
Screening Drug Quality Project Report March 2014 - WHO · Screening Drug Quality Project Report ......
27
i Screening Drug Quality Project Report – March 2014
Transcript of Screening Drug Quality Project Report March 2014 - WHO · Screening Drug Quality Project Report ......

i
Screening Drug Quality Project Report – March 2014

ii
Executive Summary
The proliferation of substandard medicines globally has become a public health concern. The scenario is even
worse in sub Saharan African countries which have weak systems of governance and regulation. Despite all
the strategies implemented by the Uganda Ministry of Health, anecdotal evidence shows that counterfeit and
substandard medicines are still prevalent in the Ugandan market. Given the high prevalence of infectious
diseases in the Ugandan population, the dealers in this business target antimicrobial medicines and distribute
them to remote and peripheral areas of the country. Because of the complexity of assuring quality in resource
limited settings, it has been advocated that drug regulatory authority activities are augmented by screening
drug quality programs run in such a manner as to collect accurate information that better represents the quality
of medicines made available to the consumers. Therefore, this drug quality screening project was conducted as
an innovation where the Drug Regulatory Authority cooperates with other stakeholders as an additional
dimension to drug quality assurance in a country such as Uganda with limited capacity.
It was a field based project employing a cross sectional design. Medicine samples of co-trimoxazole 480mg
and 960mg tablets, ciprofloxacin 500mg tablets, amoxicillin 250mg or 500mg capsules and
artemether/lumefantrine 20/120mg tablets were collected from a stratified random sample of drug outlets in
Mbarara, Arua and Iganga/Mayuge districts. The screening of drug quality was conducted in the
Pharmaceutical Chemistry Laboratory at Pharmacy Department in Makerere University using GPHF Minilabs.
Samples for screening drug quality were picked from a total of twenty nine (29) drug outlets from three
regions of Uganda. Each region contributed almost an equal number of outlets to the total sampled units with
the lowest being South West with eight (8) drug outlet and the highest being West Nile with eleven (11) drug
outlets.
All categories of drug outlets including wholesale pharmacies, retail pharmacies, drug shops, clinics, public
health facilities and informal drug outlets were represented in the sampled drug outlets.
Up to 105 drug products of the selected medicines were collected from the sampled drug outlets. These
included 31 samples of Artemether/Lumefantrine 20/120mg tablets, 25 samples of Amoxycillin 250mg or
500mg capsules, 24 samples of ciprofloxacin 500mg tablets and 25 samples of Cotrimoxazole 480mg or
960mg tablets. Consequently, 136 screening tests were conducted on all the samples of medicines.
Of all the sampled products, only Amoxycillin 250mg or 500mg capsules had some failures (5/25 samples) on
the screening tests. These products failed on the identity test as the sample spot intensity was different from
the standard spot intensity. All the other products of Artemether/Lumefantrine 20/120mg tablets,
Ciprofloxacin 500mg tablets and Co-trimoxazole 480mg or 960mg tablets passed the screening tests.
The failed Amoxycillin capsule products were forwarded to NDA Quality Control Laboratory for verification
and confirmatory tests.
iii
Acknowledgements
The Project implementation team is greatly indebted to the following;
MeTA Council Uganda Chapter for the trust and confidence they showed in assigning this task to the
project team.
MeTA Secretariat for all the effort, time, encouragement and follow up on the project progress and
most importantly for their tireless appraisal of progress and kind reminders.
World Health Organization, Uganda Office and HEPS Uganda for the effort in supervising and
evaluating the project, also providing appropriate administrative structures for conducting the
screening drug quality project.
Representatives from National Drug Authority Headquarters, Quality Control laboratory, Regional
Drug Inspectors, District Drug Inspectors and the people at the drug outlets who interacted with
members of the project implementation for their dedicated commitment, support, advice and
cooperation to ensure that the project succeeded.
And finally, the International MeTA Secretariat and DFID for providing financial support towards
purchase of the GPHF Minilabs and operational costs of implementing the project. This project would
not have been possible without that support.

iv
Table of contents
Executive Summary ............................................................................................................................................. ii Acknowledgements ............................................................................................................................................. iii Table of contents .................................................................................................................................................. iv 1. Introduction ....................................................................................................................................................... 1 2. Background ....................................................................................................................................................... 1 3. Justification ....................................................................................................................................................... 1 4. Objectives ......................................................................................................................................................... 2
4.1. Specific Objectives .................................................................................................................................... 2 5. Methods and materials ...................................................................................................................................... 2
5.1. Design ........................................................................................................................................................ 2 5.2. Study medicines ......................................................................................................................................... 2 5.3. Sentinel districts/sites................................................................................................................................. 3 5.5. Sampling, sample size and sampling plan ................................................................................................. 4 5.7. Sampling locations ..................................................................................................................................... 5 5.8. Data collection ........................................................................................................................................... 5 5.9 Packaging, labeling, transportation and storage of samples ....................................................................... 6 5.10 Summary of sample handling processes ................................................................................................... 7 5.11 Sample analysis ......................................................................................................................................... 8 5.12 Ethical issues ............................................................................................................................................. 8 5.13 Use of study results ................................................................................................................................... 8
6.0 Results of the Screening Tests ........................................................................................................................ 9 7.0 Conclusion .................................................................................................................................................... 15 Annex 1: Testing Methods, Procedures and Testing Data Reporting ................................................................... 16 Annex 2 Checklist for Sentinel Site “Drug Testing” Personnel .......................................................................... 18 Annex 3: Sentinel Site Drug Sample Collection and Testing Report Form........................................................ 19 Appendix 2: General Rules for Interpreting TLC Results ................................................................................... 22 8. References ....................................................................................................................................................... 23
1
1. Introduction
The Medicines Transparency Alliance (MeTA) is a DFID initiative that brings together public, private and
civil society stakeholders with an interest in the outcomes of the medicines market. MeTA aims to increase
transparency in the medicines market specifically in low- and middle-income countries, thereby strengthening
healthcare governance and encouraging responsible business practice.
MeTA Uganda conducted a quality assessment project on four selected medicines including Co-trimoxazole,
Amoxycillin, Ciprofloxacin and Artemether/Lumefantrine tablets to augment efforts of the National Drug
Authority in curtailing sale of poor quality medicines to the population. The project was implemented by
Makerere University Department of Pharmacy in collaboration with the National Drug Authority.
2. Background
Health care professionals and patients assume that the medicines they use are of good quality, but recent
reports indicate that substandard and counterfeit medicines are widely available, especially in countries with
resource constraints, inadequate regulations and shortage of human resources for health. The Uganda Health
system like other developing countries is over-stretched with over-whelming disease burden and limited
resources to fund ever increasing drug needs. The health worker crisis has been worsened by brain. All these
factors affect the impact of efforts implemented to ensure safe, quality and efficacious pharmaceuticals are
accorded to the populace.
The task of ensuring quality medicines in Uganda is the mandate of Uganda National Drug Authority. It is
directed by law, to ensure the quality, safety, and efficacy of all pharmaceutical products marketed in Uganda
in addition to cosmetics, chemical devices and household chemicals. Once a product has been granted
marketing authorization by the NDA Board, the quality of consequent batches of the product either locally
manufactured or imported is to be assessed regularly. Currently, the National Drug Authority conducts for-
cause testing of all anti-retroviral drugs, anti-malarial drugs, anti-tuberculosis drugs and condoms. Other
pharmaceutical products are analyzed on a needs basis.
Despite all the strategies implemented by the Uganda Ministry of Health, anecdotal evidence shows that
counterfeit and substandard medicines are still prevalent in the Ugandan market. Given the high prevalence of
infectious diseases in the Ugandan population, the dealers in this business target antimicrobial medicines and
distribute them to remote and peripheral areas of the country. Because of the complexity of assuring quality in
resource limited settings, it has been advocated that drug regulatory authority activities are augmented by
screening drug quality programs run in such a manner as to collect accurate information that better represents
the quality of medicines made available to the consumers. Such interventions should be adapted to the reality
in the field of each sentinel site, taking into consideration the availability of human and financial resources, all
the logistics required for sampling and testing drugs, and most importantly the close collaboration between
the critical stakeholders in the ensuring a healthy population. Therefore, the drug quality screening project was
conducted with this view mind so as to add another dimension to drug quality assurance in a country such as
Uganda with limited capacity.
3. Justification
The quality of medicines is a topic of global concern. Hence, monitoring the quality of all essential medicines,
once they are on the market is a high priority for the Ministry of Health. Testing is the only way to check
quality of marketed medicines. Ministry of Health and National Drug Authority has made tremendous advance
in improving the quality of medicines available to the Ugandan population. However, there is incongruence
between human and financial resources available to them versus the scale of geographical area and medicine
quality control activities to cover that some substandard and counterfeit pharmaceuticals end up in the

2
distribution chain. As a result, the screening drug quality project was proposed by MeTA Uganda as a
pragmatic strategy to augment existing regulatory and oversight infrastructure of the Uganda Ministry of
Health and National Drug Authority.
Furthermore, it was prioritized in this project that some pharmaceutical distributors in Uganda are supported to
establish or strengthen drug quality assessment and monitoring systems in their practice. The strength of such
an arrangement lay in the fact that it permits an independent and neutral external quality assurance mechanism
while building capacity of drug quality assurance in the private sector pharmaceutical distributors.
4. Objectives
To improve the quality of medicines accessed by populations in the rural areas of Uganda by
employing innovative drug quality surveillance process.
4.1. Specific Objectives
To determine the proportion of the sample medicines that has not been granted marketing
authorization by the National Drug Authority.
To screen selected drug products using the Minilabs so as to identify suspicious medicine products
To establish a mechanism of sharing information about quality of medicines between reputable
pharmaceutical distributors and the Drug Regulatory Authority.
5. Methods and materials
5.1. Design
It was a field based project employing a cross sectional design. Medicine samples of co-trimoxazole 480mg
and 960mg tablets, ciprofloxacin 500mg tablets, amoxicillin 250mg or 500mg capsules and
artemether/lumefantrine 20/120mg tablets were collected from a stratified random sample of drug outlets in
Mbarara, Arua and Iganga/Mayuge districts.
5.2. Study medicines
Tracer products of co-trimoxazole 480mg tablets, ciprofloxacin 500mg tablets, amoxicillin 250mg or 500mg
capsules and artemether/lumefantrine tablets were selected through an extensive multi-stakeholder
consultative process involving MeTA Council and the Drug Regulatory Authority. Further explanation about
the choice of medicines is provided below;
1. Antimalarial medicine; Artemether/Lumefantrine is recommended as the first line medicine for treatment
of uncomplicated malaria in the National Malaria Treatment Policy. Malaria causes significant
proportion of disease burden in Uganda and hence the antimalarials market was considered by the project
team as a good target for unscrupulous suppliers of poor quality medicines.
2. Antibacterial agents including Amoxicillin capsules, Co-trimoxazole tablets and Ciprofloxacin tablets.
Amoxicillin is widely used for conditions that have a high prevalence in Uganda such as pneumonia in
children and other bacterial respiratory infections. Co-trimoxazole is also used for bacterial respiratory
infections, enteric infection and primary prophylaxis in HIV/AIDS victims. Ciprofloxacin is used to treat
the deadly Salmonella typhi infection and urinary system infections. Because of the high prevalence of
conditions in which these medicines are used, there is high affinity for supplying poor quality medicines
and the potential negative impact of distributing sub-standard products is significant.

3
All the brands of the study medicine/formulation available at the sampled drug outlets in the sentinel
districts during the study period were collected and assessed.
5.3. Sentinel districts/sites
Sentinel districts were selected basing on information about high risk areas for poor quality medicines. In
consultation with NDA, districts that were considered major beneficiaries of unregulated ports of entry of
medicines into the country were prioritized for the first phase of this drug quality surveillance project. The
sentinel districts included in this phase/ sampling round of the project were;
Arua which is located in West Nile at a corner border point among Uganda, Southern Uganda and
Democratic Republic of Congo.
Iganga/Mayuge district which are major destinations and market for medicines that are smuggled across
lake Victoria from Kenya and Tanzania
Mbarara district which is located in the South West of Uganda. It serves as a gate way to the South West
and parts of the Western Uganda.
Within each sentinel district, the District Health office (DHO) was the point of entry and planning for
collection of data and samples in that district. Once the DHO had been briefed on the nature and approach of
the project, he delegated the District Drug Inspector to work with the consultant in planning the sampling of
drug outlets and eventual collection of medicine samples. All this was done with the knowledge of the
Regional NDA Inspector who had been contacted earlier.
The study team assumed that the District Drug Inspector was a person who was knowledgeable about the
various drug outlets that acted as sources of medicines for the population.
The study team designed this component/aspect of data collection so that the community of drug outlets did
not link the data collectors to the National Drug Authority. Any association of the data collectors and study
team with the National Drug Authority would render it difficult to collect samples of study medicines from
informal drug outlets.
The starting point for sampling was the following; for Mbarara, Iganga and Arua, the main or biggest public
hospital in the area, i.e. Mbarara Regional referral hospital, Iganga hospital and Arua hospital respectively.
Within the sentinel districts, drug outlets were categorized into formal and informal facilities.
The formal facilities were further be grouped into public health facilities, private pharmacies, private drug
shops, and clinics. Once the list of potential sample collection sites was obtained, the study team proceeded to
randomly select which facilities to use as sampling sites; two facilities of each category.
Table 1. Sampling frame for each category of facilities in Iganga/Mayuge and Arua districts
S.No Drug Outlet Total Number of Facilities
Iganga/Mayuge District
1 Public Health Facilities (Hospitals & HC IV) 2
2 Pharmacies 12
3 Drug shops 145
4 Clinics 25
5 Informal outlets (estimate) 30
Arua
1 Public Health Facilities (Hospitals & HC IV) 1

4
2 Pharmacies 7
3 Drug shops 45
4 Clinics 33
5 Informal outlets (estimate) 30
5.5. Sampling, sample size and sampling plan
5.5.1 Sampling and selection of drug outlets per category in the districts
Iganga / Mayuge
Two public health facilities were studied; Mayuge HC III and the Iganga Hospital. This was to represent the
urban and rural health facilities. The available trace drugs were collected from the centres. Mayuge district had
only one wholesale pharmacy, which was conveniently included in the sample. Other pharmacy outlets were
randomly sampled using labelled papers put in a polythene bag. Three were selected to represent wholesale
and retail outlets.
The drug shops were selected from both districts. Random sampling was done to identify each with one from
each district. Only one clinic had the tracer medicines needed in their original packs. Most did not either have
the medicines or the quantities needed were not enough in their original pack. The informal outlets did not
have the required medicines and therefore could not avail any samples for our study.
Arua
There is only one public health facility (Arua Regional Referral Hospital) situated in Arua town along the busy
Arua Main avenue. This facility was chosen to represent the public sector.
A total of seven (7) pharmacy outlets are in the district town centre, 2 are exclusively wholesalers and the
others (5) conduct both wholesale and retail business activities. The two wholesalers were conveniently
included in the sample, whereas two others were randomly sampled to represent the retailers. The names of
five pharmacy outlets were written on small pieces of paper folded and put in a polythene bag and mixed. Two
papers were randomly picked for the study.
Drug shops are spread across the district with most being in shopping centres and towns. Most are under
stocked and could not provide the required drug samples needed for this study. One registered drug shop was
identified and provided the drug samples. Similarly two clinics were sampled from the registered total, and we
took samples from one of them.
The informal outlets number was an estimate, since all are not know by the authorities. We did not have a
sampling frame for them. They were identified randomly during the movement to other drug outlets. One drug
shop and two clinics were able to avail the trace drugs we were interested in.
5.5.2 Sample size and sampling plan
The sampling strategy took into consideration the following; different lots, different regions, different
categories of drug outlets and all available sectors.
A sample consisted of a number of tablets/capsules of the same manufacturing batch collected at the same
collection site.
A sample was made of: a) three sets of at least 60 tablets (or capsules) each or b) the number of sealed
packages that is necessary to make three sets of at least 60 tablets or capsules each.
Hence, sample size was three sets of at least 60 units from the same lot number, same location/outlet; except if
fewer units are found.

5
A sample of all branded and/or generic presentations (i.e. same product name, same manufacturer, same
dosage form, same package size, same packaging material and same strength) of the selected medicines
available at each sampling site was collected. All administration units (e.g. tablet, capsule) of one sample were
of the same batch or the same dispensing container in the case of loose items.
5.7. Sampling locations
Convenience sampling was used based on following principles;
Sectoral coverage – public and private, formal and informal; give priority to following order;
wholesalers or distributors, pharmacies, retail drug outlets, hospitals and clinics.
Geographical coverage – urban, suburban and rural areas within the sentinel site areas
Main route/ flow of drug supply or distribution or circulation route of medicines and how it affects
physical access.
Common drugs and preparations from different brands, sources of manufacture, lots/batches of
artemether/lumefantrine 20/120mg, ciprofloxacin 500mg, amoxicillin 250mg and 500mg and co-
trimoxazole 480mg and 960mg.
5.8. Data collection
All samples were collected between August 29th and November 10
th 2013 from the sentinel district agreed
upon by the Study Steering Committee. Samples were sent to the testing site (Makerere University Pharmacy
Department, Pharmaceutical Chemistry laboratory) as soon as possible.
Sample collection
The study team collected up to 3 samples (cumulative) of each of the tracer medicine products; ensuring, as far
as possible, that a) all surveyed medicines and b) all circulating batches were represented while ensuring that
all units of one sample were of the same batch. If this was not possible, then less than 3 samples were sent for
testing.
The data collectors filled out the following form;
Sentinel site drug sample collection and testing report form
Additional precautions for sample collection
Sampling form was properly filled out and safely attached to sample container
The medicine samples were kept/stored according to manufacturer’s recommended storage conditions
The samples were managed in such as a manner as to allow traceability of the sample source; where
possible samples were left in their original container or package with drug label.
Arrangements were made to ensure replacement or purchase of samples collected at sampling sites,
when necessary.
Sample coding and labelling
In order to avoid confusion each sample was assigned a unique code number for identification and traceability.
This code included the sentinel district name, type of facility/drug outlet, generic name, sampling date and a
sequential number of the sample, as follows;
District name: AR for Arua, IG for Iganga, MB for Mbarara,
Type of drug outlet: Formal, F; Public Health facility: PHF
Informal I; Pharmacy, PHA
Drug shop, DS
Clinic, CL

6
Generic name of medicine (INN): AL, AM, CI, CO
Sampling date: DD-MM-YY
Sample sequential number: from 01 to 99.
E.g. for the first sample of Artemether/Lumefantrine collected in Arua on 10 August 2013, from public health
facility, the code would be: AR-PHF-AL-100813-01
Whenever it was necessary to collect more than one original package in order to obtain the required number of
units, all original packages were marked with the appropriate sample code.
Sample envelopes were labelled mentioning the sample code number as well as the generic and trade
name of each product.
Information collected
The product details were indicated for each sample collected in the Sample Collection Form, see Annex
3.
At the end of sampling the technical consultant informed the study team to organize the validation of
sampling, i.e. the verification of the samples collected (quantity, appropriateness, and suitability for
sending to testing facility) and completeness and accuracy of documentation that accompanies samples.
5.9 Packaging, labeling, transportation and storage of samples
Whenever possible such as blister pack preparations, the samples were picked in their original packaging and
labeling. The sampling form was filled out and attached to drug sample. The container or plastic bag used was
sealed, tamperproof/tamper-evident and appropriately labeled. Precaution was taken to prevent contamination,
adulteration and deterioration due to light, air and moisture. The drug samples were kept at the manufacturer’s
recommended storage conditions found on the label. Protection during transportation was done by filling the
container with cotton batting or other suitable material. Once a sample container was opened by the analyst,
the individual responsible would initial and date it.
7
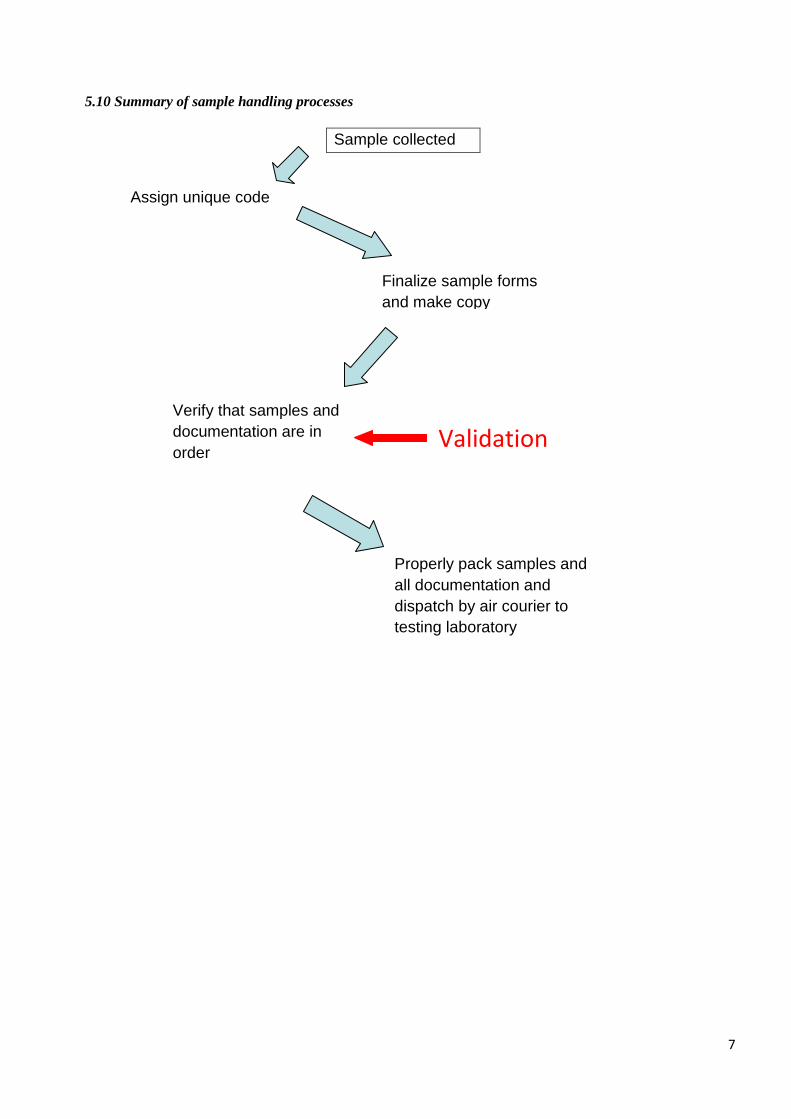
5.10 Summary of sample handling processes
Sample collected
Assign unique code
Finalize sample forms
and make copy
Verify that samples and
documentation are in
order
Properly pack samples and
all documentation and
dispatch by air courier to
testing laboratory
Validation
8
5.11 Sample analysis
After validation, samples were sent (see sample transportation below) to the Pharmaceutical Chemistry
Laboratory at Pharmacy Department, Makerere University.
Testing was done as explicated in Annex 1.
5.12 Ethical issues
No ethical issues should arise: quantities sampled were too small to affect availability of needed medicines or
viability of businesses where sampling takes place.
5.13 Use of study results
Due to the sensitive nature of drug quality monitoring and possible conflicts of interest, NO DATA or
RESULT of any preliminary or initial test data obtained at the sentinel sites will be shared with or disclosed to
third parties until it has been verified and discussed among the relevant authorities or agencies concerned
(NDA, MoH, respective distributor), and if applicable with WHO.

9
6.0 Results of the Screening Tests
Samples for screening drug quality were picked from a total of twenty nine (29) drug outlets in the three
sentinel districts selected for the screening project.
Figure 1. Distribution of drug outlets by Sentinel Region
Each region contributed almost an equal number of outlets to the total sampled units with the lowest being
South West with eight (8) drug outlet and the highest being West Nile with eleven (11) drug outlets.
Figure 2. Number of drug outlets per category in the total sampled units
The majority of the sampled drug outlets were wholesale pharmacies followed by drug shops/clinics. The
fewest drug outlets were public health facilities.

10
Table 2. Number of drug outlets by category in each sentinel region
Category of drug outlet No. of Outlets per Sentinel Region Total
West Nile South West East Central
Wholesale Pharmacy 2 3 3 8
Retail Pharmacy 2 1 2 5
Drug shop & Clinics 2 2 3 7
Informal Outlets 4 2 0 6
Public Health Facilities 1 0 2 3
Total 11 8 10 29
All categories of drug outlets were represented in the sampled drug outlets.
Table 3. Number of each drug product by category of drug outlet in each sentinel region
Drug outlet Artemether/Lumefa
ntrine 120/20mg
Amoxycillin 250mg
or 500mg
Ciprofloxacin
500mg
Co-trimoxazole
480mg or 960mg
WN SW EC WN SW EC WN SW EC WN SW EC
Wholesale Pharmacy 1 7 3 2 3 3 1 3 3 2 4 3
Retail Pharmacy 2 2 2 2 2 3 2 2 2 2 2 1
Drug Shops & Clinics 2 2 3 1 1 3 0 3 3 2 2 3
Informal Outlets 1 3 0 2 0 0 3 0 0 0 1 0
Public Health Facilities 1 - 2 1 - 2 0 - 2 1 - 2
Total 7 14 10 8 6 11 6 8 10 7 9 9
Key; WN – West Nile, SW – South West, EC – East Central
11
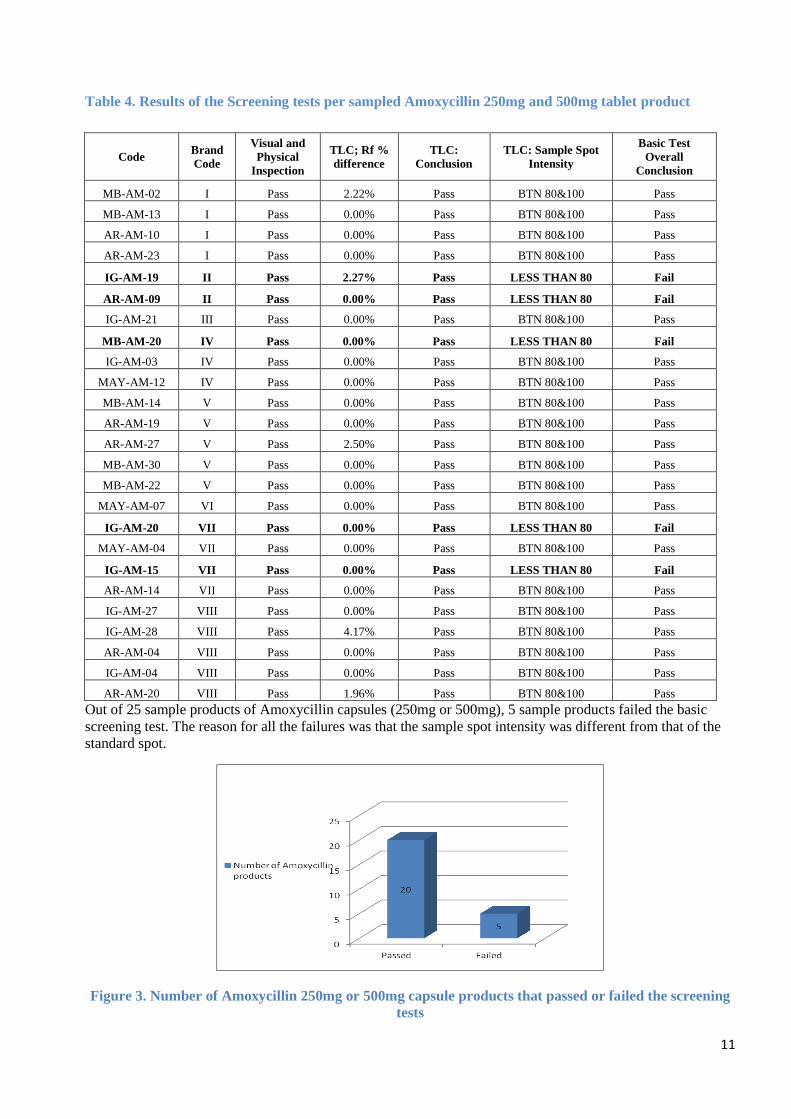
Table 4. Results of the Screening tests per sampled Amoxycillin 250mg and 500mg tablet product
Code Brand
Code
Visual and
Physical
Inspection
TLC; Rf %
difference
TLC:
Conclusion
TLC: Sample Spot
Intensity
Basic Test
Overall
Conclusion
MB-AM-02 I Pass 2.22% Pass BTN 80&100 Pass
MB-AM-13 I Pass 0.00% Pass BTN 80&100 Pass
AR-AM-10 I Pass 0.00% Pass BTN 80&100 Pass
AR-AM-23 I Pass 0.00% Pass BTN 80&100 Pass
IG-AM-19 II Pass 2.27% Pass LESS THAN 80 Fail
AR-AM-09 II Pass 0.00% Pass LESS THAN 80 Fail
IG-AM-21 III Pass 0.00% Pass BTN 80&100 Pass
MB-AM-20 IV Pass 0.00% Pass LESS THAN 80 Fail
IG-AM-03 IV Pass 0.00% Pass BTN 80&100 Pass
MAY-AM-12 IV Pass 0.00% Pass BTN 80&100 Pass
MB-AM-14 V Pass 0.00% Pass BTN 80&100 Pass
AR-AM-19 V Pass 0.00% Pass BTN 80&100 Pass
AR-AM-27 V Pass 2.50% Pass BTN 80&100 Pass
MB-AM-30 V Pass 0.00% Pass BTN 80&100 Pass
MB-AM-22 V Pass 0.00% Pass BTN 80&100 Pass
MAY-AM-07 VI Pass 0.00% Pass BTN 80&100 Pass
IG-AM-20 VII Pass 0.00% Pass LESS THAN 80 Fail
MAY-AM-04 VII Pass 0.00% Pass BTN 80&100 Pass
IG-AM-15 VII Pass 0.00% Pass LESS THAN 80 Fail
AR-AM-14 VII Pass 0.00% Pass BTN 80&100 Pass
IG-AM-27 VIII Pass 0.00% Pass BTN 80&100 Pass
IG-AM-28 VIII Pass 4.17% Pass BTN 80&100 Pass
AR-AM-04 VIII Pass 0.00% Pass BTN 80&100 Pass
IG-AM-04 VIII Pass 0.00% Pass BTN 80&100 Pass
AR-AM-20 VIII Pass 1.96% Pass BTN 80&100 Pass
Out of 25 sample products of Amoxycillin capsules (250mg or 500mg), 5 sample products failed the basic
screening test. The reason for all the failures was that the sample spot intensity was different from that of the
standard spot.
Figure 3. Number of Amoxycillin 250mg or 500mg capsule products that passed or failed the screening
tests

12
Table 5. Results of screening tests for Artemether/Lumefantrine 20/120mg tablet products
Sample Code
No.
Brand
Code Basic Test
Overall Conclusion
Visual & Physical
Inspection
Conclusion
Disintegration (time)
Disintegration Conclusion
TLC: Principal Spot
Rf % Sample
Difference
TLC: Principal Spot
Conclusion
TLC: Sample Spot Intensity
TLC: Sample Spot Intensity
Conclusion
TLC: Presence of
Impurity
Spots
TLC: Impurities
Conclusion
1 MB-AL-26 I Pass 2MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
2 MB-AL-34 I Pass 2MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
3 MB-AL-09 I Pass 3MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
4 IG-AL-12 I Pass 3MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
5 MB-AL-06 I Pass 3MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
6 MB-AL-24 I Pass 2MINUTES PASS 1.15% PASS BTN 80&100 PASS N/Ap PASS PASS
7 MAY-AL-02 I Pass 5MINUTES PASS 2.27% PASS BTN 80&100 PASS N/Ap PASS PASS
8 MB-AL-08 I Pass 6MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
9 AR-AL-16 II Pass 6MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
10 IG-AL-01 II Pass 7MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
11 MB-AL-35 II Pass 7MINUTES PASS 1.12% PASS BTN 80&100 PASS N/Ap PASS PASS
12 IG- AL- 06 III Pass 3MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
13 MB-AL-18 III Pass 4 MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
14 MB-AL-05 III Pass 3MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
15 AR-AL-01 III Pass 3MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
16 MB-AL-36 IV Pass 2MINUTES PASS 2.27% PASS BTN 80&100 PASS N/Ap PASS PASS
17 IG-AL-16 IV Pass 2MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
18 IG-AL-05 IV Pass 2MINUTES PASS 2.27% PASS BTN 80&100 PASS N/Ap PASS PASS
19 AR-AL-11 IV Pass 2MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
20 IG-AL-14 V Pass 3MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
21 IG-AL-02 V Pass 6MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
22 MB-AL-29 V Pass 3MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
23 AR-AL-06 V Pass 6 MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
24 AR-AL-18 V Pass 5MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
25 MAY-AL-06 V Pass 2MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
26 AR-AL-07 V Pass 2MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
27 AR-AL-13 V Pass 5MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
28 MB-AL-25 V Pass 5MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
29 MAY-AL-01 V Pass 4MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
30 MB-AL-17 V Pass 6MINUTES PASS 1.11% PASS BTN 80&100 PASS N/Ap PASS PASS
31 MB-AL-04 V Pass 2MINUTES PASS 0.00% PASS BTN 80&100 PASS N/Ap PASS PASS
All the Artemether/Lumefantrine 20/120mg tablet products passed the screening tests.

13
Table 6. Results of screening tests for sampled Co-trimoxazole 480mg and 960mg tablet products
Sample Code No.
Brand Code
Basic Test Overall
Conclusion
Visual &
Physical
Inspection Conclusion
Disintegration
(time)
Disintegration
Conclusion
TLC: Principal Spot
Rf % Sample
Difference
TLC:
Principal Spot
Conclusion
TLC: Sample
Spot Intensity
TLC: Sample
Spot Intensity
Conclusion
TLC: Presence
of Impurity
Spots
TLC:
Impurities
Conclusion
1 IG-CO-07 I Pass 2minutes Pass 0.00% pass 100 Pass N/Ap Pass Pass
2 MB-CO-03 I Pass 1minute Pass 0.00% Pass 100 Pass N/Ap Pass Pass
3 AR-CO-28 II Pass 3minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
4 AR-CO-02 III Pass 1 minute Pass 0.00% Pass 100 Pass N/Ap Pass Pass
5 MAY-CO-10 III Pass 1minute Pass 1.06% Pass 100 Pass N/Ap Pass Pass
6 MB-CO-07 III Pass 3minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
7 MB-CO-19 III Pass 2minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
8 MB-CO-27 III Pass 2minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
9 MAY-CO-03 III Pass 2minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
10 AR-CO-15 IV Pass 3minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
11 AR-CO-25 IV Pass 3minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
12 MB-CO-33 V Pass 2minutes Pass 0.93% Pass 100 Pass N/Ap Pass Pass
13 MB-CO-21 V Pass 4minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
14 IG-CO-09 V Pass 1minute Pass 0.00% Pass 100 Pass N/Ap Pass Pass
15 IG-CO-25 V Pass 2minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
16 MB-CO-17 V Pass 1minute Pass 0.00% Pass 100 Pass N/Ap Pass Pass
17 AR-CO-22 VI Pass 2 minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
18 AR-CO-17 VI Pass 2minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
19 MB-CO-12 VI Pass 1minute Pass 1.77% Pass 100 Pass N/Ap Pass Pass
20 IG-CO-10 VI Pass 2minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
21 AR-CO-05 VII Pass 3minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
22 MAY-CO-08 VII Pass 2minutes Pass 1.22% Pass 100 Pass N/Ap Pass Pass
23 IG-CO-17 VII Pass 3minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
24 IG-CO-26 VII Pass 2minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
25 MB-CO-11 VII Pass 2minutes Pass 0.00% Pass 100 Pass N/Ap Pass Pass
All the co-trimoxazole 480mg or 960mg tablet products passed the screening tests.
14
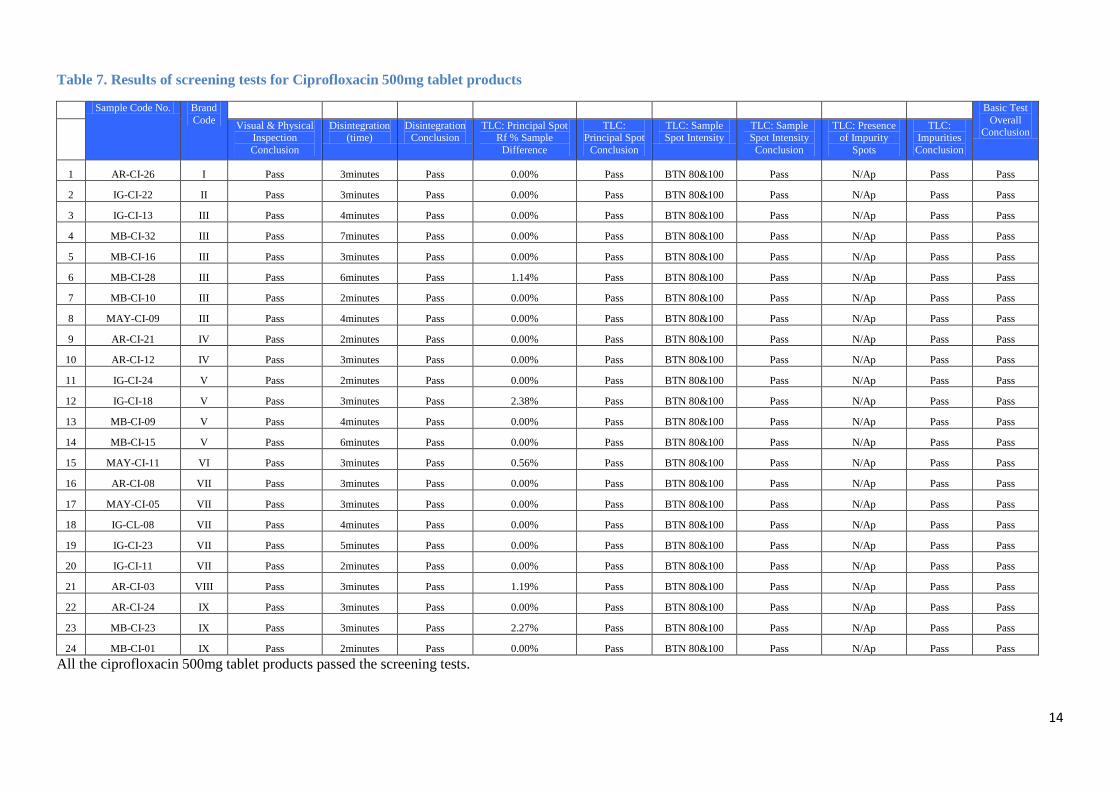
Table 7. Results of screening tests for Ciprofloxacin 500mg tablet products
Sample Code No. Brand
Code Basic Test
Overall Conclusion
Visual & Physical Inspection
Conclusion
Disintegration (time)
Disintegration Conclusion
TLC: Principal Spot Rf % Sample
Difference
TLC: Principal Spot
Conclusion
TLC: Sample Spot Intensity
TLC: Sample Spot Intensity
Conclusion
TLC: Presence of Impurity
Spots
TLC: Impurities
Conclusion
1 AR-CI-26 I Pass 3minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
2 IG-CI-22 II Pass 3minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
3 IG-CI-13 III Pass 4minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
4 MB-CI-32 III Pass 7minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
5 MB-CI-16 III Pass 3minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
6 MB-CI-28 III Pass 6minutes Pass 1.14% Pass BTN 80&100 Pass N/Ap Pass Pass
7 MB-CI-10 III Pass 2minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
8 MAY-CI-09 III Pass 4minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
9 AR-CI-21 IV Pass 2minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
10 AR-CI-12 IV Pass 3minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
11 IG-CI-24 V Pass 2minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
12 IG-CI-18 V Pass 3minutes Pass 2.38% Pass BTN 80&100 Pass N/Ap Pass Pass
13 MB-CI-09 V Pass 4minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
14 MB-CI-15 V Pass 6minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
15 MAY-CI-11 VI Pass 3minutes Pass 0.56% Pass BTN 80&100 Pass N/Ap Pass Pass
16 AR-CI-08 VII Pass 3minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
17 MAY-CI-05 VII Pass 3minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
18 IG-CL-08 VII Pass 4minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
19 IG-CI-23 VII Pass 5minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
20 IG-CI-11 VII Pass 2minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
21 AR-CI-03 VIII Pass 3minutes Pass 1.19% Pass BTN 80&100 Pass N/Ap Pass Pass
22 AR-CI-24 IX Pass 3minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
23 MB-CI-23 IX Pass 3minutes Pass 2.27% Pass BTN 80&100 Pass N/Ap Pass Pass
24 MB-CI-01 IX Pass 2minutes Pass 0.00% Pass BTN 80&100 Pass N/Ap Pass Pass
All the ciprofloxacin 500mg tablet products passed the screening tests.

15
7.0 Conclusion
Of all the sampled products, only Amoxycillin 250mg or 500mg capsules had some failures (5/25
samples) on the screening tests. These products failed on the identity test as the sample spot intensity was
different from the standard spot intensity. All the other products of Artemether/Lumefantrine 20/120mg
tablets, Ciprofloxacin 500mg tablets and Co-trimoxazole 480mg or 960mg tablets passed the screening
tests. The failed Amoxycillin capsule products were forwarded to NDA Quality Control Laboratory for
verification and confirmatory tests.

16
Annex 1: Testing Methods, Procedures and Testing Data Reporting
1. Testing methods and reference materials, substances and/or standards
• Basic testing/screening level: Testing methods and procedures are described in the GPHF-Minilab
Manual and the reference substances/product provided by GPHF-Minilab kits were used. These
tests are in conformance with USP DQI. The tests cover:
Physical/visual inspection/examination (manufacturing source, counterfeit or suspicious
drugs)
Simple disintegration for solid dosage forms
TLC (identity of active ingredient, content/concentration, impurities versus authentic
reference standards) (see Appendix 2 for General rules TLC result interpretation)

17
3. Testing data reporting
The Report from the Study team to DRA and key stakeholders should include a copy of the
completed Sentinel Site Drug Sample Collection and Testing Report Form (Annex 3). All results
(passed and failed) should be sent simultaneously to DRA.
For-cause or emergency reporting (as necessary) – The site must report any “for cause” incidents
to the NDA Lab, which will verify the testing results and will take any necessary action.

18
Annex 2 Checklist for Sentinel Site “Drug Testing” Personnel
Before going out for sampling, the sampling team must check that all the following has been complied
with:
- Training of the sampling team
- Developed written itinerary to travel efficiently and reach the maximum number of sampling sites
in shortest time and most economical way
- Checked availability of all items related to sampling and brought checklist along
- Enough Sampling Forms
One form is to be filled out for each sample - consider extra forms in case of mistakes
- Sampling Plan
The sampling team must prepare a sampling plan in accordance with the study protocol and plan
ahead of time for each day of sampling
- Enough Sampling Containers
Obtain new plastic (zipper bags are ideal), opaque, clean containers to store and transport samples.
Each sample requires a container, a label (with name of collector, name of drug, sampling site, date
of collection), and containers must be tightly closed.
Sampling forms should go into plastic bags (double check that the sampling form contains all
required information before inserting it).
Samples collected from the same site need to be placed in one labelled box.
- Indelible markers, pens and pencil
Use indelible markers to label the sampling containers
- Dedicated book to keep all notes on survey
Please use a separate book dedicated only to the study and record complete and accurate information
about samples right when they are collected.
- Sampling tools
Scissors, Gloves, Tape, Watch, Labels
- Logistics
Transportation, money (or other appropriate means) for purchasing samples, cardboard boxes to
store the samples collected.
- Optional items
If your office already has a digital camera used in pharmaceutical inspections, please use it to
take pictures of sample sites and samples.

19
Annex 3: Sentinel Site Drug Sample Collection and Testing Report Form
Report No. -------------/-----------------------------(district name)
SAMPLE INFORMATION
Sample CODE/Serial Number: )
Name of location/place where sample was taken
Street address (with telephone and fax number, if
applicable)
Date of sampling
Drug Name (trade or brand name)
Generic or INN1 name
Dosage form and strength
Manufacturer’s Batch or Lot Number
Manufacturing date
Expiry date
Registration or licensed number (if applicable)
Manufacturer name and address
Number of sample units taken (minimum 30
tablets or capsules; 50 for FDCs2)
taken in original package taken from bulk container
Brief physical/visual description of sample
Name of collector(s)/date/sign
Name of seller or representative identified of
establishment where sample was taken
PHYSICAL/VISUAL INSPECTION TEST
Labeling (requirements)
Brand Name of the drug sample (if applicable)
Generic or INN name of active ingredient(s)
Dosage form and strength
Name of reference standard used (as claimed on label
e.g.
USP, BP, IP, EP)
Manufacturer’s Batch or Lot Number
Name of manufacturer and address (with telephone and
fax number if applicable)

20
Manufacturing date
Expiry date
Storage conditions
1 INN is the International Non-proprietary name of a drug product
2 FDCs stand for fixed-dose combination preparations
Packaging
Material (blister pack/card, bottle, others specify)
Unit dose per blister card or container stated
Any print on the backing foil (if packed in blister pack
or
card)
Description of dosage form
Shape (circular, oval, flat sides, other)
Uniformity of shape
Uniformity of color
No physical damage (cracks, breaks, erosion, abrasion,
sticky)
Other observations (no foreign contaminant, dirty marks,
proper seal - for capsule)
Sample serial Number/Code
Specify the test method (s) and reference to a pharmacopeial monograph e.g. USP26, BP e.t.c
DISINTEGRATION TEST
Time of complete
Disintegration expected
30 minutes
Time of complete Disintegration
observed
---------------
Did the drug pass Disintegration
test?
Yes
No

21
RESULT OF TLC TEST
Distance moved by
Solvent front:
------------ mm
Did the drug and the standard Spots
have the same intensity?
Yes
No
Did the sample pass quality by
using the TLC test?
Yes
No
Distance moved by the
Standard spot:
------------- mm
Distance moved by the
Sample spot:
------------ mm
Rf(Sample error)
Was there any contaminant spot
on the TLC plate?
Yes
No
Rf (Standard)
Rf (Sample)
Name of API COLOUR REACTION Did sample pass colour reaction
test?
Yes No
Name of API
Yes No
FINAL COMMENTS
The sample meets standards
The sample does not meet standards. Reason:____________________________________
The sample is doubtful for its quality testing. Reason:______________________________
And further testing is needed at a reference lab
Report prepared by:
Date:
Name:
Signature:
Report reviewed by:
Date:
Name:
Signature:
22
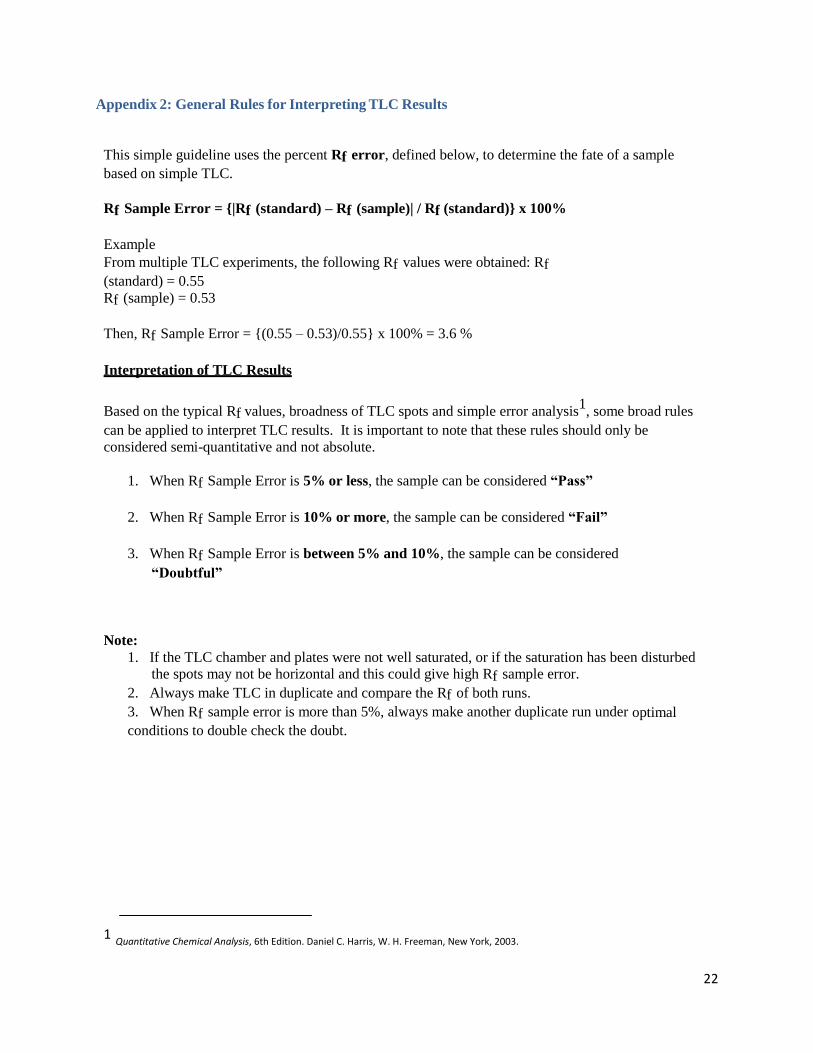
Appendix 2: General Rules for Interpreting TLC Results
This simple guideline uses the percent Rf error, defined below, to determine the fate of a sample
based on simple TLC.
Rf Sample Error = {|Rf (standard) – Rf (sample)| / Rf (standard)} x 100%
Example
From multiple TLC experiments, the following Rf values were obtained: Rf
(standard) = 0.55
Rf (sample) = 0.53
Then, Rf Sample Error = {(0.55 – 0.53)/0.55} x 100% = 3.6 %
Interpretation of TLC Results
Based on the typical Rf values, broadness of TLC spots and simple error analysis1, some broad rules
can be applied to interpret TLC results. It is important to note that these rules should only be
considered semi-quantitative and not absolute.
1. When Rf Sample Error is 5% or less, the sample can be considered “Pass”
2. When Rf Sample Error is 10% or more, the sample can be considered “Fail”
3. When Rf Sample Error is between 5% and 10%, the sample can be considered
“Doubtful”
Note:
1. If the TLC chamber and plates were not well saturated, or if the saturation has been disturbed the spots may not be horizontal and this could give high Rf sample error.
2. Always make TLC in duplicate and compare the Rf of both runs.
3. When Rf sample error is more than 5%, always make another duplicate run under optimal
conditions to double check the doubt.
1 Quantitative Chemical Analysis, 6th Edition. Daniel C. Harris, W. H. Freeman, New York, 2003.
23
8. References
Annual Health Sector Performance Report, 2006/07, 2007.08
Health Sector Strategic Investment Plan III 2010/11-2014/15
MeTA Country Work Plan Guidelines VS.6 January, 2009
MeTA Phase II Proposal, 2012
Ministry of Health.MoH. (2008). Access to and use of medicines by households in Uganda. Kampala:
Ministry of Health.MoH.
Ouagadougou Declaration on primary health Care and Health Systems in Africa 2008
Private Sector Mapping Uganda Mission report, December 2008.
Uganda MeTA Scoping mission report, April 2008
World health Organization Medicines Strategy 2004-2007
The United States Pharmacopeial Convention, Inc 2003 Guidelines for Sampling of Antimalarial Drug
Samples in the USP DQI Antimalarial Drug Quality Monitoring Project in Mekong Sub-region Countries
Newton PN, Lee SJ, Goodman C, Fernández FM, Yeung S, et al. (2009) Guidelines for field surveys of the
quality of medicines: A proposal. PLoS Med 6(3): e1000052. doi:10.1371/journal.pmed.1000052
Quantitative Chemical Analysis, 6th Edition. Daniel C. Harris, W. H. Freeman, New York, 2003
World Health Organization. WHO Technical Report Series (TRS), No. 902 (2002). Annex 3: Good practices for
national pharmaceutical control laboratories. http://whqlibdoc.who.int/trs/WHO_TRS_902.pdf#page=37


















