
– Several factors have been associated with poor outcome including • Extremes of age, Prolonged constitutional symptoms,• Multi-organ involvement,• Extensive cysts and honeycombing on the radiograph,• Severely DLCO & obstructive physiology• Prolong treatment with steroid therapy and• Associated pulmonary hypertension.

Conclusions• The variety of ILDs associated with cigarette
smoking is wider than generally appreciated, and
many forms often coexist.
• Although key high-resolution CT findings of SR-ILDs
can be recognized, mixed patterns of disease
associated with cigarette smoking may be confusing.
• An integrated clinical, radiologic, and pathologic
approach is necessary for accurate diagnosis of the
SR-ILDs.

ConclusionsRB-ILD
DIP
PLCH
AEP
SRIF
CPFE