Seminar on Physiology of Puerperium
15
SEMINAR ON PHYSIOLOGY OF PUERPERIUM, LACTATION AND LACTATION MANGEMENT SUBMITTED TO:- Mrs. SOMIBALA SUBMITTED BY:- VARSHA SHARMA MSC NURSING FIRST YEAR RUFAIDA COLLAGE OF NURSING
-
Upload
varshasharma05 -
Category
Documents
-
view
226 -
download
0
Transcript of Seminar on Physiology of Puerperium

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 1/15
SEMINAR ON PHYSIOLOGY OF
PUERPERIUM, LACTATION
AND LACTATION MANGEMENT
SUBMITTED TO:-
Mrs. SOMIBALA
SUBMITTED BY:-
VARSHA SHARMA
MSC NURSING FIRST YEAR
RUFAIDA COLLAGE OF NURSING

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 2/15
PUERPERIUM
Puerperium, the period of adjustment after childbirth during which the mother’s reproductive
system returns to its normal prepregnant state. It generally lasts six to eight weeks and ends with
the first ovulation and the return of normal menstruation.
Puerperal changes begin almost immediately after delivery, triggered by a sharp drop in the levels of
estragon and progesterone produced by the placenta during pregnancy. The uterus shrinks back to
its normal size and resumes its pre-birth position by the sixth week. During this process, called
involution, the excess muscle mass of the pregnant uterus is reduced, and the lining of the uterus
(endometrium) is re-established, usually by the third week. While the uterus returns to its normal
condition, the breasts begin lactation.
INVOLUTION: Is the process whereby the genital organs revert back approximately to the state
where before pregnancy. The women is termed as puerperal.
Puerperium begins as soon as the placenta is expelled and lasts for approximately 6 weeks when the
uteri become regressed almost to the non-pregnant size. The period is arbitrarily divided into-
1. Immediate-within 24 hours.
2. Early-up to 7 days.
3. Remote-upto 6 weeks.
Similarly change occurs following abortion but takes a shorter period for the involution to complete.
INVOLUTION OF THE UTERUS:-
UTERUS: Immediately following delivery the uterus becomes firm and retracts with alternate
hardening and softening. The uterus measures about 20*12*7.5cms.and weight about 1000gm.at
the end of 6 weeks, its measurement is almost similar to that of the non pregnant state and weight
about 60gm.the placenta site contracts rapidly presenting a raised surface with measures about
1.5cm.lower uterine segment immediately following delivery, the lower segment becomes a thin,
flabby, collapsed structure. It takes a weeks to revert back to the normal shape and size of the
isthmuseither part between the bodies of the uterus or internal us of the cervix.
CERRVIX:-The cervix contracts slowely,the external os admits two fingers for a few days but by the
end of first week, narrows down to admit the tip of a finger only. The contour of the cervix takes a
longer time to regain (6weeks) and the external OS never reverts back to the nulliparus state.
PHYSIOLOGICAL CONSIDERATION:-
The physiological process of involution is most marked in the body of the uterus.
Changes occur in following component -
a) Muscles
b) Blood vessel
c) Endometrium.

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 3/15
Muscles -
There is marked hypertrophy and hyperplasia of muscle fibres during pregnancy
and the individual muscle fibre enlarges to the extent of 10 times in length and
5 times in breadth. During puerperium, the number of muscle fibres is not decreased but there is
substantial reduction of the myometrial call size. Withdraw of steroid hormones, oestrogen and
progesterone, may lead to increase in the activity of the uterine collagens and the release of
proteolytic enzyme. Autolysis of the protoplasm occur by the proteolytic enzyme with liberation of
peptones which entre the blood stream. These are excreted through the kidneys as urea and
creatinine .This explain the increase excretion of the products in the puerperal urine. The connective
tissue undergoes the same type of degeneration. The condition which favours involution are -
1.efficiancy of the enzymatic action and 2.Relative anoxia induced by effective contraction and
retraction of the uterus.
Blood vessels -
The changes of the blood vessels are pronounced at the placental site. The arteries
are constricted by contraction of its way and thickening of the intima followed bythrombosis. New blood vessels grow inside the thrombi.
Endometrium -
Following delivery, the major part of the decidua is cast off with the expulsion of
the placenta and the membranes, more at the placental site. The endometrium left
behind varies in thickness from 2-5 mm. The superficial part containing the
degenerated decidua, blood cells and bits of fatal membranes becomes necrotic
and is cast off in lochia. Regeneration occurs from the epithelium of the uterine
gland mouths and interglandular stromal cells. Regeneration of the epithelium is
completed by 10th day and the entire endometrium is restored by the day 16,
except the placental site it takes about 6 weeks.
Clinical assessment of involution -
The rate of involution of the uterus can be assessed clinically by noting the height
of the fundus of the uterus in relation to the symphysis pubis. The measurement
should be taken carefully at fixed time every day, preferably by the same observer.
Bladder must be emptied beforehand and preferably the bowel too, as the full
bladder and the loaded bowel may raise the level of the fundus of the uterus.
The uterus is to be centralised and with a measuring tape, the fundal height is
measured above the symphysis pubis. Following delivery, the fundus lies about
13.5 cm above the symphysis pubis. During the first 24 hour, the level remains
constant, thereafter there is a steady decrease in height by 1.25 cm in 24 hours,
so that by the end of second week the uterus becomes a pelvic organ.
ABSTRACT:- VanRees, D., Bernstine, R. L. and Crawford, W. (1981), Involution of the postpartum
uterus: An ultrasonic study. J. Clin. Ultrasound, 9: 55 –57.
The involution of the uterus was studied between 1 and 40 days postpartum utilizing serial
ultrasonic scans. All pregnancies and postpartum periods were uncomplicated. The decrease in
uterine size was related to a diminution in uterine length. No difference was observed between
nullipara and primipara or breast- or bottle-feeding mothers.

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 4/15
INVOLUTION OF OTHER PELVIC STRUCTURES:
VAGINA:-
Involution of the Vagina
The vagina involutes more slowly than the uterus. Immediately after the delivery, it is swollen,toneless and appears bruised and red. The normal rugosity (wrinkles) of the vaginal walls reappear
at about the 3rd week of the postpartum period. But the size and elasticity of the tissues never
regain the pre-pregnancy state. Broad ligaments and round ligaments require considerable time to
recover from the stretching and laxation.
Pelvic floor and pelvic fascia take a long time to involute from the stretching effect during
parturition.
LOCHIA:-
Lochia is the vaginal discharge after giving birth (puerperium) containing blood, mucus, and uterine
tissue. Lochia discharge typically continues for 4 to 6 weeks after childbirth. It originates from the
uterine body, cervix and vagina. It is sterile for the first 2 –3 days, but not so by the third or fourth
day.
ODOUR AND REACTION:-It has got a peculiar offensive fishy smell. Its reaction is alkaline tending to
become acid towards the end. It progresses through three stages:-
1. Lochia rubra (RED) is the first discharge, red in colour because of the large amount of blood
it contains. It typically lasts no longer than 3 to 5 days after birth.
2. Lochia serosa is the term for lochia that has thinned and turned brownish or pink in colour. It
contains serous exudate, erythrocytes, leukocytes, and cervicalmucus. This stage continues
until around the tenth day after delivery. Lochia serosa which persists to some weeks after
birth can indicate late postpartum haemorrhaging, and should be reported to a physician.
3.
Lochia Alba (or purulent) is the name for lochia once it has turned whitish or yellowish-
white. It typically lasts from the second through the third to sixth weeks after delivery. It
contains fewer red blood cells and is mainly made up of leukocytes, epithelial cells,
cholesterol, fat, and mucus.
AMOUNT- The average amount of discharge for the 5-6 days, it’s estimated to be 250 ml.
NORMAL DURATION: Normal duration may extend up to 3 weeks. The red lochia may persists
for longer duration especially in women who get up from the bed for the first time in later
period. The discharge may be scanty, especially following premature labour or may be excessive
in twin delivery or hydramnios.
CLINICAL IMPORTANCE:-
The character of the lochia discharge gives useful information about the abnormal puerperal state.
The valve pads are to be inspected daily to get information.
ODOUR: If malodorous indicates infection .retained plug or cotton piece inside the vagina should
be kept in mind.

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 5/15
COLUR:Persistence of red colour beyond the normal limit signifies sub involution or retained bits
of bits of concepts.
DURATION: Duration of the lochia alba beyond 3 weeks suggest local genital lesions.
GENERAL PHYSIOLOGICAL CHANGES:-
PULSE:-for a few hours after the normal delivery, the pulse rate is likely to be raised which settle
down to normal during the second day .however, the pulse rate often rises with after-pain
excitement.
TEMPERATURE: -The temperature should not be above 37.2degree C (99degree F)with in the first
24 hrs. There may be slight reactionary rise following delivery by 0.5degree but comes to the normal
within 12 hrs .On the 3rd day there is slight increase in the temperature due to the breast
engorgement which should not last for more than 24 hrs .however, genitor –urinary tract infection
should be excluded if there is raise of temperature.
URINARY TRACT: -It may be slightly uncomfortable to urinate for a few days after your baby’s
birth. Pain or burning when you urinate, or the urge to urinate frequently, may indicate a bladder
infection. Bladder capacity increases the bladder may be distanced without urge to pass urine.
Common urinary problems are: overdistention, incomplete emptying and prence of residual urine
.dilated ureters and renal pelvis return to normal size within 8 weeks. There is pronounces diuresis
on the second or third day of perpurium.
GESTRO-INTESTINAL TRACT:-Increases thirst in early perpurium is due to loss of fluid in during
labour, in the lochia diurasis and perspiration constipation is a common problem .
WEIGHT LOSS :- In addition to the weight loss (5-6kg) as a consequence of the expulsion of the fetes,
placentae, liquor and blood loss. A further loss of about 2kg occur during purperium chiefly caused
by diurasis.The weight loss may continue up to 6 months of delivery.
FLUID LOSS:-There is a net fluid loss of at least 2 litters during the first week and an addition 1.5litres
during next 5 weeks .The amount of loss depends on the amount retained during pregnancy,
dehydration during labour and blood loss during delivery the loss of salt and water are larger in
women with pre elampsia and eclampsia.
BLOOD VALUES:- Decrees in blood volume due to blood loss and dehydration. Blood volume returns
to the non-pregnant level by the second week. Cardiac output increases soon after delivery to about
80%above the prelabour values but slowly return to normal within one week.
RBC volume and haematocrit values return to normal by 8bweeks.Postpartum after the hydraemia
disapper.Lecocytes to the extent of 25,000per cu mm occur following delivery probably in response
to stress of labour. Platelet count decreases soon after the separation of placenta but secondary
elevation occurs with increase in platelet count adhesiveness between 4-10 days. Fibrinogen level
high up to the second week of puerperium. A hypercoagulatin state persists up to 48hrs postpartum
and fibrinolytic activity is enhanced in first 4 day. The secondary increase in fibrinogen, factor viii and
the platelet in first week increase the risk for thrombosis the increase in fibrinolytic activity after
delivery acts as a protective mechanism.

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 6/15
MENSTRUATION AND OVULATION:-Onset of first menstruation period following delivery is very
variable and depends on lactation. If women does not breast feed her baby, the mensuration returns
by 6th week following delivery in about 40%and 12th week in 80%of cases.
In non-lactatingmothers, ovulation may occur as early as 4 weeks. And in lactating mothers about
10weeks after delivery.In lactating mother women who is exclusively breastfeeding thecontraceptive protection is about 98%upto 6 months postpartum. Lactation provide natural method
of contraception.so consell the patent to use contraceptive method from 3rd week for non lactating
mother or from 3 month for lactating mother.
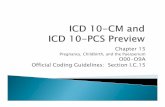
SCHEME OF MACHANISM OF AMENORRHOEA AND ANOVULATION IN
LACTATING MOTHERS:-
BRESTFEEDING – SUCKING* * FREQUENCY
*INTENSITY
*DURATION
INCRESES PROLACTIN LEVEL
INHIBITS OVARIAN RESPONSE GNRH SECRETION.
TO FSH SUPPRESSES THE RELEASE OF LH
NO LH SURGE
LESS FOLLICULAR GROWTH
HYPO-OESTROGENIC STATE ANOVULATION
NO MENSURATION

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 7/15
LACTATION
The secretion from the breast called colostrums which starts during pregnancy becomes more
abundant during the period.
Composition of colostrums: Deep yellow serous fluid, alkaline in reaction. It has got a higher specificgravity, high protein, vit A, sodium and chloride content but has got lower carbohydrate, fat and
potassium than the breast milk. It contains antibody (IgA).
ADVANTAGES: - 1. Provide immunity to the Baby.
2. Laxative action on the baby due to the large fat globules.
PHYSIOLOGY OF LACTATION:
DIVIDED INTO FOUR PHASES:-
PREPRTATION OF THE BREASTS(MAMMOGENESIS)
SYNTHESIS AND SECRETION FROM THE BREAST ALVEOLI (LACTOGENISIS).
EJECTION OF THE MILK (GALAKTOKINESIS).
MAINTENANCE OF LACTATION (GALATOPOIESIS).

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 8/15
MAMMOGENIS: - pregnancy is associate with a remarkable growth of both the ductal and lobular
alveolar system .intact nerve supply is not essential for the growth of the mammary glands during
pregnancy.
LACTOGENISIS: - milk secretion starts actually on day 3rd or 4th postpartum day. This time breast
become engorged. Tense and feel warm in spite of high prolactin level in pregnancy milk secretion is
abeyance. Steroids-estragon and progesterone is circulating so it makes unresponsive to the
prolactin when after pregnancy estragon and progesterone level decreases and prolactincomes intothe action and secretion of milk occurs.
GALACTOKINASIS: - Discharge of the milk from the mammary gland not only depends on the sucking
of the baby but also on the contractile mechanism of which expresses the milk from the alveoli into
the ducts. Oxytocin is a major gelectokinetic hormone.
Discharge of milk from the mammary glands of breast depends upon the suction exerted by the baby
during suckling. Contractile mechanism also helps by expressing the milk from alveoli into the ducts.

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 9/15
During suckling,a conditioned nervous reflex is set up. The impulses start from the nipples to
Supraoptic nucleus in brain and thence along the hypothalamus-pituitary axis to posterior pituitary.
It appears to be so complicated and essentially when the love of baby is there, all this is simply a
loving privilege of Moms!
Oxytocin is secreted from posterior pituitary which exerts several effects on the uterus and breast. Inbreasts, there iscontraction of the epithelial cells of alveoli and ducts containing the milk .
This is the "milk ejection" or "milk let down"reflex that forces the milk down into the
lactiferous ducts. From lactiferous ducts milk is expressed either by the mother by hand or sucked
out by the baby.
A sensation of rise in pressure in the breast is felt by the mother at the beginning of suckling. It is
called"draught". This effect can be produced artificially by the injection of Oxytocin hormone.
The milk ejection reflex is inhibited by several factors like pain in breasts or body,
breast engorgement, psychological upsets. In addition this ejection reflex might be weak for
several days following breast feeding and it results in breast engorgement.
GALACTOPOISE:
The hormoneProlactinappears to be the single most important factor for maintenance of
lactation.Sucking is also essential for maintenance of lactation. Sucking is essential for the
removal of milk from the glands in breast but also for the release of Prolactin.
Secretion of milk is a continuous processunless suppressed by congestion or emotional
disturbances. Milk pressure reduces the rate of breast milk production. So periodic breast feeding
is necessary to relieve the pressure that in turn maintains the secretion of milk inside the breast.
MILK PRODUCTION:-Healthy mother produce about 500-800ml milk a day to feed her baby.
Inadequate milk production (lactationfailure) it may be due to the infrequent sucking or due to
endogenous suppression of prolactin .pain anxiety .unrestricted feeding at short interval (2-3hrs)
Drugs to improve milk production: - metocloperamide10 mg thrice a day increase milk volume by
increasing prolactin level.
Management of normal puerperium
Immediately following delivery, the patient should be closely observed. She may be given
a drink of her choice or something to eat, if she is hungry.
Principles -
- To give all out attention in to restore the health status of the mother.
- To prevent infection.
- To take care of the breasts, including promotion of lactation and nursing of the child.
- To motivate the mother for contraception.

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 10/15
General management -
Rest and ambulance - It is indeed difficult to categories an uniform period of rest. After a good resting period,
the patient becomes fresh and can breast feed the baby or moves out of bed to go to the
toilet. Early ambulation is encouraged. Advantages of early ambulation are:- Provide a sense of well-being.
- Bladder complications and constipation are reduced.
- Facilitates uterine drainage.
- Hastens involution of uterus.
- Lessens puerperal venous thrombosis and embolism.
Hospital stay -
Early discharge from the hospital is an almost universal procedure. If adequate supervision
by trained health visitors is provided, there is no harm in early discharge.
Diet - The patient should be on normal diet of her choice. If the patient is lactating, high calories,
adequate protein, fat, plenty of fluids, minerals and vitamins are to be given.
Care of the bladder -
The patient is encouraged to pass urine following delivery as soon as convenient. If the patient
fails to pass urine, catheterisation should be done. Catheterisation is also indicated in case of
incomplete emptying of bladder.
ABSTRACT:-2
Saadia, Z., Roshdy, S., Sagir, F. and Abidin, S. (2013), Dietary practices of Saudi womenduring puerperium. Journal of Obstetrics and Gynaecology Research, 39: 799 –805.
Poor maternal health sometimes can be a consequence of practicing different myths during puerperium. This cross-sectional study describes the practice of different myths regarding diet among
Saudi women.Using method of comprised women attending the postnatal clinic at the Mother andChild Hospital in Buraidah from January to December 2011.hence shows that Almost 65.9% ofwomen were using a combination of herbs such as ginger (zingiber officinale), hilba (fenugreek) and black seeds (nigella sativa). The multinomial logistic regression of herbs on age, education,occupation, parity and mode of delivery was statistically significant (χ 2 [48] = 214.645, P < 0.001).
Hilba was more commonly used by women with instrumental delivery. It was common for women to
avoid different fruits and vegetables (33.89%). Eggs were avoided by 16.5% of women and 11%avoided cold drinks. The multinomial logistic regression of diet on age, education, occupation, parityand mode of delivery was statistically significant (χ
2 [72] = 389.861, P < 0.001). Individuals below
college level education were more likely to avoid fruits, vegetables and cold drinks in their diet. It
proves that Health education programs are needed to improve knowledge about dietary malpracticesduring puerperium. This may help eliminate myths regarding avoidance of certain dietary
components.
Care of the bowel -
The problem of constipation is much less because of early ambulation and liberalisation of the
dietary intake. A diet containing sufficient roughage and fluids is enough to move the bowel.
If necessary, mild laxative such as Igol (isogon husk) two teaspoons may be given at bed time.

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 11/15
ABSTRACT:-3
John M. Thorp,Peggy A. Norton,Urinary incontinence in pregnancy and the puerperium: A
prospective study American Journal of Obstetrics & Gynecology,Volume 181, Issue 2, Pages 266 –
273, August 1999
Objective: Pregnancy and childbirth are commonly thought to be associated with the development
of urinary incontinence and lower urinary tract symptoms. The purpose of this study was to assess
the relationship, if any, between pregnancy and the development of lower urinary tract symptoms.
Study Design: A prospective study of lower urinary tract symptoms was carried out in a cohort of
pregnant women who answered a series of symptom questionnaires and kept a 24-hour bladder
chart on which frequency of urination and volumes voided were recorded throughout pregnancy
and for 8 weeks after birth. Results: A total of 123 women participated in the study. Mean daily
urine output (P = .01) and the mean number of voids per day (P = .01) increased with gestational age
and declined after delivery. Episodes of urinary incontinence peaked in the third trimester and
improved after birth (P = .001). White women had higher mean voided volumes and fewer voiding
episodes than did black women. Ingestion of caffeine was associated with smaller voided volumes
and greater frequency of urination. Conclusion: Pregnancy is associated with an increase in urinary
incontinence. This phenomenon decreases in the puerperium. Pregnancy and childbirth trauma are
important factors in the development of urinary incontinence among women. These findings
warrant further investigation. (Am J Obstet Gynecol 1999;181:266-73.)
Sleep - The patient is in need of rest, both physical and mental. So she should be protected against
worries and undue fatigue. Sleep is ensured providing adequate physical and emotional support.
Care of the vulva and episiotomy -
Shortly after delivery, the vulva and buttocks are washed with soap water down over the anus
and a sterile pad is applied. The patient should look after personal cleanliness of the vulvar
region. The perinea wound should be dressed with spirit and antiseptic power after each act
micturition and defecation or at least twice a day.
Care of the breast -
The nipple should be washed with sterile water before each feeding. It should be cleaned
and kept dry after the feeding is over. Nipple soreness is avoided by frequent short feeding
rather than the prolonged feeding, keeping the nipple clean and dry.
ABSTRACT:4
- Winani S1, Wood S, Coffey P, Chirwa T, Mosha F, Changalucha J Use of a clean delivery kit
and factors associated with cord infection and puerperal sepsis in Mwanza, Tanzania. J
Midwifery Womens Health. 2007 Jan-Feb;52(1):37-43
Our objective was to determine the effectiveness of an intervention that incorporated education
about the "six cleans" with the use of a clean delivery kit in preventing cord infection and puerperalsepsis. A stepped-wedge, cross-sectional study was conducted in 10 surveillance sites across two

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 12/15

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 13/15
infections followed vaginal delivery compared to Cesarean section 121 (97.6%), 3 (2.5%)
respectively. All strains of Staph were sensitive to Vancomycin, Gentamicin and Ceftriaxone.
C. perfringens were sensitive to Ceftriaxone, Penicillins, Vancomycin and Metronidazole,
while E. cloacae were sensitive to Gentamicin and Ceftriaxone. Conclusion: despite the
limited resources in the developing countries, treatment based on cultures remains the onlysolution to reduce maternal morbidity and mortality rates following puerperal infections.
POSTNATAL CARE:-
Take your medicine as directed:
Call your primary healthcare provider if you think your medicine is not working as expected. Tell him
if you are allergic to any medicine. Keep a current list of the medicines, vitamins, and herbs you take.
Include the amounts, and when, how, and why you take them. Take the list or the pill bottles to
follow-up visits. Carry your medicine list with you in case of an emergency. Throw away old medicine
lists.
NSAIDs:
No steroidal anti-inflammatory (NSAID) medicine may decrease swelling and pain or fever. This
medicine can be bought with or without a doctor's order. This medicine can cause stomach bleeding
or kidney problems in certain people. Always read the medicine label and follow the directions on it
before using this medicine.
Follow-up visits:
Ask your caregiver when to return for a follow-up visit. Often, caregivers will want to see you six
weeks after having your baby. Your caregiver may do a vaginal exam at your visit. Tell your caregiver
if you are having any pain or other symptoms. Keep all appointments. Write down any questions you
may have. This way you will remember to ask these questions during your next visit.
Activity:
After having a baby, you may be very tired. It is very important to get enough rest after having a
baby. For a while after delivery, try to keep all activities short. You may be able to do some exercise
soon after having your baby, such as walking. Kegel exercises may help your vaginal and rectal
muscles heal faster. You can do Kegel exercises by tightening and relaxing the muscles around your
vagina. Kegel exercises help make the muscles stronger, and may prevent gas and urine from leakingout. Talk with your caregiver before you start exercising. If you work outside the home, ask your
caregiver when you can return to your job.
Breast care:
When your milk comes in, your breasts may feel full and hard. If you plan to breastfeed, ask
caregivers to show you how to hold and breastfeed your baby. Ask caregivers for more information
about how to care for your breasts even if you are not breastfeeding. Also ask your caregiver about
breastfeeding while taking medicines.

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 14/15
Constipation:
Do not try to push the bowel movement out if it is too hard. High-fibre foods, extra liquids, and
regular exercise can help you prevent constipation. Examples of high-fibre foods are fruit and bran.
Prune juice and water are good liquids to drink. Regular exercise helps your digestive system work.
You may also be told to take over-the-counter fibre and stool softener medicines. Take these items
as directed.
Haemorrhoids:
Haemorrhoids are swollen veins in or around your rectum. Pregnancy can cause haemorrhoids to
stick out or swell. You may have rectal pain because of the haemorrhoids. Ask your caregiver about
preventing and caring for haemorrhoids.
Perinea care:
Your perineum is the area between your vagina and anus. To help heal your perineum, keepthe area as clean and dry as possible. This will also help prevent infection. You can wash the
area gently with soap and water when you bathe or shower. Ask your caregiver about any
special wound care needed if you had an episiotomy. An episiotomy is an incision (cut) in
your perineum.
Your caregiver may suggest using sits baths to help decrease your pain. During a sits bath,
you will sit in a bathtub filled with warm or cold water. A cold sits bath may decrease your
pain right away. To make a cold-water sits bath, sit in slightly warm water and add ice cubes
to the water. Stay in the sits bath for 20-30 minutes, or aslong as your caregiver suggests.
Ask your caregiver for more information about sitz baths and other ways to decrease your
pain.
Vaginal discharge: You will have a vaginal discharge, called lochia, after your delivery. The lochia is bright red the first
day or two after delivery. By the third or fourth day, the amount decreases, and it turns a red
browncolour. About 7 to 14 days after having your baby, you may have a heavier flow of blood.
Sometimes the colour of the lochia changes to a yellow-white colour and may have an odor (smell).
You may need to wear a pad and change it many times each day. You may be able to use tampons if
you can insert them without any problems. Caregivers may advise you not to use tampons at night
time to lessen the risk of infection. It is normal to have lochia up to eight weeks after your baby is
born.
Monthly periods:Your period may start again within 7 to 12 weeks after your baby is born. If you are breastfeeding, it
may take longer for your period to start again. You can still get pregnant again even though you do
not have your monthly period. Talk with your caregiver about a birth control method that will be
good for you if you do not want to get pregnant.
Mood changes:Many new mothers have some kind of mood changes after delivering their baby. Some of these
changes occur because of lack of sleep, hormone changes, and caring for a new baby. Some mood
changes can be more serious, such as severe (very bad) postpartum depression (deep sadness). Talk
with your caregiver if you feel unable to care for yourself or your baby after delivery.

8/10/2019 Seminar on Physiology of Puerperium
http://slidepdf.com/reader/full/seminar-on-physiology-of-puerperium 15/15