Praeklampsie! HELLP - sgar-ssar.ch · syndrom, transfer to the childrens ICU (main building)...
48
CASE REPORT Anne M.Stauffer,MD Kantonsspital Graubünden
Transcript of Praeklampsie! HELLP - sgar-ssar.ch · syndrom, transfer to the childrens ICU (main building)...

CASE REPORTAnne M.Stauffer,MD
Kantonsspital Graubünden



Kantonsspital Graubündenmain building


Kantonsspital GraubündenKreuzspital


Kantonsspital GraubündenFontana

32j. patient, primigravida, nullipara
personal history: no pathologies
family history: pm art. hypertensionsince the age of 30.pregnancy :- presumed delivery date 8.4.2009- singul. cord artery was diagnosed in the24.week of gestation

Routine controll at 29 0/7 weeks of gestation
headache, facial oedema weight + 9 kg in 4 weekshypertension 165/110Proteinuria +++musculary reflexes ++

emergency admission to the hospital
hypertension BP 210 / 130 mmHg
minor haedachemoderate oedemaproteinuria +++ Lab :ALT (GPT) 28 U/l (7-49)
AST (GOT) 54 U/l (9-26)LDH 540 U/L (240-480)tc 204`000
diagnosis: preeclampsia
Therapy:
stabilisation :magnesium/ nepresol2h later : cesarean section in SA
(the cavum utery was cleaned by curettage)

Child
Keira Lynnweight : 940 gAPGAR -Score 7-8-9pHa : 7,37, pHv 7,4ITN because of respiratory distress syndrom, transfer to the childrens ICU (main building)

postoperative corse 2 day (delivery ward)
persistent hypertensionhyperreflexia, sensitivity to light, right upper abdominal pain, increasing oedema, decreased urinary output Lab: AST (GOT) 73 U/l ALT (GPT) 22 U/l;
LDH 1102tc 72`000, fragmentocytes

diagnosis HELLPHemolysis (LDH > 600U/L = destruction of red blood cells), elevatet liver enzymes (AST> 70U/L), low platelets (< 100`000) (Tennessee classification system)
0,5-0,9 % of all pregnancies, 10- 20 % of the cases with severe preeclampsia
70 % before delivery ( peak 27-37 weeks of gestation)
30 % within 48 h after delivery (most patients had hypertension and proteinuria prior to delivery)(The HELLP Syndrome, clin. Issues an management a review; BMC Pregnacy and Childbirth 2009)

Pathophysiology and laboratory findings
Microangiopathic hemolytic anaemia (MAHA)coombs test negativefragmentocytesincreased reticulocytesdecreased hemogloginundetectable haptoglobin levels increased LDH (red blood cell destruction)elevated AST due to liver injurydecreased platelets( < 100000) due to consumption

postpartum HELLP
increased risk of renal failure and pulmonary edema
surveillance and therapy:
Hypertension : Aldomed / Tenormin poNepresol Infusion
Eclampsia Prophylaxis : Magnesium
Corticosteriods : Celestone 12 mg ( 1x )

100
c-section
2 FFP
Tc

Max-Wert2658
LDH
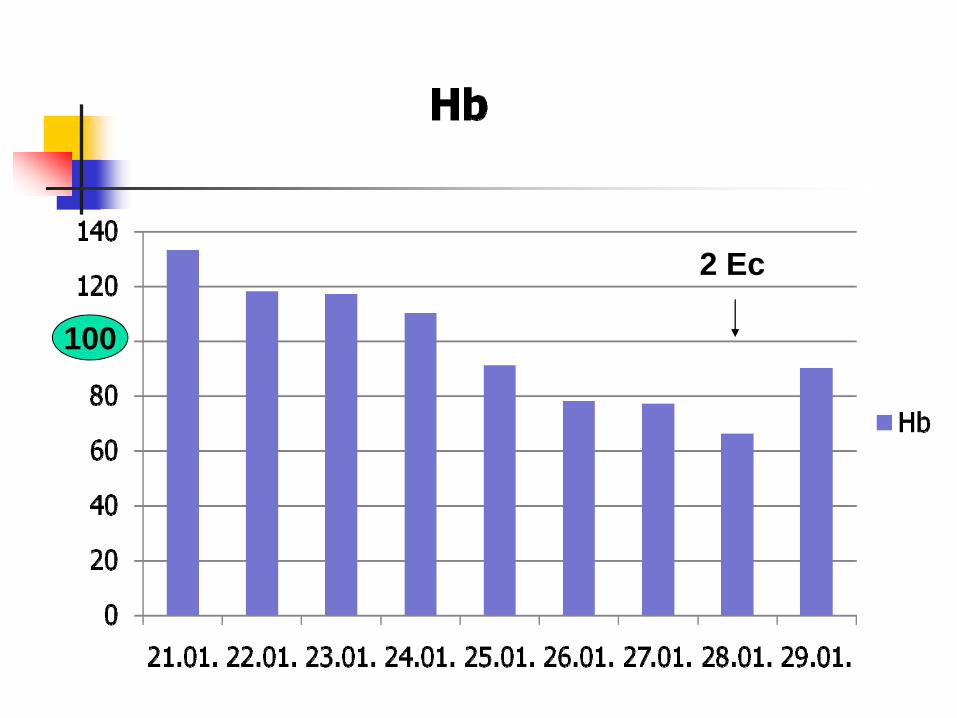
100
2 Ec

Fluid management /24h
-3000
-2000
-1000
0
1000
2000
3000
4000
22.01. 23.01. 24.01. 25.01. 26.01. 27.01. 28.01.
Zeit
ml

creatinin
100

differentialdiagnosis(after 8 days on the delivery ward )
microangiopathic haemolytic anaemia (MAHA)- hemolytic uremic syndrom (HUS)- thrombotic- thrombocytopenic Purpura (TTP)
Transfer to the ICU on 29.1.2009

What is HUS / TTP ?
First description of TTP by Moschcowitz 1924 andHUS by Gasser et al. 1955.May be manifestations of a simular mechanism of microvascular platelet aggregation. (Prof.Joel Moake,Baylor College of medecine, Methodist Hospital and Rice University, Houston , Texas the Lancet; vol 343, february 1994, hemolytic-uremic syndrom. Basic sience )
If the platelet aggregation is systemic and extensive-and especially if the central nervous system is involved, the disorder is TTP.If platelet aggregation is less extensive and involves the kidneys predominantely, the entity is HUS.

Pathogenesis ( hypothesis)
To many unusualy large von- Willebrand- Factor Multimers ( ULvWF) that leed under certain conditions ( Infection/ Pregnancy/ malignant tumor ) to a spontaneus aggregation of platelets.ADAMTS-13 deficiencyAntibodies against ADAMTS-13ADAMTS- 13 = enzyme which devides the large vWF that is procuded by the endothelia cells into smaller multimers that are responsible for the binding of clotting factor VIII.

Aethiology
Hereditary TTP : ADAMTS-13 Deficency : Schulman-Upshaw Syndrom (autosomal recessive). Recurrent TPP. Trigger infection/ operations / pregnancy
Idiopathic TTP : Autoantibodies agianst ADAMTS-13 .Trigger: pregnancy, medications, infection
Secondary TTP : medikation ( Cyclosporin, Mitomycin, Kokain, Clopidogrel) malignant disease, pregnancy
HUS : Trigger : Infections 90 % in children (verotoxin producing E.coli, Shigella, HIV) secondary HUS :Pregnancy, deficiency of complement factor H, medication...

HereditaryTTP
IdiopathicTTP
SekundaryTTP
HUS
ADAMTS 13Aktivity low
ADAMTS13Aktivityblocked
ADAMTS13Aktivitynormal
ADAMTS 13AktivityNormal
Geneticdefect
antibodies ? ?
ADAMTS-13 (A Adesintegrin and Metalloprotease with ThromboSpondinlike repeats) Prof.P. Knöbl, Dept.Hämatologie, Universitätklinik für Innere Medizin, Wien nephroscript 2.07

presentation in pregnancy
10-25 % of secondary HUS/TTP are in pregnant women or postpartum, 1:25000 Pregnancies(J.nephrol. Team 4-2003)166 pregnancy associated TTP in the english- language publications from 1955- 2006 ( James N. Martin, univertsity of Missisippi medical center; American Journal of Obstetrics and Gynecology, August 2008)
TTP 60% < 24 weeks of gestationDD to HELLP syndrome is crucial !case series with good outcome with plasmaphesresis in ongoing pregnancy ( review: Semin. Hematol. 1997; 34:148-158)
HUS predominantely postpartum

Clinical SymptomsMyoglobinuriaPurpura ( rare massive bleeding)Fever (TTP)Flucuating neurological symptomsHypertensionAbdominal painOrgan failure ( heart / pancreatitis)Signs of renal failure

Typicaly laboratory findings
AnaemiaThrombocytopenia (often rapid drop < 30`000)RetikulocytosisFragmentocytes elevatedLDH (at least 2-3x elevated) LDH/AST Ratio TPP/HUS> HELLPHaptoglobin not detectablecreatinin elevated (HUS)Normal clotting test ( INR / PTT)Coombstest negativenormal diff. blood count, Leukocytosis possible

Vollbild anzeigen.url
Vollbild anzeigen.url
Fragmentocyten

Therapy
PlasmapheresisPlasma infusions if no plasmapheresis is available evt. Steroide
Goal : elimination of ULvWF multimerselimination of auto-antibodies against ADAMTS-13replacement ADAMTS-13

contraindicated
Transfusion of Thrombocytes !!!!

therapy of our patient
Plasmaexchange with FFP
Spiricort for 5 days

Hb
020406080100120140
21.01.
22.01.
23.01.
24.01.
25.01.
26.01.
27.01.
28.01.
29.01.
30.01.
31.01.
02.02.
03.02.
04.02.
06.02.
07.02.
Hb
100 2 Ec
Plasmaexchange

Tc
0
50
100
150
200
25021.01.
22.01.
23.01.
24.01.
25.01.
26.01.
27.01.
28.01.
29.01.
30.01.
31.01.
02.02.
03.02.
04.02.
06.02.
07.02.
Tc1002 FFP
Plasma-exchange

Plasma-exchange
LDH

0
20
40
60
80
100
120
140
160
180
21.01. 25.01. 29.01. 03.02. 09.02.
Kreatinin
creatinin
100
transfer to the ICU

Outcome of TTP/ HUS
TTP in pregnancy : Without plasmabased therapy > 90 % Mortality58 % mortality (1955-1980): 17 % plasma therapy17 % mortality (1980-1996): 91.7 % plasma therapy9 % mortality (1996-2006): 96.5 % plasma therapy
AJOG; august 2008
HUS postinfectious in children < 5 % mortalitysecondary HUS prognosis is worseMany cases with permanent need for dialysisProf.J Böhler : Lebendtransplantation nach postpartalem HUS- eine medizinisches und ethisches Dilemma J nephrol. Team 4-2003; J.Gerth et al. Schwangerschaftsazzoz thrombotische Microangiopathie,Med. Klin.2002; 97: 547-52

discharge 27 days after c-section
creatinin 132umol /l ; clearance 66 ml/hproteinuria ( 4g/d)antihypertensive therapyCoversum ( ACE Inhibitor) 6mg /d

Mainly glomerular thrombotic Mikroangiopathieglomerular capillary thrombosis with some arteriolar thrombosis and necrosis
Renal biopsy as predictor for outcome

histopathology as a clue for prognosis
This pattern is normally seen in diarrhoea- associatet HUS and recovery is expected.
Most often with idiopatic HUS, particularly in adults, arterioles and small arterie show severe intimal proliferation with luminar stenosis.Here the recovery is unusual

outcome 5 month postpartum
patient without any subjecive impairmentproteinuria 0.9g /dCreatinin 83 umol/l
Special lab- Test : no congenital ADAMTS 13 Deficency

Is a subsequent pregnancy safe?
congenital ADAMTS13 Deficiency : almost 100 % risk of recurrenceSurch for antiphospolipid antibodies
In the Oklahoma review :a future pregnancy may be a save and appropriate decision for women who have recovered from TPP/ HUS(Jim George, Oklahoma HUS/ TPP Regestry; Vesseley SK et al. Transfusionen 204; 44:1149ff)

conclusion
TTP and HUS are rare but very serious conditions in pregnancy!
differentialdiagnosis must be activly searched ( Patients history /lab Test for ADAMTS-
deficancy or ADAMTS-13 Antibodies) specialists should be involved

conclusion
Woman with HELLP who demonstrate progressive elevation of bilirubin and creatinine 72 h after delivery may benefit from plasma exchage with FFP.

conclusion
Transfusion of thrombocytes can be deleterious