SEMINAR Neuro Hand-Outs

of 35
-
Upload
flordeliza-villaren-cortez -
Category
Documents
-
view
219 -
download
0
Transcript of SEMINAR Neuro Hand-Outs
-
7/31/2019 SEMINAR Neuro Hand-Outs
1/35
1
INTRODUCTION
Medical conditions associated with neuromuscular and skeletal impairment, plus
problems in body senses such as the eye, are currently increasing in prevalence in this
generation. These may be associated with a variety of factors to include genetics in origin,
autoimmunity, familial, environmental, and among others.The nervous system plays a major and extensive role in the body since it is the maste
controlling and communicating system of the body. The muscular system is essentially
responsible for body movement, acting as machines of the body, while the skeletal system is
the bodys internal framework.
According to World Health Organization (WHO, 2011), Glaucoma is considered as the
second leading cause of blindness in the world with rough estimate of 4 million Americans
affected, while, on the other hand, 5.5 million suffer in Cataract. There are also approximately
200 million women affected worldwide with osteoporosis; whereas, 62.9% among 50 patients
in the Philippine Orthopedic Center suffered fractures in line with this. For Guillane-Barre
Syndrome (GBS), approximately 1 in 100,000 is affected with this or 2,720 people in United
States (US); while in the Philippines involved 862 people only. It is also believed that there are
currently about 250,000 to 350,000 people in US who have been diagnosed with Multiple
Sclerosis.
This seminar is geared to the enhancement of knowledge to promote quality nursing
education, research, and practice. In nursing education, this is a great tool to be used in
reviewing concepts related to perception and coordination especially because nurses need
continuous knowledge even if they are already outside the four corners of the classroom. In
nursing research, this will serve as a guide and basis to expound the knowledge recently
acquired through further investigation. This may involve the statistics of each diseases, the
prognosis, and even the latest treatment or management to promote quality care. In nursing
practice, since all of these diseases needed critical attention especially because it concerns
the mastermind system of the body which is the brain, effective nursing care is needed. The
usual routine care may be involved with special consideration on the neuro-vital signs, level of
consciousness, and activity level of the clients.
-
7/31/2019 SEMINAR Neuro Hand-Outs
2/35
2
OBJECTIVES
General Objective
At the end of our 5 hour seminar, the participants will acquire and develop knowledge
and skills related to the concept of perception and coordination to promote quality, effective,
and efficient nursing care.
Specific Objectives
Specifically, the participants will be able to:
a. present a brief introduction about concept of perception and coordination with the
associated statistics per disease;
b. formulate a specific, measurable, attainable, realistic, and time-bounded objectives;
c. present an overview of the anatomy and physiology of the optic, skeletal, and
neuromuscular system;
d. describe the different diseases concerning the concept of perception and coordination in
this order: glaucoma, cataract, osteoporosis, Guillain-Barre syndrome, myasthenia
gravis, and multiple sclerosis;
e. discuss the etiology, risk factors, clinical manifestations, diagnostic tools
pathophysiology, medical-surgical management, and nursing management of each
disease; and
f. evaluate the participants learning on the discussion through creative and mind-bogglinggames/drills.
-
7/31/2019 SEMINAR Neuro Hand-Outs
3/35
3
ANATOMY AND PHYSIOLOGY
OPTIC (VISUAL) SYSTEM
External and Accessory Structures
Extrinsic eye muscles. The extrinsic muscles of the eye come from the bones of the orbit
and are movable due to broad tendons in the eyes tough outer surface. There are sixextrinsic eye muscles that function to move the eye in various directions:
1. Superior rectus muscle rotates the eye upward and toward the midline
2. Inferior rectus muscle rotates the eye downward and toward the midline
3. Medial rectus rotates the eye toward the midline
4. Lateral rectus rotates the eye away from the midline
5. Superior oblique rotates the eye downward and away from the midline
6. Inferior oblique rotates the eye upward and away from the midline
Eyelids. The eyelids protect the eyes anteriorly which meet at the medial and the latera
corners of the eye.
Conjunctiva. The conjunctiva is a mucous membrane that begins at the edge of the cornea
and lines the inside surface of the eyelids and sclera, which serves to lubricate the eye. It is
the thin, transparent tissue that covers the outer surface of the eye. This structure is
nourished by tiny blood vessels that are nearly invisible to the naked eye. The conjunctiva
is composed of 3 sections:
Palpebral Conjuctiva covers the posterior surface of the eyelids Bulbar Conjuctiva coats the anterior portion of the eyeball
Fornix the transition portion, forming the junction between the posterior eyelid and the
eyeball
Lacrimal Apparatus. The lacrimal apparatus consists of the lacrimal gland and a number of
ducts that drain the lacrimal secretions into the nasal cavity. Located above the lateral end
of each eye are the lacrimal glabds that continually release a dilute salt solution, known as
tears, onto the anterior surface of the eyeball through several small ducts.
Internal Eye structures
The Eyeball
The eye, commonly called the eyeball, is a hollow sphere and is composed of:
3 tunics or coats
-
7/31/2019 SEMINAR Neuro Hand-Outs
4/35
4
Humors the interior filled with fluids that help maintain the shape of the eye
Lens the main focusing apparatus of the eye. This structure is supported within the eye
cavity dividing it into two chambers.
TUNICS of the EYEBALL
Fibrous Tunic this is the outermost tunic and is also known as the sclera, the thick and
white connective tissue. Vascular tunic this is the middle coat of the eyeball and has three distinguishable regions
namely:
1. Choroid this is located posteriorly and lies between the sclera and the retina. It
contains the blood vessels that provide nourishment to the outer layers of the retina.
2. Ciliary Body the ciliary body is made up of ciliary muscles and ciliary processes. It lies
just behind the iris. They secrete aqueous humour.
3. Sensory Tunic this is the innermost tunic of the eye and is called the retina. This
structure extends anteriorly only to the ciliary body. It converts images into electrica
impulses that are sent along the optic nerve to the brain where the images are
interpreted.
LENS
The crystalline lens is located just behind the iris. Light entering the eye is focused on the
retina by the lens. The lens is divided into two segments namely:
1. Anterior (aqueous) segment located anterior to the lens and contains a clear wayetry fluid
called aqueous humor. The aqueous humor helps to nourish the cornea and the lens. It iscontinually produced by the ciliary body.
2. Posterior (vitreous) segment located posterior to the lens and is filled with a gel-like
substance called the vitreous humor or the vitreous body. The vitreous humor helps
maintain the shape of the eye.
SKELETAL SYSTEM
The Skeletal System provides support for the human body through a framework that allows
muscles to pull on something that is rigid.
The skeletal system is involved in:
1. Structural Support;
2. Protection;
3. Movement;
-
7/31/2019 SEMINAR Neuro Hand-Outs
5/35
5
4. Mineral Storage;
5. Red Blood Cell production; and
6. Fat Storage.
A. APPENDICULAR SKELETON
Bones of the shoulder: The shoulder joint provides a connection between the chest and the
arm. Clavicle: The clavicle, or collar bone, is a long bone that articulates with the sternum in
the chest and the scapula in the shoulder. It provides a rigid support from which the
scapula and arm are suspended and transfers stress, due to physical impact to the axia
skeleton.
Scapula: The scapula, or shoulder blade, is a triangular shaped flat bone that connects
the humerus with the clavicle. It has a large oblong process, called the acromium.
Humerus: The humerus bone makes up the upper arm between the elbow and the
shoulder. It has a large process called the head, which articulates with the scapula in
the gleonhumeral joint. At the opposite end, is a medial and lateral epicondyle, where it
forms the elbow joint with the bones of the forearm.
Bones of the upper extremity
Elbow joint: The bones of the elbow include the humerus, radius and ulna. This joint is
a pivot point for the forearm and plays a major role in hand movement and function.
Humerus: The humerus has a depression called the olecranon fossa. This depression
receives the olecranon of the ulna, while the forearm is extended. The olecranonforms the prominence of the elbow.
Radius: The radius is the lateral bone of the forearm (located on the thumb side). The
radial head articulates with the humerus and the radia notch of the ulna.
Ulna: The ulna is the medial bone of the forearm (located on the little finger side), which
articulates with the humerus in the elbow joint and the carpals in the wrist.
The wrist: or carpal bones, is made up of 8 small bones held together by ligaments
The carpal bones articulate with the radius and ulna and include the: The scaphoid,
lunate, triquetrium, pisiform, hamate, trapezium, trapezoid and the capitate.
The hand is made up of: The hand is made up of the metacarpal bones and phalange
bones. There are 5 metacarpal bones, which make up the palm. There are a total of 14
phalanges, which make up the fingers.
-
7/31/2019 SEMINAR Neuro Hand-Outs
6/35
6
Bones of the pelvis: The pelvis is located at the base of the spine and contains two sockets
for articulation with the lower extremities.
Ilium: The ilium bone articulates with the sacrum at the sacroiliac joint. This joint, along
with its ligaments, connects the lower extremities with the torso.
Ischium: The ischium bone forms the lower and back part of the pelvis. The ischium
bone also makes up part of the acetabulum and contains the obturator foramen. Pubis: The pubis bone is between the ilium and the ishium, and it forms part of the
acetabulum.
Bones of the lower extremity: the leg bones are the largest bones of the body and, along
with the ankle and feet, provide support for standing and walking.
Femur: The femur, or thighbone, is the largest and strongest bone of the human body.
It articulates with the hip at the hip joint and the bones of the lower leg at the knee joint.
Tibia: The tibia is the larger of the two shinbones. It articulates with the fibula and femur
at the knee joint and the tarsal bones of the ankle.
Fibula: The fibula is the smaller shinbone; it is more posterior than the tibia. It forms the
lateral portion of the ankle joint.
The Tarsal bones are a group of bones that make up the ankle, and the foot is made up
of meta-tarsal ones and phalange bones.
B. AXIAL SKELETON
The spine is made up of a curved stack of 33 irregular bones, known as vertebrae. This stack
can be divided into 5 regions which are, from the top, cervical (7 vertebrae), thoracic (12vertebrae), Lumbar (5 vertebrae), sacral (5 fused vertebrae) and coccygeal (4 fused
vertebrae). Two adjacent vertebrae, and all the soft tissue between them make up one
Motion segment. The vertebrae are irregular in shape, with the spinal cord running down the
neural arch or the vertebrae. Between each vertebrae is a intervertebral disc. This is a
fibrocartilaginous disc, that cushions the two bones.
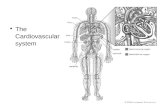
NERVOUS SYSTEM
It is the master controlling and communicating system of the body.
Organization:
A. Structural: Central Nervous System or CNS (brain and spinal cord) and Peripheral
Nervous System or PNS (nerves and ganglia)
-
7/31/2019 SEMINAR Neuro Hand-Outs
7/35
7
B. Functional: Somatic Nervous System or SNS (stimulate skeletal muscle) and Autonomic
Nervous System or ANS (stimulate smooth/cardiac muscle)
Structure:
A. Supportive connective tissue cells
Neuroglia support and protect neurons in the CNS. Specific glial cells are phagocytes.
Schwann cells myelinate neuron processes in the PNS.B. Neurons
1. Axons. These typically generate and conduct impulses away from the cell body an
release a neurotransmitter.
2. Dendrites. These typically carry electrical currents toward the cell body.
I. Central NS
- Location: within the cranial cavity of the skull
- Parts:
A. Cerebral Hemispheres. These two form the largest part of the brain. This involves
logical reasoning, moral conduct, emotional responses, sensory interpretation, and the
initiation of voluntary muscle activity.
B. Diencephalon.
1. Thalamus. This encloses the third ventricle and is the relay station for sensory
impulses passing to the sensory cortex for interpretation.
2. Hypothalamus. This makes up the floor of the third ventricle and is the most
important regulatory center of the autonomic nervous system.3. Epithalamus. This includes the pineal body and the choroid plexus.
C. Brain stem: Midbrain, Pons, and Medulla oblongata
D. Cerebellum. It coordinates muscle activity and body balance.
- Protection of the CNS:
A. Skull and vertebral column are the most external protective structures.
B. Meninges: dura mater, arachnoid mater, and pia mater
C. Cerebrospinal fluid (CSF), provides watery cushion around the brain and cord.
D. Blood-brain barrier.
- Spinal Cord is a reflex center and conduction pathway.
II. Peripheral NS
1. Cranial Nerves: 12 pairs of nerves that extend from the brain to serve the head and
neck region.
-
7/31/2019 SEMINAR Neuro Hand-Outs
8/35
8
2. Spinal Nerves: 31 pairs of nerves are formed by the union of the dorsal and ventra
roots of the spinal cord of each side.
III. Autonomic NS
1. Parasympathetic is the housekeeping system responsible for rest-and-repair
response.2. Sympathetic is the fight-or-flight response.
NEUROMUSCULAR SYSTEM
Nerves:
1. Sensory nerves - send sensory information to the spine
2. Motor nerves - send signals to the muscles
Motor Unit - is the motor nerve and all of the fibers it innervates.
Different muscles have different innervation ratios:
a. 1:10 for occular muscles- smaller motor units
b. 1:10,000 for quadriceps muscles - larger motor units
This is what results in fine versus gross motor movement.
A. Sensory Receptors
Proprioceptors - sensory receptors - sense changes in the environment.
B. Cutaneous receptors - deep pressure and touch
C. Joint and skin receptorsjoint- ruffinni endings
skin touch - (meissner)
pressure ( pacinian)
pain (free nerve endings)
D. Musculotendinous receptors
Golgi tendon organs - sensitive to stretch of the tendon due to muscular contraction and
causes the muscle to relax.
Muscle spindle - responsive to active or passive stretch. as well as the rate (phasic) and
length (tonic) of stretch.
Labyrinthine and neck proprioceptors:
labyrinthine system- orientation of the head
neck proprioceptors- orientation of the neck relative to the head.
Reflexes - preprogrammed motor patterns or nerve muscle patterns
- They do not require voluntary activation
-
7/31/2019 SEMINAR Neuro Hand-Outs
9/35
9
NEUROMUSCULAR JUNCTION
- is the synapse or junction of the axon terminal of a motor neuron with the motor end
plate, the highly-excitable region of muscle fiber plasma membrane responsible for
initiation of action potentials across the muscle's surface, ultimately causing the muscle to
contract. In vertebrates, the signal passes through the neuromuscular junction via
the neurotransmitter acetylcholine (ACh).NMJ Actions:
1. Release of ACh
When a nerve pulse reaches a synaptic end bulb, it triggers release of the
neurotransmitter ACh from synaptic vesicles that contain ACh. ACh then diffuses
across the synaptic cleft between the motor neurone and the motor end plate.
2. Activation of ACh receptors
The motor end plate contains receptors onto which the free ACh binds after diffusing
across the synaptic cleft. This binding of ACh to ACh receptors in the motor end plate
causes ion channels to open & so allow the sodium (Na+) ions to flow across the
membrane into the muscle cell.
3. Generation of muscle action potential
The flow of sodium (Na+) ions across the membrane into the muscle cell generates
a muscle action potential. This action potential then travels along the sarcolemma and
through the T-Tubules.
4. Breakdown of AChThe ACh that is released at Step (1.) is only available to take part in step (2.) for a short
time before it is broken down by an enzyme called acetylcholinesterase (AChE). This
breakdown of ACh occurs within the synaptic cleft.
-
7/31/2019 SEMINAR Neuro Hand-Outs
10/35
10
GLAUCOMA
DEFINITION: It is a disease of the major nerve of vision (optic nerve). It is characterized by a
particular pattern of progressive damage to the optic nerve that generally begins with a subtle
loss of side vision (peripheral vision). If not diagnosed and treated, it can progress to loss of
central vision and blindness.
ETIOLOGY: Elevated pressure in the eye is the main factor leading to glaucomatous damage
to the optic nerve.
RISK FACTORS:
- Age over 45 years
- Family history of glaucoma
- Black racial ancestry
- Diabetes
- History of elevated intraocular pressure
- Nearsightedness (high degree of myopia), which is the inability to see distant objects
clearly
- history of injury to the eye
- Use of cortisone (steroids), either in the eye or systemically (orally or injected)
- Farsightedness (hyperopia), which is seeing distant objects better than close ones(Farsighted people may have narrow drainage angles, which predispose them to acute
[sudden] attacks of angle-closure glaucoma.)
MANIFESTATIONS:
- Open-Angle: Visual field loss; Haziness; Halo among lights
- Close-Angle: severe eye pain, headache, nausea and vomiting, and visual blurring.
DIAGNOSTICS:
- Tonometry; Pachymetry; Gonioscopy; Ophthalmoscopy; Visual Field testing
-
7/31/2019 SEMINAR Neuro Hand-Outs
11/35
11
PATHOPHYSIOLOGY
MANAGEMENT:
Medical:
- timolol (Timoptic), levobunolol (Betagan), carteolol (Ocupress),
and metipranolol (Optipranolol)
- Prostaglandin analogs
- Adrenergic agonists
- Carbonic anhydrase inhibitors
- Parasympathomimetic agents, which are also called miotics
- Osmotic agents
Surgical:
- Laser iridotomy, Laser trabeculoplasty, Laser cyclo-ablation
Nursing Diagnosis:
Disturbed sensory perception: Visual, related to myopia and lens extraction
Anxiety, related to anticipated surgery
Deficient knowledge: lack of information regarding postoperative care
Impaired home maintenance, related to activity restrictions and impaired vision
Predisposing Factors
Age, Sex, Race, Genetics, Familial History
Precipitating Factors
Myopia/Hyperopia, Injury, Cortisone
Mircocirculation causing Ischemia/Hypoxia
Abberant Immunity
Inflammatory Cytokines in Microglia and Astrocytes causing excessive glutamate stimulation
Blockade of neutrophin and other target derived factors
Increased intraocular pressure
Optic nerve damage
GLAUCOMA
-
7/31/2019 SEMINAR Neuro Hand-Outs
12/35
12
Nursing Management:
- Provide a safe environment, placing the call light and personal care items within easy
reach.
- Encourage to express fears about surgery and its potential effect on vision.
- Explain all procedures related to surgery and recovery.- Instruct to avoid shutting the eyelids tightly, sneezing, coughing, laughing, bending over
lifting, or straining to have a bowel movement.
- Teach to wear glasses during the day and an eye shield at night to prevent injury to the
surgical site.
- Explain and demonstrate the procedure for administering eye drops.
- Provide verbal and written instructions about postoperative care, including a schedule of
follow-up examinations, potential complications, and actions to take in response.
- Refer to a discharge planner or social worker to help establish a plan for home
maintenance.
-
7/31/2019 SEMINAR Neuro Hand-Outs
13/35
13
CATARACT
DEFINITION: It is an opacity or cloudiness of the normally transparent crystalline lens. It is
also an eye disease in which the clear lens of the eye becomes cloudy opaque, causing
decrease in vision, progressing to blindness.
ETIOLOGY:
o Senile- associated with aging
o Congenital- may be hereditary
o Traumatic- associated with injury
o Secondary- associated with systemic disease (such as Diabetes)
RISK FACTORS:
- Age. Some people develop cataracts during their middle-aged years (40s and 50s), but
these cataracts tend to be very small. It is after age 60 that cataracts are most likely to
affect vision. Nearly half of people age 75 and older have cataracts.
- Gender. Women face a higher risk than men.
- Family History.
- Race and Ethnicity. African-Americans seem to have nearly twice the risk of developing
cataracts than do Caucasians. This difference may be due to other medical illnesses,
particularly diabetes. African-Americans are much more likely to become blind from
cataracts and glaucoma than Caucasians, mostly due to lack of treatment. Hispanic
Americans are also at increased risk for cataracts. In fact, cataracts are the leading cause
of visual impairment among Hispanics.
- Diabetes and Other Medical Conditions.
Diabetes. People with diabetes type 1 or 2 are at very high risk for cataracts and are much
more likely to develop them at a younger age. They also have a higher risk for nuclear
cataracts than nondiabetics. Cataract development is significantly related to high levels of
-
7/31/2019 SEMINAR Neuro Hand-Outs
14/35
14
blood sugar (hyperglycemia), and cataracts in people with diabetes are sometimes referred to
as so-called sugar cataracts.
Autoimmune Diseases and Conditions Requiring Steroid Use. Medical conditions
requiring high use of corticosteroids (commonly called steroids) pose a particularly high risk.
Many of these medical conditions are autoimmune diseases, including rheumatoid arthritis,
psoriasis, multiple sclerosis, systemic lupus erythematosus, Behcet's disease, and others.
Eye Conditions. People who are nearsighted (myopia) are at increased risk of developing
cataracts. Physical injuries to the eye (such as a hard blow, cut, or puncture) or eye
inflammation can also increase risk. Previous intraocular eye surgery increases cataract risk.
- Obesity.
- Overexposure to Sunlight
Exposure to even low-level UVB radiation from sunlight increases the risk for cataracts
especially nuclear cataracts. The risk may be highest among those who have significant sun
exposure at a young age. People whose jobs expose them to sunlight for prolonged periods
are also at increased risk.
- Smoking and Alcohol Use
- Environmental Factors
Long-term environmental lead exposure may increase the risk of developing cataracts. Gold
and copper accumulation may also cause cataracts. Prolonged exposure to ionizing radiation
(such as x-rays) can increase cataract risk.
MANIFESTATIONS:
Early:
Painless blurred vision
Decreased colour perception
Late:
Opaque or cloudy white pupil
-
7/31/2019 SEMINAR Neuro Hand-Outs
15/35
15
Vision that is better in dim light with pupil dilation
Gradual loss of vision progressing to blindness
Absence of red reflex
DIAGNOSTICS:
- Laboratory test as preoperative screening process to detect coexisting diseases (e.gdiabetes mellitus, hypertension, and cardiac anomalies).
- Ocular imaging studies: ultrasound, MRI, CT scan
- Routing visual acuity testing
- Testing for brightness acuity and contrast sensitivity
- Confrontation visual field testing
- The following tests may be performed to evaluate macular function: Maddox rod test
photostress recovery test, blue-light entoptoscopy, Purkinje entoptic phenomenon, and
visual-evoked response and electroretinography (VER-ERG).
PATHOPHYSIOLOGY:
MANAGEMENT:
Medical-Surgical:
Predisposing Factors:
Age,
Gender,
Family History,
Race & Ethnicity
Precipitating Factors:
Diabetes & Other Medical
Conditions, Obesity,
Overexposure to Sunlight,
Smoking & Alcohol, Environment
Age > 40 y/o Heredity Eye injury Systemic dse.
e. . DM II
Poor hydration
to the eye
Irregular hydration & change in connective
tissue proteinGlycosylation
of proteins
Increase advanced glycation end-products (AGE) and accumulation of sorbitol in the lens
Cloudiness and opacification of the lenses leading to blurry of vision progressing to blindness
Senile
Cataract
Congenital
CataractTraumatic
Cataract
Secondary
Cataract
-
7/31/2019 SEMINAR Neuro Hand-Outs
16/35
16
- Extracapsular Cataract Extraction (ECCE)
The lens is lifted out without removing the lens capsule may be performed with
Phacoemulsion(the lens is broken up by ultrasonic vibration & extracted)
- Intracapsular Cataract Extraction (ICCE)
The lens is removed within its capsule through a small incision
Nursing:
Pre-operative nursing care:
Instruct measures to prevent or decrease IOP
a. Avoid heavy lifting, violent coughing, bending lower than waist, reading (but
watching TV is allowed)
b. Avoid prolonged anger and sexual activity
Administer pre-op eye medications including mydriatics and cycloplegics asprescribed (i.e. Atropine)
Post-operative Nursing Care:
Elevate the head of the bed 30-45 degrees
Turn the client to the back or un-operative side
Pharmacologic: antibiotic- steroids: TobraDex; Acetominophen for minor pains
No aspirin due to its clotting effects
Instruct measures to decrease or prevent the increase of IOP
Wear glasses during the day until the pupils responds to light
Eye-shield at night while sleeping
Shower or bathing is allowed
Care of the dressing
Stool softeners
Instruct to report pain with nausea and vomiting
-
7/31/2019 SEMINAR Neuro Hand-Outs
17/35
17
OSTEOPOROSIS
DEFINITION: It is a disease characterized by low bone mass and loss of bone tissue that may
lead to weak and fragile bones.
ETIOLOGY: Osteoporosis occurs when there is an imbalance between new bone formationand old bone resorption. The body may fail to form enough new bone, or too much old bone
may be reabsorbed, or both. Two essential minerals for normal bone formation are calcium
and phosphate.
RISK FACTORS:
European or American ethnic background
Personal history of fracture as an adult
Poor general health
Smoking tobacco
Low body weight, less than 127 pounds
Estrogen deficiency
Early menopause, before age 45
Surgical removal of the ovaries before age 45
Irregular menstruation
Taking medical therapy that lowers estrogen levels, such as for breast cancer or
endometriosis
Lifelong low calcium intake
Alcoholism
Falling
Inadequate physical activity
MANIFESTATIONS:
Back pain, caused by a fractured or collapsed vertebra
Loss of height over time
A stooped posture
A bone fracture that occurs much more easily than expected
Dowagers hump
-
7/31/2019 SEMINAR Neuro Hand-Outs
18/35
18
Low calcium level
DIAGNOSTICS:
Dual X-ray absorptiometry (DXA) of the lower (lumbar) spine and hip.
-uses fan beam technology allowing for rapid scanning with very low-energy X-
rays.
Ultrasound of the heel.
-Bone density of the heel predicts overall fracture risk.
Quantitative computerized tomography (QCT) of the lower (lumbar) spine.
-This exam uses a standard CT scanner.
PATHOPHYSIOLOGY:
MANAGEMENT:
Medical-Surgical:
1. regular exercise regimen of weight-bearing exercises
Predisposing Factors:
Age, Gender,
Genetics, Race/Ethnicity,
History of Fracture,
Poor general health
Precipitating Factors:Smoking, Low weight, Estrogen
deficiency, early menopause,
oophorectomy, irregular menstruation,
low calcium, alcohol, fall, inactivity
Low dehydrocholesterol
Low UV light
Poor diet intake of Vit. D
Liver FailureRenal Failure
Calcitrol formation
Low
hos hate
Hypocalcemia
Genetics
Hypoparathyrodism
Stimulates Ca2+
receptors
Increase PTH
glucocorticoids
estrogen
DM II
insulin
mechanical
stress
Osteoid breakdown (skeletal pain, vertebral prolapse, fractures)
OSTEOPOROSIS
-
7/31/2019 SEMINAR Neuro Hand-Outs
19/35
19
2. Vitamin D. A daily intake of 400 IU
3. daily calcium intake of 1,000 mg per day
4. Kyphoplasty
5. Medications
a. Alendronate (Fosamax)
b.Risedronate (Actonel, Atelvia)
c. Ibandronate (Boniva)
d. Zoledronic acid (Reclast, Zometa)
e. Bisphosphonates
f. Calcitionin
g. Parathyroid Hormone (PTH)
Nursing Diagnosis:
Chronic pain
Disturbed body image
Dressing or grooming self-care deficit
Imbalanced nutrition: Less than body requirements
Impaired physical mobility
Risk for impaired skin integrity
Risk for injury
Nursing Management:
- Focus on careful positioning, ambulation, and prescribed exercises.
- Administer analgesics and heat to relieve pain as ordered.
- Include the patient and his family in all phases of care.
- Encourage the patient to perform as much self-care as her immobility and pain allow.
- Provide the patient activities that involve mild exercise.
- Check the patients skin daily for redness, warmth, and new pain sites.
- Monitor the patients pain level, and assess her response to analgesics, heat therapy, anddiversional activities.
- Explain all treatments, tests, and procedure to the patient.
- Make sure the patient and her family clearly understand the prescribed drug regimen.
- Tell the patient to report any new pain sites immediately, especially after trauma.
- Provide emotional support and reassurance to help the patient cope with limited mobility.
http://nursing-concept.blogspot.com/2009/02/free-nursing-care-plans-for-pneumonia.htmlhttp://nursing-concept.blogspot.com/2009/02/free-nursing-care-plans-for-pneumonia.html -
7/31/2019 SEMINAR Neuro Hand-Outs
20/35
20
GUILLAIN-BARRE SYNDROME
DEFINITION: It is an autoimmune attack of the peripheral nerve myelin. The result is acute
rapid segmental demyelination of peripheral nerves and some cranial nerves, producing
ascending weakness with dyskinesia, hyporeflexia and paresthesia.
Stages of GBS:
Acute the symptoms show between one to three weeks.
Plateau the symptoms show between several days to 2 weeks.
Recovery This is the stage wherein there is remyelination which may last up to 2 years.
ETIOLOGY:
- autoimmune disease triggered by a preceding bacterial or viral infection.
- lung infection or gastrointestinal infection
- commonly identified antecedent pathogens: Campylobacter jejuni, cytomegalovirus,
Epstein-Barr virus and Mycoplasma pneumoniae
RISK FACTORS:
The syndrome may occur at any age, but is most common in people of both sexes
between ages 30 and 50.
Precipitating factors may also include post infection e.g. to Campylobacter jejuni, poor hygienestress, poor diet and lifestyle.
MANIFESTATIONS:
- Paresthesia tingling and numbness of the lower extremities
- Muscle weakness of legs progress rapidly ascending paralysis involving the trunk
upper extremities and facial muscles which may mean complete paralysis.
- Difficulty in chewing, swallowing and talking. The cranial nerves are now involved.
- Loss of sensation and sphincter disturbances of bladder and rectum.
- Areflexia or absence of reflexes is also observed.
- Respiratory failure is the respiratory muscle function is affected.
-
7/31/2019 SEMINAR Neuro Hand-Outs
21/35
21
DIAGNOSTICS:
- Lumbar puncture: CSF sample
- ECG
- Electromyography (EMG) tests the electrical activity in muscles
- Nerve conduction velocity test: allow decreased conduction velocity of peripheral nerves
due to demyelination.- Pulmonary function test
PATHOPHYSIOLOGY
MANAGEMENT:Medical:
- No specific treatment instead they prefer symptomatic treatment
- plasmapheresis, used to remove the antibodies from the blood
- high dose immunoglobulin therapy (IVIG) that blocks the antibodies that causes
inflammation
Predisposing Factors
Age, Sex, Autoimmunity
Precipitating Factors
Infection, Poor Hygiene, Stress, Lifestyle, Diet
Infectious pathogens enter the body by the use of multinfenestrated cells or other mechanisms
Innate immune response causes uptake of the pathogens by immature antigen-presenting cells
Migrates to lymph nodes, activates T-cells and B-cells causing humoral response, activation of
complement system and phagocytosis of the bacteria
Molecular mimicry
Immune res onses directed to ca sular com onents; roduce Ab to cross-react with myelin
Lym hocytes and macro hages circulate the blood and find the myelin
Lymphocytic infiltration of spinal roots and peripheral nerves, followed by macrophage-
mediated, multifocal stri in of m elin and axonal dama e
Defects in the ro agation of electrical nerve im ulses, with conduction block
GUILLAIN-BARRE SYNDROME
-
7/31/2019 SEMINAR Neuro Hand-Outs
22/35
22
- ETT/ Tracheostomy with mechanical ventilator
- 4As: Antibiotics, Analgesic, Anticoagulants, Azathiprine & cyclophosphamide(
Immunosuppresants to decrease production)
- feeding tube may be used to prevent choking during feeding if the muscles used for
swallowing are weak
Nursing:
- Monitor vital signs, muscle weakness, gag reflex and swallowing ability.
- Position patient with the head of bed elevated to provide for maximum chest excursion.
- Avoid giving opioids and sedatives that may depress respirations.
- Position patient correctly and provide range-of-motion exercises.
- Provide good body alignment, range-of-motion exercises, and change of position to prevent
complications such as contractures, pressure sores, and dependent edema.
- Ensure adequate nutrition without the risk of aspiration.
- Provide assistive devices as needed (cane or wheelchair) to maximize independence and
activity.
- If verbal communication is possible, discuss the patients fears and concerns.
- Provide choices in care to give the patient a sense of control.
- Teach patient about breathing exercises or use of an incentive spirometer to reestablish
normal breathing patterns.
- Instruct patient to wear good supportive and protective shoes while out of bed to preveninjuries due to weakness and paresthesia.
- Instruct patient to check feet routinely for injuries because trauma may go unnoticed due to
sensory changes.
-
7/31/2019 SEMINAR Neuro Hand-Outs
23/35
23
MYASTHENIA GRAVIS
DEFINTION: It is an autoimmune disease that presents as muscular weakness and fatigue
that worsens with exercise and improves with rest. The manifestations result from a loss of
ACh receptors in the postsynaptic neurons of the neuromuscular junction.
Onset:
EARLY: 20-30 years old and Women are more affected than men
LATE: After age 50 and Men are more often affected
Classifications:
a. Ocular Form b. Generalized Form
Stages of Generalized Form:
I. Mild
II. Moderate
III. Acute Fulminating
IV. Late Severe
ETIOLOGY: The cause of MG is unknown, but 80% of people with the generalized form
of the disease have elevated titers of antibodies to the ACh receptor in their serum.
RISK FACTORS:
a. Predisposing Factors
Gender: Female and Male
Age: In female: 20-40 years old; Male: 60-70 years old
Race: Asian
b. Precipitating Factors
Thymic tumor
Occult Infection
Stress
MANIFESTATIONS:
Increasing weakness with sustained muscle contraction; muscle weakness is
greatest after exertion or at the end of the day
-
7/31/2019 SEMINAR Neuro Hand-Outs
24/35
24
Ptosis- drooping of the upper eyelid
Diplopia-double vision
Neck flexion/extension (Head-drop)
Dysarthria
Expressionless face; tendency for mouth to hang open
Dysphagia
Masticatory weakness
Dyspnea
Extreme quardiparesis/ quadriplegia
Increased salivation
Increased sweating
DIAGNOSTICS:
a. TENSILON TESTING
Edrophonium (Tensilon) is a short-acting drug that is given intravenously (Tensilon
test). A test dose of 2 mg. (for adults) is injected first. If no untoward reaction occurs
(such as increased weakness, change in heart rate or rhythm, nausea, or abdominal
cramps), the remaining 8 mg. is injected. The client is then observed for objective
manifestations of improvement in muscle strength. The effect is transitory, wearing off
after 3 to 5 minutes. Another drug, neostigmine methylsulfate (Prostigmin), may be usedbecause of its longer duration of effect on muscle strength (1 to 2 hours), which allows
better analysis of its effect.
When either drug is used, IV atropine sulphate should be available to inject as an
antidote. This medication counteracts any severe cholinergic reactions (cardiac
dysrhythmias or abdominal cramping).
b. ELECTROMYOGRAPHY (EMG)
EMG helps in confirm the diagnosis. Repetitive stimulation of the nerve with
recording from the involved muscle shows a characteristic decrementing response of
the muscle action potential. Generally, after the initial diagnostic testing is performed by
the practitioner, referral to a neurologist and/or pulmonologist may be necessary for
long-term management.
-
7/31/2019 SEMINAR Neuro Hand-Outs
25/35
25
c. ACETYLCHOLINE RECEPTOR ANTIBODIES
Acetylcholine receptor antibody is a protein found in the blood of most people with
myasthenia gravis. The antibody attacks receptors for a chemical called acetylcholine
which sends signals from nerves to muscles and between nerves in the brain.
MANAGEMENT:
Medical:
1. DRUG THERAPY
Short-acting anticholinesterase drugs- pyridostigmine (Mestinon) and
neostigmine (Prostigmin)
Dosages are highly individualized, based on physiologic response to the medication
The goal is to achieve the maximum benefit (muscle strength and endurance) with the
fewest side effects (excessive salivation, sweating, nausea, diarrhea, abdominal crampsor tachycardia).
Corticosteroids- prednisone
This drug is directed toward reducing the levels of serum ACh receptor antibodies.
Corticosteroids may temporarily worsen manifestations; however this is followed by
gradual improvement in muscle strength. A low dose of alternate-day prednisone may
be effective for many months or years. Precautions with any steroid therapy are
important, including potassium supplements if indicated and liberal use of antacids.
Potential complications of steroid use are cataracts, hypertension, diabetes, fluid
retention, delayed wound healing, and osteoporosis.
Cytotoxic and immunosuppressive drugs- azathioprine (Imuran) and cyclosporine
(Sandimmune), which reduce the level of circulating ACh receptor antibodies.
Plasmapheresis
Plasmapheresis is an adjunctive therapy for clients with refractory MG. It is a
processby which plasma is separated from formed elements of blood. The plasma is
discarded and the packed red blood cells are joined with albumin, normal saline, and
-
7/31/2019 SEMINAR Neuro Hand-Outs
26/35
26
electrolytes and returned to the client. The purpose is to remove plasma proteins
containing antibodies that are believed to cause MG.
Usually, three to five treatments given once daily over 5 to 7 days are required
Potential complications include myasthenic or cholinergic crisis and, rarely,
hypovolemia. Muscle strength should be assessed before and after the procedure , with
particular attention paid to vital capacity, swallowing ability, diplopia, and ptosis to
evaluate the effectiveness of treatment.
Intravenous Immunoglobulin (IVIG)
Intravenous immunoglobulin (IVIG) is a blood
product administered intravenously. It contains the
pooled IgG (immunoglobulin (antibody) G) extracted from the plasma of over one
thousand blood donors. IVIG's effects last between 2 weeks and 3 months. Intravenous
immune globin (IVIG) is the opposite of plasmapheresis - instead of drawing off the
offending antibodies, IVIG swamps the body with pooled gamma globulin antibodies
from many donors.
-
7/31/2019 SEMINAR Neuro Hand-Outs
27/35
27
PATHOPHYSIOLOGY:
Predisposing Factors:Gender; Age;
Familial tendency; Genetics; Race
Precipitating Factors:Thymus/Thyroid problems; Occult
infection; Medications; Autoimmunedisorders; Chemical exposure; Stress
Genetic abnormality/ Autoimmune Response
Affinity of IgG-Ab Abnormal Thymus/Hyperplasia
IgG-4 toneuromuscular junction
Muscular specifickinase (MuSK) - Ab
Impaired postsynapticmembrane differentiation
& clustering of AChR
Anti-MuSK MG
Seronegative MG
Dxcs:(+)Anti-MuSK-Ab
Dxcs:(+) Anti-MuSK-Ab;(-) Anti-AChR-Ab
Abnormal T-helpercell production
Th1/Th2
Dxcs:MRI;Chest CT scan
Abnormal proliferation of B-cell producingAcetylcholine receptor antibodies (AChR-Ab)
Anti-AChR-Ab (IgG1/IgG3 isotype)
Binds to AChR Crosslinks receptors Activates complement system
Blocks binding ofAch to receptor
sites
Endocytosis ofAChR molecules
AChR degradation
Complement-mediated lysis ofpostsynaptic membrane
Anti-AChR MG
MYASTHENIA GRAVIS
Impaired nerve impulse transmission at neuromuscular junction
muscular depolarization
Voluntary muscle weakness
Dxcs:single-fiber electromyography;repetitive nerve stimulation
Dxcs:Tensilon Test
-
7/31/2019 SEMINAR Neuro Hand-Outs
28/35
28
IIIA:Predominant
limb/axial muscle weakness
IIIB:Predominant oropharyngeal/
respiratory muscle weakness
Moderate ocular muscle weakness accompanied withIII
MYASTHENIA GRAVIS
Extraocular muscles Levator palpebrae
S/sx:Diplopia S/sx:Ptosis
Ocular muscle weakness d/t scarcity of junctional foldsI
IIA:Predominant
limb/axial muscle weakness
IIB:Predominant oropharyngeal/
res irator muscle weakness
Mild ocular muscle weakness accompanied withII
IVA:Predominant
limb/axial muscle weakness
IVB:Predominant oropharyngeal/
respiratory muscle weakness
Severe ocular muscle weakness accompanied withIV
S/sx:Limb:
descendingparalysis
Axial:Neck
flexion/extension
(Head-drop)
S/sx:Bulbar:
Dysarthria;Dysphagia;Dysphonia;Masticatoryweakness
Facial:Poor eyelid
closure;Poor cheek
puff;Drooling
Respi:Dyspnea;
Orthopnea;Tachypnea
Needed IntubationV
Management:Medical: O2 admin, ETT, MV, Plasmapheresis/IVIG; Pharm: AChE
inhibitor, immunosuppressants; Surgical: Thymectomy
If treated: Good Prognosis If not: Complications
Myasthenic Crisis Cholinergic Crisis
S/sx:Extreme quadriparesis/ quadriplegia,respiratory insufficiency, aspiration
S/sx:Diarrhea, bradycardia, pupillary
constriction, salivation, sweating
Respiratory Arrest
If treated: Fair Prognosis If not: DEATH
-
7/31/2019 SEMINAR Neuro Hand-Outs
29/35
29
Complications of Drug Therapy:
A. MYASTHENIC CRISIS
-It is precipitated with intercurrent infection or sudden withdrawal of anticholinestrase
drugs.
CLINICAL MANIFESTATIONS
Sudden marked rise in blood pressure because of hypoxia
Increased heart rate
Severe respiratory distress and cyanosis
Absent cough and swallow reflexes
Increased secretions, increased diaphoresis, and increased lacrimation
Restlessness, dysarthria
Bowel and bladder incontinence
INTERVENTION
Increased doses of cholinergic drugs as long as the client responds positively
to edrophonium treatment
Possible mechanical ventilation if respiratory muscle paralysis is acute
B. CHOLINERGIC CRISIS
-It is caused by depolarization block resulting from excessive medication.
CLINICAL MANIFESTATIONS
Weakness with difficulty swallowing, chewing, speaking, and breathing
Apprehension, nausea and vomiting
Abdominal cramps and diarrhea
Increased secretions and saliva
Sweating, lacrimation, fasciculations and blurred vision
INTERVENTION
Discontinue all cholinergic drugs until cholinergic effects decrease
-
7/31/2019 SEMINAR Neuro Hand-Outs
30/35
30
Provide adequate ventilatory support
Administration of 1 mg. intravenous atropine may be necessary to counteract
severe cholinergic reactions, as ordered
SURGICAL:
THYMECTOMY
Thymectomy is the surgical removal of the thymus gland. Located in the upper chest
below the thyroid gland and behind the breastbone, the thymus gland is part of the
body's immune system. During the formation of the fetus, the thymus migrates from the
neck into the chest, and in adults it lies beneath the breastbone (sternum). Like tonsils
and adenoids, the thymus is large in infants and gets smaller, to be replaced by fat, as
we get older, making it hardly functional. It transforms certain white blood cells
(lymphocytes) into disease-fighting T-cells, an important part of the body's defenseagainst viruses and other infections.
Indication
The most common indication for thymectomy is the presence of a tumor (thymoma)
in the thymus gland. Thymomas can be noncancerous (benign), but are potentially
cancerous (malignant) and are known to invade nearby tissue (local metastasis)
Metastasis to more distant tissue is not typical of a thymoma. Thymomas can also be
associated with myasthenia gravis (MG), an autoimmune condition in which the muscles
become weak when the individual's antibodies attack the neuromuscular junction
Thymectomy is indicated for treatment of both non-MG-associated and MG-associated
thymoma.
If most of the thymus gland is removed at surgery, myasthenic symptoms usually
lessen and in some individuals go away completely. Although the relation of the thymus
gland to myasthenia gravis is not totally understood, it appears that the thymus gland islinked to the production of acetylcholine receptor antibodies or other substances that
interfere with neuromuscular transmission.
Nursing Diagnosis:
a. Ineffective Breathing Pattern related to respiratory muscle weakness secondary
to Myasthenia Gravis
-
7/31/2019 SEMINAR Neuro Hand-Outs
31/35
31
b. Impaired gas exchange related to respiratory muscle weakness secondary to
Myasthenia Gravis
c. Ineffective airway clearance related to absence of coughing reflex secondary to
Myasthenia Gravis
d. Activity intolerance related to generalized weakness secondary to Myasthenia
Gravise. Risk for aspiration related to weakness of oropharyngeal muscles secondary to
Myasthenia Gravis
NURSING MANAGEMENT
Encourage deep breathing and coughing;
Provide suction equipment available at bedside;
Encourage adequate nutrition;
Instruct to sit upright when eating, to swallow only when the chin is tipped
downward the chest and never to speak while food is in the mouth;
Promote effective breathing pattern such as mechanical ventilation and
oxygenation;
Increase activity tolerance by providing a carefully planned activities to include
rest periods to conserve energy and muscles have a chance to regain their
strength;
Assist client in ADLs and decrease complications of immobility;
Provision of optimum vision
s
-
7/31/2019 SEMINAR Neuro Hand-Outs
32/35
32
MULTIPLE SCLEROSIS
DEFINITION: It is a disease in which the nerves of the central nervous system (brain
and spinal cord) degenerate.
Myelin, which provides a covering or insulation for nerves, improves the
conduction of impulses along the nerves and also is important for maintaining the health
of the nerves. In multiple sclerosis, inflammation causes the myelin to disappear.
Consequently, the electrical impulses that travel along the nerves decelerate,
that is, become slower. In addition, the nerves themselves are damaged. As more and
more nerves are affected, a person experiences a progressive interference with
functions that are controlled by the nervous system such as vision, speech, walking
writing, and memory.
ETIOLOGY: The cause of multiple sclerosis is still unknown, but researchers claimedthat it may be associated with autoimmune responses of our body.
RISK FACTORS:
Although its role is unclear, genetics may play a role in multiple sclerosis.
European gypsies, Eskimos and African Bantu essentially do not develop multiple
sclerosis, while Native Indians of North and South America, Japanese and other Asian
groups have a low incidence. The general population has less than a one-percen
chance of developing multiple sclerosis.
The chance increases in families where a first-degree relative has the disease.
Thus, a brother, sister, parent, or child of a person with multiple sclerosis stands a one-
percent to three percent chance of developing multiple sclerosis. Similarly, an identica
twin runs a nearly 30% chance of acquiring multiple sclerosis whereas a non-identica
twin has only a 4% chance if the other twin has the disease. These statistics suggest
that genetic factors play a major role in multiple sclerosis.
However, other data suggest that environmental factors also play an important
role.
MANIFESTATIONS:
- visual disturbances,
- limb weakness,
- muscle spasms,
- loss of sensation,
http://www.medicinenet.com/script/main/art.asp?articlekey=81245http://www.medicinenet.com/script/main/art.asp?articlekey=81245 -
7/31/2019 SEMINAR Neuro Hand-Outs
33/35
33
- speech impediment,
- tremors,
- dizziness,
- depression,
- manic depression,
- paranoia, or
- uncontrollable urge to laugh and
weep
DIAGNOSTICS:
- MRI (magnetic resonance imaging) scans with intravenous gadolinium helps to
identify, describe, and in some instances date lesions in the brain (plaques).
- An electro-physiological test, evoked potentials, examines the impulses traveling
through the nerves to determine if the impulses are moving normally or too
slowly.
- Finally, examining the cerebrospinal fluid that surrounds the brain and spinal cord
may identify abnormal chemicals (antibodies) or cells that suggest the presenceof multiple sclerosis.
PATHOPHYSIOLOGY:
MANAGEMENT:
Medical:
- There are many issues for the patient and physician to consider in treating
multiple sclerosis. Goals may include:
Predisposing Factors:
Age, Sex, Heredity,
Genetics, Autoimmunity
Precipitating Factors:
Environment, Respiratory
infections, stress, fatigue
MS T-cells infiltrate the BBB
Virus reduces the strength of the junctions forming the blood-brain barrier (BBB)
T-cells locked in the brain perceives myelin as an alien agent
T-cells attack the myelin
Activation of inflammatory response
MULTIPLE SCLEROSIS
http://www.medicinenet.com/script/main/art.asp?articlekey=421http://www.medicinenet.com/script/main/art.asp?articlekey=421 -
7/31/2019 SEMINAR Neuro Hand-Outs
34/35
34
1. improving the speed of recovery from attacks (treatment with steroid
drugs);
2. reducing the number of attacks or the number of MRI lesions; or
3. attempting to slow progression of the disease (treatment with disease
modifying drugs or DMDs).
4. An additional goal is relief from complications due to the loss of function ofaffected organs (treatment with drugs aimed at specific symptoms).
- Corticosteroids: prednisone (Deltasone, Liquid Pred, Deltasone, Orasone,
Prednicen-M) ormethylprednisolone (Medrol, Depo-Medrol)
- Interferons for relapsing MS
Nursing Diagnosis:
Self-Care Deficit Self-Esteem Disturbance
Potential for Ineffective Family Coping: Compromised
Sleep Disturbance
Social Isolation
Nursing Management:
- Provide emotional and psychological support for the patient and family.
- Increase patient comfort with massages and relaxing baths.
- Administer medications as needed.
- Promote emotional stability. Help the patient establish a daily routine to maintain
optimal functioning.
- Keep bedpan or urinal readily accessible because the need to void is immediate.
- Encourage adequate fluid intake and regular urination.
- Watch for adverse reactions to administered medications.
- Monitor bowel and bladder function during hospitalization.- Assess patients neurologic status for deficits.
- Educate the patient nad her family about this chronic disease.
- Emphasize the importance of exercise.
- Teach the patient about bowel and bladder training if necessary.
http://www.medicinenet.com/script/main/art.asp?articlekey=809http://www.medicinenet.com/script/main/art.asp?articlekey=906http://www.medicinenet.com/script/main/art.asp?articlekey=906http://www.medicinenet.com/script/main/art.asp?articlekey=809 -
7/31/2019 SEMINAR Neuro Hand-Outs
35/35
REFERENCES
Black, J. and Hawks, J., (2009). Medical-Surgical Nursing: Clinical Management for
Positive Outcomes. 8th Edition. Missouri: Saunders Elsevier.
Doenges, M., et.al., (2008). Nurses Pocket Guide: Diagnoses, Prioritized Interventions
and Rationales, 11th ed. Pennsylvania: F.A. Davis Company.
Huether, S. and McCance, K., (2008). Understanding Pathophysiology, 4th ed
Singapore: Elsevier Pte Ltd.
Marieb, E., (2008). Essentials of Human Anatomy and Physiology, 9 th ed. Singapore
Pearson Education South Pte Ltd.
McCann, J., et.al., (2010). Professional Guide to Pathophysiology, 3 rd ed. Philadelphia
Lippincott Williams and Wilkins.
Silbernagl, S., et.al., (2010). Color Atlas of Pathophysiology, 2nd. Ed. Germany: Georg
Thieme Verlag KG.
WHO, (2011). World Health Organization. Retrieved January 29, 2012 from
http://www.who.int/en/.
http://www.who.int/en/http://www.who.int/en/