Sea Urchin Spine Arthritis of the Hand
4
SCIENTIFIC ARTICLE Sea Urchin Spine Arthritis of the Hand Takuro Wada, MD, Tamotsu Soma, MD, Keiko Gaman, MD, Masamichi Usui, MD, Toshihiko Yamashita, MD Purpose Although rare, hand injury caused by puncture with the sea urchin spine can result in serious complications. To emphasize its clinical significance, this article describes a group of patients who sustained chronic granulomatous arthritis induced by puncture with sea urchin spine (designated sea urchin spine arthritis). Methods Five patients who developed sea urchin spine arthritis of the hand after puncture with sea urchin spine were treated at our hospitals. All lesions involved the proximal interphalangeal (PIP) joint (4 index fingers and 1 middle finger). Patients experienced pain, swelling, and discomfort around the site of puncture immediately after the injury. These initial symptoms subsided within a few days, and secondary symptoms including fusiform swelling, limited motion, and mild pain of the PIP joint appeared from 1 to 2 months later. Laboratory tests of inflammation and blood cell counts were negative. Plain radiographs showed soft tissue swelling and osteolysis but no visible spine. Thorough synovectomy of the PIP joint was performed, and the granulation tissue around the joint was also removed. Results No microorganism was identified from tissue culture or polymerase chain reaction in any of the 5 patients. At a mean follow-up of 21 months, 2 patients exhibited essentially normal active motion of the affected PIP joint, whereas the remaining 3 patients had diminished range of motion. Conclusions Diagnosis of sea urchin spine arthritis can be made by history of sea urchin spine injury, a symptom- free period before the development of synovitis, and the absence of laboratory test abnormalities. Neither antibiotics nor nonsteroidal anti-inflammatory agents are effective. Undertaken early enough, thorough synovectomy might avoid complications and obtain favorable results. (J Hand Surg 2008;33A:398 –401. Copyright © 2008 by the American Society for Surgery of the Hand.) Type of study/level of evidence Therapeutic IV. Key words Arthritis, granuloma, PIP, sea urchin. C UTANEOUS INJURIES OF the hand from sea urchin spines may be seen in persons who have exposure to oceans and fresh ocean products. These injuries usually raise an immediate reaction characterized by local pain, burning, erythema, and edema that subside in a few hours if the spine fragments are completely removed. 1,2 In contrast, a remnant of the spine tip remaining in the wound frequently causes a delayed response, which is called sea urchin granuloma. 3 When joints are penetrated, the inflammation may take on the form of a florid granulomatous synovitis, which can result in joint destruction (sea urchin spine arthritis) if appropriate therapy is not provided in time. There have been 7 reports including 12 patients with respect to sea urchin spine arthritis of the hand. 4 –10 Clinical manifestation, diagnosis, and management of this pathology have not been understood clearly by hand surgeons. In particular, the literature has not described the treatment outcome in detail. We present 5 patients with sea urchin spine arthritis of the hand due to sea urchin spine injury and discuss an appropriate treatment for this rare pathologic condition. MATERIALS AND METHODS This retrospective study includes 5 patients (3 men and 2 women) diagnosed with sea urchin spine arthritis of the hand due to sea urchin spine puncture who were treated from 2000 to 2004 (Table 1). Four patients were fishermen and 1 patient was involved in preparing sea urchins at a seafood company. Injuries were of the index finger in 4 patients and middle finger in 1 patient. All lesions involved the proximal interphalangeal (PIP) joint. The mean age was 37 years (range, 23 to 51 y). All 5 patients reported a sea urchin spine injury and had tried to remove the spine. The patients experienced pain, swelling, and discomfort around the site of puncture immediately after the injury. These initial symptoms subsided within a few days. The time between the injury and the development of the joint From the Department of Orthopaedic Surgery, Sapporo Medical University, Sapporo Japan; and Higashi-Hokkaido Hospital, Kushiro, Japan. Received for publication August 30, 2007; accepted in revised form November 21, 2007. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. Corresponding author: Takuro Wada, MD, Department of Orthopaedic Surgery, Sapporo Medical University, South 1, West 16, Sapporo 060-8543, Japan; e-mail: [email protected]. 0363-5023/08/33A03-0017$34.00/0 doi:10.1016/j.jhsa.2007.11.016 398 © ASSH Published by Elsevier, Inc.
-
Upload
takuro-wada -
Category
Documents
-
view
213 -
download
1
Transcript of Sea Urchin Spine Arthritis of the Hand

SCIENTIFIC ARTICLE
Cuphcfu
o
3
Sea Urchin Spine Arthritis of the Hand
TakuroWada, MD, Tamotsu Soma, MD, Keiko Gaman, MD, Masamichi Usui, MD,Toshihiko Yamashita, MD
Purpose Although rare, hand injury caused by puncture with the sea urchin spine can result in seriouscomplications. To emphasize its clinical significance, this article describes a group of patients who sustained chronicgranulomatous arthritis induced by puncture with sea urchin spine (designated sea urchin spine arthritis).
Methods Five patients who developed sea urchin spine arthritis of the hand after puncture with sea urchin spine weretreated at our hospitals. All lesions involved the proximal interphalangeal (PIP) joint (4 index fingers and 1 middle finger).Patients experienced pain, swelling, and discomfort around the site of puncture immediately after the injury. These initialsymptoms subsided within a few days, and secondary symptoms including fusiform swelling, limited motion, and mild painof the PIP joint appeared from 1 to 2 months later. Laboratory tests of inflammation and blood cell counts were negative.Plain radiographs showed soft tissue swelling and osteolysis but no visible spine. Thorough synovectomy of the PIP joint wasperformed, and the granulation tissue around the joint was also removed.
Results No microorganism was identified from tissue culture or polymerase chain reaction in any of the 5 patients.At a mean follow-up of 21 months, 2 patients exhibited essentially normal active motion of the affected PIP joint,whereas the remaining 3 patients had diminished range of motion.
Conclusions Diagnosis of sea urchin spine arthritis can be made by history of sea urchin spine injury, a symptom-free period before the development of synovitis, and the absence of laboratory test abnormalities. Neither antibioticsnor nonsteroidal anti-inflammatory agents are effective. Undertaken early enough, thorough synovectomy mightavoid complications and obtain favorable results. (J Hand Surg 2008;33A:398–401. Copyright © 2008 by theAmerican Society for Surgery of the Hand.)
Type of study/level of evidence Therapeutic IV.
Key words Arthritis, granuloma, PIP, sea urchin.
rabudul
ta
MTwhfaspt3upti
UTANEOUS INJURIES OF the hand from sea urchinspines may be seen in persons who have exposureto oceans and fresh ocean products. These injuries
sually raise an immediate reaction characterized by localain, burning, erythema, and edema that subside in a fewours if the spine fragments are completely removed.1,2 Inontrast, a remnant of the spine tip remaining in the woundrequently causes a delayed response, which is called searchin granuloma.3
When joints are penetrated, the inflammation may taken the form of a florid granulomatous synovitis, which can
From the Department of Orthopaedic Surgery, SapporoMedical University, Sapporo Japan; and Higashi-HokkaidoHospital, Kushiro, Japan.
Received for publication August 30, 2007; accepted inrevised form November 21, 2007.
No benefits in any form have been received or will bereceived from a commercial party related directly orindirectly to the subject of this article.
Corresponding author: Takuro Wada, MD, Department ofOrthopaedic Surgery, Sapporo Medical University,South 1, West 16, Sapporo 060-8543, Japan; e-mail:[email protected].
0363-5023/08/33A03-0017$34.00/0doi:10.1016/j.jhsa.2007.11.016
b
98 � © ASSH � Published by Elsevier, Inc.
esult in joint destruction (sea urchin spine arthritis) ifppropriate therapy is not provided in time. There haveeen 7 reports including 12 patients with respect to searchin spine arthritis of the hand.4–10 Clinical manifestation,iagnosis, and management of this pathology have not beennderstood clearly by hand surgeons. In particular, the
iterature has not described the treatment outcome in detail.We present 5 patients with sea urchin spine arthritis of
he hand due to sea urchin spine injury and discuss anppropriate treatment for this rare pathologic condition.
ATERIALS AND METHODShis retrospective study includes 5 patients (3 men and 2omen) diagnosed with sea urchin spine arthritis of theand due to sea urchin spine puncture who were treatedrom 2000 to 2004 (Table 1). Four patients were fishermennd 1 patient was involved in preparing sea urchins at aeafood company. Injuries were of the index finger in 4atients and middle finger in 1 patient. All lesions involvedhe proximal interphalangeal (PIP) joint. The mean age was7 years (range, 23 to 51 y). All 5 patients reported a searchin spine injury and had tried to remove the spine. Theatients experienced pain, swelling, and discomfort aroundhe site of puncture immediately after the injury. Thesenitial symptoms subsided within a few days. The time
etween the injury and the development of the joint
TABLE 1: Characteristics of PatientsWith Sea Urchin Spine Arthritis of the PIP Joint
PatientAge/
Gender Location OccupationPrimary
Treatment
TimeBetween
Injury andPrimary
Treatment(Mo)
DefinitiveSurgery
TimeBetweenInjuryand
DefinitiveSurgery(Mo)
HistologicType of
Granuloma
Follow-UpPeriod(Mo)
PostoperativeRange of Motion (°)
Extension Flexion
1 23/M Indexfinger
Fisherman NSAIDs,antibiotics
1 Debridement 3 Suppurative 13 10 30
2 31/F Indexfinger
Fisherman NSAIDs,antibiotics,drainage*
4 Debridementarthrodesis
10 Suppurative 24 15 15
3 43/M Indexfinger
Fisherman Antibiotics,drainage*
1 Debridementbone graft
3 Necrobiotic 24 0 100
4 37/M Middlefinger
Fisherman Antibiotics,drainage*
4 Debridement 8 Foreignbody
22 80 90
5 51/F Indexfinger
Seafoodpreparation
Antibiotics 1 Debridement 3 Sarcoid 21 0 100
NSAIDs, nonsteroidal anti-inflammatory drugs.*Drainage: limited excision with drainage and irrigation.
SEA
URCHIN
SPIN
EPUNCTURE
399
JHS
�VolA
,March

apdpe
fipadhhl
R
Pi1ocs(tjap
S
Tw
atctbpoaAoperf5
RNachisf
r(pode(s
DSb
F
ihspp
F
sac
400 SEA URCHIN SPINE PUNCTURE
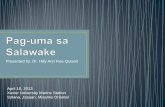
bnormalities ranged from 1 to 2 months. The secondaryhysical findings included fusiform swelling in variousegrees and limited motion of the PIP joint (Fig. 1A). Theatients reported mild to moderate pain. None of themxperienced severe pain.
All of the patients were referred cases and had receivedrst-generation antibiotics from previous doctors. Twoatients had received nonsteroidal anti-inflammatory agents,nd 3 patients had been treated with limited incision withrainage and irrigation. Painful swelling of the PIP joint,owever, persisted in all patients. At presentation at ourospitals, white blood cell count and C-reactive protein
evel were normal in all 5 patients.
adiographic Findings
lain radiographs demonstrated soft tissue swelling and osteolysisn all 5 patients. Periosteal reaction was noted in 3 patients (Fig.B). Joint space was preserved in 2 patients but was partiallybliterated in 2 patients (patients 1 and 4) and had beenompletely obliterated in 1 patient (patient 2). A spine was noteen in any of the imaging studies. Magnetic resonance imagingMRI) was available for 2 patients and showed periarticular softissue swelling. There was moderate hyperintensity inside theoint and at the space between the bone and tendons on T1-nd T2-weighted images. Abnormal signal intensity in theroximal phalanx was also noted.
urgical Technique
he average time from injury to definitive surgery by usas 5 months (range, 2 to 10 mo).
IGURE 1: Sea urchin spine arthritis of the PIP joint of the leftndex finger (patient 1). A Numerous nodules with a slightlyyperkeratotic surface on the dorsal hand. Note diffuse fusiformwelling of the index finger. B Radiographs showing osteolysis anderiosteal reaction of the proximal phalanx head. Joint space isartially obliterated.
A longitudinal skin incision was made over the dorsal T
JHS �Vol A, M
spect of the PIP joint. The extensor mechanism was split inhe midline, the dorsal capsule was excised, and the ulnarollateral ligament was released. A thorough synovectomy ofhe joint and the removal of all granulation tissue and looseone fragments when present was accomplished. In 2atients, subchondral granulation was debrided. Specimensf tissue for culture of both aerobic and anaerobic organismsnd of mycobacteria were obtained for all 5 patients.utogenous bone graft from the radial styloid was carriedut in 1 patient (patient 3). Arthrodesis was performed in 1atient (patient 2) with obliterated joint space. Follow-upvaluation ended if inflammatory signs subsided andadiographic findings and range of motion did not changeor at least 6 months. The average follow-up period for thepatients was 21 months (range, 13 to 24 mo).
ESULTSo microorganisms including aerobic and anaerobic bacteria
nd mycobacteria grew in the culture specimens. Polymerasehain reaction was also negative for mycobacteria. Theistology of surgical specimens showed giant cell granuloman all 5 patients (Fig. 2). The granuloma patterns includeduppurative type in 2 patients, necrobiotic type in 1 patient,oreign-body type in 1 patient, and sarcoid type in 1 patient.
At the final follow-up evaluation, none of the 5 patientseported pain or swelling of the affected finger. One patientpatient 2) lost PIP joint motion because of arthrodesis. Twoatients (patients 1 and 4) who had shown some obliterationf joint space in preoperative radiographs exhibitedecreased motion. The remaining 2 patients exhibitedssentially normal active motion of the affected PIP jointTable 1). There is a trend toward better outcome with ahorter interval between injury and definitive surgery.
ISCUSSIONea urchins are prickly, hard-shell marine creatureselonging to the phylum Echinodermata, class Echinoidea.
IGURE 2: Histopathology of the surgical specimen (patient 2)howing chronic granuloma associated with vascular proliferationnd infiltration of histiocytes, lymphocytes, plasma cells, and a giantell (arrow) (Hematoxylin-eosin stain; magnification �100).
he sea urchin spines are composed of calcium carbonate
arch

wivbrduftusIp
cpwhsttds
cwudsdag
tptonitrftrvssbMahl
btb
cbdm
gTo
sotAbmEf
R
1
1
1
1
1
SEA URCHIN SPINE PUNCTURE 401
ith epithelial covering.11 The covering tends to cause annflammatory reaction or possibly an immune response ofariable intensity. Two types of sea urchin spine injury haveeen described: immediate and delayed reaction. Delayedeactions may be nodular with diffuse skin lesions and areesignated sea urchin granulomas.1 The pathogenesis remainsncertain, and sea urchin granuloma was considered aoreign body reaction or an unusual immunologic responseo an as yet unidentified antigen.2,12 Although it isnknown whether calcium carbonate alone could produceuch a reaction, this problem is unique to sea urchin spines.t is also suggested that Mycobacterium marinum may play aathogenic role in some cases of sea urchin granuloma.13
Sea urchin spines occasionally cause chronic arthritis thatan result in joint destruction if appropriate therapy is notrovided in time. We found 7 reports including 12 patientsith this problem in the hand.4–10 Among them, 1 patientad amputation of the affected finger6 and 6 patients hadurgical debridement, removing the spine and granulationissue.5,7–9 The remaining 5 patients had no surgicalreatment.4,5,9,10 Although the treatment outcomes were notescribed in detail, there seems to be a trend that earlyurgical synovectomy may result in a better outcome.
All of the 5 patients described in this study were initiallyonsidered to have a possible septic arthritis and were treatedith antibiotics. Thus, it is important to recognize searchin spine arthritis and to rule out an infection. Theiagnosis of sea urchin spine arthritis is based on a history ofea urchin spine injury, a symptom-free period before theevelopment of synovitis, the absence of laboratory testbnormalities, and finally histologic evidence of a giant cellranuloma in the synovium.
Guyot-Drouot et al5 emphasized that plain radiography ishe key investigation as most sea urchin spines are opaque inlain x-rays. However, among the 12 patients reported inhe literature4–6,8–10 with inflammatory arthritis of the hand,nly 1 showed a visible spine on plain radiographs.5 Indeed,one of the 5 patients in this study showed visualized spinesn any of the imaging studies at presentation. It is likely thathe fragment of the spine remaining in the finger joint iselatively small, and delay in presentation may result inailure to show the spines radiographically as the surroundingissues absorb the calcium.14 It has been reported thatadiographic signs of arthritis due to sea urchin spine injuryary with time since the injury. Initially, joint effusion andoft tissue thickening are visible. Subsequently, osteolysis,harply demarcated bone erosion, and periosteal reaction cane seen. Liram et al4 suggested that gadolinium-enhancedRI is useful to identify some subtle changes in soft tissue
s well as bone and joint changes. In 2 of our patients, MRIelped preoperative planning by showing the precise
ocalization of the pathologic tissue.In patient 1, we left the subchondral bone defect caused
y debridement unfilled as we still suspected infection at theime of operation. Although we recommended secondary
one graft, the patient desired no further operation. As aJHS �Vol A, M
onsequence, incongruity of the joint remained. We nowelieve primary bone grafting is indicated for such a boneefect. Bone graft allows early motion, which may improveaximum recovery of range of motion.Sea urchin spine arthritis is identical to sea urchin
ranuloma of the skin in terms of giant cell granuloma.herefore, a similar problem may occur with involvementf the flexor tendon sheath.
Based on our treatment of 5 patients with sea urchinpine arthritis seen in the chronic phase of their problem andn a review of the pertinent literature, we recommend ahorough debridement of synovial and granulation tissue.ntibiotics and anti-inflammatory drugs are of little or noenefit in this problem. Temporizing with conservativeeasures seems to be of little avail and is to be discouraged.arly diagnosis and thorough synovectomy may lead to a
avorable outcome.
EFERENCES
1.Baden HP. Injuries from sea urchins. Clin Dermatol 1987;5:112–117.
2.Asada M, Komura J, Hosokawa H, Akaeda T, Asada Y. Acase of delayed hypersensitivity reaction following a seaurchin sting. Dermatologica 1990;180:99–101.
3.De La Torre CC, Toribio JJ. Sea-urchin granuloma:histologic profile. A pathologic study of 50 biopsies. J CutanPathol 2001;28:223–228.
4.Liram N, Gomori M, Perouansky M. Sea urchin punctureresulting in PIP joint synovial arthritis: case report and MRIstudy. J Travel Med 2000;7:43–45.
5.Guyot-Drouot MH, Rouneau D, Rolland JM, Solau-GervaisE, Cotten A, Flipo RM, Duquesnoy B. Arthritis, tenosynovitis,fasciitis, and bursitis due to sea urchin spines. A series of 12cases in Reunion Island. Joint Bone Spine 2000;67:94–100.
6.Cooper PP, Wakefield MMC. A sarcoid reaction to injuryby sea urchin spines. J Pathol 1974;112:33–36.
7.O’Neal RL, Halstead BW, Howard LD Jr. Injury to humantissues from sea urchin spines. Calif Med 1964;101:199–202.
8.Strauss MB, MacDonald RI. Hand injuries from sea urchinspines. Clin Orthop Relat Res 1976;114:216–218.
9.Reginato AJ, Ferreiro JL, O’Connor CR, Barbasan C, ArasaJ, Bednar J, Soler J. Clinical and pathologic studies oftwenty-six patients with penetrating foreign body injury tothe joints, bursae, and tendon sheaths. Arthritis Rheum1990;33:1753–1762.
0.Cracchiolo AA, Goldberg LL. Local and systemic reactionsto puncture injuries by the sea urchin spine and the datepalm thorn. Arthritis Rheum 1977;20:1206–1212.
1.McWilliam LJ, Curry A, Rowland PL, Watson JS. Spinousinjury caused by a sea urchin. J Clin Pathol 1991;44:428.
2.McHugh NJ, Tweed JM. Sea urchin spine synovitis. N ZMed J 1984;97:700.
3.De la Torre CC, Vega AA, Carracedo AA, Toribio JJ.Identification of Mycobacterium marinum in sea-urchingranulomas. Br J Dermatol 2001;145:114–116.
4.Newmeyer WL III. Management of sea urchin spines in the
hand. J Hand Surg 1988;13A:455–457.arch