
Implementation of the new SGAR Curriculum at Kantonsspital Baselland, Liestal

Sedation during Regional Anesthesia
A. Borgeat
Orthopedic University Clinic of Zurich/Balgrist
Switzerland
The goal of sedation is
to produce a relaxed patient who is
comfortable and cooperative
throughout the duration of surgery
analgesia sedative conscious
sedation

Predictors of patient satisfaction
with regional anesthesia
De Andrés et al.
Reg Anesth 1995;20:498,
N = 154; Spinal 85%, Epidural 9%, Peripheral nerve block 6%
Advantages
• Speaking with
relatives 73%
• Staying awake 72%
• Absence of immediate
postoperative pain 37%
Disadvantages
• Performance of the block 18%
• Fear of pain 10%
Patient attitude
• Favorable 48%
• Indifferent 45%
• Negative 7%

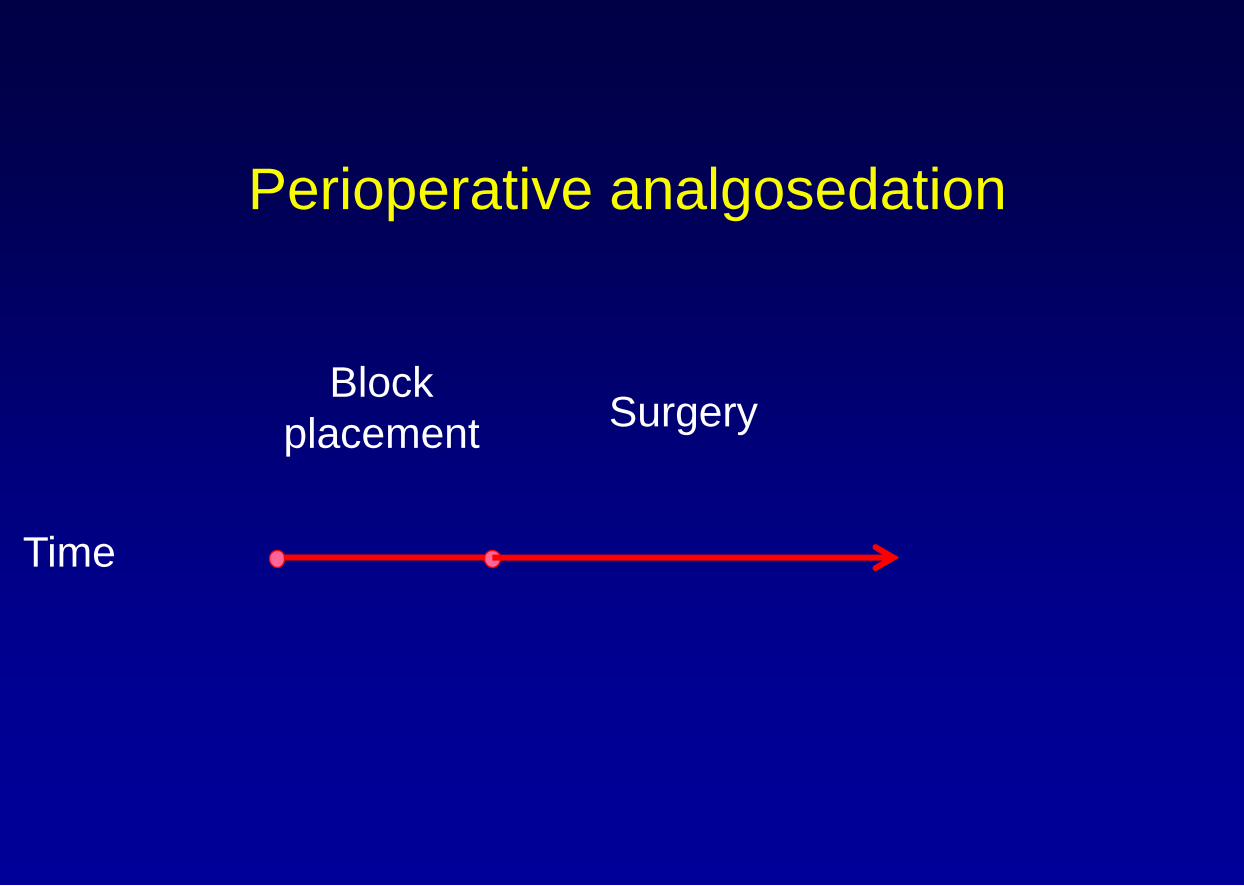
Perioperative analgosedation
Time
Block
placement
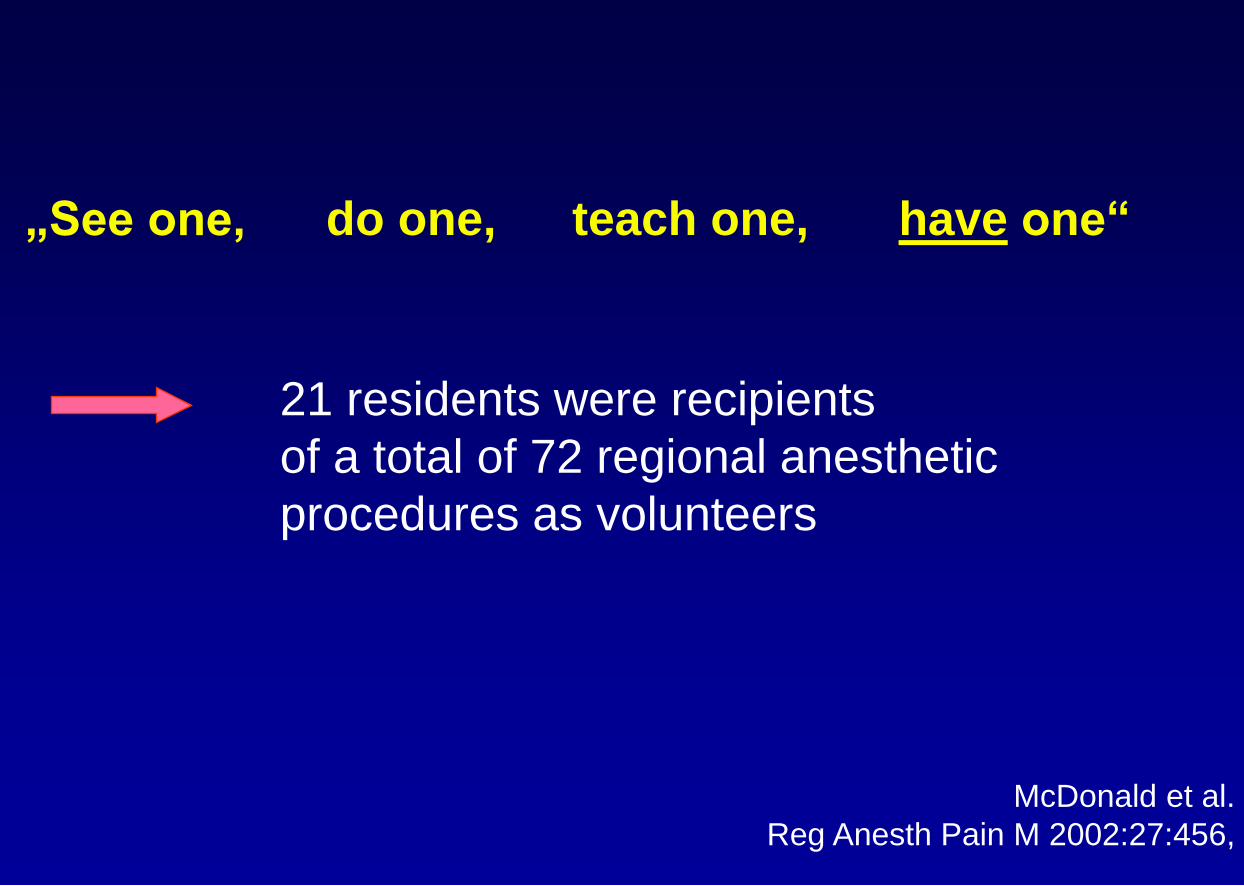
„See one,
McDonald et al.
Reg Anesth Pain M 2002:27:456,
21 residents were recipients
of a total of 72 regional anesthetic
procedures as volunteers
do one, teach one, have one“

Block placement :
the resident experiences
McDonald et al.
Reg Anesth Pain M 2002;27:456,
• Preoperative consultation +++
• Physical contact, „gentle touch“ +++
• Communication, explain action +++
• Paresthesias +++++
• Value of analgosedation ++++
• Local anesthesia infiltration ++

CNS Toxicity
time
LA concentration
threshold
)

Seizures after PNB (prospective study)
Interscalene block 3‘459 0
Supraclavicular block 1‘899 1
Axillary block 11‘024 1
Mid-humeral block 7‘402 1
Psoas compartment block 394 1
Femoral block 10‘309 0
Sciatic block 8‘507 2
Popliteal block 952 0
Performed Seizure
Auroy et al.
Anesthesiology 2002;97:1274,

Alexander et al. Can J Anaesth 1987; 34:343,
Rendoing et al. Anesth Analg 1969;26,445,
Effect of pH and pCO2 on Toxicity

Interaction Propofol - Remifentanil
Perioperative analgosedation
Time
Block
placement Surgery

Surgery : facts to consider
• boredom, anxiety
• occurrence of pain
• side-effects due to analgosedation
• discomfort
adapt and change your drug
administration quickly
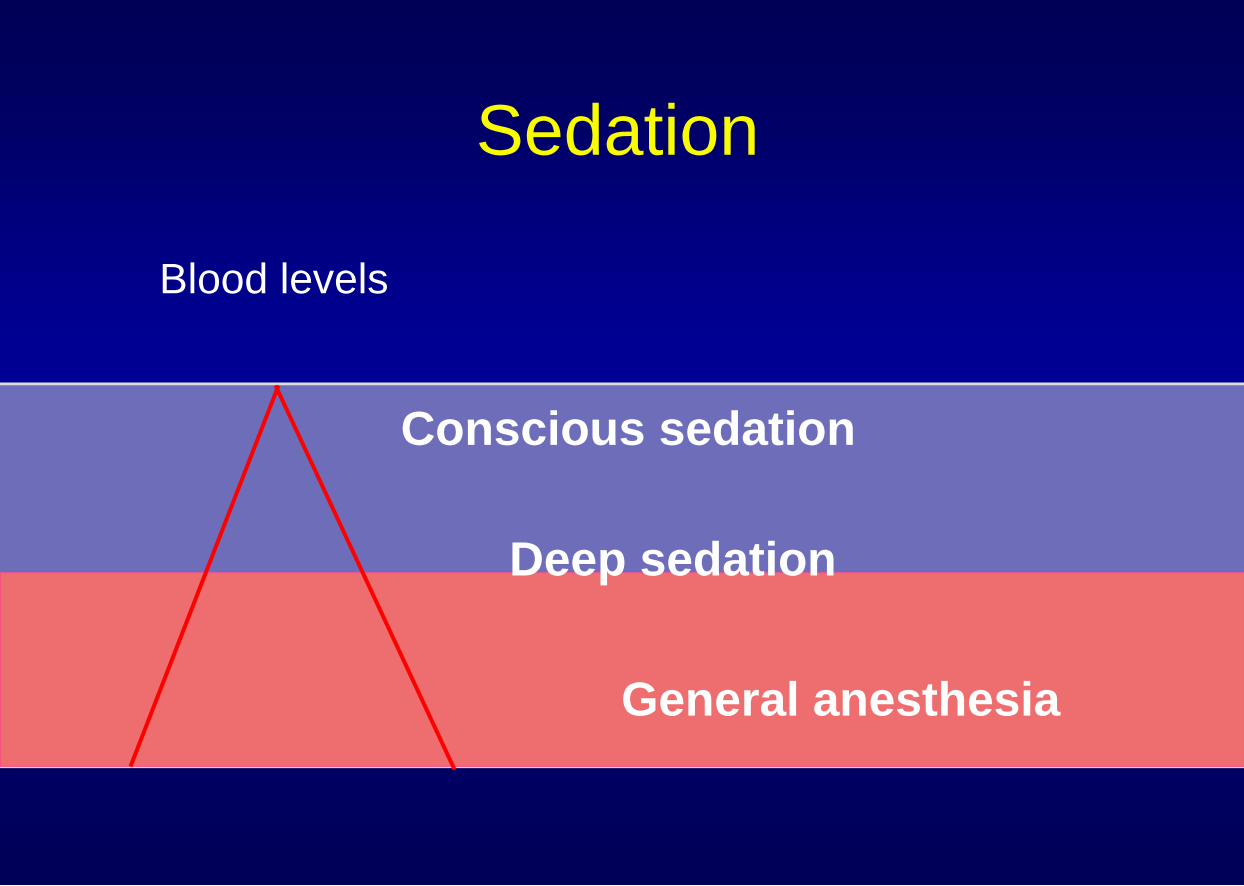
Sedation
Blood levels
Conscious sedation
Deep sedation
General anesthesia

Clinical case I
• Subacromial decompression and
arthroscopic rotator cuff repair
• ISB
• Beach chair position
• Patient 49 yrs, ASA I
Clinical case II
• Patient was unconscious, but able to
be aroused and continued to breathe
spontaneously
± DEEP SEDATION
• SpO2 97-98%
• Continuous infusion of propofol for sedation

Clinical case III
• Audible stridor, severe neck and chest
edema
• GA, LM, fibroscopic intubation ...
• After 3h SpO2 67%

Antonucci et al.
Minerva Anestesiologica 2006;72:995,

Smith et al
J. Shoulder Elbow Surg 2008; 17:415,
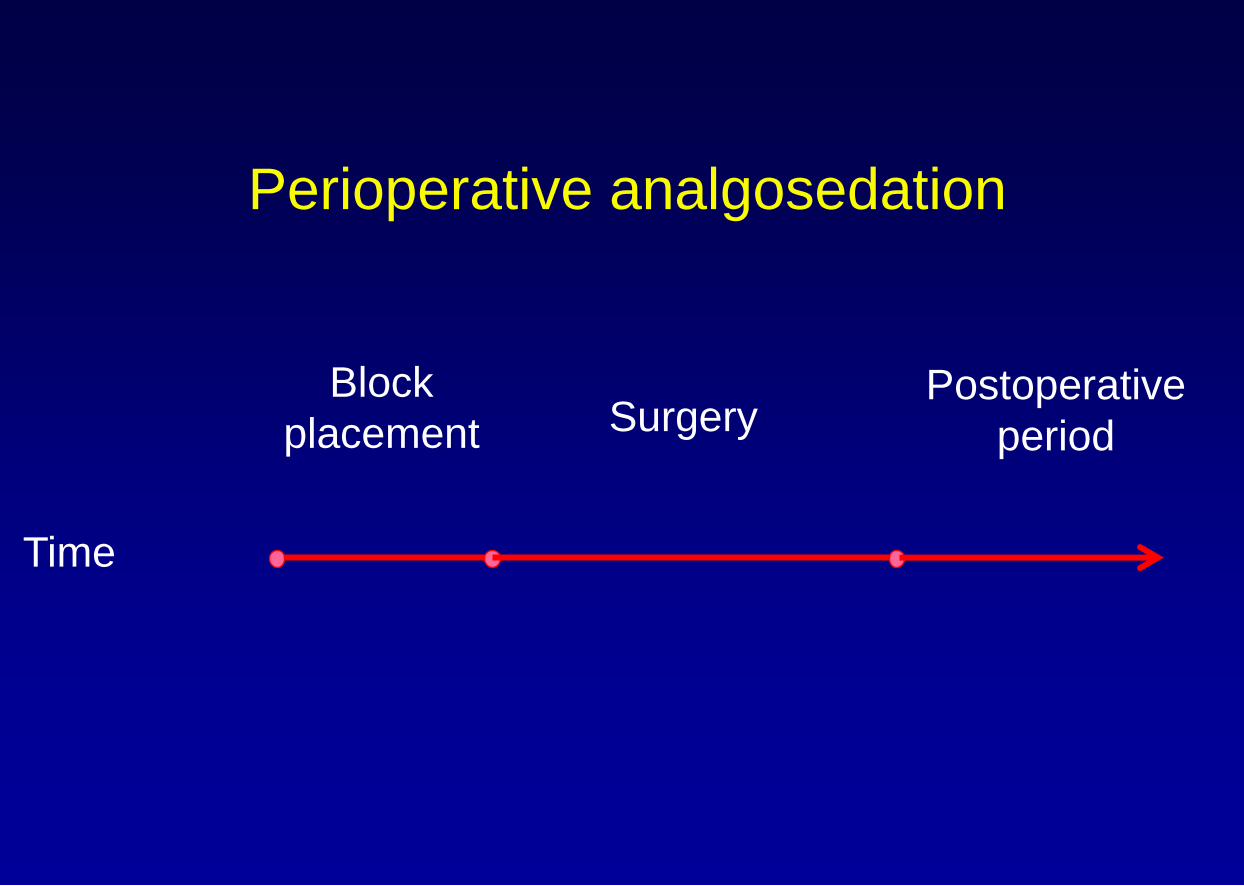
Perioperative analgosedation
Time
Block
placement Surgery Postoperative
period

Postoperative period :
facts to consider
• Side-effects due to sedation
• Level of sedation

Sieber et al
Mayo Clin Proc 2010;85:18,
L
S
L
S D
S
D
S
Po
sto
pe
rative
de
liriu
m
Du
ratio
n o
f
de
liriu
m
1.
4 0.5*
19*
40
day %
Light Sed : BIS > 80
Deep Sed : BIS ~ 50
NNT : 4.7
*p > 0.05
> 65 y

Sedation :
remifentanil vs propofol
% • Remi. 0.2µg/kg/min
(5 min before block placement
50% after block placement)
* P < 0.05
Mingus et al.
J Clin Anesth 1998;10:46,
• Prop. 100µg/kg/min
(5 min before block placement
50% after block placement)
Pa
in s
co
re
0 1 2
81
60
13 13 4
26
%
Sid
e-e
ffe
cts
N V Apnea
60
17* 21
6 8 0

Remifentanil sedation vs Propofol
during regional anesthesia
* P < 0.05
Servin et al.
Acta Anaesth Scand 2002;46:309,
%
15
92 P 500 µg/kg, 50 µgkg/min
5 *
P R
R 0.5 µg/kg, 0.1 µgkg/min
Postoperative
pain
%
2 *
27
P R
Perioperative
NV
%
19 *
46
P R
Respiratory
depression

Sedation : uncontrolled movements
• are unpredictable
• are most often associated with hypno-
sedatives
- Propofol: effect site < 0.5-0.8ug/ml
- Midazolam ?
• combination hypnosedative-opioid may
limit their occurrence

Midazolam Propofol
Dreamers 12 % 40 %*
Kim DK et al
Anesth Analg 2011;112:1076,
*p <0.05
1 very negative
5 very positive
1 only remember dreaming
5 very memorable
1 not at all vivid
5 very vivid
1 not at all intense
5 very intense
1 Not at all strange
5 very strange

Sedation : what conditions ?
• Sedation has to be easy to manage,
predictable and quickly reversible

Sedation : what conditions ?
• Sedation has to be targeted
anxiolytic, sedative
analgesic
analgo-anxiolytic
multimodal sedation

Sedation : what conditions ?
Pharmacokinetic conditions
• short onset time and short „time to peak effect“

Third
Compartment Second
Compartment
Fat Musclel
Effect
Compartment Central
Compart-
ment
Keo
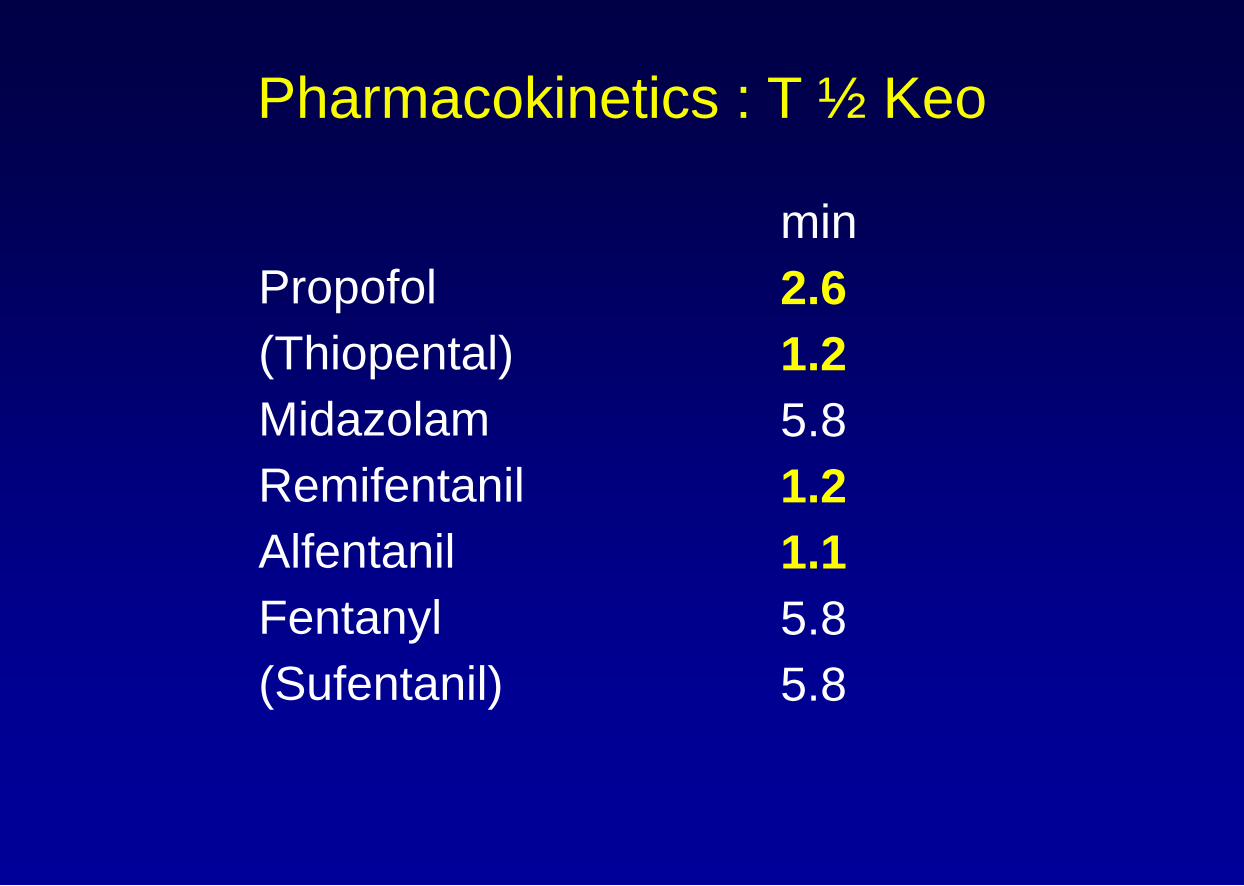
Pharmacokinetics : T ½ Keo
Propofol
(Thiopental)
Midazolam
Remifentanil
Alfentanil
Fentanyl
(Sufentanil)
min
2.6
1.2
5.8
1.2
1.1
5.8
5.8


Midazolam 2mg bolus
(peak effect at 13.5 min)
Propofol 20mg bolus
(peak effect at 3.5 min)

Pharmacokinetics
Propofol
(Thiopental)
Midazolam
Remifentanil
Alfentanil
Fentanyl
(Sufentanil)
T ½ Keo
min
2.6
1.2
5.8
1.2
1.1
5.8
5.8
TPE
min
3.5
1.4
13.5
1.5
3.0
3.5
5.8

Pharmacokinetics : clearance
Propofol
(Thiopental)
Midazolam
Remifentanil
Alfentanil
Fentanyl
(Sufentanil)
L/h
113.6
12.9
25.8
156.3
21.3
36.4
61.3

Techniques of sedation
• Repeated administration of bolus

3020100
Concentr
ation µ
g/m
l
2
1
0
Infu
sio
n R
ate
(ml/h
r)
1000
900
800
700
600
500
400
300
200
100
0
Techniques of sedation
• Repeated administration of bolus
• TCI sedation

TCI sedation
• Easy to handle
• Predictable
• Easy to adjust
Change to GA
(TCI sedation TCI-GA is easy)
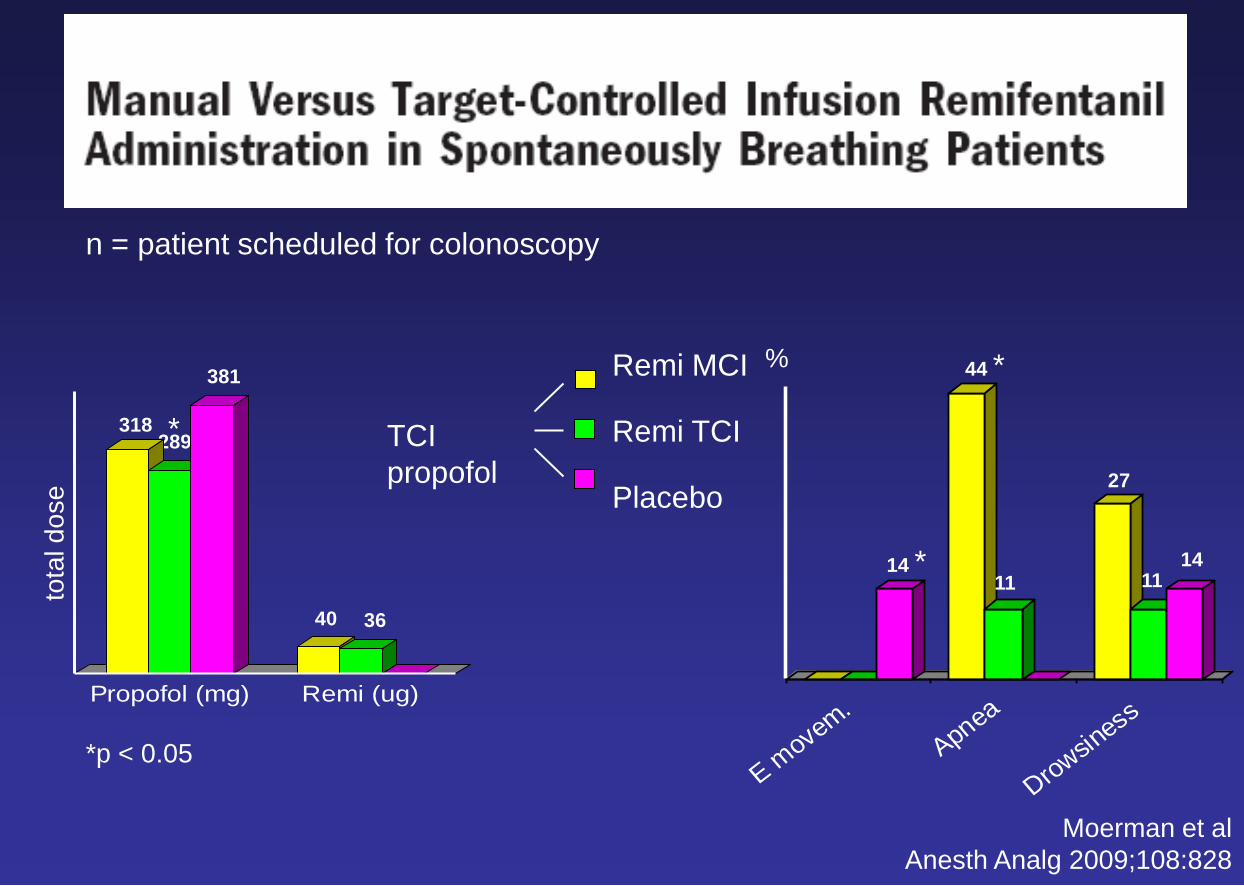
Moerman et al
Anesth Analg 2009;108:828
*p < 0.05
289
Propofol (mg) Remi (ug)
318
381
40 36
*
tota
l d
ose
E movem
.
Apnea
Drowsin
ess
11
44 *
14 * 11
27
14
%
TCI
propofol
Remi MCI
Remi TCI
Placebo
n = patient scheduled for colonoscopy

Techniques of sedation
• Repeated administration of bolus
• TCI Sedation
• Target-controlled patient-
maintained sedation
Patient-controlled sedation

Sedation / Monitoring
• Scores : Ramsay, OAA/S, Wilson
• BIS, AEP
• Standard monitoring

Sedation / Monitoring
• BIS, AEP
• Scores : Ramsay, OAA/S, Wilson
• To observe and to communicate with
the patient
• Standard monitoring
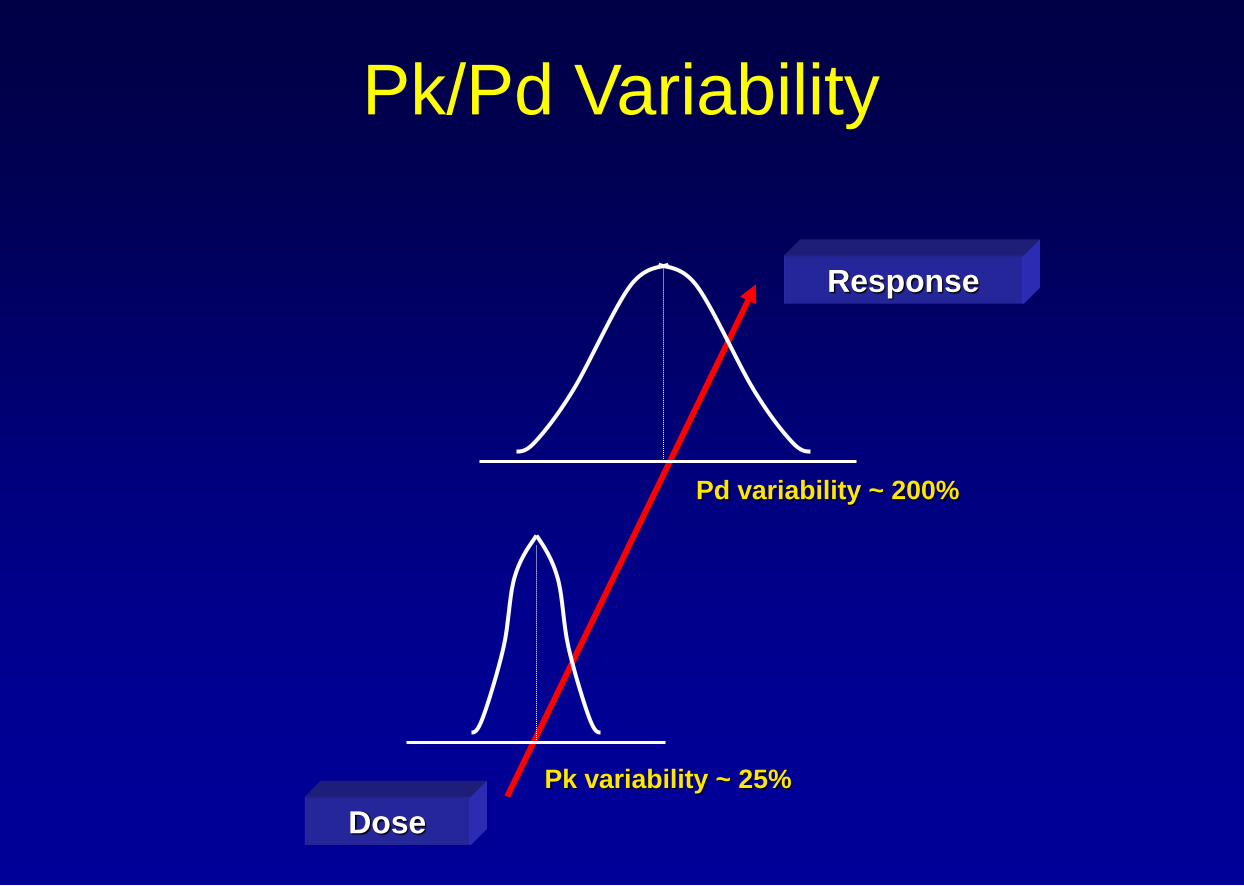
Pk/Pd Variability
Dose
Pd variability ~ 200%
Response
Pk variability ~ 25%

Guidelines
• Start at a low dose and titrate
• Supplementary nasal 02
• Allow time for effect-site equilibration
• Assess patient regularly. Respiratory rate
• Use appropriate monitoring (Sp02)
• NB sedation should not be used as analgesia

Conclusions
• Propofol and remifentanil are particularly
well suited for TCI sedation (multimodal
approach)
• Observation and communication with the
patient are fundamental during sedation
• TCI sedation is actually the technique of
choice for perioperative sedation
Thank you for you attention


















