
Site of conduction delay in children with catheter-induced right bundle branch block
4
J. ELECTROCARDIOLOGY 16 (1), 1983, 41-44 Site of Conduction Delay in Children with Catheter-Induced Right Bundle Branch Block BY AGUSTIN RAMOS, M.D., GRACE S. WOLFF, M.D. AND HENRY GELBAND, M.D. SUMMARY Eight cases of catheter-induced right bundle branch block (RBBB) in children during electrophysiologic studies are presented. Recording of right ventricular apical activation time (V-RVA) before and during the conduction delay allowed localization of the block along the course of the right bundle branch system. In the majority of patients, a signifi- cant lengthening of V-RVA was observed, indicating that proximal right bundle branch block is the most ~ommonly induced type of conduction delay. Block was transient in all patients and terminated several minutes to 24 hours after its induction. The electrocardiographic pattern of complete right bundle branch block (RBBB) is one of the most frequently observed patterns during cathe- ter manipulation of the right ventricle. 15 It has been demonstrated that in the presence of RBBB, localization of the site of conduction delay along the course of the right bundle branch system can be determined by measuring the right ventricular apical activation time (V-RVA). s-s The purpose of this paper is to report the site of RBBB block {proximal or distal)induced by catheter manipulation in eight children who were studied electrophysiologically, as determined by the V-RVA interval. MATERIALS AND METHODS The data {Table I) originate from eight children who developed RBBB during cardiac catheterization and electrophysiologic studies for congenital heart disease or rhythm disorders (2% incidence). Their clinical diagnoses were D-transposition of the great arteries, secundum atrial septal defect, ventricular septal defect, aortic stenosis, pulmonary stenosis, congestive cardiomyopathy and congenital complete atrioventri- cular block. From the University of Miami School of Medicine, Depart- ment of Pediatrics, Miami, Florida. Supported in part by Grant #HL 07436 from the National In- stitutes of Health and the American Heart Association"of Greater Miami. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked "advertisement" in accordance with 1~ a U.S.C. w 1734 solely to indicate this fact. Reprint requests to: Henry Gelband, M.D., Pediatric Cardi- ology, Department of Pediatrics, University of Miami, School of Medicine, P.O. Box 016820, Miami, Florida 33101. Catheterizations were performed in the post-absorp- tive basal state. Patients #1, 2, 4, 5, 7 and 8 were ad- ministered meperidine hydrochloride, promethazine hydrochloride and chlorpromazine hydrochloride for sedation. In addition, patients #2 and 8 received pen- tobarbital sodium and patient//5 diazepam. Patients #3 and 6 received only meperidine hydrochloride. A tripolar or tetrapolar electrode catheter was introduced percutaneously through the femoral vein and was placed in the right ventricular apical region under fluoroscopic guidance. Right ventricular apical elec- trograms were recorded according to the method of Sung et alY at filter settings of 40-500 Hz or 400-500 Hz. Simultaneously, surface ECG leads I, II (or aVF) and V 1 were displayed and recorded on a multichannel oscilloscopic photographic recorder {Electronics for Medicine, DR-8, White Plains, N.Y.). Recordings were obtained at a paper speed of 100 mndsec. An electrode catheter was then positioned across the septal leaflet of the tricuspid valve to obtain His bundle electrograms with a filter setting of 40-500 Hz. The intracardiac electrograms were analyzed and the following intervals were determined by averaging at least five successive cardiac cycles: 1) QRS, from the beginning of the earliest deflection to the end of the latest deflection of the QRS complex in any of the sur- face ECG leads. 2) HV, from the first fast wave of the His deflection to the onset of earliest ventricular depolarization, in whichever lead {surface ECG or in- tracardiac electrogram) it occurred first. 3) Right ven- tricular apical activation time (V-RVA), from the onset of ventricular depolarization on any surface ECG level to the onset of the first sharp and rapid moving deflec- tion on the RV apical electrogram. 7 Frontal plane electrical axis changes were assessed by a full set of limb ECG leads before and during block or, when not available, by estimating electrical axis from leads I and II (or aVF) on the surface elec- trograms. 41
-
Upload
agustin-ramos -
Category
Documents
-
view
217 -
download
0
Transcript of Site of conduction delay in children with catheter-induced right bundle branch block

J. ELECTROCARDIOLOGY 16 (1), 1983, 41-44
Site of Conduction Delay in Children with Catheter-Induced Right Bundle Branch Block
BY AGUSTIN RAMOS, M.D., GRACE S. WOLFF, M . D . AND HENRY GELBAND, M . D .
SUMMARY Eight cases of catheter-induced right bundle branch block (RBBB) in children during
electrophysiologic studies are presented. Recording of right ventricular apical activation time (V-RVA) before and during the conduction delay allowed localization of the block along the course of the right bundle branch system. In the majority of patients, a signifi- cant lengthening of V-RVA was observed, indicating that proximal right bundle branch block is the most ~ommonly induced type of conduction delay. Block was transient in all patients and terminated several minutes to 24 hours after its induction.
The e lec t rocard iographic p a t t e r n of comple te r igh t bundle b ranch block (RBBB) is one of the m o s t f r equen t ly obse rved p a t t e r n s du r ing cathe- t e r manipu la t ion of the r igh t ventr icle . 15 I t has been d e m o n s t r a t e d t ha t in the presence of R B B B , localizat ion of the site of conduc t ion de lay a long the course of the r igh t bundle b ranch s y s t e m can be de te rmined by measur ing the r igh t ven t r i cu la r apical ac t iva t ion t ime (V-RVA). s-s The purpose of this pape r is to r epo r t t he si te of R B B B block { p r o x i m a l o r d i s t a l ) i n d u c e d b y c a t h e t e r man ipu la t ion in e ight chi ldren who were s tudied e lec t rophys io log ica l ly , as d e t e r m i n e d by the V-RVA interval .
MATERIALS AND METHODS The data {Table I) originate from eight children who
developed RBBB during cardiac catheterization and electrophysiologic studies for congenital heart disease or rhythm disorders (2% incidence). Their clinical diagnoses were D-transposition of the great arteries, secundum atrial septal defect, ventricular septal defect, aortic stenosis, pulmonary stenosis, congestive cardiomyopathy and congenital complete atrioventri- cular block.
From the University of Miami School of Medicine, Depart- ment of Pediatrics, Miami, Florida. Supported in part by Grant #HL 07436 from the National In- stitutes of Health and the American Heart Association"of
Grea te r Miami. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked "advertisement" in accordance with 1~
a
U.S.C. w 1734 solely to indicate this fact. Reprint requests to: Henry Gelband, M.D., Pediatric Cardi- ology, Department of Pediatrics, University of Miami, School of Medicine, P.O. Box 016820, Miami, Florida 33101.
Catheterizations were performed in the post-absorp- tive basal state. Patients #1, 2, 4, 5, 7 and 8 were ad- ministered meperidine hydrochloride, promethazine hydrochloride and chlorpromazine hydrochloride for sedation. In addition, patients #2 and 8 received pen- tobarbital sodium and patient/ /5 diazepam. Patients #3 and 6 received only meperidine hydrochloride. A tripolar or tetrapolar electrode catheter was introduced percutaneously through the femoral vein and was placed in the right ventricular apical region under fluoroscopic guidance. Right ventricular apical elec- trograms were recorded according to the method of Sung et alY at filter settings of 40-500 Hz or 400-500 Hz. Simultaneously, surface ECG leads I, II (or aVF) and V 1 were displayed and recorded on a multichannel oscilloscopic photographic recorder {Electronics for Medicine, DR-8, White Plains, N.Y.). Recordings were obtained at a paper speed of 100 mndsec. An electrode catheter was then positioned across the septal leaflet of the tricuspid valve to obtain His bundle electrograms with a filter setting of 40-500 Hz.
The intracardiac electrograms were analyzed and the following intervals were determined by averaging at least five successive cardiac cycles: 1) QRS, from the beginning of the earliest deflection to the end of the latest deflection of the QRS complex in any of the sur- face ECG leads. 2) HV, from the first fast wave of the His deflection to the onset of earliest ventricular depolarization, in whichever lead {surface ECG or in- tracardiac electrogram) it occurred first. 3) Right ven- tricular apical activation time (V-RVA), from the onset of ventricular depolarization on any surface ECG level to the onset of the first sharp and rapid moving deflec- tion on the RV apical electrogram. 7
Frontal plane electrical axis changes were assessed by a full set of limb ECG leads before and during block or, when not available, by estimating electrical axis from leads I and II (or aVF) on the surface elec- trograms.
41
42 RAMOS ET AL
TABLE I
Case Age Diagnosis
ORS Duration ECG without/ HV
Diagnosis with brock (msec) (msec)
V-RVA time without/
with block (msec)
Site
of Brock
1 17 yrs PS 2 9 yrs ASD 3 10 yrs CHB 4 4 yrs VSD, PHT 5 4 yrs AS, SVT 6 7 mo TGV, VSD 7 5 yrs PS 8 2 yrs PS, Cardiomyopathy
RVH 7 0 / 1 2 0 50 RVH 9 0 / 1 2 0 49 CHB 7 5 / 1 1 5 26 RVH 8 0 / 1 3 0 45 LVH 70/1 O0 30 RVH 60/1 O0 -- RVH 7 0 / 1 1 0 22 RVH 7 5 / 1 2 0 33
8 /52 17 /60 17 /48 19 /45 10 /55 15 /35 2 0 / 2 0 12 /23
P P P P P P D D
PS = pulmonic stenosis SVT ASD = atrial septal defect TGV CHB = complete heart block RVH VSD Ve~ntricular septal defect LVH PHT = pulmonary hypertension P AS = aortic stenosis D
= supraventricular tachycardia = transposit ion of the great vessels = right ventricular hypertrophy = left ventricular hypertrophy = proximal = distal
RESULTS Table I summarizes the data. The duration of
the QRS complex increased with the development of RBBB from 60-90 msec before block to 100-130 msec after the onset of RBBB. HV intervals were normal in all patients {20-55 msec is considered normal in our laboratory}.
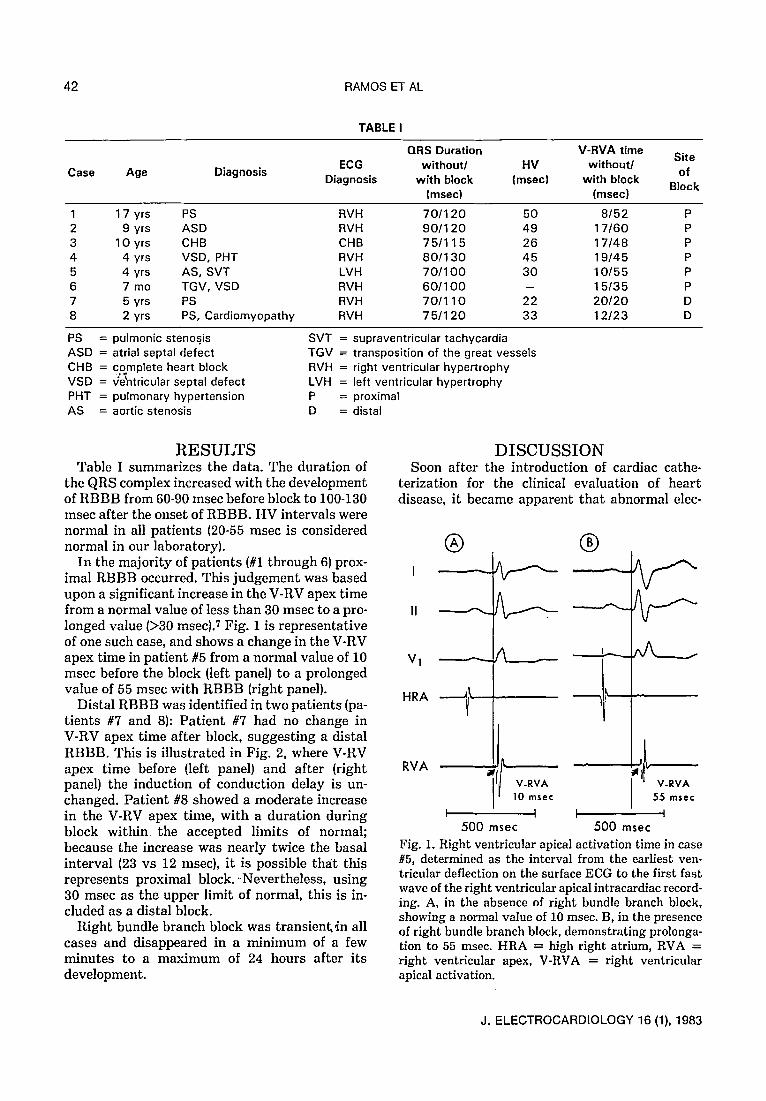
In the majori ty of patients (#1 through 6) prox- imal RBBB occurred. This judgement was based upon a significant increase in the V-RV apex time from a normal value of less than 30 msec to a pro- longed value (>30 msec). 7 Fig. 1 is representative of one such case, and shows a change in the V-RV apex time in patient #5 from a normal value of 10 msec before the block (left panel} to a prolonged value of 55 msec with RBBB (right panel}.
Distal RBBB was identified in two patients {pa- t ients #7 and 8): Pat ient #7 had no change in V-RV apex time after block, suggesting a distal RBBB. This is illustrated in Fig. 2, where V-RV apex time before {left panel} and after (right panel} the induction of conduction delay is un- changed. Patient #8 showed a moderate increase in the V-RV apex time, with a duration during block w i th in the accepted limits of normal; because the increase was nearly twice the basal interval (23 vs 12 msec), it is possible the/t this represents proximal block. - Nevertheless, using 30 msec as the upper limit of normal, this is in- cluded as a distal block.
Right bundle branch block was transienk4n all cases and disappeared in a minimum of a few minutes to a maximum of 24 hours after its development.
DISCUSSION Soon after the introduction of cardiac cathe-
terization for the clinical evaluation of heart disease, it became apparent tha t abnormal elec-
| |
V-RVA V-RVA 10 msec 55 rnsec
I I I 1 500 msec 500 msec
Fig. 1. Right ventricular apical activation time in case #5, determined as the interval from the earliest yen- tricular deflection on the surface ECG to the first fast wave of the right ventricular apical intracardiac record- ing. A, in the absence of right bundle branch block, showing a normal value of 10 msec. B, in the presence of right bundle branch block, demonstrating prolonga- tion to 55 msec. HRA ----- high right atrium, RVA =-- right ventricular apex, V-RVA = right ventricular apical activation.
J. ELECTROCARDIOLOGY 16 (1), 1983

CATHETER-INDUCED RBBB 43
|
Vl
"?
HRA -1"
RVA
V-'-"
9t V-RVA 20 msec
|
%
jr
X . . - - - _
V - R V A
20 msec
I '1 I I 250 250 msec msec
Fig. 2. Right ventricular apical activation time in case //7, determined as in Fig. 1. A, in the absence of right bundle branchblock, showing anormal value of 20 msec. B, in the presence of right bundle branch block, demon- strating a similar value. Abbreviations as in Fig. 1.
trocardiographic patterns were often induced by intracardiac catheters as a consequence of local mechanical stimulation. 1-4 The incidence of ar- rhythmias during the course of catheterization has been reported to be 3-6 percent,3.4 however, if one includes occasional atrial and ventricular ex- trasystoles the incidence of arrhythmias is prob- ably much higher. 5.9.1~ Arrhythmias have also resulted from the use of Swan-Ganz catheters for pulmonary artery pressure monitoring, 111v arid
�9 during cardiac electrophysiologic studies. 5,18"21 One of the most frequent problems is the devel-
opment of transient RBBB. Simonson 22 reported one such case as early as 1951. In a recent repor2, Akhtar et a l ) reviewed their experience with catheter induced electrocardiographic patterns during electrophysiologic studies and suggested
that traumatic right bundle branch block is generally induced when the catheter is placed at the atrioventricular junction, as for recording His bundle activity. They documented all degrees of RBBB, varying from minimal terminal conduc- tion delay to complete RBBB lasting anywhere from a few beats to four hours. Luck14 reported the occurrence of transient RBBB, lasting 3 to 35 hours, with Swan-Ganz catheterization in three patients. He emphasized that the passage of a balloon-tipped catheter through the right ventri- cle may not prevent this complication. In this situation, he suggested that a rigid catheter loop rather than the catheter tip may be the cause of mechanical damage to the right bundle.
Recently, Thompson et al. 16 also reported a high incidence of RBBB during Swan-Ganz cathe- terization of the pulmonary artery in adults with coronary ar tery disease. In addition, they reported the occurrence of complete atrioventri- cular (A-V) block associated with Swan-Ganz catheterization in two patients with pre-existing left bundle branch block. This serious complica- tion has been reported by others 5.11.19,23 and war- rants special precautions during catheter evalua- tion of patients with pre-existing LBBB. I t is recommended~,lm6,19,23 in these patients that facilities be available for ventricular pacing in the event a high degree A-V block is induced. This can be accomplished by prior careful positioning of an electrode catheter in the right ventricle. These data from studies in adults would support the hypothesis that traumatic RBBB is most fre- quently proximal as opposed to distal. One would not anticipate the development of complete A-V heart block in the presence of LBBB, unless prox- imal RBBB occurred or unless there was direct trauma to the bundle of His.
The right ventricular apical activation time (V-RVA) is useful in locating the site of conduc- tion delay 6-s since it reflects the time elapsed be- tween the beginning of ventricular depolarization (usually the left ventricle) and activation of the right ventricular apical myocardium. Block at the proximal right bundle will delay activation of the right ventricular apex, thereby lengthening the duration of the V-RVA time above normal. Block at the more distal right ventricular conduction system will not delay the timing of apicla activa- tion and will show a normal V-RVA interval.6.7 Normal values for this interval have been deter- mined in a large group of children (6 mo- 18 yrs of age) without intraventricular conduction delay, and have been found to be less than 30 msec.S
J. ELECTROCARDIOLOGY 16 (1), 1983

44 RAMOS ET AL
According to our findings, catheter induced R B B B is usually of the proximal type, because in- duction of right bundle branch block is associated with a significant increase in the V-RVA interval. This is not surprising, since the main right bundle travels only one half to one millimeter below the right-sided septal endocardium from its His bun- dle origin to the moderator band in the body of the RV. 24 This superficial course makes it acces- sible to catheter trauma. Our findings indicate tha t catheter induced RBBB of peripheral origin is also possible, although it may not be en- countered as frequently. Catheter st imulation of a branch other than those responsible for the apical region will delay depolarization of par t of the right "r thereby inducing an RBBB pat tern without delaying right ventricular activa- tion time. Whether the block was proximal or distal, it was t ransient in all pat ients , ter- minating spontaneously within twenty four hours of catheterization.
R E F E R E N C E S 1. LANDTMAN, B: Mechanically induced disturbances in
the heart action Acta Ped Stand 39:1, 1950 2. MICUEL, J, JOIINSON, A D, BRIDGES, W C,
LEIIMANN, J H, GRAY, F, FIELD, L AND GREEN, D M: Arrhythmias during intracardiac catheterization. Circulation 2:240, 1950
3. FRASER, R S, MACAULAY, W D AND ROSSALL, R E: Arrhythmias induced during intracardiac catheterization. Am Heart J 64:439, 1962
4. WENNEVOLD, A, CIIRISTIANSEN, I AND LINDENEG, O: Complications in 4,413 catheterizations of the right side of the heart. Am Heart J 69:173. 1965
5. AKIITAR, M, DAMATO, A N, GILBERT-LEEDS, C J, : BATSFORD, W P, REDDY, C P, JONES, J A C, CALON,
A H AND DHATT, M S: Induction of iatrogenic elec- trocardiographic patterns during electrophysiologic studies- Circulation 56:60, 1977
6. CASTELLANOS, A, AGllA, A S, BEFELER, B, CASTILLO, C A AND BERKOVITS, B V: A study of ar- rival of excitation at selected ventricular sites during human bundle branch block using close bipolar catheter electrodes. Chest 63:208, 1973
7. SUNG, R J, TAMER, D "M, GARCIA, O L, CASTELLANOS, A, MYERBURG, R AND GELBAND, H: Analysis of surgically-induced right bundle branch block pattern using intracardiac recording tech- niques. Circulation 54:442, 1976
8. MEIITA, A V, WOLFF, G S, TAMER, D F, GARCIA, O L, PICKOFF, A S, CASTA, A, FERRER, P L AND GELBAND, H: Right ventricular apical activation
time in children. Reference standards for clinical use. Pediatr Cardiol 2:47-50, 1982
9. GUPTA, K AND HAFT, J I: Complete heart block com- plicating cardiac catheterization. Chest 61:185, 1972
I0. FREED, M AND ROSENTIIAL, A: Complete heart block after cardiac catheterization: A rare complication. Pediatrics 51:935, 1973
11. ABERNATIIY, W S: Complete heart block caused by the Swan-Ganz catheter, Chest 65:349, 1974
12. VOUZYDIS, P C AND COIIEN, S I: Catheter-induced arrhythmias. Am Heart J 88:588, 1974
13. CAmNS, J A AND HOLDER, D: VentHcular fibrillation due to passage of a Swan-Ganz catheter. Am J Car- diol 35:589, 1975
14. LUCK, J C: Transient right bundle branch block with "Swan-Ganz" catheterization. Am Heart J 92:263, 1976
15. AGUILAR, L R, O'CALLAGIIAN, A C, DE LA HOE, J C, PEREZ, M M, MOMPO, J G, GARCIA, RC AND MARCO, M R: Bloqueo completo de rama derecha del haz de His durante la implantacion del caterer Swan-Ganz. Rev Esp Cardiol 30:309, 1977
16. TtIOMSON, I R, DALTON, B C, LAPPES, D G AND LOWENSTEIN, E: Right bundle branch block and com- ,plete heart block caused by the Swan-Ganz catheter. Anesthesiology 51:359, 1979
17. CASTELLANOS, A, RAMIREZ, A V, MAYORGA- CORTES, A, PEFKAROS, K, ROZANSKI, J J, SPRUNG, C AND MYERBURG, R J: Left fascicular blocks during right heart catheterization using the Swan-Ganz catheter. Circulation (in press).
18. PATTOR, R D, BORDIA, A, BALLANTYE, F, RYAN, G F, GOLDSTEIN, S AND HEINLE, R A: Bundle-of-His recording of complete heart block during cardiac catheterization: Electrophysiologlc documentation of bilateral bundle branch block. Am Heart J 81:108, 1971
19. KIMBIRIS, D, DREIFUS, L S AND LINIIART, J W: Complete heart block occurring during cardiac catheterization in patients with pre-existing bundle branch block. Chest 65:95, 1974
20. JOCOBSON, L B AND SCIIEINMAN, M: Catheter- induced intra-Hisian and intrafascicular block during recording of His bundle electrograms. Circulation 49:579, 1974
21. NOVICK, T L, PRITCIIETT, E L C, CAMPBELL, R W F, ROPERS, G C, WALLACE, A G AND GALLAGIIER, J J: Temporary, catheter-induced block in accessory pathways. Circulation 58:932, 1978
22. SIMONSON, E: Transient right bundle branch block produced by heart catheterization in man. Am Heart J 41:217, 1951
23. STEIN, P D, VIRENDRA, S M, HERMAN, M V AND LEVlNE, H D: Complete heart block induced during cardiac catheterization of patients with pre-existent bundle branch block. Circulation 34:783, 1966
24. MASSING, G K AND JAMES, T N: Anatomical con- figuration of the His bundle and bundle branches in the human heart. Circulation 53:609, 1976
J. ELECTROCARDIOLOGY 16 (1), 1983


















