
Schizophrenia and Other Disorders A talk given by Elaine M. Hull at the Lawton Chiles High School,...
80
Schizophrenia and Other Disorders A talk given by Elaine M. Hull at the Lawton Chiles High School, Tallahassee, FL, February 2007
-
Upload
miranda-mossop -
Category
Documents
-
view
214 -
download
0
Transcript of Schizophrenia and Other Disorders A talk given by Elaine M. Hull at the Lawton Chiles High School,...

Schizophrenia and Other Disorders
A talk given by Elaine M. Hull at the Lawton Chiles High School, Tallahassee, FL, February 2007
A bit of history
• Hideyo Noguchi, 1911: Syphilis (delusions, grandiosity, impulsivity, altered thought structure) is due to bacterium.
• Emil Kraeplin, 1919: dementia praecox (paranoia, grandiose delusions, auditory hallucinations, abnormal emotional reg., bizarre thoughts)—partly genetic
• Eugen Bleuler, 1911: key is dissociative thinking; also delusions, hallucinations, affective disturbance, autism.


Genes
• Genes scattered across all but 8 chromosomes have been implicated
• Most important: – Neuregulin 1: NMDA, GABA, & Ach receptors– Dysbindin: synaptic plasticity– Catechol-O-methyl transferase: DA metabol.– G72: regulates glutamatergic activity– Others: myelination, glial function
• Paternal age: more cell divisions in sperm

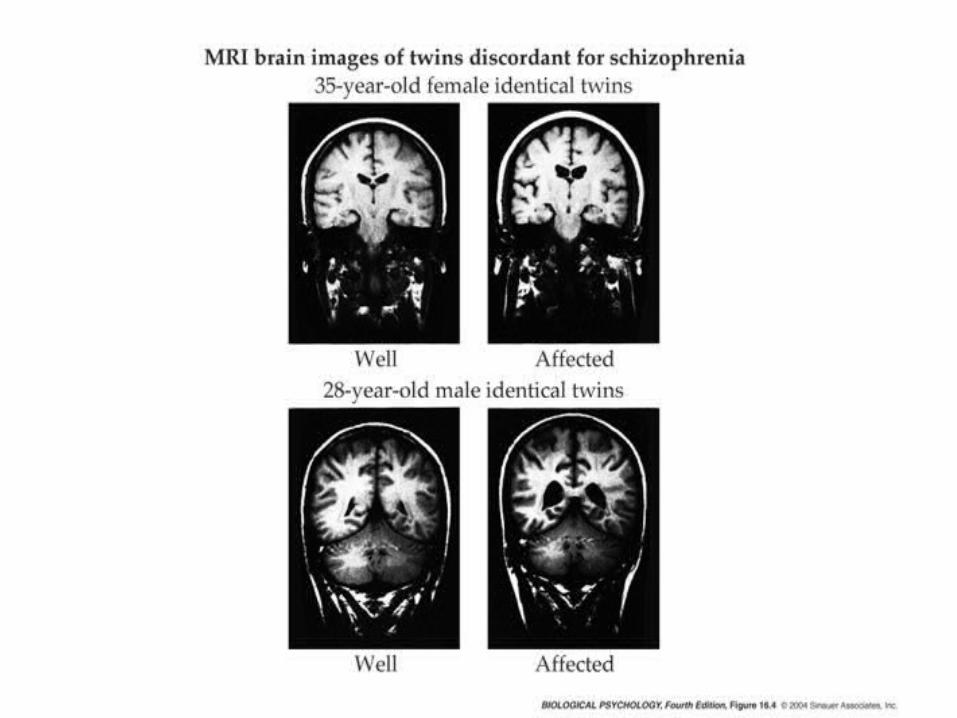
Twin studies
• Why does one twin become schizophrenic and the other does not?– Lower birth weight– More physiological distress– More submissive, tearful, sensitive– Impaired motor coordination
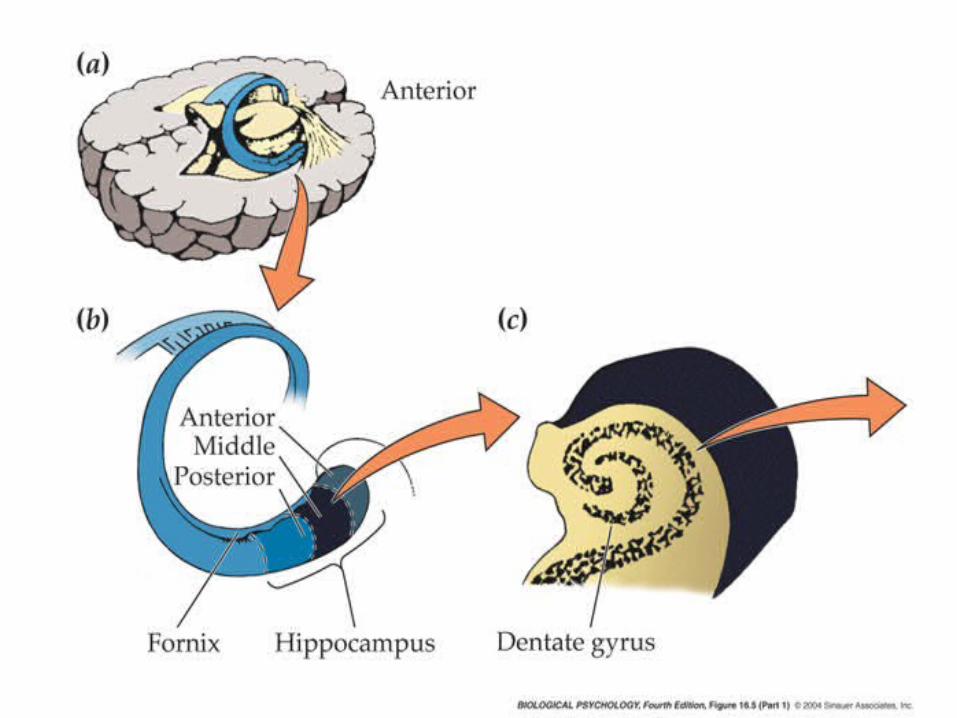
Structural changes in brain
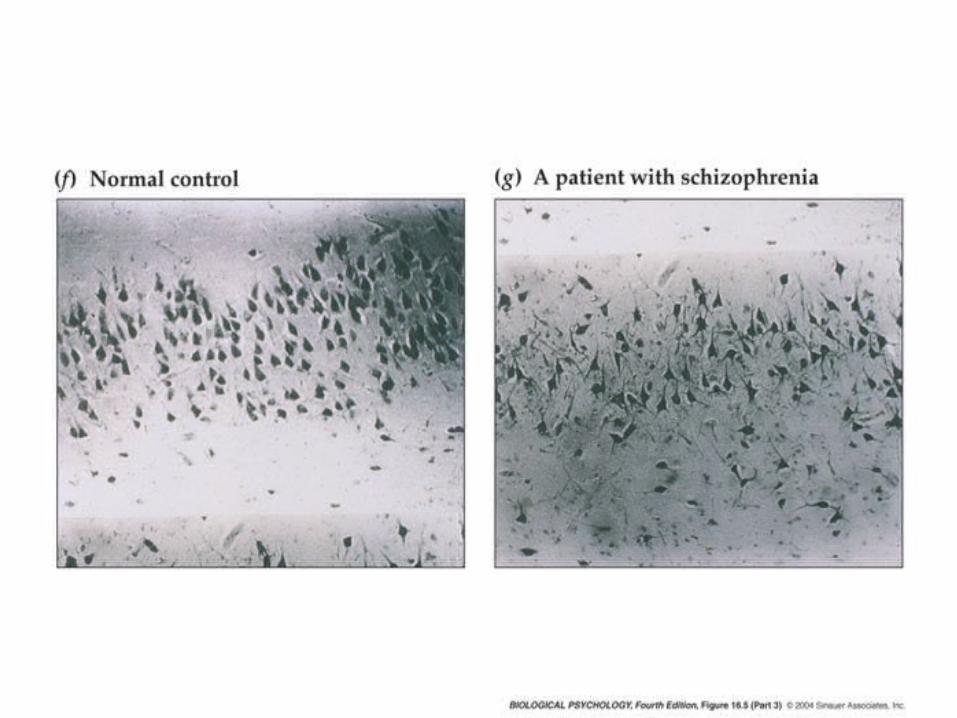
• Hippocampus, amygdala, parahippocamp.– Smaller in affected twin (static trait)– Disordered hippocampal pyramidal cells
• Correlation between cell disorder and severity• May be due to maternal influenza in 2nd trimester
– Also in entorhinal, cingulate, parahippocampal cortex

Structural changes in brain
• Larger ventricles– Subgroup: inverse correlation between
ventricle size and response to drugs
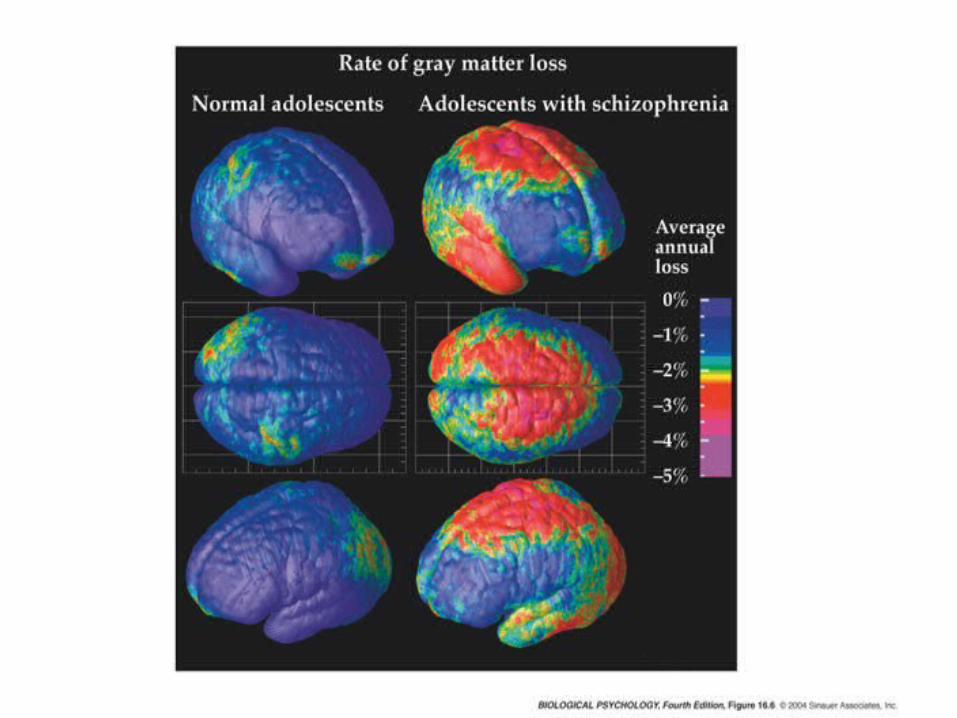
Structural changes in brain
• Increased loss of gray matter in adolescence
Structural changes in brain
• Shrinkage of cerebellar vermis
• Thicker corpus callosum
• Frontal lobes – Abnormal neuronal migration in one study– Dendrites have fewer spines– But no major structural abnormalities– Measures of frontal function impaired
Functional changes in brain
• Hypofrontality hypothesis– Discordant twins: low frontal blood flow only in
affected twin– Wisconsin card sorting task
• Schizophrenics can’t shift attn. to other criterion• Functional imaging: frontal lobe activity lower at
rest, esp. in right hemisphere, does not increase during task.
• Drug treatment increased activation of frontal lobes

Neurochemical changes
• LSD, mescaline confusion, delirium, disorientation, visual hallucinations.
• But schizophrenic hallucinations are mostly auditory
• Schizophrenics given LSD say it’s different from their symptoms

Dopamine hypothesis
• Amphetamine (very high doses) paranoia, delusions, auditory hallucination
• Also exacerbates symptoms of schiz.
• Effects blocked by DA antagonist chlorpromazine
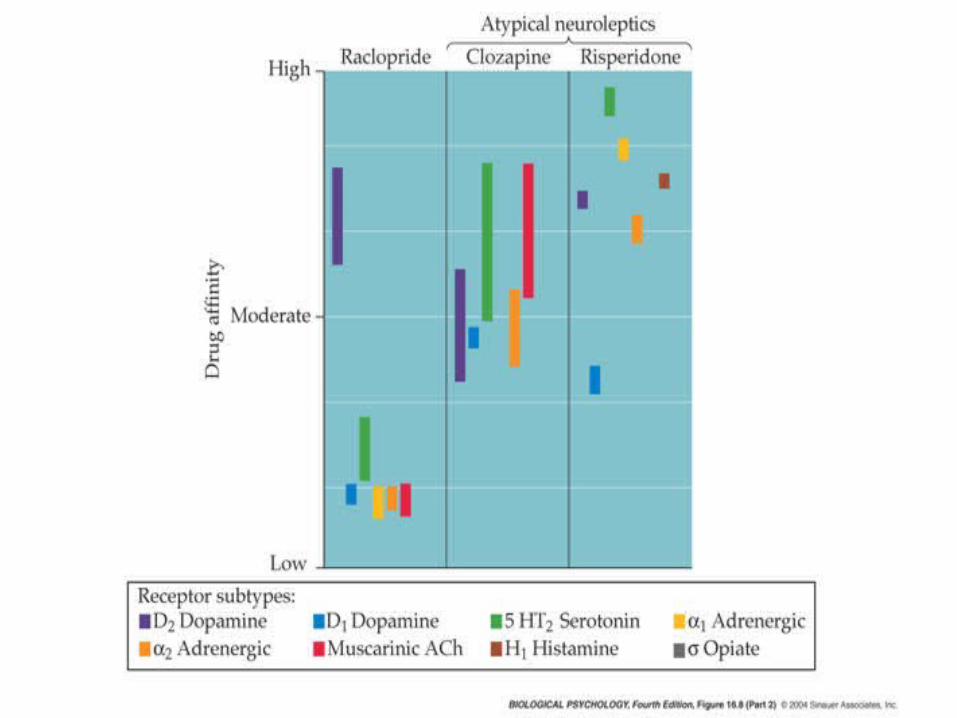
• Phenothiazines (incl. chlorprom.) & all other typical neuroleptics block D2 receptors and alleviate (+) symptoms.
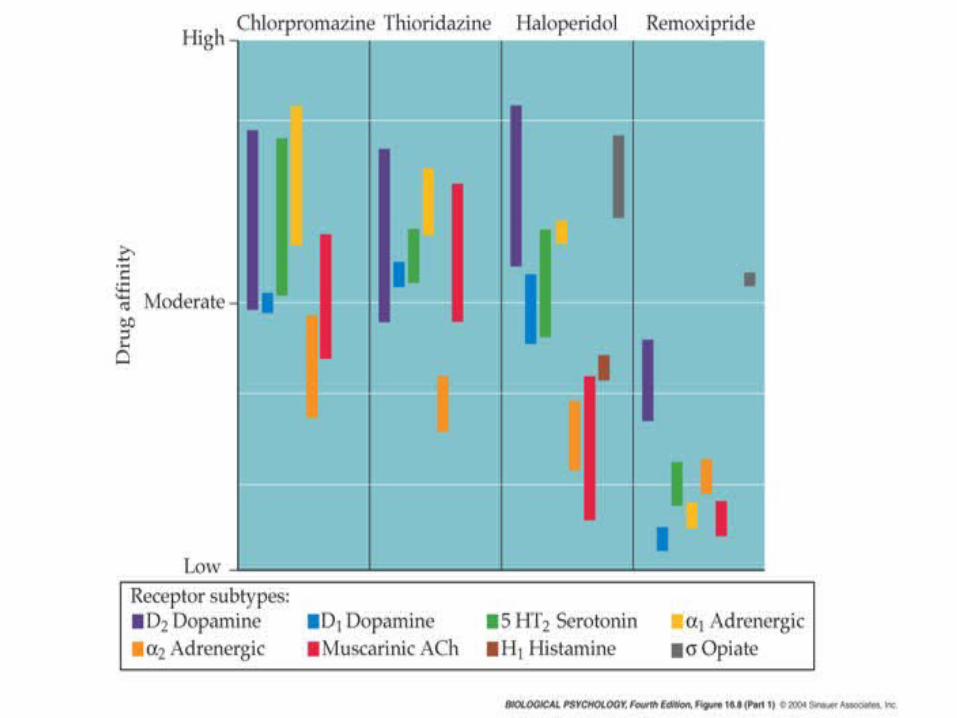
Atypical neuroleptics
• Clozapine blocks 5-HT2A receptors > D2
• As effective as typical neuroleptics on (+) symptoms, more effective on (-) symptoms
• Fewer motor side effects (tardive dyskinesia)
• Actually increase DA release in frontal cortex– L-DOPA can even be beneficial
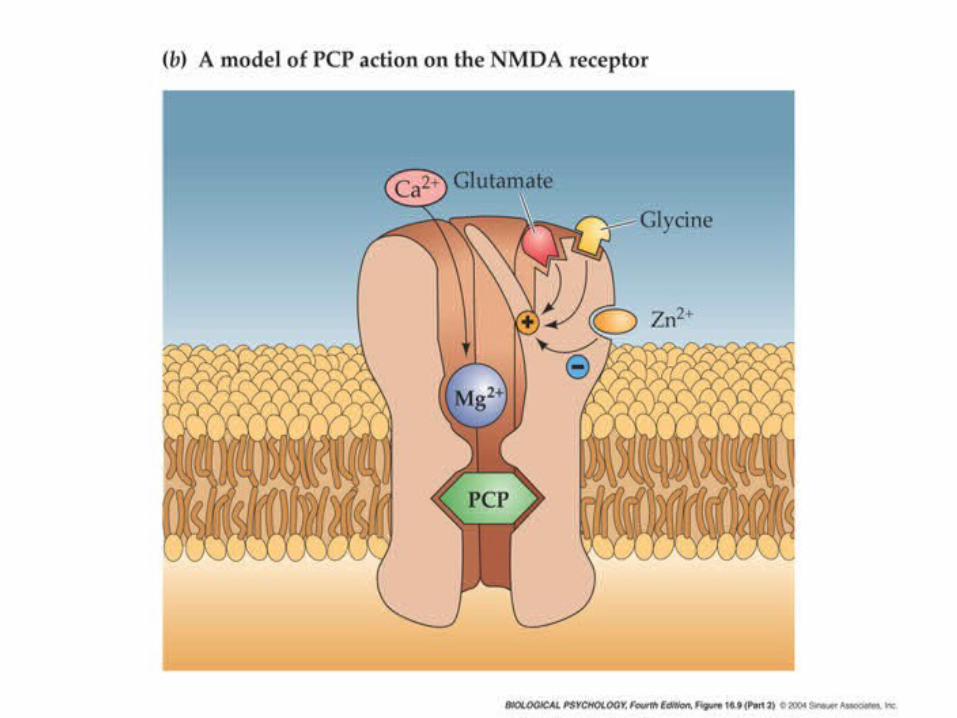
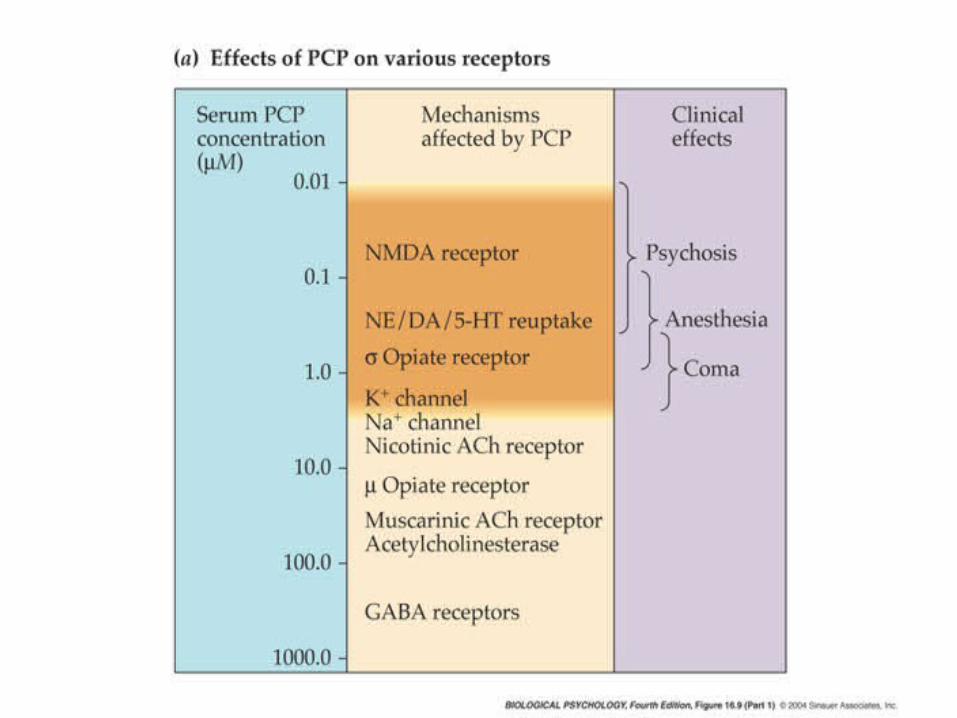
Glutamate hypothesis
• Problem with DA hypothesis: time course
• Phencyclidine (PCP): dissociative anesthetic – Auditory hallucinations– Depersonalization– Delusions– Noncompetitive NMDA antagonist (blocks
Ca2+ channel)

Glutamate hypothesis
• 2 weeks PCP in monkeys schiz.-like symptoms– Including poor performance on frontal lobe-
sensitive task
• Dose- & time-sensitive
• Ketamine (NMDA antag) similar effects
• So, why not give glutamate agonists to treat schizophrenia?????

Glutamate hypothesis
• Seizures!! (also excitotoxicity)
• Try mGluR agonists: 8 subtypes of mGluR– Some modulate glutamate release– Others modulate dopamine systems
Reconciliation
• Maybe hypofrontality results in hyper-dopaminergic state in NAc
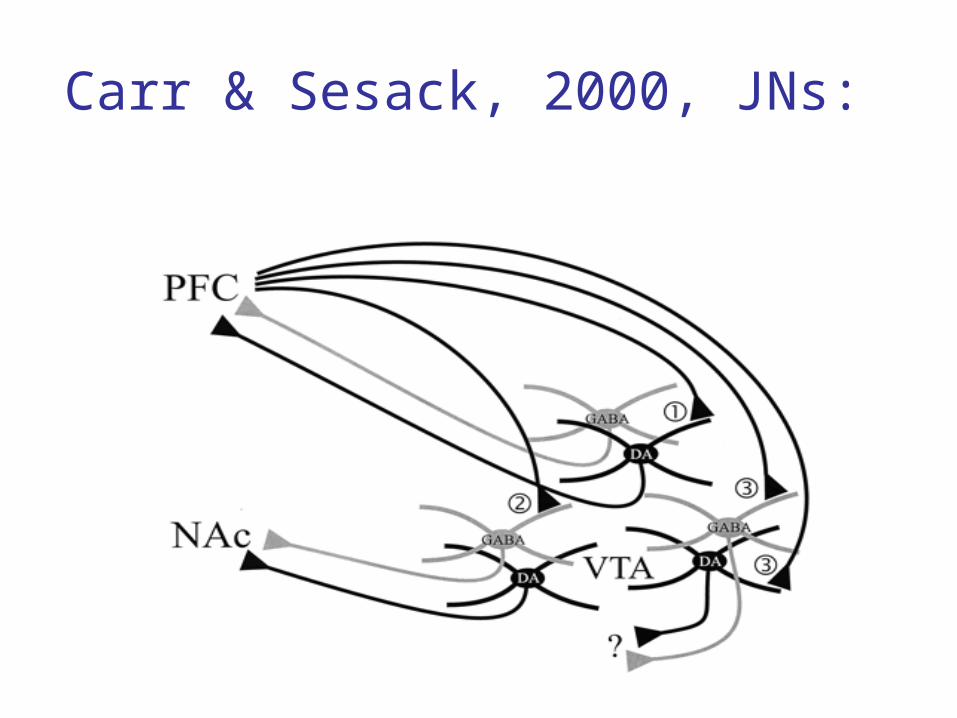
• Carr & Sesack, 2000, JNs: – PFC sends Glu axons to VTA DA cells that PFC
• Result: positive feedback to PFC
– PFC sends Glu axons to VTA GABA cells that NAc• Result: PFC inhibits NAc (probably amygdala, too)
Carr & Sesack, 2000, JNs:
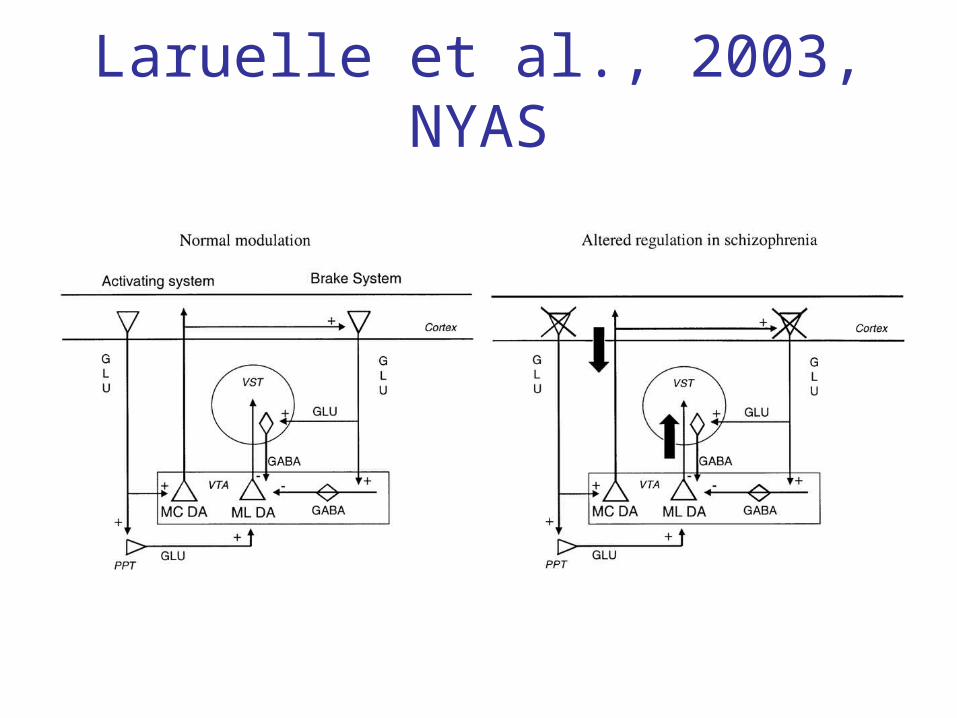
Laruelle et al., 2003, NYAS
Schizophrenia Summary
• PFC and hippocampus cell density and activity are lower in schizophrenics; neither works well.– Hippocampal neurons are also disorganized.
• There is normally a positive feedback between PFC and VTA DA neurons that PFC– Less PFC activity decreases that (+) feedback.
• There is normally a negative feedback between PFC and NAc. (May inhibit impulses, thoughts)– Less PFC activity decreases that (-) feedback.
Schizophrenia Summary
• The reason D2 antagonists help (+) symptoms: inhibits mostly NAc & other limbic structures.– Few D2 receptors in PFC.
• The reason PCP schizophrenic symptoms: mimics the PFC hypofunction, releases NAc.
• There may also be anomalies in intracellular messengers.
• No good biochemical/anatomical explanation for (-) symptoms.– Worse in those with greatest physical damage.– But atypical antipsychotics do help (-) symptoms. (How???)
Schizophrenia Summary
• Possible treatments:– Metabotropic glutamate (mGluR1) agonists
• Increase glutamate or DA release
– Glycine or cycloserine• Bind to glycine site on NMDA receptor & enable
glutamate’s effects
– Neither would seizures– Not yet tested in humans
Unipolar Depression
• Sad & helpless every day for weeks
• Loss of interests, energy, appetite
• Feel worthless
• Contemplate suicide
• Difficulty in concentrating
• Restless agitation
• Little or no pleasure from eating or sex

Unipolar Depression
• 2 X as often in women as in men• ~ 5% of adults in US have “clinically
significant” depression• A genetic component
– 60% concordance for monozygotic twins– 20% for dizygotic twins– Especially for early-onset & among female
relatives– Not a single-gene defect
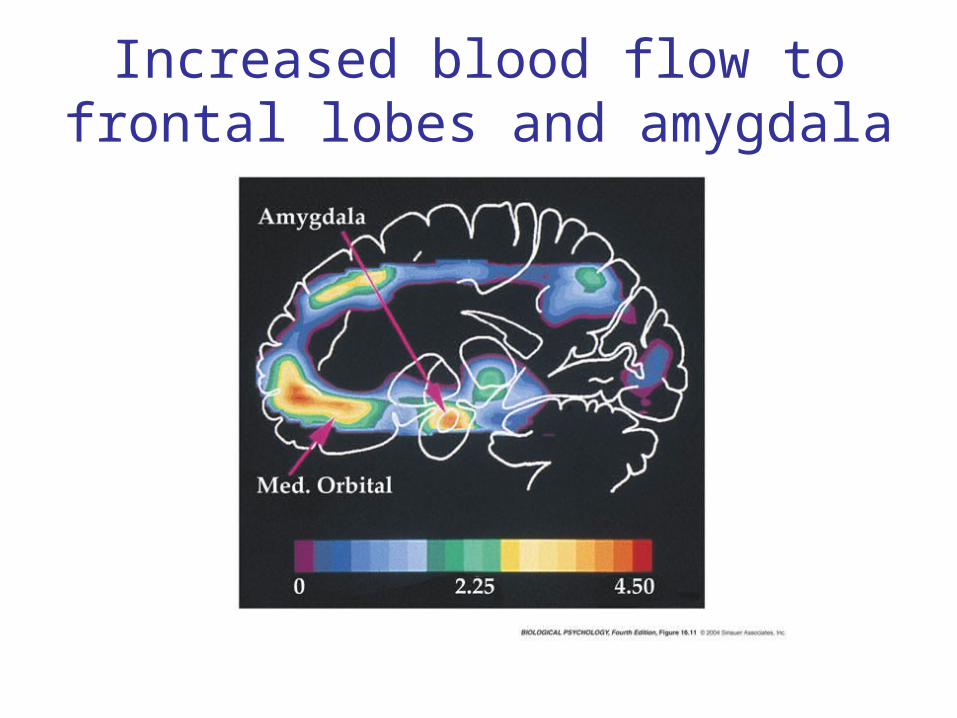
Increased blood flow to frontal lobes and amygdala

Increased blood flow also in:
• Parietal cortex (somatosensory/attention)
• Posterior temporal cortex (language)
• Anterior cingulate (emotional processing)

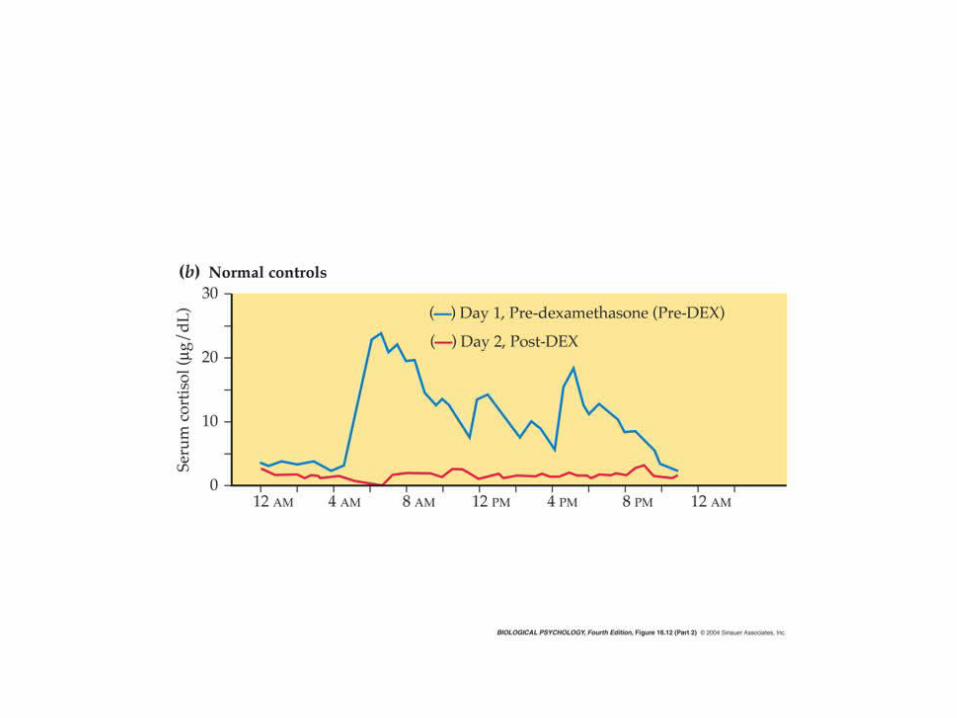
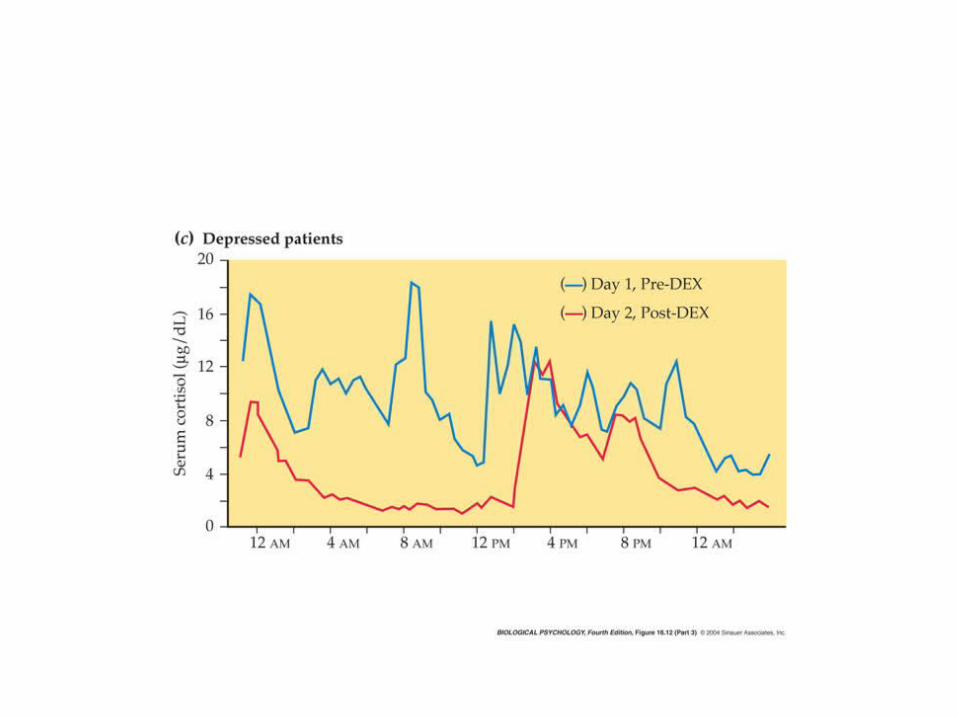
Cortisol is often increased in depressed people.

Effects of high cortisol levels
• Increase cell death in hippocampus– Probably due to apoptosis– Brief cortisol exposure increases hippocampal
activity helps remember acute stressor.– Hipp negative feedback on cortisol levels– Lengthy high levels increase cell death, also
decrease neurogenesis– As a result vicious circle: High cortisol
hipp. neurotoxicity less (-) feedback high cortisol.

Effects of high cortisol levels
• Depressed people often have bad memories and difficulty reasoning.
• SSRIs increased survival of new neurons in hipp., increased memory and reasoning.
• Hypothesis:– 5-HT &/or NE cAMP CREB BDNF– 5-HT4, -6, -7 & β are coupled to Gs
• BDNF in rats also increases cell survival in hippocampus and decreases behavioral measures of animal “depression.”

Normal sleep pattern

Sleep pattern in depression

Early entry into REM
Altering sleep patterns sometimes helps depression
• Most depressed people are phase-advanced in their sleep cycles.
• Some are helped temporarily by total sleep deprivation for 1 night.
• Others are helped by going to bed from 5pm to midnight for a week & gradually going back to normal.
Electroconvulsive therapy
• Can help those who don’t respond to drug therapy or are suicidal.
• Unclear why it works.– Increases D1 & D2 receptors in NAc– Decreases postsynaptic β NE receptors

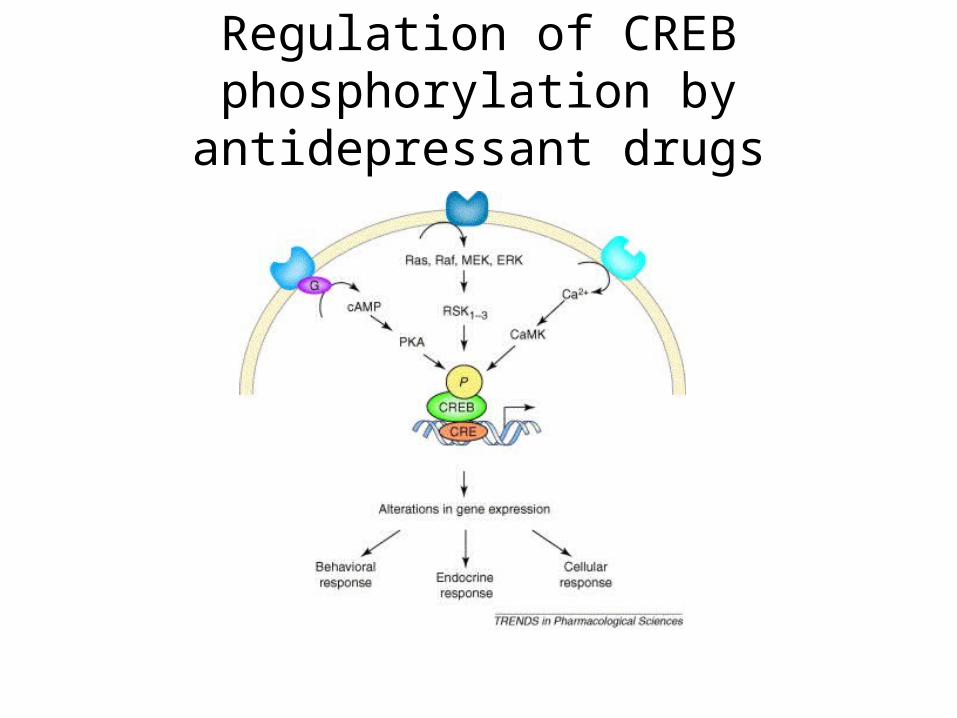
Regulation of CREB phosphorylation by antidepressant drugs

Summary of Depression• Symptoms
– Sad & helpless; feel worthless– Loss of interests, energy, appetite– Agitated; Contemplate suicide– Can’t concentrate– Little or no pleasure from eating or sex
• High cortisol damage hippocampus– Decrease neg feedback; damage memory
Summary of Depression• Diurnal rhythms phase advanced• Genetic predisposition (not just one gene)
• Women > men (decreased allopregnanolone?)
• Treatments– SSRIs, MAOIs, tricyclics
• SSRIs BDNF new neuron survival
– ECT– Don’t sleep for 1 night; Go to bed earlier– GC antagonist
Seasonal Affective Disorder
• More prevalent in winter.• Not necessarily more prevalent in far north
or south. • Treated successfully with bright light AM &
PM. – Dose response curve for both time & intensity– Suppresses melatonin (probably not critical)– 5-HT seasonal rhythm (low in winter)
• SSRIs can treat SAD
Light treatment for SAD
Bipolar Disorder
• Manic phase– Overactivity & wakefulness– Talkativeness– Grandiosity
• Depressed phase: ~ unipolar depression• Men & women: similar incidence• Earlier onset than unipolar• Genes on chromosomes 4, 11, 12, 16, 21, X
– Including gene for BDNF

Brain activity in manic vs. depressive episode
Bipolar Disorder
• Bipolar I: full-blown episodes of mania
• Bipolar II: episodes of hypomania
• Cycles can be a couple of days to a couple of years.
• ~1% of people have at least a mild case in their lifetime
• Enlarged ventricles: decreased brain vol.
• Larger amygdala than normal
Treatments for Bipolar Disorder
• Lithium (for Bipolar I)– Discovered by accident (JF Cade, uric acid)– Not clear why it works (can be toxic)– Usually given during manic phase prevents
subsequent depression and mania– Li+ alters Na+ transport & “inhibits recycling of
membranes involved in second-messenger systems” reduces responsiveness to transmitters

Treatments for Bipolar Disorder
• Valproic acid (Depakote, Depakene) or carbamazepine (anticonvulsants)– Usually effective only in Bipolar II– Increase GABA activity, block synthesis of
arachidonic acid (produced during brain
inflammation)
• Patients don’t like to lose the euphoria and creativity of the manic phase.
Summary of Bipolar Disorder
• Genes on several chromosomes (incl. BDNF)
• Bipolar I vs. Bipolar II
• Men & women similar incidence
• Enlarged ventricles, large amygdala
• Treatments– Bipolar I: lithium– Bipolar II: Anticonvulsants GABA activity,
decrease arachidonic acid
Anxiety Disorders
• Panic disorder– Can be induced by lactate or CO2 in PD
sufferers (only occasionally in normal people)– Increased activity in parahippocampal gyrus, – Decreased activity in anterior temporal cortex
& amygdala (seems odd!)– May have 3, rather than 2, repeats of a
section on chromosome 15• Also have joint laxity (bend too far)

Anxiety Disorders
• Treatments for panic disorder – Benzodiazepines (e.g., Valium)
• Increase frequency of Cl- channel openings in response to GABA
• Have little or no effect alone: safer than barbiturates
• Allopregnanolone = endogenous agonist at benzodiazepine binding site.
– Buspirone (Buspar): 5-HT1a agonist (GI/O)– SSRIs: fluoxetine (Prozac), paroxetine (Paxil)
Benzodiazepine receptors in brain

PTSD
PTSD
• Monozygotic > dizogotic concordance– Genetics 1/3 of variance
• NMDA mechanisms in amygdala – May mediate both the conditioning and the
extinction• NMDA antagonists in amygdala prevent extinction• Hippocampus and PFC also lose effectiveness in
extinction

PTSD
PTSD
• Not due to high levels of glucocorticoids:– Usually PTSD sufferers have LOWER than normal
cortisol levels, despite high CRH• Maybe it’s the high CRH that symptoms• Or maybe it’s increased responsiveness to CRH or cortisol
• Individual differences in responsiveness to trauma
• Sometimes treated with β NE antagonists (propranolol) or protein synthesis inhibitors soon after the trauma or during recall of the trauma

OCD
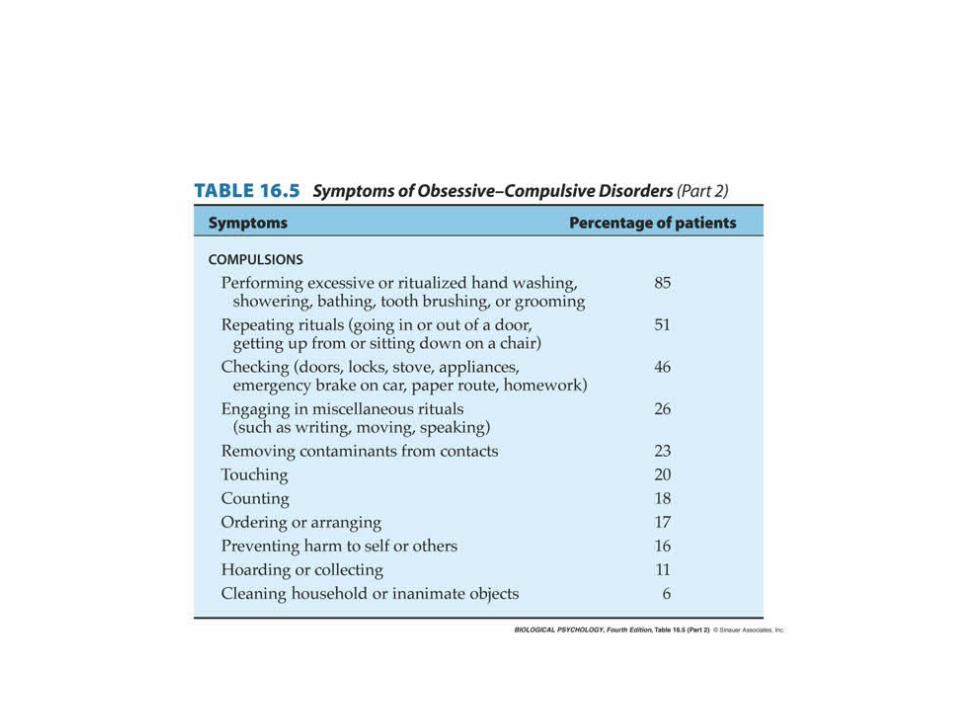
OCD
• Increased metabolism in orbitofrontal cortex, cingulate, and caudate nuclei.
• Decreased REM latency (~ to depression)
• At least 2 gene polymorphisms:– For BDNF, 5-HT2A receptor
• Treatment: SSRIs
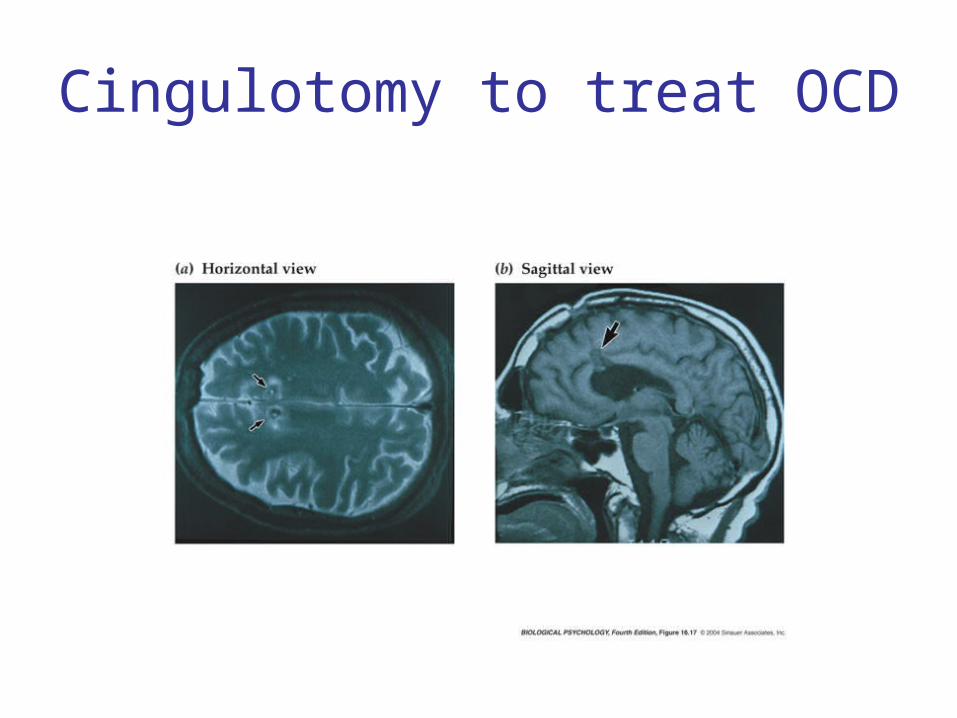
Cingulotomy to treat OCD

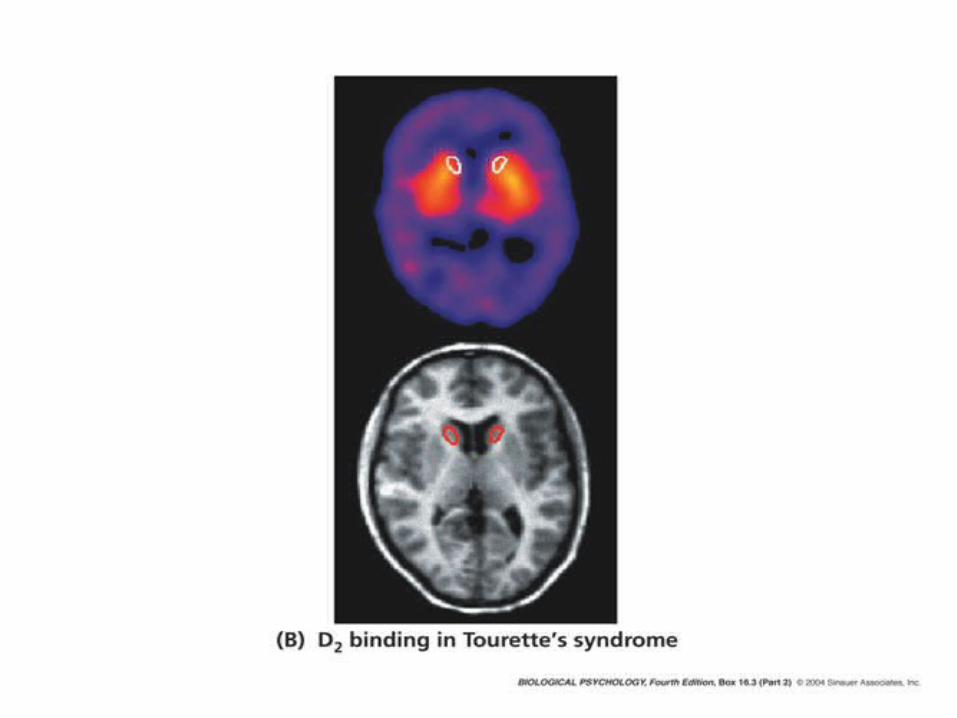
Tourette’s Syndrome

Tourette’s syndrome
• In many ways opposite Parkinson’s disease• Treated with dopamine antagonists• Monozygotic concordance: 53-77%; dizygotic
concordance: 8-23%• Witty Ticcy Ray (by Oliver Sacks): “We
Touretters…are forced into levity by our Tourette’s and forced into gravity when we take Haldol….You have a natural balance: we must make the best of an artificial balance.”

Summary of Mood Disorders
• Depression symptoms:– Sad & helpless every day for weeks– Loss of interests, energy, appetite– Feel worthless– Contemplate suicide– Difficulty in concentrating– Restless agitation– Little or no pleasure from eating or sex
Summary of Mood Disorders
• Genetic component: 60 vs 20% concordance for identical vs fraternal twins
• High activity in PFC and amygdala– PFC inhibits NAc—and therefore pleasure and behavioral
activation– Amygdala anxiety
• High cortisol levels may contribute to depression– Kills hippocampal cells, impairs memory
• Alteration of sleep cycles sometimes helps• SSRIs for unipolar depression
– ECT for severe cases that don’t respond to SSRIs
• Lithium for bipolar disorder– Or drugs that increase GABA effect for milder cases
Summary of Mood Disorders
• There is a genetic component for all.• High cortisol levels may contribute to depression
– Kills hippocampal cells, impairs memory
• Alteration of sleep cycles sometimes helps• SSRIs for unipolar depression
– ECT for severe cases that don’t respond to SSRIs
• Lithium for bipolar disorder– Or drugs that increase GABA effect for milder cases
• Anxiety: benzodiazepines, buspirone, SSRIs


















