Shaukat Khanum Guidelines for Coronavirus Disease 2019 ...€¦ · ⴕWear a simple surgical mask...
24
Shaukat Khanum Guidelines for Coronavirus Disease 2019 (COVID-19) Prepared by the Infection Control Committee Shaukat Khanum Memorial Cancer Hospital and Research Centre
Transcript of Shaukat Khanum Guidelines for Coronavirus Disease 2019 ...€¦ · ⴕWear a simple surgical mask...

Shaukat Khanum Guidelines for
Coronavirus Disease 2019 (COVID-19)
Prepared by the
Infection Control Committee
Shaukat Khanum Memorial Cancer Hospital and Research Centre

2
Shaukat Khanum Memorial Cancer Hospital & Research
Center
Infection Control Committee
Coronavirus Disease 2019 (COVID-19)
Contents
Section 1: COVID-19 Basics, Outpatient Pathway and Testing
2
Background; Case definitions 2 Isolation precautions; COVID-19 screening 3 Pathway for patients with suspected COVID-19 in the outpatient setting 4 COVID-19 Testing 6 Camp COVID Patient flow, Cleaning of rooms and medical equipment used for COVID-19 patients
7
Camp COVID PPE guidelines 8 Section 2: COVID-19 Clinical Syndromes and Inpatient Management
9
Isolation precautions and PPE for COVID-19 patients 12 Transporting COVID-19 patients 13 Room allocation for COVID-19 patients 13 COVID-19 patients requiring medical procedures 13 COVID-19 visitor policy 14 COVID-19 patients and cardiopulmonary resuscitation 14 When can isolation precautions be discontinued? 14 What if there is strong clinical suspicion but test results are negative? 14 When can the patient be discharged? 14 What instructions must patients be given on discharge? 14 Section 3: Personal Protective Equipment (PPE)
14
Recommendations for PPE use 16 Recommendations for PPE in the EAR, IPD 17 Recommendations for PPE in the ICU 18 Recommendations for staff in all clinical areas; Recommendations for PPE reuse 19 Section 4: Frequently Asked Questions (FAQs)
21
What resources are these guidelines based on? 21 What is the policy for pregnant healthcare workers? 21 What should employees with cough/cold symptoms do? 21 How can hospital staff protect themselves from COVID-19? 21 Code blue: suspected/confirmed COVID-19; Codes in the EAR Appendix A: Patient Under Investigation (PUI) Form 22

3
Section 1: COVID-19 Basics, Outpatient Pathway and
Testing
Background
• Caused by SARS-COV-2, first identified in Wuhan, China in 12/2019
• Transmission: human-to-human
modes of transmission: contact and droplets
• Incubation period: 4-14 days
• Spectrum of infection: mild respiratory illness (~80% of cases) to pneumonia/acute respiratory
distress syndrome; mortality 2-3%
Case Definitions: Suspect case Case Definition (added point 2):
A patient with acute respiratory illness (fever and at least one sign/symptom of respiratory disease, e.g., cough, shortness of breath), AND any of the following:
1. A history of travel to or residence in a location reporting community transmission of COVID-19 disease during the 14 days prior to symptom onset (includes international travel and travel from Raiwind, Karachi and Mardan) OR
2. A history of contact with a traveler from a location reporting community transmission of COVID-19 disease during the 14 days prior to symptom onset (includes international travel and travel from Raiwind, Karachi and Mardan) OR
3. Contact with a confirmed or probable COVID-19 case (see definition of contact) in the last 14 days prior to symptom onset; OR
4. A history of having attended a religious gathering or ijthima over the last 2 weeks OR
5. Absence of an alternative diagnosis that fully explains the clinical presentation.
Probable case
1. A suspect case for whom testing for the COVID-19 virus is inconclusive OR
2. A suspect case for whom testing could not be performed for any reason. Confirmed case

4
1. A person with laboratory confirmation of COVID-19 infection, irrespective of clinical signs and symptoms.
Definition of contact
A contact is a person who experienced any one of the following exposures during the 2 days before and the 14 days after the onset of symptoms of a probable or confirmed case:
1. Face-to-face contact with a probable or confirmed case within 1 meter and for more than 15 minutes;
2. Direct physical contact with a probable or confirmed case; 3. Direct care for a patient with probable or confirmed COVID-19 disease without using proper
personal protective equipment; OR
4. Other situations as indicated by local risk assessments. Note: for confirmed asymptomatic cases, the period of contact is measured as the 2 days before through the 14 days after the date on which the sample was taken which led to confirmation
Isolation Precautions:
Standard + contact+ droplet: for all patients
Standard+ contact+ airborne: for patients requiring aerosol-generating procedures e.g.
bronchoscopy, CPR, intubation, nasopharyngeal specimen collection, noninvasive ventilation,
airway suctioning, NG insertion, dental procedures ONLY. Any other procedures do not fall
under this list.
Eye protection: for all patients
COVID-19 Screening:
SKM-Lahore
9:00 am to 9:00 pm 7 days a week: Screening will be performed at designated COVID
screening counters outside the hospital
COVID Camp 24 hours, 7 days a week
PCOs inside the hospital will continue to screen all patients arriving at their counters
SKM-Peshawar:
8:00 am to 9:00 pm 7 days a week: Screening at designated COVID counters outside the
hospital
PCOs inside the hospital will continue to screen all patients arriving at their counters
For patients meeting the case definition, activate the plan for suspected COVID cases:

5
PCO to screen patient:--cough/fever/sore throat/ shortness
of breathAND
--ANY international travel; or travel to Karachi, Mardan or Raiwind; or
contact with a person with known or suspected COVID-19
--attended a religious congregation over the past 2 weeks
--Offer surgical mask (simple mask-not N-95)--Cough etiquette teachingLahore: send to camp COVIDPeshawar:Transfer to clinic room reserved for patients meeting case definitionInform Infection Control nurse and EAR resident
Assess severity of illness.
Does the patient require admission (O2 sats<94% on
room air and bilateral chest
infiltrates)?
-Inpatient management-Allocate single room-Follow contact and droplet precautions-Follow contact and airborne precautions for patients undergoing aerosol generating precedures*-Use eye protection for all patients-Collect nasopharyngeal swab for PCR ⴕ-Fill out PUI form
-Outpatient management -Follow contact and droplet precautions during evaluation-Follow contact + airborne precautions for patients undergoing aersol-generating procedures*-Use eye protection-Collect nasopharyngeal swab fro PCRⴕ-Fill out PUI form-Discharge with supportive medications
No additional steps required. Proceed as per routine.
Pathway for Patients with Suspected COVID-19 in the Outpatient Setting
YES NO
YES NO
* Patients with fever and
at least one sign/symptom
of respiratory disease, e.g.,
cough, shortness of breath
must have O2 sats checked
If < 94%, get CXR
If CXR reveals bilateral
infiltrates, test for COVID-
19 and transfer to
dedicated COVID ward
If COVID is ruled out,
admit to regular ward

6
PCO: patient care officer; PUI : person under investigation
*Aerosol generating procedures: nasopharyngeal sample collection, bronchoscopy, airway suctioning,
noninvasive ventilation, intubation, CPR, dental procedures, NG insertion, upper GI endoscopy
ⴕWear a simple surgical mask for nasopharyngeal samples collected in open air
All samples must be placed in a biohazard bag, then in a puncture proof container or a second biohazard
bag and transported to the lab.

7
COVID-19 Testing
Who should be tested for COVID-19?
Patients meeting the case definition
What COVID-19 test are we performing?
PCR on nasopharyngeal swab
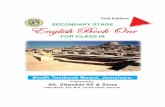
Nasopharyngeal swab must be collected as shown in the diagram below
Additionally, 5 ml of blood must be drawn in a purple top vial and transported to the lab for
storage as per NIH guidelines
Where will samples be collected?
For stable patients:
In open air
Those collecting the sample in open air should wear a surgical mask
For unstable patients in EAR/IPD/ICU:
In rooms with doors closed. Do not require negative pressure rooms for nasopharyngeal
sampling.
Those collecting the sample must wear N-95 masks
What is the reporting time for COVID-19 testing?
48 hours

8
Cleaning of rooms and medical equipment used for COVID-19 patients
The virus can persist on surfaces for up to 72 hours. It is crucial to clean rooms and medical
equipment as per hospital policy for contact and droplet/airborne precautions where applicable

9
Camp COVID PPE
PPE for all staff:
Gowns: 1 gown per shift; if leaving Camp COVID, discard your gown and use a new one once
back in Camp Covid
Surgical masks: 1 mask per shift
Faceshield: 1 faceshield per shift; if leaving Camp COVID, discard your faceshield and use a new
one once back in Camp Covid
Gloves: change between patients
Plastic apron: change between patients
PPE for those performing intubation, CPR
Gown: discard after use
N-95 masks:
discard N-95 after intubation and CPR
Faceshield: discard after use
Gloves: discard after use
PPE for those performing nasopharyngeal sampling:
Nasopharyngeal sampling must be performed in open air for stable patients wearing “PPE for all
staff” listed above
For sick patients who cannot be moved out of the camp into open air for sampling:
wear a gown, gloves, faceshield, N95, surgical mask over N95; once a sample has been collected,
discard the surgical mask and save the N-95 for reuse
PPE for transporting COVID patients (See page 13)

10
Section 2: COVID-19- Clinical Management
1. Clinical Management of COVID-19
Patients can be classified into asymptomatic, mild, moderate and
severe based on their presentation
Asymptomatic:
Nasopharyngeal RT- PCR positive for SARS CoV2 but having no symptoms
Mild:
Presence of symptoms consistent with COVID such as fever, fatigue, cough (with or without sputum
production), anorexia, malaise, muscle pain, sore throat, dyspnea, nasal congestion, or headache
without any hemodynamic compromise, need for oxygen or chest x-ray findings.
Moderate:
Hypoxia (oxygen saturation ≤ 94%) or mild infiltrate on chest x-ray. Persistent high-grade fever for >3
days. Absence of features suggestive of severe disease (listed below)
Severe
Fever, shortness of breath, signs/symptoms of respiratory tract infection and any of the following:
Adults
RR > 30 breaths/Min
Central cyanosis
Respiratory distress (unable to complete a sentence)
CURB score of more than 2
Confusion, agitation, restlessness
SpO2 ≤ 93% on Room air
Bilateral widespread infiltrates on CXR.
Clinically heart failure (gallop rhythm, raised JVP)
Oxygen Saturation/ FiO2 ratio less than 315
Evidence of heart failure (Raised JVP, Gallop rhythm)
Signs of shock: Delayed capillary refill; Cold, clammy peripheries; Mottled skin; Systolic BP less
than 90 or less than 40mm Hg of baseline in hypertensive; Urine output < 0.5 ml/kg/hr
Pediatric patients:
Central cyanosis or SpO2 < 90%
Severe respiratory distress (e.g. grunting, very severe chest indrawing)

11
Signs of pneumonia with a general danger sign: inability to breastfeed or drink, lethargy or
unconsciousness, or convulsions
Other signs of pneumonia may be present: chest indrawing, fast breathing (in breaths/min): < 2
months: ≥ 60; 2–11 months: ≥ 50; 1–5 years: ≥E 40
Criteria for admission of suspected or confirmed COVID-19 patients
Asymptomatic and mild disease
Can be managed at home with home isolation
Criteria for home isolation include (must fulfill all of the below)
1- Those with a separate room to stay in
2- Those consenting for isolation
Patients with mild or asymptomatic disease who do not have adequate home arrangements or
do not consent to stay at home should be shifted to a dedicated isolation facility (as opposed to
a hospital)
However, the following should be considered for hospital admission for observation if resources
allow.
1- Immunosuppressed (e.g. HIV, on long term steroids or other immunosuppression)
2- Age greater than or equal to 60 years
3- Co-morbid conditions: Heart Failure, Decompensated Liver Disease, Structural Lung Disease,
Uncontrolled Diabetes, Chronic Kidney Disease
If the patients cannot be admitted then clear instructions must be given to call if any worsening
occurs.
Moderate and severe disease
Patients should be admitted
Place in a negative pressure room (if available) if aerosol generating procedure(s) are
anticipated.
Other conditions requiring admission regardless of disease severity
Immunosuppressed (e.g. HIV, chemotherapy within the last 4 weeks or on long term steroids)
Heart failure,
Decompensated liver disease
Lung disease
CKD
home isolation not possible and ≥ 65 years

12
Management
Management guidelines for COVID-19 Disease are evolving rapidly. Treating physicians should consult an
infectious disease specialist. All management should be carried out only by a registered medical
practitioner.
Management of asymptomatic and mild disease
Treat with supportive care only. This includes acetaminophen for fever, oral hydration in case of
diarrhea and anti-histamines for rhinorrhea.
No specific treatment (including chloroquine or hydroxychloroquine) is recommended for
asymptomatic or mild disease. There is no role of prophylactic chloroquine or
hydroxychloroquine at this time
Management of moderate disease
Investigations
The following investigations should be done in all patients:
CBC
Electrolytes and serum creatinine
Chest X-ray
Additional investigations may include the
CRP (repeated if any evidence of clinical worsening)
LDH
Lactate
ECG (if age >40 or other comorbidities or if clinically indicated)
Cardiac enzymes if indicated
Liver function tests
Blood and respiratory cultures
Treatment
Supportive therapy with oxygen therapy via nasal cannula
Acetaminophen for fever control and intravenous fluids if needed should continue.
In case of lobar infiltrates, antibiotics may be considered especially if associated with high white
count
There is no current evidence from studies to recommend any specific anti-COVID-19 treatment
for patients with suspected or confirmed COVID-19 infection. Based on the best available
evidence, treatment with either of the following can be started:

13
1. Adults: Chloroquine 500 mg BD x 10 days; Pediatrics (Loading:10mg base/kg Maintenance:
5mg base/kg once daily Loading x 10 days)
2. Hydroxychloroquine sulfate 200 mg, three times per day x 10 days
On therapy, QT-interval must be monitored; especially if other medications are being
administered which prolong the QT-interval.
Management of severe disease
Investigations
Initial investigations and supportive care should proceed as in moderate disease.
Additional ingestions may be required according to the respiratory status of the patient,
including arterial blood gases and lactate levels.
Treatment
1. Empiric antibiotics may be considered if a secondary bacterial pneumonia is suspected (e.g. if raised
white blood cell count).
2. In patients with ARDS who are intubated, use conservative fluid management.
3. Cardiac impairment has been described and diuresis may be considered after consultation with
cardiology.
4. Do not give high-dose systemic corticosteroids or other adjunctive therapies.
5. Implement mechanical ventilation using lower tidal volumes (4–8 mL/kg predicted body weight, PBW)
and lower inspiratory pressures (plateau pressure < 30 cmH2O).
6. Finally, if expertise is available, in adults with severe ARDS, prone ventilation for 12–16 hours per day
is recommended.
There is no current evidence from studies to recommend any specific anti-COVID-19 treatment
for patients with suspected or confirmed COVID-19 infection. Based on the best available
evidence, treatment with either of the following can be started:
1. Adults: Chloroquine 500 mg BD x 10 days; Pediatrics (Loading: 10mg base/kg Maintenance:
5mg base/kg once daily Loading x 10 days)
2. Hydroxychloroquine sulfate 200 mg, three times per day during ten days
In addition other treatment options, which may be considered, include:
Lopinavir/ritonavir o 400/100mg BID 14 days
However these medications have considerable adverse effects, have limited available and
unclear efficacy. Consultation with an Infectious Diseases Specialist is mandatory prior to
prescribing.
2. Isolation Precautions and PPE for COVID-19 patients
Standard + contact+ droplet: for all patients

14
Standard+ contact+ airborne: for COVID-19 patients admitted in the ICU and those requiring
aerosol-generating procedures e.g. bronchoscopy, CPR, intubation, nasopharyngeal specimen
collection, noninvasive ventilation, airway suctioning, dental procedures, NG insertion, upper GI
endoscopy.
Eye protection: for all patients
To minimize exposure to airborne droplet nuclei, N-95 masks must form a tight seal around the
nose and mouth. Facial hair present along the edges of the mask prevents formation of this seal
and results in exposure to airborne infections.
Since specialized respirators are not available at our facility, staff members with
beards/sideburns/moustaches, who are expected to perform or assist with aerosol generating
procedures, or care for patients in the ICU or the floor must ensure that the area of the mask
seal is clean shaven The virus can persist on surfaces for up to 72 hours. Therefore, it is crucial to clean rooms and
medical equipment as per hospital policy for contact and droplet/airborne precautions where
applicable
PPE guidelines must be followed by ALL staff members entering patient rooms
3. Transporting COVID-19 patients
Patients must NOT be transported to other departments unless absolutely
In the event of transfer, do the following:
Inform the receiving department over the phone with details of isolation precautions required
Staff transferring patients from a bed to a wheelchair or stretcher are required to wear gloves,
gown and surgical mask
Once the patient has been moved and is ready for transport:
ensure that the patient wears a surgical mask
wipe the handles of wheelchair or stretcher with alcohol wipes
discard PPE and transport the patient; no PPE is required for transport
Once transferred, the patient should be moved directly to the intended IPD room/procedure
room etc. Patients must NOT be seated in the waiting area
Once inside the room at the destination unit, wear gloves, gown and surgical mask to move the
patient from the wheelchair/stretcher to the bed; remove and discard PPE inside the patient’s
room before leaving
Wheelchairs and stretchers must be disinfected with an approved disinfectant (alpha guard)
prior to reuse
4. Room allocation for COVID-19 patients
Single rooms must be allocated while patients are under investigation for COVID-19
Patients with confirmed COVID-19 may be cohorted i.e. placed in the same room

15
5. Patients with suspected or confirmed COVID-19 requiring medical
procedures
All elective procedures must be cancelled to minimize transport and avoid unnecessary
exposure to hospital staff and other patients
For patients requiring emergent/lifesaving procedures: i) schedule procedures at the end of list of possible ii) shift patients directly from the inpatient unit to the procedure room iii) bronchoscopies to be deferred; if absolutely necessary, perform in negative pressure rooms iv) In addition to standard PPE required for the planned procedure, the following apply: standard+ contact + airborne precautions + goggles/face shield for bronchoscopy standard+ contact + airborne precautions + goggles/face shield for upper GI endoscopy; disposable shoe and hair covers may be worn if procedures entail the risk of splashes standard+ contact+ droplet precautions for all other procedures that do not fall under aerosol generating procedures v) PPE guidelines must be followed by ALL staff members present inside the procedure rooms as well as housekeeping staff who clean these rooms following procedures vi) terminal cleaning of rooms to be performed as per hospital policy for contact and droplet/airborne isolation rooms
6. COVID-19 visitor policy
NO visitors will be allowed for adult patients
Pediatric patients are allowed one attendant who will be treated as though infected. The attendant will wear a mask and will not be allowed to leave the room.
7. COVID-19 patients and cardiopulmonary resuscitation Wear the appropriate PPE before participating in a code
8. When can isolation precautions be discontinued? The patient must meet the following criteria:
it has been >7 days since diagnosis AND
the patient has clinically improved and no longer requiring respiratory support AND
PCR testing is negative on 2 consecutive nasopharyngeal swabs taken 24 hours apart
9. What if there is strong clinical suspicion for COVID-19 but the test results are negative?
Continue isolation precautions and repeat nasopharyngeal PCR in 3 days
10. When can the patient be discharged?

16
Once clinically stable and deemed fit for discharge by the evaluating physician
Patients do not need to be quarantined at the hospital if medically stable
11. What instructions must patients be given on discharge? Patients with negative PCRs on 2 consecutive nasopharyngeal swabs taken at least 24 hours
apart no further steps required
Patients discharged without PCR testing on nasopharyngeal samples may be contagious until at least 7 days following initial diagnosis of infection; and 3 days after complete resolution of symptoms advise social distancing (avoid gatherings, maintain at least 1 meter distance from other individuals, frequent hand washing, practice cough etiquette)
Reinfection with SARS-CoV-2 has been reported in the literature. Patients with any worsening following discharge must return to the EAR for evaluation.

17
Section 3: Personal Protective Equipment (PPE)

18
PPE Guidelines for EAR, IPD, ICU and other Clinical Areas
Follow standard precautions and strictly adhere to the 5 moments of hand hygiene for patients in all
clinical areas
EAR
All Staff:
Must wear surgical masks
Follow the are below the elbows (BBE) policy:
Must roll sleeves to an inch above the elbows
No jewelry/rings/bracelets or wrist watches to be worn
Trim nails to < 1/4 of an inch
No nail paint or artificial nails to be worn
May wear surgical scrubs. Use OR changing rooms. Must change out of scrubs before leaving the
hospital
Staff examining/assessing patients/performing vitals/collecting samples:
Gloves, plastic apron, surgical mask
Gloves and plastic aprons must be changed between patients
Use the same surgical mask for the entire shift unless damaged or visibly soiled
If, upon evaluation, a patient in the EAR is suspected to have COVID-19:
Immediately move to an isolation room and follow droplet and contact precautions; use eye
protection
PPE includes gloves, gown, surgical mask, eye protection
Taking a COVID-19 nasopharyngeal sample in the EAR:
Must be performed in a negative pressure room, following airborne precautions
PPE includes gloves, gown, N-95 mask*, faceshield/goggles^
IPD
Suspected cases must be placed in individual isolation rooms
Confirmed COVID-19 patients may be cohorted (placed in the same room)
Staff caring for suspected/confirmed COVID-19 cases:
Follow droplet and contact precautions; use eye protection
PPE includes gloves, gown, surgical mask, faceshield/goggles^
Staff caring for suspected or confirmed COVID-19 patients undergoing aerosol generating
proceduresⴕ:

19
PPE includes gloves, gown, N-95 mask*, faceshield/goggles^
ICU
Staff caring for suspected or confirmed COVID-19 patients in the ICU:
Require airborne+ contact precautions and eye protection
PPE to be worn by all staff when entering patients’ rooms: gloves, gown, N-95 mask*,
faceshield/goggles^
ICU staff must wear ICU scrubs. Use ICU changing rooms. Must change out of scrubs before
leaving the ICU.
ⴕ Aerosol-generating procedures: bronchoscopy, CPR, intubation, nasopharyngeal specimen collection,
noninvasive ventilation, airway suctioning
^Disinfect goggles with alcohol wipes before and after use. Following use, goggles must be placed in
designated drawers in isolation trolleys to be used by the next person
*N-95
N-95 masks may be obtained from unit coordinators (UCs). UCs must maintain a record of employees
who have been issued N-95 masks with the date the mask was issued.
Write your employee code on the mask prior to use
Write employee code on a paper bag prior to use and leave on the isolation trolley. These may be
obtained from unit coordinators covering the shift (image on page 18)
Wear a surgical mask on top of the N-95 to prevent mask contamination.
Following use, discard the surgical mask
Remove the N-95 mask carefully, without touching the front surface and place in the paper bag
Masks may be reused for up to 7 days or unless visibly soiled or damaged. If your mask is damaged, or
visibly soiled or no long forms a tight seal around your face and mouth, you must notify the UC and
submit the used mask to obtain a new N-95 mask.
N95 masks worn during intubation cannot be reused and must be discarded. Please note that CDC
currently recommends that masks not be reused following any aerosol generating procedures; however,
given the regional and global shortage of N-95 masks, you may continue to reuse N-95 masks worn
during aerosol generating procedures (other than intubation) as long as you wear a surgical mask on top
of the N-95.
Yellow bins for clinical waste must be placed inside and outside patients’ rooms
Items to be removed inside patients’ rooms:
gloves, followed by gown
Items to be removed outside patients’ rooms:
goggles, followed by mask
Each isolation room must have a dedicated stethoscope
Disinfect with alcohol wipes before and after each use. Following use, leave stethoscopes inside the
room to be used by the next person

20
If multiple patients with confirmed COVID-19 need to be seen:
do not remove goggles and mask between patients
perform hand hygiene before and after seeing patients
change gown and gloves between patients
Recommendations for staff in all clinical areas:
PPE Guidelines for all staff in other clinical areas (ICU, inpatient, OPAT, chemobay, EHC, radiology,
radiation, nuclear medicine, endoscopy, phlebotomy):
Those working in clinical areas are required to wear surgical masks throughout the shift. Use 1 mask
per shift.
Secretaries/managers in the relevant departments will issue 7 masks once a week and maintain
records. Masks will be reissued once the employee has completed 7 shifts.
These masks will only be issued to those currently working these areas or expected to work in these
areas during the upcoming week.
For patients requiring additional isolation precautions (contact, airborne etc.) follow the relevant PPE
guidelines.
Recommendations for PPE Reuse:
Items to be used ONCE only: i) Gloves ii) Gowns iii) Shoe covers, where applicable
Items that can be reused
i) Goggles
Disinfect with alcohol wipes before and after use.
Following use, goggles must be placed in designated drawers in isolation trolleys to be used by the
next person
ii) N-95
N-95 masks may be obtained from unit coordinators (UCs). UCs must maintain a record of employees
who have been issued N-95 masks with the date the mask was issued.
Write your employee code on the mask prior to use
Write employee code on a paper bag prior to use and leave on the isolation trolley. These may be
obtained from unit coordinators covering the shift (image on page 18)
Wear a surgical mask on top of the N-95 to prevent mask contamination.
Following use, discard the surgical mask
Remove the N-95 mask carefully, without touching the front surface and place in the paper bag
Masks may be reused for up to 7 days or unless visibly soiled or damaged. If your mask is damaged, or
visibly soiled or no long forms a tight seal around your face and mouth, you must notify the UC and
submit the used mask to obtain a new N-95 mask.
N95 masks worn during intubation cannot be reused and must be discarded. Please note that CDC
currently recommends that masks not be reused following any aerosol generating procedures; however,

21
given the regional and global shortage of N-95 masks, you may continue to reuse N-95 masks worn
during aerosol generating procedures (other than intubation) as long as you wear a surgical mask on top
of the N-95.
iii) Surgical mask:
The same surgical mask may be worn per shift unless visibly soiled or damaged
Do not touch the front surface of the mask

22
Section 4: Frequently Asked Questions (FAQs)
1. What resources are these guidelines based on?
• CDC, WHO, NHS
2. What is the policy for pregnant healthcare workers?
• Pregnant healthcare workers will not be working in any clinical area.
3. What should employees with cough/cold symptoms do?
• Employees are being screened at the laundry services building entrance
• Those meeting the case definition will be referred to Camp COVID
4. How can hospital staff protect themselves from COVID-19?
• Adhere to hand hygiene policies
• Practicing good cough etiquette (cover your cough with your sleeve or tissue, appropriately
dispose of used tissues), avoid touching eyes and mouth
• Avoid crowds and gatherings. Social distancing.
5. What is the policy on code blue situations where the patient is a suspected or
known cases of COVID-19, or the COVID-19 infectivity status is unknown e.g
patients who are pulseless or code soon after arrival in the EAR?
• Wear gloves, gown, mask, N-95, faceshield or goggles. Do not participate in codes without the
appropriate PPE.

23
Appendix A: Patient Under Investigation (PUI) Form

24
Patient Under investigation (PUI) Form: Coronavirus Disease (COVID-19)
Shaukat Khanum Memorial Cancer Hospital & Research Centre
PUI Criteria
Date of symptom onset___________________________________________________
Does the patient have the following signs and symptoms (check all that apply)?
☐ Fever1 ☐ Cough ☐ Sore throat ☐ Shortness of breath
Does the patient have these additional signs and symptoms (check all that apply)?
☐ Chills ☐ Headache ☐ Muscle aches ☐ Vomiting ☐ Abdominal pain ☐ Diarrhea ☐ Other, Specify_______________
Any International travel over the past 14 days before symptom onset
Country name:______________________________________
Date traveled to: ___________________ Date traveled from: _________________________ Date arrived in Pakistan: ______________________________
☐ Y ☐ N ☐ Unknown
Have close contact2 with a person under investigation for COVID-19? ☐ Y ☐ N ☐ Unknown
Have close contact2 with a laboratory-confirmed COVID-19 case? In which country was the case diagnosed with COVID-19? ______________________________
☐ Y ☐ N ☐ Unknown
Have close contact2 with an individual returning from international travel? Which country did the contact return from? ______________________________
☐ Y ☐ N ☐ Unknown
Additional Patient Information
Is the patient a health care worker? ☐ Y ☐ N ☐ Unknown
Have history of being in a healthcare facility (as a patient, worker, or visitor)? ☐ Y ☐ N ☐ Unknown
Care for a COVID-19 patient? ☐ Y ☐ N ☐ Unknown
Diagnosis (select all that apply): Pneumonia (clinical or radiologic) ☐ Y ☐ N Acute respiratory distress syndrome ☐ Y ☐ N
Comorbid conditions (check all that apply): ☐ None ☐ Unknown ☐ Pregnancy ☐ Diabetes ☐ Cardiac disease ☐ Hypertension
☐ Chronic pulmonary disease ☐ Chronic kidney disease ☐ Chronic liver disease ☐ Immunocompromised
☐ Cancer, specify type
☐ Other, specify
Vital Signs: Temp: __________ Pulse: _________ RR: __________BP: __________ SpO2:__________Chest exam: _________________
Does the patient have another diagnosis/etiology for their respiratory illness? ☐ Y, Specify______________ ☐ N ☐ Unknown
Specimens for COVID-19 testing
Specimen type Collected by (Name and Employee Code)
Transported by (Name and Employee Code)
Date collected
1 Fever may not be present in some patients, such as those who are very young, elderly, immunosuppressed, or taking certain medications. Clinical judgement should be used to guide testing of patients in such situations
2 Close contact is defined as: a) being within approximately 6 feet (2 meters) or within the room or care area for a prolonged period of time (e.g., healthcare personnel, household
members) while not wearing recommended personal protective equipment (i.e., gowns, gloves, respirator, eye protection); or b) having direct contact with infectious secretions (e.g.,
being coughed on) while not wearing recommended personal protective equipment. Data to inform the definition of close contact are limited. At this time, brief interactions, such as
walking by a person, are considered low risk and do not constitute close contact
Patient first name _______________ Patient last name ___________________ Patient date of birth ______________________
Sex ☐ M ☐ F Nationality ___________________Place of Residence ________________________________________________
Patient NIC number____________________________Contact # _____________________________Marital Status:_____________
MR # (if generated) _________________________________ Screening date______________________________________
Physician’s name ___________________________________ Employee Code number_____________________________