SALIVARY GLANDS AND ORAL LESIONS IN DIABETES MELLITUS793361/FULLTEXT01.pdf · Saliva is essential...
52
UMEÅ UNIVERSITY MEDICAL DISSERTATIONS New Series No 182 — ISSN 0346-6612 From the Departments of Internal Medicine, Oral Pathology and Pathology, University of Umeå, Umeå, Sweden SALIVARY GLANDS AND ORAL LESIONS IN DIABETES MELLITUS An experimental and clinical study with special reference to the influence of metabolic control and duration of the disease Carl-Olof Reuterving À i- UMEÅ 1987
Transcript of SALIVARY GLANDS AND ORAL LESIONS IN DIABETES MELLITUS793361/FULLTEXT01.pdf · Saliva is essential...

UM EÅ UNIVERSITY M EDICAL DISSERTATIONSNew Series No 182 — ISSN 0346-6612
From the Departments o f Internal Medicine, Oral Pathology and Pathology, University o f Um eå, Umeå, Sweden
SALIVARY GLANDS AND ORAL LESIONS
IN DIABETES MELLITUS
An experimental and clinical study with special reference to the influence o f m etabolic control and duration o f the disease
Carl-Olof Reuterving
À i-
UMEÅ 1987


SALIVARY GLANDS AND ORAL LESIONS IN DIABETES MELLITUS
An experimental and clinical study with special reference to the influence of metabolic control and duration of the disease
AKADEMISK AVHANDLING
som med vederbörligt tillstånd av Rektorsämbetet vid Umeå Universitet för avläggande av medicine doktorsexamen
kommer att offentligen försvaras i aulan, administrationsbyggnaden, Regionsjukhuset, Umeå,
fredagen den 20 februari 1987, kl. 9.00
avCarl-Olof Reuterving
Umeå 1987

UMEÅ UNIVERSITY MEDICAL DISSERTATIONSNew Series No 182 — ISSN 0346-6612
ABSTRACT
Salivary glands and oral lesions in diabetes mellitus.An experimental and clinical study with special reference to
the influence of metabolic control and duration of the disease
Carl-Olof ReutervingDepartments o f Internal Medicine, Oral Pathology and Pathology,
University o f Umeå, Umeå, Sweden
Diabetes mellitus is associated with several clinically significant abnormalities in the oral cavity and salivary glands, the most common being periodontitis, salivary gland enlargement and a sensation of dry mouth. The prevalence o f dental caries in diabetics is mostly reported to be decreased or unaffected. Since there is a shortage of information concerning the influence of metabolic control and duration of diabetes on these abnormalities, the present studies were performed.
Three-month-old rats were made alloxan-diabetic and investigated after one and twelve months’ duration of diabetes for oral lesions and feeding behavior. They had free access to a standard pellet diet and tap water. Streptococcus mutans and lactobacilli were naturally occurring. In diabetic rats the proportion o f the oral flora which was lactobacilli was positively correlated to the blood glucose level. Untreated long-term alloxan-diabetic rats developed advanced periodontal disease and root surface caries in the molars at sites o f interdental impaction of foreign material. The degree of alveolar bone loss was positively correlated to the blood glucose level. Diabetic rats were hyperphagic and had a longer total eating time, including day-time eating, mainly by having longer meals but no significant increase of meal frequency, as compared with non-diabetic animals. The untreated alloxan-diabetic rats developed reduced salivary gland weight which was o f the same degree in short- and longterm diabetic animals. Short- and long-term untreated alloxan-diabetic rats showed a similar degree of morpho- metrically estimated lipid accumulation in the acinar cells of the submandibular glands, and the degree was positively correlated to the blood glucose level. However, lipid inclusion occurred only in rats with a morning nonfasting blood glucose level exceeding 15 mmol/L. The capillaries in the submandibular glands of the untreated long-term alloxan-diabetic rats had a significantly increased thickness of the basement membranes as compared with the observations in short-term diabetic and non-diabetic rats. Untreated alloxan-diabetic rats were also shown to have a decreased salivary flow rate compared with non-diabetic rats, and the decreased flow was negatively correlated to the blood glucose concentration. Salivary flow rate increased with the duration of the disease. The diabetic rats had increased salivary glucose levels, which were positively correlated to blood glucose values when the latter were above 15 mmol/L, suggesting a threshold mechanism for salivary glucose excretion. Insulin therapy reversed salivary flow rate and salivary glucose concentrations toward normal.
Salivary investigations were performed in eleven diabetic patients on two occasions with different metabolic control. Salivary flow rate showed marked interindividual differences but was not significantly changed by improved metabolic control although several of the patients initially had severely deranged glucose metabolism. A positive correlation between the glucose concentration in blood and saliva was seen in the parotid saliva during secretory stimulation. No significant change in electrolytes, amylase or antimicrobial factors was found.
Key words: diabetes mellitus, salivation, salivary glucose, saliva, submandibular gland, pilocarpine, root surface caries, periodontal disease, alloxan, feeding behavior, rats, humans.
ISBN 91-7174-274-3

UMEÀ UNIVERSITY MEDICAL DISSERTATIONSNew Series No 182 — ISSN 0346-6612
From the Departments of Internal Medicine, Oral Pathology and Pathology, University of Umeå, Umeå, Sweden
SALIVARY GLANDS AND ORAL LESIONS IN DIABETES MELLITUS
An experimental and clinical study with special reference to the influence of metabolic control and duration of the disease
Carl-OIof Reuterving
UMEÅ 1987

ISBN 91-7174-274-3
Phototype setting by Audio Visual Program AB, Umeå, Sweden
Printing by SAFAC, Nordmaling, Sweden, 1987

CONTENTS
Abstract ....................... 4Original papers ............................................................................................................. 5Introduction ........................................... 7
Aims of the present study ........................................................................................................ 15
Statistics ................................................................................................................................... 17Material .................................................................................................................................... 19
Methodology ........................................................................................................................... 21
Results .............................................................................................................. 25Discussion ................................................................................................................................ 31Summary and conclusions ...................................................................................................... 37
Acknowledgements ................................................................................................................. 41References ......................................................................... 43
Root surface caries and periodontal disease in long-term alloxan-diabetic rats ................... 51
Circadian eating and drinking habits in alloxan-diabetic rats ............................................... 59Salivary glands in long-term alloxan-diabetic rats. A quantitative light and electron-microscopic study .................................................................................................................... 69Pilocarpine-stimulated salivary flow rate and salivary glucose concentration in alloxan-diabetic rats .............................................................................................................................. 77Salivary flow rate and salivary glucose concentration in patients with diabetes mellitus .... 85

ABSTRACT
Diabetes mellitus is associated with several clinically significant abnormalities in the oral cavity and salivary glands, the most common being periodontitis, salivary gland enlargement and a sensation of dry mouth. The prevalence of dental caries in diabetics is mostly reported to be decreased or unaffected. Since there is a shortage of information concerning the influence of metabolic control and duration of diabetes on these abnormalities, the present studies were performed.
Three-month-old rats were made alloxan-diabetic and investigated after one and twelve months’ duration of diabetes for oral lesions and feeding behavior. They had free access to a standard pellet diet and tap water. Streptococcus mutans and lactobacilli were naturally occurring. In diabetic rats the proportion of the oral flora which was lactobacilli was positively correlated to the blood glucose level. Untreated long-term alloxan-diabetic rats developed advanced periodontal disease and root surface caries in the molars at sites of interdental impaction of foreign material. The degree of alveolar bone loss was positively correlated to the blood glucose level. Diabetic rats were hyperphagic and had a longer total eating time, including day-time eating, mainly by having longer meals but no significant increase of meal frequency, as compared with non-diabetic animals. The untreated alloxan-diabetic rats developed reduced salivary gland weight which was of the same degree in short- and long-term diabetic animals. Short- and long-term untreated alloxan-diabetic rats showed a similar degree of morphometrically estimated lipid accumulation in the acinar cells of the submandibular glands, and the degree was positively correlated to the blood glucose level. However, lipid inclusion occurred only in rats with a morning nonfasting blood glucose level exceeding 15 mmol/L. The capillaries in the submandibular glands of the untreated long-term alloxan-diabetic rats had a significantly increased thickness of the basement membranes as compared with the observations in short-term diabetic and non-diabetic rats. Untreated alloxan-diabetic rats were also shown to have a decreased salivary flow rate compared with non-diabetic rats, and the decreased flow was negatively correlated to the blood glucose concentration. Salivary flow rate increased with the duration of the disease. The diabetic rats had increased salivary glucose levels, which were positively correlated to blood glucose values when the latter were above 15 mmol/L, suggesting a threshold mechanism for salivary glucose excretion. Insulin therapy reversed salivary flow rate and salivary glucose concentrations toward normal.
Salivary investigations were performed in eleven diabetic patients on two occasions with different metabolic control. Salivary flow rate showed marked interindividual differences but was not significantly changed by improved metabolic control although several of the patients initially had severely deranged glucose metabolism. A positive correlation between the glucose concentration in blood and saliva was seen in the parotid saliva during secretory stimulation. No significant change in electrolytes, amylase or antimicrobial factors was found.
4

ORIGINAL PAPERS
This thesis is based on the following papers, which are referred to by their Roman numerals:
I. Reuterving C-O, Hägg E, Gustafson GT. Root surface caries and periodontal disease in long-term alloxan-diabetic rats.J Dent Res 1986;65:689-694.
II. Reuterving C-O, Hägg E. Circadian eating and drinking habits in alloxan-diabetic rats. Accepted for publication in Diabète et Metabolism.
III. Reuterving C-O, Hägg E, Henriksson R, Holm J. Salivary glands in long-term alloxan- diabetic rats. A quantitative light and electron-microscopic study.Accepted for publication in Acta Pathologica et Microbiologica Scandinavica.
IV. Reuterving C-O. Pilocarpine-stimulated salivary flow rate and salivary glucose concentration in alloxan-diabetic rats. Influence of severity and duration of diabetes.Acta Physiol Scand 1986;126:511-515.
V. Reuterving C-O, Reuterving G, Hägg E, Ericson T. Salivary flow rate and salivary glucose concentration in patients with diabetes mellitus. Influence of severity of diabetes. Submitted for publication to Diabète et Metabolism.


INTRODUCTION
Diabetes mellitus is a metabolic disease with associated generalized vascular lesions and affects on the nervous system (Cudworth et al 1982). Concerning the oral cavity and salivary glands, several clinically significant abnormalities have been described, the most common being periodontitis, salivary gland enlargement and dry mouth (xerostomia) (see Gottsegen 1970, Wolf 1977, Saadoun 1980, Murrah 1985 for reviews). However, the prevalence of dental caries is generally reported to be lower in diabetic children than in non-diabetics (Matsson and Koch 1975). Periodontal and periapical inflammatory processes also seem to impair the metabolic control in diabetic patients (Wolf 1977, Elfving et al 1979).
Xerostomia
Thirst and a sensation of dry mouth have been reported to be experienced by individuals with diabetes mellitus during periods of poor metabolic control (Mandel 1980). However, several authors have failed to demonstrate a consistent relationship between hyperglycemia and a sensation of dry mouth (Freund et al 1986, Pennebaker et al 1981, Eastman et al 1983).
Saliva
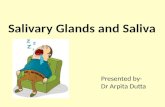
Saliva is essential for the integrity and physiology of the oral tissues. The mechanism of fluid and electrolyte secretion in the salivary glands are only partially understood. The available evidence indicates that saliva is first formed in the acini (Fig. 1) when neurotransmitters trigger a series of events involving transport of ions and as a consequence, para- or transepithelial flow of water (Gallacher and Petersen 1983, Young and Cook 1986). The composition of this nearisotonic primary saliva is then modified by the duct cells (Young et al 1981). Proteins are added to the fluid, mainly by exocytosis of secretory granules from acinar and duct cells (see Em- melin 1981 for review). Salivary secretion is influenced by the autonomic nervous system (Em- melin 1981). How the central nervous system is able to interfere with and regulate, the transport processes is still largely unknown. In addition, glandular nerves and hormones exert some long-term action. Loss of innervation or hormonal control, e.g. hypophysectomy, results in atrophy of the salivary glands (Emmelin 1981).
The volume and composition of the saliva vary with the type of stimulus used. For example, the rat submandibular gland has cholinergic, peptidergic, alfa-adrenergic and beta-adrenergic receptors (Gallacher and Petersen 1983, Bylund et al 1982). Stimulation of the first three types of receptors results in secretion of moderately large volumes of saliva with a characteristic electrolyte composition, while stimulation of beta-receptors causes the secretion of smaller volumes of saliva with a different electrolyte profile and a larger organic component (Henriksson et al 1981, Henriksson 1982, Gallacher and Petersen 1983, Martinez and Cassity 1983).
7

MOTO R N E R V E S
VASOMOTOR NERVES
SECRETORY NERVESCAPILLARYO
ACINI©
STRIATED DUCTINTERCALATEDDUCTS
EXCRETORY DUCTMYOEPITHELIALCELL GRANULAR DUCTS
Fig. 1. Schematic drawing, showing the acinus-duct system and the distribution of nerves in the rat submandibular gland. Redrawn and modified from Tamarin and Sreebny (1965) and Emmelin (1981).
Results from clinical as well as experimental studies on salivary flow rate in diabetes have been contradictory and not correlated to the degree of metabolic control or to the duration of the disease (Ulrich 1961, Conner et al 1970, Kjellman 1970a, Vogt and Zahl 1973, Marder et al 1975, Muratsu and Morioka 1985, Takai et al 1983a, Sharon et al 1985, Tenovuo et al 1986a).
A permeability or transport barrier for glucose exists across the secretory cells of the rat parotid gland resulting in a glucose concentration in the primary saliva ranging from 5 to 20% of the level in plasma (Mangos et al 1973). Small, polar non-electrolytes like glucose are thought to cross the secretory epithelium of the salivary gland and enter the saliva by a passive mechanism. In principle, this could involve not only simple diffusion but also solvent drag where the non-electrolyte is swept through a pathway that is shared with the secretory water flow (Potter et al 1984). The glucose flux of the rat submandibular gland appears to pass para- cellularly across the tight junctions (Takai et al 1983b). Stimulated final saliva of rats is virtually glucose-free (about 2% of the plasma concentration), because of reabsorption of glucose by the duct system (Takai et al 1983b).
The level of glucose in the saliva of diabetic patients is greater than normal (Englander et al 1963, Campbell 1965, Kjellman 1970b, Forbat et al 1981, Sharon et al 1985), but generally no correlation between the level of glucose in blood and saliva of diabetics has been observed (Kjellman 1970b, Campbell 1965, Forbat et al 1981, Sharon et al 1985). However, a positive correlation between glucose level in blood and parotid saliva has been reported in the period after an oral glucose load in diabetics (Englander et al 1963) and in non-diabetic healthy individuals (Shannon et al 1960, Feller and Shannon 1975, Von Ahrens 1971). On an individual basis there was a considerable variability, and there was an overlapping of the concentrations

of glucose in saliva between diabetics and non-diabetics which might be explained by, e.g., differences in salivary flow rates. It has been shown that salivary glucose levels are negatively correlated to flow rate of saliva, with a mean value of 0.07 mmol/L in parotid saliva during resting and 0.02 mmol/L during stimulation (Feller and Shannon 1975). A positive correlation between glucose in blood and saliva has been shown in experimentally diabetic dogs (Langley et al 1958) but not in diabetic rats (Matsumurà 1979). A threshold mechanism for salivary glucose excretion has been discussed in humans, but not verified (Forbat et al 1981). In experimentally diabetic dogs such a mechanism seems probable (Langley et al 1958).
Saliva is a hypotonic solution regardless of the rate of secretion. Almost all of the osmolality of saliva is accounted for by four ions: sodium, potassium, chloride, and bicarbonate. The concentration of each of these varies with the flow rate (Suddick et al 1980). Of importance for the protection against dental caries are the buffering role of bicarbonate and the concentrations of calcium and phosphate ions (Dawes 1984). Reports on electrolytes in the saliva of diabetics have been inconclusive. Sodium concentration is reported to be unchanged (Marder 1975, Sharon 1985), decreased (Vogt and Zahl 1973) or increased (Ulrich 1961); potassium to be unchanged (Vogt and Zahl 1973, Marder 1975, Ulrich 1961) or increased (Sharon et al1985); and calcium to be unchanged (Sharon et al 1985) or increased (Marder et al 1975). Salivary concentration of chloride and bicarbonate in diabetics have not been reported.
One of the most important functions of the salivary secretions is to continually provide the constituents of the protein coats for the teeth and for the oral mucosa (Boackle and Suddick 1980). In this regard, salivary secretions may be involved in processes such as lubrication of mucosa, remineralization of decayed tooth surfaces, reduction of microbial attachment to the teeth, neutralization of microbes and their products, and maintainance of taste acuity by interacting with the taste buds. Innate antimicrobial defence factors (lysozyme, lactoferrin, salivary peroxidase, myeloperoxidase, and bacteria aggregating proteins) in the saliva are important for the defence against a variety of microbiota (Tenovuo et al 1981, Ericson and Runde- gren 1983, Arnold et al 1984). The oral microorganisms are also under the continuous influence of two principal immunoglobulin classes: secretory IgA and IgG. Dimeric IgA is produced by immunocytes in the major and minor salivary glands and a secretory component of epithelial origin is added. IgG is derived from serum and reaches the oral cavity through the gingival crevices (Brandtzaeg 1984). Although insulin deficiency in man affects the overall protein metabolism (Manchester 1970) and that in the salivary glands of experimentally diabetic animals (Anderson and Shapiro 1980), it has not been conclusively shown if diabetic patients have altered amounts of protein in their saliva. A decreased level was reported by Vogt and Zahl (1973) while unchanged levels were seen by Sharon et al (1985) and Tenovuo et al (1986a) as compared with non-diabetic individuals. No difference in the level of salivary amylase is reported in diabetics as compared with controls (Sharon et al 1985, Tenovuo et al 1986a). Saliva from experimentally diabetic rats does not show a significant change in the level of total protein (Anderson and Johnson 1981, Muratsu and Morioka 1985), but salivary amylase is decreased as compared with controls (Anderson and Johnson 1981).
There is no indication of impaired antibacterial defence capacity of saliva in diabetics. In stimulated whole saliva from diabetics, Tenovuo et al (1986a) found increased levels of peroxidase, Ig A and lg G, but the same concentrations of lactoferrin and lysozyme as compared with controls. Marder et al (1975) found normal concentrations of IgA and IgG in stimulated parotid and submandibular saliva of diabetics. Experimental studies of saliva in diabetic ani-
9

mals have shown both decreased (Muratsu and Morioka 1985) and increased levels (Anderson and Johnson 1981) of salivary peroxidase as compared with controls. The former study also reported decreased levels of salivary lysozyme in the saliva of the diabetic animals.
There could be several reasons for the varying results concerning salivary flow rate and composition. The degree of metabolic control has not been considered except in salivary glucose studies. In addition, patients with other diseases have been included or it has not been explicitly stated if the diabetic patients had other concomitant diseases or if they were treated with drugs which might affect the salivary parameters.
Morphology of the salivary glands
Asymptomatic enlargement of the salivary glands has been reported to be rather common in human diabetics although it is easily overlooked (Davidson et al 1969, Rao and Rao 1979, Rusotto 1981, Baumann et al 1985). The enlargement is caused by interstitial fat infiltration (Davidson et al 1969) and increased acinar cell size due to accumulation of secretory granules (Donath and Seifert 1975, Baumann et al 1985). Rao and Rao (1979) reported that the enlargement was associated with poor metabolic control of the disease, and that glandular size was reduced when the metabolic control was improved.
The morphological changes observed in experimentally diabetic rats include atrophy of the parotid and submandibular glands, degeneration of autonomic nerves, lipid inclusions in the acinar cells, and death of acinar cells with subsequent replacement with fibrous tissue (Liu and Lin 1969, Anderson 1983, Takai et al 1983a, Hand and Weiss 1984, Cutler et al 1979, High et al 1985). Ultrastructural studies of the submandibular glands have not been based on morpho- metric measurements (Cutler et al 1979, Takai et al 1983a, Anderson and Garrett 1986). Furthermore, the influence of the severity of diabetes on gland morphology has not been evaluated.
Gingivitis and periodontitis
The rate of infection seems to be increased in diabetic patients (Larkin et al 1985). There is a positive correlation between the overall prevalence of infection and mean plasma glucose level (Rayfield et al 1982). Chemically induced diabetes has been reported to predispose for endogenous infections in rodents (Imai and Kurihara 1984).
It is generally held that diabetics have a higher prevalence of gingivitis and periodontitis than non-diabetics in spite of comparable amounts of supragingival plaque (Glavind et al 1968, Cohen et al 1970, Bernick et al 1975, Wolf 1977, Sznajder et al 1978, Gislén et al 1980, Cian- ciola et al 1982). When it comes to periodontitis, the difference between diabetics and nondiabetics is most pronounced in older individuals (Glavind et al 1986, Wolf 1977, Sznajder et al 1978).
In children and adolescents with insulin-dependent diabetes mellitus there appears to be a correlation between the degree of gingival inflammation and the level of glycosylated hemoglobin in the blood (Gislén et al 1980, Gusberti et al 1982, Ervasti et al 1985). In the studies of Ervasti et al (1985) and Tervonen and Knuutila (1986) the diabetic patients with good metabolic control had less gingivitis and periodontitis than the controls, and the patients with poor metabolic control had more gingivitis but the same degree of periodontitis. There also seems to be a
10

correlation between the degree of periodontitis and the duration of diabetes (Glavind et al 1968, Wolf 1977), although this could not be verified in the study of Nichols et al (1978).
The incidence of periodontal disease has been studied in diabetic animals (Glickman 1946, Sweeney et al 1962, Bissada et al 1966, ElGeneidy et al 1974), but the results are contradictory. This might be explained by differences in experimental models of diabetes, strains, diets, degree and duration of diabetes. No studies of the correlation between degree of periodontal disease and the degree or duration of diabetes have been performed as yet, except a study on genetically diabetic mice (ElGeneidy et al 1974).
Gingivitis is caused by substances derived from microbial plaque accumulating at or near the gingival sulcus (see Page 1986 for review). Other suspected local and systemic factors either enhance plaque accumulation or enhance the susceptibility for microbial attack. A portion of gingivitis lesions progresses to periodontitis, which is characterized by loss of periodontal ligament fibers and alveolar bone into which they are inserted. Only a few percent of the oral bacteria species are considered to be strongly associated with periodontitis. The microbiota at healthy sites include predominantly non-motile gram-positive facultative cocci and rods, while sites with gingivitis and periodontitis are associated with more complex microbiota with increasing proportions of more motile, gram-negative and anaerobic species (see Listgarten 1986 for review). An intact epithelial barrier and a high rate of epithelial turnover and surface desquamation prevent the bacteria from gaining direct access to the tissues. Under normal conditions there is a constant stream of migrating neutrophils from the vessels of the gingival plexus through the junctional epithelium to the gingival margin. Most bacteria produce substances that chemotactically attract neutrophils, and chemotactic substances are also present in the saliva. These neutrophils are members of first line of defense around the teeth; the epithelial barrier is the second. Other defence mechanisms in the gingival sulcus include flushing and antibacterial action of saliva and gingival fluid. Periodontal destruction results from episodes of acute inflammation due to an imperfectly balanced host/parasite interaction (Listgarten1986).
Impaired functions of leukocytes (Van Dyke et al 1986), changes of the microbial flora in marginal plaque (Mashimo et al 1983), increased tissue collagenolytic activity (Schneir et al 1984), thickening of basement membranes of the gingival blood-capillaries (Listgarten et al 1974, Lin et al 1975), and reduced salivary flow rate (Takai et al 1983a) have been pointed out as possible pathogenetic mechanisms for exaggerated periodontal breakdown in diabetics (see Manouchehr-Pour and Bissada 1983 for review).
Dental canes
The prevalence of dental caries in diabetics is mostly reported to be decreased in young and teen-age diabetics (Sterky et al 1971, Matsson and Koch 1975, Leeper et al 1985, Sarnat et al 1985) and unchanged in adult diabetics (Wolf 1977, Tenovuo et al 1986b, Kjellman et al 1970 ) as compared to non-diabetics. No epidemiological study has reported on the prevalence of root surface caries in diabetics, except a study in the preinsulin era (Zilz 1915) that reported profuse existence of caries at the cervical margins. However, this early report was based on clinical observation rather than on controlled investigations.
Increased caries incidence has been observed in rats with experimentally-induced diabetes (Sweeney et al 1962, Dalstein et al 1982). However, no existence of root surface caries was re
11

ported in long-term diabetic rats although they had root surfaces exposed to bacteria (Glick- man 1946, Bissada et al 1966).
Dental caries is considered to be a result of the interplay of three principal ecologie factors: the host (teeth and saliva), the microflora, and the diet (Keyes 1962). Investigations in both animals and humans have shown that the feeding pattern has a significant influence on the cariogenicity of the diet (Gustafsson et al 1954, König 1970, Theilade and Birkhed 1986). The most important parameters of feeding pattern discussed are the frequency of intake, the total daily eating time and the clearence time of carbohydrates from the oral cavity.
The composition of the diet is perhaps the most obvious factor that might differ between diabetics and non-diabetics. A “ diabetic diet” is recommended to be high in complex carbohydrates and fiber but low in simple sugars and fat (Kabadi 1986). The reduced sugar content might reduce the cariogenicity of the diet (Newbrun 1982a). However, the recommendation of separating the daily food intake into several small meals including a bedtime light meal has a caries-promoting influence if the diet has a cariogenic potential (Gustafsson et al 1954). Follow up studies of the dietary habits have shown that diabetic children and adolescents have a higher intake of protein than non-diabetics, but the amounts of fat and carbohydrates do not differ significantly (Sarnat et al 1985). However, the diabetics eat mainly polyunsaturated fatty acids and a lower proportion of the carbohydrates are refined carbohydrates, 5 to 7% in diabetics as compared with 7 to 11% in non-diabetics according to a study in Sweden (Sterky et al 1971) and 12% in diabetics and 25% in non-diabetics according to an Israeli study (Sarnat et al 1985). However, Sterky et al (1971) reported a lower average intake frequency of refined carbohydrates in the diabetic group (0.8 times per day versus non-diabetics, 1.8 times a day). Besides, Sarnat et al (1985) documented that the diabetics had six to eight regular meals a day, while the non-diabetics had three meals a day, and the diabetics had a late evening light meal not found in the nondiabetic group.
Simple sugars for acid production by acidogenic caries inducing bacteria could also be derived from the saliva and gingival crevicular fluid. The concentration of glucose in saliva is increased in diabetics but it is still less than a few percent of that in serum. In a study of 31 diabetics with blood glucose values between 4 and 20 mmol/L, the glucose concentration in stimulated parotid saliva ranged from 0.06 to 0.8 mmol/L (Forbat et al 1981). However, the glucose level in the gingival exudate approaches that of serum (Ficara et al 1975).
When root surfaces are exposed to the oral environment as a result of retraction of the marginal gingiva, the plaque retention areas may increase in extent, particularly in the large inter- proximal areas and along the cemento-enamel junction (Fejerskov and Thylstrup 1986). Due to its structure and chemistry, the root surface appears more vulnerable to mechanical and chemical destruction than the enamel (Nyvad and Fejerskov 1982). Root surface caries frequently develop as several brownish small lesions along the cemento-enamel junction. The prevalence of root surface caries increases with age. In the sixth decade the percentage of attacked root surfaces of all root surfaces with gingival recession in a selected sample of North Americans was reported to be 22% (Katz et al 1982) and the percentage of attacked teeth was 2.8% in a comprehensive study on a Finnish sample of individuals (Vehkalahti et al 1983). More than half of all new caries lesions in a study on institutionalized individuals above 50 years of age developed on root surfaces (Gustafsson et al 1954). These lesions are most frequently found on approximal and buccal surfaces. Epidemiological findings in ancient civili
12

zations and primitive populations report that root lesions occur in the absence of significant coronal decay (Jordan and Sumney 1973, Schamschula et al 1974, Molnar and Molnar 1985). Thus root surface caries can occur in populations whose diets have little sucrose (Newbrun 1982a, 1984). As research on this type of caries has been largely neglected in the past, it is obvious that our knowledge of its etiology and pathogenesis is incomplete. A specific microorganism has so far not been demonstrated to be responsible for the development of root surface caries (Ellen et al 1985). A low salivary flow rate (Ravald and Hamp 1981, Ravald et al 1986) and medication with drugs with xérostomie (Kitamura et al 1986) effects have been related to the development of root caries lesions. A high number of lactobacilli in the saliva has also been connected with the development of root surface caries (Ravald and Hamp 1981, Ravald et al 1986), but this condition could be secondary to a high consumtion of fermentable carbohydrates (Nyvad and Fejerskov 1982).
In the future, teeth will be retained longer than before in humans in the industrialized countries (Bowen 1984). The prevalence of root surface caries will probably rise, a fact that has rapidly increased the research efforts on this type of dental caries. In order to elucidate the etiology of the disease and devise effective methods of prevention, the need of well-defined animal models has been emphasized (Bowen 1984). The prevalence of naturally occuring impactions of hair between rat molars and associated induced periodontitis can be increased by mixing hair in a highly cariogenic diet and infecting the oral cavity with highly cariogenic bacteria (Guggenheim and Lutz 1985). Another way of inducing root surface caries is to reduce the salivary flow and feed the rats a cariogenic diet (Bowen et al 1986). However, in both these experimental models coronal caries also develop to a large extent, which was avoided in the briefly reported study of Weisberger et al (1940), in which desalivated rats were fed a nonspecified standard laboratory diet for as long as five months.
13


AIMS OF THE STUDY
A To study the influence of the metabolic control and duration of alloxan-induced diabetes in rats on the following parameters:
1. The occurrence of dental caries and periodontal disease in rats fed a defined laboratory diet.
2. Food and water intake, especially the circadian rhythm and the relationship between eating and drinking.
3. Salivary gland morphology.
4. Salivary fiow-rate and salivary glucose concentration.
B To study the influence of the metabolic control of diabetes in humans on salivary flow-rate and saliva composition.
15


STATISTICS
Common statistical methods were used (Colton 1974). Independent samples were compared with the Wilcoxon rank sum test. Comparisons between dependent pairs of samples were performed with the Wilcoxon matched pairs signed-rank test. Correlations between dependent variables were performed with Spearman’s rank correlation coefficient (rs). In evaluating differences of proportions between samples the Chi-square test was used. The samples were described with the mean value and standard error of the mean (SE). A p-value less than 0.05 was considered statistically significant.
17


MATERIAL
Animal studies (Paper I, II, III and IV)
AnimalsFemale albino rats of the highly inbred R-strain (Medical Faculty, Umeå, Sweden) were used. The number of rats in the different studies were:
• Paper I: 38 untreated alloxan-diabetic and 23 non-diabetic rats.
• Paper II: 35 untreated alloxan-diabetic, 10 insulin-treated alloxan-diabetic and 23 non-diabetic rats. These rats except the insulin-treated were also included in study I.
• Paper III: 50 untreated alloxan-diabetic and 58 non-diabetic rats.
• Paper IV: 22 untreated alloxah-diabetic, 7 insulin-treated alloxan-diabetic and 20 non-diabetic rats.
The animals were housed in plastic cages, bedded with wood chips, in air-conditioned rooms with a 12 h light/dark cycle (lights on 6.00 a.m. to 6.00 p.m.).
Diet. The animals had free access to tap water and a pelleted standard laboratory diet (R3 Rodent diet, Astra-Ewos, Södertälje, Sweden) containing 25.0% protein, 5% fat, 14.2% dietary fiber, 50.1% carbohydrate and 5.7% vitamins and minerals (Berglund et al 1982). Of the carbohydrates, less than 0.4% were found to be mono- and disaccharides when determined according to Fuchs et al (1974). The diet contained 15 mg fluoride per kg and the water 0.23 mg per litre.
Human study (Paper V)
Subjects. The sample consisted of eleven diabetic patients who were hospitalized because of poor metabolic control (Paper V, Table 1). Mean age was 28.7 years (range: 20 to 45 years). Salivary flow rate and composition were registered both during the period of poor metabolic control (HbAlc: 11.5±0.6%, blood glucose: 18.2±2.7 mmol/L) and one to five months later (mean 3 months) when the HbAlc-value had decreased by at least one percent-unit and the blood glucose level was below 10 mmol/L (HbAlc: 7.9±0.5%, blood glucose: 5.8±0.8 mmol/L). None of the patients had any other systemic or cardiovascular disease or any drug therapy other than that for diabetes control. None of the patients suffered from severe dental caries or advanced periodontal disease.
19


METHODOLOGY
Animal studies (Paper I, II, III and IV)
Induction and control o f diabetes. After a 48-h fast at the age of 3 months a single injection of alloxan monohydrate, 55 mg/kg, was given under ether anesthesia into a tail vein during external compression of the kidneys for five minutes according to Korec (1967). The degree of diabetes was monitored by regular determinations of the blood glucose level at about 10.00 a.m. by the glucose oxidase method (GLOX, Kabi, Stockholm). Only rats with a nonfasting blood glucose level above 10 mmol/L and glucosuria (Keto-Diastix, Ames Division, Slough, UK) during the whole experimental period were included. All control rats had a nonfasting blood glucose level below 6.3 mmol/L, and were aglucosuric.
Insulin treatment. Rats diabetic for two weeks (Study II and IV) were housed in metabolic cages and treated with a subcutaneous injection of protamine-zinc-insulin (Kabi-Vitrum, Sweden) each morning for two weeks. The doses were slowly increased according to daily urine volume and finally ranged from 1.2 to 3.0 IU.
Paper I
Dental and periodontal conditionsThe oral status was studied 1 month and 12 months after the induction of diabetes. Control rats were of the same ages. During sodium pentobarbital anesthesia the tissues of the head and neck were fixed by perfusion through the ascending aorta for 10 min. with 2% glutaraldehyde in isotonic (0.1 M) sodium cacodylate buffer, pH 7.4 (Sjöstrand 1967). All the following assessments of dental and periodontal parameters were made blindly.
The two halves of the mandible were dissected free of soft tissue, demineralized, and embedded in paraffin (Fig. 2). From one of the halves, mesio-distal sections were made through the center of the molars, and from the other half bucco-lingual sections were made through the first molar, step-wise at seven levels. The sections were stained by Meyer’s hematoxylin and eosin and by the Brown and Brenn method for bacteria (Luna 1968).
The maxilla was divided into two halves and dissected free of soft tissue. Furter treatment of the jaws and assessments are described in Fig. 2. The extent of carious decay was evaluated by using microradiographs and photographs of the molars. The following scoring system was used:
Grade 0. No demineralization was visible.
Grade 1. Demineralization was seen in the dentin at a proximal cemento-enamel junction.
21

Grade 2. The demineralization had resulted in loss of the proximal occlusal edge.
Grade 3. The disintegration of the tooth had passed half the occlusal surface.
THE MAXILLA WAS RINSED FROM SOFTTISSUERegistration of:—distance from the cemento-enamel junction at the prominence of each root to the alveolar bone crest.
THEREAFTER A MESIO-DISTAL GROUND SECTION THROUGH THE CENTER OF THE MOLARS WAS PREPARED AND A MICRORADIOGRAPH WAS TAKEN Registration of:—occlusal wear—frequency and extent of carious lesions.
THE MANDIBLE WAS DEMINERALIZED AND EMBEDDED IN PARAFFIN
A MESIO-DISTAL SECTION THROUGH THE CENTER OF THE MOLARS WAS PREPARED Registration of:—frequency of interdental impactions o f foreign material.
BUCCO-LINGUAL SECTIONS THROUGH THE FIRST MOLAR AT TEN LEVELS WERE PREPARED (Not possible in the 12-month- diabetic rats because of frequent tooth losses)Registration of:—extent of deposits on the cervical enamel.—area and apical extension of the junctional epithelium.—number of leukocytes in the junctional epithelium.—bone density, in the body of the mandible.
Fig. 2. Scheme describing treatment of the jaws for dental and periodontal assessments.
Bacteriological methods. Bacterial samples were taken with sterile cotton-coated steel pins (approx. 3 mm in diameter) from the supragingival molar regions. The diabetic and control rats were 4 to 14 months old. Bacterial cultivation was performed on blood agar, mitis-sali- varius agar (S. mutans) and Rogosa SL agar (lactobacilli).
Buffering capacity o f serum. Inflammatory exudate ought to contribute to a large proportion of the fluid that surrounds the bacterial plaque on the root surfaces. Bacterial fermentation of glucose in this exudate can yield at most twice as much acid as the amount of glucose, on a molar ratio. The ability of the exudate to counteract a drop in pH was roughly estimated. During ether anaesthesia blood was taken from 12 non-diabetic four-month-old rats by heart puncture. After coagulation the sera were pooled. Portions (50 /xl) of 1 M lactic acid were added to 8 ml of a serum sample and during stirring and gasing (C 02 5%, 0 2 20% and N2 75%) pH was measured. The experiment was repeated three times.
Paper II
Registration o f daily fo o d and water intakeThree-month-old rats were put into individual metabolic cages of a wire mesh construction with free access to food and water. Body weight, blood glucose level, glucosuria and keto-
22

nuria, food intake, water intake and urine excretion were registered daily during the period from one week before alloxan injection until four weeks thereafter. The construction of the cages did not prevent evaporation of urine during collection.
The same measurements were also performed for 48 h in rats with one and 12 months’ duration of untreated diabetes and in age-matched controls.
Continuous and simultaneous recording o f eating and drinkingShort-term diabetic and age-matched control rats were housed for 48 hours in metabolic mesh wire cages where containers for powdered standard pellet diet and water were placed on electromechanical balances with continuous and simultaneous quantitative paper recording of both eating and drinking (Spengler 1960). Recording during the last 24 hours of each rat was used. The following parameters of feeding and drinking behavior were calculated: total eating and drinking time and amount during 24 hours, eating and drinking time during each hour of the 24-hour period, number of meals and drinking bouts per 24 hours, duration of meals and drinking bouts, and meal-associated drinking pattern. When presenting results, a new meal was defined to begin whenever 15 minutes or more had elapsed since the end of the last eating period. The least interdrinking interval was defined as only 5 minutes because the act of drinking is more quickly accomplished than that of eating (Kissileff 1969).
Paper III
Morphology o f the submandibular glandSpecimens were studied one month and 12 months after the induction of diabetes. Control rats were of the same ages. Food but not water was removed from the cages at 8.00 a.m. One to three hours later the animals were anesthetized with sodium pentobarbital.
The combined submandibular/sublingual gland (SMG/SLG) on the left side was removed, quickly frozen in liquid nitrogen, stored in a plastic container and weighed. The in vivo remaining parotid glands and SMG/SLG were then fixed by perfusion (See study I).
The amount and distribution of lipid inclusions in the frozen submandibular glands were evaluated in sections that were fixed in Baker’s formol calcium and stained with the Oil Red O procedure. The proportion between lipid and acinar cell area was estimated for each rat with Weibel’s point counting method (Weibel 1979).
SMG capillary basement membrane width (CBMW) was measured ultrastructurally with a method described by Weibel and Knight (1964). The 10 first observed cross-sectioned intact capillaries of each rat were photographed in an electron microscope and a mean value of CBMW in each rat was calculated.
Paper IV
Determination o f serum osmolality was performed at the time of saliva collection in seVen untreated and seven insulin-treated alloxan-diabetic rats and in 13 age-matched controls after cutting the tail tips. The osmolality of serum from blood samples was measured by freezing point determinations with a Knauer osmometer.
23

Saliva sampling and analyses. In the morning the rats were deprived of food but not water. One to three hours later the animals were anesthetized with sodium-pentobarbital. Pilocarpine 1.25 mg/kg was given subcutaneously between the shoulders when the corneal reflex had just disappeared. Each rat was placed on a table tilted to the vertical plane with the head of the animal hanging into a plastic funnel. Saliva was collected in an ice-chilled graded tube during 15 minutes after the injection of pilocarpine (Bernarde et al 1956). The tubes were then sealed and stored at -20°C . Salivary glucose concentrations were determined by the hexoki- nase/glucose-6-phosphatase method. Blood glucose assays were performed simultaneously with collection of saliva.
Paper V
Saliva collection. All samples were collected before noon at least one hour after smoking and eating. Immediately before collection, blood glucose level was estimated. Whdle saliva was then collected during chewing. Aliquots of saliva were withdrawn for estimation of lactoba- cilli and S. mutans. Lashley cups were fixed over the parotid duct openings about 15 min later and resting parotid saliva was collected. Simultaneously submandibular/sublingual saliva was collected from the mouth-bottom with a pipett. Finally the tongue was swabbed with 2% citric acid every 30th second and parotid saliva was collected.
Laboratory analyses. HbAlc was measured at the Department of Clinical Chemistry, Umeå University Hospital. pH and buffer capacity of the whole saliva fractions were estimated. Exact portions of the stimulated parotid saliva and resting parotid and submandibular/sublingual saliva fractions for the different chemical analyses were transferred to test tubes and frozen at -20°C . Within four months the samples were thawed and analyzed for glucose (enzymatically with hexokinase and glucose-6-phosphate dehydrogenase, Sigma Co, St. Louis, MO.; the least detectable concentration was about 0.01 mmol/L), total protein, amylase, peroxidase, lysozyme, IgA, inorganic phosphate and the electrolytes Na +, K +, Ca2+ and Mg2 + . Several of the resting saliva samples were small and allowed estimation of only some of these variables. However, glucose was estimated in resting saliva from nine of the patients.
24

RESULTS
Paper I
Lactobacilli and Streptococcus mutans were naturally occurring inhabitants of the oral bacterial flora. The proportion of lactobacilli of the total cultivable bacteria was significantly (p<0.05) higher in diabetic rats (3.0±1.4%) than in controls (0.3±0.2%). The proportion of the oral flora which was lactobacilli was positively correlated with the blood glucose level in the rats with diabetes of one month’s duration (rs = 0.87, pcO.Ol).
In short-term diabetic rats (one month) there was less dental plaque in the buccal gingival region of the first mandibular molar than in control rats (p <0.01), but the density of leukocytes in the junctional epithelium was increased (p<0.05). Interdentally the gingival papillae were intact and the prevalence of foreign material impactions was as low as for the controls (17% versus 25% of all interdental spaces). The distances from the cemento-enamel junction of the molars to the most apical point of the junctional epithelium and to the alveolar bone crest were not significantly different between the diabetic and control rats. No caries lesions were seen.
In long-term diabetic rats (12 months) there was more periodontal breakdown than in the age- matched control rats (Paper I, Fig. 2). The periodontal breakdown was always associated with large interdental impactions of foreign material. In the diabetic rats there was a significantly (p<0.05) higher prevalence of impactions of foreign material in the interdental areas that were examined histologically (47%) than in the age-matched control rats (14%). In the diabetic rats, the impactions usually were composed of both hairs, food, and bedding material, while in the controls the impactions consisted of only one hair at each site. In the control rats there were no exposed root surfaces for plaque accumulation.
Caries was only seen in the diabetic rats and in sites with interdental impactions. The decay was shown to start in the cementum at the cemento-enamel junction (Fig. 3).
M, distally
M2 mesially
M2 distally
M3 mesially
Fig. 3. Mean prevalence of different degrees o f caries lesions (grade 1 - 3 , see “ Methodology” ) in the maxillary molars (Mj, M2, and M3) of rats with diabetes o f 12 months’ duration (n = 18).
i i i i i i i i I □ i» «ries Ü grade 120 40 60 80 100
DECAYED SURFACES (%) ^ grade 2 H grade 3
25

Bone loss was seen in diabetic rats, both of the central body of the mandible (one month’s diabetes) and of the alveolar crest (12 months* diabetes).
The amount of alveolar bone loss in the diabetic rats was related to the degree of hyperglycemia (rs = 0.60, p<0.05). The same tendency was seen concerning the number of caries lesions (rs = 0.40) but it did not reach statistical significance. Occlusal wear of the molars in long-term diabetic rats was significantly increased as compared with the controls.
The pH of pooled rat serum in three experiments showed a continuous and identical decrease from 7.4 to 5.0 when small quantities of lactic acid were added (Fig. 4).
8.0 -
7 0 - * .
6.0 - * * ,
x 5 0 - * ** * *
* * * * * * *
3.0 -
2.0 -
X i i i i i 1 I I I I I
10 20 30 40 50 60 70 80 90 100 110Lactic acid (mmol/l)
Fig. 4. Buffering capacity o f rat serum when adding lactic acid.
Paper II
After two days of fasting followed by alloxan injection, mean food and water intake increased and mean body weight decreased progressively during about one week and then stabilized. Glucosuria was already present in all rats from the first day after alloxan administration. Mean blood glucose concentration was about the same level from one to four weeks after alloxan injection. Transient ketonuria was seen in all rats for varying periods during the second to seventh day after alloxan injection, but thereafter was only seen sporadically in a few rats.
The rats with one and 12 months duration of diabetes ate nearly twice as much as the controls. For the diabetic rats there was a significant correlation between blood glucose level and amount of food intake (rs = 0.50, p<0.01), water intake (rs = 0.61, pCO.OOl), 24-h urine volume (rs = 0.62, p <0.001) and body weight (rs= —0.45, p<0.05).
Control rats started to eat sporadically late in the afternoon (Fig. 5). When the the light was turned off at 6.00 p.m. they markedly increased their eating and drinking. Then there was a slow decrease until 4.00 a.m. when eating and drinking abruptly increased. When the light was turned on at 6 a.m. the rats stopped both eating and drinking. The drinking and eating pattern for the diabetic rats during the dark period was essentially parallel to that of the controls but at a higher level. The biphasic eating and drinking pattern during the dark period was similar in both groups. The diabetic rats also ate and drank during most of the light period whereas the controls only ate or drank during the last three hours of the light period.
26

120 r
DARK PHASE
TIME OF DAY
Fig. 5. Circadian pattern o f food and water intake in 12 rats with 1 month duration o f diabetes (unfilled area) and 12 age-matched controls (filled area). Mean±SE.
There was no significant difference in eating frequency between diabetic rats (13±0.8 meals/24 h) and controls (11±0.6), but the diabetic rats drank twice as often as the controls (24±0.4 drinking bouts/24 h versus 12±0.8). The meal and drinking bout durations were about twice as long in the diabetic rats as in the control rats (p <0.01 for both). Most drinking occurred during the meal or within 5—15 min before or after the meal in both controls and diabetics.
Insulin therapy partly normalized the amounts of food and water intake (p <0.001, for both parameters compared with pretreatment amounts).
Paper III
Weights of the parotid glands and the combined SMG/SLG’s were about 20 to 30% lower in the diabetic rats than in the age-matched controls. The weights were not influenced by the duration of diabetes, but tended to be correlated to the blood glucose level. However, the correlations were not statistically significant (rs varying between — 0.19 and — 0.90). Only the parotid gland weight to body weight ratio, but not the combined SMG/SLG’s to body weight ratio, was decreased in the diabetic rats compared with age-matched controls.
Only diabetic rats had lipid inclusions in the submandibular glands. The inclusions were situated basally in the acinar cells, and were not seen in the ductal cells except in a few intercalated duct cells. The amount of lipid inclusions did not differ significantly between rats with diabetes for one month and 12 months. There was a significant correlation to the blood glucose level in the 12-month diabetic rats (rs = 0.79, p<0.01).
There was a non-significant tendency to an age-dependent increase of the CBMW in the nondiabetic rats. Long-term diabetic rats had significantly wider SMG capillary basement membranes than the other groups of rats (Table).
27

Table. Capillary basement membrane width (CBMW) in the submandibular glands o f diabetic rats and age-matched controls.
Age/group Number of rats CBMW nm
4 monthsControl 10 69.2±3.6Diabetic 10 65.0±3.015 monthsControl 11 83.8±3.8Diabetic 12 106.7±7.2*
*p<0.05 as compared with age-matched controls. Mean±SE. Diabetes was induced at three months’ age.
Paper IV
Salivary flow rate was significantly lower and salivary glucose concentration higher in the diabetic rats than in age-matched controls. In the diabetic animals there was a negative correlation between salivary flow rate and blood glucose level (rs= —0.44, p<0.05) and a positive correlation between salivary and blood glucose concentrations (rs = 0.71, p <0.001) at blood glucose levels exceeding 15 mmol/L. In the diabetic rats salivary flow rate increased toward normal with the duration of the disease: p <0.05 when comparing animals with 2 and 4 weeks’ duration; p<0.01 when comparing animals of 4 weeks’ and 12 months’ duration. Insulin therapy reversed salivary flow rate and salivary glucose concentration towards normal.
Serum osmolality, above approximately 15 mmol/L blood glucose level, was positively correlated to the blood glucose level (rs = 0.81, p<0.05).
Paper V
Resting and stimulated salivary flow rates were not significantly altered when the degree of metabolic control was improved. Nor was there any significant correlation between the change of blood glucose or HbAlc levels and the change of salivary flow rate between the two occasions. However, there was a positive correlation between stimulated salivary flow rate during the first and the second occasion (whole saliva rs = 0.93, p < 0.001 and parotid saliva rs = 0.77, p <0.05).
The glucose levels in the different salivary portions were about three times higher during the first investigation than during the second. There was a positive correlation between the glucose level in stimulated parotid saliva and blood at the first investigation (Fig. 6). However, no such relationship was seen concerning the resting submandibular/sublingual and parotid saliva fractions. No significant correlation between glucose levels in the salivary fractions on the one hand and HbAlc or salivary flow rate on the other hand were seen.
28

\"oEE
00oLJ
ÈEI<C/)
0.15'
0.10-
0.05
d ü ü o °o » ,■
I 10 20 30 40BLOOD GLUCOSE, m m o l/L
F/g. 5. Relationship between the concentrations o f glucose in blood and stimulated parotid saliva during worse (■, rs = 0.64, P <0 .05) and better metabolic control (□ ) .
The concentration of S. mutans in whole mixed paraffin-stimulated saliva was significantly lower during the period of improved metabolic control than at the first investigation, but no significant changes of the number of lactobacilli, salivary pH or buffering capacity were seen.
Chemical analyses of stimulated parotid saliva for total protein, amylase, peroxidase, lyzo- syme, IgA and electrolytes (Na + , K+, Ca2+, P 0 42- and Mg2+ ) did not reveal any differences between the two occasions, but the interindividual variations were pronounced.
29


DISCUSSION
Periodontal disease and caries in alloxan-diabetic rats
Increased susceptibility to periodontal disease and coronal caries has been demonstrated in alloxan-diabetic rats (Bissada et al 1966, Sweeney et al 1962). Bissada et al (1966) found that periodontal breakdown occurs in diabetic rats only at sites with a local source of irritation. Morphometrie registration or bacterial characterization were not performed and caries was not seen. In the present study large interdental impactions of hairs, food particles and bedding material were frequent in the long-term diabetic group and seemed to be a prerequisite for periodontal destruction and caries as these changes did not occur at sites free from impactions.
Alloxan diabetic rats not treated with insulin show increased levels of kininogens in plasma (Ottlecz et al 1979). This might lead to an enhanced inflammatory response (Lithner and Hägg 1975) and an enhanced bone resorption due to prostaglandin production (Gustafson and Lerner 1984, Gustafson et al 1986). The increased periodontal and medullar bone loss observed in the present investigation may be a consequence of an increased inflammatory response to bacterial and mechanical stress.
In the present study an increased number of leukocytes was seen in the gingival crevicular epithelium of the diabetic rats, which might be explained by an increased traumatic effect of the hyperphagia seen in these rats. This effect of eating was indicated in the study of Irons and Schaffer (1966). Furthermore chemically-induced diabetes has been reported to predispose for endogenous infections in rodents (Imai and Kurihara 1984). The impaired microbial host defense in diabetes may partly be ascribed to decreased chemotactic activity (Ramamurthy et al 1979, Golub et al 1982) and to lowered bactericidal capacity of the leukocytes (Dziatkowiak et al 1982). The predominant leukocyte of the gingival crevice in both health and disease is the neutrophil, and it is known that quantitative or qualitative defects of neutrophils rapidly lead to acute inflammation and destruction of the gingival tissues (Van Dyke et al 1985).
Increased prevalence of root surface caries in human diabetics or in experimental diabetes has not been shown previously. Dental caries has a complex multifactorial etiology where host, dietary and bacterial factors interact over a period of time to induce demineralization (Keyes 1962).
The enamel of molars in rats older than about 3 months, which were used in the present study, is well mineralized and very resistent to dental caries (Fitzgerald and Larson 1967). However, when gingival tissue recedes the more vulnerable cementum becomes exposed to the oral environment and dental caries may involve only the cementum and leave the enamel intact as was
31

seen in the present study (Jordan et al 1972). Decreased salivary flow rate is seen in diabetic rats (Takai et al 1983a, Reuterving 1986) and might contribute to an increased incidence of root surface caries and development of periodontal disease in these animals (Weisberger et al 1940, Bowen et al 1986, Takai et al 1985). A positive relationship between decreased salivation and development of root caries is also seen in humans (Ravald and Hamp 1981, Kitamura et al 1986).
There is overwhelming evidence that dental caries is initiated by the production of organic acid end products via carbohydrate metabolism by plaque bacteria and the subsequent dissolution of enamel mineral (see van Houte 1980 for review). The “ critical pH ” at which the overlaying dental plaque ceases to be saturated with calcium and phophate ions and below which dental mineral will dissolve is often assumed to be about 5.2 to 5.7 for mature enamel, but only about 6.0 to 6.9 for dental root hard tissue (Van Houte 1980, Hoppenbrouwers et al 1986). Therefore, only a slight decrease of pH in dental bacterial plaque may lead to root surface caries. However, the critical pH varies with the size of the pool of bound Ca and P 0 4 and the availability of this pool. At a low “ critical pH ” only certain bacteria, e.g. S. mutans and lactobacilli, are acidogenic and considered to be caries promoting (Van Houte 1980). However at a high “ critical pH ” a broader spectrum or oral bacteria become cariogenic.
Dietary sugar is pointed out as an initiating factor in the etiology of coronal caries, but the role of diet in root caries is not well understood (Newbrun 1982b). However, a relationship between the incidence of root caries and total sugar content of the food is shown in rice rats (DePalma 1983). The rats of the present study were fed a standard laboratory diet with a low cariogenic potential. However, hyperphagia and retention of food interdentally in this study might promote caries by elongating the exposure of food components to the bacteria (Birkhed1983).
The carious lesions in the present study were always associated with interdental impactions of foreign material and an inflammatory reaction in the periodontal tissue. Since the blood of the diabetic rats contained high glucose levels, the glucose of the gingival inflammatory exudate might have served as a substrate for bacterial production of acids at these sites, initiating carious lesions on the root surfaces. In human diabetics it has been shown that the concentration of glucose in the gingival exudat is only slightly lower than that in the blood (Ficara et al 1975). The rats of the present study harbored the strongly acidogenic and acid tolerant bacteria species S. mutans and lactobacilli which are able to produce lactic acid from glucose in the surrounding fluid such as saliva and inflammatory exudat (Carlsson 1984). In the present study rat serum was titrated with lactic acid and this in vitro assay suggests that a significant decrease of pH might occur in the diabetic rats as a result of bacterial metabolism of glucose in the plasma-like inflammatory exudate.
Thus it has been shown that advanced periodontitis and caries, almost exclusivly confined to the root surfaces, can appear in long-term alloxan-diabetic rats fed a low cariogenic diet and without experimental manipulation of the teeth.
Feeding behavior in diabetic rats
Rats with experimental diabetes mellitus are extremely hyperphagic when fed a standard laboratory diet which contains mostly carbohydrates and only little fat (Brodsky et al 1952, Car
32

penter and Grossman 1983). Dietary carbohydrates may serve only little more than a non-nutritive filler to a diabetic rat (Friedman 1978). Diabetic rats then have to rely on dietary fats as the primary source of metabolic fuels once endogenous lipid reserves are depleted a few days after induction of diabetes (Friedman 1978).
Both diabetic and control rats ate discrete meals separated by distinct intermeal intervals. The larger daily food intake in the diabetic rats could not be explained by a higher frequency of meals, but rather a larger meal size, which is in agreement with most previous reports (De Castro and Balagura 1975, Thomas et al 1976). Furtermore, daytime eating occurred among the diabetic rats, which only rarely was seen in the control animals.
Diabetic rats also had increased drinking (drinking frequency, drinking bout duration, and drinking rate) which was mainly meal-associated.
The hour to hour circadian pattern of food and water intake in experimental diabetes, and relationship between them, has not been reported earlier.
In desalivated rats all drinking occurs within meals in alternating periods of minute draughts and food intake which is supposed to be a response to the necessity to swallow dry food from a dry mouth (Kissileff 1969). Although rats diabetic for one month only have about 16% of the normal pilocarpine-stimulated salivary flow rate (Reuterving 1986) this pronounced prandial drinking behavior was not seen in the diabetic rats in the present study.
A longer total circadian eating time might have a caries-promoting effect (König 1970). Whether increased meal-associated drinking has the opposite effect is unsettled.
Salivary glands
As in earlier investigations (Anderson 1983, Liu and Lin 1969), an atrophy of the salivary glands was seen in diabetic animals. The trophic stimulus (Johnson and Sreebny 1982) on the salivary glands from an increased intake of pelleted diet in the diabetic rats was of minor importance compared with the influence of the diabetic condition. Salivary gland enlargement has been observed in some human diabetics (Davidson et al 1969, Donath and Seifert 1975, Rao and Rao 1979, Baumann et al 1985). However, there are no studies measuring salivary gland size in a sample of diabetic patients.
In the present study lipid inclusions were almost exclusively seen in acinar cells following alloxan-induced diabetes. This derangement has been reported previously (Anderson and Johnson 1981, Anderson 1983, Hand and Weiss 1984, Cutler et al 1979, Anderson and Garrett 1986), but the amount of lipid has not previously been quantified morphometrically. The finding of a positive correlation between the amount of lipid inclusions and blood glucose level has not been reported previously. This correlation supports the concept that the metabolic derangements associated with diabetes lead to lipid inclusions rather than the lipid inclusions being the result of alloxan toxicity. These conclusions are further strengthened by previous reports (Anderson 1983, Anderson and Garrett 1986) which show that the glandular accumulation of lipid disappears following insulin treatment. It has been suggested that thè lipid accumulation is the result of an increased uptake of lipids for use as an energy source, or a decreased utilization for the synthesis of secretory granule and plasma membrane material
33

(Anderson and Garrett 1986). Inclusion of lipid in acinar cells of salivary glands of human diabetics has not not been observed (Davidson et al 1969, Donath and Seifert 1975, Rao and Rao 1979, Baumann et al 1985).
In the present study an increased width of the capillary basement membranes in the SMG’s was found. This has not been reported previously. It is possible that changes in the salivary gland capillary basement membrane might affect its permeability and filtration properties (see Williamson and Kilo 1983 for review) thus affecting salivary fluid production.
Reduced salivary gland weight, lipid inclusions in the acinar cells and capillary basement membrane thickening in the submandibular glands of diabetic rats might be of importance for salivary gland function.
Saliva in diabetic rats
Pilocarpine is a parasympathomimetic drug that induces marked salivary fluid secretion (Abe et al 1982). Parasympathetic, sympathetic and substance P stimulation of the submandibular salivary gland of diabetic and control rats result in lower salivary flow-rate in the former, which is reversed by insulin treatment (Takai et al 1983a). This is in accordance with the observations of the present study, although Takai et al (1983a) studied rats only 10 days after induction of diabetes when the changes in energy metabolism are not yet stabilized (Booth 1972, Carpenter and Grossman 1983).
The pathogenesis of reduced pilocarpine-induced salivary flow rate in diabetic rats is not known. Several morphological and functional changes have been reported in the salivary glands of diabetic rats: reduced glycolysis (Murakami 1974), reduced protein synthesis (Anderson and Shapiro 1980, Anderson 1983), reduced weight (Liu and Lin 1969, Murakami 1974, Takai et al 1983a, Anderson 1983, Reuterving paper III), lipid deposits in glandular cells (Liu and Lin 1969, Anderson and Johnson 1981, Anderson 1983, Hand and Weiss 1984, Reuterving paper III), alterations of the basement membranes of the acini (Hand and Weiss1984) and capillaries (Reuterving paper III) and possible nerve lesions (Takai et al 1983a).
In the present study there seemed to be no correlation between salivary glucose and blood glucose concentration when the blood glucose level was below 15 mmol/L. When blood glucose levels exceeded this value salivary glucose concentration rose steeply in a linear fashion. There are several possible explanations for this phenomenon: the reabsorbtion of glucose from the ducts (Takai et al 1983b) could be limited as in the kidneys (Johansen et al 1984); the demonstrated increase of serum osmolality in rats with blood glucose levels exceeding 15 mmol/L might decrease water content in the saliva and thus increase salivary glucose concentration; impaired cellular metabolism in highly diabetic animals might perhaps cause a decrease in salivary reabsorption of glucose (Murakami 1974).
A direct toxic effect of alloxan on the salivary glands is not probable because insulin treatment in the present study increased the salivary flow rate toward normal.
The decreased salivary flow-rate and increased salivary glucose concentration in the diabetic rats might contribute to the development of periodontitis and root surface caries which is seen in these rats.
34

Saliva in human diabetes
In the present study, salivary flow rate, during both stimulation and relative rest, was not significantly affected by the metabolic control of diabetes. Thus the degree of glucose metabolic derangement does not seem to be important for salivary secretion rate in diabetics. There was, however, marked interindividual differences in salivary flow rates in the present study. In previous investigations diabetics have been reported to have similar (Marder et al 1975, Sharon et al 1985, Tenovuo et al 1986a), lower (Ulrich 1961, Conner et al 1970, Kjellman 1970a), or even higher (Vogt and Zahl 1973) salivary flow rates as compared with non-diabetic individuals. The results of salivary flow rate at different degrees of metabolic control in the present study contrasts to the results in alloxan-diabetic rats. Possible reasons for this discrepancy, besides species differences, might be different modes of secretory stimulation.
The sensation of dry mouth in some diabetics during periods of poor metabolic control does not seem to be explained by reduced salivary flow rate from the major salivary glands. However, the function of the accessory salivary glands has not been investigated.
A significant correlation between the glucose level in blood and saliva could only be demonstrated in the stimulated parotid saliva fraction. A threshold mechanism for salivary glucose excretion has been discussed in humans, but not verified (Forbat et al 1981). The results of glucose assays in stimulated parotid saliva in the present study might indicate that there is, in fact, a threshold at blood glucose levels of about 10-15 mmol/L i.e. about the same level as for urinary excretion of glucose (Johansen et al 1984).
In conclusion, the degree of diabetic metabolic control did not seem to be of major importance for salivary flow rate or composition in diabetics except for the glucose concentration and possibly the number of S. mutans. In stimulated parotid saliva a positive correlation between glucose levels in saliva and blood was seen and a blood glucose threshold for glucose excretion at about 10—15 mmol/L might be present.
35


SUMMARY AND CONCLUSIONS
Animal studies
Untreated alloxan-diabetic rats fed a standard laboratory diet were investigated after one (short-term) and 12 months’ duration of diabetes (long-term). They were compared with age- matched non-diabetic animals concerning the prevalence of caries, periodontal disease, morphology of salivary gland lesions, eating and drinking habits, salivary flow rate and salivary glucose levels. The influence of insulin treatment on feeding and salivary flow rate was also studied in short-term diabetic rats. The main findings were:
Paper I
• Streptococcus mutans and lactobacilli were naturally occurring inhabitants of the oral cavity in both control and diabetic rats.
• In short-term diabetic rats no dental caries or periodontitis were seen, but a loss of medullary bone of the mandible was registered. The proportion of the oral flora which was lactobacilli was positively correlated with the blood glucose level.
• Long-term diabetic rats developed advanced periodontal breakdown and root surface caries of the molars at sites of interdental impactions of foreign material. The alveolar bone loss was related to the degree of hyperglycemia.
Thus it has been shown that altered oral bacterial flora, advanced periodontitis and caries, almost exclusivly confined to the root surfaces, can appear in long-term alloxan-diabetic rats fed a low cariogenic diet and without experimental manipulation of the teeth. Factors predisposing for periodontitis and root surface caries appear to be the diabetic state and the interdental impactions. Long-term alloxan diabetes in rats might serve as a model for studying the genesis of root surface caries and periodontal disease.
Paper II
• Diabetic rats were hyperphagic and had longer meals and total eating time (including daytime eating) compared with non-diabetic animals and these parameters were positively correlated to blood glucose levels.
• Diabetic rats also had increased drinking (drinking frequency, drinking bout duration, and drinking rate) which was mainly meal-associated.
37

A longer total circadian eating time might have a root surface caries-promoting effect. Whether increased meal-associated drinking may have the opposite effect is unsettled.
Paper III
• Diabetic rats developed a reduced salivary gland weight which was of the same degree in short and long-term diabetic animals and was proportional to the reduced body weight in these rats. However, the parotid glands showed a relatively larger weight reduction than the combined submandibular/sublingual glands.
• Short- and long-term diabetic rats showed a similar degree of morphometrically estimated intracellular lipid accumulation in the submandibular glands which was positively correlated to blood glucose levels in the long-term group. Lipid inclusions occurred only in rats with a blood glucose level exceeding 15 mmol/L.
• Long-term diabetic rats had a significantly increased capillary basement membrane thickness in the submandibular glands compared to short-term diabetic and non-diabetic rats.
Reduced salivary gland weight, lipid inclusions in the acinar cells and capillary basement membrane thickening in the submandibular glands of the diabetic rats might be of importance for salivary gland function.
Paper IV
• Untreated alloxan-diabetic rats had decreased salivary flow rate which was negatively correlated to blood glucose concentration. Salivary flow rate increased with the duration of the disease.
• Diabetic rats had increased salivary glucose levels, which were positively correlated to blood glucose values when the latter were above 15 mmol/L, suggesting a threshold mechanism for salivary glucose excretion.
• Insulin therapy reversed these abnormalities toward normal.
The decreased salivary flow-rate and increased salivary glucose concentration in the diabetic rats might contribute to the development of periodontitis, root surface caries and an increased number of oral lactobacilli.
Human study
Paper V
Eleven diabetics underwent salivary investigations (flow rate, pH, buffering capacity, content of glucose, total protein, IgA, enzymes, electrolytes and the number of S. mutans and lactobacilli) on two occasions, one to five months apart, with different metabolic control.
38

• There was no significant difference of salivary flow rate or saliva composition except for glucose and S. mutans levels between the two investigations.
• In stimulated parotid saliva a correlation between glucose levels in saliva and blood was seen.
The degree of diabetic metabolic control did not seem to be of major importance for salivary flow rate or composition in diabetics except for the glucose concentration and possibly the number of S. mutans. There might be a blood glucose threshold for glucose excretion in stimulated parotid saliva.
39


ACKNOWLEDGEMENTS
The present thesis was carried out at the Departments of Internal Medicine, Oral Pathology, Pathology and Cariology, University of Umeå. Many thanks to all of you who have contributed to the stimulating atmosphere in which I have had the privilege to work. I especially wish to express my sincere gratitude to the following persons:
• Erik Hägg, my supervisor and friend, for his genuine interest in this work, his willingness to help out at all times despite the long periods of lull,
• Gunnar Gustafson, former head of the Department of Oral Pathology, for sharing his great knowledge and enthusiasm in research with me and supporting me with laboratory facilities. Furthermore, of course, Freja Gustafson for help with practical things,
• Jan Carlsson, head of the Department of Oral Microbiology, for his support both in a theoretical and practical sense,
• Roger Henriksson, my friend, for stimulating collaboration and invaluable discussions,
• Thorild Ericson, head of the Department of Cariology, for use of laboratory facilities and nice collaboration,
• Göran Hallmans, head at the Department of Nutritional Research, for invaluable help with all kinds of practical facilities that have been necessary for the progress of this work,
• Kjell Asplund for valuable discussions,
• Kerstin Berg, Britta Lindgren and Ingrid Boström for excellent technical assistence and invaluable help with all animal experiments,
• Margareta Jonsson, Kerstin Kristiansson, Margareta Ragnarsson, Rolf Sjöström and Ulla Öhman at the Biochemical Laboratory, Dental Faculty, for help with analysis,
• Birgitta Nilsson, Christina Bonnedahl, Inga Hamberg and Margareta Widman for assistance with saliva collection,
• Ingrid Strand, Kaj Strand and Ingegärd Söderström for careful handling with the experimental animals,
• Margareta Holmgren for skilful drawing of the figures,
41

• and finally my family, who allowed me to use much of my spare time for preparing this thesis.
This work was supported by the Faculties of Medicine and Odontology, University of Umeå, the Swedish Diabetes Association and the Swedish Dental Society.
42

REFERENCES
Abe K, Yokota Y, Dawes C. Effects o f parasympathomimetic and sympathomimetic drugs on the secretion and composition of rat sublingual saliva. J Dent Res 1982;61:52-56.
Anderson LC. Effects of alloxan diabetes and insulin in vivo on rat parotid gland. Am J Physiol 1983; 245:G431 — G437.
Anderson LC, Garrett JR. Lipid accumulation in the major salivary glands of streptozotocin-diabetic rats. Arch Oral Biol 1986;31:469-475.
Anderson LC, Johnson DA. Effects o f alloxan on rat parotid gland and saliva. Comp Biochem Physiol 1981; 70B-.725 —730.
Anderson LC, Shapiro BL. The effect o f alloxan diabetes and insulin on the rate o f protein synthesis in the rat submandibular gland. Horm Metab Res 1980; 12:47 - 5 1 .
Arnold RR, Russell JE, Devine SM, Adamson M, Pruitt KM. Antimicrobial activity o f the secretory innate defense factors lactoferrin, lactoperoxidase and lysozyme. In: Guggenheim B, ed. Cariology Today. International Congress. Zürich 1983. Basel: Karger, 1984:75-88.
Baumann H, Meyer P, Winter K, Lorenz G. Sialochemische und morphologische Untersuchungen der Glandula sub- mandibularis des Diabetikers — ein Beitrag zur diabetischen Sialadenose. Laryngol Rhinol Otol (Stuttg) 1985;64: 542 — 546v
Berglund O, Hallmans G, Nygren C, Täljedal I-B. Effects of diets rich and poor in fibres on the development o f hereditary diabetes in mice. Acta Endocrinol 1982; 100: 5 5 6 -5 6 4 .
Bernarde MA, Rosen FS, Hoppert CA, Hunt HR. A method for the collection of large quantities o f rat saliva. J Dent Res 1956;35:236-237.
Bernick SM, Cohen DW, Baker L, Laster L. Dental disease in children with diabetes mellitus. J Periodontol 1975; 46:241-245.
Birkhed D. När är kosten kariogen. Swed Dent J 1983;75: 1321-1327.
Bissada NF, Schaffer EM, Lazarow A. Effect of alloxan diabetes and local irritating factors on the periodontal structures o f the rat. Periodontics 1966;4:233-240.
Boackle RJ, Suddick RP. Salivary proteins and oral health. Mechanisms of secretion of saliva. In: Menaker L, ed. The biological basis o f dental caries. New York: Harper and Row, 1980:113-128.
Booth DA. Some characteristics o f feeding during strepto- zotocin-induced diabetes in the rat. J Comp Physiol Psychol 1972;80:238-249.
Bowen WH. Impact on research. In: Guggenheim B, ed. Cariology Today. International Congress. Zürich 1983. Basel: Karger, 1984:49-55.
Bowen WH, Pearson S, Young DA. An animal model to study root surface caries. Caries Res 1986;20:192 (Abstract).
Brandtzaeg P. Role o f antibodies in saliva: facts and extrapolations. In: Menaker L, ed. The biological basis o f dental caries. New York: Harper and Row, 1980:89-97.
Brodsky WA, Nelson N, Guest GM. Influence of food intake on ketosis, mineral balance and survival o f alloxan-diabetic rats. Metabolism 1952;1:68-79.
Bylund DB, Martinez JR, Pierce DL. Regulation o f autonomic receptors in rat submandibular gland. Mol Pharmacol 1982;21:27-35.
Campbell MJA. Glucose in the saliva of the non-diabetic and the diabetic patient. Arch Oral Biol 1965;10:197-205.
Carlsson J. Regulation o f sugar metabolism in relation to the feast-and-famine existence of plaque. In: Guggenheim B, ed. Cariology Today. International Congress. Zürich 1983. Basel: Karger, 1984:205-211.
Carpenter RG, Grossman SP. Plasma fat metabolites and hunger. Physiol Behav 1983;30:57-63.
Cianciola LJ, Park BH, Bruck E, Mosovich L, Genco RJ. Prevalence o f periodontal disease in insulin-dependent diabetes mellitus (juvenile diabetes). J Am Dent Assoc 1982;104:653-660.
43

Cohen DW, Friedman LA, Shapiro J, Kyle GC, Franklin S. Diabetes mellitus and periodontal disease: Two-year longitudinal observations. J Periodontol 1970;41:709-712.
Colton T. Statistics in medicine. Boston: Little, Brown and Company, 1974.
Conner S, Iranpour B, Mills J. Alteration in parotid salivary flow in diabetes mellitus. Oral Surg 1970;30:55-59.
Cudworth AG, Andreani D, Bodansky HJ, Squadrito G. Diabetes and its late complications. London: John Libbey, 1982.
Cutler LS, Pinney HE, Christian C, Rusotto SB. Ultrastruc- tural studies o f the rat submandibular gland in streptozoto- cin induced diabetes mellitus. Virchows Arch (Pathol Anat) 1979;382:301-311.
Dalstein JM, Ribes G, Campo P, Loubatières-Mariani MM. Effect of sodium dichloroacetate on dental caries in diabetic rats. Horm Metabol Res 1982;14:438-439.
Davidson D, Leibel BS, Berris B. Asymptomatic parotid gland enlargement in diabetes mellitus. Ann Intern Med 1969;70:31-36.
Dawes C. Inorganic constituents o f saliva in relation to caries. In: Guggenheim B, ed. Cariology Today. International Congress. Zürich 1983. Basel: Karger, 1984:70-74.
de Castro JM and Balagura S. Meal patterning in the strep- tozotocin-diabetic rat. Physiol Behav 1975;15:259-263.
DePalma J, Rosen S, Harper DS. Specific foods as etiologic factors in bone loss and root caries. J Dent Res 1983;62:295 (Abstract).
Donath K, Seifert G. Ultrastructural studies of the parotid glands in sialadenosis. Virchows Arch (Pathol Anatom) 1975;365:119-135.
Dziatkowiak H, Kowalska M, Denys A. Phagocytic and bactericidal activity o f granulocytes in diabetic children. Diabetes 1982;31:1041-1043.
Eastman BG, Johnson SB, Silverstein J, Spillar RP, Mc- Callum M. Understanding of hypo- and hyperglycemia by youngsters with diabetes and their parents. J Pediatr Psychol 1983;8:229-243.
Elfving N-G, Ljunggren J-G, Tomson K. Symtomlösa tand- infektioner — en vanlig orsak till dålig sockerinställning hos diabetiker. Läkartidningen 1979;76:717-719.
ElGeneidy AK, Stallard RE, Fillios LC, Goldman HM. Periodontal and vascular alterations: Their relationship to the changes in tissue glucose and glycogen in diabetic mice. J Periodontol 1974;45:394-401.
Ellen RP, Banting DW, Fillery ED. Longitudinal microbiological investigation of a hospitalized population of older adults with a high root surface caries risk. J Dent Res 1985;64:1377- 1381.
Emmelin N. Nervous control of salivation. Ala J Med Sci 1981;18:294-299.
Englander HR, Jeffay AI, Fuller JB, Chauncey HH. Glucose concentrations in blood plasma and parotid saliva of individuals with and without diabetes mellitus. J Dent Res 1963 ;42:1246.
Ericson T, Rundegren J. Characterization of a salivary agglutinin reacting with a serotype c strain of Streptococcus mutans. Eur J Biochem 1983;133:255-261.
Ervasti T, Knuuttila M, Poh j amo L, Haukipuro K. Relation between control o f diabetes and gingival bleeding. J Periodontol 1985;56:154- 157.
Fejerskov O, Thylstrup A. Pathology of dental caries. In: Textbook of cariology. Thylstrup A, Fejerskov O. eds. Copenhagen: Munksgaard, 1986:204-234.
Feller RP, Shannon IL. The secretion of glucose by the parotid gland. J Dent Res 1975;54(Sp iss A):57 (Abstract).
Ficara AJ, Levin MP, Grower MF, Kramer GD. A comparison of the glucose and protein content of gingival fluid from diabetics and non-diabetics. J Periodontol 1975; 10:171-175.
Fitzgerald RJ, Larson RH. Age and caries susceptibility in gnotobiotic rats. Helv Odont Acta 1967;11:49-52.
Forbat LN, Collins, RE, Maskell GK, Sönksen PH. Glucose concentrations in parotid fluid and venous blood of patients attending a diabetic clinic. J R Soc Med 1981 ;74: 72 5 -7 2 8 .
Friedman MI. Hyperphagia in rats with experimental diabetes mellitus: A response to a decreased supply of utilizable fuels. J Comp Physiol Psychol 1978;92:109-117.
Freund A, Johnson SB, Rosenbloom A, Alexander B, Ap- person Hansen C. Subjective symptoms, blood glucose estimation, and blood glucose concentrations in adolescents with diabetes. Diabetes Care 1986;9:236-243.
Fuchs G, Gawell B-M, Lidhem B-M. Quantitative determination of low-molecular carbohydrates in foods by gas- liquid chromatography. Swed J Agric Res 1974;4:49-52.
Gallacher DV, Petersen OH. Stimulus-secretion coupling in mammalian salivary glands. Int Rev Physiol 1983;28:1 — 52.
Gislén G, Nilsson KO, Matsson L. Gingival inflammation in diabetic children related to degree of metabolic control. Acta Odontol Scand 1980;38:241-246.
44

Glavind L, Lund B, Löe H. The relationship between periodontal state and diabetes duration, insulin dosage and retinal changes. J Periodontol 1968;39:341-347.
Glickman I. The periodontal structures in experimental diabetes. NY J Dent 1946;16:226-251.
Golub LM, Nicoli G A, Iacono VJ, Ramamurthy NS. In vivo crevicular leukocyte response to a chemotactic challenge: inhibition by experimental diabetes. Infect Immun 1982;63:1013- 1020.
Gottsegen R. Dental and oral aspects o f diabetes mellitus. In: Ellenberg M, Rifkin H. Diabetes mellitus. New York: McGraw-Hill Book Company, 1970:760-779.
Guggenheim B, Lutz F. A simple model for root caries and alveolar bone recession in rats. Caries Res 1985; 19: 516-518 .
Gusberti FA, Syed SA, Bacon G, Grossman N, Loesche WJ. Puberty gingivitis in insulin-dependent diabetic children. I. Cross-sectional observations. J Periodontol 1983;54:714-720.
Gustafson GT, Lerner U. Bradykinin stimulates bone resorption and lysosomal-enzyme release in cultured mouse calvaria. Biochem J 1984;219:329-332.
Gustafson GT, Ljunggren Ö, Boonekamp P, Lerner U. Stimulation of bone resorption in cultured mouse calvaria by Lys-bradykinin (kallidin), a potential mediator of bone resorption linking anaphylaxis processes to rarefying osteitis. Bone and Mineral 1986;1:267-277.
Gustafsson BE, Quensel CE, Lanke LS, Lundquist C, Grahnen H, Bonow B, Krasse B. The Vipeholm dental caries study. The effect of different levels of carbohydrate intake on caries activity in 436 individuals observed for five years (Sweden). Acta Odontol Scand 1954;11:232-364.
Hand AR, Weiss RE. Effects of streptozotocin-induced diabetes on the rat parotid gland. Lab Invest 1984;51 : 42 9 -4 4 0 .
High AS, Sutton J, Hopper AH. A morphometric study of submandibular salivary gland changes in streptozotocin-induced diabetic rats. Arch Oral Biol 1985;30:667-671.
Henriksson R. Beta-1 and beta-2 adrenoreceptor agonists have different effects on rat parotid acinar cells. Am J Physiol 1982;242:G481 — G485.
Henriksson R, Carlsöö B, Danielsson Å, Idahl L-Å. Characterization of the rat parotid beta-adrenoreceptor. Br J Pharmacol 1981;72:271-276.
Hoppenbrouwers PMM, Driessens FCM, Borggreven JMPM. Vulnerability of unexposed human dental roots to demineralization. Caries Res 1986;20:190 (Abstract).
Imai A, Kurihara Y. Endogenous infection in mice with streptozotocin-induced diabetes. A feature of bacterial translocation. Can J Microbiol 1984;30:1344-1348.
Irons WB, Schaffer EM. Circadian rhythms in the oral and gingival epithelium of the rat. Periodontics 1966; 4:316-321.
Johansen K, Aaby-Svendsen P, Lorup B. Variations in renal threshold for glucose in type 1 (insulin-dependent) diabetes mellitus. Diabetologia 1984;26:180-182.
Johnson DA, Sreebny LM. Effect of increasing the bulk content of the diet on the rat parotid gland and saliva. J Dent Res 1982;61:691-696.
Jordan HV, Keyes PH, Bellack S. Periodontal lesions in hamsters and gnotobiotic rats infected with actinomyces of human origin. J Periodont Res 1972;7:21-28.
Jordan HV, Sumnay DL. Root surface caries: review of the literature and significance of the problem. J Periodontol 1973;44:158-163.
Kabadi UM. Nutritional therapy in diabetes. Rationale and recommendations. Diabetes Therapy 1986;79:145-156.
Katz RV, Hazen SP, Chilton NW, Mumma RD. Prevalence and intraoral distribution of root caries in an adult population. Caries Res 1982;16:265-271.
Keyes PH. Recent advances in dental caries research, bacteriology, bacteriological findings and biological implications. Int Dent J 1962;12:443-464.
Kissileff HR. Oropharyngeal control of prandial drinking. J Comp Physiol Psychol 1969;67:309-319.
Kitamura M, Kiyak HA, Mulligan K. Predictors o f root caries in the elderly. Community Dent Oral Epidemiol 1986;14:34-38.
Kjellman O. Secretion rate and buffering action of whole mixed saliva in subjects with insulin-treated diabetes mellitus. Odontol Revy 1970a;21:159 — 168.
Kjellman O. The presence o f glucose in gingival exudate and resting saliva of subjects with insulin-treated diabetes mellitus. Swed Dent J 1970b;63:11 - 19.
Kjellman O, Henriksson C-O, Berghagen N, Andersson B. Oral conditions in 105 subjects with insulin-treated diabetes mellitus. Swed Dent J 1970c;63:99-110.
Korec R. Experimental diabetes mellitus in rat. Bratislava: Publishing House of the Slovak Academy of Sciences, 1967:112-115.
König KG. Feeding regimes and caries. J Dent Res 1970; 49(suppl):1327— 1333.
45

Langley LL, Gunthorpe CH, Beall WA. Salivary glucose threshold. Am J Physiol 1958;192:482-484.
Larkin JG, Frier BM, Ireland JT. Diabetes mellitus and infection. Postgrad Med J 1985;61:233-237.
Leeper SH, Kalkwarf KL, Strom EA. Oral status o f “ controlled” adolescent type I diabetics. J Oral Med 1985; 40:127-133.
Lin JH, Duffy JL, Roginsky MS. Microcirculation in diabetes mellitus. A study of gingival biopsies. Hum Pathol 1975;6:77-96.
Listgarten MA, Ricker FH, Laster L, Shapiro, Cohen DW. Vascular basement lamina thickness in the normal and inflamed gingiva o f diabetics and non-diabetics. J Periodon- tol 1974;45:676-684.
Listgarten MA. Pathogenesis o f periodontitis. J Clin Perio- dontol 1986;13:418-425.
Lithner F, Hägg E. Cutaneous reactions of alloxan-diabetic rats to local thermal trauma. Upsala J Med Sci 1975;80: 9 9 -1 0 2 .
Liu FTY, Lin HS. Role o f insulin in body growth and growth of salivary glands in rats. J Dent Res 1969; 48:559-567.
Luna LG. Manual o f Histologic Staining Methods of the Armed Forces Institute of Pathology. New York: McGraw- Hill Book Company, 1968.
Manchester KL. Protein metabolism. In: Ellenberg M, Rifkin H, eds. Diabetes mellitus. Theory and practice. New York: McGraw-Hill, 1970:28-77.
Mandel ID. Sialochemistry in disease and clinical situations affecting salivary glands. CRC Crit Rev Clin Lab Sci 1980; 11:321-366.
Mangos JA, Maragos N, McSherry NR. Micropuncture and microperfusion study of glucose excretion in rat parotid saliva. Am J Physiol 1973;224:1260-1264.
Manouchehr-Pour M, Bissada NF. Periodontal disease in juvenile and adult diabetic patients: A review of the literature. J Am Dent Assoc 1983;107:766-770.
Marder MZ, Abelson DC, Mandel ID. Salivary alterations in diabetes mellitus. J Periodontol 1975;46:567-569.
Martinez JR, Cassity N. Effect o f transport inhibitors on secretion by perfused rat submandibular gland. Am J Physiol 1983;245:G711 — G716.
Mashimo PA, Yamamoto Y, Slots J, Park BH, Genco RJ. The periodontal microflora of juvenile diabetics. Culture, immunofluorescence, and serum antibody studies. J Periodontol 1983;54:420-430.
Matsson L, Koch G. Caries frequency in children with controlled diabetes. Scand J Dent Res 1975;83:327-332.
Matsumura T. Analyses of monosaccharides in parotid saliva obtained from normal and diabetic animals. J Osaka Univ Dent Soc 1979;24:40-53.
Molnar S, Molnar I. Observations of dental disease among prehistoric populations o f Hungary. Am J Phys Anthropol 1985;67:51-63.
Murakami H. Changes in activities o f several enzymes for carbohydrate metabolism in rat submaxillary gland in response to experimental diabetes and insulin treatment. J Nihon Sch Dent 1974;16:91-94.
Muratsu K, Morioka T. Levels o f salivary lysozyme, lacto- peroxidase, and lactoferrin in diabetic hamsters. Infect Immun 1985;48:389-394.
Murrah VA. Diabetes mellitus and associated oral manifestations: a review. J Oral Pathol 1985;14:271-281.
Newbrun E. Sucrose in the dynamics o f the carious process. Int Dent J 1982a;32:13 — 23.
Newbrun E. Sugar and dental caries: A review of human studies. Science 1982b;217:418-423.
Newbrun E. Diet and dental caries. In: Guggenheim B, ed. Cariology Today. International Congress. Zürich 1983. Basel: Karger, 1984:75-88.
Nichols C, Laster LL, Bodak-Gyovai LZ. Diabetes mellitus and periodontal disease. J Periodontol 1978;49:85-88.
Nyvad B, Fejerskov O. Root surface caries: clinical, histo- pathological and microbiological features and clinical implications. Int Dent J 1982;32:312-326.
Ottlecz A, Koltai M, Geese A. Plasmakinin system in alloxan-diabetic rats. Adv Biosci 1979;17:57-63.
Page RC. Gingivitis. J Clin Periodontol 1986;13:345-355.
Pennebaker JW, Cox DJ, Gonder-Frederick L, Wunsch MG, Evans WS, Pohl S. Physical symptoms related to blood glucose in insulin-dependent diabetics. Psychosom Med 1981;43:489-500.
Potter AJ, Steward MC, Case RM. Effect o f Acetylcholine concentration on non-electrolyte secretion by the perfused rabbit mandibular salivary gland. In: Case RM, Lingard JA, Young JA, eds. Secretion. Mechanisms and control. Manchester: Manchester University Press, 1984:137- 141.
46

Ramamurthy NS, Siegel M, Iacono VJ, Golub LM. Leukocyte response in the gingival crevice o f the diabetic rat. J Periodont Res 1979;14:289-296.
Rao KS, Rao YK. Parotid biopsies in young diabetics. J Indian Med Assoc 1979;72:77-79.
Ravald N, Hamp S-E. Prediction of root surface caries in patients treated for advanced periodontal disease. J Clin Periodontol 1981;8:400-414.
Ravald N, Hamp S-E , Birkhed D. Long-term evaluation of root surface caries in periodontally treated patients. J Clin Periodontol 1986;13:758-767.
Rayfield EJ, Ault MJ, Keusch GT, Brothers MJ, Nechemias C, Smith H. Infection and diabetes: the case for glucose control. Am J Med 1982;72:439-450.
Reuterving C-O. Pilocarpine-stimulated salivary flow rate and salivary glucose concentration in alloxan-diabetic rats. Acta Physiol Scand 1986;126:511-515.
Rusotto SB. Asymptomatic parotid gland enlargement in diabetes mellitus. Oral Surg 1981;52:594-598.
Saadoun AP. Diabetes and periodontal disease: A review and update. J West Soc Periodont Abstr 1980;28:116—139.
Sarnat H, Eliaz R, Feiman G, Flexer Z, Karp M, Laron Z. Carbohydrate consumtion and oral status of diabetic and non-diabetic young adolescents. Clin Prev Dent 1985;7:20-23.
Schamschula RG, Barmes DE, Keyes PH, Gulbinat W. Prevalence and interrelationships of root surface caries in Lufa, Papua New Guinea. Community Dent Oral Epidemiol 1974;2:295-304.
Schneir ML, Ramamurthy NS, Golub LM. Extensive degradation of recently synthesized collagen in gingiva of normal and streptozotocin-induced diabetic rats. J Dent Res 1984;63:23-27.
Shannon IL, Prigmore JR, Brooks RA. Glucose concentrations in parotid fluid and blood serum following intravenous glucose loading. Oral Surg 1960;13:1010-1012.
Sharon A, Ben-Aryeh H, Itzhak B, Yoram K, Szargel R, Gutman D. Salivary composition in diabetics. J Oral Med 1985;40:23-26.
Sjöstrand FS. Electron Microscopy of Cells and Tissues. Vol. 1, London: Academic Press 1967:155-175.
Spengler J. Ein Apparat zur quantitatativen fortlaufenden Registrierung der Nahrungs- und Wasseraufnahme von Ratten. Helv Physiol Acta 1960;18:50-55.
Sterky G, Kjellman O, Högberg O, Löfroth A-L. Dietary composition and dental disease in adolescent diabetics. Acta Pediat Scand 1971;60:461-464.
Suddick RP, Hyde RJ, Feiler RP. Salivary water and electrolytes and oral health. In: Menaker L. ed. The biological basis o f dental caries. New York: Harper and Row, 1980: 132-146.
Sweeney EA, Shaw JH, Rubin RP. Effect o f alloxan diabetes on fluoride retention and caries incicence in rats. J Dent Res 1962;41:866-874.
Sznajder N, Carraro JJ, Rugna S, Sereday M. Periodontal findings in diabetic and non-diabetic patients. J Periodontol 1978;49:445-448.
Takai N, Uchihashi K, Yoshida Y, Kakudo Y. Salivational and histological damage of submandibular and sublingual glands in streptozotocin-induced diabetic rats. J Osaka Dent Univ 1983a; 17:65 — 72.
Takai N, Yoshida Y, Kakudo Y. Secretion and re-absorption of glucose in rat submandibular and sublingual saliva. J Dent Res 1983b;62:1022-1025.
Takai N, Shinohara M, Yoshida Y, Mori M, Kakudo Y. Studies on saliva in ODU plaque-susceptible rats having experimental gingivitis. J Periodont Res 1985;20:317-320.
Tamarin A, Sreebny LM. The rat submaxillary salivary gland. A correlative study by light and electron microscopy. J Morphol 1965;117:295-352.
Tenovuo J, Lehtonen O-P, Viikari J, Larjava H, Vilja P, Tuohimaa P. Immunoglobulins and innate antimicrobial factors in whole saliva of patients with insulin-dependent diabetes mellitus. J Dent Res 1986a;65:62-66.
Tenovuo J, Alanen P, Larjava H, Viikari J, Lehtonen O-P. Oral health o f patients with insulin-dependent diabetes mellitus. Scand J Dent Res 1986b;94:338-346.
Tenovuo J, Månsson-Rahemtulla B, Pruitt KM, Arnold RR. Inhibition of dental plaque acid production by salivary lactoperoxidase antimicrobial system. Infect Immun 1981;34:208-214.
Tervonen T, Knuutila M. Relation of diabetes control to periodontal pocketing and alveolar bone level. Oral Surg 1986;61:346-349.
Theilade A, Birkhed D. Diet and dental caries In: Textbook of cariology. Thylstrup A, Fejerskov O. eds. Copenhagen: Munksgaard, 1986:131 — 166.
Thomas DW, Scharrer E, Mayer J. Effects of alloxan induced diabetes on the feeding patterns of rats. Physiol Behav 1976;17:345-349.
47

Ulrich KH. Mundspeichel und Zuckerkrankheit. Zahn Mund Kieferheilkd 1961;35:353-360.
Van Dyke TE, Levine MJ, Genco RJ. Neutrophil function and oral disease. J Oral Pathol 1985;14:95-120.
Van Houte J. Bacterial specificity in the etiology of dental caries. Int J Dent Res 1980;30:305-326.
Vehkalahti M, Rajala M, Tuominen R, Paunio I. Prevalence of root caries in the adult finnish population. Community Dent Oral Epidemiol 1983;11:188-190.
Vogt K, Zahl J. Über Einflüsse von Diabetes und Geschlecht auf die Sekretion der Glandula parotis des Menschen. Archiv für klinische und experimentelle Ohren-, Nasen- und .Kehlkopfheilkunde 1973;203:310-324.
Von Ahrens G. Über die alimentäre Beeinflussbarkeit der Glukose-, Phosphat- und Kalziumkonzentration in Blut und Speichel. Dtsch Zahnaerztl Z 1971;26:16-21.
Weibel ER. Stereological methods. Practical methods for biological morphometry. Vol. 1. London: Academic Press, 1979.
Weibel ER, Knight BW. A morphometric study on the thickness of the pulmonary air-blood barrier. J Cell Biol 1964;21:367-384.
Weisberger DMD, Nelson CT, Boyle PE. The development of caries in the teeth of albino rats following extirpation of the salivary glands. Am J Orthodont Oral Surg 1940;26:88.
Williamson JR, Kilo C. Capillary basement membranes in diabetes. Diabetes 1983;32:96-100.
Wolf J. Dental and periodontal conditions in diabetes mellitus. Academic dissertation. University o f Helsinki. Proc Finnish Dent Soc 1977;73:Suppl 6.
Young JA, Cook DI. Fluid and electrolyte secretion. Paper presented at the 10th international conference on oral biology in the regime of I ADR — Saliva and salivary glands. Amsterdam, The Netherlands, 1986.
Young JA, Case RM, Conigrave AD, Novak I, Thompson CH. Secretory processes in the perfused rabbit mandibular gland. Adv Physiol Sci 1981;28:35-46.
Zilz J. Statistical observations on diabetes and pyorrhea alveolaris. Dent Cosmos 1915;57:102-103.
48