Severe acute respiratory distress syndrome in coronavirus ...manuelosses.cl/BNN/2021/Severe acute...
10
Severe acute respiratory distress syndrome in coronavirus disease 2019einfected pregnancy: obstetric and intensive care considerations William T. Schnettler, MD; Yousef Al Ahwel, MD; Anju Suhag, MD Since the emergence of a novel coronavirus (severe acute respiratory syndrome coronavirus 2) in Wuhan, China, at the end of December 2019, coronavirus disease 2019 has been associated with severe morbidity and mortality and has left world governments, healthcare systems, and pro- viders caring for vulnerable populations, such as pregnant women, wrestling with the optimal management strategy. Unique physiologic and ethical considerations negate a one-size-fits-all approach when caring for critically ill pregnant women with coronavirus disease 2019, and few resources exist to guide the multidisciplinary team through decisions regarding optimal maternal-fetal surveillance, intensive care procedures, and delivery timing. We present a case of rapid clinical decompensation and development of severe acute respiratory distress syndrome in a woman at 31 weeks’ gestation to highlight these unique considerations and present an algorithmic approach to the diagnosis and management of the disease. Key words: acute SARS-CoV-2, ARDS, coronavirus, COVID-19, pneu- monia, pregnancy, respiratory distress syndrome A s of April 3, 2020, there have been 972,303 total cases of coronavirus disease 2019 (COVID-19) with 50,322 deaths (5.2% mortality rate) worldwide, and it is spreading rapidly with a basic reproduction number (R0) of 2e2.5, suggesting that 2e3 people will become infected from an index patient. 1,2 Although the United States now has the highest number of cases (239,279), the US mortality rate is less than half than that seen worldwide at 2.3% (5443 confirmed deaths) and the hospitaliza- tion rate remains low at 24.1 per 100,000 population. 3 These statistics may encourage skeptics eager to challenge the severity of this public health crisis. However, the rates of critical illness and mortality associated with COVID-19 among pregnant women—a potentially highly vulnerable population—remain unclear. 4e7 We present the clinical challenges and potential strategies for optimal maternal-fetal surveillance, intensive care procedures, and delivery timing in a case of a pregnant woman at 31 weeks’ gestation who presented to a tertiary care hospital in Cincinnati, Ohio, with COVID-19 symptoms, laboratory ab- normalities, and chest-imaging findings immediately before the development of rapid clinical decompensation and se- vere acute respiratory distress syndrome (ARDS) requiring prolonged mechanical ventilation and ultimately indicated preterm delivery. Case Study A 39-year-old white G6 P2031 with a 31.0-week live singleton intrauterine gestation conceived through in vitro fertilization required admission on March 24, 2020, from the emergency department of a tertiary care center in Cincinnati, Ohio, due to complaints of 5 days of worsening nonproductive cough, shortness of breath, fever, and malaise. Four days before admission (March 20, 2020; COVID-19 day 1, Figure 1), she had been discharged from the emer- gency department after workup for a milder presentation of these symptoms that included normal findings on chest x-ray examination, normal vital sign assessment, and normal results of a res- piratory viral pathogen laboratory anal- ysis including influenza A and B rapid screening. Of note, a nasopharyngeal swab for COVID-19 reverse transcrip- tase polymerase chain reaction (RT- PCR) was sent to the Ohio Department of Health at that time, but results did not return for 8 days and were still pending when she re-presented on March 24, 2020 (COVID-19 day 5). She had pre- viously established early and complete prenatal care through the Maternal-Fetal Medicine (MFM) service owing to un- derlying mild myotonic dystrophy (without cardiomyopathy), bicuspid aortic valve (without aortic dilation, stenosis, or regurgitation), history of 2 previous low-transverse cesarean de- liveries, and history of a previous mild cerebrovascular accident while on com- bined oral contraceptives. Her pregravid body mass index was 24.7 kg/m 2 , and she denied any tobacco or illicit substance abuse. Serial surveillance with obstetric ultrasound imaging and maternal echo- cardiography suggested that her preg- nancy had thus far been without complication, and she had been compliant with prescribed daily pro- phylactic low-molecular-weight heparin. Upon re-presentation to the emer- gency department (COVID-19 day 5), her symptoms had progressed to include fever at 101 F, worsening shortness of breath adversely affecting the ability to complete full sentences, and persistent nonproductive cough (Figure 1). Initial vital sign assessment identified signifi- cant tachypnea (respiratory rate of 32 breaths per minute), mild tachycardia (heart rate in the low 100’ s beats per minute), low normal blood pressure (mean arterial pressure [MAP] in the low 70’ s mm Hg), and mild hypoxia (SpO 2 93%) despite 4 L of oxygen via nasal cannula. Physical examination was Cite this article as: Schnettler WT, Al Ahwel Y, Suhag A. Severe acute respiratory distress syndrome in COVID-19- infected pregnancy. Am J Obstet Gynecol MFM 2020;2:100120. 2589-9333/$36.00 ª 2020 Elsevier Inc. All rights reserved. https://doi.org/10.1016/j.ajogmf.2020.100120 AUGUST 2020 AJOG MFM 1 Research Letter
Transcript of Severe acute respiratory distress syndrome in coronavirus ...manuelosses.cl/BNN/2021/Severe acute...

Research Letter
Severe acute respiratory distress syndrome incoronavirus disease 2019einfected pregnancy:obstetric and intensive care considerations
William T. Schnettler, MD; Yousef Al Ahwel, MD; Anju Suhag, MDSince the emergence of a novel coronavirus (severe acute respiratory regarding optimal maternal-fetal surveillance, intensive care procedures,
syndrome coronavirus 2) in Wuhan, China, at the end of December 2019,
coronavirus disease 2019 has been associated with severe morbidity and
mortality and has left world governments, healthcare systems, and pro-
viders caring for vulnerable populations, such as pregnant women,
wrestling with the optimal management strategy. Unique physiologic and
ethical considerations negate a one-size-fits-all approach when caring for
critically ill pregnant women with coronavirus disease 2019, and few
resources exist to guide the multidisciplinary team through decisions
Cite this article as: Schnettler WT, Al Ahwel Y, Suhag A.Severe acute respiratory distress syndrome in COVID-19-
infected pregnancy. Am J Obstet Gynecol MFM
2020;2:100120.
2589-9333/$36.00ª 2020 Elsevier Inc. All rights reserved.https://doi.org/10.1016/j.ajogmf.2020.100120
and delivery timing. We present a case of rapid clinical decompensation
and development of severe acute respiratory distress syndrome in a
woman at 31 weeks’ gestation to highlight these unique considerations
and present an algorithmic approach to the diagnosis and management of
the disease.
Key words: acute SARS-CoV-2, ARDS, coronavirus, COVID-19, pneu-monia, pregnancy, respiratory distress syndrome
s of April 3, 2020, there have been
A 972,303 total cases of coronavirusdisease 2019 (COVID-19) with 50,322deaths (5.2% mortality rate) worldwide,and it is spreading rapidly with a basicreproduction number (R0) of 2e2.5,suggesting that 2e3 people will becomeinfected from an index patient.1,2Although the United States now has thehighest number of cases (239,279), theUS mortality rate is less than half thanthat seen worldwide at 2.3% (5443confirmed deaths) and the hospitaliza-tion rate remains low at 24.1 per 100,000population.3 These statistics mayencourage skeptics eager to challenge theseverity of this public health crisis.However, the rates of critical illness andmortality associated with COVID-19among pregnant women—a potentiallyhighly vulnerable population—remainunclear.4e7
We present the clinical challengesand potential strategies for optimalmaternal-fetal surveillance, intensivecare procedures, and delivery timing in acase of a pregnant woman at 31 weeks’gestationwho presented to a tertiary care
hospital in Cincinnati, Ohio, withCOVID-19 symptoms, laboratory ab-normalities, and chest-imaging findingsimmediately before the development ofrapid clinical decompensation and se-vere acute respiratory distress syndrome(ARDS) requiring prolongedmechanicalventilation and ultimately indicatedpreterm delivery.
Case StudyA 39-year-old white G6 P2031 with a31.0-week live singleton intrauterinegestation conceived through in vitrofertilization required admission onMarch 24, 2020, from the emergencydepartment of a tertiary care center inCincinnati, Ohio, due to complaints of 5days of worsening nonproductive cough,shortness of breath, fever, and malaise.Four days before admission (March 20,2020; COVID-19 day 1, Figure 1), shehad been discharged from the emer-gency department after workup for amilder presentation of these symptomsthat included normal findings on chestx-ray examination, normal vital signassessment, and normal results of a res-piratory viral pathogen laboratory anal-ysis including influenza A and B rapidscreening. Of note, a nasopharyngealswab for COVID-19 reverse transcrip-tase polymerase chain reaction (RT-PCR) was sent to the Ohio Departmentof Health at that time, but results did notreturn for 8 days and were still pendingwhen she re-presented on March 24,
2020 (COVID-19 day 5). She had pre-viously established early and completeprenatal care through theMaternal-FetalMedicine (MFM) service owing to un-derlying mild myotonic dystrophy(without cardiomyopathy), bicuspidaortic valve (without aortic dilation,stenosis, or regurgitation), history of 2previous low-transverse cesarean de-liveries, and history of a previous mildcerebrovascular accident while on com-bined oral contraceptives. Her pregravidbodymass index was 24.7 kg/m2, and shedenied any tobacco or illicit substanceabuse. Serial surveillance with obstetricultrasound imaging and maternal echo-cardiography suggested that her preg-nancy had thus far been withoutcomplication, and she had beencompliant with prescribed daily pro-phylactic low-molecular-weight heparin.
Upon re-presentation to the emer-gency department (COVID-19 day 5),her symptoms had progressed to includefever at 101�F, worsening shortness ofbreath adversely affecting the ability tocomplete full sentences, and persistentnonproductive cough (Figure 1). Initialvital sign assessment identified signifi-cant tachypnea (respiratory rate of 32breaths per minute), mild tachycardia(heart rate in the low 100’s beats perminute), low normal blood pressure(mean arterial pressure [MAP] in thelow 70’s mm Hg), and mild hypoxia(SpO2 93%) despite 4 L of oxygen vianasal cannula. Physical examination was
AUGUST 2020 AJOG MFM 1

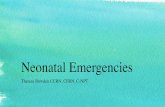
FIGURE 1Clinical course, major symptoms, and outcomes from illness onset in thispatient with COVID-19erelated critical illness and severe ARDS
FeverCough
DyspneaSevere ARDS/ICU admission
Invasive ven�la�onHydroxychloroquine
RemdesivirDays a�er illness onset 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 (COVID disease day #)
RT-PCR returned posi�ve DeliveryARDS, acute respiratory distress syndrome; COVID-19, coronavirus disease 2019; ICU, intensive care unit.
Schnettler et al. Severe acute respiratory distress syndrome in COVID-19einfected pregnancy. AJOG MFM 2020.
Research Letter
notable for rhonchi and egophonythroughout all lung fields. A chest x-ray,computed tomography (CT) pulmonaryangiogram, and lung ultrasound assess-ment were performed (Figure 2). Theattending emergency department pro-vider ordered the CT pulmonary angio-gram to investigate the potential forpulmonary embolism, and lung ultra-sound was performed at bedside by theattending MFM physician to furtherinvestigate the potential for COVID-19pneumonia. Specifically, her chest x-rayexamination identified bilateral diffusepulmonary infiltrates, and her chest CTscan identified bilateral airspace diseasecharacterized by ground-glass appear-ance with peripheral consolidationscompatible with viral pneumonia. Herlung ultrasound demonstrated bilateralpleural thickening and nodularity of thevisceral pleura (Figure 2). Horizontal A-lines representing normal aerated lungwere absent and replaced by multiple B-lines, pleural nodularity and thickening,and an overall “white lung” appearancewith focal areas of consolidation.
Laboratory analysis identified anormal PaO2:FiO2 ratio of >300 (sug-gesting no evidence of ARDS) but defi-nite leukopenia (7700/mL), lymphopenia(800/mL), thrombocytopenia (114,000/mL), elevated transaminases (AST 65 IU/L), and a mildly elevated procalcitonin(0.33 ng/mL). Although the results fromher previous COVID-19 RT-PCR werepending, her clinical presentation sup-ported the diagnosis of COVID-19 withpneumonia and the potential for ARDS.
2 AJOG MFM AUGUST 2020
The emergency department physicianthought that her SpO2 of 93% on 4 L/min oxygen via nasal cannula andPaO2:FiO2 ratio of >300 were appro-priate for admission to the hospital’slower-acuity COVID-19 floor, and herdisposition was planned to that unit.However, the attending MFM physicianrecognized her SpO2 as abnormal forpregnancy and redirected her care to theintensive care unit (ICU). The degree ofprobable COVID-19 at this point wassevere.8
Upon arrival to a negative pressureroom in the ICU, she was placed on strictisolation with airborne precautions.Reassessment of her SpO2 revealedworsening hypoxia (78%) despite 4 L/min of oxygen via nasal cannula. Anonrebreather mask was applied, andinhaled oxygen rate was increased to 15L/min. Her SpO2 increased to 82%, butshe complained of feeling exhaustedwith inspiration; hence the decision wasmade to proceed with rapid sequenceintubation with planned mechanicalventilation for respiratory failure andcritical illness severity (approximately9.5 hours after presentation to theemergency department). Continuouselectronic fetal monitoring was initiatedand demonstrated a 3-minute prolongedfetal heart rate deceleration to 80 beatsper minute that spontaneously resolvedafter intubation. During this briefperiod, plan for emergent delivery wasconsidered. However, maximal ventila-tory assistance was applied, and both thematernal and fetal status improved,
prompting initiation of both antenatalcorticosteroid administration and mag-nesium sulfate for the dual benefit offetal neuroprotection and control ofmaternal bronchospasm (6-g bolus over20 minutes intravenously followed by 2g/h intravenously). She required largedosages of intravenous (IV) benzodiaz-epines and narcotics for sedation, andher MAP dropped below 65 mm Hgrequiring continuous infusion ofnorepinephrine.
Over the next 8 hours, the ventilatorsettings were increased to 100% FiO2
and positive end-expiratory pressure(PEEP) of 10 cm H2O, without com-plete resolution of hypoxia (SpO2
approximately 90%e93%). A volumecontrol ventilation modality withautomatic pressure augmentation(VCþ) was employed to minimizevolu- and barotrauma with thefollowing settings: respiratory rate of 20breaths per minute, tidal volume of 6mL/kg, FiO2 of 100%, inspiratory-to-expiratory time of 1:1.3, and PEEPof 10cmH2O. The PaO2:FiO2 ratio remainedbelow 150, signifying severe ARDS perAmerican-European Consensus Con-ference criteria.9 Surprisingly, the fetalheart rate remained reassuring andsignified a certain degree of maternalstability. Per recommendations bythe infectious disease specialist, thefollowing medications were initiated:ceftriaxone, azithromycin, oseltamivir,and hydroxychloroquine. There wasno marked improvement in heroxygenation until the team manuallyplaced her in a prone position per thePROSEVA study protocol.9 The initialplan included using a mechanicalrotating bed designed for prone ventila-tion, but manual prone positioning waspreferred due to the ability to morequickly return her to supine positioningfor performance of cardiopulmonaryresuscitation or emergent delivery.Manual pronation required a collabora-tive effort involving the intensive careand obstetric team members to establishinvasive hemodynamic monitoring(central venous access and arterial lineaccess), secure her airway, cushion andsupport her gravid abdomen, andmaintain continuous tocodynamometry

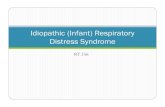
FIGURE 2Lung imaging findings and sonography location in a case of COVID-19
Patient’s chest imaging including chest CT (A) with ground-glass opacities and peripheral consolidation bilaterally (arrows), chest x-ray film (B) indicatingbilateral diffuse pulmonary infiltrates (arrow), normal (different healthy patient) lung ultrasound (C) with characteristic normal A-lines (arrow), and thepatient’s abnormal lung ultrasound images (DeF) demonstrating abnormal B-lines (arrow, D), pleural thickening and nodularity (arrow, E), and focalsubpleural consolidation (arrow, F) with underlying “white lung” (arrow, F), and a schematic (G) depicting the 12 anatomic locations to thoroughly evaluatethe lung with sonography.COVID-19, coronavirus disease 2019.
Schnettler et al. Severe acute respiratory distress syndrome in COVID-19einfected pregnancy. AJOG MFM 2020.
Research Letter
and electronic fetal heart rate moni-toring (Figure 3). This allowed forgradual reduction of FiO2 and PEEPrequirements.
Her care throughout the followingweek involved multidisciplinary “hud-dles” twice daily to elicit input from theInfectious Disease specialists,
Pulmonology and Critical care teams,MFM teams, Anesthesia Critical Carespecialists, Cardiology, Cardiothoracicsurgeons, Neonatology, and Obstetric
AUGUST 2020 AJOG MFM 3

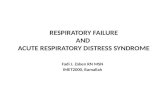
FIGURE 3A depiction of pad placement andbody positioning to achievemanual prone ventilation in apregnant woman with severecoronavirus disease2019erelated acute respiratorydistress syndrome
When the patient is supine, 6 to 8 standardhospital bed pillows are placed across the pa-tient’s face, upper chest and arms, lateralabdomen on each side, pelvis, and upper legs. Abedsheet is draped over these pillows and thenrolled together with the bedsheet beneath thepatient’s back on each side to create a “sand-wich.” The team members grasp the rolledsheets on each side and use them to roll thepatient onto her side and then prone such thatthe pillows remain in position as shown.
Schnettler et al. Severe acute respiratory distress syndrome inCOVID-19einfected pregnancy. AJOG MFM 2020.
Research Letter
nursing teams. Plans were establishedregarding staff exposure mitigation,emergency preparedness, deliverytiming, neonatal resuscitation, nutri-tional support (oral gavage feedings),venous thromboembolism prophylaxis(subcutaneous heparin twice daily), andadjunctive measures including the po-tential for inhaled pulmonary vasodila-tors (epoprostenol) and extracorporealmembrane oxygenation (ECMO). Shehad a positive COVID-19 RT-PCR resulton hospital day 4 (COVID-19 day 8),and strict isolation with airborne dropletprecautions was maintained. Consentand regulatory permission were ob-tained to allow for initiation of a 10-daycourse of remdesivir—a promisingantiviral agent targeting a wide array ofRNA viruses including severe acute res-piratory syndrome (SARS)/Middle Eastrespiratory syndrome coronavirus.7
Daily lung ultrasound assessments
4 AJOG MFM AUGUST 2020
revealed a lack of visual improvement toher sonographic findings. She wasrotated between the prone and left lateraldecubitus positions each day with agradual tolerance toward longer dura-tions out of the prone position on hos-pital days 6 and 7. This tolerancecombined with a gradual reduction inFiO2 and PEEP requirements negatedthe need to move forward with deliveryor to institute inhaled pulmonary vaso-dilators or ECMO.On hospital day 8 (COVID-9 day 13)
at 32.0 weeks’ gestation, continuoustocodynamometry and fetal heart ratetracing began to demonstrate regularuterine contractions with persistent latedecelerations. This prompted a “huddle”and mobilization of all teams to preparefor urgent but nonemergent delivery viarepeat cesarean delivery. Her ICUventilator circuit was maintained andtransported with her to the operatingsuite to minimize exposure duringtransport. Bedside echocardiographywas used to monitor her intravascularvolume status to help guide fluid resus-citation. Repeat laboratory assessmentrevealed a mild coagulopathy (elevatedinternational normalized ratio, 1.7;prothrombin time, 20.2 seconds; andactivated partial thromboplastin time,35.1 seconds), and preparations weremade for prevention of massive hemor-rhage including procurement of bloodproducts and uterotonics (oxytocin andmisoprostol) in the operating room. Avertical midline skin incision was madeto optimize exposure and minimizevascular injury in case of hemorrhage.Delayed cord clamping was intentionallynot employed, and the neonatology teamused an adjacent operating room forneonatal resuscitation to minimize staffand newborn exposure to the mother.The patient tolerated the repeat low-transverse cesarean delivery quite wellwithout postpartum hemorrhage orrespiratory compromise. She returned tothe ICU where her status continued toimprove over the next several days. A“de-brief” was held among all teammembers to review opportunities forimprovement. Umbilical cord blood gasanalysis revealed a normal pH of 7.2,PCO2 of 63 mmHg, PaO2 of 21 mmHg,
and base deficit of 3, and the malenewborn transitioned to extrauterine lifewithout complication and was extubatedon day of life (DOL) 3. His amnioticfluid and nasopharyngeal swabs weresent for COVID-19 RT-PCR analysis onDOL 1 and 2 (24 hours apart), and thetest results were negative. Because of theneed to maintain strict isolation andairborne/droplet precautions, the pa-tient’s husband was prohibited fromvisiting either his wife or his newbornson for a total of 14 days. Currently(hospital day 17/COVID-19 day 22), sheis improving but continues on synchro-nized intermittent mandatory ventila-tion with FiO2 of 35%, no PEEPrequirement, and daily attempts ofspontaneous breathing trials.
DiscussionThis case highlights the rapidity ofCOVID-19 in pregnancy with develop-ment of severe COVID-19erelatedARDS within 10 hours of admission andthe importance of considering physio-logic maternal adaptations in delineatingan algorithmic approach. The maternalphysiologic adaptations to pregnancynot only leave the woman more vulner-able to cell-mediated viral infectionssuch as COVID-19 but also more sus-ceptible to rapid cardiopulmonarydecompensation because of reducedcardiac and pulmonary reserves. Suchconsiderations may not be the priorityfor intensive care team members, andthese physiologic alterations must beemphasized by the obstetric providersbecause they assist in serving in a“quarter-back” role, leading the imple-mentation of the algorithmic approach.Such approach must entail input frommultiple disciplines and establish aframework for optimal team dynamicsusing daily “huddles” or other openmeans of direct communication. Thisplanning should occur before any pa-tient’s arrival wherein the myriad ofteam members establish a consensusregarding optimal imaging in-vestigations, laboratory studies, COVIDtesting, fetal assessment, and admissionlocations for these women. The team’ssafety must also remain a priorityensuring appropriate personal protective

FIGURE 4AeC, Example management algorithm for the pregnant patient with COVID-19
Schnettler et al. Severe acute respiratory distress syndrome in COVID-19einfected pregnancy. AJOG MFM 2020. (continued)
Research Letter
equipment, staffing (nurse-to-patientratio), facilities equipped to minimizeexposure, and mobile or handheldequipment with easy cleaning/disinfect-ing. An example of our managementalgorithm is included for reference butshould be individualized to one’s owninstitution (Figure 4).
One of the most difficult yet crucialaspects of the management approach isdetermining the delivery timing. Thephysiologic adaptations to labor, de-livery, and immediate postpartumperiod include maximization of thematernal cardiac output, autotransfu-sion of up to 500 mL of blood back intothe intravascular compartment, a cate-cholaminergic surge, release of inflam-matory mediators within theendothelium, and considerable fluidshifts between the interstitial, intracel-lular, and intravascular compartments.In the setting of severe systemic infec-tion, these physiologic changes canexacerbate dysregulated inflammatorycascade leading to a higher potential forendothelial dysfunction, pulmonary
edema, myocardial edema, and cardiacdysfunction.10 Thus, the decision toproceed toward delivery should be de-ferred in severe and critical maternalCOVID-19 cases until maternal cardio-pulmonary stability can be achievedunless the pregnancy has reached fullterm, fetal status is nonreassuring, ormaternal status is so dire that evacuationof the uterus is likely to facilitateimprovement in cardiopulmonaryfunction.4 Consideration for adminis-tration of antenatal corticosteroidsbefore anticipated preterm birth iscontroversial in severe maternalCOVID-19 cases. Evidence from treat-ment studies for SARS suggested thathigh dosages of corticosteroids posed arisk for severe adverse effects that dras-tically affected prognosis, but shortercourses of low to moderate dosages maybe considered in the care for the criticallyill patient with COVID-19.11 The deci-sion regarding administration magne-sium sulfate administration for fetalneuroprotection before 32 weeks’ gesta-tion should proceed per standard
indications in that this agent may pro-vide an additional benefit of broncho-dilation in the setting of bronchospasmafter intubation. Caution is advised tominimize fluid overload with theadministration of magnesium sulfatebecause of the potential for developmentof additional pulmonary edema, and werecommend restricting the total volumeof infused IV fluids to 125 mL/h or less.Delayed cord clamping and immediateskin-to-skin maternal contact shouldbe avoided.4 Table 1 represents ourapproach to delivery considerationsincluding timing, location, andmedications.
When attempting to defer deliveryand achieve resolution of acute maternalillness with supportive care, severaladjunctive therapies should be consid-ered. Emerging evidence suggests thatantiviral agents such as hydroxy-chloroquine and remdesivir may beeffective against severe acute respiratorysyndrome coronavirus 2, but neur-aminidase inhibitors such as oseltamivirhave no proven benefit.12,13 Although
AUGUST 2020 AJOG MFM 5

FIGURE 4(Continued )
Schnettler et al. Severe acute respiratory distress syndrome in COVID-19einfected pregnancy. AJOG MFM 2020. (continued)
Research Letter
the safety of these agents in pregnancyhas not been definitely determined andtheir efficacy remains controversial, thepharmacokinetic properties and mech-anisms of action may support theirjudicious use while we await furtherclinical trials. Noninvasive modes ofventilation such as “continuous positiveairway pressure ” or “bilevel positiveairway pressure” are not recommendedfor managing acute hypoxemic respira-tory failure owing to their increasedlikelihood of failure with need for moreurgent transition to invasive ventila-tion.14 Rapid sequence endotrachealintubation should be performed perroutine but with consideration for aslightly smaller endotracheal tube size
6 AJOG MFM AUGUST 2020
because of the potentially edematousand narrowed airway calibers in preg-nancy. Oxygenation and ventilatorygoals include consideration for physio-logic mild respiratory alkalosis in preg-nancy, diminished functional residualvolume, higher PEEP requirement, andpotential for less lung compliance withhigher innate plateau pressures owingto diaphragmatic compression by thegravid uterus and chest wall compres-sion by enlarged breast tissue. Physio-logic tidal volumes in pregnancy aregreater than the target value of 6 mL/kgideal body weight used in the ARDSNetwork study.15 This, coupled withdecreased chest wall/diaphragmaticcompliance, presents a challenge to the
“lung protective” strategy for mechan-ical ventilation in pregnant patients.Our clinical observation suggests a5-cm H2O difference in plateau pres-sures before and immediately afterevacuation of the gravid uterus.Therefore, it seems reasonable to in-crease tidal volume and/or PEEP tomeet goal PCO2 and oxygenation tar-gets, while being mindful not to allowalveolar plateau pressures to exceed35-cm H2O (Table 2).
The prone position can help over-come some of these issues. Prone venti-lation has been found to significantlyimprove oxygenation in the setting ofARDS, and its feasibility and safety inpregnancy have been documented.16,17

FIGURE 4(Continued )
Research Letter
AUGUST 2020 AJOG MFM 7

TABLE 1Delivery considerations for pregnant patients with COVID-19
Gestational age Illness severity Delivery considerations
GA<24 wk Noncritically ill � If previable PTL—can deliver in the COVID unit or LDR
GA<24 wk Critically ill � Avoid delivery in an “unstable” mother� If previable PTL—deliver in the ICU, or main OR if D&C required
GA 24e34 wk Severe but noncritically ill � Attempt to delay delivery and stabilize/treat mother� Betamethasone if imminent delivery within a week� MgSO4 for fetal neuroprotection if GA<32 wk (if benefits outweigh risk of pul-
monary edema)� Consider delivery for NRFHTs (category 3 or persistent category 2 fetal tracing) if
stable mother� Imminent need for SVD—move to LDR� Imminent need for cesarean delivery—move to L&D OR
GA 24e34 wk Critically ill � Avoid delivery in “unstable” mother� Attempt to delay delivery and stabilize/treat mother� Case-by-case determination of delivery for maternal or fetal benefit if stable
mother� Betamethasone “only” if “high” risk for imminent delivery within a week� MgSO4 for fetal neuroprotection if GA<32 wk (if benefits outweigh risk of pul-
monary edema)� Imminent need for SVD—deliver in ICU� Imminent need for cesarean delivery—move to main OR� Perimortem cesarean delivery—proceed in ICU
GA�34 wk Severe but noncritically ill � Attempt to delay delivery and stabilize/treat mother� Case-by-case determination of delivery for maternal or fetal benefit if stable
mother� Consider delivery for NRFHTs if stable mother� Avoid late preterm betamethasone� Imminent need for SVD—move to LDR� Imminent need for cesarean delivery—move to L&D OR
GA�34 wk Critically ill � Avoid delivery in “unstable” mother� Case-by-case determination of delivery for maternal or fetal benefit if stable
mother� Avoid late preterm betamethasone� Imminent need for SVD—deliver in the ICU� Imminent need for cesarean delivery—move to the main OR� Perimortem cesarean delivery—proceed in ICU
COVID-19, coronavirus disease 2019; D&C, dilation and curettage; GA, gestational age; ICU, intensive care unit; L&D, Labor and Delivery; MgSO4, magnesium sulfate; NRFHT, nonreassuring fetalheart tracing; OR, operating room; PTL, preterm labor; SVD, spontaneous vaginal delivery.
Schnettler et al. Severe acute respiratory distress syndrome in COVID-19einfected pregnancy. AJOG MFM 2020.
=
Research Letter
Finally, veno-venous ECMO is a provenlife-saving salvage therapy for severe,reversible respiratory failure, and itsbenefit among critically ill pregnantwomen has been reported.18 Consider-ation for ECMO cannulation should beentertained among a multidisciplinary
ABG, arterial blood gas; BID, twice daily; CBC, complete blood cell councoronavirus disease 2019; CRP, C-reactive protein; CT, computed tomodepartment; ICU, intensive care unit; LDR, labor, delivery, and recovery roorate tracing; NST, nonstress test; ODH, Ohio Department of Health; OR, opQA, Quality Assurance committee; SMFM, Society for Maternal-Fetal Me
Schnettler et al. Severe acute respiratory distress syndrome in C
8 AJOG MFM AUGUST 2020
team of experienced providers in situ-ations where the patient’s oxygenationis so severely compromised as torequire maximal ventilatory supportearly in the disease process (less than 7days of mechanical ventilatory sup-port). Therapeutic anticoagulation is
t; CDC, Centers for Disease Control and Prevention; CEFM, continuous elegraphy; D&C, dilation and curettage; EFM, electronic fetal monitoring; FHm; LR, lactated Ringer’s solution;MAP, mean arterial pressure;MgSO4,maerating room; PCR, polymerase chain reaction; PEEP, positive end-expiratdicine; SOB, shortness of breath; SVD, spontaneous vaginal delivery, US,
OVID-19einfected pregnancy. AJOG MFM 2020.
often required, and the postpartumperiod appears to be a potentiallytenuous time point for initiation ofECMO with 100% maternal mortalityin a recent case series.18
In summary, this case of rapid clinicaldecompensation and development of
ctronic fetal monitoring; CMP, complete metabolic panel; COVID-19,T, fetal heart tones; GA, gestational age; HA, headache; HD, healthgnesium sulfate;NC, nasal cannula;NRFHT, nonreassuring fetal heartory pressure; PPE, personal protective equipment; PTL, preterm labor;ultrasound.

TABLE 2Critical care goals and considerations in pregnant patients with COVID-19
Measure Target Considerations
MAP >65 mm Hg � First assess if fluid responsive with passive leg raise or bolus LR 500 mL to see if MAP increasesto >65 mm Hg
� Start norepinephrine at 5 mg/min (uptitrate to 10 mg/min) for MAP<65 mm Hg� Ensure CEFM if GA>24 wk
SpO2 >94% � Increase PEEP to 10e24 cm H2O� Consider VCþ modality� Consider prone positioning� Ensure finger is warm or place monitor on forehead
PaO2 >80 mm Hg � Increase PEEP to 10e24 cm H2O� Increase I:E ratio� Consider prone positioning
PCo2 <40 mm Hg � Increase ventilatory/respiratory rate to 20e25 bpm� Consider higher tidal volume than 6 mL/kg ideal body weight� Ensure no “auto-PEEP”—keep plateau pressure of <35 cm H2O
pH 7.3e7.5 � First assess if acidemic or alkalemic� Then assess which is more out of range (PO2 or PCO2)� If metabolic acidosis, assess anion gap and ensure appropriate ventilatory compensation
(bicarb � 1.5)þ8¼PCO2
Bicarb 16e22 mm Hg � Consider addition of IV bicarb if low and pH is <7.1
Anion gap 6e15 � Correct for hypoalbuminemia (add 2.5 to gap for every 1 g/dL albumin below level of 2.5 g/dL)
PiP <35 mm Hg � Check PiP on vent and ensure <40 cm H2O� Consider VCþ modality
UOP >20 mL/kg/h � Place Foley and ensure strict Is/Os plus daily weights
Skin No breakdown � Evaluate skin front and back daily (especially under fetal monitors)
VTE Prophylaxis � Consider institution of heparin 7500 U twice a day in second trimester and 10,000 U twice a day inthird trimester if delivery is not imminent
Peptic ulcer Prophylaxis � Consider H2 blockade
CEFM Category 1e2 � Delivery for category 3 if GA>28 wk� Worsening category 2 may signal worsening maternal status
Sedation Lowest achievable � Goal is to achieve RASS of 0 (alert and calm) while on mechanical ventilation� May need to increase sedation with propofol, fentanyl, and midazolam� May need paralytic (cisatracurium) especially when proning
CEFM, continuous electronic fetal monitoring; I:E ratio, inspiratory:expiratory ratio; GA, gestational age; LR, lactated Ringer’s solution; MAP, mean arterial pressure; PEEP, positive end-expiratorypressure; PiP, peak inspiratory pressure; RASS, Richmond Agitation and Sedation Scale; UOP, urine output; VC, volume control; VTE, venous thromboembolism.
Schnettler et al. Severe acute respiratory distress syndrome in COVID-19einfected pregnancy. AJOG MFM 2020.
Research Letter
severe (PaO2:FiO2<150) COVID-19erelated ARDS in a woman at 31 weeks’gestation highlights many physiologicand management considerations for thecare of critically ill pregnant womenwithCOVID-19. Few contemporary re-sources exist to guide the multidisci-plinary team through decisionsregarding optimal maternal-fetal sur-veillance, intensive care procedures, anddelivery timing. This detailed case re-views the thought process, team-basedstrategy, and algorithmic approach tothis emerging disease’s diagnosis andmanagement. n
References
1.World Health Organization. Coronavirusdisease 2019 (COVID-19) Situation Report e74. Available at: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200403-sitrep-74-covid-19-mp.pdf?sfvrsn¼4e043d03_14. Accessed April 3, 2020.
2. Salata C, Calistri A, Parolin C, Palù G. Coro-naviruses: a paradigmof new emerging zoonoticdiseases. Pathog Dis 2019;77:ftaa006.
3. Centers for Disease Control and Prevention.Cases of Coronavirus Disease (COVID-19) inthe U.S. Available at: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html. Accessed April 3, 2020.
4. Dashraath P, Jing Lin Jeslyn W, Mei XianKaren L, et al. Coronavirus disease 2019
(COVID-19) pandemic and pregnancy. Am JObstet Gynecol [In press].5. Schwartz DA. An analysis of 38 pregnantwomen with COVID-19, their newborn infants,and maternal-fetal transmission of SARS-CoV-2: maternal coronavirus infections and preg-nancy outcomes. Arch Pathol Lab Med 2020[Epub ahead of print].6. Di Mascio D, Khalil A, Saccone G, et al.Outcome of coronavirus spectrum infections(SARS,MERS,COVID1-19) during pregnancy: asystematic review and meta-analysis. Am JObstet Gynecol MFM 2020 [Epub ahead ofprint].7. Breslin N, Baptiste C, Gyamfi-Bannerman C,et al. COVID-19 infection among asymptomaticand symptomatic pregnant women: two weeksof confirmed presentations to an affiliated pair of
AUGUST 2020 AJOG MFM 9

Research Letter
New York City hospitals. Am J Obstet GynecolMFM 2020 [Epub ahead of print].8. Wu Z, McGoogan JM. Characteristicsof and important lessons from the corona-virus disease 2019 (COVID-19) outbreakin China: summary of a report of 72 314cases from the Chinese Center for DiseaseControl and Prevention. JAMA 2020;323:1239–42.9. Guérin C, Reignier J, Richard JC, et al.Prone positioning in severe acute respiratorydistress syndrome. N Engl J Med 2013;368:2159–68.10. Juusela A, Nazir M, Gimovsky M. Two casesof COVID-19 related cardiomyopathy in preg-nancy. Am J Obstet Gynecol MFM 2020 [Epubahead of print].11. Yi Y, Lagniton PNP, Ye S, Li E, Xu RH.COVID-19: what has been learned and to belearned about the novel coronavirus disease. IntJ Biol Sci 2020;16:1753–66.12.Wang M, Cao R, Zhang L, et al. Remdesivirand chloroquine effectively inhibit the recently
10 AJOG MFM AUGUST 2020
emerged novel coronavirus (2019-nCoV) in vitro.Cell Res 2020;30:269–71.13. Li H, Wang YM, Xu JY, Cao B. Potentialantiviral therapeutics for 2019 novel coronavirus.Zhonghua Jie He Hu Xi Za Zhi 2020;43:170–2.14. Arabi YM, Fowler R, Hayden FG. Critical caremanagement of adults with community-ac-quired severe respiratory viral infection. IntensiveCare Med 2020;46:315–28.15. Eisner MD, Thompson T, Hudson LD, et al.Efficacy of low tidal volume ventilation in patientswith different clinical risk factors for acute lunginjury and the acute respiratory distress syn-drome. Am J Respir Crit Care Med 2001;164:231–6.16. Dennis AT, Hardy L, Leeton L. The proneposition in healthy pregnant women and inwomen with preeclampsia—a pilot study. BMCPregnancy Childbirth 2018;18:445.17. AkatsukaM, Tatsumi H, YamaN, Masuda Y.Therapeutic evaluation of computed tomogra-phy findings for efficacy of prone ventilation inacute respiratory distress syndrome patients
with abdominal surgery. J Crit Care Med (TarguMures) 2020;6:32–40.18.Webster CM, Smith KA, Manuck TA. Extra-corporeal membrane oxygenation in pregnantand postpartum women: a ten-year case series.Am JObstet Gynecol MFM2020 [Epub ahead ofprint].
Author and article informationFrom the Divisions of Maternal-Fetal Medicine (Drs
Schnettler and Suhag) and Pulmonology and Critical Care
Medicine (Dr Al Ahwel), TriHealth-Good Samaritan Hos-
pital, Cincinnati, OH.
Received April 7, 2020; revised April 9, 2020;
accepted April 10, 2020.
This paper is part of a supplement that represents a
collection of COVID-related articles selected for publica-
tion by the editors of AJOG MFM without additional
financial support.
The authors report no conflict of interest.
Corresponding author: William T. Schnettler, MD.