Screening with New Modalities: Breast Ultrasound Imaging Symposium 2016... · Screening with New...
77
Screening with New Modalities: Breast Ultrasound Wendie A. Berg, MD, PhD Professor of Radiology Magee-Womens Hospital of UPMC University of Pittsburgh School of Medicine
-
Upload
vuongkhanh -
Category
Documents
-
view
214 -
download
1
Transcript of Screening with New Modalities: Breast Ultrasound Imaging Symposium 2016... · Screening with New...

Screening with New Modalities: Breast Ultrasound
Wendie A. Berg, MD, PhD Professor of Radiology
Magee-Womens Hospital of UPMC University of Pittsburgh School of Medicine

Disclosures
No personal financial conflicts of interest Philips Healthcare loaning equipment for
ultrasound clinical trial

Objectives Describe effect on cancer detection from adding
screening US to mammography or tomosynthesis in women with dense breasts
Discuss sources of false positives on screening US and ways to reduce them
Compare outcomes from different methods of screening breast US

Evidence Supporting Screening
Disease-specific mortality reduction Only studied for mammography
Reduction in node-positive disease Increase in node-negative invasive cancers
Reduction in interval cancers Fewer than 10% of all cancers diagnosed

Failure Analysis Webb ML et al Cancer 2013, epub 9/11/13 7301 invasive breast cancer dx 1990-1999 f/u 2007 609 breast cancer deaths; median age 49 yr at dx 29% ca deaths were among women screened
19% screen detected 10% interval cancers
71% deaths among unscreened women

Interval Cancer Cancer dx by clinical symptoms in interval
between recommended screenings Worse prognosis and worse outcome
~1/2 deaths in screened women diagnosed in
their 40s are due to interval cancers

Mammography Failure Analysis
#1 If not performed at all #2 High-risk women #3 Dense breasts

BI-RADS® Density
A. Almost entirely fatty B. Scattered fibroglandular density C. Heterogeneously dense which could
obscure detection of small masses D. Extremely dense, which lowers the
sensitivity of mammography


Breast Density as Function of Age
Kerlikowske et al. JNCI 2007; 99:386-395
40% of women of mammographic age have dense breasts

Masking of cancers with increasing breast density
Increased risk of developing breast cancer

Interval Cancers and Breast Density Density Odds Ratio 95% CI < 10% 1.0 - 10-24% 2.1 (0.9, 5.2) 25-49% 3.6 (1.5, 8.7) 50-74% 5.6 (2.1, 15.3) ≥ 75% 17.8 (4.8, 65.9)
p < .001 Boyd NF, et al. NEJM 2007;356:227-36

Referent “Average” Pt, Hazard Ratios
A B C D Premeno 0.46 1 1.62 2.04 Postmeno no HT 0.57 1 1.35 1.51 Postmeno E+P 0.45 1 1.58 2.09
Kerlikowske K et al J Clin Onc 2010;28:3830-3837

Increased Deaths Chiu SY et al. Cancer Epidemiol Biomarkers Prev 2010;19:1219-28
25 yr f/u Sweden 15,658 women 45-59 12.7% had dense breasts
Increased breast cancer mortality with dense breasts RR 1.91 (95%CI 1.26-2.91) Attributed to higher incidence Shorter sojourn time

www.DenseBreast-info.org 3/13/16
24 States require some sort of density notification

Possible tests to add to mammography Modality vs. Mammography alone
Absolute ↑ Cancer Detection per 1000 screens
Clinical breast exam 0.3 Double Read or CAD 1 Tomosynthesis 1-2 Ultrasound 3-4 Molecular Breast Imaging, CEDM
7-8
MRI 10 Copyright Wendie Berg, MD, PhD

Unable to Tolerate MRI: ACRIN 6666
18.5% (1 in 5.4) (95% CI 16.4 to 20.8%) women who had completed 3 years of screening with US and mammography were unable to undergo an MRI
Berg WA et al. Radiology 2010;254:79-87

Ultrasound
No radiation Not limited by dense tissue No injection of contrast or radioactive
material Inexpensive

US to Replace Mammo? Berg WA et al JNCI 2016; 108, epub 12/18/15 111 breast ca dx among 2809 women ACRIN 6666 129 US to detect one cancer, 127 for mammo Of 89 invasive cancers, 53 (60%) seen on US vs. 41
(46%) on mammography, p = .11 More likely node negative when found by US: 34/53
(64%) vs. 18/41 (44%), p = .003

US but not Mammo Inv Ca Detection Density, % US Mammo US, not
Mammo ≤ 25 0/1 (0) 0/1 (0) 0/1 (0) 26-40 6/10 (60) 6/10 (60) 2/10 (20) 41-60 16/30 (53) 17/30 (57) 8/30 (27) 61-80 22/36 (61) 13/36 (36) 14/36 (39) >80 9/12 (75) 5/12 (42) 6/12 (50) P trend .23 .19 .06
Berg WA et al JNCI 2016; 108, epub 12/18/15

False Positives Over 3 Years US Mammo P-value
Recall Rate 515 (10.7%) 453 (9.4%) .03 Biopsy Rate 266 (5.5%) 97 (2.0%) <.001 PPV Biopsies 31/266 (11.7%) 37/97 (38.1%) <.001
Berg WA et al JNCI 2016; 108, epub 12/18/15

US and Mammo Complementary
Of 22 DCIS, 18 (82%) seen on mammography vs. 5 (23%) on US, p=.002
Sensitivity of mammography + US 0.76 (0.65-0.85) vs. 0.52 (0.40-0.64) mammo alone (p < .001)
Berg WA et al JAMA 2012;307:1394-1404

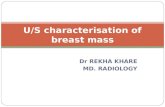
48F screening
Courtesy Dr. Wei Yang, MD Anderson

RT CC MAG RT ML MAG Courtesy Dr. Wei Yang, MD Anderson

Stereotactic biopsy: High nuclear grade DCIS solid type with comedo necrosis, with microinvasion, ER, PR-, HER2 +
Skin-sparing mastectomy, 0/4 SLN

Supplemental US
Physician Performed Technologist Performed Automated

Handheld US High-frequency transducer, 12-18 MHz linear array Survey scanning transverse and sagittal Document 1 image per quadrant, 1 behind nipple for
negative exam Lesions (all studies to date): Orthogonal views ±
calipers; optional color or power Doppler image Positive test: BI-RADS 3 or higher assessment, or
recommendation for further imaging (BI-RADS 0)

Author N screens
ICDR per
1000
Recall Rate (%)
Bx Rate (% women)
PPV3 Bx Performed
Corsetti 9157 4.0 NS 449 (4.9) 50/623 (8.0)
Berg yr1 2659 5.3 401 (15.1) 207 (7.8) 14/264 (5.3)
Berg yr2-3 4841 3.7 356 (7.4) 242 (5.0) 21/276 (7.6)
TOTAL 16,657 4.4 10% 898 (5.4) 85/1163 (7.3)
Physician Performed US: Multicenter Results
4.9% of women had biopsies for benign findings

Tech-Performed US (USA): Prevalent Screens
Author N ICDR per 1000
Recall Rate (%) Bx Rate (%) PPV3 Bx Performed
Kaplan, 2001 1,862 2.7 176 (9.5) 97 (5.2) 6/96 (6.3)
Hooley, 2012 648* 4.6 154 (23.8) 46 (7.1) 3/58 (5.2)
Weigert, 2012 8,647 2.8 1,196 (13.8) 429 (5.0) 25/418 (6.7)
Parris, 2012 5,519 1.8 680 (12.3) 185 (3.3) 10/181 (5.5)
Overall 16,676 2.5 2,206 (13.2) 757 (4.5) 47/753 (6.2)
*analysis presented for women with negative screening mammograms
Berg WA and Mendelson EB. Radiology 2014;272:12-27

Recalls: Tech-Performed HHUS 2,206/16,676 (13.2%) test positive on prevalence
screen 1,399 (8.4%) all women BI-RADS 3 757 (4.5%) all women BI-RADS 4
44/753 (5.8%) found to have cancer Only 43/16,676 (0.3%) recalled for additional
evaluation (BI-RADS 0) prior to final assessment
Berg WA and Mendelson EB. Radiology 2014;272:12-27

Disease Prevalence Affects Yield
Moderate Risk* No Known Risks P-value
Kolb 2002 14/2914 (4.8 per 1000) 14/7901 (1.8 per 1000) .011
Crystal 2003
4/318 (12.5 per 1000) 3/1199 (2.5 per 1000) <.04
Overall 18/3232 (5.6 per 1000) 17/9100 (1.9 per 1000)
*Personal hx of breast cancer or first-degree relative with breast cancer vs. no risks

Japan Tohno E et al Breast Cancer 2012;19:138-146 2-day educational program; results of
training/testing for 415 technologists and 422 physicians
Observers worse with experience < 100 cases Video sensitivity, still image sensitivity, and
disease agreement for technologists > for MDs

Node-Negative Invasive Cancers
Across 10 series, 475 cancers seen only on US, 415 (87.4%) invasive
273/303 (90.1%) with staging were node negative
22/91 (24%) ILC

By Participant, Yield/1000, ACRIN 6666
Year M+US M Supp. Yield, 95% CI P-value
1 12.8 7.5 5.3 (2.1, 8.4) .0001
2 10.0 6.4 3.6 (0.9, 6.4) .004
3 13.8 9.9 3.9 (0.9, 6.8) .004
Supplemental yield of US is significant each year and similar for incidence and prevalence screens
Berg WA et al JAMA 2012;307:1394-404

Weigert: Recalls Incidence Screens
Year 1 8647 (12%) women screening US Recall rate 13.8% (n=1196): 767 (8.9%) BR 3; 429
(5.0%) BR 4,5; PPV3 5.6% 24 cancers, CDR 2.8 per 1000
Year 2 10,282 (17.9%) women Recall rate 12.7% (n=1310); CDR 2.3 per 1000 (24)
Year 3 4128 (12.8%) women Recall rate 7.7% (n=316); CDR 2.7 per 1000 (11)

Courtesy WP Evans, III, MD
60F, 5-yr risk 2.5%, 24-mo US: 12 mm grade 1 IDC-DCIS, N0
Radial Antiradial

Courtesy Gary Whitman, MD, MD Anderson
75F personal hx Lt cancer 17 mm grade 3 IDC-DCIS, N0 Seen only on 24-month US Seen in retrospect on mammo
Radial Antiradial

70F personal hx rt mastectomy, BRCA-1 mutation carrier 24 mo screen US+ 19 mm grade 3 IDC-DCIS, N0
Courtesy Dr. Mary Mahoney, U Cincinnati

ACRIN 6666: Breast Density Density n Yield per 1000 P-value
≤ 25% 124 0 26-40% 785 6.4 .026 41-60% 2314 3.0 .008 61-80% 2807 4.3 .0006 >80% 1443 5.5 .005
Berg WA, et al., RSNA 2009

Interval Cancer Rate: ACRIN 6666
Yr N Interval N Cancers (%) 1 2 36 5.6 2 4 29 14 3 3 46 6.5
All 9 111 8.1
Interval Ca Rate: 9/7473 screens = 1.2 per 1000 8% of all cancers
Berg WA et al JAMA 2012;307:1394-404

Interval Cancer Rate Italy
Corsetti V et al Cancer 2011;47:1021-6 Interval cancer rate in fatty breasts
1.0 per 1000
Interval cancer rate in dense breasts after adding screening US 1.1 per 1000

J-START Ohuchi N et al Lancet 2015, epub 11/4/2015 Asymptomatic women aged 40-49 at 42 sites Randomized to M+US or M alone twice in 2 yrs 36,869 to intervention and 36,139 to control
group

Results J-START first round Intervention Control P-value
Sensitivity 91.1 (87.2-95.0) 77.0 (70.3-83.7) .0004
Specificity 87.7 (87.3-88.0) 91.4 (91.1-91.7) <.0001
% Stage 0, I 144/184 (71.3) 79/117 (52.0) .019
Interval Cancers 18 (0.05%) 35 (0.10%) .034
Ohuchi N et al Lancet 2015, epub 11/4/2015

Time to Perform US: ACRIN 6666
Bilateral scan, not including time discussing results with patient nor creation of report
Year Median (min) Mean SD 1 17 19.2 11.9 2 15 16.7 10.4 3 13 14.7 9.2

Reducing False Positives BI-RADS 3 lesions
Prevalence of 15-20% of all patients having screening US in prior series (Barr et al; Hooley et al; Chae et al)
Across all series, only 1 lesion had suspicious change yielding malignancy at 6-mo follow-up
12-month follow-up reasonable


Orthogonal Views
Required for any mass for which future comparison is desirable Not necessary for simple cysts
Incomplete characterization without this

RAD ARAD
Berg WA and Mendelson EB Radiology 2014;262:309-315 Courtesy Dr. Christophe Tourasse
53F Papillary DCIS with microinvasion

Berg WA and Mendelson EB Radiology 2014 2014;262:309-315
50F invasive ductal carcinoma; echogenic rim in arad view only

Cysts ACRIN 6666 1255/2662 (47.1%) women over the three years
998 (37.5%) of 2659 year one 537/1363 (39.4%) post-menopausal participants, had cysts
73 using estrogen replacement 48 (66%) had cysts
1290 no HRT 489 (37.9%) had cysts (p<.0001, less common)
516/793 (65.1%) premenopausal women had cysts (p<.0001)
Berg WA, et al Radiol Clin N Amer 2010;48:931-987

Complicated Cysts ACRIN 6666 376 (14.1%) of 2662 participants
301 (80%) had at least one simple cyst 84 (22%) multiple, bilateral
Overall 2/475 (0.42%) such lesions malignant
Berg WA, et al Radiol Clin N Amer 2010;48:931-987

Complicated Cysts N N Malignant (%)
Kolb et al 1998 126 0 Venta et al 1999 308 1 Buchberger et al 1999 133 0 Berg et al 2003 38 0 Chang et al 2007 35 0 Daly et al 2008 228 1 ACRIN 6666 475 2 TOTAL 1343 4 (0.3)
Berg WA et al Radiol Clin N Amer 2010,48:931-987

Cyst or Solid?
Radial Antiradial 53F incidental finding on US, aspirated, cytology: benign cyst with apocrine cells

Radial Antiradial 51F strong FH, incidental finding on US Aspirated to resolution, thick cloudy yellow fluid, cyst

61F with new mass on mammography, prior ipsilateral cancer

Radial Antiradial
12 month follow-up US enlarged: 14-g US-guided bx papillary DCIS

BI-RADS 3
Chae EY et al AJR 2016;206:666-672 With mammographic abnormality, 4/184
(2.2%) malignant Without mammographic abnormality,
4/980 (0.4%) malignant (p=.025)

Clustered Microcysts 3.9 to 5.8% of US examinations 1/235 (0.4%) malignant across 5 series Mean age 48 years (32-71) Short-interval follow-up if uncertainty Caution if new mass on mammogram, post-menopausal
woman not on HRT May merit biopsy
Berg WA AJR 2005;185:952 Berg WA, et al Radiol Clin N Amer 2010;48:931-987

48F new mass on screening mammogram

60F ipsilateral cancer elsewhere US-guided core biopsy DCIS, intermediate grade

Lesions Synchronous to New Cancer
Kim SJ et al AJR 2008;191:653-8 55/482 (11.4%) BI-RADS 3 lesions
malignant 36/170 (21.2%) in same quadrant as 1º 12/122 (9.8%) in different quadrant 8/190 (4.2%) in contralateral breast

M-B Circumscribed Masses: US Berg WA et al Radiology 2013:268:673-683 2172 women in ACRIN 6666 135 (6.2%) participants had 153 unique findings
described as M-B masses on screening US over 3 annual screens 98 complicated cysts with debris 43 solid, circumscribed, oval masses 7 solid masses with 2-3 lobulations 5 clustered microcysts
No malignancies (95%CI up to 2.4%)

Billing
CPT codes 76641, unilateral complete right 76641, unilateral complete left Medicare reimbursement averages $165 Subject to deductible and copays

Billing
ICD-10 92.2 “Inconclusive mammogram” Applicable to dense breasts, NOS Inconclusive mammogram due to dense
breasts
http://www.icd10data.com/ICD10CM/Codes/R00-R99/R90-R94/R92-/R92.2

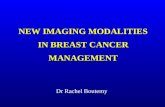
A – Tower B – Y-axis Gantry & Transducer Carrier C – X-axis Gantry D – Ultrasound Machine Monitor E – Touch Screen / Monitor F – Transducer Holster G – Patient Bed
Automated Arm US

Automated Arm Results Kelly KM et al Eur Radiol 2010; 20:734-742 4419 women, 6425 exams, 8 facilities
40% women at ≥ intermediate risk 23 cancers mammography 46 cancers M+US Supplemental yield 3.6 per 1000 (95% CI 2.3 to 5.4) 10% recall rate 23/75 (31%) biopsies showed cancer

Automated Breast US 12 MHz 15 cm footprint 3 acquisitions per
breast in ~15 minutes 3D dataset
Transverse Created coronal and
sagittal displays


ABUS Results Brem RF et al Radiology 2015;273:663-673 15,318 women BI-RADS 1 or 2 mammo, dense breasts,
automated whole breast US 30 (2/1000) cancers only by ABUS 25 detailed: 23 (92%) invasive, mean size 13 mm, 18
(78%) of those N0 20/23 (87%) ER+ 3/22 (14%) stage IIB or higher 13% absolute increase in recall rate—immediate
additional evaluation, not a final assessment

HHUS vs. AUS HHUS AUS
Time to acquire images 13 min (but range up to 90)
15 min
Training to “ “ Yes, months, technologist
Minimal
Sensitivity ~85% ~74% Number of images 5-20 1000-1700 Time to interpret < 30 sec 5-10 min Recalls 13%
Final assessment typically rendered
13% Incomplete, needs
targeted US Interobserver Variability Κ = 0.53 (SE 0.02) Κ = 0.04 to 0.50

Is screening ultrasound still of benefit after tomosynthesis?

ASTOUND trial Tagliafico AS et al JCO 2016;epub 3/9/2016 3231 women with dense breasts, negative mammogram,
5 centers in Italy DBT 13 cancers (ICDR 4.0/1000 95%CI 1.8 to 6.2) US 23 cancers (ICDR 7.1/1000, 95%CI 4.2 to 10.0,
p=0.006) False positive recall DBT 53 vs. US 65 (p=0.26)

DBTUST study UPMC Pittsburgh UPMC Hamot, Erie Weinstein Imaging 6200 women DBT and technologist-performed
screening US each year for three years NIH and PABCC funding

Three-Step Implementation
1) Does the woman have at least 10-yr life expectancy? No, then CBE only, with mammography only if
warranted by symptoms

2) Is the patient at “high risk” for breast cancer and under age 70? Yes, then MRI annually beginning:
When ascertained to be high risk Age 25 if BRCA1/2 or other pathogenic mutation 8yr after chest XRT if XRT before age 30
If unable to tolerate MRI, then US

3) Dense? Yes: Supplement annual mammography with
US beginning at age 40-45 No: Tomosynthesis beginning at age 40-45

Mam+US
Mammo
MRI