Saturday, May 11, 2013 09:00 - 17:15 IFHIMA Educatio
118
Saturday, May 11, 2013 09:00 - 17:15 IFHIMA Education Day (Open to all delegates) 517d 08:30 - 17:30 NHIMA Meeting 522a 12:00 - 13:00 Break and Lunch 16:30 - 18:00 IFHIMA - National Directors Orientation Meeting 522bc
Transcript of Saturday, May 11, 2013 09:00 - 17:15 IFHIMA Educatio

Saturday, May 11, 2013 09:00 - 17:15 IFHIMA Education Day (Open to all delegates) 517d 08:30 - 17:30 NHIMA Meeting 522a 12:00 - 13:00 Break and Lunch 16:30 - 18:00 IFHIMA - National Directors Orientation Meeting 522bc
Sunday, May 12, 2013 09:00 - 16:45 IFHIMA General Assembly 517d 08:30 - 15:45 CNIA Workshop 525 The Science and Practice of Nursing Informatics 09:00 - 17:00 Program Coordinator’s Meeting 522a 12:00 - 13:00 Break and Lunch
17:00 - 18:30 Regional Meetings North America – Room 517d Africa and EM – Room 525ab Europe – Room 518a South East Asia – Room 522a Western Pacific – Room 518b
18:00 - 19:30 Welcome Reception in Exhibit Hall 517ab
(Open to all delegates to attend) Please note the IFHIMA Posters will be available for viewing in the Exhibit Hall, room 517ab, during the Welcome Reception, coffee breaks and lunch breaks. To view the IFHIMA Posters please go to the Wednesday afternoon schedule.

Monday, May 13, 2013
07:45 - 08:10 Opening Ceremonies Chair: Tamara Stefanits, Vice-President of CHIMA
517d
FS1 08:10 - 09:00 Speaker Showcase Canada - Jowi Taylor 517d
The Six String National Guitar Chair: Tamara Stefanits, Vice-President of CHIMA
FS2 09:00 - 09:40 Feature Speaker: Richard Alvarez 517d
Transforming Health Care in Canada Through Digital Health Chair: Tamara Stefanits, Vice-President of CHIMA
09:40 - 10:30 Feature Panel: Managing Consent in EHR Systems Chair: Tamara Stefanits, Vice-President of CHIMA
517d
PAN1 09:40 Managing Consent in EHR Systems
Stanley Ratajczak1 ; Joan Roch1; David Morgan2; Debra Grant3; Chantal Leonard4; Brendan Seaton5 1Canada Health Infoway, Montreal, QC, Canada; 2Newfoundland and Labrador Centre for Health Information, St. John's, NF, Canada; 3Office of the Privacy Commissioner of Ontario, Toronto, ON, Canada; 4Canadian Nurses Protective Society, Ottawa, ON, Canada; 5ITAC Health, Toronto, ON, Canada Session Sponsored by: Lanier Healthcare Canada
10:30 - 11:00 Coffee Break & Visit Exhibitors & Posters 517ab Sponsored by: Canadian Patient Safety Institute (CPSI)
11:00 - 12:30 Concurrent Sessions 1 - 1.1 EHR - Implementation & Adoption 524a
Chair: Carol Adam, IFHIMA PSC Member Session Sponsored by: Canada Health Infoway
CS1.1.1 11:00 Doing It Right: Deploying Alberta's Provincial Electronic Health Record
Barb Goertzen Alberta Health, Brooks, AB, Canada

CS1.1.2 11:20 How Hard Can It Be? Implementing an Integrated Electronic Medical
Record (EMR) Beyond the Basics to Benefits Realization
Diane Edlund Healthcare Consulting, Edmonton, AB, Canada
CS1.1.3 11:40 Spain IB-Salut Case Study: Implementing an Integrated Delivery Model for Population-based Disease Management and Integrated Clinical Pathways
Chris Hobson Orion Health, Toronto, ON, Canada
CS1.1.4 12:00 Proposed Implementation and Evaluation of a Thoracic Surgery Quality Monitoring, Information Management, and Clinical Documentation System in a Cancer Assessment Clinic
Jelena Ivanovic1; Tim Ramsay2; Donna Maziak3; Sebastien Gilbert3; Farid Shamji3; Sudhir Sundaresan3; Andrew Seely3 1University of Ottawa, Ottawa, ON, Canada; 2Ottawa Hospital Research Institute, Ottawa, ON, Canada; 3The Ottawa Hospital, Ottawa, ON, Canada
11:00 - 12:30 Concurrent Sessions 1 - 1.2 Data Quality - Compliance & Re-abstraction Studies 518a
Chair: Angelika Haendel, IFHIMA Board Member Session Sponsored by: MED2020
CS1.2.1 11:00 Coding Compliance Begins with Defining Your Core Designated Medical Record Set of Documents
Bonnie Cassidy Nuance Communications, Inc, Burlington, MA, United States
CS1.2.2 11:20 ***CANCELLED*** Enabling Medication Management Through Health Information Technology (Health IT)
Funmilola Elizabeth Taiwo Adytas Technologies, Ibadan, Oyo, Nigeria
CS1.2.3 11:40 Quality Audit of Coding Question Service
Margaret Penchoff Canadian Institute for Health Information, Ottawa, ON, Canada
CS1.2.4 12:00 Assessing the Quality of Canada’s Discharge Abstract Database
Rachel Benoit; Josie Bellemare; Maureen Kelly Canadian Institute for Health Information, Ottawa, ON, Canada
11:00 - 12:30 Concurrent Sessions 1 - 1.3 Privacy 524b
Chair: Marci MacDonald, IFHIMA Board Member Session Sponsored by: HealthPort

CS1.3.1 11:00 The Legal Foundations of Access, Privacy and Confidentiality and a Look
Ahead to the Future of Access
Marianthi Kakouratos O'Sullivan College, Montreal, QC, Canada
CS1.3.2 11:20 Security and Data Privacy: Technology is Not Enough
Kerry Matre Hewlett-Packard, Lyons, CO, United States
CS1.3.3 11:40 Collision Course or Collaboration Course? Healthcare Delivery and Technology Changes Meet Evolving Privacy Law
Brian Foran1; Joan Roch1; Wendy Robillard2; Heather McLaren3; Alison Blair4; David Morgan5; Debra Grant6
1Canada Health Infoway, Montreal, QC, Canada; 2Alberta Health and Wellness, Edmonton, AB, Canada; 3Manitoba eHealth, Winnipeg, MB, Canada; 4Ontario Ministry of Health and Long Term Care, Toronto, ON, Canada; 5Newfoundland and Labrador Centre for Health Information, St. John's, NB, Canada; 6Office of the Privacy Commissioner of Ontario, Toronto, ON, Canada
11:00 - 12:30 Concurrent Sessions 1 - 1.4 Workforce Transformation - Decision Support-Clinical Administration 524c
Chair: Bojay Hansen, CHIMA Board Member
CS1.4.1 11:00 Linking Strategy to Operational Execution Through Enterprise Business Intelligence
Maria Muia; Eugene Wong North York General Hospital, Toronto, ON, Canada
CS1.4.2 11:20 Health System Use & the Electronic Health Record - Opportunities to Support Decision Making at the Point of Care and From a Health System Perspective
Valerie Leung1; Alex Mair2 1Canada Health Infoway, Toronto, ON, Canada; 2Canada Health Infoway, Halifax, NS, Canada
CS1.4.3 11:40 Business Intelligence (BI) in Healthcare Adjusting Your Sail and Improving Financial Health
Lisa Gregoire Emerald Health Information Systems, Ottawa, ON, Canada
CS1.4.4 12:00 Specialized Skills Required by HIM Professionals for Decision Support in a National Organization
Janet Manuel Canadian Institute for Health Information, Summerville, NS, Canada

11:00 - 12:30 Concurrent Sessions 1 - 1.5 Developing Countries 519a Chair: Lili Levesque, CHIMA Member CS1.5.1 11:00 The Survey Report on the Needs of the Developing Countries
Stuart Green1; Yukiko Yokobori2; Lorraine Nicholson3 1Bradford Teaching Hospitals NHS Foundation Trust St Lukes Hospital, Bradford, West Yorkshire, United Kingdom; 2Japan Hospital Association, Tokyo, Japan; 3IFHIMA Immediate Past President, Rochdale, Lancaster, United Kingdom
CS1.5.2 11:20 Health Information Management Education and Training in India: A Situational Analysis
Sabu Karakkamandapam Manipal College of Allied Health Sciences, Manipal University, Manipal, Karnataka, India
CS1.5.3 11:40 Electronic Health Record (EHR) Implementation in Rwanda: The Role of and Need for HIM Expertise
Kelly Abrams1; Murray Abrams2 1CHIMA, Regina, SK, Canada; 2Regina Qu'Appelle Health Region, Regina, SK, Canada
CS1.5.4 12:00 Improvement Career Development for Medical Record an Health Information Government Employee on Advance Level in Indonesia
Elise Garmelia Pormiki, West Jakarta, DKI Jakarta, Indonesia
11:00 - 12:30 Concurrent Sessions CNIA 1 - 1.1 Clinical Standards and Patient Outcomes 525b
Chair: Leanne Currie, Associate Professor, University of British Columbia School of Nursing
CNIA1.1.1 11:00 Finding Value in the Collection of Standardized Clinical Outcomes
Peggy White; Ian Purdy Institute for Clinical Evaluative Sciences HOBIC, Toronto, ON, Canada
CNIA1.1.2 11:20 C-HOBIC -- Standardizing Clinical Outcomes in Canada
Kathryn Hannah1; Peggy White2 1C-HOBIC, Calgary, AB, Canada; 2Institute for Clinical Evaluative Sciences HOBIC, Toronto, ON, Canada
CNIA1.1.3 11:40 Technology-Enabled Evidence-Based Practice, Outcome Evaluation and Knowledge Creation
Rita Wilson; Irmajean Bajnok Registered Nurses' Association of Ontario, Toronto, ON, Canada

CNIA1.1.4 12:00 When Home Care Nurses Use Technology at the Point-of-Care, Do Client Outcomes Change?
Cheryl Reid Haughian1; Diane Doran2; Jennifer Carryer2 1Knowledge and Innovation ParaMed Home Health Care, Toronto, ON, Canada; 2Lawrence S. Bloomberg Faculty of Nursing, University of Toronto, Toronto, ON, Canada
12:30 - 13:45 Lunch Break & Visit Exhibitors & Posters 517ab FS3 13:45 - 14:30 Feature Speaker: Hugh MacLeod 517d
ASK.LISTEN.TALK The Patient Voice Meets the Determinants of Health Chair: Gail Crook, CEO & Registrar of CHIMA
FS4 14:30 - 15:15 CNIA Feature Speaker: Lynn Nagle 517d
Nursing Outcomes & Coded Data: What is the Value Proposition? Chair: Margaret Kennedy, CNIA President
15:15 - 15:40 Coffee Break & Visit Exhibitors & Posters 517ab Sponsored by: Terra Nova
15:40 - 16:50 Concurrent Sessions 2 - 2.1 EHR - Auto-Coding & Scanning 524a
Chair: Ann Marion, CHIMA Member Session Sponsored by: Canada Health Infoway
CS2.1.1 15:40 This Presentation will Discuss the Application of Computer-assisted Coding Technology in a Healthcare System. Technology Issues will be Presented as well as Benefits and Obstacles to Implementation.
Sandra Fuller eCatalyst Consulting, Grayslake, IL, United States
CS2.1.2 16:00 Journey to a Scanned Medical Record: Six Years On
Jennifer Bowman; Kate Horkings Southern Health, Clayton, Victoria, Australia
CS2.1.3 16:20 Expediting a Hospital's Adoption of Electronic Patient Records Through an Innovative Scanning & Document Management Process - A Health Information Management Case Study of Trillium Health Centre

Valerie Alston1; Scott McMillan2; Julie Sternik1 1Trillium Health Centre, Mississauga, ON, Canada; 2Salumatics Inc., Montreal, QC, Canada
15:40 - 16:50 Concurrent Sessions 2 - 2.2 Data Quality - Data Integrity 524b
Chair: Cheryle Facey, CHIMA Member Session Sponsored by: MED2020
CS2.2.1 15:40 Information Integrity in the Electronic Health Record
Lou Ann Wiedemann1; Lydia Washington2 1AHIMA, Chicago, IL, United States; 2AHIMA, Pearland, TX, United States
CS2.2.2 16:00 Building a Systems Approach to Data Quality
Agnes Vander Vecht1; Jennifer McCallum1; Kim Planques1; Lisa Clarke1; Monica Poole2 1London Health Sciences Centre, London, ON, Canada; 2BORN Ontario, London, ON, Canada
CS2.2.3 16:20 Implementation of Enterprise-Wide EMR and Data Governance - Lessons Learned
Rita Bowen HealthPort, Alpharetta, GA, United States
15:40 - 16:50 Concurrent Sessions 2 - 2.3 Data Quality - Clinical Coding 518a
Chair: Christine Bolduc, IFHIMA PSC Member Session Sponsored by: MED2020
CS2.3.1 15:40 Implementing New ICD Versions in a Complex Environment: The US Experience
Margaret Skurka1; Sue Bowman2; Rita Scichilone2 1Indiana University Northwest, Gary, IN, United States; 2AHIMA, Chicago, IL, United States
CS2.3.2 16:00 Coder Productivity When Moving from ICD-9-CM to ICD-10-CM/PCS: A Study
Susan Fenton1; Mary Stanfill2; Kathleen Beal3 1Texas State University, San Marcos, TX, United States; 2United Audit Systems, Inc., Walnut Hills, OH, United States; 3University of Cincinnati, Cincinnati, OH, United States
CS2.3.3 16:20 Improving Documentation for ICD-10: Challenges and Opportunities
Melanie Endicott AHIMA, Chicago, IL, United States

15:40 - 16:50 Concurrent Sessions 2 - 2.4 Education Advancement 518c Chair: Paula Weisflock, Director of CCHIM (CHIMA) CS2.4.1 15:40 Online Teaching, Making the Connection
Leslie Gordon1; Tracy Locke2; Lynette Williamson3 1University of Alaska Southeast, Sitka, AK, United States; 2Alfred State, Canandaigua, NY, United States; 3Santa Barbara City College, Oley, PA, United States
CS2.4.2 16:20 Online Learning: A Unique Saskatchewan Perspective
Ida Sadowski Saskatchewan Institute of Applied Science and Technology, Regina, SK, Canada
15:40 - 16:50 Concurrent Sessions 2 - 2.5 Workforce Transformation - Health Information Analysis and Other 524c
Chair: Kelly Abrams, Vice-President of CCHIM (CHIMA)
CS2.5.1 15:40 Changing Demands of Clinical Analytics and Quality Improvement: Opportunities and Lessons for HIM Professionals
Linda Kloss Kloss Strategic Advisors, Chicago, IL, United States
CS2.5.2 16:00 What Information Does the Patient Really Need - Challenges in Presenting Clinical Data to Non-experts
Markus Stein1; Wolfang Beinhauer2; Udo Bräu3; Elisabeth Büllesfeld2; Katrin Fusko1; Peter Görlich1; Dagmar Häbe2; Angelika Lackner3; Sabine Radestock1 1Ethianum Hospital, Heidelberg, Germany; 2Fraunhofer Institute for Industrial Engineering, Stuttgart, Germany; 3Meierhofer AG, Munich, Germany
CS2.5.3 16:20 Transformation of Health Information Management (HIM) Workforce for New Roles and Elevated Positions: Oh The Places You Will Go!
Barbara Odom-Wesley1; Diann Brown Smith2 1DeVry University, Irving, TX, United States; 2Texas Health Resources, Arlington, TX, United States
15:40 - 16:50 Concurrent Sessions CNIA 2 - 2.1 Issues Related to Clinical Adoption 525b
Chair: Margaret Ann Kennedy, CNIA President
CNIA2.1.1 15:40 Choosing a Theoretical Framework to Evaluate Electronic Health Record and Other Technology Implementations
Kathy Momtahan The Ottawa Hospital, Ottawa, ON, Canada

CNIA2.1.2 16:00 Creating a Culture of Clinical Adoption: Benefits Realization of Technology
Liz Nemeth Healthtech Consultants, Toronto, ON, Canada
CNIA2.1.3 16:20 Healthcare Knowledge for Manitoba eHealth Managers
Pat Rothney Global Village Consulting Inc., Winnipeg, MB, Canada
15:40 - 16:50 Concurrent Sessions CNIA 2 - 2.2 Patient Safety and Quality 518b
Chair: Eithne Reichert, Clinical Consultant for PHC Project, eHealth Saskatchewan
CNIA2.2.1 15:40 What Are Some of the Causal Relationships That Lead to Successful Order Set Adoption?
Susan Hall Kingston General Hospital, Kingston, ON, Canada
CNIA2.2.2 16:00 The Electronic Whiteboard: Can it Support Patient Safety and Quality of Patient Care?
Robyn Alpert; Arthom Barlis Mackenzie Health, Richmond Hill, ON, Canada
CNIA2.2.3 16:20 Does Work Experience Using Technology Influence NI Competencies by End of 4th Year?
Marie-Pierre Dionne Montfort Hospital, Ottawa, ON, Canada
16:50 - 17:00 Day In Review & Announcements 517d
17:00 - 18:00 Lanier Product Showcase 518a
Speech Everywhere Jake Cormier; Chris Welbourn
Lanier Healthcare Canada is happy to invite you to the “Speech Everywhere” showcase. We will discuss many lessons learned during our Speech implementations and show you a number of just released solutions for Speech. Please drop by and we will enter your name into our “Free iPad contest for the show”.

Tuesday, May 14, 2013 08:00 - 08:15 Welcome & Developing Countries Spotlight 517d Chair: Tamara Stefanits, Vice-President of CHIMA FS5 08:15 - 09:00 Motivational Speaker: Jessica Holmes 517d
Laugh it Off and Bring it On Chair: Tamara Stefanits, Vice-President of CHIMA
FS6 09:00 - 09:45 Feature Speaker: Lorraine Nicholson 517d
The Sun Never Sets…! Chair: Margaret Skurka, IFHIMA President Session Sponsored by: Canadian Institute for Health Information
FS7 09:45 - 10:30 Feature Speaker: John Wright 517d
Better Data. Better Decisions. Healthier Canadians. Chair: Margaret Skurka, IFHIMA President
10:30 - 11:00 Coffee Break & Visit Exhibitors & Posters 517ab Sponsored by: Crescendo Systems Corporation 11:00 - 12:30 Concurrent Sessions 3 - 3.1 EHR - Governance 524a Chair: Margaret Skurka, IFHIMA President
CS3.1.1 11:00 Information Governance and Information Lifecycle - Unlocking the Value of Your Structured and Unstructured Data
Michele O'Connor1; Lorraine Fernandes2 1IBM, Clifton, NJ, United States; 2IBM, San Ramon, CA, United States
CS3.1.2 11:20 Big Data and Predictive Analytics are Transforming Healthcare
Lorraine Fernandes1; Michele O'Connor2 1IBM, San Ramon, CA, United States; 2IBM, Clifton, NJ, United States
CS3.1.3 11:40 Creating and Operationalizing an Enterprise Information Management Governance Framework in Alberta Health Services.
Kathleen Addison; Sharilyn Kmech Health Information Management - Alberta Health Services, Calgary, AB, Canada

CS3.1.4 12:00 The Impact of Multiple Custodians of EHR/EMR Content
Karanne Miller Lambton; Cindy Nikiforuk Alberta Health Services, Calgary, AB, Canada
11:00 - 12:30 Concurrent Sessions 3 - 3.2 Data Quality - Data Integrity 524b
Chair: Jessica Giesbrecht, CHIMA Program Manager Session Sponsored by: 3M Health Information Systems
CS3.2.1 11:00 International DRG Panel
Makoto Anan1; Angela Kennedy2; Joon Hong3; Angelika Haendel4 1Representing Japan; 2Representing USA; 3Representing Korea; 4Representing Germany
CS3.2.2 11:40 CIHI's New Data Quality Initiative: Using Analytics to Support Ontario's Health Based Allocation Model
Chrissy Willemse1; Maureen Kelly1; Stacey Colameco2 1Canadian Institute for Health Information, Ottawa, ON, Canada; 2Ontario Ministry of Health and Long-Term Care, Toronto, ON, Canada
CS3.2.3 12:00 A Strategy for Training Data Users
Aisling Mulligan; Jacqui Curley Health Research and Information Division, The Economic and Social Research Institute, Dublin, Ireland
11:00 - 12:30 Concurrent Sessions 3 - 3.3 Data Quality - Clinical Coding
518a
Chair: Shirley Learmoth, CHIMA Board Member Session Sponsored by: 3M Health Information Systems
CS3.3.1 11:00 Present on Admission and Measuring the Success of a Clinical Documentation Improvement Program
Nancy Ignatowicz Loyola University Medical Center, Maywood, IL, United States
CS3.3.2 11:20 Analysis of the Questions about the Morbidity Coding Posted on the Online Coding Clinic
YooKyung Boo1; Whiejong M. Han1; Hyunsook Lim2; Youngjin Choi3 1Eulji University, Seongnam, Korea, Republic of; 2Department of Public Health Administration, Hanyang Woman's University, Seoul, Korea, Republic of; 3Department of Healthcare Administration, Eulji University, Seongnam, Korea, Republic of
CS3.3.3 11:40 Hospital Standardized Mortality Ratio Project Success Guides Creation of a Documentation and Coding Quality Framework
Kathy Lavelle

Lakeridge Health, Oshawa, ON, Canada
CS3.3.4 12:00 Impact of Information Technology on Clinical Decision Making and Clinical Documentation in Global Health: A Gift or Challenge for Clinical Coding?
Chet Deshmukh VASTACCESS - A Global Institute for Clinical Health Information Management and Education, Apex, NC, United States
11:00 - 12:30 Concurrent Sessions 3 - 3.4 Workforce Transformation - Other
524c
Chair: Sharon Baigent, CHIMA Board Member
CS3.4.1 11:00 Transforming Health Information Management - The Evolution of the Health Information Management Professional
Gail Crook1; Kelly Abrams2 1CHIMA, London, ON, Canada; 2CHIMA, Regina, SK, Canada
CS3.4.2 11:20 Health Information Management Professionals in Canada: Supply and Graduate Trends
Julie Goulet; Lan Wang; Yasmine Léger Canadian Institute for Health Information, Ottawa, ON, Canada
CS3.4.3 11:40 HIT Workforce Needs Assessment Results: Implications for HIM
Susan Fenton Texas State University, San Marcos, TX, United States
CS3.4.4 12:00 Consumer Engagement: An Opportunity for Health Information Management to Contribute to Better Health Care
Lydia Washington1; Julie Wolter2; Marsha Dolan3 1American Health Information Management Association (AHIMA), Pearland, TX, United States; 2St. Louis University, St. Louis, MO, United States; 3Missouri Western State University, St. Joseph, MO, United States
11:00 - 12:30 Concurrent Sessions 3 - 3.5 Privacy 518b
Chair: Leah Goguen, CHIMA Board Member Session Sponsored by: HealthPort
CS3.5.1 11:00 Ensuring Privacy and Security of Patient Information in a Mobile World
Debra Primeau1; Cynthia Doyon2 1Prime Health Information Consulting, Torrance, CA, United States; 2Precyse Solutions, Wayne, PA, United States
CS3.5.2 11:20 Social Media and Health Data Privacy Majorie Hendricks; Jermaine Martin

Jamaica Medical Records Assoc. Ministry of Health, Kingston, Jamaica
CS3.5.3 11:40 Mobile Devices- Are They Secure Enough for our Patient's Data?
Aaron Hendriks University Health Network - Shared Information Management Services, Toronto, ON, Canada
CS3.5.4 12:00 Monitoring Access Patterns: If Credit Card Companies Can Develop Fraud Alert Technology, So Can We!
Debbie Mikels; Karen Grant Partners HealthCare System, Wellesley, United States
11:00 - 12:30 Concurrent Sessions 3 - 3.6 Workforce Transformation - Coding
518c
Chair: Nancy Haugen, CHIMA Board Member CS3.6.1 11:00 Moving to ICD-10? Myths Debunked and Explained
Doris Gemmell Nuance Communications, Ottawa, ON, Canada
CS3.6.2 11:20 HIM and Clinical Coding Revolution in the Kingdom of Saudi Arabia!
Hussein Albishi Ministry of Health, Riyadh, Saudi Arabia
CS3.6.3 11:40 A Comprehensive Workforce/Education Partnership Model for ICD-10 Implementation that Improves Understanding of Codes and Employee Satisfaction
Lily Hsu1; Diana Lindo2; Kira Khazatsky3; Jacqueline Donahue3 1Massachusetts College of Pharmacy and Health Sciences, Boston, MA, United States; 2Boston Children's Hospital, Boston, MA, United States; 3Jewish Vocational Services, Boston, MA, United States
CS3.6.4 12:00 Experiences Training of Transfer ICD 9 to ICD 10 at Primary Health Care in Indonesia to Improve the Implementation the HIS by MOH
Elise Garmelia1; Vensya Sitohang2 1Pormiki, West Jakarta, DKI Jakarta, Indonesia; 2Center for Data Health and Information, Ministry of Health, Jakarta, Indonesia
11:00 - 12:30 Concurrent Sessions 3 - 3.7 Developing Countries 519b
Chair: Kim Durofil, Program Coordinator, Health Information Management Program, George Brown College
CS3.7.1 11:00 An Effort to Improve Health Care in Ethiopia: Building the HIM Profession in the Country from "Scratch"
Sheila Carlon Regis University-RHCHP, Denver, CO, United States

CS3.7.2 11:20 Improving Availability of Laboratory Test Results
Sooneeraz Monohur; Satianand Bheekun; Goolam Rassool Lall Mahomed; Champa Ramdhean; Neerunjun Gopee; Nasser Jeeanody Ministry of Health and Quality of Life, Port Louis, Mauritius
CS3.7.3 11:40 Impact of Technology on Health Information: An Overview of Health Management Information System of Rajasthan, India.
Divya K Bhati Indian Institute of Health Management Research (IIHMR), Jaipur, Rajasthan, India
CS3.7.4 12:00 Two Way Web-based Interactive Video EConsult System (TWIVeS): A Sustainable Telehealth Solution for Remote and Rural Area
Kenneth Nwosu; Norm Archer McMaster University, Hamilton, ON, Canada
11:00 - 12:30 Concurrent Sessions CNIA 3 - 3.1 Nursing Leadership in Informatics
525b
Chair: Susan Hall, Consultant, Clinical Documentation Department, Kingston General Hospital
CNIA3.1.1 11:00 Establishing Innovative Nursing Informatics Leadership Roles
Sally Remus1; Diane Salois-Swallow2 1Mackenzie Health, Richmond Hill, ON, Canada; 2Mackenzie Health, Southlake Regional Health Centre and Stevenson Memorial, Richmond Hill, ON, Canada
CNIA3.1.2 11:20 Informaticians: The Next Generation
Lynn Nagle Nagle and Associates, Toronto, ON, Canada
CNIA3.1.3 11:40 Leveraging the Power of the TIGER in Canada
Margaret Kennedy1; Sally Schlak2 1Global Village Consulting Inc., Merigomish, NS, Canada; 2The TIGER Initiative Foundation, Chicago, IL, United States
CNIA3.1.4 12:00 Findings in Clinical Adoption of Nurses and Nurse Practitioners Using an EMR
Eithne Reichert; Margaret Timmons RWI Informatics Inc., Saskatoon, SK, Canada
12:30 - 13:45 Lunch Break & Visit Exhibitors & Posters 517ab

FS8 13:45 - 14:30 CNIA Feature Speaker: Maureen McTeer 517d
Technologies and Health: A Canadian Nursing Call to Action Chair: Maureen Charlebois, Chief Nursing Executive & Group Director – Clinical Adoption, Canada Health Infoway
14:30 - 15:00 CNIA Feature Panel & CHIMA Representative 517d
Health System Transformation – Dialogue to Action Chair: Pat Rothney, Business Analysis and Project Management & Clinical SME, Global Village Consulting Inc.
PAN2 14:30 Health System Transformation - Dialogue to Action
Lynn Nagle1; Vickie Kaminski2; Cheryl Reid-Haiughian3; Pamela Thorsteinsson4; Candace Gibson5 1CNIA, University of Toronto, Nagles & Associates, Inc, Toronto, ON, Canada; 2Eastern Regional Health Authority, Newfoundland and Labrador, NL, Canada; 3ParaMed Home Health Care, Ottawa, ON, Canada; 4Fraser Health Authority, Surrey, BC, Canada; 5University of Western Ontario, London, ON, Canada Session Sponsored by: Mckesson Canada
15:00 - 15:40 Coffee Break & Visit Exhibitors & Posters 517ab 15:40 - 16:50 Concurrent Sessions 4 - 4.1 EHR - Standards 524a Chair: Patricia Hewes, CHIMA Program Coordinator CS4.1.1 15:40 Global Standards: Making a Difference in Health Information Management
Rita Scichilone American Health Information Management Association, Washington, DC, United States
CS4.1.2 16:00 Standards for Health System Use: Development of a Canadian Institute for Health Information Reference Data Model
Dawn Nicolson; Cristina Tomsa; Mark Fuller Canadian Institute for Health Information, Ottawa, ON, Canada
CS4.1.3 16:20 Building the EMR Value Proposition Through an Integration Engine
Gary Folker; Chris Hobson Orion Health, Toronto, ON, Canada
15:40 - 16:50 Concurrent Sessions 4 - 4.2 Workforce Transformation - Identity Management 518b

Chair: Carol Adam, IFHIMA PSC Member
CS4.2.1 15:40 To Improve Response Rate for Consultation by 6-Sigma Management Technique in a General Hospital
Misook Kim Shinheung College, Eujungbu, Kyunggi, Korea, Republic of
CS4.2.2 16:00 Health Information Management and its Impact on Health Care Consumers
Julie Wolter1; Marsha Dolan2 1Saint Louis University, St. Louis, MO, United States; 2Missouri Western State University, St. Joseph, MO, United States
CS4.2.3 16:20 Defining Hybrid Opportunities for the Health Sector: eHealth Occupations
Sandra Irobi; Meenakshi Gupta Information and Communications Technology Council of Canada, Ottawa, ON, Canada
15:40 - 16:50 Concurrent Sessions 4 - 4.3 Education Advancement 518c Chair: Kelly Abrams, Vice-President of CCHIM (CHIMA)
CS4.3.1 15:40 Examples of Electronic Medical Record Technology in a Bachelor Degree Health Information Management Curriculum
Megan Tober; Toni Windquist; Marybeth Pieri-Smith; Thomas J. Hunt Davenport University, Grand Rapids, MI, United States
CS4.3.2 16:00 The Relationship among Burnout, Personality, and Stress in Healthcare Workers
Angela Kennedy Department of Health Informatics & Information Management, College of Applied and Natural Sciences, Ruston, LA, United States
CS4.3.3 16:20 Preparing Nursing Graduates for the Electronic World of Health Care Delivery
Anna Sherlock1; Kristine Crosby2 1Canada Health Infoway, Toronto, ON, Canada; 2Canadian Association of Schools of Nursing, Ottawa, ON, Canada
15:40 - 16:50 Concurrent Sessions 4 - 4.4 Data Quality - Clinical Coding 518a
Chair: Marci MacDonald, IFHIMA Board Member Session Sponsored by: 3M Health Information Systems
CS4.4.1 15:40 Progress Report on an International Examination for Morbidity Coders Joon Hong1; Carol A. Lewis2

1WHO-FIC Education and Implementation Committee, Goyangsi, Kyunggido, Korea, Republic of; 2WHO-FIC Education and Implementation Committee, Rockville, MD, United States
CS4.4.2 16:00 Assessing the Accuracy of Coding in the Japanese Case-mix System (DPC: Diagnosis Procedure Combination) and the Role of HIM for Improvement
Makoto Anan National Kyushu Medical Center, Fukuoka-Shi, Japan
CS4.4.3 16:20 Improvements in the Coding of Strokes in Canada's Discharge Abstract Database
Josie Bellemare; Jin Wang; Maureen Kelly Canadian Institute for Health Information, Ottawa, ON, Canada
15:40 - 16:50 Concurrent Sessions 4 - 4.5 Data Quality - Data Integrity 524b
Chair: Paula Weisflock, Director of CCHIM (CHIMA) Session Sponsored by: 3M Health Information Systems
CS4.5.1 15:40 Ensuring the Quality of Health Information: The Canadian Experience
Maureen Kelly; Heather Richards Canadian Institute for Health Information, Ottawa, ON, Canada
CS4.5.2 16:00 Are Electronic Patient Records Associated with Better Data Quality than Paper-based Records?
Ashif Kachra1; Marian J Vermeulen1; Xuesong Wang2; Chelsea Hellings2; Michael J Schull1 1Sunnybrook Research Institute / Institute for Clinical Evaluative Sciences, Toronto, ON, Canada; 2Institute for Clinical Evaluative Sciences, Toronto, ON, Canada
CS4.5.3 16:20 Building a Database for Estimated Patient Medication History from Prescription Data in CPOE
Kei Teramoto1; Shigeki Kuwata2; Takeda Toshihiro3; Taizo Murata3; Shiro Manabe3; Naoki Mihara3; Kondo Hiroshi4; Yasushi Matsumura3 1Osaka University Hospital, Suita, Japan; 2Department of Medical Informatics, National Cerebral and Cardiovascular Center, Osaka, Japan, Suita, Osaka, Japan; 3 Department of Medical Informatics, Osaka University Hospital, Suita, Osaka, Japan; 4 Department of Medical Informatics, Tottori University Hospital, Yonago, Tottori, Japan
15:40 - 16:50 Concurrent Sessions 4 - 4.6 Clinical 524c Chair: Candace Gibson, Chair of CHIMA Board of Directors
CS4.6.1 15:40 Communicating the Pan-Canadian Nursing Perspective and Contribution to an Evolving Electronic Health Record

Cindy Hollister
Canada Health Infoway, Toronto, ON, Canada
CS4.6.2 16:00 The Doctor's Directory - An Innovative Health Systems Information Tool for Junior Doctors
Jonathan Clarke1; James Houston2; Jim Buckley2 1Department of Health, Informatics Directorate, London, United Kingdom; 2North West London Hospitals NHS Trust, Harrow, London, United Kingdom
CS4.6.3 16:20 Physician Documentation Improvement Project at Vancouver Coastal Health Authority
Gerald Yu Providence Health Care - Lower Mainland Health Information Management, Vancouver, BC, Canada
15:40 - 16:50 Concurrent Sessions CNIA 4 - 4.1 Technology to Enhance Nurses' Work
525b
Chair: Pat Rothney, Business Analysis and Project Management and Clinical SME at Global Village Consulting Inc.
CNIA4.1.1 15:40 Wireless Communication Device Implementation in Environments with Unique Needs: Results from an Adult Intensive Care Unit
Susan Hall; Rosemary Wilson; Lenora Duhn; Paola Gonzales; Yolande Chan; Elizabeth VanDenKerkof Kingston General Hospital, Kingston, ON, Canada
CNIA4.1.2 16:00 Remote Monitoring of Congestive Heart Failure Clients in Home Care: Innovation, Cost Effectiveness and Best Possible Client Outcomes
Cheryl Reid Haughian; Emily Seto; Jonathan Tomkun; Caterina Masino; Joseph Cafazzo; Deb Mulholland Knowledge and Innovation ParaMed Home Health Care, Toronto, ON, Canada
CNIA4.1.3 16:20 Positive Patient Identifiers at CVH..."It's a Perfect Match"
Lina Ranieri Trillium Health Partners, Toronto, ON, Canada
16:50 - 17:00 Day In Review & Announcements 517d 19:00 – 22:30 Night of 1000 Festivals – Social Event 710a

Wednesday, May 15, 2013 08:00 – 08:10 Welcome 517d Chair: Candace Gibson, Chair of CHIMA Board of Directors 08:10 – 09:15 Feature Panel: HIM/HI & CNIA Representative 517d
Chair: Sandy Fuller, Senior Vice President and Executive Consultant, eCatalyst Consulting
PAN3 08:10 HIM/HI Workforce Transformation
Margaret Kennedy1; Gail Crook2; Sallyanne Wissmann3; Namir Anani4; Don Newsham5; Lynne Thomas Gordon6 1Global Village Consulting Inc, Nova Scotia, NS, Canada; 2CHIMA, London, ON, Canada; 3Mater Health Services, South Brisbane, QLD, Australia; 4 Information and Communications Technology Council, Ottawa, ON, Canada; 5Canada’s Health Informatics Association, Toronto, ON, Canada; 6AHIMA, Chicago, IL, United States
09:15 – 10:25 Concurrent Sessions 5 – 5.1 HER 524a Chair: Angelika Haendel, IFHIMA Board Member
CS5.1.1 09:15 The Quality of Surgery-Specific Information on Post-operative Discharge Letters – A Retrospecitve Analysis and Investigation of Stakeholder Data Requirements
Jonathan Clarke; Charles Gutteridge Department of Health, Informatics Directorate, London, United Kingdom
CS5.1.2 09:35 Alternatives for Secure Telemedicine and for Video Conferences Including PHI.
Aaron Hendriks University Health Network –Shared Information Management Services, Toronto, ON, Canada
CS5.1.3 09:55 “The Re-ACT© Connection”
Sue Kelly We Care Home Health Services, Toronto, ON, Canada
09:15 – 10:25 Concurrent Sessions 5 – 5.2 Data Quality – Clinical Coding 518a
Chair: Candace Gibson, Chair of CHIMA Board of Directors

CS5.2.1 09:15 Does Concurrent Coding Improve Physician Documentation and Ultimately the Quality of Health Information? – Concurrent Coding Pilots within Alberta Health Services
Shirley Learmonth; Donna Sired; Karen Armitage; David Zygun; Reza Shahpori Alberta Health Services, Calgary, AB, Canada
CS5.2.2 09:35 Balancing Coding Quality, Throughput and Outcomes at a Teaching Hospital
Katherine Henning; Wei Xiong; Joanna Li UHN, Toronto, ON, Canada
CS5.2.3 09:55 The Role of the HIM Professional and Technology in Ensuring Data Integrity
Kathy Hartman, RN1; Michelle Dougherty, RHIA, CHP2; William Rudman, PhD2; Ann Chenoweth3; Sandra Seabold1 1Cleveland Clinic Health Systems, Cleveland, OH, United States; 2American Health Information Management Association, Chicago, IL, United States; 33M Health Information Systems, Salt Lake City, UT, United States
09:15 – 10:25 Concurrent Sessions 5 – 5.3 Workforce Transformation 524c Chair: Leah Goguen, CHIMA Board Member
CS5.3.1 09:15 Implementing a Regional, Off the Shelf, Surgical eBooking & Wait Times System – an eHealth Success Story
Karol Eskedjian1; Leslie Motz1; John Sinclair2 1Lakeridge Health Corporation, Oshawa, ON, Canada; 2Novari Health, Kingston, ON, Canada
CS5.3.2 09:35 A Three Year Status Report on the Montreal Regional Deployment of the Electronic Health Record
Christine J Bolduc Hôpital Louis-H. Lafontaine – Institut universitaire en santé mentale, Montréal, QC, Canada
CS5.3.3 09:55 Today’s Case Costing Environment: Emerging Roles and Opportunities for the Health Information Management (HIM) Professional – Workforce Transformation
Rosemarie Lourenco University Health Network, Toronto, ON, Canada
09:15 – 10:25 Concurrent Sessions 5 – 5.4 Clinical 524b Chair: Bill Pascal, CHIMA Board Member

CS5.4.1 09:15 Danish Health Sector With National Multidisciplinary Groups: Health Information Management of “Upper Gastrointestinal Cancer Group (UGCG)”
Darley Petersen Odense University Hospital, Odense, Denmark
CS5.4.2 09:35 Making it happen! Clinician Peer Support Network Program To Advance Adoption of Electronic Health Record Systems in a Clinical Setting
Anne Tran Fazzalari Canada Health Infoway, Toronto, ON, Canada
CS5.4.3 09:55 Experiencing the Challenges of Integrating Behavioral Health and Primary Health Services
Ruby Nicholson; Patti Nenna The Kent Center for Human and Organizational Development, Warwick, RI, United States
09:15 – 10:25 Concurrent Sessions 5 – 5.5 Educational Advancement 518c Chair: Margaret Skurka, IFHIMA President
CS5.5.1 09:15 The Effectiveness and Refinements of Special Program for Passing Japanese Health Information Manager Certification Exam in Fujita Health University
Haruka Murai; Tetsuya Kamei; Fumiaki Horiba; Masatsugu Iwase; Nobuko Kurono; Yukinori Murata; Koichi Muto; Michio Naito; Masanori Shinzato; Jiharu Hamako Fujita Health University, School of Health Science, Toyoake, Aichi, Japan
CS5.5.2 09:35 Knowing Is Better Than Not Knowing – An Educational Campaign For Clinicians
Anna Sherlock Canada Health Infoway, Toronto, ON, Canada
CS5.5.3 09:55 Quality Assurance in HIM Education at OHIMI, Sultanate of Oman
George Kennedy OHIMI, Oman
09:15 – 10:25 Concurrent Sessions CNIA 5 – 5.1 Informatics Competencies in Nursing Education 525b
Chair: Cheryl Reid- Haughian, Director of Professional Practice, Knowledge and Innovation at ParaMed Home Health Care

CNIA5.1.1 09:15 iNurse, iTeach: Barriers and Facilitators in Using Mobile Technology
Shauna Davies1; Sandra Bassendowski1; Pamela Petruucka1; Lorna Breitkreuz2; Christine Demyen2 1University of Saskatchewan, Saskatoon, SK, Canada; 2All Nations’ Healing Hospital, Fort Qu’Appelle, SK, Canada
CNIA5.1.2 09:35 Wound Healing Rates Before and After Alert to Wound Management Specialist
Leanne Currie1; Shannon Hanfield2; David Johns2; Lori Block2 1School of Nursing, University of British Columbia, Vancouver, BC, Canada; 2Vancouver Coastal Health Authority, Vancouver, BC, Canada
CNIA5.1.3 09:55 The Integration of Mobile Learning and Teaching in Nursing Education
Glynda Doyle British Columbia Institute of Technology, Burnaby, BC, Canada
10:25 – 11:00 Coffee Break 517d Foyer Sponsored by: Sigma Global 11:00 – 12:30 CNIA Board Meeting 522a 11:00 - 12:10 Concurrent Sessions 6 - 6.1 EHR - Information Systems 524a Chair: Bojay Hansen, CHIMA Board Member
CS6.1.1 11:00 Surgical Data Integration into a Coding Software System. Development of a Custom Screen for Interactive Interfacing of Operative Room Data
Joyce Taki1; Ladan Irannejad2 1Providence Health Care/Lower Mainland Health Information Management, Port Moody, BC, Canada; 2Providence Health Care/Lower Mainland Health Information Management, Vancouver, BC, Canada
CS6.1.2 11:20 An Operation Model of Digital Medical Image Exchange with Potable Media among Hospitals for Regional Medical Collaboration in Japan
Shigeki Kuwata; Hitomi Yamada; Megumi Inagaki; Yuki Hamada; Taiki Ozaki; Satomi Miyajima Department of Medical Informatics, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan
CS6.1.3 11:40 Quality Criteria for Electronic Health Record Systems (EHRs)
Rolf Engelbrecht1; Angelika Haendel2 1ProRec-DE, Ismaning, Germany; 2Universitätsklinikum Erlangen, Erlangen, Germany

11:00 - 12:10 Concurrent Sessions 6 - 6.2 Data Quality - Coding & Documentation 518a
Chair: Christine Bolduc, IFHIMA PSC Member
CS6.2.1 11:00 Re-engineering Health Records Coding Processes to Streamline Analysis of Key Performance Indicators and Reduce Costs
Anthony Hoad-Reddick1; Steven Green2 1York Central Hospital, Richmond Hill, ON, Canada; 2Salumatics Inc., Mississauga, ON, Canada Session Sponsored by: Salutnatics
CS6.2.2 11:20 How Meaningful is the Provider Documentation in the EHR? Success Strategies Associated with Bridging Clinical Documentation Gaps in the Electronic Record
Cassi Birnbaum Peak Health Solutions, San Diego, CA, United States
CS6.2.3 11:40 Measuring Quality Against the Bottom Line
Maria French Terra Nova, St. Johns, NF, Canada
11:00 - 12:10 Concurrent Sessions 6 - 6.3 Clinical 524b Chair: Bill Pascal, CHIMA Board Member
CS6.3.1 11:00 Expected Benefits of Primary Health Care Electronic Medical Record Content Standards (PHC EMR CS) for Patients and Health System Managers in Canada
Alison Bidie; Patricia Sullivan-Taylor Canadian Institute for Health Information, Toronto, ON, Canada
CS6.3.2 11:20 Transforming the Next Generation: Clinicians-in-Training
Anne Tran Fazzalari1; Maureen Charlebois1; Irving Gold2; Cynthia Baker3; Harold Lopatka4; Kristine Crosby3 1Canada Health Infoway, Toronto, ON, Canada; 2Association of Faculties of Medicine of Canada, Ottawa, ON, Canada; 3The Canadian Association of Schools of Nursing, Ottawa, ON, Canada; 4Association of Faculties of Pharmacy of Canada, Edmonton, AB, Canada
11:00 - 12:10 Concurrent Sessions 6 - 6.4 Developing Countries 519a Chair: Nancy Haugen, CHIMA Board Member

CS6.4.1 11:00 The Needs for Electronic Medical Records in Large Level Hospital in Nepal
Laxman Paudel1; Lorraine Nicholson2 1Western Regional Hospital, Pokhara, Gandaki Zone, Nepal; 2International Federation of Health Information Management Associations, Rochdale, Greater Manchester, United Kingdom
CS6.4.2 11:20 Development and Implementation of a Health Information Management System for St. Lucia
Margaret Samuel1; Brunette Willius1; Grantley Charlemagne2 1St Jude Hospital, Vieux-Fort, Saint Lucia; 2Public Service, Castries, Saint Lucia
CS6.4.3 11:40 Survey on Implementation and Use of Electronic Health Records in Nigeria
Lorraine Nicholson1; Olawole Ajayi2 1International Federation of Health Information Management Associations, Rochdale, Greater Manchester, United Kingdom; 2Health Information Managers Association of Nigeria, Lagos, Nigeria
11:00 - 12:10 Concurrent Sessions 6 - 6.5 EHR - Terminologies 518b Chair: Kelly Abrams, Vice-President of CCHIM (CHIMA)
CS6.5.1 11:00 Implementing Primary Health Care EMR Content Standards and Terminology Reference Sets in Canada: Tips for Success
Alison Bidie1; Beverly Knight2; Patricia Sullivan-Taylor1 1Canadian Institute for Health Information, Toronto, ON, Canada; 2Canada Health Infoway, Toronto, ON, Canada
CS6.5.2 11:20 Roles and Competencies for Managing Terminology Assets
Sue Schneider1; Kathy Giannangelo2; Kelly Abrams3; Rita Scichilone4 1eHealth Ontario, Toronto, ON, Canada; 2International Health Terminology Standards Development Organisation, Copenhagen, Denmark; 3Canadian College of Health Information Management, London, ON, Canada; 4American Health Information Management Association, Chicago, IL, United States
CS6.5.3 11:40 Health Data Dictionary Access: Making a Commercial Terminology Server Product Publicly Available
Marc Berlinguet1; Kasey Poon2; Oktavian Weiser3 13M HIS, Wallingford, CT, United States; 23M HIS, Salt Lake City, UT, United States; 33M HIS, Frankfurt, Germany
11:00 - 12:10 Concurrent Sessions 6 - 6.6 Records Management & Change 524c
Chair: Sharon Baigent, CHIMA Board Member

CS6.6.1 11:00 Post-Earthquake Health Information Management: Status and Challenges
Yukiko Yokobori1; Tuneo Sakai1; Takahisa Takeda1; Toshio Oi2 1Japan Hospital Association, Chiyoda-ku, Tokyo, Japan; 2Japan Society of Health Information Management, Tokyo, Japan
CS6.6.2 11:20 Alberta Health Services Recovery of Data in the Wake of a Major Health Information System Failure
Shirley Learmonth Alberta Health Services, Calgary, AB, Canada
CS6.6.3 11:40 Measuring Staff Perception of Change
Margaret Penchoff Canadian Institute for Health Information, Ottawa, ON, Canada
12:10 - 12:20 Closing Session 517d 14:00 - 14:45 CHIMA AGM 518c 15:00 - 17:00 CHIMA Board Meeting 522a

Posters
P1 Locating Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT®) Concepts for the Canadian Emergency Department Diagnosis Shortlist
Roberta Cardiff Canadian Institute for Health Information, Toronto, ON, Canada
P2 ROI and Breach: Reducing Your Risk in a Digital World
Rita Bowen HealthPort, Alpharetta, GA, United States
P3 An Effective Approach for Enhancing the Quality of Medical Records by Auditing Electronic Medical Records
Hitomi Yamada; Shigeki Kuwata Department of Medical Informatics, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan
P5 Modular-phase Implementation of Electronic Health Information in Hospitals with Complete Paper Medical Record - A Success Story
Francis Kirubagaran Qatar Orthopaedic Sports Medicine Hospital, Doha, Doha, Qatar
P6 A Vision for a Paperless Future: The Understanding of Indonesian Medical Records Students About Electronic Medical Records
Dwi Margawati; M. Kes Rosyidah Department of Public Health, University of Ahmad Dahlan, Yogyakarta, Indonesia
P7 Challenges and Prospects for Electronic Health Records in Nigeria
Lorraine Nicholson1; Olawole Ajayi2 1International Federation of Health Information Management Associations, Rochdale, Greater Manchester, United Kingdom; 2Health Information Managers Association of Nigeria, Lagos, Lagos State, Nigeria
P8 Implementation/Adoption of Electronic Health Records in Developing Countries: Literature Review of its Practical Application in Nigeria
Eunice Omidoyin University of Ilorin Teaching Hospital, Ilorin, Kwara State, Nigeria
P9 Impediments and Socio-Technical Factors Affecting the Adoption of Electronic Health Record
Mojirola Shote1; Yusuf Abideen2 1Chevron Nigeria Limited, Lagos, Nigeria; 2Atlas Systems & Technology, Lagos, Nigeria

P10 Transitioning into the EHR
Julie Sternik; Sue Rocchetti The Credit Valley and The Trillium Health Centre, Mississauga, ON, Canada
P11 Global Implementation of Electronic Health Information
Chandrika Thal Consultant, Ajax, ON, Canada
P12 Quality of Pharmaceutical Care After the Use of E-prescribing in Grha Kedoya Hospital
Lily Widjaja1; Yuni Mujiarti1; Veny -1; Sis Wuryanto2 1Esa Unggul University, Jakarta Barat, DKI, Indonesia; 2Mitra Husada School of Medical Record, Karang Anyar, Central of Java, Indonesia
P13 The Needs of Improvement of Graduated Health Information Management Competency Program in Indonesia
Lily Widjaja1; Laela Indawati1; Sis Wuryanto2 1Esa Unggul University, Jakarta Barat, DKI, Indonesia; 2Mitra Husada School of Medical Record, Karang Anyar, Central of Java, Indonesia
P14 The Experience of ICD Utilization on Verbal Autopsy Data to Obtain Trend of Cause of Death in Indonesian Population (1992-2007)
Sarimawar Djaja National Institute Health Research and Development, Ministry of Health, Jakarta, DKI Jakarta, Indonesia
P15 Role of International Federation of Health Records Organizations (IFHRO) in the Evolution of Medical Records in India
Goverdhan Mogli Dr. Mogli Health Care Management Consultancy, Secunderabad, Andhra Pradesh, India
P16 Use of LEAN Methodology to Improve Hospital Patient Records Utilization by Staff and Researchers at a Rehabilitation Hospital
Vijitha Anton Mariathas; Marie Disotto-Monastero St. John's Rehab Program at Sunnybrook Health Sciences Centre, Toronto, ON, Canada
P17 Training Need Assesment for Medical Record and Health Information in Harapan Kita - Women's and Children's Hospital, Jakarta-Indonesia
Elise Garmelia HIM Manager, West Jakarta, DKI Jakarta, Indonesia
P18 Analysis of Computerized Physicians Order Entry System Data of Inpatients with Diabetes as a Complication to Improve Intervention
Ryoma Seto1; Akemi Nishio1; Tomoki Nakano2; Aizan Hirai3 1Division of Healthcare Informatics, Faculty of Healthcare, Tokyo Healthcare

University, Setagaya, Tokyo, Japan; 2Department of Endocrinology and Diabetes, JMA Higashi Saitama General Hospital, Saitama, Japan; 3Chiba Prefectural Togane Hospital, Chiba, Japan
P19 Leveraging HIM Skills to Optimize the Use of Data Across the Spectrum of Health Care
Donna Boyd Alberta Perinatal Health Program, Edmonton, AB, Canada
P20 The Role of Health Informatics Professionals Within Addiction Agencies in the Health Care System
Alison Zwaagstra; Patryk Simon; Shaun Black Addiction Prevention and Treatment Services, Capital District Health Authority, Dartmouth, NS, Canada
P21 HIM in 2016: Guiding Principles for Enterprise Information Management and Governance
Linda Kloss1; Jeffry Levitt2 1Kloss Strategic Advisors, Chicago, IL, United States; 2Precyse Solutions, LLC, Wayne, PA, United States
P22 Reporting Drug Resistant Microorganisms Infections and Carriers
Neomi Goshen; Yonit Sonego; Tali Avraham; Nava Teitler; Tuvia Tiosano Emek Medical Center, Afula, Israel
P23 "small changes, BIG GAINS" Use of LEAN Methodology to Improve Completion of National Rehabilitation Reporting System (NRS) Assessments by Clinicians at a Rehabilitation Hospital
Grace Liu St. John's Rehab Hospital, Toronto, ON, Canada
P24 Health Related Problems, 10th Revision, Canada (ICD-10-CA), and the Canadian Classifications of Health Interventions (CCI) to Inform Future Directions
Karen Carvell Canadian Institute for Health Information, Montreal, QC, Canada
P25 A Multifaceted Approach to Resolving Clinical Coding Data Quality Issues
Denise Cullen Canadian Institute for Health Information, Ottawa, ON, Canada
P27 Quality Measures Reporting in the US: A Case Study of Meaningful Use in Rural Hospitals
Trina Lower1; Ryan Sandefer2; Brooke Palkie2 1Mercy Hospital, Moose Lake, MN, United States; 2The College of St. Scholastica, Duluth, MN, United States

P29 Electronic Health Record Systems and Medication Errors: A Study of the
Indian Health Service (IHS) System.
Godwin Odia U.S.Public Health Service, Baltimore, MD, United States
P30 Family Attitudes Toward a Personal Health Record (PHR) in a Long Term Care Facility
Pria Nippak; Winston Isaac; Alice Geersten Ryerson University, Toronto, ON, Canada
P31 A Study of Knowledge and Attitudes of Doctors Towards Health Information Management at National Hospital Abuja Nigeria
Rasaq Adio National Hospital Abuja, Abuja, FCT, Nigeria
P32 Beyond the RAC: New Methods to Mitigate Audit Risk in 2013
Lori Brocato; Merritt Beaver HealthPort, Alpharetta, GA, United States
P33 Clinical Program Scorecard Development: Famework, Processes and Partnerships for Improved Information
Desa Marin; Diamond Watson-Hill; Mohan Ariyath William Osler Health System, Brampton, ON, Canada
P35 The Unleashed Vocational School Reloaded. Striking a New Path in the Vocational Training of H.I.M. in an Academic Landscape
Ulrich Wirth University Medical Center of the Johannes Gutenberg University Mainz, Mainz, Germany
P36 Beyond the Code Of Ethics: Infusing Ethical Principles Throughout the Health Information/Coding Specialist Curriculum
Marsha Holey; Linda Tyacke St. Catherine University, Minneapolis, MN, United States
P37 Health Information Management and Meaningful Use: Through the Lens of Regional Extension Centers in the United States
Janelle Wapola; Ryan Sandefer The College of St. Scholastica, Duluth, MN, United States
P38 Advancing the Health Information Management Profession Through Personal Relationships: The Leader-Member Exchange Leadership Theory
Thomas J. Hunt Davenport University, Grand Rapids, MI, United States

45
BOOK OF ABSTRACTS

46
IFHIMA Program Concurrent Sessions Abstracts CS1.1.1 Doing It Right: Deploying Alberta's Provincial Electronic Health Record Barb Goertzen Alberta Health, Brooks, AB, Canada Introduction and Objectives: Electronic Health Records (EHR's) are tools used for sustaining and improving publicly funded health systems. Deployment is the biggest hurdle for EHR implementation. Alberta Netcare is a program encompassing projects, processes, and services necessary to make Alberta’s Electronic Health Record (EHR) a reality. Key stakeholders currently include Alberta Health (Ministry), Alberta Health Services (Provincial Health Facilities/Services), Physician Office System Program (POSP) EHR vendors, physicians, pharmacists and nurses. Methods: As a foundation, Alberta chose the provincial health number as a Unique Lifetime Identifier (ULI) to build a Provincial Client Registry (PCR) and unique facility identification is captured in a provincial registry. Cornerstones are the Alberta Netcare Portal (ANP) and the Pharmacy Information Network (PIN). PIN is a repository for all dispensed medications in Alberta and a prescribe tool. ANP provides access to Alberta-wide laboratory test results, diagnostic imaging reports, Alberta Health Services (AHS) transcribed reports, and patient events. Data is contributed from multiple data sources across the province. The present deployment model utilizes a decentralized provincial team using a 4-phase implementation framework of: Foundation & Readiness, Planning & Participation, Training & Implementation and Evaluation & Follow-up. The team is supported by a user registration desk, specialty support, a training environment, printed resources, and a 24/7 Provincial Help Desk. Designated responsibilities are divided by geographical area and assigned to cover all AHS and community sites (physician offices and pharmacies). ANP training is delivered by various modes, with continuing educations credits given and ANP training also integrated into education institution programs. The team will also provide training and support to related real-time integration initiatives, e-Prescribe and e-Referral. Alberta has adopted a custodian centric deployment model in response to the Health Information Act (HIA) with dependencies on facility-based security. A Privacy Impact Assessment (PIA) and Provincial Organization Readiness Assessment (pORA) are required for each authorized custodian before granting ANP access. Results: The multifunctional team supports many deployment functions allowing sites to be at different stages of EHR implementation. The team supports ongoing ANP deployments, various real-time integration functionality involving ANP and is poised to deliver future EHR related initiatives. Conclusions: ANP deployment is maturing for three provider groups setting the stage for further defined providers. Benefits of timely access to health information and improved workflow processes via real-time integration reduce the need to market the EHR. HIA review, electronic access, e-learning and ANP access workflow re-engineering initiatives will streamline deployment activities. CS1.1.2 How Hard Can It Be? Implementing an Integrated Electronic Medical Record (EMR) Beyond the Basics to Benefits Realization Diane Edlund Healthcare Consulting, Edmonton, AB, Canada Introduction and Objectives: While Electronic Health Records (EHRs) in Canada are growing into comprehensive health information repositories and becoming the de facto standard of care, Electronic Medical Records (EMRs) used in physician offices and clinics are less mature in their evolution and are often not utilized to their utmost capacity. Truly integrating health care information into the clinical experience can improve decision making with respect to individual patients and ultimately turn information into knowledge to improve individual health outcomes. This knowledge can then inform population health decisions turning that knowledge into wisdom that can make a world of difference. So why haven’t we embraced the functionalities available in EMRs and other innovative initiatives to realize the potential benefits? Methods: Examining the question of low EMR adoption as well as the challenge of utilizing EMRs to their utmost capacities to gain tangible benefits must take a multifaceted approach. Visioning the Future: In order to realize benefits offered by an EMR, simple tools can be used together with strategic thinking to determine what a successful EMR implementation looks like. There are silos of innovative advances in technology, such as Teledermatology consultations, that provide out of the box examples with positive outcomes for Canadians. Visioning requires gathering current state metrics and future state requirements and then performing a gap analysis to understand the challenges ahead.

47
Overcoming Interoperability Challenges: As EMR technology tools emerged in Canada, it became clear that standards were required to allow systems to exchange information effectively while concurrently respecting various privacy and security considerations. Incorporating Change Management: There are many challenges impacting EMR adoption, such as preparing for, managing and reinforcing the change required to truly integrate EMRs and capitalize on the potential benefits. A repeatable change management model can be used to determine the risk involved in implementing an EMR as well as provide concrete ways of mitigating that risk. Results: We have learned, from implementing EMRs across Alberta, that managing the people side of change by visioning and overlaying an effective change management model on top of a proven project management methodology can improve the integration of EMRs into clinical environments. Only then can utilization of advanced EMR functionalities lead to improved population health care. Conclusions: People are the most important aspect to consider when integrating electronic health information systems into clinical workflows and environments. A fully integrated EMR can be successfully adopted with visioning, interoperability and change management incorporated into the implementation plan. Realizing EMR benefits allows people to manage health information, gaining knowledge and wisdom to truly make a difference in the world! CS1.1.3 Spain IB-Salut Case Study: Implementing an Integrated Delivery Model for Population-based Disease Management and Integrated Clinical Pathways Chris Hobson Orion Health, Toronto, ON, Canada Introduction: The reality is that our current models of care delivery are focused on acute care. A key issue preventing improved care for patients with chronic disease are silos, which lead to fragmentation & a resultant lack of care coordination, which is important for patients with long term chronic conditions because they are cared for by multiple providers in various care settings. Objectives: IB-Salut recognized the need to improve information availability & the coordination of care across silos & over long time periods. Their vision for a new health system included making complete medical information readily available to clinicians at all points of care across the region, streamlining & coordinating the delivery of services such as primary care & internal medicine. The leadership team recognized the need for patient centric, integrated clinical pathways that clinicians would use completely independent of the physical care setting/organizational silo. They recognized the central role of a shared care plan in this effort & sought appropriate technology. The project had several goals including the provision of a single clinician desktop with complete patient data viewable from any PC/device anywhere across the region; immediate access to context linked clinical guidelines from any part of the record; & development of integrated clinical pathways addressing clinical conditions like COPD, stroke & cardiovascular disease, etc. Methods: In 2006, the Spanish regional health authority for the Balearic Island in Palma Mallorca, (IB-Salut) began deploying an integrated health record to serve the region’s population of 1.2 mil. Commencing in 2009, the health authority added further applications to leverage the integrated health record to better manage patients with key chronic disease states. As an example of the use of integrated clinical pathways, the Stroke Telehealth program enabled nurses in remote areas to reliably and efficiently diagnose and treat potential stroke patients working in close collaboration with specialists in major hospitals, made possible via the region-wide accessible forms, protocols & shared care plans. The Chronic Disease Management program addressed a number of chronic conditions including COPD, diabetes, hypertension, dyslipidemia, smoking, obesity, chronic kidney disease. IB-Salut also established automated support for nursing care plans, geriatric care, social work, etc. Results: IB-Salut received the 2008 Award for Innovation in the Overall Improvement of Quality of Care from the Spanish Ministry of Health. Results from November 2011 showed that the system had assigned 250 patients to the COPD Program, 950 to the Cardiovascular Risk Program & 450 to the Nursing Care program. 82% of the patients have continued to receive follow-up in the primary care clinic, 90% of patients in primary care assigned a risk factor for nephrology & 84% of the patients that were determined to have a neurological risk factor, are in hospital specialist care. CS1.1.4 Proposed Implementation and Evaluation of a Thoracic Surgery Quality Monitoring, Information Management, and Clinical Documentation System in a Cancer Assessment Clinic Jelena Ivanovic 1; Tim Ramsay 2; Donna Maziak 3; Sebastien Gilbert 3; Farid Shamji 3; Sudhir Sundaresan 3; Andrew Seely 3

48
1University of Ottawa, Ottawa, ON, Canada; 2Ottawa Hospital Research Institute, Ottawa, ON, Canada; 3The Ottawa Hospital, Ottawa, ON, Canada Introduction and Objectives: The importance of implementing and using health information technology to automate clinical transactions and to improve quality and efficiency of care has been increasingly recognized. Moreover, with the introduction of tablet/wireless technology into the healthcare setting, an opportunity exists to bring real-time information to the patient’s bedside. In the Ottawa Hospital’s Cancer Assessment Clinic (CAC), efforts are underway to implement the Thoracic Surgery Quality Monitoring, Information Management, and Clinical Documentation (TSQIC) system as a means of facilitating clinical information gathering and access at the bedside. The objective is to provide a qualitative overview of the TSQIC system, including its conceptualization, development, planned implementation and evaluation strategies, and clinical impact. Methods: A systematic four-phased approach will be undertaken consisting of: i) development; ii) pre-pilot; iii) pilot randomized controlled trial (RCT; and iv) clustered RCT. Results: By means of an extensive and iterative process, the development phase of the TSQIC system is now complete. The TSQIC system is a browser-based, iPad-optimized, point-of-care software application for capturing automated and standardized patient consults, operative notes, post-operative thoracic morbidity, and follow-up visits. In the pre-pilot phase, metrics to measure study outcomes, including quality of documentation, and timeliness and efficiency of care were developed. Currently, in the pilot phase, we are evaluating organizational aspects of the CAC and physician/user acceptance to expedite the implementation process of the TSQIC system. Conclusions: Electronic capture of clinical encounters can improve quality and timeliness of care by preventing errors, promoting patient safety, and enhancing patient confidence. The TSQIC system has the potential to strengthen both the organizational and operating efficiency of the Ottawa Hospital’s CAC and to improve management of patient care. The TSQIC system provides a robust and innovative platform to improve the delivery of care, while ensuring privacy and security. Results of this ongoing and comprehensive examination will determine the direct impact of the TSQIC system on clinical performance and patient care. CS1.2.1 Coding Compliance Begins with Defining Your Core Designated Medical Record Set of Documents Bonnie Cassidy Nuance Communications, Inc, Burlington, MA, United States Introduction: It is time to review your Coding Compliance Policy and test it to the 2012 challenges that face the health information management (HIM) professional staff in your organization. It does not matter if your medical record is paper-based, hybrid or electronic, a Coding Compliance Policy should be written and updated at least once per year. The focus of this article, is the identification of the key source documents or core designated record set for coding which is to be used by your coding professionals as they conduct all the medical coding for your organization. Methods: I did a literature search which included a detailed evaluation of the AHIMA Body of Knowledge and the internet looking for any thing related to coding compliance, key documents used for coding, etc. In addition, I conducted interviews with HIM Directors asking if they had a Coding Compliance Policy or Program, and if they did, what documents were required for the coder to review for coding. Results: What has never been defined are the actual core medical record documents that should be used as the designated record set for coding. Your Coding Compliance Policy must identify medical record documents that require a mandatory review by your coding staff. All Coders review the following medical record documents to identify all diagnoses and procedures requiring coding and to increase the accuracy and specificity of coding. Conclusions: A Coding Compliance Policy is essential to your organization's overall compliance program. The four key areas where you will rely on your coding compliance policy are: a. Coding: Organizations using diagnosis and procedure codes to report healthcare services must have formal policies and corresponding procedures in place that provide instruction on the entire process-from the point of service to the billing statement or claim form. b. Coding Audits: Coding compliance policies serve as a guide to performing coding and billing functions and provide documentation of the organization's intent to correctly report services. c. Outsourcing coding work: The policies should include facility-specific documentation requirements, payer regulations and policies, and contractual arrangements for coding consultants and outsourcing services. The outsourcing vendor does not tell you what documents that they will use to code your medical records, you are in charge of this process and have your outsourcing partner follow your best practice or coding compliance policy. d. Computer Assisted Coding: In selecting a business partner to build a technology enabled coding process, use your coding compliance policy for your vendor to create a customized CAC for you. Simply said, you do not need

49
to load your entire electronic medical record into the CAC when you have already identified your core designated record set of documents for coding compliance. CS1.2.3 Quality Audit of Coding Question Service Margaret Penchoff Canadian Institute for Health Information, Ottawa, ON, Canada Introduction and Objectives: The coding question service provides direction to assist classification users with proper code selection using ICD-10-CA and CCI and with the appropriate application of the accompanying coding standards, for data submitted to the Discharge Abstract Database (DAD) and the National Ambulatory Care Reporting System (NACRS). To-date an audit of the coding question service had not been undertaken. Methods: A summary was created of the questions that were answered which were submitted for 2010-2011. Review of all coding questions was not feasible or realistic given the number of data elements being collected and the human resource and temporal constraints. To help determine a feasible and realistic sample size, a time study was undertaken. The results led to selection of questions as the target sample size. Questions that pertained to topics of national interest as identified in CIHI's nationally published reports, e.g. post intervention conditions, were selected. Six members of the Classifications and Terminologies team reviewed the answers. The focus of the audit was on data quality dimensions, accuracy and timeliness. Results: The review team identified closed answers with which they agreed and answers with which they did not agree. The discrepancies were further broken down by reason. The results showed the average turn-around-time for the questions that were reviewed. The turn-around-time was further analyzed using various statistical calculations. The results were also analyzed by patient type (i.e. inpatient, day surgery and ambulatory care); product (i.e. ICD-10-CA, CCI and Canadian Coding Standards for ICD-10-CA and CCI); and ICD-10-CA chapter; CCI section; and coding standards chapter. Note: We will share the actual results during this presentation; however, the results have not yet been made public so they cannot be included in this abstract at this time. Conclusions: The overall results of the audit were positive. The accuracy rate was calculated. The audit identified that we need to improve the service in the data quality dimension, timeliness. The turn-around-time was identified as an area where we have to significantly improve. We have to reduce the turn-around-time to a reasonable and achievable timeframe to help facilitate submission of accurate and complete data to the DAD and NACRS database within the jurisdictional and nationally imposed data submission deadlines. The findings and results led to recommendations and implementation of measures to improve the turn-around-time. The turn-around-time will be monitored closely on an ongoing basis to ensure that the measures implemented, have, in fact, led to an improvement in the dimension of quality, timeliness. CS1.2.4 Assessing the Quality of Canada’s Discharge Abstract Database Rachel Benoit ; Josie Bellemare ; Maureen Kelly Canadian Institute for Health Information, Ottawa, ON, Canada Introduction: The Discharge Abstract Database (DAD) housed at the Canadian Institute for Health Information (CIHI) captures administrative, clinical and demographic information on discharges from inpatient acute care hospitals across Canada. High quality data is crucial as the information is used extensively by hospitals, health authorities, ministries of health and researchers. As part of its comprehensive data quality program CIHI undertook a five-year series of reabstraction studies to assess the quality of the data submitted to the DAD, in particular the diagnosis and intervention data captured using ICD-10-CA and CCI respectively. Methods: Reabstraction studies were carried out on data submitted to the DAD from 2005-2006 to 2009-2010. Each study had a similar methodology, but each year had a special focus and therefore a different sample design. For example, the focus of the 2005-2006 study was on ambulatory care sensitive conditions and in 2008-2009 it was stroke. In addition, the samples in 2005-2006, 2007-2008 and 2009-2010 were designed to enable provincial/territorial and pan-Canadian estimates of overall coding quality. For each study, a stratified random sample of abstracts was selected based on the sample design. Reabstractors were recruited, trained and then visited each sampled hospital to do a chart review and reabstraction of the data from the sampled abstracts. The reabstracted and original DAD data was then compared. Key statistics calculated included the positive predictive value (PPV) and sensitivity of the diagnosis and intervention reported, and the percentage agreement to measure consistency of coding using ICD-10-CA and CCI. Results: The 2009-2010 study showed that the DAD data maintained the high quality achieved in 2007-2008, which showed improvement compared with 2005-2006. The improvements achieved for the selection and coding

50
of the most responsible diagnoses in 2007--2008 were maintained in 2009-2010. This is particularly important because the most responsible diagnosis is a key component in health care system analysis, research and grouping methodologies. There was less consistency in determining whether or not a pre- or post-admit diagnosis had significantly contributed to the patient's acute care stay. Conclusion: Canada seems to be unique in conducting such an extensive series of reabstraction studies that have enabled pan-Canadian estimates of overall coding quality for its hospital data. A literature review suggested that other countries have either focused their chart review/reabstraction studies on specific disease groups and/or specific geographic areas or hospitals. Through these studies, CIHI has established a solid baseline for the quality of data in the DAD, which will continue to be monitored through data mining and ongoing surveillance. While large scale reabstraction studies are costly to conduct in a time sensitive manner, targeted reabstractions will always be an option should the need arise. CS1.3.1 The Legal Foundations of Access, Privacy and Confidentiality and a Look Ahead to the Future of Access Marianthi Kakouratos O'Sullivan College, Montreal, QC, Canada Introduction and Objectives: Along with a brief introduction to access to health records in Canada, three issues related to the future of access and consequently, privacy and confidentiality, will be breached. The first will be a look at the interoperability of the rules regarding privacy and confidentiality of health records. It’s not uncommon for individuals to be treated in different states/provinces or countries to their place of origin and as an increasing number of jurisdictions implement electronic health records. That information can be sent across the world with a single click. The trouble is that different rules govern access, privacy and confidentiality in different jurisdictions. Second will be an examination of ownership of information as it relates to access. More specifically, with a look at proprietary rights of information held in a virtual database (cloud computing) and how this concept affects access. Third, the more we learn about our genetic makeup and the genetic origins of certain diseases or disorders, the more sensitive the information in our health records becomes, and thus the more crucial its protection. Our health information will change with the advancements in genetics, genomics etc. Consequently, the role of genetic information in employment and insurance will change. A look at the current protection and what is required as future protection of this information is necessary. Methods: In order to understand the interoperability of rules regarding the respect of privacy and confidentiality, forcibly a study of international law in the area is required. There will be a comparative analysis of the concept of ownership and proprietary rights to personal health information and information technology in Canada in order to better understand the legal concept and how it affects the right to access, privacy and confidentiality. There will be a study of the legislation pertaining to genetic information and the right to privacy and confidentiality, how this information relates to employment and insurance, and how that information is being protected. Results: Although there are certain agreements between states regarding the exchange of information, there is not a comprehensive piece of legislation specific to the protection of privacy as health information crosses international borders. The concept of ownership of records and the information found therein differ depending on the jurisdiction and thus affect rules regarding access. Despite certain international treaties on genetics and human rights (which include privacy and confidentiality) there seems to be a legislative void on this topic domestically and particularly as it relates to insurance and employment. Conclusions: The legislative requirements currently in place regarding access and to protect the privacy and confidentiality of medical records and personal health information are not sufficient and will be even less so as science and technology progress. CS1.3.2 Security and Data Privacy: Technology is Not Enough Kerry Matre Hewlett-Packard, Lyons, CO, United States Introduction: Many organizations deploy technology to ensure security and data privacy. This includes firewalls, IDS/IPS, proxies and various other devices. Some organizations have deployed security information even monitoring (SIEM) systems to correlate this data. The existence of processes and procedures guiding the use of these systems varies greatly amongst organizations leading to a discrepancy in the maturity and effectiveness of

51
their security operations capabilities. Methods: 100+ Security operations center (SOC) builds and maturity assessments were performed over a 5 year period. The primary technology implemented was a Security Information Event Monitoring (SIEM) system which correlates security information feeds from external devices such as firewalls, IDS/IPS, virus scanners, proxies, etc. Additional services were provided to assess the maturity of the SOCs after implementation. Processes, procedures, staff training were also taken into consideration during the assessments. Results: In technology-only implementations, organizations failed to monitor the security devices. If they did detect attacks there was typically minimal staff available to review logs and little or no experience in forensics to investigate a breach. Organizations lacked process and procedures that identify roles and responsibilities and tasks in the event (inevitability) of a breach. Subsequently, breach response became a fire drill and many resources are wasted opening up a window of liability. Organizations that used a holistic approach utilizing people, process and technology components scored higher in their maturity assessments and showed greater risk reduction and operational efficiency. Conclusion: Organizations that have implemented technology-only solutions without the associated structure of processes and procedures were not realizing comparable risk reduction and operational efficiencies as organizations who implemented their SOCs with a holistic approach including people, process and technology aspects. The gained operational efficiency also led to reduced staff needs and reduced time to resolution for breaches. CS1.3.3 Collision Course or Collaboration Course? Healthcare Delivery and Technology Changes Meet Evolving Privacy Law Brian Foran1; Joan Roch1; Wendy Robillard 2; Heather McLaren 3;Alison Blair 4; David Morgan 5; Debra Grant 6 1Canada Health Infoway, Montreal, QC, Canada; 2Alberta Health and Wellness, Edmonton, AB, Canada; 3Manitoba eHealth, Winnipeg, MB, Canada; 4Ontario Ministry of Health and Long Term Care, Toronto, ON, Canada; 5Newfoundland and Labrador Centre for Health Information, St. John's, NB, Canada; 6Office of the Privacy Commissioner of Ontario, Toronto, ON, Canada Introduction and Objectives: Most governments in Canada have enacted health information privacy legislation that sets out how personal health information is to be collected, used and disclosed to provide health care and support other authorized uses such as health system management. This legislative framework helps to assure Canadians that their personal health information is safeguarded and their privacy is respected. These same governments are facing increasing pressures to streamline healthcare delivery and to make health information more widely available. The continued deployment and linkage of electronic health records and other emerging technologies offer new ways to address these pressures. For example, shared care models in primary care and concepts such as open data can promote seamless service delivery and improve access to data. These innovative solutions, however, can also pose challenges to health information privacy and existing privacy legislation. This presentation will: * provide health information management professionals an opportunity to dialogue with jurisdictional health information privacy experts about the implications of changes in healthcare delivery for the health information privacy legislative framework, * provide insights into the impact that continued deployment and linkage of provincial and territorial health records, electronic medical records, personal health records and portals have on developing and amending health information legislation, * describe the collaborative approach taken by privacy experts in addressing these issues and how their work has been of help in framing some responses. Methods: Panelists from a mix of small and large jurisdictions, ministries and eHealth agencies, will discuss with the audience "pressure points" between health information privacy legislation and changes in healthcare delivery models and technology. The discussion will focus on questions such as: How are we managing these issues in the continuing evolution of health information legislation? What is the right balance between privacy protection and access to information? When do we go too far? Are we going far enough? Results and Conclusions: Drawing on a series of "common understandings" developed collaboratively by the Canada Health Infoway-sponsored Health Information Privacy Group, the panel will discuss potential approaches to these issues.

52
CS1.4.1 Linking Strategy to Operational Execution Through Enterprise Business Intelligence Maria Muia ; Eugene Wong North York General Hospital, Toronto, ON, Canada Introduction: Health care has never seen a time when the demand for better, faster and more information is greater than it is today. Not unlike many hospitals, North York General Hospital (NYGH) faced the traditional information challenges of being data rich but information poor. Information and data is coming at us from many systems, in multiple mediums and at an unprecedented speed. Yet, using traditional methods to access and use that information is nearly impossible. Bringing it all together in the form of an enterprise Business Intelligence (BI) has transformed how decisions are made at the hospital. Virtually no decision are made without evidence and information. The implementation of a BI strategy and system has created a culture of transparancy and accountability throughout the hospital. It has helped improve patient safety and outcomes and monitor the hospital's progress towards achieving its strategy. Methods: North York General Hospital engaged in a BI strategic planning process where structure, processes and tools were highlighted as key success factors in helping the hospital achieve its strategic and operational goals. This presentation will focus on how the selection and implementation of a state of the art BI system has helped the hospital achieve the following goals: •cascade the hospital's balanced score card to program and service levels in a manner that links strategy to operational execution •enable leaders to be able to monitor their program or service performance as it relates to the hospital's strategic goals in a timely and proacive manner that allows for operational adjustmes as required, and •monitor performance in accordance with internal key performance indicators (KPIs) and external requirements such as wait times, government accountability agreements and other obligations. NYGH selected and implemented an enterprise BI system as a foundation to an enterprise-wide approach to performance management. The BI system provides the tools and information necessary to allow NYGH's leaders to make better decisions at the operational, strategic and governance levels. Fifteen data sources were brought into a corporate data warehouse providing the data sources to populate over 150 KPI. The KPIs are presented in various dashboards and scorecards. Accountability for performance of the hospitals KPIs is built into the system where there is a designated owner of each KPI responsible to monitor and adjust performance as required to achieve desired outcomes. Results: Information led transformation of the hospital's culture improved patient safety and outcomes (e.g. low Hospital Standardized Mortality Ratio, dramatic improvement in Emergency Department Wait Times, good peformance in patient safety indicators, improved patient satisfaction). Conclusions: Leveraging data from multiple systems including EMRs presenting it in a useable format significantly impacts hospital performance and patient outcomes. CS1.4.2 Health System Use & the Electronic Health Record - Opportunities to Support Decision Making at the Point of Care and From a Health System Perspective Valerie Leung 1; Alex Mair 2 1Canada Health Infoway, Toronto, ON, Canada; 2Canada Health Infoway, Halifax, NS, Canada Introduction and Objectives: Health System Use (HSU) of data refers to the use of health information to improve health of Canadians and the health care system. Opportunities exist where HSU can enable insights that support both Health System improvements and transformation. With capture of health information occurring via Electronic Health Records and Electrical Medical Records, improvements in the availability and quality of data presents new opportunities for HSU of information that can further support system improvements and transformation. In order to realize this opportunity, a common vision and framework are foundational. The objective of the HSU Architecture and Deployment Models project is to assist jurisdictions and other stakeholders to align to a pan-Canadian vision and ensure a foundation is in place at all levels for future needs. In order to achieve this, an information and system architectural framework is articulated to assist system and solution architects, vendors and healthcare organizations in developing a common understanding of HSU system architecture concepts based on current and future business requirements. Methods: Because this project anticipates a future state beyond sharing of information to one of using "information" to support patient centred collaborative care across different settings, needs identification, business requirements definition, options research, analysis and technical architecture were key components. An extensive literature search, environmental scan and stakeholder consultation phase led to the development of 8 business scenarios.
53
Results: Eight distinct business scenarios were created to provide business context for the system architecture component of the project. Using these scenarios, identification of insights and requirements in the form of reusable patterns formed the basis for the definition of the functional capabilities in the HSU system architecture framework. Conclusions: In addition to top down requirements focused on larger health system outcomes, HSU architecture needs to also support bottom up requirements that are tied to local needs and be adaptable to meet the changing needs of the health care system. This is achieved by bringing primary use of information for care and HSU analytic requirements closer together at the point of care and by providing a framework that leverages information captured at the point of care across all categories and levels of use. CS1.4.3 Business Intelligence (BI) in Healthcare —Adjusting Your Sail and Improving Financial Health Lisa Gregoire Emerald Health Information Systems, Ottawa, ON, Canada Introduction: Healthcare lags behind other industries in the adoption of BI and this is unfortunate because the ability to measure key metrics in a holistic and timely fashion only leads to performance improvement. There is an opportunity to leverage healthcare data to improve productivity, medical outcomes, and patient satisfaction and to analyze potential cost savings by service line spending. Until these barriers have been conquered cost management will continue to be a challenge and organizational performance will not be optimal. Regardless of what you read in the healthcare industry literature we are still data rich and information poor. If you cannot measure it you cannot manage it! BI allows healthcare organizations to make informed decisions using data that most stakeholders did not have prior access to and were forced to wait for month-end reporting in order to perform meaningful analysis. With BI you can analyze Key Performance Indicators (KPI) on a real-time basis and adjust your sails accordingly before the storm hits. Methods: Healthcare organizations must have a central source of the truth by leveraging all legacy and disparate systems in order to effectively manage and improve performance. This data warehouse can be built across the continuum of care and across multiple site facilities and geographical regions. Advanced analytics are designed to manage patient information and operational flows. The critical step in this process is to review and clearly define the Key Performance Indicators (KPIs) with the knowledge that as performance improves the KPIs will also evolve in this new information sharing culture. Results: Real-time information allows managers and executives to act not react. Having accurate, real-time and integrated information allows the managers to manage patient flow in a proactive manner thus enhancing their bottom line. Healthcare organizations will meet strategic goals with real-time performance management in a much more collaborative and focused manner. Providing stakeholders with the ability to select KPIs on a self-serve basis with the ability to drill-down in order to analyze measured metrics allows for more accountability and a better understanding of the information. This practice drives the process improvement process and enhances data quality. Performance targets can be continuously monitored and reset when milestones have been achieved. Conclusion: Data analysis is an important part of improving operational efficiency but in today’s environment it continues to be a challenge with disparate data and information solutions that require highly skilled IT staff to extract information. The healthcare industry is a prime candidate for business metrics and BI is the solution to assist stakeholders with the continuous challenge of improving patient outcomes while being under the constant pressure of cost containment. CS1.4.4 Specialized Skills Required by HIM Professionals for Decision Support in a National Organization Janet Manuel Canadian Institute for Health Information, Summerville, NS, Canada Introduction and Objectives: This presentation will provide a window into the 'behind the scenes' contribution of HIM professionals to the success of Canadian national analytic reports, with specific examples. In Canada, research and analysis of data from national clinical administrative databases is becoming increasingly complex and moving well beyond the mere counting and of cases or calculating of rates. Linking the records of specific case selected patients to track their 'pathways of care' across the continuum of care for select conditions, surgical outcomes and additional services such as continuing care or rehabilitation, requires a team of seasoned HIM professionals to advise the research teams. These teams are typically comprised of data analysts, methodologists and epidemiologists. The HIM professional brings to the table the knowledge of the classifications, the 'rules' by which the data is entered into the databases (Coding Standards), and the abstracted code 'scenarios'
54
which will provide the answers to research questions. In tracking data across fiscal years, cyclical enhancements and changes to classifications and coding standards present data trending issues which the HIM professional can account for in an analytic study, by experienced knowledge and documentation of changes. At CIHI HIM professionals in the Classifications and Terminologies branch have become a vital part of the support to research and analysis teams the major program areas, with recent studies on breast cancer surgery and stroke pathways of care requiring very close collaboration with the study teams. Methods: Using the Canadian Coding Standards (especially knowledge of the application of diagnosis typing rules), the knowledge of enhancements/deletion of codes and classification of diseases and interventions in the International Classification of Diseases and Related Health Problems, Tenth Revision, Canada (ICD-10-CA) and the Canadian Classification of Health Interventions (CCI) as applied to the major Canadian hospitalization databases, the Discharge Abstract Database (DAD) and the National Ambulatory Care Reporting System (NACRS), and the Registries that derive data from them, specific methodologies for data extraction were developed for key CIHI reports and analyses. Results: Robust cooperation between CIHI analytic teams and the Classifications support staff (HIM professionals) to produce the reports and analyses. Conclusions: There is a vital role for HIM professionals in providing national level support. CS1.5.1 The Survey Report on the Needs of the Developing Countries Stuart Green 1; Yukiko Yokobori 2; Lorraine Nicholson 3 1Bradford Teaching Hospitals NHS Foundation Trust St Lukes Hospital, Bradford, West Yorkshire, United Kingdom; 2Japan Hospital Association, Tokyo, Japan; 3IFHIMA Immediate Past President, Rochdale, Lancaster, United Kingdom Introduction: In Milan November 2010, a number of projects were identified and each Director was tasked with leading and taking forward a particular project. Stuart Green and Yukiko Yokobori were tasked to lead on the Developing Countries Project. Methods: Building a framework of the project: Stuart wrote to volunteers and the Executive Board and tried to prioritise what they felt would be manageable and achievable with limited time and funding. On the 4th May 2012, Stuart wrote out globally to five key named contacts asking if they would be interested in the support from IFHIMA. Dr Y C Chong - WHO/SEAR (Indonesia) Dr S Pilanbangchang - South East Asia (India) Dr Shin Young-Soo - Western Pacific (Philippines) Dr L Sambo - Africa (Congo) Dr Ala Alwan - Eastern Mediterranean (Egypt) Survey on the needs of developing countries: Also, a basic research on SEAR has been conducted focusing on awareness of health information management. We directly sent a questionnaire to WHO country offices and Ministry of Health of 11 SEAR countries. The main goal of this research is to understand specific needs of the specific countries. Alongside, current status on education of health information management around the world has been researched by asking to fill in the table to a contact of each country. Result: Building a framework of the project: We agreed to progress the following: * Increase awareness of the profession in the SEAR region and * Increase the utilisation of the Education Modules, potentially to include having a certificate awarded at the end and the use of an online learning platform. As to the five key named contacts, Stuart did not receive one acknowledgement to his email. Stuart wrote out again on the 22nd June 2012 and to date have still not had a reply. Survey on the needs of developing countries: As to SEAR countries, we received answers from 3 countries and collected other information on the internet. As to the research of current status on education, we collected the data of 41 countries including developed and developing countries. Conclusion: Building a framework of the project: In spite of attempts to contact the key players in what would have been a useful acquisition to a Developing Country, we seem to have drawn a blank moving the project to a successful conclusion. One question remains: Should the project concentrate on a select country initially? � This in our opinion would be yes, providing we can contact the lead person for the selected country. Alternatively, we could select a country and subsequently a region or a hospital and work directly with them. Survey on the needs of developing countries: As a result of Survey, problems of each country became apparent.

55
The needs and problems each developing country have are different and not uniform. The survey result is still in the process of analysis, but it seems that effective utilization of data is more important. CS1.5.2 Health Information Management Education and Training in India: A Situational Analysis Sabu Karakkamandapam Manipal College of Allied Health Sciences, Manipal University, Manipal, Karnataka, India Introduction and Objectives: The Health Information Management (HIM) education and training in India is still in dormant state. Academic institutions in India have not recognized the necessity and importance of structured academic programs in HIM domain. The significant growth achieved in implementing Information Technology in many sectors of healthcare system has not transformed the growth of HIM education and training in the country. The study aimed to explore the current situation of HIM education and training in India. Methods: The study was conducted through an intensive online search of information from various national educational website and health reports. Results: Twelve prominent educational and eight government website pertaining to healthcare and professional education in the country were accessed for data collection. The results indicate, current situation of HIM education and training in India is abysmal. Among 613 universities in India, only three (0.48%) universities offers bachelors and two universities offers masters level program in HIM domain. In addition, few institutions conduct distance education program at bachelors or diploma level. Few established educational institutions are still holding on conventional Medical Records program. Last three year statistics shows; on an average only 30 - 40 students graduates in a year with HIM qualification. There is also a concern over job prospectus of HIM professionals as there is no visibility for HIM profession in India. On the other side, statistics of 2010 shows on enormous increase (more than 100%) in the number of medical and healthcare management professional programs in the country compare to the year 2002. Similarly, there is a huge leap in healthcare infrastructure of India; currently has more than 1, 75000 healthcare facility. Study reveals, the academic and research progress in the area of HIM is paltry compared to other healthcare management disciplines. There are no statutory bodies or a professional body to regulate HIM profession or forecast the future requirement of HIM professionals in the country. Conclusions: In India, current growth of healthcare sector point towards large requirement of qualified and trained HIM professionals at various levels. There are no committed efforts from educational institutions and academicians in strengthening the HIM education in India to meet the challenges in management of Health Information. To attain remarkable progress in public healthcare system, India needs to capitalize on academic and research initiatives in the HIM domain. Professional, Educational and Research collaborations in HIM domain is the need of the hour. CS1.5.3 Electronic Health Record (EHR) Implementation in Rwanda: The Role of and Need for HIM Expertise Kelly Abrams 1; Murray Abrams 2 1CHIMA, Regina, SK, Canada; 2Regina Qu'Appelle Health Region, Regina, SK, Canada Introduction: For two weeks in August 2012, I worked as an HIM consultant with the Rwandan Ministry of Health on their EHR implementation. My role dealt specifically with the HIM component of the EHR implementation as there is no HIM expertise or training in the country. Methods: This presentation will be a case study based on my personal experience of the process, challenges, and opportunities for EHR implementation that occurred before, during, and after the visit. Results: Great advances have been made in Rwanda in terms of improving living conditions: Life expectancy has increased by at least 10 years in the last 10 years (statistics vary between 39.3 and 47 in 2000 to 58.4 in 2011 total population); the maternal death rate has decreased from 1071/100,000 deaths in 2000 to 487/100,000 in 2010; and the mortality rate of children under 5 has decreased from 152/1,000 live births in 2005 to 62.5/1,000 (est. 2012). The improvement has been linked to better health facilities, equipment, and providers (e.g., Rwanda now has midwives) as well as the implementation and strengthening of universal health care (95% of Rwandans now covered). The implementation of the EHR is expected to support continued advances. In terms of the EHR, there are a number of challenges: • there is no HIM expertise in the country • currently two different classification systems are used for diagnosis coding (same level of care, same institutions) • creation of country code sets but not appropriately (e.g., combining of two systems, no limits on individuals creating new codes for items) • the EHR developers have little if any health care experience, and • transition from a non-existent or very rudimentary record system to an electronic information system.
56
Conclusion: The need for HIM expertise in the planning, implementation, and ongoing maintenance of the EHR is highlighted in the microcosm of the Rwandan experience. The lack of HIM expertise has a clear impact on the EHR implementation process and has resulted in troubling decisions (e.g., creation of unique code sets, lack of control of code creation so one item may have many codes attached to it). Going from virtually nothing in terms of the paper record (e.g., formal paper records are not always created, no filing system so continuity of care is problematic) to the electronic record poses many challenges and opportunities. There are no policies and procedures specific to the stages of the information management lifecycle; there is limited understanding of terminology mapping including new version implementation, maintenance and retention of previous versions; and education in HIM in the workplace and at the universities is missing. There is a wonderful opportunity for HIM participation at these early stages of EHR development to support the ongoing health care system advances. CS1.5.4 Improvement Career Development for Medical Record an Health Information Government Employee on Advance Level in Indonesia Elise Garmelia Pormiki, West Jakarta, DKI Jakarta, Indonesia Background: The Medical Record and Health Information Profession in Indonesia as a Health Profession by the regulation no 32/1996. The existence of this profession graduates have received awards in the fungsional position with a credit points of works activity but only the goverment employee by the Regulation of Ministry Administrative Reform No.135/2002. Education of Medical Record and Health Information in Indonesia have been developed vocational degree to Science degree regarding of demands associated with the development of health services in Indonesia such as e-health (Jakarta Health Networking); Referal system report by electronic (call center) dan Integrated Emergency services system, EHR on Practice hospital and e-health developed by MOH regarding the implementation of goverment insurance in Indonesia. All of activities need the skill and knowledge of HIM profession. Indonesia have approximately 1.800 hospitals and 900 primary health care. Estimated demand of profession are 26.000 profession and we have 5.764 graduate (vocassional degree) and needs the bachelor degree approximately 1.800 gradute and we have only 568 person. Goal and Objectives: a. Coaching, career developement, strenghtening organizational performance and increasing benefits of profession. b. Revision of Functional activities point of career profession levels (Skill levels -- diplome graduate) and create the points activity assesment for career profession levels (Advance levels- bachelor). Methods: Applied the Proposed of HIM career Development and Submit the texts academic of HIM to government employee to MOH, meeting will be done for 5 times between MOH and PORMIKI, Final text Academic will presented to National Personel Administration and the Ministry Administrative Reform, Validation test of element activities by HIM profession at three places. Result: Asses points of activity : Education, Medical record and health information management (80 %), supporting activity and profession development. (20 %) The total points of activity : Vocational / Skill Level and Advance Level : 327 points. Validation test will be done at 3 places: the sample of each 96 staff, validation test for skill level : 53 staff graduate D3 (41= 77,35%), D4 (12=22,65%) and Advance Level 43 staff graduate D4 (100%). After validation test be done, the result value from Makasar average 1.177,16 (32 sampling), Bogor average value 1.167,94 (34 sampling) and Surabaya average value 1.172,50 (30 sampling) and the total average value 1.172,80 (under requirement of working indicator staff need per year). Conclusion: The MOH have make regulation for level position and have give the profession award as a levels career.PORMIKI should be advocacy to MOH to improve the benefits for government employee especially MR profession. The Career development through credit points assesment will be improve the performance quality of goverment employee to assure the coach of level, position, loyality and professionalism. CS2.1.1 This Presentation will Discuss the Application of Computer-assisted Coding Technology in a Healthcare System. Technology Issues will be Presented as well as Benefits and Obstacles to Implementation. Sandra Fuller eCatalyst Consulting, Grayslake, IL, United States Introduction: A twelve hospital system in the United States is faced with the challenge of implementing ICD-10 without the inherent productivity loss. Financialpressures require a solution that improves the speed and accuracy of coding, updates to ICD-10 without any increase in staff. Optimally, there would be a cost reduction through

57
reduction in outsourcing. To accomplish these goals the system is acquiring a computer-assisted coding system. The implementation is complicated by two different EMR systems in place across the system. Methods: This applied research will follow the productivity, quality, consistency and adherence to operational timelines and costs. Pre-implementation baseline will be assembled across the 12 hospitals prior to the implementation of the CAC solution. Results of key factors will be tracked monthly across the system. Coder satisfaction studies will also be done at key points prior to, during and post=implementation. A methodical study of this nature should provide insight into the application of technology to significantly reduce the need for human intervention in the coding process. Results: Although not available at this time, it is anticipated that sufficient results will be available prior to May, 2013. Results will be compared to the baseline and will be monitored across time. Conclusions: Computer-assisted coding holds a promise to significantly improve the quality of coded data through systematic application of coding rules and guidelines to text that is normalized based on natural language processing. Variation can be identified, understood and systematically eliminated from the coding process. Productivity gains are required to reduce the overall cost of data collection in the face of increasing demand for data. Disciplined implementation of this technology with monitoring of the process outcomes can not only be applied to the implementation of this technology in other environments, but may be applicable to other technology adoption. CS2.1.2 Journey to a Scanned Medical Record: Six Years On Jennifer Bowman ; Kate Horkings Southern Health, Clayton, Victoria, Australia Introduction and Objectives: Southern Health aspires to be an Australian leader in improving the health and wellbeing of the community, by planning and delivering safe, effective and high quality services that anticipates and responds to the community's health needs. For Health Information Services (HIS) to assist in achieving this vision, integrated and readily accessible medical records are essential. The introduction of a Scanned Medical Record (SMR) provided opportunity to improve the accessibility to medical records, improve the efficiency of record management and add a disaster recovery capability not viable in the paper world. Southern Health has not reached the end of this road. Six years on, now an established scanning centre, HIS continue on the journey to improving efficiencies and the clinician experience. Methods: The opening of a brand new campus in 2004 provided the opportunity and funding to introduce a SMR. Four years later SMR was rolled out across Southern's four paper based sites. Training, support staff and regular communication were provided in key clinical areas prior to and on implementation day. Strict performance indicators were developed and adhered to, to ensure sufficient turnaround time of scanned notes. A priority scanning system was also introduced. Over time mental health and community health records have been integrated into SMR. Additional computers were purchased for clinical areas and wireless technology has been introduced to facilitate the use of handheld tablets and improve access. Results: Health Information Services found monitoring systems of a paper based department are still paramount. Initial customer surveys and clinical workshops at the pilot site showed a strong acceptance of SMR amongst clinical staff. However, some clinicians at paper based sites expressed dissatisfaction with the new world. The Victorian Statement Government Department of Health's Accreditors and Southern Health clinicians acknowledged an improvement to patient care and communication through the integration of community records. Clinicians who struggle to find their forms are more likely to express dissatisfaction. Improving document identification through naming, dating and filing it according to what makes clinical sense (not necessarily traditional Medical Records logic) improves satisfaction. Conclusions: Turnaround time, a good audit program and responsive staff are essential in building trust with clinicians. The introduction of category filters for form groups has been advantageous along with the direct load of documents. The transitioning technology of scanning has forced some clinicians to consider electronic forms with the first pilot of growth charts. The clinical demand for the continued development of the scanned medical record is assisting the funding/investment decision making process where funding is limited and direct patient care initiatives are a priority. CS2.1.3 Expediting a Hospital's Adoption of Electronic Patient Records Through an Innovative Scanning & Document Management Process - A Health Information Management Case Study of Trillium Health Centre Valerie Alston 1; Scott McMillan 2; Julie Sternik 1 1Trillium Health Centre, Mississauga, ON, Canada; 2Salumatics Inc., Montreal, QC, Canada

58
Purpose and Objectives: To describe how Trillium Health Centre - one of Canada’s largest academically-affiliated hospitals providing care to more than one million residents of Mississauga, Ontario - developed their journey toward electronic patient records when an accreditation audit documented 9,000 incomplete charts. Approach: During the initial stages of Trillium’s journey to implement electronic patient records (EPRs), paper records were still being maintained in parallel with the development of the EPRs and were stored off-site at a facility that was rapidly running out of space. Lease costs were high, and courier costs to retrieve and shuttle charts between the storage facility and Trillium’s two sites were considerable. In a typical day, between 700 and 1,000 charts were pulled for multiple clinics; some of those charts were needed in several places at the same time. There were a large number of incomplete charts, and physicians could not always complete their charting because files were unavailable or didn’t arrive when expected. A 2007 accreditation survey documented more than 9,000 incomplete charts. After an extensive, competitive procurement process, Trillium selected a document management and imaging software solution. In conjunction, Trillium began outsourcing paper chart scanning to document conversion and scanning provider. Results: To facilitate the change management process and overcome some initial scepticism, the Health Information Management (HIM) team conducted extensive consultation and training with stakeholders including physicians, nurses, clinical managers and unit clerks. The service provider picked up boxes of paper charts daily, and transported them in unmarked trucks to a secure production facility where all were logged in. Charts were prepared for high-speed scanning, then scanned, indexed and uploaded into the document management software. Initially, the HIM team reassured clinical staff that they would run a parallel system, meaning charts scanned daily for next day’s clinic patients would still have paper records pulled and available. This parallel system was used for four months, as acceptance of the software and scanning process progressed. Conclusions: Trillium is sending approximately six boxes to the service provider daily for scanning, seven days a week, which represents more than 16,000 pages per day or approximately six million images per year. Using scanning services and document management software has transformed workflow processes in HIM. Previously, the records process involved manual assembly, filing, retrieval and checking, work that was done by 12 people. Now that records are scanned and retrieval is electronic, Trillium has reduced clerical headcount by the equivalent of 10 full-time staff. And what about those incomplete charts? The HIM team has reduced the number from 9,000 in 2007 to 335 today, an impressive 96% reduction. CS2.2.1 Information Integrity in the Electronic Health Record Lou Ann Wiedemann 1; Lydia Washington 2 1AHIMA, Chicago, IL, United States; 2AHIMA, Pearland, TX, United States Introduction: Quality patient care is dependent on the availability and quality of patient information. Poor documentation, inaccurate data, and insufficient information can result in poor patient outcomes and increased healthcare expense. Indeed, inaccurate data can threaten the very lives a healthcare organization is trying to improve. In addition, poor documentation can affect the full spectrum in the continuum of care and inaccurate information may cascade to a variety of healthcare organizations, including primary care providers, specialists, ancillary service providers, and so on. Information in the health record should clearly and concisely relay the full story of the care that is delivered. Sound information management practices are required to achieve this. The challenges of information integrity in the electronic health record (EHR) are different than those with paper records. For example, with an EHR there is the potential for data to be overwritten. This presentation will provide attendees with an overview of the risks of bad data, successful tips for mitigating errors in information, and best practices when working with an EHR. Methods: Other examples include the different methods that must be employed to make corrections, complexities associated with updating information in interfaced systems, and redundancies that can result from the use of copy/paste functionality. These challenges, which do not exist with paper medical records, pose significant risk for information integrity. Methods to be discussed include information capture, EHR management and use, hybrid records management, and sharing of information. Results: Best practices and successful tips for addressing the different methods used when incorporating information into the EHR. These will be discussed via a series of case scenarios which identify incorrect integrity practices and then discuss appropriate methods that would lead to better integrity. Conclusions: Data integrity is nonnegotiable. It gives clinical care providers the ability to trust EHR information to make important care decisions. In today's competitive and rapidly changing environment, healthcare organizations need sound information integrity practices that ensure the accuracy, consistency, and reliability of

59
the health information that is needed to support patient safety, quality initiatives, various reporting activities, and patient care across the continuum. CS2.2.2 Building a Systems Approach to Data Quality Agnes Vander Vecht 1; Jennifer McCallum 1; Kim Planques 1; Lisa Clarke 1; Monica Poole 2 1London Health Sciences Centre, London, ON, Canada; 2BORN Ontario, London, ON, Canada Introduction: On Saturday June 4, 2011 St Joseph's Health Centre stopped admitting women in labour as the obstetrical care services, including high-risk antenatal care, and the neonatal intensive care unit were moved to London Health Sciences Centre. The transfer of perinatal and NICU services was part of the acute care redevelopment project. As a result of the program move it became apparent that amalgamation of processes involving an existing Perinatal Database, the necessity of submitting to a new BORN Ontario Registry and documentation data quality were issues which needed to be addressed. Other issues were loosing the Epidemiologist Database Administrator in the program move and incorporating two processes for the extraction of perinatal health data, with two distinct reporting hierarchy. Since the program transition, Health Records, along with the remaining perinatal staff, obstetrical program Leaders, obstetrical physician representation and Decision Support, have been working collaboratively to identify the best processes and sources of information. Objectives: To work collaboratively through data quality initiatives; To utilize BORN Ontario web-based tool for data collection in a collaborative systems approach. Antenatal clinic areas will capture the antenatal information, registration clerks will enter the newborn demographic information, and Health Records will enter the labour, birth (Mother/Child) and postpartum (Mother/Child) health information into the BORN web-based tool. Midwifery would enter their information for all encounter types; To change the processes for entering information into the existing Hospital Perinatal Database; To educate people on the "data out" reporting tools in the new system and how they can be used to facilitate and improve care, do QI projects and report on care quality; To maintain the high level of quality that our physician leaders and researchers are accustomed to, as they provide high quality evidence based patient care and promote patient safety. Methods: The project team is creating a strategy for the realignment of initiatives and processes to meet the emerging needs for the collection of maternal and newborn health information. This strategy is based on the following: →Dimensions: Timeliness, validity, reliability, usability, and knowledge - to Action →Framework: A "Help it to happen" approach [dissemination, targeted messages and targeted reports] Results: Submission of perinatal information to BORN Ontario since April 2012; Improved Documentation; Reliable Information. Conclusion: The result of the above project has been a collaborative approach to data quality initiatives that result in a SMART strategy which is in alignment with London Health Sciences corporate strategic priorities, which include Performance Excellence, Scholarly Leadership and Exemplary Partnerships. CS2.2.3 Implementation of Enterprise-Wide EMR and Data Governance - Lessons Learned Rita Bowen HealthPort, Alpharetta, GA, United States Introduction: Does your organization need to improve data quality? Are you ready for meaningful use/data sharing? The current "age of accountability" demands compliance. This is a "must attend" session for HIM professionals involved in data governance and data integration initiatives. Attendees will learn how data governance impacts the conversion and quality control of data, and more importantly how to create a proactive plan for data governance. Methods: Speaker will share important steps for a proper data governance plan. Results: Attendees will learn how a data governance plan improves organizational design and development, ability for auditing and reporting, life cycle management for data, stewardship and value creation. Conclusion: By the end of this session, the participant will be able to: - Understand the roles of executive sponsors, stewards, and other parties involved with data governance. - Recognize data policies and progress indicators - Implement best practices for a successful data governance plan

60
CS2.3.1 Implementing New ICD Versions in a Complex Environment: The US Experience Margaret Skurka 1; Sue Bowman 2; Rita Scichilone 2 1Indiana University Northwest, Gary, IN, United States; 2AHIMA, Chicago, IL, United States Introduction: On January 16, 2009, the US Department of Health and Human Services published a federal regulation definitively adopting ICD-10-CM and ICD-10-PCS (Procedure Coding System) as replacements for the ICD-9-CM diagnosis and procedure codes, respectively. This regulation followed ten years of public debate and government hearings. The initial implementation date established in the 2009 regulation was October 1, 2013 (“compliance date”). In April 2012, a federal regulation was published proposing that the compliance date be pushed back to October 1, 2014 amidst opposition to ICD-10-CM/PCS implementation from certain healthcare industry sector, doubts about industry readiness, and providers’ concerns about costs and competing government initiatives. Oct. 1, 2014 is now a firm date for implementation. Methods and Results: Due to the size and complexity of the US healthcare industry, the migration to ICD-10-CM/PCS involves a massive transformational effort affecting many systems, processes, and people. A successful transition to ICD-10-CM/PCS requires careful strategic planning and coordination of resources across the entire organization. Key transition steps include establishing an interdisciplinary steering committee; assessing the impact of the ICD-10-CM/PCS transition across all operations; developing a budget; assessing the quality of medical record documentation; and assessing the impact on longitudinal data. The ICD-10-CM/PCS orientation and training process in the US is daunting. Multiple categories of data users require varying levels and types of education. These include coding professionals, physicians, clinical department managers, patient registration personnel, and quality management staff. Multiple resources and a variety of methods are required, including online (internet based) distance learning, books, workbooks, and webinars. Professional associations and industry groups provide timelines, checklists, readiness assessments, mapping tools and more to prepare a nation for change in the use of new classification systems. Conclusions: This paper address the process of migration and implementation efforts required to prepare a complex healthcare system for a new version of the classification. In addition, the education requirements are described in detail for the benefit of other countries that may be faced with a similar challenge. Risk mitigation strategies are also addressed. For example, anticipated reductions in coding accuracy and productivity can be mitigated with proper advance training and innovative documentation improvement strategies. CS2.3.2 Coder Productivity When Moving from ICD-9-CM to ICD-10-CM/PCS: A Study Susan Fenton 1; Mary Stanfill 2; Kathleen Beal 3 1Texas State University, San Marcos, TX, United States; 2United Audit Systems, Inc., Walnut Hills, OH, United States; 3University of Cincinnati, Cincinnati, OH, United States Introduction: The United States is implementing ICD-10-CM and ICD-10-PCS for all diagnostic and procedural coding by October 1, 2014. This is expected to have an impact across the healthcare industry. ICD-10-CM (the clinical modification) consists of more than 68,000 diagnosis codes compared to approximately 13,000 ICD-9-CM diagnosis codes. ICD-10-PCS has 70,000+ potential codes compared to just over 4,000 in ICD-9-CM, volume 3. The greater level of specificity and clinical detail as well as the improvements in the capture of medical technology advances in ICD-10-CM/PCS are expected to result in an improved ability to analyze trend and cost data; a reduced need for manual review of health records to perform research and data mining and adjudicate reimbursement claims; and the improved ability to ascertain disease severity for risk and severity of illness adjustment. Methods: Multiple coding professionals at an academic medical center, ranging from expert to beginning ICD-10-CM/PCS coders, participated in this study. Their time to code medical and surgical inpatient charts in ICD-9-CM was compared to the time to code using ICD-10-CM/PCS. Care was taken to simulate current revenue cycle workflow and consider all factors that impact coding productivity. Results: Overall on average it took 17.72 minutes or 69% longer to code a record in ICD-10-CM/PCS. Coders with comprehensive ICD-10-CM/CPS training took an additional 14.7 minutes (54.4%) per case on average. Coders who received only basic training needed an additional 17.0 minutes (81.8%) on average. Individual coder results ranged from 10.6 to 27.7 minutes. Conclusions: Previous coder productivity impact estimates for ICD-10-CM/PCS implementation in the U.S. may have been underestimated. Training appears to have an impact; however, this analysis did not find coder experience or education levels to be significant. Limitations of this study include the small sample size, the low number of coder participants, and the lack of longitudinal data.

61
Ensuring sufficient staff to support revenue cycle operations is a key factor to successfully transition to ICD-10-CM/PCS. Experience in moving to ICD-10 based code sets in other countries has shown that productivity levels drop by as much as 50%. This is the first study of the productivity impact in the United States. CS2.3.3 Improving Documentation for ICD-10: Challenges and Opportunities Melanie Endicott AHIMA, Chicago, IL, United States Introduction and Objectives: The transition to ICD-10 in the United States is requiring organizations to take a close look at their documentation to evaluate potential gaps. The use of clinical documentation improvement (CDI) professionals is crucial during this time of transition. Many challenges and opportunties exist for CDI professionals to work together with clinicians and coders to ensure a smooth transition to ICD-10. Methods: Leading up to the October 1, 2014 implementation date of ICD-10 in the United States, CDI professionals are working with clinicians to educate them on the nuances of ICD-10 to ensure that the appropriate documentation is included in the medical record documentation. Various educational modalities are being used, including verbal and written queries, and formal presentations to clinicians regarding documentation necessities. Results: The clinical documentation improvement efforts are improving the quality of the data, which results in better patient care. Obtaining the appropriate documentation on the medical record while the patient is still in the hospital is advantageous to both the caregivers for quality of care, and to the coding staff to have complete documentation to accurately assign codes, which will result in appropriate reimbursement. Conclusions: Organizations are seeing positive results with their clinical documentation efforts on both the bottom line and increased quality of care. Challenges do sometimes exist regarding physician buy-in to the CDI programs, but time, patience, and persistence can overcome this obstacle. The key is working together, not against one another to improve the quality of documentation, which in turn, improves the overall quality of care. CS2.4.1 Online Teaching, Making the Connection Leslie Gordon 1; Tracy Locke 2; Lynette Williamson 3 1University of Alaska Southeast, Sitka, AK, United States; 2Alfred State, Canandaigua, NY, United States; 3Santa Barbara City College, Oley, PA, United States Introduction and Objectives: This presentation will provide panel perspective and discussion on lessons learned from teaching online. Methods: Use of technology tools, email, forum discussion, external web links, and AHIMA Virtual lab will be discussed. This presentation will highlight the word ONLINE by using key words that will spark ideas and identify challenges; organization, optimize, overload, netiquette, navigate, leadership, integrate, insight, nurture, new, energize, and expedition. Results: Results will focus on tools and strategies that have worked in the online education for Health Information Technology, Medical coding, and Cancer Information Management (CIM). Conclusions: At the end of this presentation the following questions should be answered. How do you make the connection with your students when teaching online? How to you keep them engaged and active in the course? What is "good" online course participation? CS2.4.2 Online Learning: A Unique Saskatchewan Perspective Ida Sadowski Saskatchewan Institute of Applied Science and Technology, Regina, SK, Canada The Saskatchewan Institute of Applied Science and Technology (SIAST) determined that providing an online learning environment would benefit many students throughout the province who were either unable or unprepared to move to Regina for the on-campus Health Information Management (HIM) program. In 2004, the first course was developed by a project management team, with health information management (HIM) professionals serving as the Subject Matter Experts (SME's). The team also consisted of a project manager, course developer, graphic artist, and a media consultant. Every year since 2004, the HIM program has developed an online course, or moved on to revise many of the initial courses. The team has looked at new and innovative ways for students to receive content, just as students in a face-to-face learning environment would. The importance of interacting with peer students, as well as with software activities is considered the strength of the many online courses developed. The following is a list of some of the online activities which provide unique learning experiences:
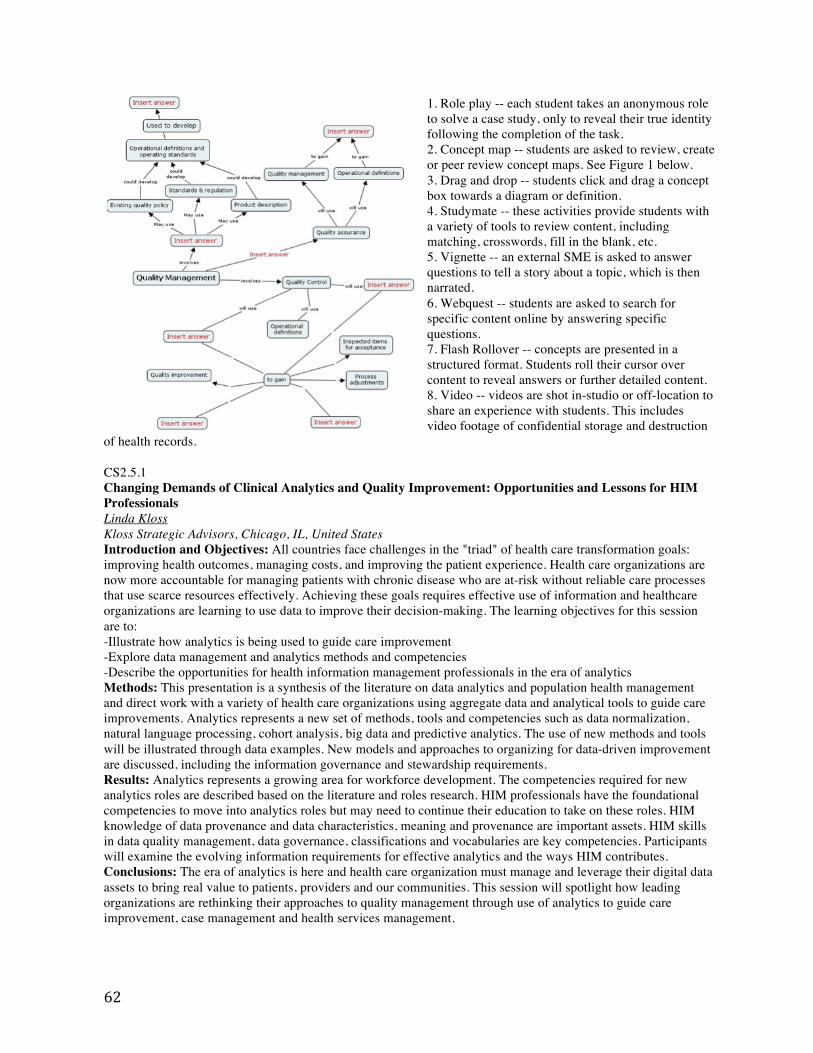
62
1. Role play -- each student takes an anonymous role to solve a case study, only to reveal their true identity following the completion of the task. 2. Concept map -- students are asked to review, create or peer review concept maps. See Figure 1 below. 3. Drag and drop -- students click and drag a concept box towards a diagram or definition. 4. Studymate -- these activities provide students with a variety of tools to review content, including matching, crosswords, fill in the blank, etc. 5. Vignette -- an external SME is asked to answer questions to tell a story about a topic, which is then narrated. 6. Webquest -- students are asked to search for specific content online by answering specific questions. 7. Flash Rollover -- concepts are presented in a structured format. Students roll their cursor over content to reveal answers or further detailed content. 8. Video -- videos are shot in-studio or off-location to share an experience with students. This includes video footage of confidential storage and destruction
of health records.
CS2.5.1 Changing Demands of Clinical Analytics and Quality Improvement: Opportunities and Lessons for HIM Professionals Linda Kloss Kloss Strategic Advisors, Chicago, IL, United States Introduction and Objectives: All countries face challenges in the "triad" of health care transformation goals: improving health outcomes, managing costs, and improving the patient experience. Health care organizations are now more accountable for managing patients with chronic disease who are at-risk without reliable care processes that use scarce resources effectively. Achieving these goals requires effective use of information and healthcare organizations are learning to use data to improve their decision-making. The learning objectives for this session are to: -Illustrate how analytics is being used to guide care improvement -Explore data management and analytics methods and competencies -Describe the opportunities for health information management professionals in the era of analytics Methods: This presentation is a synthesis of the literature on data analytics and population health management and direct work with a variety of health care organizations using aggregate data and analytical tools to guide care improvements. Analytics represents a new set of methods, tools and competencies such as data normalization, natural language processing, cohort analysis, big data and predictive analytics. The use of new methods and tools will be illustrated through data examples. New models and approaches to organizing for data-driven improvement are discussed, including the information governance and stewardship requirements. Results: Analytics represents a growing area for workforce development. The competencies required for new analytics roles are described based on the literature and roles research. HIM professionals have the foundational competencies to move into analytics roles but may need to continue their education to take on these roles. HIM knowledge of data provenance and data characteristics, meaning and provenance are important assets. HIM skills in data quality management, data governance, classifications and vocabularies are key competencies. Participants will examine the evolving information requirements for effective analytics and the ways HIM contributes. Conclusions: The era of analytics is here and health care organization must manage and leverage their digital data assets to bring real value to patients, providers and our communities. This session will spotlight how leading organizations are rethinking their approaches to quality management through use of analytics to guide care improvement, case management and health services management.

63
CS2.5.2 What Information Does the Patient Really Need - Challenges in Presenting Clinical Data to Non-experts Markus Stein 1; Wolfang Beinhauer 2; Udo Bräu 3; Elisabeth Büllesfeld 2; Katrin Fusko 1; Peter Görlich 1; Dagmar Häbe 2; Angelika Lackner 3; Sabine Radestock 1 1Ethianum Hospital, Heidelberg, Germany; 2Fraunhofer Institute for Industrial Engineering, Stuttgart, Germany; 3Meierhofer AG, Munich, Germany Introduction and Objectives: As part of a new approach to designing and implementing clinical pathways into hospital information systems our group wants to add a patient's view to his hospital treatment. The EDP-based pathway model will have an interface to appropriate devices to present the individual pathway to each chosen patient. The question to solve for the project PARTICEPS, funded by the German Ministry of Education & Research, is the patient's view. Does he really want to know all details about his hospital treatment or does he rely on the medical and nursing staff and neglect the information? Methods: A multi-disciplinary team, consisting of hospital managers, process managers, nurses, medical doctors and clinical psychologists, designed a questionnaire after having searched online database sources. 24 questions will be asked to at least 50 patients at two visits - the first at the hospital admission before surgery, the second 2 to 3 days after surgery. The questionnaire will not only try to build up a knowledge of the patient's needs for clinical data, but also how this should be presented to him with appropriate media. The study will start in October 2012 and the recruitment of patients will stop at the beginning of December 2012. Analysis of the study will be finished until the end of 2012. Results: As the study just begins no final results could be presented in the abstract but will be presented at the IFHIMA conference. Preliminary discussions and pre-tests may expect a high interest of patients in the knowledge of their clinical pathway. The minimum of 50 patients and the examination at two timestamps will lead to valid answers to our questions relating to the patients needs. Conclusions: The results of the study will be used for the design of the patient's interface to the PARTICEPS pathway software. The study will influence the software ergonomics and the way to cluster detailed path information. As the funding of the German Ministry is strictly limited to 2 years the PARTICEPS software prototype will be finished until April 2014. An introduction to the PARTICEPS project of a "information-chain" between medical experts, their clinical information systems and the patients will be added to the presentation of the study results. CS2.5.3 Transformation of Health Information Management (HIM) Workforce for New Roles and Elevated Positions: Oh The Places You Will Go! Barbara Odom-Wesley 1; Diann Brown Smith 2 1DeVry University, Irving, TX, United States; 2Texas Health Resources, Arlington, TX, United States Introduction and Objectives: This presentation explores changes in the HIM workforce resulting from the HIM revolution in roles, functions and responsibilities. Additionally, the impact of these changes on educational programs that prepares graduates for HIM positions will be discussed. Objectives include: 1. Describe changes in the HIM workforce as a result of the electronic health record revolution 2. Discuss the impact of changing roles on HIM education 3. Promote the HIM workforce to lead the revolution and embrace change 4. Identify tools for advancing to the C-suite; taking positions that make dreams a reality Methods: Diann H. Smith is currently the vice-president of HIM services for Texas Health Resources, a corporation which has 25 owned, operated, joint-ventured or affiliated hospitals with 4,100 licensed beds in Dallas-Fort Worth, North Texas. She will discuss how she made the transition from secretary to HIM department director to her current position with a career that spans 30 years. Dr. Barbara Odom-Wesley, AHIMA president in 2002, has worked as an HIM educator for 40 years. She has directed HIM degree programs in 3 different higher education institutions in Texas. As HIM roles evolve, educators are challenged to continue to prepare graduates who are currently competent. She will present changes that are required to prepare health information professionals for the future. The presenters will report on interviews of five HIM professionals who have made the transition to the C-suite. Their corporate experiences will be analyzed to convert their wisdom into tools that help others advance their careers. Results: The presenters will share strategies and tools to guide HIM professionals to higher level positions in the healthcare industry. The evolution of educational preparation for these elevated roles will be presented. Conclusions: The HIM roles and functions have been revolutionized by "game changers" including the electronic

64
health record and the emphasis on data integrity/quality. Experiences of successful HIM professionals will help identify tools that can steer others to higher positions. A review of new skills needed today will facilitate changes in education of the HIM workforce. CS3.1.1 Information Governance and Information Lifecycle - Unlocking the Value of Your Structured and Unstructured Data Michele O'Connor 1; Lorraine Fernandes 2 1IBM, Clifton, NJ, United States; 2IBM, San Ramon, CA, United States Introduction: An explosion of data and information is happening. Healthcare has always been data rich, mostly in an unstructured format. What we need to do is get more useful information from the data we have been collecting. This presentation will focus on Information Governance to create order in the data chaos by tying together the people, processes and technologies available to leverage the structured AND the un-structured data healthcare has been collecting for decades. Method: Presentation will include Customer use cases, analyst briefings and literature review. Results: Information Governance is the exercise of decision rights to optimize, secure and leverage data as an enterprise asset. Information Governance allows organizations to create order of this information chaos. It provides the means by which organizations can manage this explosion of information. Its about enabling people to do their jobs more effectively by providing them with the decision rights to optimize, secure and leverage enterprise data as an asset that can drive business opportunities. Current initiatives include analyzing existing data to understand disease processes and treatment methodologies as well as looking at patterns and trends in the data to help providers predict future events and intervene appropriately. One example is identifying key medical and social factors associated with Congestive Heart Failure. Having this data will enable researchers to target the key contributors that lead to readmissions for these patients. Armed with this knowledge, the healthcare team can provide the appropriate level of medical and social care necessary to keep the patient healthy and at home. The management of data through governance is no longer ‘optional’. Organizations have to do this to be competitive and information governance is strategically significant to addressing challenges of increasing costs, quality and access to healthcare services. This presentation will cover the Key master Data Governance Considerations. 1. What entities need to be governed? 2. How do you define these entities? 3. What is the business case to govern these entities? 4. Who owns the data? 5. Regulatory Compliance 6. Privacy and Security 7. Information Lifecycle Conclusions: Information governance doesn’t have to be difficult or mysterious. At its most basic, it involves organizing people, processes and technology to optimize, protect and leverage information—both structured and unstructured—as an enterprise asset that must be protected, meet quality standards and managed throughout its lifecycle. Even if you feel removed from aspects of governance, you can still learn the vocabulary and rules. It’s easy, effective and it can help solve a lot of information-related problems that may have eluded resolution for years. CS3.1.2 Big Data and Predictive Analytics are Transforming Healthcare Lorraine Fernandes 1; Michele O'Connor 2 1IBM, San Ramon, CA, United States; 2IBM, Clifton, NJ, United States Introduction: Healthcare is facing a global cost and quality challenge. This presentation will discuss Big data, its underlying principles, and how Big Data and predictive analytics can improve quality and reduce costs. Methods: Customer interactions, analyst briefings, literature review. Results: In this era of information overload a new catch phrase has arrived - it's Big Data. The volume of data is growing at staggering rates. The ability and desire to make use of this data has launched an era of data interrogation and predictive analytics. Many describe Big Data in principles of volume, velocity and variety. 1. Volume - A decade ago we talked about data in gigabytes or perhaps terabytes. Today the volume conversation is terabytes or petabytes. Big Deal, an online publication, says 90% of the data has been created in the past two years, thus highlighting the immense challenges of today, and even greater challenges of tomorrow. And, this data explosion sees no end in sight due to the volume of data being created by monitoring equipment in all industries,

65
social media, and adoption of standards increase structured data. 2. Velocity- The dramatic increase in stream data from sensors, monitoring equipment, and social media is creating velocity. The pace of change and computer advancement has accelerated beyond what anyone could have imagined even a decade ago. Open source platforms such as Hadoop are dramatically simplifying the complexity of analyzing high velocity data. 3. Variety - Healthcare has decades of unstructured data from paper -based records. Structured data is now becoming more common as a result of EMR adoption. Images from radiology, cardiology, as well as video surgery and telehealth create variety. Governmental agencies, healthcare providers, and payers (government and private) and pharmaceutical companies will benefit from Big Data such as, * Fraud detection * Monitoring data for disease or epidemiology surveillance * Defining best practices for business process re-alignment to improve quality and reduce costs * Integrating claims/payment and clinical data to define wellness and consumer empowerment activities * Research initiatives that need to combine clinical, climate, and genomics data in their research. Conclusions: While Big Data holds tremendous potential to help transform today's healthcare delivery system, this potential is fraught with managing the issues of privacy and security. Applying established Information Governance principles of managing privacy, defining and creating master data, securing data from both an internal and external perspective, and managing integration and data quality are keys to any successful Big Data initiative. The presentation will include case studies from healthcare that illustrate early use of Big Data, Information Governance, and predictive analytic solutions. CS3.1.3 Creating and Operationalizing an Enterprise Information Management Governance Framework in Alberta Health Services. Kathleen Addison ; Sharilyn Kmech Health Information Management - Alberta Health Services, Calgary, AB, Canada Introduction: The transition to a single provincial health service has identified significant data challenges. Clinical and non clinical information systems (paper and electronic) were implemented from a region-specific perspective with lacking and inconsistent use of data standards, data capture methods and different methods for data aggregation and data duplication. Automation and integration of information systems has exposed our data vulnerabilities. AHS Executives acknowledged the data AHS collects, stores, manages and maintains and the information derived from data are valuable organization assets however there was no centralized coordinated information management governance structure within AHS. Methods: The VP, Health Information Management, through key stakeholder engagement, created an Enterprise Information Management Governance Framework as a starting point to a larger Enterprise Information Management Program. This structure supports AHS in its assurance that the risks to its information, and thereby the operational capabilities and integrity of the organization, are effectively identified and managed.

66
Purpose: * Strategic oversight and leadership regarding information assets * Single formalized structure to standardize information management practices across AHS and minimize associated risks, regardless of the medium (paper or electronic) * Build awareness that data is an organizational asset to support business operations and strategic initiatives in alignment with AHS goals of quality, access, and sustainability * Established processes for the adoption, implementation, maintenance and consistent use of data and information standards to support interoperability Results: * Support quality and patient safety * Assure the data/information risks are effectively identified and managed * Enable enterprise-wide decision making * Ensure transparency of processes; * Ensure appropriate and consistent use of data standards for interoperability * Adopt common approaches to data and information management issues * Reduce effort and increase effectiveness, i.e. leveraging common work products (common data dictionaries) -- develop and document once, then re-purpose * Enable collaboration among internal/external stakeholders; * Support the Internal Audit and Enterprise Risk Management framework * Trust in the data as an enterprise asset Conclusion: The focus of the IMG Framework is at the enterprise level and continues to influence and improve the Information Management lifecycle, including consistent data, data definitions, data use and best practices. The IMG Framework is the first step in the progression of AHS towards an Enterprise-wide Information Management Program with the goals of increased adoption of data standards and standardized practice, reduced cost for development and use of standards, and reduced risk related to established standards.
CS3.1.4 The Impact of Multiple Custodians of EHR/EMR Content Karanne Miller Lambton ; Cindy Nikiforuk Alberta Health Services, Calgary, AB, Canada Introduction: Privacy Legislation, Regulation and Policy around the globe are written with the privacy and security accountabilities (access, use and disclosure) of a single information custodian in mind. In Alberta, Canada

67
a unique information sharing environment has developed, requiring a new perspective on custodial rights and responsibilities for electronic health information that is used across legal and jurisdictional boundaries. Methods: With the deployment of a single Ambulatory EMR that is documented and used by both private practice physicians and corporate health system staff, a mix of legal entities exists where no single clinician or single organization has complete control over the clinical content. An Information Sharing Framework (ISF) has been established between three corporate entities, the Alberta Medical Association, Alberta Health Services and Covenant Health. Results: The Information Sharing Framework Agreements establish Alberta Health Services as the information manager for a shared medical record and the rules for access, use and disclosure of information held in the shared ambulatory record. Special consideration is required when a medical record is shared among many providers with many custodians, including agreements as to how patient information will be captured, stored, managed and shared. The agreements include a Memorandum of Understanding, Information Sharing Agreement, Information Management Agreement and Information Exchange Protocol. Conclusions: This change requires an overall project management plan to create and manage the ISF operational rollout on behalf of all custodians. This plan incorporates work plans from AHS Operations (IT, HIM, Legal & Privacy, Security & Compliance), Communications and custodial organizations (regional/zone organizations, Universities, provincial medical association) and ISF Governance structure, including a provincial Information Stewardship Office. The purpose and nuances of each will be described in the presentation. CS3.2.1 International DRG Panel Makoto. Anan 1; Angela Kennedy 2; Joon Hong 3; Angelika Haendel 4 1Representing Japan; 2Representing USA; 3Representing Korea; 4Representing Germany Topics of this session include brief history of DRG implementation, the DRG version currently being used, where the DRG's are being used. CS3.2.2 CIHI's New Data Quality Initiative: Using Analytics to Support Ontario's Health Based Allocation Model Chrissy Willemse 1; Maureen Kelly 1; Stacey Colameco 2 1Canadian Institute for Health Information, Ottawa, ON, Canada; 2Ontario Ministry of Health and Long-Term Care, Toronto, ON, Canada Introduction: Data mining is emerging as a cost effective and timely method for examining data quality. The use of these techniques will become increasingly important as more jurisdictions in Canada move towards using healthcare data for funding purposes. The Canadian Institute for Health Information (CIHI) conducted a series of data mining activities to examine the quality of its data to support the Ontario Ministry of Health and Long-Term Care (MOHLTC) implementation of its new funding model – the Health Based Allocation Model (HBAM). The analysis provided information on the quality of the data used for HBAM and identified key quality areas to be monitored through regular data quality reporting. Methods: Ontario’s HBAM estimates expected health care expenses for hospitals based on patient demographic data, clinical data and financial cost data. The data mining analysis examined the clinical data from 2007-2008 to 2010-2011 housed in five CIHI databases: the Discharge Abstract Database (DAD); the National Ambulatory Care Reporting System (NACRS); the Ontario Mental Health Reporting System (OMHRS), the National Rehabilitation Reporting System (NRS), and the Continuing Care Reporting System (CCRS). Exploratory data mining analysis and data linkage were used to examine patterns, longitudinal trends and facility-level differences of select data elements that are used by HBAM. Data visualization techniques were also employed to highlight expected trends and for identifying data anomalies requiring further investigation. Results: The analysis performed provided evidence that the data are generally of good quality with some areas identified for ongoing data quality monitoring. Analysis of ambulatory care data and the coding of interventions within high-volume functional centres showed that the interventions reported by some hospitals were different than expected. For inpatient rehabilitation, it was found that large variation exists across hospitals in the coding of co-morbid conditions. Analysis of mental health episodes showed variation across hospitals in the reporting of service interruptions and days away from bed. Linkage analysis of the all the inpatient data revealed that most concurrent activity appeared to be legitimate but some data quality issues exist in the reporting of data elements that describe the patient's transition between services or hospitals. Conclusion: The results showed that the clinical data used by HBAM are generally of good quality. However, ongoing monitoring is essential to mitigate the influence that the funding model may have on coding and ensure that the integrity of the data is maintained. CIHI continues to work closely with the Ontario MOHLTC to produce

68
data quality monitoring reports based on results from the data mining analysis and will continue to work together to build a foundation for ongoing quality monitoring and continued data quality analysis. CS3.2.3 A Strategy for Training Data Users Aisling Mulligan ; Jacqui Curley Health Research and Information Division, The Economic and Social Research Institute, Dublin, Ireland Introduction and Objectives: The Economic and Social Research Institute (ESRI) has developed and supported the Hospital In-Patient Enquiry (HIPE) health information system to ensure that the scope and intensity of the hospital activity workload is accurately and comprehensively represented by this data collection system. Currently clinical data in HIPE are captured using ICD-10-AM/ACHI/ACS, 6th Edition. HIPE data have a wide variety of applications in the policy formation and planning of health services in Ireland. More recently HIPE data are been used by an expanding group of users with little or no background in the field of data collection or classification, this has brought its own challenges. The ESRI has striven to make data more readily available to an expanding group of users and we are now challenged with moving HIPE beyond the coding office and into the board room. Methods: Some of the challenges of access are that Data Users must understand the nature of the clinical classifications and the data collection process in order to interpret and analyse HIPE coded patient data. The ESRI has met these challenges by designing a training course for HIPE Data Users. The aim of this training is to provide Data Users with enough understanding to see the classification and guidelines as an important consideration in any analysis of HIPE data and to ensure that they know they can contact the ESRI for advice regarding classification, data collection and analysis. Results: There are challenges in providing Data User training to users who lack access to coding expertise and for whom training may not address specific questions. The training aims to introduce users to a number of important concepts; • principles of classifications and key coding guidelines • what is collected and what is not collected • analysing data sets across years and accounting for changes in classification, practice and variables • the importance of maintaining confidentiality and data security Training sessions illustrate the changes in guidelines, classification or data collection and include tailored case studies. Conclusions: User feedback from the training courses has been positive and there is now greater communication between Data Users and the ESRI regarding coding classification, data quality issues and data analysis queries. As HIPE data becomes available on an ESRI secure central server to authorised users the need for this training will increase. In these challenging economic times health service providers are seeking the optimum value from the health service and HIPE data provide the detailed information to support these initiatives. Greater use of HIPE data in evidence-based policy requires that data not only be available to users but that support is provided to them in how best to interpret and understand this rich source of hospital data. CS3.3.2 Analysis of the Questions about the Morbidity Coding Posted on the Online Coding Clinic YooKyung Boo 1; Whiejong M. Han 1; Hyunsook Lim 2; Youngjin Choi 3 1Eulji University, Seongnam, Korea, Republic of; 2Department of Public Health Administration, Hanyang Woman's University, Seoul, Korea, Republic of; 3Department of Healthcare Administration, Eulji University, Seongnam, Korea, Republic of Backgrounds and Objectives: Accuracy and consistency of morbidity coding are important in clinical research. This study identifies the type and disease groups, for which coders face difficulties in coding, by analyzing questions posted on Online Coding Clinic (OCC) operating by the Korean Medical Records Association. The study also investigates frequency and differences in questions, by size of hospitals as well as characteristics of questioners. Methods: The data analysis was conducted in following two stages: 1) a frequency analysis, a cross-tabulation and chi-square test were performed to identify differences in questions posted. 2) Fisher¡¯s exact test was conducted to identify differences in disease groups, by characteristics of questioners and size of hospitals. Results: General hospitals and hospitals with less than 500 beds are more likely to post questions on OCC. Interestingly, health information managers (HIMs) with more than 5 years of certification use OCC more than managers with less experienced. Morbidity codes showing higher frequency of the questions were as follows by International Classification of Diseases, 10th revision(ICD-10): S00-T98(Injury, poisoning, and certain other consequences of external causes), M00-M99(Diseases of the musculoskeletal system and connective tissue), C00-D48(Neoplasms), V01-Y98(External causes of morbidity and mortality), I00-I99(Diseases of the circulatory system), K00-K93(Diseases of the digestive system), and G00-G99(Diseases of the nervous system). In the hospitals with less than 500 beds, the codes shown the higher frequency were S00-T98(Injury, poisoning, and

69
certain other consequences of external causes) and M00-M99(Diseases of the musculoskeletal system and connective tissue) while in the hospitals with 500-999 beds codes S00-T98(Injury, poisoning, and certain other consequences of external causes), M00-M99(Diseases of the musculoskeletal system and connective tissue), C00-D48(Neoplasms), I00-I99(Diseases of the circulatory system), K00-K99(Diseases of the digestive system) showed evenly high frequency. Discussions and Conclusions: The Coding Clinic Committee should periodically review morbidity codes and provide accurate codes with a guideline. To improve quality of medical records continuing education or training to HIMs is suggested. In addition, building user-friendly database would help HIMs in search and identifying appropriate codes. CS3.3.3 Hospital Standardized Mortality Ratio Project Success Guides Creation of a Documentation and Coding Quality Framework Kathy Lavelle Lakeridge Health, Oshawa, ON, Canada Introduction: In 2009, we identified a trend towards increased mortality at Lakeridge Health as measured by the Hospital Standardized Mortality Ratio (HSMR). Analysis revealed that for the 2007-2008 and 2008-2009 fiscal years, our HSMR scores were 114 and 110 respectively. In response to this trend, we created an improvement team of frontline clinicians and administrative personnel to investigate and understand the causes of our rising HSMR. A Data Quality Steering Committee was created with senior management representation to oversee the project, and it was endorsed by the Medical Advisory Committee. We identified the need for an accurate HSMR that could inform decisions about clinical improvement initiatives. Methods: Since the HSMR methodology is highly dependent on accurate coding and clinical documentation, phase one focused on review of all charts contributing to mortality. We reviewed all death charts for 2009-2010 to capture discrepancies in documentation and coding of the most responsible diagnosis, palliative care status, and Charlson Index comorbidities. Reviews were conducted by two clinical auditors with the use of a standardized trigger tool. A tip sheet was created to aid clinicians in better documentation, the inpatient face sheet was re-designed, a feedback mechanism with physicians was created to enable chart completion and correction, and presentations were given to various physician groups. Educational sessions were conducted for coding staff, and quarterly coding quality reviews were performed. In phase two, there was a continued focus on accurate documentation and coding through on-going chart reviews, as well as identification of clinical quality improvement projects. Being confident in the data quality, we analyzed our 2009-2010 HSMR data to identify areas of clinical improvement and selected the implementation of an Early Warning System. Results: Prior to initiation of the project, our internal estimate for the 2009-2010 HSMR was 107. With the increased accuracy of documentation and coding through Phase One, our HSMR was reported to be 92. With the continuation of Phase Two, our HSMR continued to improve to 87 in 2010-2011 (statistically significant). The success of the HSMR project led to the creation of a Documentation & Coding Data Quality Framework that structured the processes into a standardized framework to guide future improvement initiatives. Conclusion: To utilize HSMR effectively, we improved documentation and coding practices to ensure the HSMR accurately reflected clinical practice. Phase one allowed us to improve our coding and documentation processes and to increase our confidence in the validity of our HSMR. It was only after this review process that we felt comfortable to analyse our HSMR to identify areas for clinical improvement. The standardized framework that was created can be utilized to monitor the quality of documentation, coding and care processes in a systematic way.

70
CS3.3.4 Impact of Information Technology on Clinical Decision Making and Clinical Documentation in Global Health: A Gift or Challenge for Clinical Coding? Chet Deshmukh VASTACCESS - A Global Institute for Clinical Health Information Management and Education, Apex, NC, United States Healthcare organizations are generating, acquiring, storing and destroying substantial amounts of data related to clinical care, hospital stays, outpatient treatments and same-day surgical interventions. Electronic Medical Records and "Cloud" Technology has expanded the creation of clinical data exponentially. While Technology can be an enabler of accurate and timely knowledge for clinical decision making healthcare providers and organizations are challenged with information overload. In-addition to the protected health information or PHI (defined under the Health Insurance Portability and Accountability Act ["HIPAA"] of 1996) there are volumes of electronic and paper files containing valuable data about physician/ non-physician clinician practice patterns that can directly impact decision making by physicians. Providers have increasingly adopted new technology to help them in their clinical decisions in arriving at a final diagnosis. The complex algorithms are based on mathematical models and decision trees that have a foundation on past clinical data. Applying that technology to reverse engineer critical thinking can be a paradigm shift as can be seen with Natural Language Processing engines. Clinical Coding is now increasing relying on use of Natural Language Processing. We are all too familiar with Differential Diagnosis and the logic of Clinical Coding. This presentation aims to address some critical elements on the future of Clinical Documentation and Clinical Coding through the fundamentals of Anatomy and Pathophysiology for Clinical Correlation. CS3.4.1 Transforming Health Information Management - The Evolution of the Health Information Management Professional Gail Crook 1; Kelly Abrams 2 1CHIMA, London, ON, Canada; 2CHIMA, Regina, SK, Canada Health care in Canada is currently undergoing significant reforms. The Electronic Health Record (EHR) has been advanced as an innovation that will both reduce health costs and improve patient care. Numerous studies and reference papers describe the advantages of the EHR; however, little attention has been directed to assessing the human and fiscal resources necessary to implement and effectively manage the EHR. As Canadian health settings move from paper to electronic health records, the role of Health Information Management (HIM®1) professionals will correspondingly change to meet the demands of an increasingly digital workplace. In 2009, the Health Informatics and Health Information Management Sector Study (O'Grady 2009) confirmed a

71
significant skills shortage and increasing demand for HIM and health informatics (HI) professionals by 2014. Study findings suggested that HI and HIM skills deficits would significantly delay the development and implementation of the EHR in Canada. EHR implementation is inarguably a laudable policy direction; however, significant challenges will remain without a corresponding systematic effort to develop the human resources necessary to support its implementation and maintenance. The Canadian Health Information Management Association (CHIMA) is the certifying body and national association for approximately 5000 HIM professionals across Canada. CHIMA has an essential role to play in the evolution of the HIM profession. As the certifying and accrediting body for HIM in Canada, CHIMA is uniquely situated to address the evolving skills and training needs necessary to support the transition to the EHR. A coordinated strategy developed in collaboration with health stakeholders at all levels is needed to identify and address the skills and training required to implement and maintain the EHR. Only then will the financial efficiencies and patient care benefits of the EHR be realized. In 2012, CHIMA completed two projects that examined HIM labour shortages and HIM skills upgrading necessary to support the transition to the EHR environment. The first of these initiatives, Workforce Transformation, described skills training, new roles, and career pathways for the changing HIM profession. The second initiative, Evolve the College, detailed proposed changes to HIM certification, specialization, and training. This presentation will detail the two project outcomes. 1HIM® is a registered trademark of CHIMA CS3.4.2 Health Information Management Professionals in Canada: Supply and Graduate Trends Julie Goulet ; Lan Wang ; Yasmine Léger Canadian Institute for Health Information, Ottawa, ON, Canada Introduction and Objectives: Effective health human resources planning and management is key to ensuring that adequate health services are available for all Canadians. The purpose of this study is to compare new Health Information Management (HIM) graduates to the supply of HIM professionals in Canada from 1992 to 2011. Methods: The Health Personnel Database (HPDB) from CIHI is a national database that maintains information on 24 health occupations in Canada. This study looks at HIM supply, demographic and graduate trends and the ratio of supply and graduates using 1992–2011 HPDB data. Results: In 2011, there were 5,010 HIM professionals in Canada, an increase of 23% over the past 20 years (1992-2011). From 1992 to 2011, all provinces experienced growth ranging from 2% for Manitoba to 107% for Newfoundland and Labrador, with the exception of Nova Scotia, which declined by 20%. The proportion of HIM professionals in Canada per 100,000 population decreased from 14.3 in 1992 to 6.5 in 2001 and then increased to 14.5 in 2011; an overall change of 1%. The Canadian population increased by 21% over the same 20-year period. In 2011, 60% of HIM professionals were 45 years old or over, 92% were female, 4% were male and 3% was gender unknown. Though HIM remained a female-dominated profession, the proportion of males was higher (10%) in younger age groups than in older age groups (5% or less). Between 1992 and 2011, the number of HIM graduates decreased by 6%. The proportion of graduates per 100,000 population declined from 1.3 in 1992 to 0.4 in 2001 and increased to 1.0 in 2011; an overall decrease of 23%. The proportion of the supply of HIM professionals represented by new graduates was 9.4% in 1992, 6.0% in 2001 and 7.2% in 2011; an overall decrease of 24%. Conclusions: Over the last twenty years (1992-2011), the number of HIM professionals in Canada continued to grow, despite a decrease in the number of new HIM graduates. Monitoring trends and understanding entry to the health workforce will provide valuable information to inform health system efficiency and effective health human resources planning now and in the future. CS3.4.3 HIT Workforce Needs Assessment Results: Implications for HIM Susan Fenton Texas State University, San Marcos, TX, United States Introduction: The United States healthcare industry is implementing electronic health records on a very large scale due to a federally-funded incentive policy. Estimates from the federal government indicated a need for an additional 50,000 health information technology (HIT) workers total. However, no study had confirmed this estimate, a secondary data analysis. Texas has one of the largest physician populations in the nation, approximately 600 licensed hospitals, and a number of private payors and associations offering support to physicians and others who are interested in adopting HIT. A strong healthcare industry, which requires a well-qualified HIT workforce, is necessary to support the large and growing Texas population.Texas State University led a state government-funded research project to perform a state-wide HIT workforce needs assessment and

72
educational institution inventory with the end goal of developing a multistakeholder, long-term Texas HIT workforce educational plan. Methods: The study began with 4 months of HIT employer focus groups conducted across the state and via web conferencing. A workforce study center assisted with the development of a survey utilizing the focus group results. The state-wide HIT employer needs assessment survey was administered online. Curriculum and syllabi data were collected from health information educational institutions. Results: Ninety-four (94) of 312 HIT employers responded to the online survey regarding the competencies they needed in their HIT workforce, as well as the numbers of HIT employees they were using in 2011, vacancies remaining in 2011, and the expected number of additional HIT employees they will be expecting to hire in 2013. The respondents, both provider and non-provider, reported an additional 1,341 employees needed between 2011 and 2013. A conservative extrapolation was conducted resulting in an estimated need for an additional 10,000 HIT workers needed. The HIT employers were also asked about the barriers they face when attempting to fill vacancies. Accessing qualified candidates; staff retention in a competitive market; lack of a well-defined HIT career ladder; the high cost of qualified consultants; and the lack of employee computer skills/ability to learn new skills were reported as barriers by more than 60% of the respondents. Conclusions: Challenges for HIM educators include increased collaborative efforts between employers, educational providers, public organizations, and and others which includes standardizing HIT roles, competencies and titles; developing common curriculum and training above and beyond the continuing education and health information management roles; as well as developing new models of education/employer collaboration to facilitate continued development of programs to meet employer needs in this fast-growing, evolving field. CS3.5.1 Ensuring Privacy and Security of Patient Information in a Mobile World Debra Primeau 1; Cynthia Doyon 2 1Prime Health Information Consulting, Torrance, CA, United States; 2Precyse Solutions, Wayne, PA, United States Introduction: Mobility is a clear avenue for improving patient care and lowering its costs. CIOs, Clinicians, and patients use smart phones and tablets to access electronic health records, double-check dosing information or drug interactions, and communicate easily with other care givers. While tablets, laptops, and smart phones can reshape our healthcare delivery processes and systems, the embrace of mobile devices creates many challenges for IT and HIM departments that support healthcare organizations. This presentation highlights the way changes in the use of mobile devices are affecting the security of patient and healthcare information. It will outline a set of best practices for controlling access within and beyond perimeter protections. Methods: Based upon research conducted through articles, government regulations, interviews of health information management and information technology professionals, and HIM and IT professional organizations, the presenters have identified specific approaches to minimize the risk associated with breaches of patient information accessed via mobile devices. Results: Mobile technology is being rapidly expanding throughout the world with at least 10,000 health related apps that can be downloaded to a mobile device such as an iPad, iPhone, and Android smart phones and tablet computers. These devices are increasingly being used by consumers and healthcare providers to manage various aspects of health maintenance and healthcare. The United States and world-wide health regulation and best practices are being identified to develop policies aimed at protecting the integrity and privacy of patient health records. A number of US and World agencies are identifying opportunities to regulate the use of the devices through various approaches in monitoring healthcare mobile device use. Healthcare provides are increasingly encouraged to develop privacy and security practices that ensure patient information is not compromised. Conclusion: Mobility is creating a fertile ground for innovation in patient care. More users have multiple mobile devices that run a myriad of applications and changes need to be made to accommodate the demand. Privacy and security policies and practices must be developed to address how mobile devices. The use of mobile devices brings new regulatory, legal and technological considerations for the management of health records. This is an opportunity for health information professionals to apply specialized skills and provide guidance to ensure patient information is kept secure and confidential in a mobile age. CS3.5.2 Social Media and Health Data Privacy Majorie Hendricks ; Jermaine Martin Jamaica Medical Records Assoc. Ministry of Health, Kingston, Jamaica

73
Introduction and Objectives: Health information management professionals play a critical role in the delivery of healthcare worldwide; through their focus on data collection, and the maintenance and use of quality data in private and confidential environment. It is therefore important that health information about patients be kept confidential in order to avoid the information being misused by unauthorized personnel. It is the aim of the Health Records units in Jamaica to enhance safety of all patients' health information, promote confidentiality within the services and maintain data integrity throughout. This can be achieved through the provision of adequate resources to effectively address the problems associated with any breech of privacy of patient's health information. In addition to this, ongoing training and sensitisation of all stakeholders is very critical. Methods: A qualitative research was conducted using random sampling with the use of questionnaires consisting open and closed ended items to gather the data. A total 100 questionnaires were distributed by hand to medical, nursing and health records staff and were later collated and grouped based on responses. This was then transferred to a spreadsheet and analysed using the Statistical Package for the Social Sciences (SPSS). Participants were 76 females and 24 males with age ranging from 18 to 60 years. Interviews and selected site visits were also done in order for the researcher to observe and assess the operations within health record departments. Results: There is a need for an overhaul of the current system governing safety, security and the release of patients' health information in order to facilitate improvement in the safety and security of patients' health records. Ambiguities exist among allied health care practitioners in relation to policies governing the release of client health information. Findings also revealed inadequate storage for health records, unsecured health records, among other haphazard matters such as the absence of clear policies within health care facilities to effectively deal with medical identity theft. The social media and the impact they have on confidentiality of and access to client information, were the most significant contributing factors in relation to unauthorized disclosure of patients' medical information. Conclusions: Initial results and feedback from the study indicate the need for health facilities to develop structured systems, policies and guidelines to govern the protection of patients' medical information against any unauthorized access and disclosure and the release of information. While these barriers exist, there is a need for ongoing sensitisation of all stakeholders on adherence toward current policies on the release of clients' health information. CS3.5.3 Mobile Devices- Are They Secure Enough for our Patient's Data? Aaron Hendriks University Health Network - Shared Information Management Services, Toronto, ON, Canada Introduction and Objectives: Mobile devices are becoming a common tool for providing patient care. Because of this UHN Information Security has evaluated the security of the most common Android and iOS devices. The purpose of the evaluation was to ensure the devices meet the data encryption requirements UHN has been mandated to meet for all portable devices. Methods: The UHN Information Security team has purchased and tested Android and iOS devices to perform security testing on the devices. All devices were given the most secure configuration possible. The android devices were configured with complex passcodes and fully encrypted. The iOS devices were given complex passcodes. After this configuration the devices were tested for what information could be accessed from the devices when in a locked state. Results: The android devices are incredibly hard to access any data on the device and the iOS only protects the OS, email and apps that are set to secure the data. All other areas of an iOS device are open even when the device is locked and the passcode is completely unknown. The data we accessed were all pictures as well as all data in custom and purchased apps that did not have the security configuration turned on. Conclusions: For these devices we have to ensure they are properly configured with secure passwords and that the encryption is set for the user. We also have to ensure the devices are not jail-broken or rooted as this often bypasses all security. Overall it is up to the organization to install mobile device management (MDM) systems as well as informing policies and procedures to the device users. We also have to ensure all the applications our organizations develop and those we purchase are configured to protect our patient’s data. If we lose patient trust to give us information, with a privacy breach, we are losing one of the primary tools we have at our disposal. CS3.5.4 Monitoring Access Patterns: If Credit Card Companies Can Develop Fraud Alert Technology, So Can We! Debbie Mikels ; Karen Grant Partners HealthCare System, Wellesley, United States

74
Introduction: This presentation outlines a research project conducted to develop data mining methodology in order to identify cases where there appears to be a high likelihood of inappropriate access. Today many Health Information Departments conduct random audits, complaint-based audits, and audits of "VIP's", however since most Users are accessing appropriately, audits are often very labor-intensive, and rarely find inappropriate behavior. We will describe a "Monitoring Access Patterns" Database that was created, containing Patient and User information from multiple source systems. Analysis of activity patterns was able to identify unusual patterns of activity that could then be validated through HIS analysis. Methods: Do you realize that every action taken when accessing a patient health record is audited? Although Health Information Services reviews audit reports, it is impossible to review reports of every access made to every record. An audit is often triggered by a patient complaint, an employee review of self-audit, or other means. This project would greatly enhance our ability to identify cases that may have greater likelihood of suspicious activity. Electronic patient information should only be accessed by Users as needed in order to perform their jobs. Availability of online medical records enhances quality and safety of care, allowing users to access the data when & where they need it; however, this also presents a potential security risk as Users could inappropriately access data unrelated to their job responsibilities. We would like to develop better safeguards that will promote a balance between ease of access and protecting confidential data. Adding hard-coded roles-based or rules-based technical controls would require a large investment in manpower to maintain and update static rules. The MAP – Monitoring Activity Patterns Research Project was conceived in response to our ongoing efforts to build adequate Chart Access Control (CAC) measures that would support appropriate access using technical controls within our online PHS Electronic Health Record systems. This study proposed that if we could gather enough information about the user/application and patient at, or as near as possible, to the time of access, then we could use this information to: 1. Better understand user workflows: WHO are our users and WHAT are they doing? 2. Use Data Mining to find patterns in user accesses to find potentially inappropriate accesses. This research project focused on developing and improving upon access pattern recognition in order to identify suspicious accesses. Our long term goal is to develop effective data mining models to intelligently and dynamically identify inappropriate accesses BEFORE they occur, and either prevent, or prompt users for additional information before access is permitted. Results and Conclusions: Results proved that data mining can in fact identify instances where there is a high potential of unauthorized access. CS3.6.2 HIM and Clinical Coding Revolution in the Kingdom of Saudi Arabia! Hussein Albishi Ministry of Health, Riyadh, Saudi Arabia It is my pleasure to write about our fast growing profession “Health Information Management” (HIM) which is considered the lifeblood of every healthcare organization. My first experience with the International Federation of Health Information Management Associations (IFHIMA) formerly known as the International Federation for Health Records Organizations (IFHRO) was back in 2009 in “Down Under” Australia. It was during the IFHRO SEAR & the Health Information Management Association of Australia (HIMAA) conference that I presented our country’s (Saudi Arabia) HIS update along with other Health Information Managers (HIMs) from international countries. Attending HIM, Clinical Coding, e-health and Health Informatics events is one of my professional development commitments as a HIM. Conferences, symposiums, workshops, and seminars allow for mixing with different professional HIMs and healthcare specialists whom we can learn from or exchange experiences with. In Saudi Arabia the HIM profession, as the profession is still considered to be new, is found in the Medical Records Department. This has been the case in many other developed countries such as the United States of America (USA) where Registered Health Information Administrators (RHIAs) where known before as Registered Records Administrators (RRAs). Back in 1991, my first boss was an RRA holder (Mr. Philip Venn). This was when I received my first job as a Senior Medical Records Clerk in the Saudi Arabian National Guard Health Affairs (SANGHA) King Khalid National Guard Hospital – Jeddah. But the HIM profession has witnessed a real revolution in the last ten years. The “Custodian of the two Holy Mosques” King Abdullah’s Scholarship Program and other healthcare organization’s scholarship programs have sponsored thousands of Saudi Nationals males/females to go overseas and seek the best education from any university or research center around the globe. Especially in an already existing shortage of and due to the lack of awareness of future opportunities that HIM degree can offer in Saudi Arabia as well as globally, a small percentage of those Saudi Arabian students have decided to study the HIM programs. In my opinion, I believe that it is a golden opportunity for us as HIMs working in Saudi Arabia to utilize the existing huge industrial, educational, and general developments in every corner that the Saudis are experiencing on a daily basis. “Marketing… marketing... marketing... for yourselves and your profession”, this was one of many valuable advises given to us as HIM students by Mrs. Barbara Postle

75
during our HIM program at Curtin University of Technology, Perth, Australia (2005-2008). The Ministry of Health Reforming its Hospitals’ Medical Record Departments There are 244 MOH hospitals and more than 2000 MOH primary care centers. Hundreds of Saudi Medical Records Specialists and Technicians are getting a huge support in terms of training/education and scholarships to make Saudi Arabia ready! CS3.6.3 A Comprehensive Workforce/Education Partnership Model for ICD-10 Implementation that Improves Understanding of Codes and Employee Satisfaction Lily Hsu 1; Diana Lindo 2; Kira Khazatsky 3; Jacqueline Donahue 3 1Massachusetts College of Pharmacy and Health Sciences, Boston, MA, United States; 2Boston Children's Hospital, Boston, MA, United States; 3Jewish Vocational Services, Boston, MA, United States Introduction and Objectives: Boston Children's Hospital (BCH) Medical Coding department requested a comprehensive model to prepare their staff to smoothly transition to ICD 10 codes by the U.S. October 1, 2014 deadline. BCH's Workforce Development office convened a meeting in January 2011 with Massachusetts College of Pharmacy and Health Sciences (MCPHS) and JVS Healthcare Training Institute. This partnership developed a model that integrates learning and academic support in a seamless format. The objective for this model was 100 percent student success and employee satisfaction. The curriculum was designed to provide a foundation in understanding the human body, clinical diseases and pharmacology. JVS conducted pre-testing in reading, writing, math and medical terminology to assess baseline levels of staff. Sessions were delivered weekly prior to the academic classes. These sessions strengthened the staff's pre-requisite skills needed to complete a university level program while still continuing to fulfill their full time work schedules. MCPHS developed the Basic Health Science Certificate that includes courses in anatomy and physiology, pathophysiology and pharmacology. Due to the complexity and specifity of the ICD-10 codes BCH wanted coders to recognize inconsistencies in medical records to avoid errors and improve processing. The objectives of the project were to: a. Develop a university level certificate in health sciences; b. Provide academic support before and during the program; c. Achieve 100% academic success among students. Methods: All courses were delivered in a blended learning format with half of the course content delivered asynchronously online and half delivered in class. The online component was accessible 24/7 through MCPHS. Project challenges included full commitment from the medical coders to the program, funding, curriculum development, range of prior college experience, age range and years of coding experience. None of the participants had experience with online learning. Results: The program was successfully launched with all 10 medical coding staff in July 2011. The academic program began in January 2012 and will end December 2012. At this time 100% of the students have met or exceeded the minimum academic requirement of 73%. Directors from the hospital report that staff performance has improved and that staff are applying the information they have learned to their work. BCH sees this as an indication of higher job satisfaction. Conclusion: The success of this model is due to the partnership that exhibited active involvement in all phases of the project. Communication was consistent throughout. This model is now being explored by other departments. CS3.6.4 Experiences Training of Transfer ICD 9 to ICD 10 at Primary Health Care in Indonesia to Improve the Implementation the HIS by MOH Elise Garmelia 1; Vensya Sitohang 2 1Pormiki, West Jakarta, DKI Jakarta, Indonesia; 2Center for Data Health and Information the Ministry of Health, Jarkarta, Indonesia Introduction: Indonesia is an archipelago of 17 thousand islands and have 1.800 hospitals such as government hospital, private hospitals and military hospitals and 9.000 primary health care. The Medical Record Department have Medical Record Director with variation graduate background in a hospital. Some of the preparation activities necessary for implementation provide benefits to the organization even before ICD-10 is implemented, such as medical record documentation improvement strategies and efforts to expand coding staff knowledge and skills. Educate senior management, IS personnel, clinical department managers, and medical staff on the coming transition to ICD-10 and the necessity for this transition (e.g., department managers' meetings, medical staff meetings, specialized meetings with senior management and IS). Method: Will be done training of transfer ICD 9 to ICD 10 to 139 district from 33 province i Indonesia. The audience are Medical record profesion who working at Primary health care and MOH distric personel from 33 province. The audience should fill in the material (pretest and posttest) at the training activity. The material were distributed
76
in some training event during Mei -- July 2012 with 210 samples were already filled by Medical Record staff (MRD) from primary health care and 190 staff from MOH District from 33 province The material data consist of 2 field questions ware as followed 1. The Capability of knowing data on IT system 2. Introduce about ICD 10 dan ICD 9CM. The data were collect and analyze by SPSS. Result: Medical record staff : Only 40 % staff answerd true and 32 % False and 18 % blank and 10 % not aplicable (Pretest) and average improve 28,6 % for all audience (posttest) MOH District staff : 46 % staff answerd true and 54 % blank (they do not know about ICD code) -- Pretest. Average 40 % all audience knowing about the ICD code (posttest) Monitoring and evaluation that ICD 10 already done in Primary Health care, but they do not used the indexing classification. Conclusion: Evaluate current data flow, work flows, and operational processes to identify processes and reports that will be affected and determine opportunities for improvement. Assess extent of changes to systems, processes, policies/procedures, and education needs; to improve the data quality between Primary health care -- District MOH and Central data and health Information of MOH . Educate data users on differences in classification of diseases and procedures in the new coding systems, including definitions and code category composition, in order to assess impact on data trends. CS3.7.1 An Effort to Improve Health Care in Ethiopia: Building the HIM Profession in the Country from "Scratch" Sheila Carlon Regis University-RHCHP, Denver, CO, United States Introduction and Objectives: Ethiopia is one of the poorest countries in Africa and the world and healthcare isn't always at the top of the list of important initiatives since food, shelter and other basic needs are first and foremost. However, in an effort to improve the current health care delivery, the medical profession and researchers in Ethiopia realized that the missing piece in their care was documentation. They looked to other countries for expertise in how to bring this missing piece into their infrastructure. Presentation Objectives: After attending this presentation, attendees should be able to: 1. Understand the barriers and challenges in implementing HIM/HIT in third world countries. 2. Articulate the steps involved in developing the profession in third world countries. 3. Understand the cultural challenges in implementing the HIM/T profession in other countries. 4. Understand the infrastructure required to implement the HIM/T profession other countries with limited resources. 5. Identify ways to help and provide resources and assistance in implementing HIM in other countries. Results: The curriculum was finalized, developed and rolled out to the Health Science Colleges as HIT Curriculum and a Diploma Program in the Ethiopian Educational Structure with the first classes to graduate in Summer of 2012. Conclusions: While there were some challenges along the way and some changes are being made due to recommendations from the Ministry of Education regarding several curricular programs, the health care and education community is confident that HIM/T will be a growing field and will improve the delivery of health care through quality information. CS3.7.2 Improving Availability of Laboratory Test Results Sooneeraz Monohur ; Satianand Bheekun ; Goolam Rassool Lall Mahomed ; Champa Ramdhean ; Neerunjun Gopee ; Nasser Jeeanody Ministry of Health and Quality of Life, Port Louis, Mauritius Introduction: The objective of the study was to identify the factors leading to the unavailability of test results for patients seen during Sorted outpatient clinics of public hospitals and to make recommendations to improve the situation. Methods: The study was carried out on the activities of the laboratory department and the health records sections of ten public hospitals and the Chest Clinic from 15 to 17 November 2011. Randomly selected officers of these two departments were requested to complete specific questionnaires. The opinion of doctors and nurses, who were selected using the stratified sampling method, was also anonymously captured on related issues.

77
Results: The study shows that 21% of laboratory results were not available at the beginning of the outpatient clinic; 10% were traced during the clinic while 11% remained untraced at the end of the clinic. On average, a patient has to wait during 34 minutes because of a missing result. It was also found that tests were either not carried out or reports were not released by the laboratory department for around 3% of collected specimens. Unavailability of laboratory reports prior to consultation at the sorted OPD results from shortcomings at the level of form layout, filling of request forms, phlebotomists' aptitude, communication, results notification, staffing requirements, adequacy of tools and equipment, despatch system and patients’ commitment. Improvements can be achieved through a shared responsibility of management, staff and patients. Conclusions: During a half-day dissemination workshop, all relevant stakeholders agreed on the following: Doctors should be solely responsible for the filling of request forms to ensure completeness and to prevent abuse. Pre-printed patient identification stickers should be introduced. The counter service at the laboratory should be reviewed and a robust despatch system should be put in place. Request forms should be made more user-friendly and a computerised local area network be established at every hospital for the timely issue of copies of laboratory results. Health records staff should be recruited and medical records procedures and working arrangements should be reviewed for the proper coverage of outpatient clinics. Training should be provided to phlebotomists and the use of vacuum syringes should be considered. Patients should be regularly informed about the established procedures. CS3.7.3 Impact of Technology on Health Information: An Overview of Health Management Information System of Rajasthan, India. Divya K Bhati Indian Institute of Health Management Research (IIHMR), Jaipur, Rajasthan, India Introduction: India is a large country with population of 1.22 billion and complex health system where health of the people plays a significant role in overall economic and social development of a nation. In 1946, the Bhore Committee, India formed the basis of the health system and sound health information system. Health information system is composed of subsystems which includes information on demography, vital events, health status, environmental health statistics, health resources, health services utilization, health outcomes also health development financial statistics. Objectives: This study is an attempt to give a overview of the health system of Rajasthan, India and management of the information with the help of technology at each level of health system. Also, identify the challenges in the existing Health Management Information System. Materials and Methods: A cross-sectional study was designed to understand the health information system of Rajasthan, India. In-depth interviews were taken from health personnel at different levels of the health system i.e. Sub-center, Primary health Center and Community health Center. Secondary data collection included review of annual reports of Ministry Of Health and Family Welfare and Central Bureau of Health Intelligence and registers from the selected health facilities. Results: In terms of monitoring child health, it is one of the largest e-government projects of the country. As a part of Health Information System for Government (HEALING), this on line system makes it possible to track every single pregnant woman in the state and provide subsequent health services till the delivery and immunization of every child till the age of sixteen. The Pregnancy ,Child Tracking and Health services Management System is extremely useful in ensuring better health for women, minimizing maternal mortality, neo natal mortality and in tracing areas with decreasing sex ratio at birth. The challenges were mainly related to sustainable use of information, cross-verification from the source, inconsistencies within two datasets, staff adaptability issues for new system, work overload, duplication of information and lack of logical planning and training huge manpower, logistic issue like maintenance of computer systems and lack of electricity to continuously use the systems, data privacy and confidentiality issues lastly, there is no Health Management Information System policy initiated by the government. There is a feedback system in place which can work as an opportunity where the issues can be resolved collectively by two-way approach i.e. from health personnel and governance. Conclusion: Technology is the driving force of any civilization. There is a paradigm shift from traditional methods to use of information technology in health. In a growing world, this technology is playing a vital role in healthcare and it has changed the way how healthcare is delivered and monitored in Rajasthan, India. CS3.7.4 Two Way Web-based Interactive Video EConsult System (TWIVeS): A Sustainable Telehealth Solution for Remote and Rural Area

78
Kenneth Nwosu ; Norm Archer McMaster University, Hamilton, ON, Canada Introduction and Objectives: This paper proposes a sustainable Telehealth solution for access to care in remote and rural communities with critical shortages of highly trained healthcare providers. Many remote areas suffer shortages as a result of internal emigration to urban centers, brain drain to other countries, low workforce productivity, or population growth. In certain countries, existing medical and nursing schools in these communities cannot train enough workers to meet the increasing demand for services. The objective of this work is to demonstrate a Proof of Concept (POC) of a browser-based video consult application (TWIVeS) that runs on low bandwidth Internet network connections and offers an inexpensive care alternative best suited for remote/rural communities and emergency situations, when commuting to a medical appointment is not an option. Methods: A search of the literature confirmed the high cost of telemedicine solutions and some discussion of sustainable alternatives for areas with limited funding and health system capacity. This proposal describes the development of a Proof of Concept (POC) to review the feasibility and sustainability of a system for remote access to medical consults that is ready to be deployed in regions with poor access to local medical care and with low Internet bandwidth. Results: As with many technological innovations in healthcare, assessments of telemedicine and correlative policies are driven by economic and technological criteria that emphasize cost reduction and technological efficiency. With relatively simple Internet devices, users of TWIVeS (including enrolled patients and health care workers) can connect with and access the services of healthcare providers at distant locations for assistance with delivery of medical diagnosis and advice. Using this system, a patient could connect through the Internet with a healthcare provider remotely from home or by visiting a community health center with Internet access. Conclusions: This proposal delivers a sustainable web-based video consult application for healthcare delivery in rural areas; enabling community health workers and enrolled patients to access the services of healthcare providers at distant locations. CS4.1.1 Global Standards: Making a Difference in Health Information Management Rita Scichilone American Health Information Management Association, Washington, DC, United States Introduction and Objectives: Without standards the world would be a different place entirely. In 2011 AHIMA became the American National Standards Institute’s (ANSI) designated secretariat for the International Organization for Standardization’s technical committee 215 for health informatics (ISO TC 215). Over the last decade, Health Information Management (HIM) professionals have been called upon to participate in standards development activities in order to ensure the inclusion of HIM principles, best practices, professional guidance and ethics. The objective of this work is to demonstrate the compelling need for HIM participation in global standards development. Methods: Using examples from recognized global standards development organizations, examples of HIM standards are explored and compelling reasons for participation offered. The following global standards are included in this study: 1. International Organization for Standarization Technical Committee (ISO TC 215) Health Informatics 2. Health Level Seven (HL7) 3. International Health Terminology Standards Development Organisation (IHTSDO) 4. World Health Organization Family of International Classifications (WHO-FIC) Results: Around the world there are two types of standards impacting HIM: The first is a formal process is used to create the standard such as the established ISO process. The second type of standard is not formally developed by an authoritative body but generally considered and agreed on as a normative process or approach. An example of this type is the accepted use of Microsoft Word® for preparing an abstract for consideration for an international professional congress or convention. Conclusions: HIM professionals, their professional associations and societies must all become more aware of and participatory in standards affecting their future. This profession collectively possesses a rich body of knowledge to inform future standards development based on sound information management principles and established practice standards. This knowledge must be shared with standards development organizations to continuously improve the utility and usefulness of mandated or agreed upon standards used in professional practice settings. CS4.1.2 Standards for Health System Use: Development of a Canadian Institute for Health Information Reference Data Model

79
Dawn Nicolson ; Cristina Tomsa ; Mark Fuller Canadian Institute for Health Information, Ottawa, ON, Canada Introduction and Objectives: The Canadian Institute for Health Information (CIHI) is an independent non-profit organization whose mandate is to lead the development and maintenance of comprehensive and integrated health information that enables sound policy and effective health system management that improves health and health care. At the core of CIHI's business is Health System Use (aka "secondary use") of data. Because many existing reference data models such as HL7's Reference Information Model have a Point of Service focus and do not include concepts specific to health system use, CIHI identified a need to develop a reference data model that would represent health system use and enable semantic interoperability and data integration among CIHI's data assets. Methods: Requirements for a reference data model were gathered through consultation with representatives from across CIHI's business areas. These requirements were used to develop health system use concepts that were common or significant to CIHI's business. Supporting metadata was developed and documented in a data dictionary that adapted the ISO 11179 standard to ensure that documentation of the metadata was standardized. Where feasible, an effort was made to align the concepts to pan-Canadian EHR and international standards. A governance structure was developed that allowed business areas to confirm that the concepts accurately represented and met their requirements before final approval was granted. Results: 18 concepts were approved and included in the first version of the reference data model. The model was validated through use in a number of new development and re-engineering projects. The validation process resulted in the model being established as a CIHI standard to be used for all new developments and re-engineering projects. A top-down bottom-up approach allows for changes and additions to the reference data made to be made iteratively. Conclusions: The reference data model has enabled CIHI to collect, store and analyze data in a consistent manner for health system use and as a result, support data integration and semantic interoperability for analysis and reporting across the continuum of care. There has been some discussion regarding the potential of using the CIHI reference data model as a pan-Canadian Health System Use reference data model in the future. CS4.1.3 Building the EMR Value Proposition Through an Integration Engine Gary Folker ; Chris Hobson Orion Health, Toronto, ON, Canada Introduction and Objectives: This presentation will provide a look at the architecture behind a large-scale electronic medical records (EMR) integration project and its role in establishing much-needed industry standardization and driving the highest level of EMR penetration in the country. Methods and Approach: The project was piloted in early 2010 with eHealth Ontario, OntarioMD, North Simcoe Muskoka, Central West LHINs, and included four hospitals, five physician family health teams, two EMR systems and approx 130 physicians. The system is now being rolled out across Ontario. Through this approach, hospitals and Independent Health Facilities (IHF) can use the system to transmit reports into community physicians’ EMRs that are Ontario, Specification 4.0 Certified. The ability to integrate multiple data streams from multiple resources has been a major catalyst in speeding processes, improving doctor/patient relationships and maximizing the value of EMR adoption. A key foundation for enabling the sharing of data is the Orion Health Rhapsody Integration Engine. The Rhapsody solution maps text-based reports in a variety of formats from hospital-based systems for transformation into a standards based Ontario EMR Core Data Set in XML format which is now part of Ontario’s EMR Specification 4.0 certification for all funding eligible vendors in Ontario. With this approach, patient information can be integrated from any Ontario hospital to any certified EMR through a single standard interface without the physician’s practice needing to purchase expensive proprietary interfaces. Results: Evaluation findings to date have indicated the following: - A reduction in input and transmission of hospital-based reports to the EMR from 12 days to approx 30 minutes after transcription - A reduction in time spent by the family health team on scanning, filing and inputting data into the EMR from 4.5 hours one day to two - From a hospital perspective, savings over the course of one year include reducing costs, duplication, and improving the reporting accuracy - Faster information access supports improved coordination and quality of care; reduces patient anxiety and improves their satisfaction with the healthcare system. Conclusions: eHealth Ontario’s provincial strategy is to accelerate the deployment of hospital report offerings. To that end, the system lays a solid foundation for a broader exchange of health data, because of its flexibility and

80
ability to deliver reports from different sources into the EMR. Through these efforts, the province is moving to a single standard that can be leveraged for all EMR vendor offerings without the need to incur the high costs of building individual interfaces to different reporting systems. The system offers a viable, cost-effective means to increase EMR utility. CS4.2.1 To Improve Response Rate for Consultation by 6-Sigma Management Technique in a General Hospital Misook Kim Shinheung College, Eujungbu, Kyunggi, Korea, Republic of Introduction: Response rate for consultation is one of indicators to measure quality of medical care in hospital. The contents of consultation report influence doctor's making decision in terms of rapid and accurate medical care, patient's satisfaction. Also if it is delayed to answer for consultation and to write the answer report for consultation, it can cause patient's dissatisfaction and the loss of hospital income. To keep high response rate for consultation is a necessary condition for improving quality of medical care. Our government makes the criteria of response for consultation, the items to evaluate the quality of consultation and requires to keep it strictly for all hospitals. We purposed to improve quality of medical care and make optimal response system for consultation by management of response rate for consultation and to fulfill government's requisitions for hospitals. Methods: We used 6 sigma management technique as a methodology to improve the response rate for consultation, classified into emergent type and regular type. The emergent response was defined as the situation, which of the result of consultation was written in medical record within 24 hours after requested doctor examined the referred patient. We surveyed the doctors(33staff doctors, 55 resident doctors)by questionares about existed criteria of consultation response and analyzed it by excel. We collected those from 2th March to 12th March in 2010. Also we analyze 3.371 data items by Excel, Minitab from 1st January to 28th February in 2010. The sigma level of consultation response was calculated 2.4 sigma in regular cases, 1.95 sigma in emergent cases, and then we set a goal to 3.0 sigma both. Results: There were significant problems to delay response for consultation, we found that doctors did not recognize the importance to write response report for consultation, it was impossible to check the consultation report in real time, staff doctors were not interested in answering requested consultation, unnecessary request was done for just a diagnostic test. We called those critical to quality(CTQ) in 6 Sigma management technique and analyzed those by why-why diagram, mind map, excel. We planed to resolve those problems after analysis. As a result of acting as planned, the response rate for consultation improved remarkably. Conclusion: We performed quality assurance activities to improve the response rate for consultation by 6 sigma management technique in order to enhance quality of medical care. We set the goal to 3.0 sigma when we started this project, however we have achieved 2.7 sigma in regular cases, 2.3 sigma in emergent cases. Also we got some financial profit, which is 6.5 million won per one year through this project. We are going to carry out this project continuously by updating methodology. CS4.2.2 Health Information Management and its Impact on Health Care Consumers Julie Wolter 1; Marsha Dolan 2 1Saint Louis University, St. Louis, MO, United States; 2Missouri Western State University, St. Joseph, MO, United States Introduction and Objectives: Health Information Management (HIM) and its impact on healthcare consumers is a topic that has not been widely explored, yet we know that on a daily basis HIM professionals provide assistance outside the job to others who need assistance with understanding and navigating the healthcare system. This presentation will highlight the expertise that HIM professionals bring to the everyday lives of family and friends to help make a difference as they work their way through the healthcare maze. Methods: In the spring of 2012 a survey was sent to HIM professionals in Missouri, USA. They were asked how they assisted their family and friends with healthcare issues using their HIM skills. It is anticipated that the survey will be sent nationwide in the fall of 2012 and, potentially, internationally in the winter of 2012/2013. Results: Missouri survey respondents overwhelmingly stated they were actively involved helping family and friends to navigate the healthcare system. Most assisted with access to their patient information, going with family to doctor visits, interpreting test results, understanding healthcare or medical bills, and helping with creation of a personal health record. Our hypothesis for the nationwide survey would be that the results are similar. It will be

81
very interesting to see the results from the international survey. With the varied healthcare systems and HIM education the results could be very different. Conclusions: HIM professionals are the "go to people", both on the job and at home. From explaining disease processes to describing how to get copies of health records, we interact on many different levels with our families and friends. This presentation will describe all aspects of health information management and how HIM professionals can engage with the healthcare consumer. CS4.2.3 Defining Hybrid Opportunities for the Health Sector: eHealth Occupations Sandra Irobi ; Meenakshi Gupta Information and Communications Technology Council of Canada, Ottawa, ON, Canada Introduction and Objectives: New global paradigm in professional practice shows the evolution of hybrid occupations, a combination of two or more traditional disciplines. Defining opportunities that exist within hybrid disciplines, such as eHealth is essential in addressing skills shortage and human resource challenges. In Canada, minimal work has been done to clearly identify and define the spectrum of key in-demand eHealth occupations. No standardized profiles have been developed that describe competencies required for professional practice in eHealth, nor that targets mitigating challenges and knowledge gaps between existing training programs, and the acquisition of relevant skills required to function in such uniquely hybrid occupations. From 2010 to 2012, ICTC’s eHealth project in Canada, aimed at identifying eHealth priority occupations and developing competency profiles that facilitates human resource strategies targeted at training and recruitment. In this paper, we present the results and challenges of this project. We also describe ICTC’s methodology for competency framework that ensures synthesis and verification of priority occupations from first principles and an iterative profile development process. The methodology can be generically applied to other fields. Methodology: The methodology developed and used facilitated synthesis of eHealth occupations from interacting disciplines, and the development of competency profiles for each occupation iteratively. It has three phases: occupation synthesis, profiles development, and integrated validation phases. The occupation synthesis phase comprises sector scoping and verification, featuring research, data collection, key informant interviews, online survey and data analysis to determine industry trends. In the profiles development phase, straw models were developed and populated by subject matter experts (SMEs) using the 3PER method, which analyzes and highlights Problems, Prospects, Processes, Expectations and Realities for each occupation. SMEs provided descriptions, sample job titles, typical backgrounds, key activities, tasks, business/interpersonal and technical competencies. Phases were verified and validated independently and integrally. Over a period of 24 months, about 2,000 SMEs were engaged from the academia, public and private health sectors, ICT vendors and other stakeholders across Canada. Process verification was also performed to ensure quality assurance. Results and Conclusion: Our results show that the eHealth space comprises more interacting disciplines than Health and ICT. Twelve eHealth priority occupations were identified. For each identified occupation, competency profiles , which express skills, knowledge and abilities required to successfully perform each job has been developed. Sample use cases for the profiles were collated and analyzed. The results show that profiles are easy to adapt and apply irrespective of organizational structures and uniqueness. CS4.3.1 Examples of Electronic Medical Record Technology in a Bachelor Degree Health Information Management Curriculum Megan Tober ; Toni Windquist ; Marybeth Pieri-Smith ; Thomas J. Hunt Davenport University, Grand Rapids, MI, United States Introduction and Objectives: This presentation will provide example learning activities utilizing the American Health Information Management Association (AHIMA) Virtual Lab inpatient electronic health record software, as well as MedTrak outpatient electronic health record (EHR). The activities are utilized in parallel online and traditional on-campus learning environments. It also addresses the practices of using virtual labs to teach information and communication technologies, specialty software, and health information systems used in the healthcare industry. The presentation will discuss the benefits and challenges of using EHR technology in both the online and traditional classroom setting. Methods: Learning activities in relation to various aspects of the EHR in the inpatient and outpatient settings such as release of information, deficiency analysis, and document creation, clinical pathways, and more were implemented in various phases of an American Health Information Management (HIM) bachelor degree program. The program is delivered in both online and on-campus formats. Results: Exercises utilizing both the AHIMA Virtual Lab and MedTrak were successfully implemented in 100,

82
200, 300, and 400 level coursework in online and on-campus delivery methods. This provided exposure to the technology at all levels, and a progressive building of skill with the specific applications with the overall concepts related to planning and policy. Conclusions: There were delivery challenges in both online and on-campus settings; however, the benefits appear to outweigh the challenges. The examples of exercises and systems used as well as pros & cons encountered could assist in the widespread adoption of EMR technology in the classroom. CS4.3.3 Preparing Nursing Graduates for the Electronic World of Health Care Delivery Anna Sherlock 1; Kristine Crosby 2 1Canada Health Infoway, Toronto, ON, Canada; 2Canadian Association of Schools of Nursing, Ottawa, ON, Canada Introduction: Information and communications technologies (ICTs) are increasingly used to support the delivery of patient care. Yet, the growing use of electronic systems presents a new set of challenges for undergraduate students enrolled in health science programs. Early understanding of, and exposure to various point-of-care systems as well as interconnected systems can significantly impact how trainees learn and develop clinical decision making skills. To help ensure the next generations of nurses are ready to practice in a technology-enabled environment when they graduate, Canada Health Infoway (Infoway) has established a project with the Canadian Association of Schools of Nursing (CASN). Project Objectives: The objectives of the three-year Nurses-in-Training initiative are threefold: 1) To promote a national dialogue among nurse educators, informatics experts, and nursing students on integrating nursing informatics into entry-to-practice competencies; 2) To increase the capacity of Canadian nurse educators to teach nursing informatics; and 3) To engage nursing's key stakeholders in developing nursing informatics outcome-based objectives for undergraduate nursing curricula. Methods: An initial set of nursing informatics competencies was drafted by a working group based on an extensive review of both academic and grey literature from national and international sources, as well as the existing provincial and national regulatory competencies. An initial draft of thirty competencies was presented at a National Stakeholder Symposium attended by over 50 nursing informatics experts from across Canada. The second draft of the document, consisting of 20 competencies was then sent to the Deans and Directors of CANS member schools and was presented to Infoway's Nursing Reference Group and at the 2012 CASN Nursing Research Conference for feedback. Project Outputs: The final document, titled "Nursing Informatics Entry-to-Practice Competencies for Registered Nurses" is a foundational document containing nursing informatics competencies that all registered nurses should possess upon graduating from an undergraduate nursing program in Canada. In addition, the supporting document, "Nursing Informatics Inventory: A Report of Existing Teaching and Learning Resources", was developed to help nursing educators incorporate the competencies in to their core curricula. Plans are also underway to develop a series of learning modules for nurse educators and students. Conclusion: The CASN-Infoway Nurses-in-Training initiative aims to improve clinical practice and patient care by supporting nursing faculty and students in their adoption and use of ICTs. To use information systems effectively, students must learn how health information within these systems (i.e., care plans, laboratory results, or medications) is used within the context of the health care system in combination with the delivery of compassionate, competent, and safe patient care. CS4.4.1 Progress Report on an International Examination for Morbidity Coders Joon Hong 1; Carol A. Lewis 2 1WHO-FIC Education and Implementation Committee, Goyangsi, Kyunggido, Korea, Republic of; 2WHO-FIC Education and Implementation Committee, Rockville, MD, United States Introduction and Objectives: For the past decade the World Health Organization Family of International Classifications (WHO-FIC) and the International Federation of Health Information Management Associations (IFHIMA) have been working together to develop an international coder training and certification program. The goals of the program are production of high quality, consistent and timely coded health data and increase of the international coder workforce with well-trained coders. Methods: After awarding international certificates to 79 ICD-10 mortality coders in four countries in 2007, the feasibility of awarding international certificates to morbidity coders was explored and a preliminary survey was

83
conducted with positive results. A pilot test for experienced morbidity coders was developed and conducted in Korea in 2010 and repeated in Japan, Jamaica, Sri Lanka and Sweden in 2011. The tests were not for awarding certificates but for obtaining information regarding an international examination for morbidity coders. Results: Even though the test results were disappointingly low, the pilot tests provided much useful information for improving basic and continuing education programs for morbidity coders. The project also identified the resources required to develop and conduct such examinations. Conclusions: Based on the information and experience gained from the 5 pilot tests, in March 2012WHO-FIC Education and Implementation Committee (EIC) concluded that while international certification of morbidity coders is not currently feasible, the examination should be available to individuals to assess their own abilities and to provide guidance to educators. The exam should continuously be promoted and efforts be made to enrich it by soliciting additional questions for future exams. This will require the collaboration of many countries in collecting the exam questions and in conducting the pilot test. The paper would include a report on the results of activities undertaken during 2012 and early 2013. CS4.4.2 Assessing the Accuracy of Coding in the Japanese Case-mix System (DPC: Diagnosis Procedure Combination) and the Role of HIM for Improvement Makoto Anan National Kyushu Medical Center, Fukuoka-Shi, Japan Introduction and Objectives: The Japanese case-mix system, known as the DPC/PDPS (Diagnosis Procedures Combination / Per Diem Payment System) was introduced for acute care hospitals in 2003. In 2012, there are 7,587 hospitals in Japan. The number of DPC hospital was 82 in 2003, 1,505 (479,539 beds) in 2012, which now provides 53.1% of acute care beds. The DPC grouping logic is based on the ICD10 (J ver. 2003), the Japanese procedure code (K-code) and the choice of a complication, adjuvant, severity and other variables. And DPC has 18 Major Diagnostic Categories (MDC).Therefore accuracy of ICD coding is an extremely important element. DPC Hospitals have to submit their clinical information and medical claim data to the Ministry of Health, Labor and Welfare (MHLW). Since DPC was introduced, some problems have occurred. One of the problems is that ICD has not adopted medical claims under the national health insurance system. Firstly, we did not have an effective solution for the abundance of unspecified codes (dot 9 codes) and there was a lack of accurate coding. In 2010, DPC hospitals needed to establish a committee with HIM for coding accuracy and when their unspecified codes exceeded 40% (20% in 2012), there was a penalty. This study aimed to assess the accuracy of coding data and consider the role of HIM. Methods: In 2010, 952 hospitals voluntarily attended and participated in this study. They submitted 3,181,847 records of patient data from June to December. Their data, the ICD codes for their principal diagnosis were analyzed the proportion of the dot9 and dot8 codes in all 18 MDCs. Results: There were 463,751 dot9 codes (14.7%) and 196,712 dot8 codes (6.2%), dot8 codes were used in MDC5,18*,01 (19.6%-14.3%). An average proportion of dot9 codes decreased 28.1% (2006) to 14.7% (2010). Some MDC dot 9 codes decreased notably, 04: 45.6% (2006)>>14.2% (2010), 09: 47.2% (2006)>>15.3% (2010). Conclusion: The duty of establishing a committee with an HIM and a setup of the coding standard of dot9 codes (40%>>20%) had an achieving effect. There are some cases of the average of dot codes increasing related to a decrease of the average of dot9 codes. ICD coding of some hospitals may be arbitrary. Knowledge about ICD coding is spreading and coding skill is improving. The role of a HIM has become more important. CS4.4.3 Improvements in the Coding of Strokes in Canada's Discharge Abstract Database Josie Bellemare ; Jin Wang ; Maureen Kelly Canadian Institute for Health Information, Ottawa, ON, Canada Introduction: In 2009, analysts using data from the Discharge Abstract Database (DAD) housed at the Canadian Institute for Health Information (CIHI) identified that a relatively high proportion of strokes were coded as unspecified. As a result, CIHI focused the 2008-2009 DAD reabstraction study on the coding of strokes. In the study, 35% of cases in which unspecified stroke was reported to the DAD, the reabstractor was able to capture a more specific stroke code, predominately ischemic stroke. Following the study, CIHI developed an eLearning course for hospital coders focused on the coding of strokes, which was released in April 2011. In 2012, CIHI conducted an analysis of the DAD data to investigate what, if any, changes had occurred in the coding of strokes in the DAD following the reabstraction study and introduction of the eLearning course.

84
Methods: Four years’ of DAD data was analyzed to investigate trends in the coding of strokes: from 2008-2009 (the year of data examined in the stroke reabstraction study) to 2011-2012, the year after the introduction of the eLearning course. Variations in coding were analyzed by hospital characteristics including: participation in the stroke reabstraction study; availability of imaging technology to assist with the more accurate coding of strokes; and whether staff had completed CIHI’s eLearning course. In order to do this analysis, the DAD data was supplemented with other CIHI information to identify hospitals with appropriate imaging technology (Medical Imaging Technology Survey) and that had completed the education course (CIHI’s Learning Management System). Results: Among DAD abstracts with a significant diagnosis of stroke, the coding of unspecified stroke (I64) halved from 29% in 2008-2009 to 15% in 2011-2012. There was also a corresponding increase in the proportion of abstracts coded as ischemic stroke (from 46% to 60%). The data also showed variations in coding by the hospital characteristics: the proportion of stroke abstracts coded as unspecified was lowest (6%) among hospitals that had participated in the reabstraction study, had imaging technology and had participated in the education and highest (47%) among hospitals that did not have imaging technology nor had participated in the study or education. Conclusion: The results showed both the completion of reabstraction study itself and the introduction of the eLearning education course had a positive impact on the quality of the coding of strokes within the DAD. However, there is still hospital variation in the proportion of stroke abstracts coded as unspecified (after taking into account the availability of imaging technology) suggesting there is still room for improvement. CIHI will continue to monitor the data and provide feedback to hospitals and ministries of health on the quality of stroke. CS4.5.1 Ensuring the Quality of Health Information: The Canadian Experience Maureen Kelly ; Heather Richards Canadian Institute for Health Information, Ottawa, ON, Canada Introduction: High quality health information is critical for quality health care and for effective and efficient management of the health care system. The Canadian Institute for Health Information (CIHI) has over 30 data holdings that provide crucial information to stakeholders, including health system managers, policy makers and clinicians. CIHI has five dimensions of data quality: accuracy, timeliness, comparability, usability and relevance. This presentation provides an overview of the strategies and programs that support these dimensions of quality health information; and describes examples that illustrate data quality strategies in action-prevention, monitoring, feedback and continuous improvement. Methods: CIHI data holdings include information on individuals receiving health care services as well as the organizations and individuals providing the services. Data are captured and submitted in a variety of ways, by many different data providers depending on the sector and type of information. CIHI supports a broad range of prevention strategies to avoid the collection and submission of poor quality data, including data and technical standards, system edits and audits and training and support. Monitoring and feedback strategies provide information to others in the data quality chain to help influence and document the quality of the data. These include: operational reporting and feedback; data quality assessments; reabstraction and other validation studies; analysis and data mining; transparency and reporting. CIHI developed the CIHI Data Quality Framework, an objective approach to assessing data quality and producing standard documentation to support these activities. These prevention, monitoring and feedback strategies are the foundation for continuous improvement activities which link into the annual business cycle for each data holding, planning for standards and training and CIHI's regular consultations with stakeholders on quality issues. Results: Examples of these different strategies in action include: measuring the quality of clinical data from hospital emergency departments through a special reabstraction study; identifying and resolving acute care coding issues with eLearning; the development and reporting of compliance assessment tool to assess the quality of hospital financial and statistical data; and a multi-faceted approach to preventing data quality issues in hospital, continuing care and residential care. Conclusion: CIHI has a strong data quality culture. The diversity of CIHI's data requires not only an overarching data quality program, but also customized strategies to address the unique challenges of each data holding. CIHI collaborates with the many organizations along the data supply chain and fosters a sense of stewardship for its quality. CIHI's data quality program will continue to evolve as new data sources, such as electronic health records emerge, and to meet the changing information needs of its stakeholders. CS4.5.2 Are Electronic Patient Records Associated with Better Data Quality than Paper-based Records? Ashif Kachra 1; Marian J Vermeulen 1; Xuesong Wang 2; Chelsea Hellings 2; Michael J Schull 1
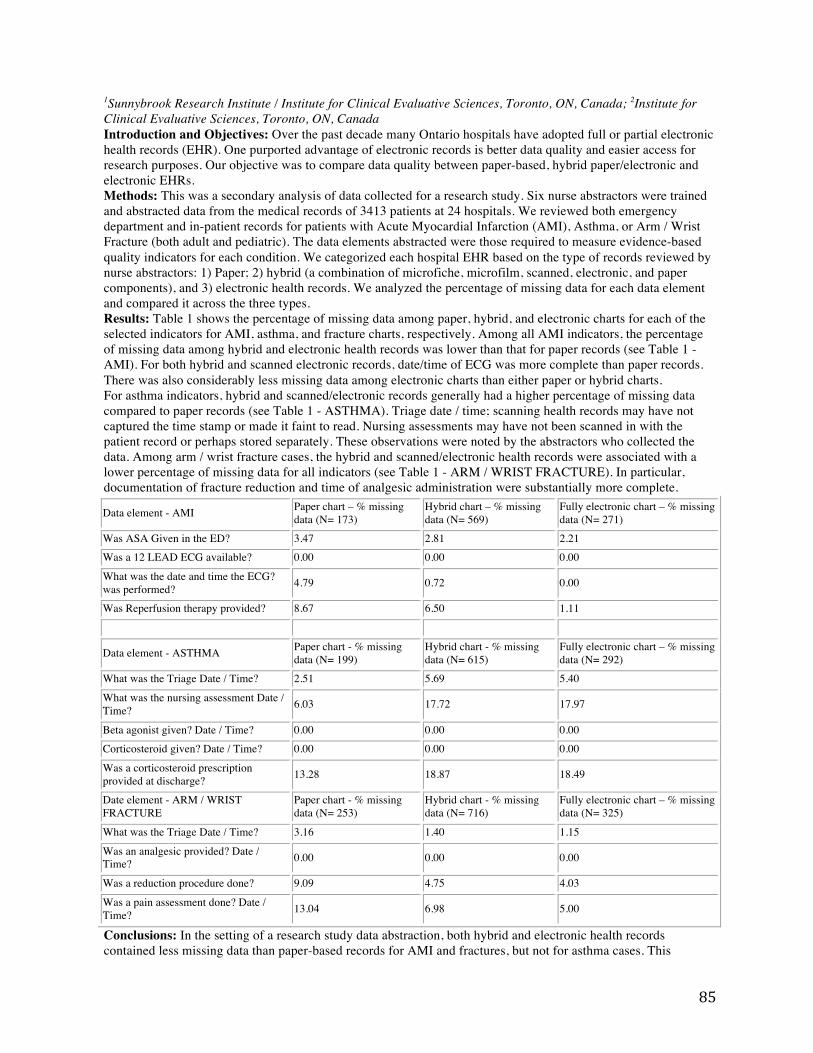
85
1Sunnybrook Research Institute / Institute for Clinical Evaluative Sciences, Toronto, ON, Canada; 2Institute for Clinical Evaluative Sciences, Toronto, ON, Canada Introduction and Objectives: Over the past decade many Ontario hospitals have adopted full or partial electronic health records (EHR). One purported advantage of electronic records is better data quality and easier access for research purposes. Our objective was to compare data quality between paper-based, hybrid paper/electronic and electronic EHRs. Methods: This was a secondary analysis of data collected for a research study. Six nurse abstractors were trained and abstracted data from the medical records of 3413 patients at 24 hospitals. We reviewed both emergency department and in-patient records for patients with Acute Myocardial Infarction (AMI), Asthma, or Arm / Wrist Fracture (both adult and pediatric). The data elements abstracted were those required to measure evidence-based quality indicators for each condition. We categorized each hospital EHR based on the type of records reviewed by nurse abstractors: 1) Paper; 2) hybrid (a combination of microfiche, microfilm, scanned, electronic, and paper components), and 3) electronic health records. We analyzed the percentage of missing data for each data element and compared it across the three types. Results: Table 1 shows the percentage of missing data among paper, hybrid, and electronic charts for each of the selected indicators for AMI, asthma, and fracture charts, respectively. Among all AMI indicators, the percentage of missing data among hybrid and electronic health records was lower than that for paper records (see Table 1 - AMI). For both hybrid and scanned electronic records, date/time of ECG was more complete than paper records. There was also considerably less missing data among electronic charts than either paper or hybrid charts. For asthma indicators, hybrid and scanned/electronic records generally had a higher percentage of missing data compared to paper records (see Table 1 - ASTHMA). Triage date / time; scanning health records may have not captured the time stamp or made it faint to read. Nursing assessments may have not been scanned in with the patient record or perhaps stored separately. These observations were noted by the abstractors who collected the data. Among arm / wrist fracture cases, the hybrid and scanned/electronic health records were associated with a lower percentage of missing data for all indicators (see Table 1 - ARM / WRIST FRACTURE). In particular, documentation of fracture reduction and time of analgesic administration were substantially more complete.
Data element - AMI Paper chart – % missing data (N= 173)
Hybrid chart – % missing data (N= 569)
Fully electronic chart – % missing data (N= 271)
Was ASA Given in the ED? 3.47 2.81 2.21 Was a 12 LEAD ECG available? 0.00 0.00 0.00
What was the date and time the ECG? was performed? 4.79 0.72 0.00
Was Reperfusion therapy provided? 8.67 6.50 1.11
Data element - ASTHMA Paper chart - % missing data (N= 199)
Hybrid chart - % missing data (N= 615)
Fully electronic chart – % missing data (N= 292)
What was the Triage Date / Time? 2.51 5.69 5.40
What was the nursing assessment Date / Time? 6.03 17.72 17.97
Beta agonist given? Date / Time? 0.00 0.00 0.00 Corticosteroid given? Date / Time? 0.00 0.00 0.00
Was a corticosteroid prescription provided at discharge? 13.28 18.87 18.49
Date element - ARM / WRIST FRACTURE
Paper chart - % missing data (N= 253)
Hybrid chart - % missing data (N= 716)
Fully electronic chart – % missing data (N= 325)
What was the Triage Date / Time? 3.16 1.40 1.15
Was an analgesic provided? Date / Time? 0.00 0.00 0.00
Was a reduction procedure done? 9.09 4.75 4.03
Was a pain assessment done? Date / Time? 13.04 6.98 5.00
Conclusions: In the setting of a research study data abstraction, both hybrid and electronic health records contained less missing data than paper-based records for AMI and fractures, but not for asthma cases. This

86
suggests that electronic data capture is advantageous for data quality in some, but not all, cases. This suggests that simply moving to electronic health records does not always guarantee greater data quality. CS4.5.3 Building a Database for Estimated Patient Medication History from Prescription Data in CPOE Kei Teramoto 1; Shigeki Kuwata 2; Takeda Toshihiro 3; Taizo Murata 3; Shiro Manabe 3; Naoki Mihara 3; Kondo Hiroshi 4; Yasushi Matsumura 3 1Osaka University Hospital, Suita, Japan; 2Department of Medical Informatics, National Cerebral and Cardiovascular Center, Osaka, Japan, Suita, Osaka, Japan; 3Department of Medical Informatics, Osaka University Hospital, Suita, Osaka, Japan; 4Department of Medical Informatics, Tottori University Hospital, Yonago, Tottori, Japan Introduction and Objectives: Prescription order data in CPOE are expected to be used for pharmacoepidemiology (PE). Fundamental information in PE studies includes a period of time during which medicines are taken by target patients. An exact medication history of a patient, however, cannot be readily obtained from the order data which are separately stored in every prescription in the CPOE database. Besides, correction should be made with regard to duplication and lack of prescription orders, since a period of prescription is not identical to that of the prescribed medicines actually taken by a patient. Accordingly the authors developed a program which estimates a possible medication history from the order data to create a patient medication database available for PE at Osaka University Hospital (OUH). Methods: Processes of the developed program are as follows; (1) For the same medicine taken by the same patient, a prescription period is combined with the subsequent period if the last day in the former comes later than the first day in the latter (duplicate periods). (2) Even if the periods are not duplicated, they are combined if quantity of the residual medicines at the end of the former, calculated from the difference between total prescribed quantity and possible consumption of the medicines, is not less than that of estimated consumption during a gap between the periods. (3) The possible consumption is adjusted by a factor depending on the probability that a patient misses a dose ordered by a doctor. The factor is defined as a reciprocal of the probability; the possible consumption is calculated by the prescribed quantity divided by the factor. Prescription order data (166,585 records for 405 patients) were extracted from the CPOE database at OUH and were processed with the program. Results and Conclusion: The original order records were combined to 36,641 records (-78%) on the assumption of no missing doses. With the factors of 1.0, 1.2 and 1.3 for once, twice and more than three times a day as dosing schedules of the prescription, respectively, the records were reduced to 31,786 (-81%). The processes of the program contributed to creating a plausible medication history database. The database would facilitate the investigation on the adverse events that occur in association with specific medicines. CS4.6.1 Communicating the Pan-Canadian Nursing Perspective and Contribution to an Evolving Electronic Health Record Cindy Hollister Canada Health Infoway, Toronto, ON, Canada Introduction and Objectives: Use of a fully evolved electronic health record (EHR) will enable collaborative, patient-centred care by allowing for timely access and secure sharing of patient information across disciplines and care settings and will promote optimal client/patient/resident outcomes supported by advanced analytics and clinical decision support. The objectives of this presentation are to provide an opportunity for the audience to gain insight into what nurses identified to facilitate their profession's clinical adoption and optimized use of an EHR, understand the process used to develop the nursing reference document of EHR business and functional elements to support clinical practice and to contrast the nursing perspective with their own professions' requirements for EHR adoption and optimized use. Method: Canada Health Infoway (Infoway) has created opportunities to include nurses in shaping the EHR. In 2009, the Nursing Reference Group (NRG) was established to provide national nursing leadership, engagement, expertise and input to inform nursing strategies and plans to accelerate nurses' adoption and benefits realization of the EHR. One of six key strategic goals developed was: "Identification of nursing key business and functional requirements for the electronic health record". Over the next 18 months, a Nursing EHR working group produced a draft reference document which was endorsed by the NRG and validated by a nursing focus group. Results: As an outcome of this strategy, the "Pan-Canadian Nursing EHR Business and Functional Elements Supporting Clinical Practice", was published as a reference document on Infoway's website in June 2012. The Reference Document describes considerations for pan-Canadian nursing EHR business and functional elements, along with the guiding principles and assumptions identified and used by stakeholders during the development

87
process. Thirty EHR business elements and over 100 functional elements were identified and grouped broadly under: Patient/client/resident; Nursing Practice and Health Information. Conclusion: Although approached from a nursing perspective, many of the EHR business and functional elements could be applicable to other health care professions. This presentation will increase the audience's understanding of how the EHR could support their own practices and demonstrate the similarities and/or gaps in EHR business and functional elements required by other professions. It is essential that all healthcare professions recognize the value to be gained from an EHR and be able to contribute and communicate business and functional needs for their professions to help ensure an EHR evolution which enables professionals across the care continuum to work together toward informing and providing safe, coordinated and quality patient care. CS4.6.2 The Doctor's Directory - An Innovative Health Systems Information Tool for Junior Doctors Jonathan Clarke 1; James Houston 2; Jim Buckley 2 1Department of Health, Informatics Directorate, London, United Kingdom; 2North West London Hospitals NHS Trust, Harrow, London, United Kingdom Introduction and Objectives: In the United Kingdom, junior doctors frequently rotate through work in different hospitals and specialties. During this time, their clinical skills and knowledge continue, increase, however the transition from one rotation to the next is associated with new health systems, referral pathways and contact details. Inadequate induction programmes and limited access to hospital specific information are thought to reduce the efficiency of junior doctor work, and therefore have the potential to adversely affect patient safety. This study aims to assess impact of the introduction of an intranet 'wiki' providing hospital and specialty specific information to junior doctors. Methods: An intranet 'wiki' website - The Doctor's Directory (DD) - was developed by junior doctors at a busy, urban, acute hospital. The site was accessible from all terminals and contained induction details for all specialties, referral pathways, contact telephone and pager numbers, information on ordering specific tests and investigations and 'out-of-hours' service provisions. The site was advertised to all junior doctors on their arrival at the hospital. A survey was distributed to all junior doctors on their fifth day of clinical practice to assess their knowledge of specific aspects of their role and to identify which sources of information they access to answer specific questions relating to requesting investigations, contact details and referral pathways. The survey was repeated one month later following the introduction of the Doctor's Directory. Results: 33 junior doctors were surveyed on their fifth day of clinical practice, and 21 were surveyed one month later. At induction, junior doctors felt unprepared to make referrals (12.5% felt prepared), request tests (30.3% felt prepared), or access contact details (6.8% felt prepared). The mean perceived time spent finding the information to complete a task at month 0 was 109.62 minutes per day (SD = 103.1), and 51.9 minutes per day (SD = 43.4) at month 1. Paired t-test: P=0.023. After one month, 81% of junior doctors had used the Doctor's Directory. 94% of those using it had found it a useful source of information, 100% felt it had saved them time at work. The estimated time saved as a result of the DD was 39.4 minutes per day, 95% CI = 27.0 to 51.7 minutes per day. 88.2% used the DD to find out how to request tests, 82.4% used the DD to find pager or telephone numbers, 82.4% used the DD to find referral pathways. Conclusions: Junior doctors feel unprepared for clinical practice due to hospital and specialty specific factors, rather than deficiencies in clinical knowledge. The Doctor's Directory is an effective, well-received and adaptable system to facilitate access to such information that has been shown to save significant time for junior doctors each day. This intervention has the potential to improve the working patterns of junior doctors and consequently improve patient care. CS4.6.3 Physician Documentation Improvement Project at Vancouver Coastal Health Authority Gerald Yu Providence Health Care - Lower Mainland Health Information Management, Vancouver, BC, Canada Introduction: In order to improve continuity of care and physician documentation for coding and reporting, Vancouver Coastal Health and Health Information Management embarked on a journey of bringing back proven old school practices with modern day tools. The results a year later translated into 100% dictated standardized discharge summary for continuity of care and more comprehensive documentation for coding and reporting. Methods: By working closely with Medical Affairs, with the support of the Executive, a standardized discharge summary template was implemented. To improve compliance, an online education course for documentation was developed along with an electronic reference card for quick reference. Suspension policy for non-compliance was

88
brought back and enforced. To support physicians, a physician documentation educator (a HIM professional) was hired. As for change management, data were collected and reported periodically for timeliness of dictation as well as the quality of the content of the discharge summary along with chart reviews by physicians and the educator. Results: The dictation rate of discharge summary went from 38% to 100%. For the first time, family physicians were receiving timely discharge summaries for continuity of care. The quality of the content of the discharge summary was greatly improved for coding and reporting. The relationships between physicians and HIM professionals were enhanced by the project enabling sharing of knowledge. Conclusions: The improvement project updated proven practices from the past with modern day communication tools enabling continuity of care, richer data for decision making and greater physician engagement with HIM professionals. CS5.1.1 The Quality of Surgery-Specific Information on Post-operative Discharge Letters - A Retrospecitve Analysis and Investigation of Stakeholder Data Requirements Jonathan Clarke ; Charles Gutteridge Department of Health, Informatics Directorate, London, United Kingdom Introduction and Objectives: As surgery becomes more specialized, and procedures become more technical, the difference between the procedure specific knowledge of the surgeons and the community physician has widened. For a patient to be safely discharged from hospital after an operation, it is essential that there is safe and comprehensive transfer of information to community physicians for their ongoing care at home. Currently there are no guidelines in the United Kingdom to indicate the surgery specific information required on a post-operative discharge summary. This study aimed to identify the current quality of surgical discharge information and evaluate the expectations and perceptions of general practitioners (GPs) (those generally reading such letters) and junior doctors (those generally writing such letters) with regard to post-operative discharge letters. Methods: All post-operative discharge summaries for a one-month period at a busy, urban, acute surgical hospital were analyzed for the documentation of surgery specific information. GPs were surveyed to assess their perceptions of the quality of surgery specific information on discharge letters. Hospital-based junior doctors were surveyed to assess their confidence in providing the same surgery specific information. Both groups were asked to indicate which surgery specific information should be included on the post-operative discharge letter. Results: 190 post-operative discharge letters for general surgery and vascular surgery patients were analysed. 91 letters (48%) were written by junior doctors, 99 letters (52%) were written by surgical trainees or consultant surgeons. 79 (80%) of letters completed by surgeons were written using a day-surgery specific proforma with surgery specific fields, 20% were written using a non-specific electronic discharge system used by junior doctors. The date of the operation was explicitly stated in 6.3% of cases, the side of the operation was stated in 80% of cases. Information on wound care, patient instructions and GP instructions was provided in 57.4%, 58.4% and 21.6% of cases respectively. Follow-up requirements were documented in 91% of cases. The documentation of the operation date, wound care, patient instruction and GP instructions was significantly improved (P = 0.0001) with the use of the day-case proforma, for both junior doctors and senior surgeons. 65 junior doctors and 39 GPs were surveyed. Information on operation date, operation performed, wound care requirements, patient and GP instructions and follow-up requirements were required by >85% of respondents. Conclusions: Surgical discharge letters currently provide inadequate data for the needs of GPs. The use of a surgery specific proforma may improve information transfer. GPs require specific post-operative information that could be provided by such a system. This study identifies a minimum dataset required for post-operative discharge letters. CS5.1.2 Alternatives for Secure Telemedicine and for Video Conferences Including PHI. Aaron Hendriks University Health Network -Shared Information Management Services, Toronto, ON, Canada Introduction and Objectives: There exists a considerable gap in terms of access to care in Canada. Recently Telemedicine has been used to address this gap by providing access to specialists around the country to those in remote regions. Delivery of this care in a secure, efficient and cost effective manner has been a very large challenge. Often there are provincial programs running but there can be times that alternatives are required. Due to many requests for alternative video conference solutions the UHN security office has evaluated several alternatives to the regional systems. These requests came from doctors who were traveling out of the service range, had patients out of the service range or wanted the systems for rounds/medical discussions between doctors.

89
Our purpose was to evaluate the most popular alternatives to be able to approve the use of these systems for PHI inclusive meetings. Methods: Starting in summer 2012 the UHN information Security Officer compiled a list of the most popular alternatives of video conferencing tools and/or applications. The popularity of the systems was based on the number of requests for use to the Information security office since summer 2011. The alternatives were: CISCO/Tandberg MOVI, Polycom M100 and Polycom iOS app, Gotomeeting with video and Webex with video. The evaluation was based on total requirements/infrastructure for the system, ease of installation/configuration, ease of use, ability to include people outside of your internal network, total cost per use, total cost over 3 years and complete system security. Results: The UHN ISO evaluated all systems on security first to ensure the primary concern of the office was met. After this was completed we evaluated the rest of the criteria. The summary of the findings are below: • The Cisco system was complex to set up as it requires a large supporting infrastructure. Due to this and the costs associated we rated this last. • The Polycom m100 software had the lowest cost and met all requirements other than connection to a party outside of the internal network. To address this shortcoming a bridging service or large infrastructure was required. • The Polycom iOS app failed as it does not provide security of the transmission so no PHI could be used on this system. • Gotomeeting met all requirements when properly set up by the meeting host. This meant that the host had to ensure the meeting had a secure login and that no one was able to record the meetings. • Webex again met all requirements when properly set up by the meeting host. The additional features found with this system are the ability to set up a corporate account that will mandate all proper security for the users and ensure the meetings meet all requirements. Conclusions: Each system, other than the Polycom iOS app, met all requirements. The question of what is right for your needs is more determined on how much you have to spend and how large of an IT staff you have to run the system. CS5.1.3 "The Re-ACT© Connection" Sue Kelly We Care Home Health Services, Toronto, ON, Canada Introduction and Objectives: Re-ACT© is an eHealth solution that allows people with one or more chronic diseases to remain at home. It provides the knowledge and inspiration they need for healthy living and disease self-management. It also engages them in decision-making, goal setting and care planning by connecting them with education, health information and helpful support. Under Re-ACT©, one Registered Nurse connects with up to 100 clients who regularly monitor their own blood pressure, pulse, weight, blood glucose and blood oxygen from their homes. Re-ACT© uses wireless technology to transmit those data to a remote monitoring centre where results are tracked and interventions are facilitated by a nurse. Our objective is to share the results of the Re-Act program on quality of life indicators. Methods: We Care conducted a study to investigate the quality of life of clients once discharged from the program through detailed client surveys. Results: Indicated that 32% of discharged clients did not experience any adverse events subsequent to discharge after completion of care plan. These cases were patients that were generally classified as "C" in the CDPM level where Re-Act has the most significant impact. Additionally, events were significantly reduced in remaining "complex" clients while on the program. This monitoring has been shown to reduce ER visits by 34 per cent and hospital admissions by 16 per cent. Improved safety has reduced falls by 43per cent. Other benefits included reduced complications and improved medication adherence. Conclusion: Re-ACT© is an innovative partnership involving the Aging at Home initiative with the Ministry of Health and Long-Term Care (MOHLTC), the North Simcoe Muskoka Community Care Access Centre (CCAC), We Care Home Health Services and Healthanywhere, Inc. In addition to helping seniors maintain their independence at home, it also provides valuable peace of mind for their families. CS5.2.1 Does Concurrent Coding Improve Physician Documentation and Ultimately the Quality of Health Information? - Concurrent Coding Pilots within Alberta Health Services

90
Shirley Learmonth ; Donna Sired ; Karen Armitage ; David Zygun ; Reza Shahpori Alberta Health Services, Calgary, AB, Canada Introduction and Objectives: Concurrent coding improves clinical documentation, increases identification of co-morbid conditions, and by combining clinical knowledge with the expertise of the coder provides opportunities to improve quality of health information. Alberta Health Services initiated three separate concurrent coding trial projects: 1) In ICU, at Foothills Medical Centre in Calgary, to determine the feasibility of integration of trained Health Information Management (HIM) specialists with the health care team to concurrently code diagnoses and interventions. The objectives of the project were to understand the resources requirements, establish a coding and feedback process, determine coding accuracy and investigate the usefulness of concurrent coding diagnoses. 2) On various medical units across three facilities in Calgary with the aim to improve Length of Stay (LOS) by helping the team work towards a LOS goal and to improve documentation and data accuracy thus resulting in a more reliable Estimated LOS (ELOS). 3) In Edmonton, two facilities participated with concurrent coding in the General Internal Medicine, Family Medicine, Neurology, and Geriatric units. The focus of the project was to improve physician awareness of length of stay and improve documentation to better reflect the patient experience. Methods: Although all projects relied on the HIM coding specialists attending the unit to code the chart while the patient was in hospital, the process varied from the HIM specialists being embedded within the Nursing Unit as part of the care team to the coding specialist going to the unit to code charts and then return to the HIM department. The method of evaluation varied between the three pilots including a random allocation into blind and non-blind groups, as well as a retrospective comparison and the use of qualitative and quantitative evaluation methods. Results: In ICU, during the 6 month trail phase, 1061 cases were concurrently coded. 508 cases were assigned to the blind group and 553 cases to the non-blind group. A mean of 10.71 ICD10 codes and 12.55 ICD 10 codes in the non-blind group. Prior to initiation of the trial a sample of 993 retrospective patients revealed post discharge coding captured 10.86 diagnoses per case. Conclusion: In ICU it was determined that concurrent coding, although requiring extra resources, captured 2 more ICD10 diagnoses and one main reason for ICU admission diagnoses per case. In all pilots, the coding specialists reported that the interaction between the physician and the coding specialists improved the documentation and thus the specificity of the coding. CS5.2.2 Balancing Coding Quality, Throughput and Outcomes at a Teaching Hospital Katherine Henning ; Wei Xiong ; Joanna Li UHN, Toronto, ON, Canada Introduction and Objectives: In Canada, there is no current standard for coding productivity as to how many charts should be coded per day per coder. [1] Although, there are many informal benchmarking comparisons done with peer organizations. In an international study comparing coding productivity, it was reported that the requirement was 30 minutes per inpatient record on average in the US. [2] University Health Network (UHN) is a tertiary, quaternary teaching hospital in downtown Toronto with major programs in Neurosurgery, Oncology, Transplant and Cardiac care. In addition to the complex patient population, the information technology infrastructure is multifaceted and involves a best of breed philosophy and a hybrid environment with electronic and scanned medical records. As such, the Coding and Abstracting process is complex and we found that the existing productivity standards quoted were not always helpful for our specific situation. Consequently, we undertook a study to explore and propose an optimal time for coding inpatient charts at UHN, that would balance throughput, coding quality and outcomes. Methods: Inpatient charts were categorized by length of stay (LOS: 1-3 days, 4-10 days, 11-30 days and >=31 days), medical versus surgical, and typical versus atypical, to adjust for patient chart complexity. Six experienced coders were assigned to this study. On an entry log form, each coder recorded diagnosis codes and procedure codes that they extracted every 10 minutes. After coding was completed, an independent, experienced coder entered into the coding system the abstracted diagnosis codes and procedure coders to calculate Resource Intensity Weight (RIW) value obtained at each time interval. This study hypothesizes that at an optimal coding time point, the amount of extracted chart information reaches a peak, and then the rest of coding time produces information of little benefit (i.e., law of dimishing returns). RIW value is a good indicator as to how much information is extracted from a chart and thus selected as the main outcome measure. The number of diagnosis codes and procedure codes are additional outcome indicators that estimate to what extent the information is extracted. Scatter plots of outcome measures (average RIW, number of diagnosis and procedure codes) over coding time were used

91
to determine the hypothesized optimal coding time. Results: In total, there were 276 inpatient charts, including 216 typical and 60 atypical charts, 151 medical and 125 surgical charts. The maximum time coders spent coding charts and proposed optimal coding time is summarized below. Coding Time (minutes)
Charts: 1-3 days
Charts: 4-10 days
Medical Charts: 4-10 days
Charts: 11-30 days
Atypical Charts: 11-30 days
Charts: >+ 31 days
Maximum 40 60 40 120 80 110
Optimal 20-30 30-40 20-30 50-60 30-40 50-60
Conclusions: This study determined maximum and optimal coding time for inpatient charts at UHN based on LOS and patient type and can be used as a managment tool for setting productivity goals with staff. The proposed optimal coding time has potential benefits for coding productivity and efficiency at UHN. CS5.2.3 The Role of the HIM Professional and Technology in Ensuring Data Integrity Kathy Hartman, RN 1; Michelle Dougherty, RHIA, CHP 2; William Rudman, PhD 2; Ann Chenoweth 3; Sandra Seabold 1 1Cleveland Clinic Health Systems, Cleveland, OH, United States; 2American Health Information Management Association, Chicago, IL, United States; 33M Health Information Systems, Salt Lake City, UT, United States Introduction and Objectives:This two-phase study examines how the interface between technology and the Health Information Management (HIM) professional may positively impact data integrity issues related to data quality and timeliness. Phase 1 examined how the integration of computer-assisted coding (CAC) technology impacts coding practices related to ICD-9. Phase 2 will examine how the transition from ICD-9 to ICD-10 will impact the accuracy and timeliness of data throughout the transition period. The goal is to develop a more concise understanding of the use of technology in addressing issues of healthcare reform and the human interface with technology in the health information management field. Authors will report results of Phase 1 of the study. Methods: To ensure rigor in the research project, a Solomon 4 quasi-experimental design was employed. Study questions were defined as: • Is there a measurable difference between traditional coding and the use of CAC in terms of coding accuracy, timeliness and data integrity? • Will the use of credentialed coders in conjunction with the use of CAC result in improved accuracy, timeliness and data integrity? Coding professionals were randomized into six groups. Each group included six coders randomly selected from coders will a similar set of skill and experiences. To control for time and complexity of the record, all coders and the CAC technology coded the same 25 records. In addition, all coding was performed in the same location and all coders received the same training on the CAC technology. Results: The groups of coders were first evaluated for speed of coding. The average time for groups manually coding a chart was 77 minutes, and those using CAC was 65 minutes. In summary, the coder using technology achieved a 17 percent increase in efficiency. Quality of coding was assessed by evaluating the Principal Diagnosis/Procedure selected by the coder in comparison with the coding gold standard. In coding the Principal Diagnosis, the manual group achieved 67 percent accuracy and the group with CAC achieved 69 percent accuracy for a 2 percent increase in accuracy with CAC technology. Coding of Principal Procedure using CAC achieved 83 percent accuracy, a 10 percent increase in accuracy over the 73 percent achieved by the manual group. The overall result was a 6 percent increase in accuracy. Conclusion: Study findings confirm that CAC technology can achieve an increase in efficiency over manual coding. Smaller gains were achieved in coding accuracy, but findings indicate there was no reduction in coding accuracy or increased error rates. The introduction of institution-specific coding rules to the CAC technology has the potential to increase accuracy rates and will be evaluated in Phase 2. Finally, CAC technology can be effective in identifying specific variables across coders, promoting greater consistency of coding among diverse coders and a range of skill levels. CS5.3.1 Implementing a Regional, Off the Shelf, Surgical eBooking & Wait Times System - an eHealth Success Story Karol Eskedjian 1; Leslie Motz 1; John Sinclair 2 1Lakeridge Health Corporation, Oshawa, ON, Canada; 2Novari Health, Kingston, ON, Canada

92
Introduction and Objectives: The SUBMIT Project to improve surgical patient Wait Times was developed between the Central East LHIN and the 7 hospitals to implement a regional system that supports e-booking and wait list management for Surgeons, provides information electronically to the hospital (registration, OR booking office, Pre-Op and WTIS office) and automates the provincial WTIS reporting. The objectives were to: eliminate paper processes and duplication of data entry, improve data quality, shorten patient's procedure booking time, develop data collection and pre-operative standards, and provide real time regional reporting. The surprising added-value of the solution was to transform the workforce both at the surgeon's office and hospitals. Methods: The team leveraged an off the shelf solution, Novari Access to Care, and developed a planning process for each hospital /surgeon office that determined core system standards while allowing each organization's customizations. Hospital teams reviewed and evaluated data and processes of the "current state". Through user testing and training the way the users viewed and utilized the data changed. They were encouraged to provide feedback and implement changes in their own processes. Regional committees / groups were put in place as to identify and suggest improvements and support information sharing. Results: The resulting system, the largest Canadian regional implementation, now allows 380+ surgeons offices to electronically manage their patient wait list(s) at multiple organizations. It provides the ability for patients to leave their surgical consult appointment with an OR booking date, the Pre-Op appointments and preparatory information. Reduction in phone calls /faxes for hospital registration, OR booking changes, patient status and communication between providers is now real time significantly reducing effort required by staff. Hospital registration is now an automated request from the surgeon's office; the pre-op information is pre-gathered at the surgical consult, and the e-booking is sent directly into the OR system through an HL7 interface. Previous piles of paper passed between offices and on the OR booking desk has been eliminated, and now contact is made and tracked between staff through a secure messaging system in real time. Conclusions: The two key conclusions are that 1) workforce/ front line direct involvement early and through the entire process of e-Health implementation will provide a better and sustained result and 2) the transformation in the work and the workforce is usually what is expected, and if diligent with #1, it will be more successful than anticipated. CS5.3.2 A Three Year Status Report on the Montreal Regional Deployment of the Electronic Health Record Christine J Bolduc Hôpital Louis-H. Lafontaine - Institut universitaire en santé mentale, Montréal, QC, Canada Introduction: At the 2010 IFHIMA Congress in Milan we presented the ambitious project of deploying a standardized electronic health record (EHR) to over 90 health and social service establishments on the island of Montreal. Where are we at today? How many establishments have deployed the electronic health record? What challenges were met and how were they addressed? How did the clinical staff receive the EHR? What was the impact on the HIM department? Conclusions: The presentation will seek to answer these questions as well as share the lessons learned, the strategies developed to meet the challenges, and the future plans as we enter phases two and three of the project. CS5.3.3 Today's Case Costing Environment: Emerging Roles and Opportunities for the Health Information Management (HIM) Professional - Workforce Transformation Rosemarie Lourenco University Health Network, Toronto, ON, Canada Introduction and Objectives: A paradigm shift is occurring where the HIM professionals are no longer limited to shuffling paper based health records. They will experience a quantum leap in the near future and should position themselves to be ready to use case costing tools and provide expertise and analytics for case costing reports that identify efficiencies, deficiencies, continuous improvement recommendations, benchmarking, trend analysis and superior quality control. HIM professionals must learn where the HIM profession could be playing a part in the future of health care and what transformations will be required to stay ahead of the curve for example: more reliance on critical thinking to provide analysis, recommendations and business process improvements to system stakeholders. Methods: HIM professionals must understand the changing demands in the current health care field and adopt strategies to successfully adapt themselves to use the newly created data sets which will be relied on by more and more top health providers to support their decision making and research to provide effective and efficient funding decisions. HIM professionals will need to recognize the potential for upgrades, revisions or optimization of existing business methods and funding formulas using Case Costing Methodology and expand beyond their

93
traditional skill sets and knowledge bases to perform at a superior level in both clinical and financial areas. The profession must be educated on Case Costing methodology and recognize it as an enabler to streamline the collection of the data and improve the efficiencies within health care organizations. Results: A matrix of skills would be developed to address the knowledge gaps of both clinical and financial by any HIM professional to become a Case Costing practitioner. Conclusions: Continuing education and acquiring new skills to improve on the data collected to provide a better data that addresses the actual specific costs required to care for patients in the already funding constraints of the health care system. The following goals would be achieved: greater accountability, improved efficiency and effectiveness, increased use of scientific evidence in decision making and policy, enhancing capacity for stewardship of the healthcare system. CS5.4.1 Danish Health Sector With National Multidisciplinary Groups: Health Information Management of "Upper Gastrointestinal Cancer Group (UGCG)" Darley Petersen Odense University Hospital, Odense, Denmark Introduction and Objectives: In 2005, the Danish National Board of Health established collaboration between specific groups of cancer diseases, called Danish Multidisciplinary Groups (DMCGs), in order to strengthen clinical cancer research. The work within the individual groups is aimed to focus on all aspects of clinical research regarding prevention, treatment (surgical, medical, and oncological) and also rehabilitation within the area of the cancer diseases. Methods: The specific cancer diseases must include an acceptable amount of patients (incidence/prevalence) in order to provide background for organizing an individual DMCG. The purpose of a DMCG is to develop and collect knowledge and to transform the presence of new knowledge into results that may be used in clinical practice for the benefit of patients. The work within DMCG includes the possibility of internal and external evaluation and quality control. Since 2005, a vast number of Danish Multidisciplinary Groups has been established and they all collaborate within the regional competence centres (databases, biobanking, etc.). Results: The DMCG "Upper Gastrointestinal Cancer Group (UGCG)" includes Danish Esophageal, Cardiac, and Gastric Cancer Group (DECV), Danish Pancreatic Cancer Group (DPCG) and Danish Liver and Gallbladder Cancer Group (DLGCG), including intra/extra hepatic bile duct cancer and liver metastases. These groups were formalized in 2007 with a central coordinating administration at the Danish Pancreas Cancer Group's secretariat within Unit of Clinical Research, Department of Surgery at Odense University Hospital, Denmark. Information systems between the 5 national treatment centres within UGCG were accordingly established. One of the objectives for UGCG is to focus on the latest development within examination and treatment of upper gastrointestinal cancer, as well as an obligation to spread knowledge through annual seminars. The aims of these seminars are to develop and harmonize the expertise within the specialty and to focus on strengthening the professional competences of all personal groups involved. Conclusion: Each DMCG is based on appointed specialists from scientific societies, research environments and treatment institutions. Each DMCG is working within a well defined disease entity, i.e. "Upper Gastrointestinal Cancer Group (UGCG)". Each DMCG publishes periodically results of research activities, annual reports, and makes future plans for databases including updates of guidelines, cancer patients' pathways, and setting up clinical cancer research programmes. CS5.4.2 Making it happen! Clinician Peer Support Network Program To Advance Adoption of Electronic Health Record Systems in a Clinical Setting Anne Tran Fazzalari Canada Health Infoway, Toronto, ON, Canada Introduction: Clinician engagement is critical to the effective implementation and use of health information and communications technology (ICT) systems across the country. Clinical transformation using electronic health record (EHR) systems requires clinicians to be engaged along every step of the adoption journey. Canada Health Infoway’s Clinician Peer Support Network program objectives are: 1) To support clinicians in achieving value, in their practice and for their patients, through accelerating adoption and effective use of technology within the

94
practice setting; 2) To link experienced clinicians, with their peers for support, mentoring and sharing of knowledge, experiences, lessons learned and leading practices; and 3) To accelerate adoption by providing supports such as change management and quality improvement support; clinical practice redesign to make efficient and effective use of health ICTs. Methods: The Clinician Peer Support Network program enables the establishment of clinicians as Peer Leaders to provide leadership in supporting and coaching their colleagues to integrate technology into clinical practice. A collaborative approach is taken among project partners to advance a national strategy aimed at building sustainability and capacity to achieve adoption and benefits realization of EHR systems in clinical practice. Results: Infoway will discuss the national clinical engagement strategy, the Peer Network program and its strategic objectives, as well as details of local Peer Network implementations. Interdisciplinary perspectives will be shared around how the Peer Leaders addressed change management issues, challenges, opportunities, and lessons learned. Peer Leaders have a significant impact in providing leadership, in fact, surveys to date revealed that over 96% of surveyed Peer Leaders felt that “in my role as Peer Leader, I believe I have positively influenced my colleagues in their understanding and adoption of EMR/other technology systems in their practice settings.” Although respondents were drawn from health care spectrum, the majority of respondents’ from primary care (64%) and community care (17%). Lastly 89% of Peer Leaders felt that “Peer Network is beneficial to clinicians and/or clinic managers/staff.” Since analysis of the Peer Network program is on-going, updated results will be shared with conference participants. Conclusions: The implementation of electronic health record systems is likely the most complex and powerful transformation in clinical practice and delivery of health care services this century. It requires a team based approach of all stakeholders and at all levels. Critical to success is clinician leadership, engagement and most importantly the use and integration of these systems in practice to support decision making and improve patient/client outcomes. Considerations of how the Peer Network model could be applied in an alternate setting will also be discussed. CS5.4.3 Experiencing the Challenges of Integrating Behavioral Health and Primary Health Services Ruby Nicholson ; Patti Nenna The Kent Center for Human and Organizational Development, Warwick, RI, United States Introduction and Objective: Unique differences between behavioral health and physical health services design, information sharing and processing, coding and documentation present challenges to the implementation of an integrated system of care. The Center discovered that integrating their existing behavioral health programs with their primary care practice required reviewing workflows of the two practice settings, assignment of diagnostic codes, documentation requirements for two distinct systems, policies for laws governing the release of highly sensitive information, and participation in a Health Information Exchange were all essential to successful integration of services. This project enabled the organization to accomplish their organizational goal and assisted in other initiatives as a Medicaid Health Home coordinating services with other primary care providers. Methods: Starting in February 2012 a cross-functional team met to develop strategies to address each stage of implementation for integration. The primary focus was initially on the use of an electronic record in the behavioral health practice. Information workflows were developed identifying duplicity in the systems, where differences in documentation requirements existed, and how to ensure information from both practice settings could be integrated. Structured notes were developed in order to capture Meaningful Use Requirements. Policies, procedures and job descriptions were revised to reflect changes in workflow and integration of information. Sharing of encrypted information with external providers was established through a Direct secure email account. Agreements were established with other healthcare providers to ensure information could be legally shared, particularly substance abuse information governed under more stringent laws. Participation in a Health Information Exchange was necessary for viewing and exchanging data with data sharing partners. The integration team continued to meet to assess the process and identify successes and barriers. Results: Despite frustrations with software issues, unmet timelines, attempts to align documentation requirements and other issues that developed during the implementation process staff were able to implement an electronic record with integrated service plans, diagnoses, labs, medications and plans of care. There was a decrease in redundancy, and increase in data sharing, and more accurate, timely information available for all providers involved in the patient's care. Conclusion: Initial feedback from staff members participating in the process and persons receiving services indicate a more comprehensive, streamlined approach to health and wellness and improved outcomes. There is still a need to fine tune some of the processes, enchance the integrated practice approach, and prepare for Stage 2 Meaningful Use.

95
CS5.5.1 The Effectiveness and Refinements of Special Program for Passing Japanese Health Information Manager Certification Exam in Fujita Health University Haruka Murai ; Tetsuya Kamei ; Fumiaki Horiba ; Masatsugu Iwase ; Nobuko Kurono ; Yukinori Murata ; Koichi Muto ; Michio Naito ; Masanori Shinzato ; Jiharu Hamako Fujita Health University, School of Health Science, Toyoake, Aichi, Japan Introduction and Objectives: Fujita Health University, School of Healthcare Science, Faculty of Medical Management and Information Science has been founded as a three-year college in 1996 and transformed into a four-year college in 2008. Since its establishment in 1996, the college has produced 750 Health Information Managers (HIMs). In the past two years since the four-year college has started, the examination pass rate for HIM of the school has been 100 percent among junior-year students while the average nationwide pass rate was as low as about 50 percent in the past five years. Special preparation program was implemented for maintaining the top level performance. Methods: Starting in 1998, the following three approaches have been applied. They were, (1) the intensive tutorial system by senior students, (2) the mock exams throughout the year with the original study guide, (3) special preparation lectures with the original guide book by almost all the faculty members in the department. As students can take the certification exam in their junior year, selected high-achieving senior students who already passed the exam in their junior year share their experiences and knowledge as supporting students. Faculty members assessed the trend in the exam questions, created original questions, and conducted the mock exams 6 times. At the same time, they held extra lectures to prepare the exam even if some of them had not directly come out of health information management field. This framework was made for enhancing the sense of unity among faculty and students for preventing dropout. After the certification exam, questionnaire survey to junior students regarding the real exam and the special lectures was carried out to refine the program. Results: Questionnaire survey in 2011 indicated that more than 60 percent of the students were satisfied with tutorial system. On the other hand, 85 percent answered that the special course by tutors should have started earlier. Besides, 23 percent of the students also perceived that the number of the mock exams as not enough, while 68 percent as adequate. 37 percent of the students answered that the extra lectures by faculty members were not satisfactory whereas the others answered satisfactory. Conclusions: Overall, the pass rate of the certification exam indicated the effectiveness of the methods above. However, based on the survey results, in 2012, the tutor program was planned to start earlier and the number of mock exams increased from 6 to 7 times. Some instructors of special lectures were shifted and e-learning system was newly implemented. The principle, which means that all the faculty members involve in for the exam preparation, has been encouraged. CS5.5.2 Knowing Is Better Than Not Knowing - An Educational Campaign For Clinicians Anna Sherlock Canada Health Infoway, Toronto, ON, Canada Introduction: The use of information and communication technology (ICT) in health care is gaining momentum. Health care professionals in many parts of the country are already working with electronic systems and seeing easier access to information needed for care, improved communication and coordination with colleagues, more efficient ways of working, and other benefits. Objectives: Building on this progress, Canada Health Infoway (Infoway) worked with their clinical engagement groups to jointly develop a Clinician Education Campaign. By targeting front-line clinicians as well as clinicians-in-training, the campaign aims to: 1) Increase the understanding of interconnected point-of-care and electronic health record systems for clinicians; 2) Increase awareness among clinicians that Canada-wide initiatives are in place to build a network of electronic systems in every province/territory, and eventually across the country; and 3) Provide clinicians with a place where they can get more information and offer opportunities to engage with peer leaders. The theme of the campaign is "Knowing is Better than Not Knowing." Methods: Qualitative research was conducted with front-line clinicians across Canada to gain insight into the current level of awareness and understanding of interconnected electronic health record systems as well as the impact and value proposition of ICT for the clinical community. Based on findings from this research, educational resources were developed in consultation with an Interdisciplinary Working Group and a Clinical Reference Group, comprised of 42 members consisting of front-line nurses, pharmacists and physicians from various health care settings (i.e. acute care, primary care, community, long-term care and public health). The draft resources were also tested in focus groups with over 80 clinicians including nurses, pharmacist and physicians across Canada.

96
Outputs: The Clinician Education Campaign launched on September 24, 2012 and is being delivered through our Clinical Champions to reach as many clinicians across Canada as possible. As part of the launch, the "Knowing is Better for Clinicians Toolkit" was made available on Infoway's website at www.knowingisbetter.ca as well as on several of our clinical partner's website. The toolkit includes a series of animated videos and peer-story videos where clinicians share their personal experience using technology in their day-to-day practice and highlights the key benefit areas such as timely access to information and improved communication and collaboration. The toolkit also comes complete with an Orientation Guide for participating Clinical Champions as well as a customizable PowerPoint presentation template, a Frequently Asked Questions document and a Template Article to help Champions spread the word about the campaign. Conclusion: Through this campaign, Infoway, together with their Clinical Champions, will raise awareness of the clinical value of information and communication technologies in practice and engage clinicians across the country. CS5.5.3 Quality Assurance in HIM Education at OHIMI, Sultanate of Oman George Kennedy OHIMI, Oman The educational system in Oman is experiencing a tremendous growth in response to the country’s demand over the last 25 years. Currently there are now over 200 diploma and degree programs offered in Oman, sourced from different countries. In the area of Quality Education, Oman’s first initiative was created in 1999 when the Oman Accreditation Council (now known as Oman Academic Accreditation Authority) was formed in order to accredit institutions and programs by using standards, information reviews and quality improvement process and to maintain the national qualification framework (Carroll et al, 2009). The initial version of the quality management system was known as Requirements for Omanis’ System of Quality Assurance (ROSQA). In 2006, a quality plan was developed that led to the establishment of an Oman Quality Network (OQN) to facilitate communication and exchange of ideas and effective practices (OAC, 2006). The Directorate General of Education and Training is responsible for leadership and management of all the institutes of the Ministry of Health. It has been involved in the development of the strategic plan contributing to the domain of human resources. One of the objectives of this strategy is to ensure quality standards of graduates of MOH professional education institutes through establishment of quality assurance system. The DGET quality assurance committee was commissioned to develop this strategic plan. Based on this, we at the Oman Health Information Management Institute (OHIMI) have developed our Operational plan. This paper presents the advances made in our institute in relation to the quality assurance process, infrastructural policies and framework, program standards and a range of quality enhancement activities. CS6.1.1 Surgical Data Integration into a Coding Software System. Development of a Custom Screen for Interactive Interfacing of Operative Room Data Joyce Taki 1; Ladan Irannejad 2 1Providence Health Care/Lower Mainland Health Information Management, Port Moody, BC, Canada; 2Providence Health Care/Lower Mainland Health Information Management, Vancouver, BC, Canada Introduction: A custom surgical screen is being developed to integrate surgical data entered into our enterprise-wide (core vendor) software system, into our external Coding software system. This will enable coders to view all surgical procedures on a custom screen. The screen will be interactive, allowing coders to select and copy entries from the custom screen to the standard coding intervention screen. This will improve the Coding process, making it more efficient. Since data will now be shared between our disparate systems, the accuracy and data consistency of the two systems will be enhanced. A robust Surgical data set will be available for reporting from our Coding software system. Additional data which is valuable for internal reporting, but not mandated for submission to the Canadian Institution for Health Information (CIHI), will be captured. Methods: We consulted with the surgical informatics team, menus and reports were reviewed and new reports written to check the surgical data available against the required data for submission to CIHI. Fields were mapped to either an existing table or a new table within our Coding Software System. There was an initiative in British Columbia at the time to map the facility specific procedure values to the standard Canadian Classification of Therapeutic Interventions (CCI) codes. This was integral to the success of our new custom surgical interface. We incorporated as many key fields as possible from the Operating Room system for reporting within our Health Authority, even if they are not reported to the Ministry. Field placers were assigned for SNOMED CT (Systematized Nomenclature of Medicine, Clinical Terms) for future mapping. A batch interface was written to transfer the data from our enterprise-wide (core vendor) software system, into our external Coding software

97
system. Results: The Go-Live date is set for February 2013. Increased Coder satisfaction and productivity is expected, based on a review of the facility specific procedures that can be mapped to standard CCI codes and process changes that will be made. Conclusions: Through deployment of the surgical custom screen and streaming of the operative room data to the Coding software system, we expect this will enhance data accuracy and lead to production gains of 5-10%. CS6.1.2 An Operation Model of Digital Medical Image Exchange with Potable Media among Hospitals for Regional Medical Collaboration in Japan Shigeki Kuwata ; Hitomi Yamada ; Megumi Inagaki ; Yuki Hamada ; Taiki Ozaki ; Satomi Miyajima Department of Medical Informatics, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan Introduction and Objectives: Adoption rate of picture archiving and communication systems (PACS) in Japan amounts to approximately 95% for hospitals with 600+ beds and 60—65% for those with 200-399 beds. Such trends have brought about a shift from films to digitized media to be used for information sharing of radiology test results. At present, use of portable media such as CD-R upon referral has become a standard method to share and exchange medical image data among medical institutions in Japan. Although emerging technology and standards, such as IHE XDS, are already implemented to achieve online information exchange, problems associated with the use of potable media should be addressed until the infrastructure based on such technology is securely and comprehensively introduced and utilized. An operation model was presented in this study to achieve smooth exchange of medical images with potable media among medical institutions. Methods: The model was developed and examined in practical settings at a national hospital in a Japanese urban area with approximately 600 beds where electronic patient records (EMR) and PACS were already in operation. For outgoing media, to be sent to a counterpart hospital, disc publishing systems (DPS) were introduced and connected with EMR. Orders issued by physicians were transferred to DPS to create the media that were subsequently handed to the patient responsible for media delivery to the institution to which referral was made. For incoming media, upon receipt at the information center of the hospital, whole data in the media were transferred to the computers that physicians use in the clinic before their consultation for the outpatients. For the secondary use, the data were copied to the long-term storage according to the physician's order after the consultation. Results: Due to growing demand for medical image exchange upon referral, delays in creating media used to frequently occur before the installation. In addition, due to the limited resources at the hospital, it used to be impossible to import data from incoming media prior to the consultation, though such needs were recognized to smooth the consultation flow by physicians. With the operation based on the model, the number of orders for outgoing media increased and time consumed for the operation reduced, approximately in average, by 100 per month and by 10 minutes per order, respectively. The simple implementation model made it feasible to import incoming data before physician's consultation. The number of imported data amounted to 13.9 per day in average, while the data transferred to the long-term storage amounted to 3.4 GB per day in average. Conclusions: The model contributed to the operational workflow in practical settings for regional medical collaboration with the limited resources available at the hospital. Further improvement would be needed while new technologies are examined in practical perspectives. CS6.1.3 Quality Criteria for Electronic Health Record Systems (EHRs) Rolf Engelbrecht 1; Angelika Haendel 2 1ProRec-DE, Ismaning, Germany; 2Universitätsklinikum Erlangen, Erlangen, Germany Introduction & Objectives: Clinical and managerial decisions in health care are based on information which are stored in electronic health records (EHR) The EHR is the nucleus of the relationship between the patient, the HC delivery system and all its professionals. As such, an EHR should be the core of Health Information Management. Main objective of the use of EHRs must be to improve quality in care by having the EHR and its associated information always available. The use of EHRs should lead to direct benefits for the professionals by making their work more efficient, improving medical knowledge and disease management, and allowing better preventive care and patient handling. The European Institute for Healthcare Records and Management (EuroRec) represents a permanent network of national non-profit organisations (the "ProRec centres"), ProRec centres are established to build awareness of the limitations, shortcomings and obstacles on the way towards widespread development, implementation and use of quality Electronic Health Records (EHR) and pointing them out using quality criteria.

98
EU and national funded projects (QREC project and thematic network) were set up between 2005 and 2011 to develop formal methods and to create a mechanism for the quality labelling of EHR systems in Europe, in primary- and hospital-care settings. Methods: EuroRec's short term strategy was to firstly collect high priority criteria from existing certification systems and EHR systems in Europe (and worldwide) and to analyse how they could be used in certification procedures. Over 1400 functional and other criteria have been analysed, decomposed, reworded in a consistent way and have resulted in this first limited list of EHRs quality criteria called fine grain statements (FGS). Each FGS is purely descriptive and contains reference(s) to the source, see screen shot. The ProRec-centres are the mediator between the users and the criteria. For a substantial set of the criteria translations in 20 European languages were performed for ease of use and acceptance. Several tools were developed for the country-specific introduction of quality criteria. In an iterative way using scoring 2 sets of statements were selected by the ProRec-centres for benchmarking. For accessing the fine grain statements different indexes were built, e.g a catalogue of business functions like “medical decision making” and “medication management”, health care setting and type of statement. The fine grain statements were broader described as good practice management. Results: They are described in previous paragraphs already. A set of tools for access and maintenance are available on www.EuroRec.org. About 25 evaluations on EHRs are done and resulted in EuroRec seals.
Conclusion: Quality statements, translations and tools were created. In all countries there are different regulations. A broad adaptation and use is expected for better health information management and quality of health care. CS6.2.1 Re-engineering Health Records Coding Processes to Streamline Analysis of Key Performance Indicators and Reduce Costs Anthony Hoad-Reddick 1; Steven Green 2 1York Central Hospital, Richmond Hill, ON, Canada; 2Salumatics Inc., Mississauga, ON, Canada Introduction: To describe how York Central Hospital (YCH), a 506-bed Toronto, Canada area community hospital, has streamlined data quality analysis, exceeded reporting obligations and expedited access to patient information. Through outsourcing the coding and abstracting of their health records to a service provider with access to a large pool of Canadian Health Information Management Association (CHIMA) certified coding staff, YCH has also achieved significant savings in health record coding costs over a ten year period. Methods: In 2001, YCH entered into a partnership with a service provider to outsource all of YCH’s health
99
records coding requirements. Since then, the service provider has coded all patient visits, including In-patient, Day Surgery, Emergency Room (ER) and clinics. The service provider also performs all coding-related data quality validation and audits prior to the hospital submitting the required data to both the Canadian Institute for Health Information (CIHI) and the provincial health ministry (MOHLTC). The service provider incurs all expenses related to recruiting, training, vacation and sick coverage with no increase in the fees charged to the hospital. Utilizing the coded health record and other sources of data, YCH’s performance management team continues to provide valuable data analysis and reports to both internal and external YCH stakeholders. Results: Over the ten year period YCH has realized substantial annual savings in coding costs. Regardless of the volume of visits to be coded monthly, the per-record fee remains the same and all visits are coded by the agreed-upon completion date. The YCH Performance Management team now has access to completed ER reporting data by the third business day of the next month and by the 30th day of the following month for In-Patient and Day Surgery. The “freshness” of the data allows for virtually real time internal reporting and analysis of key performance indicators, which are tied to funding through the pay for performance incentive program. As an added benefit of the existing partnership, YCH was able to meet the requirements of two additional programs. First, they recently commenced collecting data for the Canadian Joint Replacement Registry program. Second, Cancer Care Ontario recently reduced the reporting time lines for the CCO data book. As a direct result of their work with the service provider, collection of data for both these programs is performed by the remote coders with no impact on YCH resources. Conclusions: The partnership between hospital and service provider is recommended as it allows both parties to focus on what they do best. The service provider supplies experienced, qualified coding specialists. The hospital conducts close-to-real-time analysis and reporting of key performance data to support areas such as services and program planning, program management, and MOHLTC and hospital reporting with resulting cost savings being available for re-investment. CS6.2.2 How Meaningful is the Provider Documentation in the EHR? Success Strategies Associated with Bridging Clinical Documentation Gaps in the Electronic Record Cassi Birnbaum Peak Health Solutions, San Diego, CA, United States Introduction and Objectives: A degradation seen in clinical content is an artifact of the EHR unless an aggressive multi-faceted strategy is undertaken to counteract this concerning trend. It is of critical importance that best practice strategies be employed to assure that all documentation is meaningful, relevant and devoid of replicative, outdated and irrelevant documentation to assure that the patient's story isn't lost or buried. Methods: A decrease in meaningful clinical documentation is a natural phenomenon as the physician transitions from the paper world to electronic. As part of the change process, a physician has some fear the patient's story is going to be lost in the electronic world. Thus, the physician feels obligated to include all data at every patient encounter. Extensive end-user education on the EHR and physician ease or comfort with the system are the best way to stem the tide against the note bloat phenomenon. Cassi Birnbaum will chronicle her EHR journey and the research performed to illustrate how notes quickly built on the next one and replicated artifact detract from new information, and quickly the notes became unreadable to other physicians. It becomes very difficult to distinguish what was new clinical as information from documentation which described a condition from a day, week or month ago. Results: Best practice solutions and approaches will be showcased from developing specialty specific templates to facilitate patient care communication, the transition to ICD-10 required diagnosis and procedural specificity to capture of meaningful use measures. Other forms of alternative capture will be presented as part of an integrated approach to attack the documentation gaps head on. Success strategies associated with engaging physicians in improving their documentation will be presented on behalf of Nicolas Holmes, MD, MBA a practicing surgeon who has lead EHR, CDI, and ICD-10 initiatives. Rady Children's Hospital of San Diego, which began its EHR journey in early 2000, discovered that notes in its niche neonatology documentation system quickly built on the next one and replicated artifact detracted from new information. As a result, it didn't take long before the notes became unreadable to other physicians. It became difficult to distinguish new clinical data from documentation that may be describing a condition from a day, a week, or a month ago. Although the neonatologists felt the system saved them time, other physicians found their notes to be unhelpful. Conclusions: This example illustrates the need for relevant, timely, accurate, and succinct documentation in the EHR. Clinicians must be assured that the note reflects how sick the patient actually is. Although, there is not perfect system or tool to prevent "note bloat", Rady Children's Hospital has created a best practice model from

100
which other organizations can carefully construct their documentation programs to prevent notes that are unreadable from appearing. At Rady Children's its EHR motto "its for the kids" is imbedded in everything associated with the EHR roll-out, and its continued optimization. The prevention of "note bloat" ties back to its mission to assure that the documentation in the EHR serves as a useful tool to support the care and treatment of its patients across the continuum of care. Research Findings in an article published in the June 2009 issue of the American Journal of Medicine, Eugenia L. Seigler, MD, and Ronald Adelman, MD, identified hazards in electronic documentation that can lead to reduced credibility of recorded findings, clouding clinical thinking, limiting proper coding, and rob the record of its narrative flow and function. CS6.2.3 Measuring Quality Against the Bottom Line Maria French Terra Nova, St. Johns, NF, Canada Introduction: HIM professionals are constantly challenged with managing cost effective clinical documentation. Ten years ago, traditional dictation/transcription was by far the predominant method used to create clinical documentation. But today's marketplace options lean heavily towards technology-based solutions including speech, voice and EHR templates. While the drive towards greater technological-enablement of the documentation process is good, progress is thwarted and medical errors run rampant when transcriptionists are removed from the production process. Long relied upon by physicians for their ability to check accuracy of the spoken word, transcriptionists are the second set of eyes and ears for quality clinical documentation-but at what cost? This session identifies the key concerns surrounding EHR, template-based documentation and medical error prevention. Speakers compare and contrast four different documentation options to help attendees make the best, go-forward decision for their clinicians and organizations. Finally, the role of natural language processing (NLP) in clinical documentation is explored. Methods: Documentation error percentages introduced by physicians using different technology options. Impact of documentation errors on quality care, patient outcomes, coding and billing. Comparisons between various process management and technology options, and impact on documentation including review of technology issues, human issues and quality concerns. Differentiating the cost advantages of each system. Assess the value of a hybrid documentation environment. Evaluate the role of natural language processing (NLP) in clinical documentation. Results: By the end of this session, the participant will be able to: Assess the best clinical documentation methodology to ensure quality, efficiency and cost effectiveness. Understand the benefit and rationale of a hybrid documentation environment. Implement best practices and utilize take home checklists for clinical documentation workflow and management; regardless of methodology. Conclusion: In a market driven by technology concerns over labor considerations, it is important to remember no technology situation can stand on its own. A variety of clinical documentation options are now available and each must be assessed to determine the best solution for each, individual organization. Information to help attendees choose the best clinical documentation approach is the goal of this session. CS6.3.1 Expected Benefits of Primary Health Care Electronic Medical Record Content Standards (PHC EMR CS) for Patients and Health System Managers in Canada Alison Bidie ; Patricia Sullivan-Taylor Canadian Institute for Health Information, Toronto, ON, Canada Introduction: Across Canada, primary health care (PHC) is one of the busiest parts of the health care system with increasing need for more and better information to support health system improvements. The Canadian Institute for Health Information (CIHI) led the development of the draft Pan-Canadian Primary Health Care Electronic Medical Record Content Standard (PHC EMR CS) in collaboration with jurisdictions and Canada Health Infoway. The PHC EMR CS describes a subset of data elements in EMRs that can be captured in a standardized way across PHC settings. In addition, the PHC Data Extract Specification supports the ability to extract data from EMRs to facilitate reporting at the practice-level and submission to secondary sources for health system use. Implementation of the standard will directly benefit patient care and health system management needs in Canada. Methods: The presentation will examine the value of standards to improve EMR use and functionality to support quality of care and health information for clinical practice management and health system management needs. To better understand the clinical value, CIHI have engaged with key stakeholders on jurisdictional EMR

101
demonstration projects. Participating PHC practices, submit their EMR data to CIHI’s PHC Voluntary Reporting System for analysis. Feedback reports are provided to vendors to inform compliance to the PHC EMR CS and data quality. Clinicians receive quality improvement tools to support patient care and population management. Results: Participants will gain an insight into PHC EMR CS implementation across Canada and the lessons learned to date and examples of the clinical value of standardized EMR data and how it supports clinicians and health care system decision-makers with information to improve quality of care such as prevention, chronic disease management, outcomes and access to care. Conclusions: The PHC EMR CS when implemented in EMRs is a building block to supporting high-quality PHC data for both patient care and health system management needs. Preliminary results and lessons learned point to considerable benefits to implementing the content standard in EMRs. Ongoing jurisdictional support around implementation and shared solutions will be essential to its success. CS6.3.2 Transforming the Next Generation: Clinicians-in-Training Anne Tran Fazzalari 1; Maureen Charlebois 1; Irving Gold 2; Cynthia Baker 3; Harold Lopatka 4; Kristine Crosby 3 1Canada Health Infoway, Toronto, ON, Canada; 2Association of Faculties of Medicine of Canada, Ottawa, ON, Canada; 3The Canadian Association of Schools of Nursing, Ottawa, ON, Canada; 4Association of Faculties of Pharmacy of Canada, Edmonton, AB, Canada Introduction: Canada is home to world class medical, nursing and pharmacy schools whose educators and students recognize the value and potential of information and communication technologies (ICT) to improve health and health care. Canada Health Infoway (Infoway) has collaborated with the Association of Faculties of Medicine of Canada (AFMC), the Canadian Association of Schools of Nursing (CASN) and the Association of Faculties of Pharmacy of Canada (AFPC) to engage faculty and the next generation of clinicians to strengthen learning on effective clinical use of ICT. Methods: A collaborative approach was taken among project partners to develop and advance a national strategy aimed at building sustainability and capacity to achieve adoption and benefits realization of ICT in clinical practice. Results: Infoway will discuss the national clinical engagement strategy and the ‘Clinicians-in-Training Joint Collaborative’ with participating partners AFPC, AFMC and CASN. AFPC will discuss how ICTs are supporting the rapidly expanding pharmacist’s scope of practices and associated health information needs as well as their approach in preparing undergraduate pharmacy students to optimize the use of pharmacy and health information / information technology. AFMC will focus on medical informatics curriculum in faculties of medicine across Canada, including the comprehensive stakeholder engagement process to review, dialogue and ultimately in the creation of new e-learning resources to support informatics curriculum on electronic health record service systems. A virtual patient challenge will also be discussed. CASN will discuss their national initiative towards developing a culture within nursing education in Canada that embraces the integration of nursing informatics in curricula and professional practice and the aim to facilitate the successful delivery of health care in an increasingly technology enabled practice environment. The engagement of nursing faculty, students and other key stakeholders in a national consensus building process so that new nursing graduates enter the workplace able to practice effectively in the increasingly electronic world of health care delivery will also be explored. Conclusions: As Canada moves towards the implementation of the electronic health record, it is critical that clinicians enter the workforce prepared for the reality of rapid advances in health information technology. The Clinicians-in-Training strategy approach aims to integrate concepts and expectations related to the use of informatics into the curricula design/educational processes of the Faculties of Medicine, Nursing and Pharmacy; generate supportive learning environments for faculty and students; and demonstrates the importance of learning on effective uses of ICT in practice to provide enhance patient and family centered care. CS6.4.1 The Needs for Electronic Medical Records in Large Level Hospital in Nepal Laxman Paudel 1; Lorraine Nicholson 2 1Western Regional Hospital, Pokhara, Gandaki Zone, Nepal; 2International Federation of Health Information Management Associations, Rochdale, Greater Manchester, United Kingdom Introduction: The medical record is a patient-centered document used to support existing and future care. It can also used as legal document. Poor quality medical records do not help medical practitioners and other clinicians to make an accurate diagnosis or support the provision of appropriate clinical care to the individual patient. Incomplete medical records do not support specific case reviews and or the management of clinical support

102
departments. This study aims to assess the completeness of discharged patients’ summary sheets in the Western Regional Hospital, a regional level Government Hospital in Nepal. Methods: A cross sectional study was conducted by analyzing all discharge summary sheets of patients during a 15 days period (July 1 to July 15, 2012) in the Western Regional Hospital in Pokhara. During this period the total number of discharged patients was 904 including in-patients. The format of the hospital’s discharge summary was taken as a standard and evaluation for completeness was made on the basis of a check sheet. Descriptive statistics were used in this study and Microsoft Office Excel was used for data analysis. The study was limited to identifying whether discharge summaries in the Western Regional Hospital in Pokhara were complete or incomplete. There may be also be a need to study existing practices for medical record keeping and for procedures to monitor and improve the quality of hospital data in the future. Results: Numbers and percentages of missing data items in the 904 discharge summaries examined were as follows: Patient condition at discharge/outcome of care 680 75.22% Initial patient history and investigation 24 2.65% Names and signatures of doctors 325 35.95%
Final diagnoses were missing 485 53.65
Full local address 106 11.72% Details of patients' name of guardians 43 4.75%
Time of admission 7 0.77%
Patient's occupation 81 8.96% Patient's religion 53 5.86%
Patient's Marital Status 40 4.42%
The following data items were complete in all the discharge summaries examined: Patient's name; Patient’s age; Patient’s gender; Length of stay in hospital; Provisional diagnosis. Conclusion: The discharge summaries examined showed that not all were fully completed during the patient’s stay. In particular; condition on discharge, name and signature of doctors, final diagnosis, full address, brief history and details of investigations. These deficiencies in documentation resulting in incomplete or missing data could be addressed by use of electronic medical records. Because the Western Regional Hospital in Pokhara, like other large level hospitals, has the facilities to deliver a full range of services, an electronic medical record system with mandatory data fields would be more effective in reducing the incidence of missing data than paper-based medical records. Therefore the use of electronic medical records in this hospital and other large level hospitals in Nepal should be a priority. CS6.4.2 Development and Implementation of a Health Information Management System for St. Lucia Margaret Samuel 1; Brunette Willius 1; Grantley Charlemagne 2 1St Jude Hospital, Vieux-Fort, Saint Lucia; 2Public Service, Castries, Saint Lucia Introduction and Objectives: The health Information system in St. Lucia like other developing countries is faced with challenges such as a cultural resistance to change, poor legal framework to support the system, lack or poor vision and mission statements, lack of continuity of a sustained leadership role. The system also suffers from lack of funding and trained staff. Also, they are under-resourced, weak and disjointed, this causes the information and statistics generated to be insufficient to support evidence based decisions and planning. However, over the last six years great progress was made when it was decided that the health information system should be developed and implemented with a primary health care focus/emphasis through the primary health care centers with a capability to expand to secondary and tertiary health care levels as it develops. Method: Preliminary research was done to assess the health information situation, committees were appointed to handle the legal, marketing, change management, clinical, pharmaceutical and other aspects of the system. Workshops were conducted and experiences were drawn from developing countries like Belize and Jamaica who already had systems in progress. A fully staffed Health Information Management Secretariat was appointed with trained staff. The Pan American Health Organization worked with us throughout the journey. Results: Diabetes and Hypertension are diseases that are highly prevalent in St. Lucia. Because of the health information management system, the government administration, along with other stakeholders have been able to access reliable data on these diseases along with data on other non-communicable and communicable diseases, also information on maternal health and child care resulting in better management of these conditions.

103
Conclusion: It is a long journey. The decision to start the implementation of the system at the primary health care level has worked well as it allowed for implementation at a less complicated level and it will easily facilitate expansion to the secondary level as we move into the future. With strong political and national will and hard work the expansion of the health information system should be much easier. CS6.4.3 Survey on Implementation and Use of Electronic Health Records in Nigeria Lorraine Nicholson 1; Olawole Ajayi 2 1International Federation of Health Information Management Associations, Rochdale, Greater Manchester, United Kingdom; 2Health Information Managers Association of Nigeria, Lagos, Nigeria Introduction and Objectives: A survey on the implementation and use of Electronic Health Records (EHRs) in Nigeria was conducted during the HIMAN national conference in Lagos, Nigeria in 27-30 August 2012 to collect information from all conference delegates representing different healthcare organisations from different states in Nigeria. Methods: A peer-reviewed anonymous questionnaire was developed and distributed to all delegates at the conference and they were asked to return the completed questionnaires before the end of the event. Information was then sought on gender and age (within one of six specified age groups) and about the respondent's personal computer usage, existing skills and whether formal training had been undertaken or whether they were self-taught in use of computer hardware and software. Information was then sought on the electronic health record (EHR) and the healthcare organization in which the respondent worked, whether any type of electronic health record was already in use and what type of training had been provided in the use of an existing EHR system or if there was an EHR implementation planned in the future. Qualitative information was then sought regarding health record-keeping, patient care, patient safety, perceived benefits and, if their healthcare organisation was not planning to implement an electronic health record system, the reasons why this was so. Results: The data from this very recent survey are currently being analysed and they cover: * Anonymous personal information about respondents * Respondent's experience and expertise in use of IT and software applications * Training undertaken in use of IT and software applications * The types of healthcare organisations where respondents are employed * Current and future planning for EHR implementation in the respondent's employing organisation * Anticipated benefits for patients, for the healthcare organisation, for individual HIM practitioners and for healthcare delivery in Nigeria Conclusions: It is anticipated that the information derived from this survey will identify potential EHR implementation issues to be addressed including resource constraints in different healthcare settings in Nigeria. CS6.5.1 Implementing Primary Health Care EMR Content Standards and Terminology Reference Sets in Canada: Tips for Success Alison Bidie 1; Beverly Knight 2; Patricia Sullivan-Taylor 1 1Canadian Institute for Health Information, Toronto, ON, Canada; 2Canada Health Infoway, Toronto, ON, Canada Introduction: In an effort to improve the standardization of primary health care (PHC) data in electronic medical records (EMRs), the Canadian Institute for Health Information (CIHI) and Canada Health Infoway (Infoway) collaborated on the development of PHC reference sets to provide implementers with a list of allowable coded values to be collected at the point of service systems in support of the PHC EMR Content Standard version 2.1(PHC EMR CS). PHC Reference Sets can also be leveraged by other clinical applications such as eReferrals, chronic disease management or electronic health records. They are designed to support point of service as well as interoperability and health system use. To date, 41 PHC Reference Sets have been developed to support priority clinical and administrative data elements. The reference sets were developed by using numerous source code systems including SNOMED CT®, pCLOCD/LOINC, HL7® code systems and ISO 639-3. Through ongoing collaboration, CIHI and Infoway will support jurisdictions with implementation of the PHC EMR CS and PHC Reference Sets. Lessons learned from the development process and pilot projects will inform next steps to facilitate EMR adoption across Canada. Methods: The presentation will provide an overview of the development and future maintenance of the PHC EMR CS and PHC Reference Sets. This will include the engagement process with jurisdictions and clinicians for input. An environmental scan was conducted across Canada to understand the status of adoption of the PHC EMR CS
104
and PHC Reference Sets as well as jurisdictional priorities, challenges and enablers. In addition, a PHC reference set pilot project is underway to inform the next steps on implementation. Results: Participants will gain an insight into lessons learned from developing a pan-Canadian content standard and PHC Reference Sets and their anticipated or early benefits, implementation and maintenance considerations based on pilot findings. Environmental scan results and EMR adoption experiences will be shared. These results will identify jurisdictional needs and the next steps towards implementation of the content standard and reference sets in Canada. Conclusions: The PHC EMR CS and PHC Reference sets are the foundation to supporting high-quality PHC data for point of service and health system management needs. Lessons learned from the development and implementation experience to date, will inform future considerations. Preliminary results indicate considerable benefits to standardized PHC EMR data. Ongoing jurisdictional support will be essential to its success. CS6.5.2 Roles and Competencies for Managing Terminology Assets Sue Schneider 1; Kathy Giannangelo 2; Kelly Abrams 3; Rita Scichilone 4 1eHealth Ontario, Toronto, ON, Canada; 2International Health Terminology Standards Development Organisation, Copenhagen, Denmark; 3Canadian College of Health Information Management, London, ON, Canada; 4American Health Information Management Association, Chicago, IL, United States Introduction and Objectives: The management of health information is rapidly changing revealing some gaps in professional knowledge and experience with the use of terminologies used for health records and information sharing between healthcare providers, institutions, government and consumers. This paper addresses terminology asset management trends and skills and competency requirements for Health Information Management (HIM) professionals. The primary objective of this work is to raise awareness of the emergence of terminology asset management in healthcare and confirm the roles and competencies required for expanded, specialized employment opportunities for HIM around the world. Methods: A team of HIM professionals from Canada and the United States affiliated with Health Information Management Associations came together in 2009 and 2010 to explore and confirm the opportunities for HIM professionals in this new role. Papers about terminology asset management were presented in 2009 for the Revolutionizing Health Care with Informatics: From Research to Practice conference in Victoria, British Columbia, Canada and the IFHIMA 16th Congress in Milan, Italy in 2010. This new work describes the current trends, skills and competencies for terminology asset management work with additional insight on job requirements and educational or training needs. Learning levels were used to inform educational needs: 1. Awareness of emerging roles 2. Knowledge of job requirements 3. Analysis of terminology management 4. Advanced concepts in terminology asset management Results: Confirmation of job descriptions, job functions and experience requirements are compiled with examples of knowledge clusters important for these roles in health care. Because the use of standard terminologies is essential to semantic interoperability in electronic health records examples of job roles and competencies are featured. Conclusions: The profession of health information management is experiencing transformation to a new workplace requiring deeper knowledge and experience with clinical terminologies used in electronic environments. Terminologies of the future are the new building blocks for health record management and information exchange. There are data deployment, data mapping, data governance and data integrity challenges to meet and new skills to acquire to be eligible for emerging roles. This changing world truly contributes to advancing opportunities with HIM professionals taking on these new roles, making a world of difference in healthcare. CS6.5.3 Health Data Dictionary Access: Making a Commercial Terminology Server Product Publicly Available Marc Berlinguet 1; Kasey Poon 2; Oktavian Weiser 3 13M HIS, Wallingford, CT, United States; 23M HIS, Salt Lake City, UT, United States; 33M HIS, Frankfurt, Germany Introduction: In May 2012, 3M announced that, in partnership with the U.S. Department of Defense (DoD) and the U.S. Department of Veterans Affairs (VA), HDD software and content is progressively to be made available in

105
the public domain. 3M has provided the DoD Military Health System (MHS) with this technology for many years, and this arrangement will facilitate the DoD’s and VA’s efforts to achieve semantic interoperability with each other and between health systems everywhere. Methods: The 3M Healthcare Data Dictionary (HDD) is a concept-based, controlled medical terminology server software application that has been commercially available since 1996. It contains several terminology standards and healthcare code sets, such as ICD-9, ICD-10, LOINC, SNOMED CT, and RxNorm. 3M customers have been using the HDD to facilitate information exchange, become compliant with vocabulary standards, and normalize disparate clinical data. The HDD contains over 2.5 million concepts, over 17.5 million representations, and over 15.5 million relationships. Objectives: The philosophy behind the HDD is to have a single, centralized source for terminology mapping and maintenance, as opposed to point-to-point mapping. This approach makes both initial mapping and maintenance mapping easier and more manageable. Results: This approach makes it possible to manage several different terminologies and code sets simultaneously. This provides a mechanism by which users can be agnostic in terms of standards compliance. Instead of having to choose only one standard or a few with which to comply, an HDD user can load and map a variety of standards into the HDD database and be compliant with all of them. The publicly available version of the 3M HDD is called HDD Access: initially 214 799 concepts and 442 184 relations. This presentation provides examples of how the HDD structure enables normalization and exchange of information. Each HDD concept is identified by a meaningless Numerical Concept IDentifier (NCID), and the identifiers from external terminologies are also mapped to it. For instance, the concept of chickenpox has the UMLS Concept Unique Identifier (CUI) of C0008049 and the SNOMED CT ConceptID of 186513009 as mapped representations. It also has an "ICD9CM Code" relationship to "052.9". Conclusion: Details of how to access it and use it can be found at hddaccess.com. The commercial HDD continues to be available for users who desire a support and maintenance infrastructure. Also, the commercial HDD currently contains several third party code sets that HDD Access does not yet have, such as LOINC, SNOMED CT, and RxNorm. CS6.6.1 Post-Earthquake Health Information Management: Status and Challenges Yukiko Yokobori 1; Tuneo Sakai 1; Takahisa Takeda 1; Toshio Oi 2 1Japan Hospital Association, Chiyoda-ku, Tokyo, Japan; 2Japan Society of Health Information Management, Tokyo, Japan Introduction:The Great East Japan Earthquake occurred at 14:46 on March 11, 2011, setting off tsunamis that towered more than 10 meters, causing large-scale fire and destroying nuclear power plants. The area was seriously damaged. Methods: 1. Shortly after the earthquake, Japan Hospital Association (JHA), Japan Society of Health Information Management (JHIM) and Japan Health Information Manager Association (JHIMA) jointly sent out mails/email to their members in east Japan (JHA 106 hospitals/2,500 hospitals, JHIM 242 members/5,700 members and JHIMA 418 members/2,830 members) asking for information about their safety. A notice was also uploaded to their websites. 2. We received inquiries from health information managers in the affected areas asking for advice on how they should practice HIM, in light of Japanese legislation, as they faced a situation that impeded them from keeping confidentiality and fulfilling archiving responsibilities. JHA, JHIM and JHIMA jointly forwarded the inquiry to the Ministry of Health, Labour and Welfare. 3. In July 2012, JHA conducted a survey on the current situation of the students living in the affected areas who were enrolled in JHA's distant training program. Results: 1. The members of conditions and their needs were identified and donations, relief goods and healthcare professionals were sent. Their membership fees were exempted. 2. The responses from the Ministry of Health, Labour and Welfare were distributed through newsletters and websites to the members immediately after reception. Other disaster-related information was also posted. 3. From the survey results, we were unable to learn accurately about the lost health records, but they showed overall living conditions of the respondents were progressively worsening. In Fukushima Pref. that suffered nuclear accidents, the respondents were evidently affected professionally (lost or changed jobs), economically and mentally. Regarding Health Information Management in post-earthquake situation, JHIM, Japanese Association for Acute

106
Medicine and other organizations formed a joint study team shortly after the earthquake. The team officially established the “Joint Committee on Post-Disaster Strategy for Health Information Management” in 2012 and began discussions on concrete strategies. Conclusions: We identified a need for national-level policy discussion on how Health Information Management should be implemented in an unpredictably serious situation as Japan had experienced. As for the effects of radiation from power plant meltdowns on people's health, long-term studies in various fields based on accurate records are required. To tackle this very serious challenge, the government, healthcare institutions and HIMs must fulfill their roles in working together to advance the studies. In post-disaster situation, HIMs are expected to practice the best-possible Health Information Management in given situations, and must be equipped with an extensive exper (…) CS6.6.2 Alberta Health Services Recovery of Data in the Wake of a Major Health Information System Failure Shirley Learmonth Alberta Health Services, Calgary, AB, Canada Introduction and Objectives: On July 11th 2012, the province of Alberta experienced one of the largest information technology down times in its history. A fire in an electrical room at Shaw Communications' building in downtown Calgary housing many government, healthcare and private industry's information technology infrastructure, put radio stations off the air, cut internet and telephone service, affected health care systems and many city and provincial government computer networks. City officials activated the municipal emergency plan and Alberta Health Services activated their Zone Emergency Operation Centres (EOC). What happens when a health care organization, strongly reliant on an Electronic Health Record (EHR) and information technology, loses its access to electronic information to conduct its business of healthcare? This presentation will speak to the challenges, lessons learned, what worked well and the Health Information Management (HIM) involvement in this major incident. Methods: The Calgary Zone was the hardest hit with approximately 200 applications non-functioning. Lab, Diagnostic Imaging, Pharmacy, ADT, Regional on Call Application, to name a few, were all impacted. Sunrise Clinical Manager (SCM), the Calgary Zone's EHR, had to be taken down because of the potential impact to patient safety and the lack of information flow from ADT and other systems. With e-mail and LYNC down communication across the zone and within the province was a challenge. A Major Incident (MI) conference line was established soon followed by the establishment of a ZEOC set up under the leadership of Senior Executive Vice-Presidents. HIM established regular bridge calls with representatives participating in both the MI and ZEOC calls. Results: After functioning in a manual mode for 36 hours, permission was given to begin the reconciliation of applications. Clinical Informatics and HIM were tasked with the development of a reconciliation strategy to ensure the appropriate sequencing of clinical applications to reduce the potential impact to patient safety and care delivery. ADT, the foundational application, had to be reconciled first and only then, could other applications begin their process. HIM facilitated the process with cross-site teams working in close partnership with IT and clinical program areas over several days. Conclusion: Opportunities for improvement and lessons worth sharing were captured in the post-downtime debriefs, some of which included: the need for a central library or paper holding for key documents, system redundancy/backups, up-to-date disaster fan-out lists, inventory of applications, defining roles and responsibilities, accessing downtime numbers, accessing physician on-call information, and more. There were also many things that worked well under the circumstances: For example, collaboration and partnership between disciplines and HIM engagement and leadership on key strategies. CS6.6.3 Measuring Staff Perception of Change Margaret Penchoff Canadian Institute for Health Information, Ottawa, ON, Canada Introduction and Objectives: The health care industry has undergone many changes over the years. From advancements in care, to medical innovations, to new technology, to new delivery modes and models, to restructuring and reorganization, change in health care is inevitable. The health care system in the Province of New Brunswick has undergone a number of changes since the 1960s. The most recent change, which was announced March 11, 2008 and which was effective September 1, 2008, was a transition from eight regional health authorities to two regions. In addition to this change, the government created a public sector company, to assume responsibility for certain

107
non-clinical services and programs such as materials management, information technology and telecommunications, and laundry services. The changes were an attempt to improve the efficiency of health care delivery and to reduce duplication of services in the province. In addition to the transition, employees encountered a number of other changes such as changes to reporting structure, physical relocation, the implementation of new policies, procedures, processes and technology. The amount of change that occurred within the various departments of the organization was anecdotal. A study was undertaken to quantify what changed and to measure the staff's perception of the changes that took place. Methods: A four-page "change" questionnaire consisting of 39 close-ended questions and one open-ended question was developed and administered to employees. The questions were classified under the following categories: people, tasks, technology and change. The survey was an anonymous, self-administered questionnaire completed by employees on a voluntary basis. Consent was implied by completion of the questionnaire. The same employees had participated in a First STEP (Strategic Transformation of Existing Processes) project which included review and assessment of the various roles, processes and functions to identify opportunities for quality improvement. Inefficiencies, delays and/or steps with no added value that affected the staff member's ability to work efficiently and effectively were identified. Suggested changes were implemented. The staff then completed an employee satisfaction survey. The information gained from the "change" questionnaire would complement the information elicited from the First STEP project; hence these employees in each of the four zones were selected to complete the "change" questionnaire. Results: The survey response rate was 32%, zone "a"; 9%, zone "b"; 31%, zone "c"; and 27 completed questionnaires from zone "d". Conclusions: Being aware that change is going to happen, what impact the change will have on the individual, what the individual can do to prepare for the change and involvement in planning for the change are all important components of successful implementation of change. Strong leadership and effective and regular communication are also important. Panel Sessions Abstracts PAN1 Managing Consent in EHR Systems Roch, Joan1; Morgan, David2; Grant, Debra3; Leonard, Chantal4; Seaton, Brendan5; Ratajczak, Stanley1 1Canada Health Infoway, Montreal, QC, Canada; 2Newfoundland and Labrador Centre for Health Information, St. John's, NF, Canada; 3Office of the Privacy Commissioner of Ontario, Toronto, ON, Canada; 4Canadian Nurses Protective Society, Ottawa, ON, Canada; 5ITAC Health, Toronto, ON, Canada Introduction and Objectives: This session will present business, technical and architectural considerations identified in a Canada Health Infoway-sponsored project on consent management in electronic health information systems. The project aimed to help Canadian jurisdictions meet their legal and policy requirements related to consent for sharing personal health information in electronic health record (EHR) systems. Key topics such as granularity and interoperability of consent will be discussed by a panel that includes ministry, privacy oversight, clinician and vendor representation. Methods: The project drew on expertise from the pan-Canadian Health Information Privacy Group (made up of jurisdictional health/e-health ministry representatives), as well as input from a broader stakeholder group that included representation from clinician groups, oversight bodies, vendors and system architects. Results: Findings of the project include: * Consent management solutions currently in place appear to have limited functionality and are not interoperable across EHR system components within a jurisdiction. * Currently if an individual wishes to mask certain information, typically the entire record in the clinical domain is masked or rendered inaccessible. Clinicians indicate that there may be patient safety issues in reviewing a record which does not include potentially relevant clinical information. * It is also difficult to assure individuals that their wishes are being respected when the information they are trying to restrict may be discerned from other data in the system. Consequently, at this time most jurisdictions have chosen to mask all domains. This is viewed as the best and safest means for ensuring that the individual's wishes are respected. Conclusions: * Jurisdictions determine the consent approach and solutions that meet their unique needs and may take a mix of approaches given legacy systems and EHR implementations to date. However, given the ongoing implementation

108
of system components and expected future integration of information systems, movement towards some consistency in consent management could be helpful. Such an approach needs to be flexible to accommodate o the wide range of jurisdictional needs o the integration of multiple EHR systems, including legacy systems o the management of differences in consent granularity among systems and o the evolution of the consent environment as more solutions come online. * Tools that promote consistency, such as standard messaging and taxonomy to allow solutions to interact with one another when required, can help achieve interoperability at the jurisdictional level and in the longer term, across jurisdictions. It could also make Canada a more attractive customer for consent solutions in the global marketplace. PAN2 Health System Transformation - Dialogue to Action Nagle, Lynn1; Kaminski, Vickie2; Reid-Haiughian, Cheryl3; Thorsteinsson, Pamela4; Gibson, Candace5 1CNIA, University of Toronto, Nagles & Associates, Inc, Toronto, ON, Canada; 2Eastern Regional Health Authority, Newfoundland and Labrador, NL, Canada; 3ParaMed Home Health Care, Ottawa, ON, Canada; 4Fraser Health Authority, Surrey, BC, Canada; 5University of Western Ontario, London, ON, Canada The national Nursing action plan promotes transformation of the Canadian healthcare system, including using technology to its fullest. Sharing the national consultation journey and the plan for contributing to the national health agenda. Steps to Action! PAN3 HIM/HI Workforce Transformation Kennedy, Margaret1; Crook, Gail2; Wissmann, Sallyanne3; Anani, Namir4; Newsham, Don5; Thomas Gordon, Lynne6 1Global Village Consulting Inc, Nova Scotia, NS, Canada; 2CHIMA, London, ON, Canada; 3Mater Health Services, South Brisbane, QLD, Australia; 4Information and Communications Technology Council, Ottawa, ON, Canada; 5Canada's Health Informatics Association, Toronto, ON, Canada; 6AHIMA, Chicago, IL, United States For the last few years the Health Informatics community, and Health Information Management Community have been working towards defining new roles and competencies for HI and HIM in the eHealth Industry. Together and individually Associations have invested a great amount of time and resources to researching the future needs for the full deployment of the Electronic Health Record (E.H.R.) and what roles HI and HIM need to establish. While roles and competencies are being developed, there is also a need to work with Industry leaders and Educators to ensure the HI and HIM professionals will have the necessary skills for these new roles. In Canada the information, Communications and Technology Council of Canada (ICTC) is looking at the economic impact of HI and HIM roles. AHIMA has not only defined new roles, but is also deploying their new tool - a skills matrix for their HIM members. the Canadian Nursing Informatics Association of Canada (CNIA) has also studied the roles and competencies that nurses will require in an ehealth environment. CHIMA has published a report on new roles and competencies for the Canadian HIM, as well as a strategy for Workforce Transformation. The HI Association in Canada is COACH, and the CEO will share their recent work on competencies for HI in Canada. The final panelist is from Australia (IFHIMA) and she will share the Australian perspective. This panel brings together a group of experts who will share their work and perspective on the HI and HIM Future Roles. This is a "must attend " session, with an opportunity for audience participation. CNIA Concurrent Sessions Abstracts CNIA1.1.1 Finding Value in the Collection of Standardized Clinical Outcomes Peggy White ; Ian Purdy Institute for Clinical Evaluative Sciences HOBIC, Toronto, ON, Canada
109
Health Outcomes for Better Information and Care is implementing the electronic collection of standardized clinical outcomes in health care organizations. Lessons learned from working with organizations in using this information to drive system improvements will be presented with a focus on the value of outcomes data for improvements in patient care. CNIA1.1.2 C-HOBIC -- Standardizing Clinical Outcomes in Canada Kathryn Hannah 1; Peggy White 2 1C-HOBIC, Calgary, AB, Canada; 2Institute for Clinical Evaluative Sciences HOBIC, Toronto, ON, Canada C-HOBIC, an initiative of the Canadian Nurses Association, is leading the way with the collection of standardized clinical outcomes in Canada. This presentation will provide the background and approach for coding the clinical outcomes. In addition the presentation will explore the value of this information for the health care system. CNIA1.1.3 Technology-Enabled Evidence-Based Practice, Outcome Evaluation and Knowledge Creation Rita Wilson ; Irmajean Bajnok Registered Nurses' Association of Ontario, Toronto, ON, Canada This presentation demonstrates the benefits of leveraging technology to transfer research knowledge into nursing practice to foster evidence-informed clinical decision-making. It also highlights components of a quality improvement initiative that links nursing interventions to nursing-sensitive outcome indicators and paves the way for knowledge creation through seamless collection of clinical data. CNIA1.1.4 When Home Care Nurses Use Technology at the Point-of-Care, Do Client Outcomes Change? Cheryl Reid Haughian 1; Diane Doran 2; Jennifer Carryer 2 1Knowledge and Innovation ParaMed Home Health Care, Toronto, ON, Canada; 2Lawrence S. Bloomberg Faculty of Nursing, University of Toronto, Toronto, ON, Canada A large home care organization recently provided home care nurses with smart phones for documenting client assessments and for accessing clinical resources at the point-of-care. This presentation focuses on the trends in client outcomes at various stages of introducing the information and communication technologies and practice changes. CNIA2.1.1 Choosing a Theoretical Framework to Evaluate Electronic Health Record and Other Technology Implementations Kathy Momtahan The Ottawa Hospital, Ottawa, ON, Canada Choosing a theoretical framework to evaluate electronic health records and other technology implementations can often be challenging in a hospital environment due to lack of resources, expertise, and timing. Strengths and weaknesses of various frameworks will be reviewed, including an assessment of resources needed to effectively implement them. CNIA2.1.2 Creating a Culture of Clinical Adoption: Benefits Realization of Technology Liz Nemeth Healthtech Consultants, Toronto, ON, Canada A regional health portal deployed to clinicians offering access to health information across the continuum of care. Learn how an innovative approach using organizational innovation theory, analyzing principles that are critical to the success of technology designed to change behavior, thereby influencing its adoption were instrumental in successful uptake and adoption. CNIA2.1.3 Healthcare Knowledge for Manitoba eHealth Managers Pat Rothney Global Village Consulting Inc., Winnipeg, MB, Canada In today's highly dynamic business environment partnerships based on trust, shared vision, and shared leadership create a clear advantage. This Master's inquiry examined the importance of understanding key health business
110
concepts and the learning needs of IT managers. The inquiry methodology, findings, conclusions, recommendations, and implications will be presented. CNIA2.2.1 What Are Some of the Causal Relationships That Lead to Successful Order Set Adoption? Susan Hall Kingston General Hospital, Kingston, ON, Canada Achieving order set adoption in the complex adaptive system of the hospital setting is challenging. Using the realist review methodology and a focus group of interview participants this review explored some of the causal relationships that lead to effective and successful order set adoption in paper, electronic and/or CPOE formats. CNIA2.2.2 The Electronic Whiteboard: Can it Support Patient Safety and Quality of Patient Care? Robyn Alpert ; Arthom Barlis Mackenzie Health, Richmond Hill, ON, Canada This presentation will focus on how Best Practice Guidelines have been integrated into our Electronic White Board. We will highlight our key successes and lessons learned and our pre and post Implementation measurements on its impact on Patient Safety and Quality of Patient Care. CNIA2.2.3 Does Work Experience Using Technology Influence NI Competencies by End of 4th Year? Marie-Pierre Dionne Montfort Hospital, Ottawa, ON, Canada This thesis will examine two questions: 1) Do nursing students increase their NI competencies progressively from year 1 to 4 of their school program? 2) Do students with work experience using technology outside of the curriculum gain competencies more rapidly than those without by the end of 4th year? CNIA3.1.1 Establishing Innovative Nursing Informatics Leadership Roles Sally Remus 1; Diane Salois-Swallow 2 1Mackenzie Health, Richmond Hill, ON, Canada; 2Mackenzie Health, Southlake Regional Health Centre and Stevenson Memorial, Richmond Hill, ON, Canada Launching innovative leadership roles, 'nursing informatics' (NI) within eHealth project governance structures positions organizations to realize the benefits of patient safety, quality care and staff/patient satisfaction through leveraging ICTs. Further, organizations that endorse NI skills/knowledge to support clinical transformation efforts will emerge as 'trendsetters' that create sustainable health system delivery. CNIA3.1.2 Informaticians: The Next Generation Lynn Nagle Nagle and Associates, Toronto, ON, Canada Over the last 3 decades, informaticians have played a significant part in the evolution and dissemination of information and communication technologies (ICT). In this presentation, the author will present a perspective on the essential leadership roles and directions for the next generation of informaticians. CNIA3.1.3 Leveraging the Power of the TIGER in Canada Margaret Kennedy 1; Sally Schlak 2 1Global Village Consulting Inc., Merigomish, NS, Canada; 2The TIGER Initiative Foundation, Chicago, IL, United States This presentation provides an overview of the Technology Informatics Guiding Education Reform (TIGER) initiative, the Virtual Learning Environment, and the internationalization efforts to date. Opportunities to leverage TIGER for NI in Canada are explored in terms of practice, academia, and liaison through CNIA. CNIA3.1.4

111
Findings in Clinical Adoption of Nurses and Nurse Practitioners Using an EMR Eithne Reichert ; Margaret Timmons RWI Informatics Inc., Saskatoon, SK, Canada This presentation will share findings of clinical adoption of the EMR by Nurses and Nurse Practitioners in community practice, defining the clinical business requirements, configuration adjustments, and adoption techniques to augment the medical model of the EMR. Findings will include improved understanding of nursing requirements for electronic systems, including sharing records and collaborative team practice. CNIA4.1.1 Wireless Communication Device Implementation in Environments with Unique Needs: Results from an Adult Intensive Care Unit Susan Hall ; Rosemary Wilson ; Lenora Duhn ; Paola Gonzales ; Yolande Chan ; Elizabeth VanDenKerkof Kingston General Hospital, Kingston, ON, Canada Wireless technology in healthcare has been associated with communication-related improvements in workflow. This pre-post study using the Theory of Planned Behavior examined attitudes and perceptions related to implementation of a wireless communication device (Vocera) in intensive care and compares finding with an earlier study on a surgical unit. CNIA4.1.2 Remote Monitoring of Congestive Heart Failure Clients in Home Care: Innovation, Cost Effectiveness and Best Possible Client Outcomes Cheryl Reid Haughian ; Emily Seto ; Jonathan Tomkun ; Caterina Masino ; Joseph Cafazzo ; Deb Mulholland Knowledge and Innovation ParaMed Home Health Care, Toronto, ON, Canada Remote monitoring is a potential important strategy in evolving home care delivery models. A cost effective system that results in best possible client outcomes is critical to the sustainability of a new model. This presentation will summarize a heart failure remote monitoring project, lessons learned, and preliminary research results. CNIA4.1.3 Positive Patient Identifiers at CVH..."It's a Perfect Match" Lina Ranieri Trillium Health Partners, Toronto, ON, Canada Participants will be presented with highlights of the Credit Valley Hospital Positive Patient Identification Policy and Procedure which establishes the standardization of patient identification at point of entry, point of care, and documentation. Positive outcomes include improvements in registration practices and implementation of bar-coded printable devices to decrease misidentification errors. CNIA5.1.1 iNurse, iTeach: Barriers and Facilitators in Using Mobile Technology Shauna Davies 1; Sandra Bassendowski 1; Pamela Petruucka 1; Lorna Breitkreuz 2; Christine Demyen 2 1University of Saskatchewan, Saskatoon, SK, Canada; 2All Nations' Healing Hospital, Fort Qu'Appelle, SK, Canada This project utilized a mixed methods participatory action research approach to assess the impact of medical applications on clients' understanding of their condition and treatment plan. The barriers and facilitators of utilizing mobile technology in the rural and remote health care environments were identified. CNIA5.1.2 Wound Healing Rates Before and After Alert to Wound Management Specialist Leanne Currie 1; Shannon Hanfield 2; David Johns 2; Lori Block 2 1School of Nursing, University of British Columbia, Vancouver, BC, Canada; 2Vancouver Coastal Health Authority, Vancouver, BC, Canada The purpose of this study was to examine healing rates before and after the implementation of an alert designed to notify wound care specialty nurses who provide expert support for homecare nurses. Wound healed an average of 13.6 days faster after the alert was implemented (t=7.67, p<0.001).

112
CNIA5.1.3 The Integration of Mobile Learning and Teaching in Nursing Education Glynda Doyle British Columbia Institute of Technology, Burnaby, BC, Canada The incorporation of mobile devices to support student learning has become a growing trend in nursing education. This presentation discusses the use of Rogers' Diffusion of Innovation Model as a framework to guide the integration of mobile technologies into nursing programs at the British Columbia Institute of Technology. Education Day Sessions Abstracts ED1.2 Coding Education Around the World Carol A. Lewis 1; Joon H. Hong 2 1WHO-FIC Education and Implementation Committee, Rockville, MD, United States; 2WHO-FIC Education and Implementation Committee, IFHIMA Regional Director, Rockville, MD, United States Introduction and Objectives: ICD-10 is the global health information standard for mortality and morbidity statistics. ICD is used in clinical care and research to manage health care, monitor outcomes and allocate resources. The goal of the WHO-FIC Education and Implementation Committee (EIC) is to ensure standardized, high quality coding of health data for comparability within and among WHO Member States. The EIC has undertaken a number of activities directed to the development and approval of educational materials and the evaluation of the competence of coders by conducting pilot tests for ICD-10 mortality and morbidity coders/trainers. The results of the pilot tests for morbidity coders demonstrated the desirability of obtaining more information about coding education and the evaluation of coding quality and identifying steps for improvement. Methods: Coding educators and clinical coders in many countries are being surveyed, using different questionnaires, to obtain information on coding education and the evaluation of coding quality. The results will be summarized and presented for discussion at the Education Day session. Results: The analysis of the responses to the questionnaires will provide information on: the version of ICD-10 currently in use, the characteristics of the coding education imparted and received, the evaluation of coding quality, and knowledge of resources available to coders from WHO-IFHIMA, e.g., Core Curriculum for Morbidity Coders, ICD-10 e-learning tool. Conclusions: The discussion of the findings of the survey of coding educators and clinical coders should enrich those educators participating in the session. It could also lead to the creation of an on-line discussion group of coding educators for the exchange of information following the Congress. The identification of areas for improvement will benefit the EIC. ED3.1 The Challenges for HIM Education in Developing Countries Lorraine Nicholson International Federation of Health Information Management Associations, Rochdale, Greater Manchester, United Kingdom The objective of this session will be to describe a broad picture of HIM issues in developing countries including issues relating to HIM education and training and to provide an overview of IFHIMA's role in two areas of focus: 1. HIM education in a global perspective in the WHO regions (Africa, The Americas, Eastern Mediterranean, Europe, South East Asia and the Western Pacific) 2. The challenges for HIM training in developing countries

113
Poster Session Abstracts P1 Locating Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT®) Concepts for the Canadian Emergency Department Diagnosis Shortlist Roberta Cardiff Canadian Institute for Health Information, Toronto, ON, Canada Introduction and Objective: The Canadian Emergency Department Diagnoses Shortlist (CED-DxS) is a pick list of 837 ICD-10-CA diagnosis codes with a corresponding common term, in both English and French. For this exercise, the 837 English Common Terms from CED-DxS served as a source reference set for locating corresponding Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT®) concepts, with a goal to locate a semantic match for each. In addition, a main objective of the project was to build expertise and knowledge of SNOMED CT and the mapping process. Methods: Possible target concepts were limited to active concepts from the July 31, 2009 international release of SNOMED CT. A search using the wording of each common term was performed in the CliniClue browser. In instances where the wording of the common term could not be located in CliniClue, synonymous terms were used. Possible target concepts were evaluated based on hierarchy, meaning and defining relationships to determine an appropriate match for the common term. Once a match was identified, the Concept ID, Description ID of the Preferred Term for each was documented. In some instances a synonym of the concept was closer in wording. In these cases, the Concept ID, Description ID of the Synonym of the concept was included in addition to the Preferred Term. Results: Concepts representing the meaning of each of the source terms were located for all but 7 of the 837 Common Terms. The remaining terms were either too broad in meaning (e.g. Abnormal results function studies) for a concept to be located or required post coordination (e.g. Diffuse brain Injury + Open Wound), which was out of scope for this project. Partial validation of the matches was completed by two independent parties. This analysis identified additional parameters to incorporate into the procedure, items related to versioning that had occurred since the completion of the project and direction on how post coordination might be used to address the terms that could not be matched using one concept only. Conclusion: This exercise served as beneficial in both developing parameters for and locating SNOMED CT concepts for a list of diagnostic terms. The objective to build expertise and knowledge related to SNOMED CT and the mapping process was met and there were several lessons learned regarding concept selection and maintenance that can be applied to similar projects. Future activities related to this project would involve a thorough validation of each target concept as well as the development and implementation of a maintenance cycle to ensure all target concepts have an Active status. Specific direction regarding terms where no match is found or those requiring post coordination must also be established. P2 ROI and Breach: Reducing Your Risk in a Digital World Rita Bowen HealthPort, Alpharetta, GA, United States Introduction: Breach risks are rising. Record requests are sky-rocketing. Electronic records may expedite processing, but also present new challenges for wrongful disclosure. Attendees to this session will learn how to tighten internal workflows and technology controls to ensure compliance and prevent information breach, particularly in a digital world. Method: Each step in the ROI process will be discussed with particular focus on breach prevention. Attendees will receive take-home checklists for safer handling of ROI requests, better compliance with HIPAA rules, and enterprise-wide analysis of vulnerabilities. Results: Topics will include: •Understanding current regulations, breach penalties and their ramifications. •Identifying the costs associated with a breach. •Knowing where breaches occur in electronic environments: massive breaches and single events. •Eliminating vulnerabilities throughout the organization. •How to shore-up ROI processes and workflows to better prevent breach. Conclusion: By the end of this session, the participant will be able to:

114
•Identify potential weaknesses in technology handling and release of information processing. •Prepare and implement HIM workflow improvement protocols and utilize take home checklists for safer information handling. P3 An Effective Approach for Enhancing the Quality of Medical Records by Auditing Electronic Medical Records Hitomi Yamada ; Shigeki Kuwata Department of Medical Informatics, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan Introduction and Objectives: Adoption rate of the electronic medical records (EMR) for medical institutions, regardless of their scales, has been increasing in Japan. It is true that EMR is superior to conventional paper-based records in some aspects such as information sharing, but EMR itself is not supposed to assure the quality of medical records; Principles on medical records are to be strictly followed and be independent of the media in which the records are kept. Thus it is of great importance to qualitatively audit the records for EMRs as well as conventional records to enhance their completeness and accuracy. This study aimed to develop efficient and comprehensive audit methods for large-scale hospitals and to evaluate the effectiveness of feedback on the audit results to physicians. Methods: The target records were derived from 4,602 patients discharged between 1st of May and 31th of August in 2011 (4 months) at a national hospital with approximately 900 beds, located in a Japanese urban area. Data for analysis were extracted from EMR database of the hospital. The qualitative audit developed by the authors was composed of 49 checkpoints that were largely categorized into seven sections. For each checkpoint, evaluation was given according to the number of faults in the records: 4 pts. (no faults), 3 pts. (1), 2 pts. (2) and 1 pt. (3+) by six hospital employees including two certified health information managers. Its feedback to physicians who input the records was given thorough supervisors at each clinical department in the middle of the target period. The evaluation before the feedback was compared with that after the feedback for each section and clinical department. Results: For overall evaluation, in which the point for each section averaged, medians (M) and quartile deviations (QD) were obtained as M=2.3/QD=2.35 (N=2,064) and M=2.5/QD 2.5 (N=2,538) for the pre-feedback and post-feedback periods, respectively, corresponding to significant improvement of the quality (p<0.0001). For four out of seven audit sections and for 13 of 32 clinical departments, the points significantly increased (P<0.0001 and P<0.05, respectively). Conclusions: It was found that the feedback of the audit results was in general effective to improve the quality of EMRs. The difference among the departments was considered to depend upon whether the supervisors who received the results were able to manage their subordinate physicians: Some of them did not properly understand their roles in this audit scheme. Therefore possible measures to make the audit more effective for a wider range of physicians would be direct feedback to the physicians responsible for the records, and the subsequent educational framework for them. In addition, assistance of information technology such as e-learning would be essential to facilitate their participation and retention for the education and to save its cost. P5 Modular-phase Implementation of Electronic Health Information in Hospitals with Complete Paper Medical Record - A Success Story Francis Kirubagaran Qatar Orthopaedic Sports Medicine Hospital, Doha, Doha, Qatar Introduction and Objective: During the last decade, Information Technology has developed in a tremendous speed towards the health sector and contributed significantly to Medical Record management. Nowadays every hospital including small clinics have computers for Electronic Health Information or at least for Patient Registration and billing purposes. This modular-phase implementation is my experience of implementing Electronic Health Information System in 4 multi speciality hospitals which works with satisfaction of the concerned department and brought successful implementation. This model is feasible for hospitals in developing countries with complete paper Medical Record. Methods: Selecting modules for each phase and sequencing of phases are key factors for the successful implementation. This implementation of 30 modules in 6 phases initially took 2½ years and reduced to 1 year in the 4th implementation. Each hospital implementation has given productive experience to reduce the duration in subsequent implementation in other locations. Each module-training version was installed in user’s computers for training and improvement of the module. The training of users was carried out on one-to-one, on-site and hand-on basis by super users. Result: Every phase of implementation resulted in satisfactory outcome for involved departments in improving

115
overall functions of the department, hospital and patient care. Other department users were so motivated that they prepared the required information for the development and implementation of their module. Conclusion: Literature review explains extensively on formal detailed planning, system analysis, customization, training and user acceptance of the modules through top management. The key difference in this implementation is departmental level gain focused, which resulted in module by module satisfactory and successful implementation. A senior, renowned, well-connected and respected clinician who was enthusiastic to witness the successful implementation in the group of hospitals has led the implementation team along with 3 deputies from the department of Information Technology, Medical Records and General Medicine. The Medical Record Professional is the right person to establish the documentation systems by coordinating between technical and healthcare professionals during the transition of paper medical record to electronic medical record. The progressive process resulted in reduction of papers in maintaining medical records, with complete satisfaction of different departments. Ultimately the modular-phase implementation will lead to paperless Electronic Medical Record. P6 A Vision for a Paperless Future: The Understanding of Indonesian Medical Records Students About Electronic Medical Records Dwi Margawati ; M. Kes Rosyidah Department of Public Health, University of Ahmad Dahlan, Yogyakarta, Indonesia Introduction and Objectives: Electronic Medical Records(EMR) is still an issue in this world, especially for developing countries. Many programs in Health Services are moving towards EMR. By implementing EMR in Health services we can ascertain helpful, effective, and efficient benefits. Indonesia is a developing country with a high population and has a very big opportunity to implement EMR. Many steps should be prepared before implementing EMR. One of those steps is preparing human resources. Medical Records Students have a big role towards implementation of EMR in the future. But now, how much do the Medical Records Students understand, and how much have they studied concerning EMR? How important do they believe EMR is? Methods: In September 2012 I conducted a survey about the understanding of Indonesian Medical Records Students concerning EMR. The Data accumulated corresponded to random interviews from 150 respondents who are 2nd or 3rd year Indonesian Medical Records Students from 3 different Medical Records Institutions in Yogyakarta, Indonesia: Bhakti Setya Indonesia Health Academy, Permata Indonesia Health Academy, and the Vocational School of Gadjah Mada University. Results: The result is 20.67% of the Indonesian Medical Records Students did not know and understand the term of EMR, 74.67% only knew the term EMR, 4.67% knew and understood the term EMR, 80.44% want to know and understand EMR. Conclusions: From the research conducted, we know that Indonesian Medical Records Students are still lacking information about EMR, even from the institution itself. However, they are willing to learn in order to understand more about EMR. They responded positively to a vision of a paperless future. Knowing this, they should have a special class or course for EMR and its implementation. In relation to its importance, we know that no Indonesian hospitals implement EMR. A course, for example, a comparative study or internship in a developed country which has been implementing EMR is needed. Preparing the Indonesian Medical Records Students towards knowing and understanding EMR is the first and basic step for creating a vision for a paperless future in Indonesia. P7 Challenges and Prospects for Electronic Health Records in Nigeria Lorraine Nicholson 1; Olawole Ajayi 2 1International Federation of Health Information Management Associations, Rochdale, Greater Manchester, United Kingdom; 2Health Information Managers Association of Nigeria, Lagos, Lagos State, Nigeria Introduction and Objectives: The challenges of EHR implementation in Nigeria are identified in a study in 2011, "Towards Implementing a Nationwide Electronic Health Record System in Nigeria" , which said that WHO identified inadequate Health Information Systems as a challenge. Many developed countries have either implemented or are in the process of implementing Electronic Health Record (EHR) systems because of potential benefits. Pilot projects in developing countries are demonstrating the viability of EHR in resource constrained areas. The study shows the health system in Nigeria is pluralistic and complex with Federal, State and Local Governments, Health Related Agencies, Non-Governmental Organizations, private healthcare providers, patients, and researchers as major stakeholders. Drivers for adoption of a national EHR include the need to report data, improve patient safety, improve work place efficiency; comply with government reforms to reduce cost and
116
increase access to health services. Corruption, poor coordination among stakeholders and lack of reliable electricity supply are some of the barriers to a successful implementation. Factors considered critical to successful implementation include enforceable legislation, a trained and motivated workforce, and significant and sustainable funding. This paper identifies EHR implementation challenges and benefits in these 6 different dimensions: 1. Organisational challenges for healthcare organisations in Nigeria 2. Personal Challenges for HIMs 3. Professional Challenges for HIMs 4. Challenges for the Health Information Managers (HIMAN) as a professional association 5. Challenges of EHR Implementation in Nigeria (possible implementation problems) 6. Benefits of successful Implementation of EHR in Nigeria Methods: A paper providing a high-level overview of the challenges for healthcare organizations as they move towards EHR implementation was presented at the HIMAN national conference in Lagos, Nigeria in August 2012. It covered the transition from paper to electronic records, managing health records in a mixed economy of paper and electronic records (the hybrid record), personal and professional challenges for HIM professionals, evolving roles for HIM professionals in the electronic environment, what IFHIMA can do to help HIM's at this interesting and challenging time and what individual HIM's can do to address their professional challenges. Syndicate groups then discussed and identified the 6 dimensions of EHR implementation shown above. Results: Each group provided a structured written report and verbal feedback to inform the development of this paper. Conclusions: EHR implementation in Nigeria is still in its infancy, some hospitals such as National Hospital Abuja attained partial computerisation. Strenuous efforts are being made to ensure full implementation of EHRs but the burden of the various identified challenges still need to be dealt with effectively to ensure successful implementation. P8 Implementation/Adoption of Electronic Health Records in Developing Countries: Literature Review of its Practical Application in Nigeria Eunice Omidoyin University of Ilorin Teaching Hospital, Ilorin, Kwara State, Nigeria Introduction and Objectives: Application of Information Technology to Healthcare Industry is a major issue that has triggered a marked amount of research. Success of an e-health system is dependent on the success of Electronic Health Records (EHRs) system. The study set out to review literature on the adoption EHRs in Nigeria i.e. the status, benefits, barrier and driving factors to adoption of EHRs in Nigeria. Methodology: This study is a review article and has been conducted using library and electronic resources. The literature search was conducted with the help of Google and other search engines and also by using citation and reference tracking methods. In this study, more than 200 articles and reports were collected and about 90 of them were selected based on their relevancy. This study was not limited to any publication date. Results: It was discovered that there is low diffusion of EHRs in Nigeria. Health Records production is still largely based on citation and paper-based systems because EHRs have not been widely adopted or where adopted, have not been thoroughly implemented. Benefits of EHRs are numerous and greatly outweighs the cost of implementation which includes, • Better Decision making and more coordinated patient care • Improves quality and convenience of patient care • Increases patient participation in their care • Improves accuracy of diagnosis and health outcomes • Increases practice efficiencies and costs saving. However, corruption, poor coordination among stakeholders and lack of constant supply of electricity are some of the barriers to a successful implementation of a Nationwide EHRs in Nigeria. The drivers for adoption of a Nationwide EHRs in Nigeria includes the need to report data, improve patient safety, improve work place efficiency, comply with government reforms aimed at reducing costs and increasing access to health services. Conclusions: The study concluded that EHRs is an emerging trend in Nigeria with slow movement in adoption and implementation. Despite its numerous benefits, there are multiple risks and barriers to its adoption in Nigeria which stems from people, government, dilapidating ICT Infrastructures and its poor development. All Stakeholders to provision of quality health care service delivery (including International Healthcare Agencies) must encourage realizing the driving factors for adoption of EHRs in Nigeria.

117
P9 Impediments and Socio-Technical Factors Affecting the Adoption of Electronic Health Record Mojirola Shote 1; Yusuf Abideen 2 1Chevron Nigeria Limited, Lagos, Nigeria; 2Atlas Systems & Technology, Lagos, Nigeria Introduction and Objectives: Electronic health record system is recognized as an essential factor in the development of health care services in Nigeria. The adoption of EHR is however slow due to impending factors affecting its adoption and sustainability. Identifying the barriers and challenges will prepare health care organizations to anticipate and manage a successful implementation process. To implement a successful Electronic health system, health care institutions must be prepared to take cognitive steps to anticipate possible hindrances and manage the change process that often arise during the stage of implementation. The objective is to identify the challenges facing health information system implementation (HIMS) and to understand the socio-technical factors affecting the adoption of the technology. Methods: A Technology Acceptance model used to predict the discretionary use of information technology was developed using survey methods and case study. An online survey was distributed to 130 participants and this resulted in an average of 52% responders. The analysis of data was carefully evaluated from the researcher’s experiences and beliefs. Evident challenges affecting adoption and implementation as captured includes: unstable power supply, cost of peripherals, attitude of health care professionals, and the impact of relationship between patient and doctor. Results: Respondents believe that success will be determined by the provision of adequate technical support, sufficient training and management support. The role management is considered as a key factor in the adoption and implementation HIMS project. 52% agreed that the introduction of HIMS technology will enhance medical processes, though many were apprehensive about the sustainability of the technology. Involvement of key stakeholders such as the physicians, nurses, lab scientist, pharmacist, radiologist and other clinician were perceived to drive a successful transition and implementation. Conclusions: Most projects were observed to have been abandoned due to the inability to gain acceptance from stakeholders and members of the organizations thereby minimizing the ability to successfully benefit the potential for an effective, affordable and quality health care services. Support from information technology specialist is considered to be crucial to the sustainability of HIMS. Subject also desire, round the clock supports from the technical team. The failure of EHR has been attributed to human factors as well as resistance to change, lack of understanding of the technology, fear of the unknown and the inability to apply the technology using a constructive and methodological approach. P10 Transitioning into the EHR Julie Sternik ; Sue Rocchetti The Credit Valley and The Trillium Health Centre, Mississauga, ON, Canada Introduction and Objectives: We were running out of space to store patient records at our off-site storage facility, which was being staffed by 10 FTE’s retrieving and filing charts. It was costing the department thousands of dollars not only to store the charts off-site, but also to transport charts to and from our 2 sites. There was no option to move the storage space back to the hospital, as HIM was losing space to accommodate patient areas. We also had approximately 9000 incomplete charts. It quickly became evident that we needed to look at ways to decrease the space required, cost and still be able to deliver excellent customer service (physicians, clinicians and patients). Methods: In the spring of 2009, a contract was signed to begin scanning our patient records and using a Document Management System. We began to scan completed discharges from June 1, 2009 (day forward). It is important to note, that we were only going to scan hand written documents. We were not going to scan anything that was available in other electronic systems within our facility. We worked with a Document Management vendor to build workflows within the system that incorporated our manual processes and automated them in the application. Prior to our go-live, we arranged some in-class training classes for clinicians and Unit Clerks. The purpose for these sessions was to train the end users on the application, but also to inform them of some process changes that would impact them. Results: Having now been scanning for over 3 years, we have reached a number of milestones. Our incomplete charts have been substantially reduced. Physicians have access to complete their charts on-line anywhere in the hospital and in their offices. We now have approximately 400 outstanding charts. We have also been able to allow our coders to work from home. This has freed space within the hospital and has also increased the coders’ productivity and job satisfaction. Our turnaround times have decreased in all areas, including Transcription,

118
Quantitative Analysis, Release of Information and Coding. Clinicians have easy access to patient records and can view patients’ historical records at the bedside. We have also decreased FTE’s in the record processing area. Conclusions: The feedback we have received from the clinicians have been positive. Having access to the patient records have help them improve patient care and are able to complete their work more efficiently and effectively. P11 Global Implementation of Electronic Health Information Chandrika Thal Consultant, Ajax, ON, Canada Introduction: We can connect travellers with their connection flights globally. We can access our bank accounts globally. Why can’t we access our health information globally? A very complex information technology is used in the aviation and banking industry. In larger banks, all branches are connected via networks to the bank's "data center", where the bank’s mainframe and servers are housed. They require upgrading from time to time and new software may be installed to fit the user's needs. Also with larger banks, they usually have interconnected call centers which work together to serve the customer's needs. The banking system has the highest data integrity, security and privacy. Why don’t we apply the same technology in connecting our health information internationally? This can assist travellers in receiving better healthcare by allowing practitioners to have access to health information right at their fingertips. Method: Use a banking technology in connecting personal health information globally, such that it is readily available when one requires care, and ultimately transferring the right data to the right people instantly. In today’s electronic era, other applications already exist within government services, airports, financial systems and other markets; as a result, not having data available for even a second in these industries is considered unacceptable. Result: Use a strategic and systematic approach that supports people and their organizations in the successful transition and adoption of electronic health information. The International Federation of Health Information Management Association (IFHIMA) can play a vital role in developing a network that provides health information internationally by partnering with the World Health Organization, a representative from each country and Unisys, a global network provider who designs, builds, and manages mission-critical environments for businesses and governments. By partnering with these clients, Unisys can offer a high-volume, transaction-intensive, and secure computing to deliver the safest data with peace of mind. It can offer a new method of storage security and virtualization that allows consolidating multiple storage networks, each dedicated to a single security level or community of interest, onto a single, virtualized storage infrastructure. Conclusion: The significance of a breakthrough in the health information system is to deliver the right data to the right people at the right time at a global level. This will be the next innovation in the electronic health information era by using a safe, secure and sophisticated computer network system which is already used in the aviation and banking industry. P12 Quality of Pharmaceutical Care After the Use of E-prescribing in Grha Kedoya Hospital Lily Widjaja 1; Yuni Mujiarti 1; Veny - 1; Sis Wuryanto 2 1Esa Unggul University, Jakarta Barat, DKI, Indonesia; 2Mitra Husada School of Medical Record, Karang Anyar, Central of Java, Indonesia Introduction and Objectives: According to the Center for Medicare & Medicaid Services , electronic prescribing is "the ability to send prescriptions in an accurate, error-free and understandable way, received by the pharmacy straight from the treatment room. Grha Kedoya Hospital is a new hospital that has been operational since December 2010. Since its establishment, the patients' medical record has been handled conventionally using manual record on paper, although it has a Hospital Information System that can be used electronically. The purpose of this study was to measure the quality of electronic prescribing service by looking at medication errors done by pharmacy before and after use electronic prescribing . The two factors that were monitored were prescription waiting time and the accuracy of drug prescription. Methods: The population was taken 5554 inpatient's prescription in April 2012 for pre-electronic prescribing and 6219 in August 2012 after using electronic prescribing . Samples were taken each as much as 392 .The time is measured from the time of receipt of prescription and delivery times indicated on the prescription drug. Data for the accuracy of drug prescription were taken for pre-electronic prescribing is from January 2011 up to June 2012 and in August for after electronic prescribing. Results: This study indicate that using electronic prescribing can increase the quality of services provided by the pharmacy. The average time it took to manually prescribe inpatients is 46 minutes. This commonly included delays from delivering the needed drugs from the pharmacy to the patients' rooms. After using electronic
119
prescribing , this average time is reduced by only 25 minutes, and the mean error rate of drug delivery can be solved. There was an medication errors 10 times, after using the electronic prescribing no errors . The time to prepare the necessary drug has met the standards (<15 minutes), but the time of delivery of pharmaceutical drugs in the basement to the wards on the 6th.,7th. and 8th. floors still requires an additional 7-10 minutes. Conclusions: The use of electronic prescribing patient safety is more assured and prescription waiting time has been reduced although the time to send the drug still takes 7-10 minutes. Once enacted electronic prescribing prescriptions not found error . Our suggested solution is to installation pneumo tube (aerocom) to connect the pharmaceutical space with all wards except for liquid injectable drugs and other liquid drugs. P13 The Needs of Improvement of Graduated Health Information Management Competency Program in Indonesia Lily Widjaja 1; Laela Indawati 1; Sis Wuryanto 2 1Esa Unggul University, Jakarta Barat, DKI, Indonesia; 2Mitra Husada School of Medical Record, Karang Anyar, Central of Java, Indonesia Introduction and Objectives: Indonesia has 22 types of health personnel professions, including professionals Health Information Management .HIM professionals come from 33 HIM academies, which are distributed in 5 of Indonesia's big islands. These academies have limited number of teachers who teach core courses on HIM Competency . Because of this, it is difficult to increase the quality of the graduates of HIM Competency programs to meet the standards set by Minister of Health of the Republic of Indonesia in 2013. HIM Competency test is a process to measure competencies (knowledge,skills,attitudes) of health workers,to being in accordance with the professional standards that already exist.For this reason the "Council of Health Personnel Indonesia"was formed in 2011 to organize a competency test in Indonesia. Council of Health Personnel Indonesia Competency Test shall be carry out for those in the medical profession and the competency test certificate is given for successful test takers.This will allow them to obtain the Certificate of Registration which will be one of the requirements to obtain work permit and practicing permit for medical personnel. Methods: The HIM Competency test will be conducted for all university students in their last year of HIM program in all Indonesian academies starting from 2013. The preparation to conduct this test is done as a collaboration of the Ministry of Health, Ministry of Education, and several professional organizations such as Indonesian Medical Record and Health Information Professional Organization or PORMIKI. Results: Starting in 2012,the HIM Professionals who have graduated and worked in health care institutions, who had not have an HIM work permit, will have to register for one. This included about 5600 people who graduated from 1992 to 2012. They do not have to take the HIM Competency test, but by registering will be given an equivalent certification. This has been completed for all graduates. Conclusions: From 2012, those who have received the HIM professionals certificate of competence will be listed as a health worker and obtained the Certificate of Registration and work permit for health workers. By 2013, all personnel in HIM service facilities throughout Indonesia must have this work permit issued by the Ministry of Health. P14 The Experience of ICD Utilization on Verbal Autopsy Data to Obtain Trend of Cause of Death in Indonesian Population (1992-2007) Sarimawar Djaja National Institute Haelth Research and Development, Ministry of Health, Jakarta, DKI Jakarta, Indonesia Introduction and Objective: Cause of death data is necessary for arranging health programs. The needs of these data is not fulfill yet through reporting and recording system from health facilities, and national health survei should be conducted regularly. From the data which collected for several years we might obtain cause of death trends in the populations. Methods: Material taken from Nasional Health Survey 1992, 1995, 2001, 2007 covering 56,900 households, 65,664 household, 206,240 household, 211,168 household, 258,366 household based on stratified random sampling technique. National Health Survey sample in 1992, 1995, 2001, 2007 using a Socio Economic National Survey. We used the core and or module sample that taken with a Probability Proportional to Size. Cause of death data was collected by structured questionnaire using verbal autopsy technique and was classified based on ICD 9 and ICD 10. Results: From the verbal autopsy data collection in each survey obtained disease patterns of cause of death from 1992 to 2007. In Indonesia, the non-communicable diseases are likely to increase and communicable diseases (infectious, maternal, perinatal, nutritional deficiencies) decrease. Reduction burden of disease is focused on

120
communicable disease (infectious, maternal-perinatal, nutritional deficiencies) and non-communicable disease. Non-communicable diseases to be prevented and treated properly is endocrine disease, diseases of the circulatory system (heart and blood vessels including stroke), and neoplasm. Conclusions: Cause of death which determined from verbal autopsy data and classified based on ICD can produce cause of death statistic that are useful for planning health programme in Indonesia. P15 Role of International Federation of Health Records Organizations (IFHRO) in the Evolution of Medical Records in India Goverdhan Mogli Dr. Mogli Health Care Management Consultancy, Secunderabad, Andhra Pradesh, India Introduction: India had a glorious period with ample evidence exists to substantiate the flourishing of medical practice many centuries before the birth of Christ. Throughout the millennia, medical records evolved in conjunction with the advances in the art and science of medicine. The successive invasions of India declined the indigenous system of medicine and the post independent medical records status was poor. The Government of India established Central Bureau of Health Intelligence (CBHI) in 1961 after the recommendation of Dr. Mc Gibony, American Expert, and the importance of medical record departments that initiated first medical record training program in 1962. The author enlightens the striking variation of medical records status in India during the period as a member of IFHRO from 1976-1984 and the outcome not being member till date. Methods: The Indian Association of Health Records (IAHR) was formed in 1972, affiliated to IFHRO in 1976 with 67 registered members. The CBHI conducted series of workshops on ICD 9th Revision at selected regions and deputed MR personnel to developed countries during the period 1978-1984. On IFHRO efforts, an International Workshop for Medical Records Teachers was conducted in India in 1979. The IAHR conducted conferences in 1977 and 1980 more than 120 and 150 members participated respectively. The IAHR was active member of IFHRO unto 1984. As Dr. Mogli; the founder of the association and other seniors left the country; the IAHR ceased functioning, thus not represented in the IFHRO conferences since then. Nevertheless, Dr. Mogli participated in the IFHRO congress as a Director of IAHR from 1976-1984, and rest of the congress as an Associate member uninterruptedly. India experienced professional lull for 17 years from 1985-2001. Only after three day conference held in Chennai under the guidance of Dr. G.D. Mogli, Sr. Consultant, MOH of Oman, and the Tamilnadu formed association and started conducing annual conferences. Results: As a member of IFHRO (1976 to 1984) -India participated in many IFHRO meetings. -IAHRO efforts with government for MR. -Provided facilities for growth of MRD. -Enhanced MR training centers. -State associations with national object. -Conferences involving IFHRO members. -Involved policy makers in MR field. Not a member of IFHRO (1984-todate). -Not a single time after 1984. -No guidance from association to government. -Lack of facilities for development of MR. -Weaken number of training centers. -Few state associations with individual object. -No relation with IFHRO- participation. -No efforts made with policy makers. Conclusions: It is quite evident that nations can benefit tremendously being a member of IFHRO; and can contribute efficiently to fulfill the national healthcare delivery goal. P16 Use of LEAN Methodology to Improve Hospital Patient Records Utilization by Staff and Researchers at a Rehabilitation Hospital Vijitha Anton Mariathas ; Marie Disotto-Monastero St. John's Rehab Program at Sunnybrook Health Sciences Centre, Toronto, ON, Canada Introduction: St. John’s Rehab program at Sunnybrook Health Sciences Centre used Lean methodology to improve access to patient records by hospital staff and researchers to facilitate timely delivery of Patient Records

121
by Health Information Services (HIS) department. To retrieve 7,400 paper-based patient records per year is challenging, as this number increases by 5% annually and process improvement was the solution. Methods: The LEAN methodology was used. The standard Kaizen concept was followed to map the process: 1. Continuous Improvement a. CHALLENGE: communicate targets, meet targets using courage and creativity. b. KAIZEN: improve operations continually; focus on baby steps, not big changes. c. GENCHI GENBUTSU: go to the source to find facts, spend time at where the work is done. 2. Respect for People a. RESPECT: understand each other, take responsibility and build mutual trust. b. TEAMWORK: maximize individual and team performance, share opportunities for development. 3. Value Stream Mapping a. Flow of information and materials to identify, eliminate waste and to improve processes. A Kaizen Charter was defined and a two-day Kaizen event was conducted with the Health Information Services department to map both the current and ideal Patient Records Management process. Results Prior to the LEAN initiative there were: 1. Lack of systematic tracking to manage the inventory of patient records; 2. No formal policy and procedure to request patient records; 3. Minimal accountability to access and return patient records; and 4. No statistical data on requests of patient records. The Kaizen event produced the following results: 1. Development of patient health records management process map 2. Development of roles and responsibilities of staff 3. Development of various tools: - Patient Health Records “Tracker” based on Excel - Patient Health Records Requisition Policy & Procedure - Patient Health Records Requisition Form One year post-implementation data analysis showed that on average the HIS Department retrieves 162 patient record requests per month and can articulate volumes of requests by various departments. Conclusions: The Health Information Services department of St. John’s Rehab program at Sunnybrook Health Sciences Centre now supports patient care and research through the timely retrieval of paper based patient records. The volumes of requests received from various departments are articulated. Impact on quality of care has improved as clinical and non-clinical staffs receive patient records within 24 hours of initial request. Staff resources are now allocated efficiently. A Lean process was successfully implemented with no investment towards purchasing an electronic system or hiring additional staff.

122
P17 Training Need Assesment for Medical Record and Health Information in Harapan Kita - Women's and Children's Hospital, Jakarta-Indonesia Elise Garmelia HIM Manager, West Jakarta, DKI Jakarta, Indonesia Background: Harapan Kita Women’s and Children’s Hospital (CMH) is a government hospital the location in Jakarta the Capital city of Indonesia. CMH have 327 beds capacity. Department of Medical Record have been change to be Health Information Management Department on 2012. The system of medical record are manually, but we have computerized system to manage the data. The HIM department have 43 government employee with the 8 vocational degree and 31 highs school plus

123
(having a training of medical record management) and 2 staff other bachelor. To improve the skill and knowledge of the employee needed to know, what they need to train. So we have make a program training need assessment for staff. Method: The questioner distributed to 43 staff in HIM department. The content of questioner are as follow : 1. Motivation, 2. Behaviour, 3. Competence, 4. Knowledge. Collecting data and analyst by SPSS. Result: 100 % staff fill in this questioner, 4 % not satisfied about they job,12 % not loyality with they job. All staff are know about they role or job description but only 8,6 % staff do not know about competence of HIM profession. Conclusion: Training Need assessment should be done continuing in department. The goals are we know about training to improve the HIM services. P18 Analysis of Computerized Physicians Order Entry System Data of Inpatients with Diabetes as a Complication to Improve Intervention Ryoma Seto 1; Akemi Nishio 1; Tomoki Nakano 2; Aizan Hirai 3 1Division of Healthcare Informatics, Faculty of Healthcare, Tokyo Healthcare University, Setagaya, Tokyo, Japan; 2Department of Endocrinology and Diabetes, JMA Higashi Saitama General Hospital, Saitama, Japan; 3Chiba Prefectural Togane Hospital, Chiba, Japan Introduction and Objectives: The number of patients with diabetes is increasing rapidly, and some patients require microangiopathy (e.g., patients with CKD) and/or macroangiopathy (e.g., patients with AMI). Patients with type 2 diabetes, however, often do not manage their disease well and their condition may worsen. Therefore, disease management for patients with diabetes is very important to improve the quality of care and reduce medical costs. Currently, the development of easy methods of disease management for physicians, pharmacists, nurses, and data managers is required1)-3). The purpose of this study was to develop and evaluate a screening method for patients requiring disease management. Methods: Data collection was performed at three Tokyo hospitals for patients treated in June 2009. Data were collected from two types of patients: A) inpatients who had been registered in the computerized physicians order entry (CPOE) system as having diabetes as a complication to other primary disease and were surveyed about the type of diabetes care that was provided, e.g., self-measurement of blood sugar (SMBG); B) inpatients who were actually receiving diabetes care and were surveyed about the type of disease they had been registered as having by their physicians. Results: Type A data could only be collected and analyzed from one of the three hospitals (75 patients) because the other two only recorded whether the patient was registered as having diabetes as the primary disease. Hospital data analyses showed that the type of diabetes care given to the patient (e.g., SMBG or insulin prescription) was ignored in about 70% patients by some of the non-diabetes units (e.g., ophthalmology). Type B data could be collected and analyzed from all three hospitals because data regarding medical procedures and/or nursing care ordered in the CPOE were recorded; 130 patients were surveyed. The percentage of inpatients who had diabetes recorded �gas complications� in all diabetes patients were 55--92% in the three hospitals. The main diseases for these patients were carcinoma, stroke, and pneumonia. Conclusions: These results showed that diabetes was frequently present in patients registered as having other primary diseases, although some of the diseases were caused by diabetes. In addition, some patients registered as having other diseases with diabetes as a complication sometimes ignored the care given to treat diabetes. As a result, two issues were observed. First, is a clinical issue of non-diabetes hospital units that do not consider the care given for diabetes as a complication in the other types of care they provide and the other is a data management issue of hospitals that do not register diabetes as a complication. In conclusion, it was practically verified that the data entered into the CPOE are very effective in supporting disease management for diabetes. Acknowledgment: This work was supported by JSPS KAKENHI Grant Number 24790628. P19 Leveraging HIM Skills to Optimize the Use of Data Across the Spectrum of Health Care Donna Boyd Alberta Perinatal Health Program, Edmonton, AB, Canada Introduction and Objectives: The traditional role of Health Information Management professionals (HIMs) has been in health care facilities--collecting, coding and analyzing clinical information. Exciting roles exist in today's health care system for HIMs to apply their expertise to inform clinical practice, program planning, executive decision-making and health ministries. The objective of this presentation is to demonstrate how HIM skills are used - beyond traditional roles in health records departments - to transform data into information for use across the

124
spectrum of health care. Methods: In the 21st century, organizations are increasingly complex and inter-related, depending more on reliable data to support decision-making and program planning. The traditional roles of coding, abstracting and analyzing CIHI data has set HIMs up for success in non-traditional roles. HIMs offer a unique and desired perspective in contrast to conventional information systems (IS) data analysts in the data analyst role outside of health records departments. HIMs: •are familiar with terminology, best practice, clinical significance and data usage that are not necessarily inherent in the IS analyst role. •are detail-oriented, promote accuracy and a standardized approach to data collection •understand the context of data and offer ideas of how data can be used to promote problem-solving or solutions Examples of non-traditional places of work are: •government out-patient mental health clinic •Workers' Compensation Board •Regional Quality Office •Alberta Perinatal Health Program In these positions HIM skills and privacy expertise apply directly to local data collection and identity verification, validation, extraction and reporting within a specific clinical area. Experience is gained in: •ascertainment of eligible patient events •liaison with data providers (including CIHI and health records department contacts, and Health and Justice Ministry personnel) •building databases and data collection tools •working with consultants as a data expert for large projects •regional and provincial exposure and participation in planning for clinical and outcome related data collection Results: The core business goal of HIMs is to collaborate with stakeholders to define, collect, validate, maintain, analyze and report data. This work can be found anywhere in health care where data is used to inform the practice of health professionals, clinical decision-makers, executives and health ministries. Conclusions: HIMs are poised to offer valuable skills that support information management and research, leadership, quality improvement/quality assurance, education and practice support. For the HIM, a broader perspective is gained by utilizing varied and new skills in a clinical or focused area. P20 The Role of Health Informatics Professionals Within Addiction Agencies in the Health Care System Alison Zwaagstra ; Patryk Simon ; Shaun Black Addiction Prevention and Treatment Services, Capital District Health Authority, Dartmouth, NS, Canada Introduction and Objectives: Historically, addiction agencies did not see information management as a priority and reports mainly focused on client characteristics and activity volumes (Rush et al., 2012). Due to the increasing need for accountability, mechanisms are required to evaluate and monitor the effectiveness of services being provided. Addiction agencies, not unlike any other services in the health care system, require the expertise of health informatics professionals to ensure clinical and administrative data is used to inform and improve the decision-making process. The experiences of two health informatics professionals involved with establishing the health information needs and priorities at one addiction agency over the past three years are shared. Methods: Initial discussions in 2010 involved obtaining feedback from leaders and frontline staff to determine the types of reports required to evaluate the clinical effectiveness of the service delivery model. A data quality framework was implemented to ensure all data was regularly checked systematically and to inform staff on the importance of having high quality data. An extensive review of the information management and information technology framework at the agency was completed in 2012. The literature was appraised and synthesized to identify evidence-based performance indicators and outcome monitoring approaches specifically for addiction agencies. Results: Leaders and frontline staff now place more value on data collection and have a better understanding of the need for high quality data to support decision-making. Reports shared on a quarterly basis with all staff help stimulate quality improvement discussions. The review of the provincial administrative database identified significant gaps including a lack of standardized classification systems and that health information standards to facilitate the exchange of messages between multiple systems were not being followed. Recommendations to address concerns surrounding clinical documentation, data quality, privacy and reporting were also brought forward to the agency’s leadership team. Unfortunately, due to financial and other barriers, it will take time for these issues to be resolved and the benefits realized. Conclusions: Health informatics professionals were enthusiastically welcomed at an addiction agency that had never employed staff with expertise in this area. The role of health informatics professionals at addiction agencies is becoming increasingly important to advocate for the adoption of eHealth solutions that will ensure information
125
is readily available to support the delivery of the highest quality addiction treatment to clients, families and communities harmfully involved with alcohol, other drugs and/or gambling. P21 HIM in 2016: Guiding Principles for Enterprise Information Management and Governance Linda Kloss 1; Jeffry Levitt 2 1Kloss Strategic Advisors, Chicago, IL, United States; 2Precyse Solutions, LLC, Wayne, PA, United States Introduction and Objectives: The scope of Health information management (HIM) is expanding beyond the organizational boundaries to the continuum of care. It is also expanding from core patient health records to other types of health care data and information, personally identifiable and aggregate. This expanded scope of practice requires new models of practice, new guiding principles and practice innovation. Objectives of this session are to: -Take a journey to HIM practice in 2016 and examine how health system changes and technology are reshaping traditional HIM practices. - Review guiding principles and how they may be used to assess current practice and set priorities. -To outline next goals for the HIM Community as it prepares for transformations in practice. Methods: In this poster session, participants examine the work of an informal HIM Innovation Community that has been meeting to advance thought leadership in shaping the HIM functions and services of the future. Members of this Community are HIM directors at leading health care organizations across the US. This work has produced a set of key trends shaping the future of HIM and a working model for enterprise information management. The Community also prepared scenario stories about HIM practice in 2016 and recently completed work on a set of guiding principles for each of the key building blocks for future Health Information Management and Governance. Precyse Solutions, LLC has supported the work of the HIM Innovation Community. Results: This poster presentation highlights the HIM Innovation Community’s journey of learning. Specifically it illustrates a) the trends impacting how HIM is does its work b) scenario stories of HIM practice in 2016 c) a model for enterprise information management (EIM), and d) a set of guiding principles for each building block of the EIM model. The Community’s work is reported in two white papers and these too will be made available to participants. Conclusions: Health information management professionals should advance the vision and benefits of improving the management and governance of information assets and convene the stakeholders needed to shape sound policies and practices. This poster presentation highlights the ongoing work of a group of experienced HIM leaders across the US. This work is intended to proactively shape and inform the future rather than be shaped by it. P22 Reporting Drug Resistant Microorganisms Infections and Carriers Neomi Goshen ; Yonit Sonego ; Tali Avraham ; Nava Teitler ; Tuvia Tiosano Emek Medical Center, Afula, Israel Introduction and Objectives: Drug resistant microorganisms (DRM) are found in most general hospitals. Some of these microorganisms are “permanent residents” and can harm patients and even endanger their lives. The detection and identification of patients carrying DRM early in their hospitalization is vital in order to ensure that they are isolated and cared for using strict practices of infection control. This study concentrates on early detection through documentation in hospital patients records. Part of the problem in identifying these patients was the inadequate documentation of patients known to be carriers of DRM from previous hospitalizations. If these patients were readmitted they were not being immediately identified as a potential “risk” and the required infection control procedures were not implemented there-by increasing the risk of cross infection of other patients and the spread of infection within the hospital. The objective was to improve the documentation of DRM in patient records thereby enabling the medical team to take the necessary precautions immediately upon the patient's admission and also to achieve full compliance with the Israeli Ministry of Health and the WHO requirements for coding diagnosis of DRM. A table was developed show the abbreviations commonly used by doctors alongside the proper terms and codes used by the WHO which was distributed to doctors to enable easy identification of the proper diagnosis, for example MRSA instead of Methicillin Resistant Staphylococcal Aureus. Methods: The microbiology laboratory reports all hospitalized patients with a positive result for DRM.The medical records of these patients are inspected with the assistance of the infection control coordinator. If not documented the relevant doctor is contacted and asked to correct the documentation. The records are inspected close to the patients release when the chances of implementing the process are higher. Results: Hospital wide there was a rise in the number of cases of DRM accurately documented by the doctors in the medical record from 34% at the beginning of 2009 to 45% in 2010, 64% in 2011, and 67% in the first quarter

126
of 2012. Conclusions: Full reporting of DRM was ultimately achieved through cross checking positive laboratory results of DRM with the relevant patient’s medical record. The data was chosen as a quality indicator for the departments and results are reported quarterly to hospital leadership. The early identification of these patients prevents cross infection. Accurate documentation plays an important part in the identification of these patients. Multi- disciplinary cooperation increased knowledge and awareness, the coding team learnt to identify cases from the microbiology reports and the medical teams learnt the importance of accurate documentation of DRM. P23 "small changes, BIG GAINS" Use of LEAN Methodology to Improve Completion of National Rehabilitation Reporting System (NRS) Assessments by Clinicians at a Rehabilitation Hospital Grace Liu St. John's Rehab Hospital, Toronto, ON, Canada Introduction and Objectives: Our rehabilitation facility submits over 5000 admission and discharge National Rehabilitation Reporting System (NRS) records to the Canadian Institute for Health Information annually. The purpose is to develop and implement an effective process for the completion of NRS admission assessments by clinicians. The NRS is completed by over 200 clinicians (Nurses, Physiotherapists, Occupational Therapists, and Speech Language Pathologists) and Health Information Professionals. Since the NRS admission assessments have an impact on funding of the hospital, completion of the NRS became a quality indicator on the Hospital’s Quality Dashboard. The target goal is to complete 75% of admission assessments within 72 hours of admission. Methods: Using the LEAN Methodology, a new process improvement strategy was implemented to improve data quality for the completion of NRS admission assessments by clinicians in Fiscal 2011-2012. The NRS Implementation Team was formed to train clinical staff to enter the NRS assessments directly on the new software application system. The Team held a Mini Kaizen event to improve the data quality for completion of the NRS. During the Mini Kaizen event, the Team mapped out a new process: 1) Introduce GREEN DOTS and BLUE STARS on the Patient Scheduling Board to remind clinicians to complete admission and discharge assessments. 2) The Admission must be completed before the discharge assessment, so all the clinicians must complete their sections on a timely basis. 3) The accountability for completing assessments is removed from Health Information Services staff to the clinicians and managers on the units. Results: Prior to the new process, the rate of completion was 36% hospital-wide (Q1-F2011/2012). After implementation, the rate increased to 75% hospital-wide (Q4-F2011/12). Time spent by Health Information Services staff tracking incomplete admission assessments decreased from 45 minutes to 15 minutes per day. Conclusions: As of March/2012, we have successfully implemented this new improvement process strategy hospital-wide. After implementation, the hospital was able to meet the target of 75% completion rate on the NRS without additional investment cost. In fact, there was a decrease in time spent by Health Information Services staff, which improved operational efficiency. Using LEAN Methodology, this process improvement strategy was effective and emphasized teamwork, ownership and empowered clinicians to be accountable. This strategy cultivated best practice emphasizing accuracy of data, timeliness and quality. In conclusion, these small changes made BIG GAINS, which has an impact on the Hospital’s quality and operational efficiency. P24 Health Related Problems, 10th Revision, Canada (ICD-10-CA), and the Canadian Classifications of Health Interventions (CCI) to Inform Future Directions Karen Carvell Canadian Institute for Health Information, Montreal, QC, Canada Introduction and Objectives: The ICD-10-CA and CCI were implemented by the Canadian Institute for Health Information for use in Canada in 2001. Ten years of experience with the use and maintenance of these classifications offers an opportunity to explore the effectiveness, efficiencies, utility and future directions, and the data collection requirements for data analyses, reporting. The objectives of the assessment project are to examine the uses of ICD-10-CA and CCI data to determine the level of specificity required for different use cases and assess the implications of reporting varying levels of specificity from these classifications. Methods: Phase one of the project, initiated in 2012, included data analyses to determine the frequency of ICD-

127
10-CA and CCI codes reported to the Canadian Institute for Health Information data holdings. Surveys were developed and conducted to obtain feedback from internal users of these data for various analytical products and services such as eReporting, pan Canadian performance indicators and health reports. External clients in healthcare facilities, regional health authorities, and ministries of health will be consulted as part in phase 2 of the project. Results: A report on phase one will be completed November 30th, 2012 and will include key findings and observations from the data analyses and internal client survey responses. Recommendations will provide direction to support decision making and short and long term priority setting. Recommendations will address the level of detail required from the classifications specific to acute inpatient, emergency department, ambulatory care and day surgery coding as well as nonacute care coding. A feasibility analysis will be undertaken for each recommendation to determine implementation requirements and impact to external clients and the Canadian Institute for Health Information products. Conclusions: A significant amount of resources are required to update, revise, and maintain ICD-10-CA and CCI. As well, a heavy resource burden exists among Health Information Management, coding professionals to collect coded clinical data. The Canadian Institute for Health Information will seek ways to streamline its own internal processes in the updating, revising and maintaining the classifications, and adapt data collection and reporting requirements to enhance efficiency while meeting varying health information needs. P25 A Multifaceted Approach to Resolving Clinical Coding Data Quality Issues Denise Cullen Canadian Institute for Health Information, Ottawa, ON, Canada Introduction and Objectives: Data quality is intrinsic to the Canadian Institute for Health Information’s (CIHI) mandate to inform public policy, support health care management and build public awareness about the factors that affect health. The Clinical Administrative Databases (CAD), Classifications, Data Quality (DQ) Collaboration Working Group (CCDQC) exists to support continuous quality improvement by sharing data quality results related to coded data as identified by stakeholders, and make recommendations for follow-up action as needed. This group uses a multifaceted approach to resolving these DQ issues. Methods: The CCDQC was implemented in 2009 to encourage CIHI program areas to work together to track topics of interest. Once a data quality issue is identified and investigated, an approach to resolve it is discussed and implemented. This may be a single or multiple method approach. The complexity, relevance and volume of each issue dictate the specific method(s) required. Methods used are client follow-up, a Tip for Coders, the DQ Technical Specifications Document, enhancements to the classifications, amendments to the Canadian Coding Standards, education, and edits. For instance, an edit will completely disallow a particular error to be made if the issue is straightforward and requires direct action or, if more complex, education or a new coding standard may be the preferred approach. Each data quality issue is subsequently monitored to assess effectiveness of actions taken. Results: Many topics have been brought to the working group. Collaboration has improved communications within CIHI. Several issues have been improved or even resolved. One area of interest already reviewed by the team is diagnosis type assignment to palliative care codes. Notable errors were easily rectified with amendments to the Canadian Coding Standards and edits put in place to ensure complete compliance. Coding practices associated with coronary angioplasty, being a more ‘complicated’ issue, required enhancements to the classification, the Canadian Coding Standards and education as well as addition to the DQ Technical Specifications Document and edits where possible. One noted key success of this process was finding a previously unknown DQ issue involving a specific facility which was contacted directly facilitating changes to data for the 2010-2011 fiscal year. Conclusions: The CCDQC working group fosters communication between departments within CIHI with a goal to improve the quality of our coded data. Use of a multifaceted approach to improving data quality provides those involved in data capture, as well as CIHI, different ‘tools’ to improve overall understanding of issues or to correct suspect data. Continuous monitoring by CCDQC allows CIHI staff to work together to correct open year data, monitor coding compliance and ensure higher quality within our databases. P27 Quality Measures Reporting in the US: A Case Study of Meaningful Use in Rural Hospitals Trina Lower 1; Ryan Sandefer 2; Brooke Palkie 2 1Mercy Hospital, Moose Lake, MN, United States; 2The College of St. Scholastica, Duluth, MN, United States Introduction and Objectives: The Health Information Technology for Economic and Clinical Health (HITECH) provision of the American Recovery and Reinvestment Act of 2009 provides incentive payments to eligible professionals and eligible hospitals to adopt, implement, upgrade or demonstrate “meaningful use” (MU) of

128
certified Electronic Health Record (EHR) technology. The College of St. Scholastica (CSS) collaborated with five rural hospitals and their HIT support center to develop best practices on electronic capture and direct reporting of clinical data from each hospital’s EHR system. The objective was to standardize collection of clinical quality data among critical access hospitals that use the same EHR platform, by using data captured in the EHR; standardize collection of clinical data, ease capture, reporting and analysis of clinical quality; and provide data to clinicians. Methods: Needs assessment was used to collect data on rural-specific challenges, and approaches to quality reporting. Five quality measures were selected for reporting directly out of each EHR. Documentation of current state was completed, utilizing a tool identifying data sources for each quality measure along with the EHR vendor’s documentation. Standardization workshops were held to facilitate collaboration on data collection processes across sites. Results: Rural hospitals face challenges specific to their locations as well as the same technical barriers as other hospitals. Data required for quality reporting reside in the EHR, it is commonly not captured as structured data/standardized format. To meet MU requirements, hospitals must construct a healthcare data infrastructure within their EHR systems which must assure capture of standardized and structured data specifically needed to report quality measures. Technical barriers exist including lack of: standardized data sets, e-measures and formats; relationship between data for quality measurement and data captured/built in clinical documentation templates; adherence to clinical guidelines; and standards for software, process, terminology, and data are in their infancy. Conclusion: The findings indicate successful capture, calculation, and reporting of MU quality measures from the EHR is difficult, particularly for rural hospitals. Despite working from a common EHR system, variations exist in what data is collected, by whom, when and in what format. Complete standardization of data capture proved elusive, the interdisciplinary process encouraged standardization at the level of data element definitions, capture of data as a product of an efficient clinical workflow, eased the difficulty of building the reporting modules, and promoted useful interdisciplinary and interfacility collaboration. Participating hospitals have implemented workflows based on workflow documentation created during the workshops, and built the data infrastructure needed to collect data and all hospitals have successfully attested to MU. P29 Electronic Health Record Systems and Medication Errors: A Study of the Indian Health Service (IHS) System. Godwin Odia U.S.Public Health Service, Baltimore, MD, United States Introduction and Objectives: There are over 7,000 deaths every year due to medication errors. Medication errors on average increase hospital stays by nearly 5 days at an excess cost of $5,000.00 per incident. Implementation of electronic health (EHR) record is being done by most health care organizations in the United States. Is EHR alone the solution to medication error reduction? Are there other factors that may help reduce medication errors? Are new factors that could potentially increase errors being introduced to health care system as result of EHR? Indian Health Service (IHS) needs to understand the impact of EHR in order to increase patient safety. Methods: Nineteen facilities (n =19) were selected in two Indian Health Service regions. Seven facilities in the west and twelve facilities in the Midwestern part of the United States were selected. The source of data for this study were Medmarx and Webcidents report from these facilities were using the core elements of EHR system for at least two years' time frame for which data were available. Data reviewed were pre and post implementation of EHR. Data collection was limited to self-reported errors documented in the error reporting systems used by each facility. Results: We notice the number of errors dropping in the first year post implementation and then rising, went up the second year and then rose the third year. The increase in errors observed in the post implementation is not unusual since EHR implementation was still in its early years and more data will be needed for several more years to comprehensively compare it to pre-implementation years. Although the errors did not conclusively show reduction in the study, possibility exist that it will eventually reduce errors as the system becomes fully implemented and all users are fully trained with additional of more decision support system. When reviewed individually by area the apparent lack of significant differences in medication errors in this study is supported by other studies by King, WJ., et al., 2003 and Gandhi, TK, et al 2005 which found no differences in error rates in two different studies post implementation of EHR systems. Despite this variability in the findings after EHR implementations, EHR has and will continue to provide medication error reductions post implementation of the system across health care.

129
P30 Family Attitudes Toward a Personal Health Record (PHR) in a Long Term Care Facility Pria Nippak ; Winston Isaac ; Alice Geersten Ryerson University, Toronto, ON, Canada Introductions and Objectives: In response to increasing consumer demand for access to one's own health information, there has been greater focus on the development of personal health records (PHRs) and patient portals that help to facilitate the sharing of information found in electronic health record (EHR) systems. While PHRs have been implemented in a variety of acute care and outpatient settings, less is known about how useful they might be to families of residents in a long term care setting. The focus of this study was to identify and prioritize the types of information that family members would like to have access to through a PHR in a 472 bed long term care facility, if made available to them, and any related concerns. Methods: An online survey comprised of 5 questions about MyChart, a PHR developed by Sunnybrook Hospital in Toronto, Ontario, was sent to 188 family members. Information was collected on the level of interest in MyChart, the types of information families would most like access to from the institution's EHR, how they anticipate a PHR would help them and any related concerns. Results: Interest was very high with 74% of respondents stating that having such access was very important or extremely important to them. The top four kinds of information respondents most desired access to were similar to findings reported in other settings. In particular, test results, doctor's notes, summary notes of clinic visits and the nursing care plan were rated highest, in that order. However, the results also demonstrated that families preferred to receive comprehensive information rather than select elements from the health record. With respect to how families perceived a PHR would be helpful to them, most responses fell into three categories. Individuals described how they felt a PHR would help to facilitate access to information or make it more readily available (66%), it would help them feel more informed or aware (68%) of their loved one's health status and allow them to be more effective partners in care, and finally, it would help to reassure (23%) them that their loved one is receiving the care they expect. With respect to any concerns related to MyChart, the vast majority (68%) stated they had no concerns; however a small percentage (30%) did express concerns related to security or confidentiality of private health information. Conclusions: Recommendations based on these findings included suggestions to make any information provided through MyChart as meaningful and as comprehensive as possible and to continue to include family members in the development process to help maximize the chances that families will ultimately benefit from this technology. P31 A Study of Knowledge and Attitudes of Doctors Towards Health Information Management at National Hospital Abuja Nigeria Rasaq Adio National Hospital Abuja, Abuja, FCT, Nigeria Background: Health information management is crucial in evidence based medical practice, clinical judgment, treatment planning, monitoring and evaluation. It is equally an essential tool being used during planning and implementation of health programs. Health Information as a determinant of good service delivery, it is important to study the knowledge and attitudes of doctors who are major creators of information so as to be able to use the outcome for the improvement of health information that will be henceforth generated in our health institutions. Objectives: The objective of this study is to assess the knowledge and attitudes of Doctors towards Health Information Management at National Hospital Abuja. Methods: The method used for the study is self-structured questionnaire that probed into the knowledge and attitudes of Doctors towards health information management which were administered to a randomly selected group of 100 doctors. Descriptive statistics on their knowledge and attitudes patterns were calculated, analyzed and discussed. Results: The demographic result showed that 41.7% of the respondents are males while 58.3% are females and that majority of the respondents (47.2%) belonged to age group 31-40 years. The analysis of the professional status revealed that majority (52.8%) of the respondents are Registrars while the least respondents (8.3%) are Medical Consultants. Discussion: The outcome of the study showed that majority (43.1%) of the respondents have good knowledge, 27.8% have very good knowledge, 15.3% have fair knowledge while 2.8% have poor knowledge towards health information management at National Hospitals Abuja. It was also discovered that 70.8% of the respondents have good attitudes, 27.8% have fair attitudes while 1.4% of the respondents have poor attitudes towards health information management in National Hospital Abuja. Conclusion: The fact that this study revealed that significant percentage of Doctors did not have good knowledge

130
and attitudes towards health information management suggests that they need more knowledge and change of attitude towards health information management. P32 Beyond the RAC: New Methods to Mitigate Audit Risk in 2013 Lori Brocato ; Merritt Beaver HealthPort, Alpharetta, GA, United States Introduction: This session examines new tips and advice on how to prepare strategic, proactive and preventive protocols for all types of audits in 2013. Through these best-of-the-best audit tactics, HIM professionals will discover innovative methods to beat the auditors; not just the RACs. Methods: Because new audit initiatives and programs are introduced seemingly every day, this session also shares year-to-date information on nationwide auditor activity. Patterns and trends across a number of HIM sites will be discussed as predictors for the year ahead. Results: • Establishing HIM best practices for audit appeals and prevention • Benefitting from audit data • Current trends and predictions Conclusion: By the end of this session, the participant will be able to: • Achieve the best possible RAC and other audit outcomes • Identify areas of weakness and opportunity regarding audits conducted thus far in 2013 P33 Clinical Program Scorecard Development: Famework, Processes and Partnerships for Improved Information Desa Marin ; Diamond Watson-Hill ; Mohan Ariyath William Osler Health System, Brampton, ON, Canada Introduction and Objectives: Performance reporting at a clinical program level with specific focus on target achievement is an essential step for patient safety and quality monitoring within a healthcare organization, and important to allow relevant reporting to the Board level. At William Osler Health System, clinical program scorecards are reported in a business intelligence environment with clear linkages to established corporate priorities. With a need to improve timeliness, standardization and transparency of reported information, scorecards transitioned from manually updated documents reported in spreadsheet format to partially automated scorecards reported in a business intelligence environment. Methods: Corporate level performance priorities were defined and aligned to quality improvement process indicators, hospital service accountability agreements, and other organization-specific priorities. These priorities were to be measured, where applicable, at a clinical program level and in addition, clinical programs were to track performance on program-specific measures. Stakeholders including Clinical Programs, Decision Support, other data contributors, and the Business Intelligence team worked together to ensure automated program scorecards delivered relevant and accurate information. Key activities included consistent communication to clinical programs to ensure common reporting standards, communication of stakeholder roles and responsibilities related to data stewardship and data quality, clearly defined and documented metrics (calculations, definitions), and examination of baseline performance in relation to setting annual targets. Results: William Osler Health System has twenty-one program level scorecards available in its business intelligence tool reporting performance for inpatient, outpatient and key clinical service areas as of July 2012. The uptake and monitoring of scorecards has increased since automation due to improved timeliness of scorecard updates (monthly), clearer linkages to corporate level priorities, transparency of reported information across programs. Improved supporting information for metrics by way of up-to-date documentation was realized due to the definition of data ownership across stakeholders. The ‘commenting’ function within the business intelligence tool is under investigation and is expected to increase uptake by being the main communication tool used among clinical areas to provide addition information on reported results. A documentation project is underway to support the automation of indicator calculations, with an expected outcome of efficiencies in the existing monthly reporting processes. Conclusions: Program scorecard reporting in a business intelligence environment resulted in timely and transparent performance reporting across William Osler Health System and will enable continued development of an accountability framework.

131
P35 The Unleashed Vocational School Reloaded. Striking a New Path in the Vocational Training of H.I.M. in an Academic Landscape Ulrich Wirth University Medical Center of the Johannes Gutenberg University Mainz, Mainz, Germany Introduction and Objectives: The concept of the "unleashed vocational school" goes to the next round. Back in 2010 at IFHIMA's 17th Congress in Milan, the author presented the so-called "unleashed university", a well-known but controversial concept in higher education in Germany. It has garnered controversy because some critics are concerned that academic freedom could be sacrificed at the cost of business considerations and economic rationality. In Milan, the author presented the main points of his concept from the perspective of a vocational school where Health Information Managers were trained for more than ten years, that was maintained by an educational institution operating in the private sector whose aim is to make profit. Three years later, the author is still working in the field of adult education but has changed his employer, which is now the University Medical Center of the Johannes Gutenberg University Mainz. He has been there since March 2012. Amongst other things, he is now responsible for the training of employees (e.g. nurses, ancillary staff) who are not able to work in their learned profession anymore. Due mostly to work-related health problems, these colleagues are in need of rehabilitation. The rehabilitation program, which lasts two years, includes training in health information management. Changing from the private sector into an academic environment, therefore from the secondary sector into the so-called tertiary sector, resulted into a total revision of the existing concept. On the one hand this is connected with the academic environment, on the other hand it's all about the specific target group. Methods: The presentation's aim is to outline what measures were taken to rethink and adjust the concept of education and why they had to be taken. Consequentially, this method is more descriptive. Results: The training will not begin before April 2013, but what can be said now is that the training requirements are completely different from those in the private sector. But why? This has mostly to do with the specific target group: all of them have good knowledge of medicine as well as knowledge of place and organizational culture. This influences the curriculum, and in the way of breaking it down into education. Another considerable challenge is that the University Medical Center wants a practical education to make use of their manpower during the training. This means the trainees will be trained fulltime, and with full salary. Conclusions: On the one hand the University Medical Center considers the training of HIMs as a good way to help ill colleagues to come back on board as healthy and motivated employees. On the other hand it is a way to make the University Medical Center itself sustainable in face of the demographic shift. Sometimes this is reminiscent of squaring a circle. P36 Beyond the Code Of Ethics: Infusing Ethical Principles Throughout the Health Information/Coding Specialist Curriculum Marsha Holey ; Linda Tyacke St. Catherine University, Minneapolis, MN, United States In summary, our goal for this presentation is to describe our journey from applying the AHIMA Code of Ethics to specific professional situations, to infusing ethical principles including the AHIMA Code of Ethics throughout our curriculum. The outcome is to have students who act with academic integrity in their courses, tests and assignments and to graduate health information professionals who are able to make ethical decisions when faced with new situations in this complex and global world. P37 Health Information Management and Meaningful Use: Through the Lens of Regional Extension Centers in the United States Janelle Wapola ; Ryan Sandefer The College of St. Scholastica, Duluth, MN, United States Introduction and Objectives: Meaningful Use (MU) has become an overwhelming task for all organizations. This presentation will provide a brief overview of MU, the purpose of a Regional Extension Center Program (REC); the Minnesota (MN) and North Dakota (ND) Extension Center; overall acceptance of MU in the United States and how the Health Information Management (HIM) faculty at The College of St. Scholastica (CSS) are benefiting from participation. Methods: Starting its inception, CSS and their HIM faculty have been a part of the REC program that serves MN and ND. The REC currently has 4,800 eligible providers and 175 hospitals that are receiving technical assistance.

132
Satisfaction surveys are mailed out annually to participating clients and statistics are compiled by the federal government to compare the program nationally. Results: The purpose of the REC program is to assist small and rural hospitals and clinics achieve meaningful use of their electronic health records and therefore receive financial incentive payments. CSS is a lead organization in this endeavor with the HIM Department having three faculty providing direct technical assistance to clients. The remaining HIM faculty members have also engaged as subject matter experts for a variety projects. To date, over 30% of REACH clients have attested to MU, as compared to the national average of 17% of REC clients. This presentation will discuss the current state of RECs nationally, but will utilize the experiences of the local REC as an in-depth case study. One focus of the presentation will be on the outcomes of RECs to date, including challenges of assisting hospitals and providers achieve MU within the confines of the federal program. Another focus will be on the experiences of HIM faculty working with a REC and how the experience impacts their teaching, scholarship, professional development, and leadership skills. Conclusions: Achieving MU is challenging, particularly for small and rural facilities serving underserved populations. This REC program has proved highly successful for engaging hospitals and provider organizations, including the interpretation of the policy requirements, adoption of technology, and assistance with organizational change. The program has received high satisfaction scores and the rate of meaningful use attestation is significantly above the national average. Finally, the faculty participating in this project have had the opportunity to obtain hands on experience that is directly relevant and can be applied in the classroom. P38 Advancing the Health Information Management Profession Through Personal Relationships: The Leader-Member Exchange Leadership Theory Thomas J. Hunt Davenport University, Grand Rapids, MI, United States Introduction and Objectives: The Leader-Member Exchange (LMX) theory of leadership was first introduced in 1975 regarding vertical dyad relationships in organizations. The theory has evolved since then; however, it continues to focus on the benefits of high quality personal relationships between leaders and followers. The objective of this presentation is to promote awareness of this concept to those in the Health Information Management (HIM) profession and outline benefits found in previous research. Methods: A literature review was conducted to ascertain the benefits and criticisms found through previous research of this concept. Research spanning 1975 through 2011 from North America, Europe, and Asia were examined regarding LMX benefits to leaders, benefits to followers, and criticisms of the theory. Results: Review of the literature found evidence of positive outcomes regarding team performance, employee job satisfaction, citizenship behaviors, and lower intended turnover. Those with higher quality relationships to their leader tended to have faster career progression, more perceived organizational influence, and a higher level of complexity & responsibility in roles assigned. Challenges and criticism of the idea were also found. Conclusions: Formal HIM degree programs and continuing education offerings have many aspects of clinical, technical, and administrative topics to cover. It may be important in preparing HIM professionals to succeed in the workplace to focus not only on technical competency but also on interpersonal relationships and leadership. Evidence in multiple cultures suggests high quality LMX relationships are beneficial in individual career advancement & success, and may benefit the professional workforce as a whole.