Safety of Maternal Immunization Against Pertussis: A ...Denis Macina Received: May 8, 2019/Published...
26
REVIEW Safety of Maternal Immunization Against Pertussis: A Systematic Review Caroline D’Heilly . Charlotte Switzer . Denis Macina Received: May 8, 2019 / Published online: September 17, 2019 Ó The Author(s) 2019 Abstract: The WHO recommends vaccination of all children against pertussis. However, newborn infants remain vulnerable to infec- tion. Pertussis vaccination during pregnancy has been introduced in several countries to protect newborns via transplacental transfer of maternal pertussis antibodies to the infant. We reviewed the impact of maternal pertussis vac- cination on the health of pregnant women, the developing fetus, and health of the newborn. We searched PubMed/MEDLINE, EMBASE, Sco- pus (Elsevier), Cochrane Database of Systematic Reviews, ProQuest, and Science Direct to iden- tify studies that assessed the safety of maternal pertussis vaccination. Twenty-seven English language publications published between Jan- uary 1995 and December 2018 were included in this review. Pregnant women receiving pertussis vaccines did not have increased rates of sys- temic or local reactions. There were no safety concerns with repeat vaccination with other tetanus-containing vaccines or their concomitant administration with influenza vaccines. Maternal pertussis vaccination did not adversely affect pregnancy, birth or neonatal outcomes. This review confirms the safety of maternal pertussis vaccination during pregnancy. Funding: Sanofi Pasteur. Plain Language Summary: Plain language summary available for this article. Keywords: Maternal immunization; Pertussis; Pregnancy; Vaccine; Whooping cough PLAIN LANGUAGE SUMMARY Newborn infants are particularly vulnerable to whooping cough in the first few months after birth. When women are vaccinated against whooping cough during pregnancy, their anti- bodies are transferred to the fetus, which pro- tects the newborn infant from the disease. We summarized the published evidence of the safety of maternal immunization against whooping cough, both for the mother and infant. We found that vaccination against whooping cough was safe for both mothers and their newborn infants. Pregnant women were no more likely than non-pregnant women to experience injection site reactions or whole- body effects. There were no negative effects on the pregnancy, birth or the infant. Vaccination of pregnant women can be recommended for Enhanced Digital Features To view enhanced digital features for this article go to https://doi.org/10.6084/ m9.figshare.9742721. C. D’Heilly Á D. Macina (&) Sanofi Pasteur, Vaccines Epidemiology and Modeling, Lyon, France e-mail: denis.macina@sanofi.com C. Switzer Sanofi Pasteur, Pharmacoepidemiology, Toronto, Canada Infect Dis Ther (2019) 8:543–568 https://doi.org/10.1007/s40121-019-00265-6
Transcript of Safety of Maternal Immunization Against Pertussis: A ...Denis Macina Received: May 8, 2019/Published...

REVIEW
Safety of Maternal Immunization Against Pertussis:A Systematic Review
Caroline D’Heilly . Charlotte Switzer . Denis Macina
Received: May 8, 2019 / Published online: September 17, 2019� The Author(s) 2019
Abstract: The WHO recommends vaccinationof all children against pertussis. However,newborn infants remain vulnerable to infec-tion. Pertussis vaccination during pregnancyhas been introduced in several countries toprotect newborns via transplacental transfer ofmaternal pertussis antibodies to the infant. Wereviewed the impact of maternal pertussis vac-cination on the health of pregnant women, thedeveloping fetus, and health of the newborn.We searched PubMed/MEDLINE, EMBASE, Sco-pus (Elsevier), Cochrane Database of SystematicReviews, ProQuest, and Science Direct to iden-tify studies that assessed the safety of maternalpertussis vaccination. Twenty-seven Englishlanguage publications published between Jan-uary 1995 and December 2018 were included inthis review. Pregnant women receiving pertussisvaccines did not have increased rates of sys-temic or local reactions. There were no safetyconcerns with repeat vaccination with othertetanus-containing vaccines or their
concomitant administration with influenzavaccines. Maternal pertussis vaccination did notadversely affect pregnancy, birth or neonataloutcomes. This review confirms the safety ofmaternal pertussis vaccination duringpregnancy.Funding: Sanofi Pasteur.Plain Language Summary: Plain languagesummary available for this article.
Keywords: Maternal immunization; Pertussis;Pregnancy; Vaccine; Whooping cough
PLAIN LANGUAGE SUMMARY
Newborn infants are particularly vulnerable towhooping cough in the first few months afterbirth. When women are vaccinated againstwhooping cough during pregnancy, their anti-bodies are transferred to the fetus, which pro-tects the newborn infant from the disease. Wesummarized the published evidence of thesafety of maternal immunization againstwhooping cough, both for the mother andinfant. We found that vaccination againstwhooping cough was safe for both mothers andtheir newborn infants. Pregnant women wereno more likely than non-pregnant women toexperience injection site reactions or whole-body effects. There were no negative effects onthe pregnancy, birth or the infant. Vaccinationof pregnant women can be recommended for
Enhanced Digital Features To view enhanced digitalfeatures for this article go to https://doi.org/10.6084/m9.figshare.9742721.
C. D’Heilly � D. Macina (&)Sanofi Pasteur, Vaccines Epidemiology andModeling, Lyon, Francee-mail: [email protected]
C. SwitzerSanofi Pasteur, Pharmacoepidemiology, Toronto,Canada
Infect Dis Ther (2019) 8:543–568
https://doi.org/10.1007/s40121-019-00265-6

protection of vulnerable infants during theirfirst weeks of life.
INTRODUCTION
Pertussis affects individuals of all ages but isespecially concerning in infants, who accountfor most of the hospitalizations and deathsassociated with the disease [1]. A modelingstudy based on World Health Organization(WHO) data from 2014 estimated that 24.1million cases and 160,700 deaths could beattributed to pertussis among childrenaged\5 years. Of these, 5.1 million (21%) casesand 85,900 (53%) deaths occurred in infantsaged\1 year [2].
To reduce pertussis-related morbidity andmortality in infants and young children, theWHO recommends acellular pertussis (aP) orwhole-cell pertussis (wP) vaccination for allinfants, with the primary immunization seriesinitiated at 6 weeks, and no later than 8 weeksof age [3]. However, infants are particularlysusceptible to pertussis infection from multiplesources during the period between birth andstart of their primary immunization series [4–7].Studies have consistently documented highincidence rates and significant mortality inyoung infants [8–11]. For example, in the USA,the incidence of pertussis was 117.7/100,000person-years in infants aged\1 year between2005 and 2010, with the highest rate in thoseaged 2 or 3 months (235.3/100,000 person-yearsor 247.7/100,000 person-years, respectively) [8].Elsewhere, pertussis-related deaths were esti-mated to be 0.6 per 100,000 maternities forinfants aged\ 66 days in England during 2001and 2011 [11]. The WHO does not currentlyrecommend vaccination against pertussis before6 weeks of age due to paucity of data on efficacyand safety, and lack of stand-alone aP vaccine[3, 12]. Risk-management through cocooning,where close contacts of the infants are vacci-nated, has had limited success [3].
Maternal immunization during pregnancy,taking advantage of transplacental transfer ofpertussis antibodies [1, 3, 12], was proposed toindirectly protect neonates against pertussis.This strategy achieves high pertussis antibody
concentrations in infants [13], and is 64–93%effective in preventing disease among infantsaged\2 months [14–21]. Moreover, break-through disease among infants whose motherswere vaccinated during pregnancy was lesssevere than those born to unvaccinated moth-ers [22]. The WHO also suggests that vaccina-tion of pregnant women is likely to be the mosteffective and cost-effective strategy for diseaseprevention in infants too young to be vacci-nated [3].
Some patients and healthcare providers arehesitant to or do not vaccinate during preg-nancy because of perceived (vaccine) safety[23–25]. Other barriers to vaccination duringpregnancy from the patient and healthcareperspective include negative media, missedvaccination opportunity (immunization notoffered or requested), lack of vaccine stock,inadequate reimbursement, and limited patientinterest [26–31]. Evidence-based educationalprograms that emphasize vaccine safety duringpregnancy and protection against disease ininfancy help support vaccine confidence andrecommendations. To capture supporting evi-dence, we conducted a systematic review of thesafety of maternal pertussis vaccination (Tdapand Tdap-IPV vaccines) during pregnancy.
METHODS
Studies assessing pertussis vaccination duringpregnancy were identified from a systematicsearch of PubMed/MEDLINE, EMBASE, Scopus(Elsevier), Cochrane Database of SystematicReviews, ProQuest, and Science Direct. We alsoscanned the reference lists of identified publi-cations and searched ProQuest thesis, Clinical-trials.gov, relevant conference and congressabstracts, and the Trial Trove database. Theprotocol for this systematic review was regis-tered on PROSPERO (PROSPERO2016:CRD42016038317) [32].
Our initial search was restricted to Englishlanguage publications between January 1995and June 2016. Further searches were performedto capture relevant studies published betweenJuly 2016 and October 2018. We used a com-bination of keywords that included the
544 Infect Dis Ther (2019) 8:543–568

following: [1]: [(pertussis OR whooping cough)AND (vaccine OR Tdap OR immunization) AND(pregnancy OR pregnant OR pre-partum ORgestation OR maternal)], [2]: [1] AND (safety ORadverse event OR adverse reaction OR congen-ital abnormalities OR congenital disorder ORcongenital malformation OR birth defects ORteratogens OR teratogenic agent OR terato-genicity OR pregnancy outcome OR pregnancytermination OR congenital anomaly OR devel-opmental disorder OR adverse birth outcome).
PICOS (Patient Population or Problem,Intervention [treatment/test], Comparison[group or treatment], Outcomes, and Setting)criteria [33] were applied while consideringinterventional and observational studies inhumans. Pregnant women and their offspringconstituted the studied population. The inter-vention was pertussis immunization duringpregnancy and the infant series of vaccination.Comparison groups were either no vaccinationor standard of care vaccination, as well aspregnancy or no pregnancy. Outcomesreviewed were qualitative (nature, severity) andquantitative characterization of adverse events{number, frequencies, and relative measures[e.g. odds ratios (OR) and relative risk (RR)]} inpregnant women (including but not limited tolocal reactions and fever), in fetuses (includingbut not limited to spontaneous abortion, still-birth, premature birth, birth weight, fetalgrowth, congenital malformation), and ininfants prior to the first dose of primaryimmunization.
Reviews, meta-analyses, case reports, opin-ion pieces, letters to editors, and modelingstudies were excluded. We also excluded studieson vaccination program improvement, vaccineuptake, vaccine acceptability and perceptionstudies, and health economics studies.
A two-step process involving two indepen-dent reviewers at each step was employed toselect studies for inclusion in the review. Thefirst step included scanning titles and abstractsof retrieved references to select publicationsbased on their relevance to our review. Publi-cations of primary research studies reportingthe safety of pre-partum pertussis vaccinationwere retained for full-text review. The secondstep consisted of a full-text review of the article
to assess whether the report met the inclusionand exclusion criteria. Pre-structured MS Excelforms were used to extract relevant data fromthe included studies. Multiple factors includingheterogeneity in study designs, vaccines used,outcomes measured, measurement/analysismethods, and the background pertussis inci-dence precluded a meta-analysis of the safetyfindings of the included studies.
This article is based on previously conductedstudies and does not contain any studies withhuman participants or animals performed byany of the authors.
RESULTS
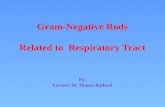
A total of 335 articles were identified from thecomprehensive search criteria, of which 27articles (summarized in Table 1) were includedin this review (Fig. 1).
Vaccine Reactogenicity in PregnantWomen
Fifteen studies reported vaccine reactogenicityamong pregnant women following immuniza-tion with Tdap or Tdap-IPV, among which ninewere prospective clinical trials [13, 34–41] andsix were database analyses [42–47] (Table 1). Themost commonly reported reactions were injec-tion site reactions, consistent with the Tdaplabel. While injection site reactions such aspain/tenderness, induration/swelling, itching,and erythema/redness were reported after Tdap/Tdap-IPV administration in most clinical stud-ies, pregnancy was not considered to haveincreased the rates of these events[13, 34, 36–38, 40]. However, moderate-to-sev-ere injection site pain was more frequent inpregnant women than nonpregnant women inone study [34]. Injection site reactions assessedover 7 days were more common after Tdap thanplacebo in one small clinical study [13] butoccurred at similar rates over 48 h in anotherslightly larger study [40]. Systemic and localreactions occurred at similar frequencies inpregnant women receiving Tdap and thosereceiving tetanus vaccines in two clinical stud-ies [35, 36].
Infect Dis Ther (2019) 8:543–568 545

Table1
Characteristics
andresults
ofthereview
edstudies
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Retrospectivedatabasereviews
Berensonetal.
[50]
Chartreview
[EMRof
PW
deliveringat
the
Universityof
Texas
MedicalBranchat
Galveston,G
alveston
County,USA
]
Nov
2012–Jun
2014
PW—singletonbirthat
C27
GW
andadequate
prenatal
care
Tdap(n
=1109)a
Tdap27–3
6GW
(n=835)
a
NoTdap(n
=650)
a
Databaseanalysisof
PWMaternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Nosignificant
differencesin
frequencyof
individualor
combined
maternaloutcom
esbforTdapvs.n
oTdap;
including
chorioam
nionitis(aOR=1.53
[95%
CI0.80–2
.90];p=0.19)
Adverse
birthandneon
atal
outcom
es:
Nosignificant
differencesin
frequencyof
individualor
combined
neonataloutcom
escforTdapvs.n
oTdap
Defectscwererare
andfrequencynotsignificantlydifferentfor
Tdapvs.n
oTdap
Forinfantsadmittedto
NIC
U,n
umberof
days
intheun
it
(p=0.001)
andfrequencyof
admission
forpreterm
birth
(p=0.03)or
anem
ia(p
=0.03)lower
forTdapvs.n
oTdap
Moroet
al.
[44]
Databasereview
[VAERS
database,U
SAvs.o
lder
publishedsafety
data]
Oct
2011–Jun
2015
(database)
(vs.Jan
2005–Jun
2010
[published
data])
TdapPW
withreported
AEs
followingTdap
Tdapat0–
13GW
(8.7%),
14–2
7GW
(12.0%
)or
C28
GW
(79.2%
);
followingACIP
recommendationsfor
Tdapin
PW
(n=392)
a
Tdap(Adacel,Sanofi
Pasteur[59.7%
],
Boostrix,GSK
[33.2%
],
unknow
n[7.1%])
(vs.
Tdapin
first[77%
],
second
[19%
]or
third
trim
ester[4%]before
recommendations
[n=132]
a )
Databaseanalysisof
PW
reportingAEs(vs.
publishedsafety
data)
Reactogenicity:
Mostfrequently:ISR
s(11.9%
),system
icreactions(e.g.,fever,chills;
4.3%
),musculoskeletalandconn
ective
tissue
disorders(3.6%),
andim
mun
esystem
disorders(e.g.,allergicreactions;3.6%
)
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Mostfrequently:oligohydramnios
(3.1%),stillbirth(2.8%),and
preterm
delivery(2.8%),spontaneousabortion
(1.0%)
Adverse
birthandneon
atal
outcom
es:
Death
(n=1),m
ajor
birthdefect
(n=4;
1.0%
)
Other:
Proportion
ofstillbirths
(2.8%
vs.1.5%)andISRs(11.9%
vs.4.5%)
increasedandspontaneousabortionsdecreased(16.7%
vs.1
.0%)
aftervs.b
eforeACIP
recommendations
546 Infect Dis Ther (2019) 8:543–568

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Kharbanda
etal.[42]
Cohortdatabase
review
[Claim
s,administrative
andEHRdata
from
7
VSD
sitesin
theUSA
f
andEHR-linked
vaccine
registries]
DeliveryJan
2007–N
ov
2013
PWwithlivebirth(gestational
trophoblasticdisease,ectopic
pregnancy,abortion,stillbirth,
orun
know
npregnancy
outcom
e)
Tdapduring
pregnancy
(any
trim
ester)
(n=53,885)
TdapC
20GW
(n=44,063)
NoTdap(n
=109,253)
Databaseanalysis
Reactogenicity:
Rateof
anyeventd0–
3days
(ARR=1.19
[95%
CI0.81–1
.73])or
anyneurologicalevente0–
42days
(ARR=0.98
[95%
CI
0.70–1
.37])similarafterTdapvs.n
oTdap(allevents
rate\
0.1%
)
Rateof
medicalvisitsforfeverwithin3days
increasedwithTdap
vs.n
oTdap(ARR=5.4[95%
CI2.1–
13.9])
Maternaladverseevents:
Rateof
proteinu
ria(ARR=0.81
[95%
CI0.6–
1.05])
orVTE
(ARR=0.65
[95%
CI0.40–1
.05])similarafterTdapvs.n
o
Tdap(rateforboth\
0.1%
)
Rateof
gestationaldiabetes(ARR=0.96
[95%
CI0.89–1.03]),
thrombocytopenia(ARR=0.85
[95%
CI0.73–0.98]),VTE
(ARR=0.58
[95%
CI0.35–0.97]),cardiacevents(ARR=0.90
[95%
CI0.70–1.15])notincreasedby
TdapC
20GW
vs.noTdap
Sukumaran
etal.[46]
Cohortdatabase
review
[Claim
s,administrative
andEHRdata
from
7
VSD
sitesin
theUSA
f
andEHR-linked
vaccine
registries]
DeliveryJan
2007–N
ov
2013
TdapPW
,aged14–4
9y,with
priortetanu
s-containing
vaccinedata,singleton
livebirth
(liveor
non-Tdap
tetanu
s-containing
vaccine
during
pregnancy,
trophoblasticdisease,
abortion,stillbirth,o
rectopic
pregnancy)
Tdapduring
pregnancy
with\
2yprior
tetanu
s-containing
vaccine(n
=4812)
Tdapduring
pregnancy
with2–
5yprior
tetanu
s-containing
vaccine(n
=9999)
Tdapduring
pregnancy
with[
5yprior
tetanu
s-containing
vaccine(n
=14,344)
Databaseanalysis
Reactogenicity:
Acutefever0–
3days
afterTdap:
0–3.5/10,000
PWin
each
group;
0–7days
afterTdap:
1.0–
6.2/10,000
PWin
each
group
Allergicreaction
0–3days
afterTdap:
1.0–
2.1/10,000
PW;
0–7days
afterTdap:
3.5–
4.2/10,000
PW
Localreaction
0–3days
afterTdap:
4.2–
11.2/10,000PW
;
0–7days
afterTdap:
12.5–1
7.0/10,000
PW
Fever,allergicreactions,or
localreactions
notsignificantlydifferent
inPW
who
received
tetanu
s-containing
vaccine\
2yvs.[
5y
or2–
5yvs.[
5y
Noreportsof
anaphylaxis,Arthusreactions,or
Guillain–B
arre
synd
rome
Maternaladverseevents,adversefetalou
tcom
espre-delivery,
birthandneon
atal
outcom
es:
Preterm
delivery(&
6.5%
),lowbirthweight(&
5%),SG
A
(&9%
)notsignificantlydifferentin
infantsof
PWwho
received
tetanu
s-containing
vaccine\
2yvs.[
5yor
2–5yvs.[
5y
Other:
MostPW
who
hadreceived
atetanu
s-containing
vaccine\
2y
(94%
)or
2–5y(85%
)previouslyhadreceived
Tdapvs.only17%
ofthe[
5ygroup
Infect Dis Ther (2019) 8:543–568 547

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Sukumaran
etal.[45]
Cohortdatabase
review
[Claim
s,administrative
andEHRdata
from
7
VSD
sitesin
theUSA
f
andEHR-linked
vaccine
registries]
Jan2007–N
ov
2013
PWaged
14–4
9y,singleton
livebirth,T
dapandinfluenza
vaccineduring
pregnancy(any
livevaccines
inpregnancy,
multiplegestations,
trophoblasticdisease,
abortion,stillbirth,o
rectopic
pregnancy,[
1tetanu
s
vaccineor
similarinfluenza
vaccinein
pregnancy)
Tdap20–3
7
GW
?influenza
vaccineconcom
itantly
during
pregnancy(any
trim
ester)
(n=8464)
Tdap20–3
7
GW
?influenza
vaccinesequentially
during
pregnancy(any
trim
ester)
(n=28,380)
Databaseanalysis
Reactogenicity:
Frequencyof
medicallyattend
edfever(\
4.5/10,000)andany
acutereaction
(\25.5/10,000)
(0–3
daysand0–7
days)didnot
differ
betweenPW
receivingTdapandinfluenza
vaccines
concom
itantly
vs.sequentially
(p[
0.3)
There
wereno
casesof
Arthusreaction
orGuillain–B
arre
Synd
rome
There
was
nointeractionbetweenacuteAEsandGW
atTdap
vaccination
Maternaladverseevents,adversefetalou
tcom
espre-delivery,
birthandneon
atal
outcom
es(N
=4554
vs.4440):
Preterm
delivery(&
7%),lowbirthweight(&
6%),SG
A
(&10%)notsignificantlydifferentin
infantsof
PWwho
received
Tdapandinfluenza
vaccineconcom
itantly
vs.
sequentially(p[
0.3)
Therewasno
interactionbetweenadversebirthoutcom
esandGW
atTdapvaccination
Datwaniet
al.
[51]
Databasereview
[VAERS
database,U
SA]
Jul1990–F
eb
2014
PWwithchorioam
nionitis
Any
vaccineduring
pregnancy(including
Tdap)
(n=31)
Databaseanalysis
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Chorioamnionitis:
Vaccinesmostfrequentlydocumentedin
reportsof
chorioam
nionitiswereinactivatedvaccines
(90%
),most
commonly2009
H1N
1inactivatedinfluenza
(32%
),quadrivalent
human
papillomavirus
(29%
),andTdap(26%
)
In58%
ofreports,PW
hadC
1risk
factor
forchorioam
nionitis
Additionaladverseoutcom
esspecified
butassociationwithspecific
vaccinenotreported
Adverse
birthandneon
atal
outcom
es:
Adverseoutcom
esspecified
butassociationwithspecificvaccinenot
reported
548 Infect Dis Ther (2019) 8:543–568

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Wanget
al.
[57]
Registryreview
[Sanofi
PasteurAdacelP
regnancy
Registry]
Jun2005–Jan
2011
PWreceivingAdacelduring
or\
30days
before
pregnancy
Tdap(Adacel,Sanofi
Pasteur)
(n=539)
a :
PhaseIV
studies(n
=49)
Prospectivereports
(n=480)
Retrospective
reports
(n=10)
Databaseanalysis
Maternalevents:
PhaseIV
studies:10%
non-seriousAEs,20%
SAEs,69%
noAEs
Prospectivereports:7%
non-seriousAEs,6%
SAEs,55%
noAEs,
33%
NR
Retrospective
reports:20%
SAEs,80%
noAEs
Maternaladverseevents,adversefetalou
tcom
espre-delivery,
birthandneon
atal
outcom
es:
PhaseIV
studies:86%
term
delivery,4%
preterm
delivery,4%
elective
abortion,2
%spontaneousabortion,and
4%lostto
follow-up
43infantswithno
congenitalanom
aly,1withright-side
hydronephrosis
Prospectivereports:19%
term
delivery,2%
preterm
delivery,\
1%
verypretermdeliverywith
nocongenitalabnormality,\
1%elective
abortion,
3%spontaneousabortion,
26%
lostto
follow-up,50%
awaitin
gpregnancyoutcom
e
Retrospective
reports:80%
term
delivery,20%
spontaneous
abortion
7infantsno
congenitalabnorm
ality,1infant
withpatent
foramen
ovaleandperipheralpulmonicstenosis
Other:
Dataraise
noconcerns
formaternalorinfant
health
followingTdap
durin
gpregnancy
Infect Dis Ther (2019) 8:543–568 549

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Morganet
al.
[55]
Cohortdatabase
review
[EPIC
electronicmedical
charting
system
at
Parkland
hospitaland
affiliatedclinics,Texas,
USA
]
Jun2013–Jul
2014
PWTdapC
32GW
(n=7152)
NoTdap(n
=226)
PriorTdap(\
5
y)?
TdapC
32GW
(n=1229)
TdapC
32GW
(single
dose)(n
=4159)
Databaseanalysis
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Frequencyof
stillbirths
andchorioam
nionitisforTdapvs.n
oTdap
notsignificantlydifferent
Preterm
birthratesincreasedwithno
Tdapvs.T
dap(AOR=1.88
[95%
CI1.25–2
.84])
Adverse
birthandneon
atal
outcom
es:
Frequencyof
major
malform
ations,5
-min
Apgar
score\
4,cord
bloodpH
B7,
andneonatalrequirem
entforventilation,
intraventricular
hemorrhage,sepsis,and
deathforTdapvs.n
o
Tdapnotsignificantlydifferent
Frequencyof
SGA(10%
vs.15%
,p=0.03)andlength
ofneonatal
hospitalization(3.9
says
vs.4
.7days,p
\0.001)
lower
forTdap
vs.n
oTdap
Deliveryandneonataloutcom
esgnotsignificant
differentbetween
wom
enwho
received
multipledosesof
Tdapvs.those
who
received
asingledose
Donegan
etal.
[53]
Cohortdatabase
review
[Clin
icalPractice
ResearchDatalinkdata
from
[650prim
arycare
practicesin
theUK]
Oct
2012–M
ar
2013
PWAny
pertussis-containing
vaccine30–3
6GW
(n=6185)
Novaccine(H
C)
(n=18,523)
Database
analysis?
comparison
withpublishednational
data
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Frequencyof
stillbirth,
preeclam
psia,eclam
psia,p
lacentaprevia,
cesarean
section,
prem
aturelabor(without
delivery),p
ostpartum
hemorrhagenotsignificantlydifferentbetweenTdapandno
Tdap
Observedstillbirthrate
in17,560
vaccinated
PWvs.expected
stillbirthratein
publishednationalstatisticsdataratio:0.69
(95%
CI0.23–1
.62)
Adverse
birthandneon
atal
outcom
es:
Intrauterine
grow
thretardation/lowbirthweight/weight\
2500
g
andneonataldeath(within7days)notsignificantlydifferent
betweenTdapandno
Tdap
550 Infect Dis Ther (2019) 8:543–568

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Kharbanda
etal.[54]
Cohortdatabase
review
[Adm
inistrativeand
EHRdata
from
2Kaiser
Perm
anente
VSD
sites
(NorthernandSouthern
Califo
rnia),USA
]
DeliveryJan
2010–N
ov
2012
PWaged
14–4
9y,singleton
livebirth
(C1livevaccine
during
pregnancy;Tdap,
B7days
afterestimated
pregnancystartor
B7days
before
delivery)
Tdap(Adacelin
majority)
during
pregnancy
(n=26,229)a
Second
?thirdtrim
ester
(92%
)
NoTdap(n
=97,265)a
Tdapbefore
pregnancy
(46%
)
Databaseanalysis
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Chorioamnionitis:
6.1%
vs.5
.5%
forTdapvs.n
oTdap;
ARR=1.19
(95%
CI
1.13–1
.26;
p\
0.001)
Tdapat27–3
6GW
vs.n
oTdapARR=1.11
(95%
CI1.03–1
.21;
p=0.009)
Hypertensivedisorder
ofpregnancy:
8.2%
vs.8.0%
forTdap\
20GW
vs.noTdap;
ARR=1.09
(95%
CI0.99–1
.20)
Preterm
delivery(\
37GW):
Tdapat
anytimeduring
pregnancynotassociated
withincreased
risk
ofpreterm
delivery(ARR=1.03
[95%
CI0.97–1
.09)
Tdapat27–3
6GW
vs.n
oTdapARR=0.88
(95%
CI0.80–0
.95;
p=0.002)
Adverse
birthandneon
atal
outcom
es:
Tdapat
anytimeduring
pregnancynotassociated
withincreased
risk
ofSG
A(ARR=1.00
[95%
CI0.96–1
.06)
Tdapat27–3
6GW
vs.noTdapARR=1.03
(95%
CI0.96–1
.10)
Shakib
etal.
[56]
Cohortdatabase
review
[EHRof
Interm
ountain
Health
care
Enterprise
DataWarehouse,U
SA]
May
2005–A
ug
2009
PWTdapduring
pregnancy
(n=138)
Firsttrim
ester(63%
),
second
trim
ester(17%
),
thirdtrim
ester(20%
)
NoTdap(n
=552)
Databaseanalysis
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Spontaneousor
elective
abortion:2.9%
vs.8
.9%
forTdapvs.n
o
Tdap
Stillbirth:
0vs.0
.9%
forTdapvs.n
oTdap
Preterm
livebirth(\
37GW):6.0%
vs.7.5%forTdapvs.noTdap
Nosignificant
differencesbetweenTdapandno
Tdap
Adverse
birthandneon
atal
outcom
es:
Noincreasedrisk
ofcongenitalabnorm
alitiesor
additionalhealth
problemsin
thefirstyear
oflifeforinfantsof
TdapPW
vs.n
o
TdapPW
Infect Dis Ther (2019) 8:543–568 551

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Zheteyeva
etal.[47]
Databasereview
[VAERS
database,U
SA]
Jan2005–Jun
2010
PWwho
received
Tdapduring
pregnancywithor
without
adverseevents
Tdap(Adacel,Sanofi
Pasteur[72%
],
Boostrix,GSK
[15.2%
],
unknow
n[12.9%
])
during
pregnancy(any
trim
ester)a(n
=132)
Firsttrim
ester(77%
)
Databaseanalysis
Reactogenicity:
ISRsin
4.5%
ofreports
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Mostfrequentlyreported:spontaneousabortion
(16.7%
)at
5–16
GW,9
–61days
afterTdap
Stillbirthin
2reportsandpreterm
deliveryin
3reports
Adverse
birthandneon
atal
outcom
es:
Isolated
adverseinfant
outcom
esin
4.5%
ofreports;major
birth
defect
reported
in1infant
(gastroschisis)
Other:
Noun
usualpattern
ofadversematernal,birthor
neonataloutcom
es
reported
Laytonet
al.
[43]
Databasereview
[Truven
MarketScan�
Com
mercialClaim
sand
Encountersinsurance
claimsdatabase]
2010–2
014
PWwithsingletonlivebirth
or
stillbirthborn
[26
GW
?
infants
TdapC
27GW
(n=123,780)
a
Tdap\
27GW
(n=25,037)a
TdapB
7days
postpartum
(n=59,040)a
NoTdap(n
=871,117)
a
Matched
newborns
(n=677,075)
a
Databaseanalysis
Reactogenicity:
Uncom
mon;mostfrequentlylocalpain
(24.22
per10,000
PW);
appeared
leastcommon
withTdapC
27GW
Feverreported
in6.2per10,000
PW
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Placentalabruption,
prem
atureruptureof
mem
branes,caesarian
section,
preeclam
psia/eclam
psia
generally
similarbetween
TdapC
27GW
vs.n
oTdapin
PW
Chorioamnionitis:
IPTW-weightedrisks:2.8%
–3.6%
TdapC
27GW
vs.n
oTdap:
RR=1.11
(95%
CI1.07–1
.15)
Tdap\
27GW
vs.n
oTdap:
RR=1.19
(95%
CI1.11–1
.28)
Postpartum
hemorrhage:
IPTW-weightedrisks:2.3%
–3.1%
TdapC
27GW
vs.n
oTdap:
RR=1.23
(95%
CI1.18–1
.28)
Tdap\
27GW
vs.n
oTdap:
RR=1.34
(95%
CI1.25–1
.44)
Adverse
birthandneon
atal
outcom
es:
Noincreasedrisk
ofadverseneonataloutcom
eswithTdapat
C27
GW
or\
27GW
vs.n
oTdap
552 Infect Dis Ther (2019) 8:543–568

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
DeSilvaet
al.
[52]
Databasereview
[Adm
inistrativeand
EHRdata
from
7VSD
sitesin
Califo
rnia,
Colorado,
Minnesota,
Oregon,
Washingtonand
Wisconsin,U
SA]
Jan2010–S
ep
2013
PWwithsingletonlivebirth,C
1
outpatient
visitduring
pregnancy,(Tdap\
8days
afterpregnancystart
or\
8days
before
delivery,
livevaccine)
Tdapduring
pregnancy
(n=45,008)a
Tdap27–3
6GW
(n=22,772)a
NoTdap(n
=152,556)
a
Databaseanalysis
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Chorioamnionitis:
Tdapvs.n
oTdapin
PW:6.4%
vs.5
.2%;ARR=1.23
(95%
CI
1.17–1
.28)
Tdap27–3
6GW
vs.n
oTdapin
PW:6
.3%
vs.5.3%;A
RR=1.20
(95%
CI1.14–1
.28)
Adverse
birthandneon
atal
outcom
es:
Transient
tachypneaof
newborn,n
eonatalsepsis,n
eonatal
pneumonia,respiratory
distresssynd
rome,newborn
convulsions,
orthecompositeof
anyof
theseoutcom
essimilarbetweenTdap
vs.n
oTdapin
PWandTdap27–3
6GW
vs.n
oTdapin
PW
Becerra-
Culqui
etal.[59]
Cohortdatabase
review
[KaiserPerm
anente
Southern
Califo
rnia
hospitals,USA
]
DeliveryJan
2011–D
ec
2014
PWwithnaturalconception
and
singletonlivebirth
at22–4
5
GW
Tdap(Adacel,Sanofi
Pasteur)
during
pregnancy
(interquartilerange
26–3
3GW)
(n=39,077)
NoTdap(n
=42,916)
Databaseanalysiswith
1.2–
6.5yof
follow-up
data
Adverse
birthandneon
atal
outcom
es:
Autism
spectrum
disorder:incidence
rateof
3.78/1000person-y
in
childrenof
vaccinated
PWvs.4.05/1000
person-y
inchildrenof
unvaccinated
PW;aH
R0.85
(95%
CI:0.77–0
.95)
Infect Dis Ther (2019) 8:543–568 553

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Griffinet
al.
[48]
Cohortdatabase
review
[NationalHealth
Index
(NHI)
Database
includingallpregnant
wom
enin
New
Zealand
]
2013
PWwithliveor
stillbirthC
20
GW
in2013
(birthweight\
400g,missing
maternalor
gestationalage,
livebirths\
28GW,n
ot
eligibleforTdapat
28–3
8
GW
in2013)
Tdap28–3
8GW
(Boostrix,GSK
)
(n=8178)a
NoTdap(n
=60,372)a
Databaseanalysis
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Gestationalhypertension,p
reeclampsia,intrauterinegrow
th
retardation,
postpartum
hemorrhage,gestationaldiabetes
mellitus,chorioamnionitis,p
lacentalabruption,
prem
ature
ruptureof
mem
branes,fetaldistress,m
aternalfeverbeforeor
after
labor,anem
iaduring
pregnancyandpurpura,maternaln
eurologic
disorderssimilarbetweenTdapvs.n
oTdap(aHR=0.85–1
.10
acrossoutcom
es)
Tdapassociated
withreducedrisk
ofpre-eclampsiawithsevere
features
(aHR=0.61;95%
CI0.39–0
.94),p
reterm
labor(0.32;
0.17–0
.62)
anddelivery(0.72;
0.63–0
.83),antenatalbleeding
(0.61;
0.49–0
.78)
Tdapassociated
withincreasedrisk
ofhospitalizationforlactation
disorders(1.63,
1.15–2
.33)
Chorioamnionitis:
Tdapvs.n
oTdap:
aHR=1.10
(95%
CI0.70–1
.75)
Postpartum
hemorrhage:
Tdapvs.n
oTdap:
aHR=1.05
(95%
CI0.96–1
.15)
One
maternaldeath(noTdapgroup);insufficientcasesof
eclampsiaandstillbirthin
Tdapgroupforanalysis
Sukumaran
etal.[60]
Case–controldatabase
review
[VSD
data
from
KaiserPerm
anente
NorthernCalifo
rnia,
Southern
Califo
rnia,
ColoradoandNorthwest,
andMarshfield
Clin
ic
ResearchFoun
dation
hospitals,USA
]
DeliveryJan
2004–Jun
e
2014
PWenrolledat
aVSD
site
with
C1prenatalcare
visit;their
infantsenrolledun
tilage
6mo
ordeath(livevaccineduring
pregnancy,multiplegestation,
birthat\
34GW,infant
withmajor
birthdefectsor
deathduring
delivery)
Matched
controlsforoutcom
es
ofinterest
25,222
casesof
hospitalized
infants,
25,222
matched
controls;
157infants
died,1
57matched
controls
Tdapand/or
influenza
vaccine
NoTdapand/or
influenza
vaccine
Conditionallogistic
regression
analysisto
estimateodds
of
maternalvaccination
in
matched
casesand
controls
Riskof
hospitalization:
aORforTdap:
0.94
(95%
CI0.88–1
.01;
p=0.09)
aORforTdapor
influenza
vaccine:0.97
(95%
CI0.90–1
.05;
p=0.44)
Riskof
death:
aORforTdap:
0.44
(95%
CI0.17–1
.13;
p=0.09)
aORforTdapor
influenza
vaccine:0.32
(95%
CI0.08–1
.24;
p=0.10)
Prospectivestu
dies
554 Infect Dis Ther (2019) 8:543–568

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Mun
ozet
al.
[13]
Randomized,d
ouble-blind,
placebo-controlled[N
IH
VTEU
sitesin
theUSA
(n=3:
Houston,
Durham,S
eattle)]
Oct
2008–M
ay
2012
PWaged
18–4
5y
Non-PW
age-matched
toPW
(previousTdapor
anytetanu
s-
containing
vaccinewithinthe
prior2y,high
risk
forobstetric
complications)
PW:T
dap(Adacel,Sanofi
Pasteur)
at30–3
2GW
Infants:DTaP-IPV
-Hib
(Pentacel)at
2,4,
6,12
mo(33PW
and
infants)
PW:Placebo(Tdap
[Adacel]postpartum
)
Infants:DTaP-IPV
-Hib
(Pentacel)at
2,4,
6,12
mo(15PW
and
infants)
Non-PW:Tdap(Adacel)
(n=32)
AEmonitoringin
clinical
trial(infantsforup
to
13mo)
Reactogenicity:
Frequencyof
anyISRafterTdapwas
notdifferentforPW
(78.8%
[95%
CI61.1–9
1.0]),postpartum
wom
en(80.0%
[95%
CI
51.9–9
5.7])andnonp
regnantwom
en(78.1%
[95%
CI
60.0–9
0.7])(p[
0.99)butwas
lower
afterplacebo(PW:20.0%
[95%
CI4.3–
48.1];postpartum
wom
en:18.2%
[95%
CI
7.0–
35.5]);usually
mild
andresolved
within72
h
Mostfrequently:localpain
([70%
pergroup;
p=0.94);swellin
g
anderythemainfrequent
(\13%
pergroup;
p[
0.3)
Frequencyof
anysystem
icsymptom
afterTdapwas
not
significantlydifferentforPW
(36.4%
[95%
CI20.4–5
4.9]),
postpartum
wom
en(73.3%
[95%
CI44.9–9
2.2])or
in
nonp
regnantwom
en(53.1%
(95%
CI34.7–7
0.9%
])(p
=0.055);
usually
mild
andself-lim
iting
Frequencyof
feverafterTdapwas
higher
inpostpartum
wom
en
(26.7%
[95%
CI7.8–
55.1])than
PW(3.0%
[95%
CI0.1–
15.8])
ornonp
regnantwom
en(9.4%
[95%
CI2.0–
25.0])
(p=0.04)
butwassimilarin
postpartum
wom
enreceivingTdapvs.placebo
(15.2%
[95%
CI5.1–
31.9];p=0.43)andin
TdapPW
and
Tdapnonp
regnantwom
en(p
=0.36)
Frequenciesof
headache,m
yalgia,and
malaise
notsignificantly
differentbetweengroups
(pC
0.35);headache
wasmostfrequent
(33.3%
and46.7%
forPW
andpostpartum
wom
en,respectively)
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Noneattributed
toTdap
Birth
andneon
atal
outcom
es:
Allliveborn,m
ostly
atterm
andby
vaginaldelivery
Nosignificant
differencesin
gestationalages,b
irth
weights,A
pgar
scores,n
eonatalexam
inations,com
plications,growth
or
developm
ent
Infect Dis Ther (2019) 8:543–568 555

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Regan
etal.
[39]
Cohort[Telephone
survey
ofPW
receivingTdap
and/or
TIV
inWestern
Australia,A
ustralia]
Apr
2015–Jun
2015
PWTdap(Adacel,Sanofi
Pasteur[76.9%
],
Boostrix,GSK
[23%
],
unknow
n[0.1%])
second
/third
trim
ester
(n=1257)
TIV
anytrim
ester(no
Tdap)
(n=1584)
Tdapthird
trim
ester?
TIV
any
trim
ester(n
=1506)
Telephone
survey
ofPW
receivingTdapand/or
TIV
Reactogenicity:
Frequencyof
anyreaction,fever,rigors,fatigue,vomiting,malaise,
myalgia,o
rmedicallyattend
edeventssimilarin
PWreceiving
Tdap,
TIV,o
rTdap?
TIV
(p[
0.1)
Frequencyof
ISRs(Tdap:
7.1%
,TIV:3.2%
,Tdap?
TIV:5.4%
;
p\
0.001forTdapvs.T
IV,p
=0.002forTdap?
TIV
vs.
TIV),rash
(0.9%,0
.3%,0
.3%;p=0.03,1
.00),h
eadache(2.8%,
4.3%
,3.9%;p=0.03,0
.58),and
congestion
(2.9%,4
.3%,3
.1%,
p=0.04,0
.07)
significantlydifferentforTdapvs.T
IV
Any
maternalAEafterTdapin
2015
morefrequent
inPW
who
hadalso
received
Tdapin
2011–2
012(13/70;18.6%
)than
those
who
hadnot(291/2693;
10.8%;p=0.04;OR=1.88
[95%
CI
1.02–3
.48])h
Adverse
birthandneon
atal
outcom
es:
Allwom
enwho
haddelivered
atfollow-uphadahealthyinfant
Hoang
etal.
[36]
Randomized,controlled[H
a
Nam
province
(3
villages),N
orthern
Vietnam
]
DeliveryFeb
2013–O
ct
2013
PWPW
:Tdap(Adacel,Sanofi
Pasteur,Canada)
18–3
6GW
(n=52)
Infants:DTaP-IPV
-Hib-
HepB(Infanrixhexa,
GSK
)at
age2,
3,4mo
Tetanus
vaccine(IVAC,
Vietnam
)(n
=51)
Infants:DTaP-IPV
-Hib-
HepB(Infanrixhexa,
GSK
)at
age2,
3,4mo
AEmonitoringin
clinical
trial
Reactogenicity:
23PW
experiencedC
1solicited
AEafterTdap(m
eanduration,
1.3days)and22
PWexperiencedC
1solicited
AEaftertetanu
s
vaccine(m
eanduration,1
.2days)
Mostcommon
adverseeventswerestiffness,swellin
gandinjection
site
itching
SeriousAEsreported
withTdap:
fever(n
=1)
andfatigue(n
=1)
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Prem
aturecontractions
[1moafterTdap(n
=2)
ortetanu
s
vaccine(n
=1)
Adverse
birthandneon
atal
outcom
es:
NoAEsrelatedto
vaccinationreported
556 Infect Dis Ther (2019) 8:543–568

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Maertensetal.
[37]
Controlledcohort[Five
hospitalsin
Antwerp,
Belgium
]
Feb2012–S
ep
2014
PWwithhealthylivebirths,no
pertussis-containing
vaccine
forC
10y
Tdap(Boostrix,GSK
)
mean28.6
GW
(PW:
57,infants(Infanrix
hexa,G
SK):55)
NoTdap(PW:42,
infants:26)
AEmonitoringin
clinical
trial
Reactogenicity:
Adverse
events,m
ostly
mild
andself-lim
iting,reported
by46
PW
afterTdap
Mostfrequent
AEswereinjectionsitestiffness(N
=42)andminor
injectionsiteswellin
g;feverreported
in1PW
afterTdap(1.75%
)
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
Ofthe
11seriousAEsiin
PWreceivingTdap,none
relatedto
Tdap
Three
SAEreported
inPW
notreceivingTdap
Adverse
birthandneon
atal
outcom
es:
SeriousAEsrequiringinfant
hospitalizationreported
afterTdap
(n=7)
andno
Tdap(n
=1)
j
Nocongenitaldisordersdetected
Petousis-
Harris
etal.[38]
Observational,cohort
[Primarycare
and
antenatalcentersin
North
Island
(3District
Health
Boards)or
South
Island
(Canterbury)
of
New
Zealand
]
North
Island
:
Jan
2014–Jun
2014
SouthIsland
:
Sep
2012–Jun
2014
PWwithC
1ultrasound
during
pregnancy,adequate
prenatal
care,±
TIV
Tdap(Boostrix,GSK
)at
28–3
8GW
(n=793)
k
ActiveAEmonitoringfor
upto
4weeks
after
vaccination
Reactogenicity:
Mostfrequent
ISRwas
pain
(mild-m
oderate:78.9%,severe:2.6%
);
swellin
g(7.6%)anderythema(5.8%)un
common
andresolved
in\
48hin
&50%
ofcases
System
iceventswerefever(2.1%),headache/dizziness(3.9%),
nausea/vom
iting(2.8%),fatigue(8.4%)andmyalgia/arthralgia
(3.0%)
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
SAEsin
31PW
(3.9%),23
resulting
inhospitalization(obstetric
bleeding
[4],hypertension
[2],infection[4],tachycardia[1],
preterm
labor[9],exacerbation
ofpre-existing
cond
ition[2],
preeclam
psia[1])
Adverse
birthandneon
atal
outcom
es:
Twoperinatald
eaths(congenitalabnormality[1],un
explained[1])
Wallset
al.
[58]
Observational,cohort
[Canterburyregion
of
New
Zealand
]
Sep2012–N
ov
2014
PWwithC
1ultrasound
during
earlypregnancy,adequate
prenatalcare,±
TIV
(fetus
withcongenital/severe
structural/chrom
osom
al
abnorm
alitiesduring
prenatal
screening)
Tdap(Boostrix,GSK
)
28–3
8GW
(403
PW?
408infants:
345followed
for12
mo,
63followed
for
6–12
mo)
a
Maternalreportsand
healthcare
provider
inform
ation
prospectivelycollected
Birth
andneon
atal
outcom
es:
94%
delivered
atterm
;6%
delivered
pre-term
(\37
GW)
Isolated
medicallysignificant
eventsin
10infants(2.5%);1stillborn
(reasonun
know
ndespitepostmortem)
Noevidence
ofincreasein
anyadverseneonatal/infantoutcom
evs.
baselin
epopulation
rates
Infect Dis Ther (2019) 8:543–568 557

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Villarreal
Perezet
al.
[40]
Randomized,d
ouble-blind,
parallelgroup,
placebo-
controlled[12outpatient
health
centersof
the
Nuevo
LeonHealth
Services,M
exico]
Sep2011–A
ug
2014
PWaged
18–3
8y,lowobstetric
risk,n
ormalanatom
ical
ultrasound
insecond
trim
ester(psychiatricor
severe
physicaldisease,drug
or
tobaccouse,historyof
severe
reactionsto
anyvaccineor
febrile
illnessin
the72
hprior
tovaccination,
immun
ization
againsttetanu
sand/or
pertussis\
2ypreviously)
Tdapat
30–3
2GW
(90
PW?
infants)
Placebo(81
PW?
infants)
AEmonitoringin
clinical
trial
Reactogenicity:
Uncom
mon,A
Esreported
in41%of
PWwithTdapand31%with
placeboin
first24
h;mostfrequentlylocalreactionsthat
had
resolved
by48
h
Mostcommon
within24
h:mild
localpain;similarwithTdapvs.
placebo(22%
vs.2
1%)
Fortneret
al.
[34]
Observational,cohort[Two
CDC-fun
dedCISA
centers(Vanderbilt
UniversityMedical
Center,DukeUniversity
Health
System
),USA
]
Jul2014–Jul
2015
PWaged
18–4
5ywithsingleton
pregnancyandTdap
vaccinationat
20–3
3GW
Controls:non-PW
aged
18–4
5y
Tdap(Adacelo
rBoostrix)
20–3
3GW
(374
PW)
Tdap(Adacelo
rBoostrix)
(225
non-PW
)
ActiveAEmonitoringfor
upto
4weeks
after
vaccination
Reactogenicity:
Localsymptom
sin
PWvs.n
on-PW:moderate/severe
pain
(17.9%
vs.1
1.1%
),tend
erness(19.0%
vs.1
6.9%
),swellin
g/induration
(5.6%
vs.5
.8%),erythema(5.6%
vs.5
.3%);each
eventsevere
in\
2%of
PWand\
3.5%
ofnon-PW
Moderate/severe
pain
was
morecommon
inPW
than
non-PW
System
icsymptom
sin
PWvs.n
on-PW:moderate/severe
fever
(0.5%
vs.2
.2%),feverishness(3.2%
vs.4
.0%),malaise
(10.4%
vs.
4.9%
),body
aches/myalgias(7.8%
vs.5.3%),headaches(7.2%
vs.
8.9%
);each
eventseverein\
1%of
PWand\
2.5%
ofnon-PW
Nowom
anrequired
medicalcare
foranyreaction
Moderate/severeandseverelocaland
system
icreactionsn
otaffected
byprevious
Tdapvaccination
558 Infect Dis Ther (2019) 8:543–568

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Halperinetal.
[35]
Randomized,single-blind,
parallelgroup,
Td-
controlled[C
entersin
Canada(H
alifax,
Montreal,Ottaw
a,
Calgary,E
dmonton,
Vancouver)]
Nov
2007–Jun
2011
and
Mar
2012–A
pr
2014
Health
yPW
aged
18–4
5y
atC
30GW,w
ithlowrisk
forcomplications
(history
of
significant
medicaldisorder,
receiptof
high-dosesystem
ic
corticosteroidsor,inprevious
5y,pertussisor
previous
Td/
Tdapor,w
ithin3mo,
blood
productsor
immun
oglobulin
,
except
rhesus
immun
oglobulin
or,w
ithin2weeks,any
vaccine,except
influenza,o
r
sensitivityto
anycomponent
ofTdor
Tdap)
Tdap(Adacel,Sanofi
Pasteur)
C30
GW
(n=135)
TdC
30GW
(n=138)
AEmonitoringfor8days
aftervaccination;
infant
developm
ental
testing(Bayley-III
Scales
ofInfant
and
Toddler
Development)
atage18
mo
Reactogenicity:
Injectionsite
pain
in[
80%
ofboth
groups;predom
inantly
mild
Erythem
a,swellin
gin
about10%–2
0%of
both
groups;
predom
inantly
mild
Muscleaches,fatigue,headache
in16.9%–3
4.4%
ofboth
groups;
predom
inantly
mild
Eventslesscommon
withTdapvs.T
d:mild
fatigue(13.3%
vs.
23.4%;p=0.041),m
ildmuscleaches(4.4%
vs.2
0.4%
;
p\
0.001)
Eventsmorecommon
withTdapvs.T
d:severemuscleaches(4.4%
vs.0
%;p=0.014)
Maternaladverseevents
andadversefetalou
tcom
espre-
delivery:
NoseriousAEsin
PWconsidered
relatedto
Tdapor
Tdexcept:
gestationalh
ypertension(n
=1Tdap)
andhemolysis,elevatedliver
enzymes,low
platelet
coun
t
synd
rome?
preeclam
psia?
prem
aturedelivery(n
=1Td)—
possiblyrelated
Adverse
birthandneon
atal
outcom
es:
Nodifferencesin
ratesof
congenitalabnorm
alitiesor
neonatal
complications
betweeninfantsof
TdapandTdPW
NoseriousAEsin
infantsconsidered
relatedto
Tdapor
Td
Nodevelopm
entaldifferencesbetweeninfantsof
TdapandTdPW
(3%
abnorm
alfin
dingsin
each
group)
Infect Dis Ther (2019) 8:543–568 559

Table1
continued
Autho
r,year
[references]
Stud
ydesign
[setting/data
source]
Recruitment/
stud
ydates
Inclusion(exclusion
)criteria
Intervention
s(num
berof
participants)
Metho
dsResults
Wanlapakorn
etal.[41]
Randomized,controlled
[KingChulalongkorn
Mem
orialHospital,
Bangkok,T
hailand
]
Apr
2015–S
ep
2016
Health
yPW
aged
18–4
5y,with
lowrisk
forcomplications;
infantsborn
after36
GW
and
weighing2500
g
PW:Tdap(Boostrix,
GSK
)26–3
6GW
(n=370)
ActiveAEmonitoringfor
7days
after
vaccination;
passiveAE
monitoringthereafter
Reactogenicity:
NoAEsreported
inthefirst30
min
aftervaccination
Mostfrequentlylocalpain
(76.2%
;mild:62.4%,m
oderate:13.8%)
then
low-grade
fever(5.1%),swellin
g(4.1%;mild:4.1%
),
erythema(1.4%,m
ild:1.4%
)
Not
affected
byreceiptof
previous
tetanu
s-containing
vaccine
Maternaladverse
eventsandadversefetalo
utcomes
pre-delivery:
NoseriousAEsin
PWconsidered
relatedto
Tdap
Gestationaldiabetes
(2.7%)or
hypertension
(1.4%),prem
ature
delivery(6.7%)andotherseriousAEsnotmorefrequent
than
reported
amongalldeliveriesin
hospital(N
=4636)
Not
affected
byreceiptof
previous
tetanu
s-containing
vaccine
Chorioamnionitis:0.5%
Adverse
birthandneon
atal
outcom
es:
NoseriousAEs(including
deaths,congenitaldefectsandbirth
asphyxia)in
infantsconsidered
relatedto
Tdap
Notaffected
bymaternalreceiptofprevioustetanus-containing
vaccine
ACIP
AdvisoryCom
mitteeon
Immun
izationPractices,AEadverseevent,ARRadjusted
rate
ratio/relative
risk,aHRadjusted
hazard
ratio,
aORadjusted
odds
ratio,
CIconfi
denceinterval,CDC
CentersforDisease
Control
and
Prevention,C
ISAClin
icalIm
mun
izationSafety
Assessm
ent,CNScentralnervoussystem
,EHRelectronichealth
record,E
MRelectronicmedicalrecords,GW
gestationalweeks,H
Chistoricalcontrol,IPTW
inverse-probability
of
treatm
entweights,ISR
injectionsitereaction,m
omonth(s),NICUneonatalintensivecareun
it,N
IHVTEUNationalInstituteof
Health
Vaccine
TreatmentEvaluationUnit,NRnotreported,O
Rodds
ratio,PW
pregnant
wom
en,R
R
relative
risk,S
AEseriousadverseevents,SGAsm
allforgestationalage,TIV
trivalentinfluenza
vaccine,VSD
Vaccine
Safety
Datalink,
VAERSVaccine
Adverse
Event
Reporting
System
,WAWestern
Australia,y
year(s)
aPW
couldhave
also
received
othervaccines,including
anyof
influenza,h
epatitisA,h
epatitisB,m
eningococcal,and
pneumococcalvaccine
bMaternalo
utcomesincluded
chorioam
nionitis,postpartum
endometritis,preterm
prem
atureruptureof
mem
branes,preterm
delivery(delivery\
37GW),andacompositeendpoint
includingtheseoutcom
es.M
odeof
deliveryand
need
forinductionwerealso
considered
cNeonataloutcomesincluded
lowbirthweight,verylowbirthweight,sm
allfor
gestationalage,A
pgarscore\
8at5min
oflife,admission
toNIC
U,and
birthdefects.Birth
defectsincluded
spinabifida,transpositionof
greatarteries,
atrioventricular
septaldefect,cleftpalate,cleftlip,and
diaphragmatichemia(all0–
2%frequencypergroup);Tetralogy
ofFallot,rectalandlargeintestinalatresia/stenosis,reductiondeform
ityof
upperlim
bs,and
gastroschisisnot
observed
dAny
eventincluded
allergicreaction,fever,m
alaise,seizure,alteredmentalstatus,o
rlocalor
otherreaction
eAny
neurologicaleventincluded
autonomicdisorders,cranialnervedisorders,CNSdegeneration/dem
yelin
atingcond
itions,p
eripheralneuropathy,Guillain–B
arre
synd
rome,meningoencephalitides,movem
entdisorders,paralytic
synd
romes,and
spinocerebellardisease
fKaiserPerm
anente
NorthernCalifo
rnia,S
outhernCalifo
rnia,C
oloradoandNorthwest(O
regonandWashington),M
arshfield
Clin
ic(W
isconsin),Group
Health
Cooperative
(Washington),and
Health
Partners(M
innesota)
gDeliveryandneonataloutcom
esincluded
gestationalageat
delivery,stillbirthandmajor
malform
ationrate,n
eonatalcare
admission,ventilation
requirem
ents,and
incidenceof
neonataldeath
hWom
enwereconsidered
tohave
received
aprevious
dose
ofTdaponlyifrecord
ofavaccinationduring
thearea’s2011–2
012parentalpertussisvaccinationprogram
couldbe
locatedon
theprogram
database
iSA
Esincluded
preeclam
psia,p
rematurecontractions,h
ypertension,
oligohydramnios,and
placenta
previa
jThe
8SA
Erequiringinfant
hospitalizationforatleast1hwereprem
aturedelivery,feveratbirth,hypoglycem
iaatbirth,pn
eumoniaatbirth,infectionattheageof
1months,infectionattheageof
5months,febrile
seizuresattheage
of2months,andextrem
evomitingat
theageof
5months(n
=1forall)
kTIV
administeredwithTdapin
27.5%
560 Infect Dis Ther (2019) 8:543–568

Most studies, irrespective of whether data-base analyses [42–46, 48] or clinical studies[13, 34, 36–39, 41] reported fever in womenwho received pertussis vaccination duringpregnancy; the incidence ranged from 0% to5.1% in Tdap vaccinated pregnant women(Table 1). Kharbanda et al. [42] found that Tdap-vaccinated pregnant women were 5.4-timesmore likely to experience medically attended(i.e. requiring a visit to a health care profes-sional) fever in the 3 days post-vaccination thanunvaccinated pregnant women in a large data-base analysis (adjusted incident rate ratio[AIRR] = 5.4 [95% CI 2.1–13.9]). In contrast, asmall clinical study by Munoz et al. [13] showedthat the frequency of fever in Tdap-vaccinatedpregnant women was comparable with thatfollowing placebo, and to that among Tdap-vaccinated non-pregnant women, but lowerthan that in women vaccinated postpartum. A
factor potentially contributing to differences inthe reported rate of fever was the timing ofvaccination. The rate of fever appears lower inwomen vaccinated C 27 weeks’ gestation thanin those vaccinated earlier (\ 27 weeks’ gesta-tion) or within 7 days postpartum (3.80 per10,000 pregnant women vs. 5.19 per 10,000 and11.69 per 10,000 women, respectively) [43].Database analyses and clinical studies thatreported other systemic adverse events follow-ing Tdap vaccination during pregnancy, such asheadache, nausea/vomiting, malaise, myalgiaand fatigue, found that pregnancy did notincrease the reported rate of these adverseevents [13, 34, 36–38, 40, 42].
The reactogenicity events reported werepredominantly mild and self-limiting. Twoclinical studies reported that either no [41]or\2% [34] of pregnant women experiencedserious injection site reactions after Tdap
Records iden�fied through database searching
(n = 335)
Addi�onal records iden�fied through other sources
(n = 3)
Records a�er duplicates removed(n = 194)
Records screened(n = 194)
Records excluded(n = 167)
No relevant results: (n = 154) Duplicates: (n = 13)
Full-text ar�cles assessed for eligibility
(n = 27)
Full-text ar�cles excluded
(n=0)
Studies included in review(n = 27)
Fig. 1 PRISMA diagram of results of search strategy
Infect Dis Ther (2019) 8:543–568 561

and\ 1% experienced serious systemic symp-toms [34]. Across individual reactogenicitysymptoms,\20% of pregnant women experi-enced moderate-to-severe events, commonlyinjection site pain or tenderness [34, 41].
Concerns about the safety of repeat vacci-nation with Tdap (or in women who had pre-viously received a tetanus-containing vaccine)at sometimes short intervals between successivepregnancies persist [49]. Regan et al. [39]reported a trend towards increased odds of sev-eral adverse event in women with a history ofTdap vaccination 3 years before the currentTdap vaccination during pregnancy (in2011–2012 vs. current year 2015), but myalgiawas the only specific event reported with sig-nificantly increased odds [odd ration; 4.92(1.11–21.83)]. The frequency of systemic andlocal reactions, including fever, among Tdap-vaccinated pregnant women who had received adose of tetanus-containing vaccine within 1–-5 years previously was similar to that in thosewho had no such vaccinations in two clinicalstudies [34, 41]. In addition, the rate of acuteadverse events reported in a database analysis,among pregnant women who received a teta-nus-containing vaccine\ 2 years and 2–5 yearswas similar to that reported in those vacci-nated[ 5 years previously [45].
The safety of concomitant maternal vacci-nation with Tdap and influenza vaccines duringpregnancy was assessed in two studies [39, 45].Regan et al. [39] found no evidence of enhancedsafety risks with concomitant Tdap and triva-lent influenza vaccination compared with Tdapvaccination, as reported by pregnant womenusing a variety of reactogenicity measures(Table 1). A large US database review found nodifferences in the frequency of medicallyattended fever or any acute reaction betweenpregnant women who received Tdap and influ-enza vaccines concomitantly compared withsequentially [45].
Maternal Adverse Events and Adverse FetalOutcomes Pre-delivery
Twenty-one publications were identified thatassessed maternal adverse events in women who
received Tdap during pregnancy and pregnancyoutcomes (Table 1). Of these, 15 were databaseanalyses [42–48, 50–57]. Chorioamnionitis wasidentified as slightly increased in pregnantwomen who received Tdap (relative risk 1.19;95% confidence interval [CI] 1.13–1.26) in a2010–2012 retrospective, observational, cohortstudy using data from two Vaccine SafetyDatalink sites [54]. Chorioamnionitis increasedby a marginally lesser extent in women vacci-nated between 27 and 36 gestational weeks(1.11; 95% CI 1.03–1.21). However, pre-termbirth (a major chorioamnionitis sequela) wasnot increased. Subsequently, similar resultswere reported from database analyses by Laytonet al. [43] and DeSilva et al. [52]; both analysesfound small but significant increases inchorioamnionitis in women vaccinated withTdap during pregnancy compared with unvac-cinated pregnant women [43, 52]. In contrast,other database analyses found no significantdifference in chorioamnionitis between womenwho did and did not receive the Tdap vaccineduring pregnancy [48, 50, 55], including thosewho received C 2 Tdap doses in the past 5 years[55]. An analysis of 31 chorioamnionitis casesamong 3389 pregnancy reports in the VaccineAdverse Event Reporting System (VAERS) data-base (between 1990 and 2014) identified that58% of cases were in women with pre-existingrisk factors [51]. Tdap (26%), H1N1 inactivatedinfluenza vaccine (32%) and the quadrivalenthuman papillomavirus vaccine (29%) accoun-ted for the majority of chorioamnionitis casesreported to the VAERS.
Other pregnancy outcomes, including pre-eclampsia/eclampsia, intrauterine growth retar-dation, premature labor/contraction, postpar-tum hemorrhage, placenta previa, elective andspontaneous abortions, oligohydramnios, pro-teinuria, venous thromboembolism, cardiacevents, and gestational hypertensive disorderhave also been evaluated. These adverse eventswere not significantly increased among Tdap-vaccinated vs. non-vaccinated pregnant womenacross multiple database analyses[42, 43, 47, 48, 50, 53–56] and clinical studies[13, 41, 58], even when consecutive doses ofTdap vaccine were repeated at intervalsof\ 5 years [55]. Although Layton et al. [43]
562 Infect Dis Ther (2019) 8:543–568

found a small increase in postpartum hemor-rhage in Tdap vaccinated compared withunvaccinated pregnant women (RR = 1.23; 95%CI 1.18–1.28) [43], the database analyses ofDonegan et al. [53] and Griffin et al. [48] foundno such increase with vaccination. ‘‘Serious’’adverse pregnancy outcomes occurred at similarrates in Tdap- and Td-vaccinated pregnantwomen in a randomized prospective trial [35],and in Tdap plus influenza sequentially- orconcomitantly-vaccinated pregnant womenidentified in an other database analysis [45].
There was no causal association between theTdap vaccine and adverse outcomes reported inseveral clinical studies [13, 37, 38, 41].
Adverse Birth and Neonatal Outcomes/Complications
Concerns regarding potential adverse birth andneonatal outcomes can influence decisions andrecommendations about Tdap vaccination dur-ing pregnancy. Outcomes assessed includedpreterm birth, stillbirth, development-relatedparameters such as low/very low birth weight orsmall size for gestational age, neonatal death,birth defects (including atrioventricular septaldefect, spina bifida, cleft palate, cleft lip anddiaphragmatic hernia), major malformations,congenital anomalies, neonatal complications,respiratory disorders, APGAR score, and cordblood pH values (Table 1). No significantincrease in any of these outcomes were identi-fied among infants of Tdap-vaccinated com-pared to non-vaccinated pregnant women, orfrom expected norms, regardless of design(database analysis vs. clinical trial), population,or setting [13, 41, 43, 50, 52–56, 58]. In addi-tion, no differences in the rates of seriousadverse outcomes were observed in infants ofTdap- and Td-vaccinated pregnant women, andnone of the serious adverse outcomes reportedwere considered related to vaccination [35].Hoang et al. [36] reported that infants of Tdap-vaccinated women presented common symp-toms of respiratory and gastrointestinal dis-eases, although no events were serious orconsidered related to vaccination. Furthermore,Tdap vaccination during pregnancy does not
appear to be associated with an increase in thediagnosis of autism spectrum disorder [59].
There was no increase in acute adverseevents or adverse birth outcomes in infants ofwomen who received Tdap vaccination duringpregnancy following previous vaccinationwith a tetanus-containing vaccine\ 2 years or2–5 years before compared with those whosemothers had been vaccinated[5 years [45].Nor between infants of women who hadreceived single vs. multiple (\5 years) doses ofTdap [55]. The timing of Tdap relative to influ-enza vaccine in had no influence on the fre-quency of preterm delivery, low birth weightand small for gestational age in infants ofwomen who received sequential or concomi-tant immunization with these vaccines duringpregnancy [46].
Infants of women who received Tdap duringpregnancy did not need more or more intensehealthcare support than those from womenwho did not receive the vaccine, with noincreases recorded in the days of neonatal hos-pitalization or neonatal intensive care unit(NICU) admission [50, 55], or in the number ofhealth encounters with complex chronic con-ditions by age 12 months [56]. In addition,there was no significant association betweeninfant hospitalization or death in the first6 months of life and receipt of maternal Tdap orTdap plus influenza vaccine [60].
DISCUSSION
Concerns about maternal pertussis vaccination,at a time when the mother is cautious abouttheir own health and that of their unborn child,may adversely influence acceptance and uptakeof the vaccine. This review confirms the safetyof maternal pertussis vaccination during preg-nancy, and provides evidence to support deci-sion-making and counseling on thisintervention. Although local and systemicreactions were reported among vaccinatedpregnant women in clinical studies and data-base analyses, these were usually mild and self-limiting and generally well tolerated. Suchreactions were not influenced by repeat expo-sure to Tdap, vaccines containing tetanus
Infect Dis Ther (2019) 8:543–568 563

toxoid or by concomitant vaccination withinfluenza vaccines (Table 1).
This review provides reassurance that vacci-nation against pertussis during pregnancy doesnot adversely affect maternal, fetal or neonatalhealth (Table 1). Although the studies reviewedused different methodologies and reportingmeasures, they were generally in agreement.However, in the future, it may be possible tobetter synthesize the available data if initiatives,such as that of the Global Alignment ofImmunization Safety Assessment in Pregnancy(GAIA) project, coordinated by the BrightonCollaboration Foundation [61], are adopted.The GAIA project was initiated to provideguidance for harmonizing the data collected incase report forms used for safety monitoring,with the aim of improving data collection andunderstanding of vaccine-related outcomes inpregnancy.
The potential impact of Tdap vaccinationduring pregnancy on chorioamnionitis varies,with some studies suggesting an increased rateof the condition [43, 52, 54] and others no suchincrease [48, 50, 55]. Nonetheless, chorioam-nionitis is uncommonly reported (1% of preg-nancy reports to VAERS databases), and usuallyobserved in pregnant women with known riskfactors for the condition [51].
There is currently no definitive reactogenic-ity data by trimester, or on pregnancy, birth andneonatal outcomes. In Ireland, the NationalImmunization Advisory Committee (NIAC)recommended (in 2016) that pregnant womenshould be given the vaccine as early as 16 weeks’gestational [62]. This advice was based on astudy [63] which found that the immuneresponse was robust when the vaccine was givenearly in second trimester. The extended eligi-bility criteria for the vaccine in the UK made thevaccine available to women beginning in thesixteenth week of pregnancy since April 2016(previously available from 28 weeks), and mayhave contributed to the increase in the coverageduring pregnancy [64]. Examination of theimpact of the earlier vaccination during preg-nancy will be informative.
In recent years, many countries includingthe UK, USA, Australia, New Zealand, and sev-eral others in Europe and Latin America have
introduced pertussis vaccination during preg-nancy. Of note, this review included data frommost of these countries and regions. There wereno apparent geographic differences in the safetyprofile of maternal pertussis immunizationduring pregnancy and on infant outcomes.
Our systematic review has a number of lim-itations that need to be considered. Despite arigorous systematic search to identify all avail-able articles published between 1995 and 2018,we cannot exclude the possibility of missingsome studies and nor did we assess publicationbias. Our broad inclusion criteria resulted in adiverse range of included studies which com-plicates the overall interpretation of results asthere was no standardized reporting of adverseevents/complications. In addition, a large pro-portion of the articles reviewed were from theUSA. The strength of our review lies in ourgeneral adherence to established methods forconducting systematic reviews, including anextensive search across multiple databases, anda wide inclusive publication date range.
CONCLUSION
In conclusion, our review consolidates knowl-edge on the safety profile of maternal pertussisimmunization during pregnancy and on theinfant. Maternal immunization does notadversely affect pregnancy, birth or neonataloutcomes. Evidence presented confirms thesafety of maternal pertussis immunization, andsupports recommendations for pertussis vacci-nation during pregnancy.
ACKNOWLEDGEMENTS
Funding. This review and the journal’s rapidservice fee were funded by Sanofi Pasteur,
Medical Writing and Editorial Assis-tance. Editorial assistance with the preparationof the manuscript was provided by CarolineSpencer on behalf of inScience Communica-tions, Springer Healthcare, UK, and was fundedby Sanofi Pasteur. The authors also thank
564 Infect Dis Ther (2019) 8:543–568

Burnedette Rose Hill for editorial assistance andmanuscript coordination on behalf of Sanofi-Pasteur.
Authorship. All named authors meet theInternational Committee of Medical JournalEditors (ICMJE) criteria for authorship for thisarticle, take responsibility for the integrity ofthe work as a whole, and have given theirapproval for this version to be published.
Disclosures. Charlotte Switzer is anemployee of Sanofi Pasteur. Caroline D’Heilly isan employee of Sanofi Pasteur. Denis Macina isan employee of Sanofi Pasteur.
Compliance with Ethics Guidelines. Thisarticle is based on previously conducted studiesand does not contain any studies with humanparticipants or animals performed by any of theauthors.
Open Access. This article is distributedunder the terms of the Creative CommonsAttribution-NonCommercial 4.0 InternationalLicense (http://creativecommons.org/licenses/by-nc/4.0/), which permits any non-commercial use, distribution, and reproductionin any medium, provided you give appropriatecredit to the original author(s) and the source,provide a link to the Creative Commons license,and indicate if changes were made.
REFERENCES
1. Edwards KM, Decker MD. Pertussis vaccines. In:Plotkin SA, Orenstein WA, Offit PA, Edwards KM,editors. Plotkin’s vaccines. 7th ed. Philadelphia:Elsevier; 2018. p. 711–61.
2. Yeung KHT, Duclos P, Nelson EAS, Hutubessy RCW.An update of the global burden of pertussis inchildren younger than 5 years: a modelling study.Lancet Infect Dis. 2017;17(9):974–80.
3. WHO. Pertussis vaccines: WHO position paper—September 2015. Wkly Epidemiol Rec.2015;90(35):433–58.
4. Bento AI, King AA, Rohani P. Maternal pertussisimmunisation: clinical gains and epidemiologicallegacy. Euro Surveill. 2017;22:15.
5. Poolman JT. Shortcomings of pertussis vaccines:why we need a third generation vaccine. Expert RevVaccines. 2014;13(10):1159–62.
6. Skoff TH, Kenyon C, Cocoros N, Liko J, Miller L,Kudish K, et al. Sources of infant pertussis infectionin the United States. Pediatrics.2015;136(4):635–41.
7. Wiley KE, Zuo Y, Macartney KK, McIntyre PB.Sources of pertussis infection in young infants: areview of key evidence informing targeting of thecocoon strategy. Vaccine. 2013;31(4):618–25.
8. Masseria C, Martin CK, Krishnarajah G, Becker LK,Buikema A, Tan TQ. Incidence and burden of per-tussis among infants less than 1 year of age. PediatrInfect Dis J. 2017;36(3):e54–61.
9. Romanin V, Agustinho V, Califano G, Sagradini S,Aquino A, Juarez Mdel V, et al. Epidemiologicalsituation of pertussis and strategies to control it:Argentina, 2002–2011. Arch Argent Pediatr.2014;112(5):413–20.
10. Torres RS, Santos TZ, Torres RA, Pereira VV, FaveroLA, Otavio Filho RM, et al. Resurgence of pertussisat the age of vaccination: clinical, epidemiological,and molecular aspects. J Pediatr (Rio J).2015;91(4):333–8.
11. van Hoek AJ, Campbell H, Amirthalingam G,Andrews N, Miller E. The number of deaths amonginfants under one year of age in England with per-tussis: results of a capture/recapture analysis for theperiod 2001 to 2011. Euro Surveill. 2013;18:9.
12. Esposito S, Principi N. Immunization against per-tussis in adolescents and adults. Clin MicrobiolInfect. 2016;22(Suppl 5):S89–95.
13. Munoz FM, Bond NH, Maccato M, Pinell P, Ham-mill HA, Swamy GK, et al. Safety and immuno-genicity of tetanus diphtheria and acellularpertussis (Tdap) immunization during pregnancy inmothers and infants: a randomized clinical trial.JAMA. 2014;311(17):1760–9.
14. Amirthalingam G, Andrews N, Campbell H, RibeiroS, Kara E, Donegan K, et al. Effectiveness of mater-nal pertussis vaccination in England: an observa-tional study. Lancet. 2014;384(9953):1521–8.
15. Amirthalingam G, Campbell H, Ribeiro S, Fry NK,Ramsay M, Miller E, et al. sustained effectiveness ofthe maternal pertussis immunization program inEngland 3 years following introduction. Clin InfectDis. 2016;63(suppl 4):S236–43.
16. Baxter R, Bartlett J, Fireman B, Lewis E, Klein NP.Effectiveness of vaccination during pregnancy toprevent infant pertussis. Pediatrics. 2017;139:5.
Infect Dis Ther (2019) 8:543–568 565

17. Dabrera G, Amirthalingam G, Andrews N, Camp-bell H, Ribeiro S, Kara E, et al. A case–control studyto estimate the effectiveness of maternal pertussisvaccination in protecting newborn infants in Eng-land and Wales, 2012–2013. Clin Infect Dis.2015;60(3):333–7.
18. Romanin V, Acosta AM, Sagradini S, Briere E, San-chez SM, Sevilla ME, et al. Effectiveness of Tdapvaccination during pregnancy in preventing infantpertussis in a country with whole-cell pertussisvaccines during childhood: preliminary results of acase–control study in Argentina. Open ForumInfect Dis. 2015;2(Suppl 1):S447.
19. Saul N, Wang K, Bag S, Baldwin H, Alexander K,Chandra M, et al. Effectiveness of maternal pertus-sis vaccination in preventing infection and diseasein infants: the NSW Public Health Networkcase–control study. Vaccine. 2018;36(14):1887–92.
20. Skoff TH, Blain AE, Watt J, Scherzinger K, McMa-hon M, Zansky SM, et al. Impact of the US maternaltetanus, diphtheria, and acellular pertussis vacci-nation program on preventing pertussis inInfants\2 months of age: a case–control evalua-tion. Clin Infect Dis. 2017;65(12):1977–83.
21. Winter K, Nickell S, Powell M, Harriman K. Effec-tiveness of prenatal versus postpartum tetanus,diphtheria, and acellular pertussis vaccination inpreventing infant pertussis. Clin Infect Dis.2017;64(1):3–8.
22. Winter K, Cherry JD, Harriman K. Effectiveness ofprenatal tetanus, diphtheria, and acellular pertussisvaccination on pertussis severity in infants. ClinInfect Dis. 2017;64(1):9–14.
23. Bonville CA, Cibula DA, Domachowske JB,Suryadevara M. Vaccine attitudes and practicesamong obstetric providers in New York State fol-lowing the recommendation for pertussis vaccina-tion during pregnancy. Hum Vaccin Immunother.2015;11(3):713–8.
24. Chamberlain AT, Seib K, Ault KA, Orenstein WA,Frew PM, Malik F, et al. Factors associated withintention to receive influenza and tetanus, diph-theria, and acellular pertussis (Tdap) vaccines dur-ing pregnancy: a focus on vaccine hesitancy andperceptions of disease severity and vaccine safety.PLoS Curr. 2015;2015:7.
25. Wilson RJ, Paterson P, Jarrett C, Larson HJ. Under-standing factors influencing vaccination accep-tance during pregnancy globally: a literaturereview. Vaccine. 2015;33(47):6420–9.
26. Jones KM, Carroll S, Hawks D, McElwain CA,Schulkin J. Efforts to improve immunization
coverage during pregnancy among Ob-Gyns. InfectDis Obstet Gynecol. 2016;2016:6120701.
27. Vishram B, Letley L, Jan Van Hoek A, Silverton L,Donovan H, Adams C, et al. Vaccination in preg-nancy: attitudes of nurses, midwives and healthvisitors in England. Hum Vaccin Immunother.2018;14(1):179–88.
28. Wilcox CR, Bottrell K, Paterson P, Schulz WS,Vandrevala T, Larson HJ, et al. Influenza and per-tussis vaccination in pregnancy: portrayal in onlinemedia articles and perceptions of pregnant womenand healthcare professionals. Vaccine.2018;36(50):7625–31.
29. Maisa A, Milligan S, Quinn A, Boulter D, Johnston J,Treanor C, et al. Vaccination against pertussis andinfluenza in pregnancy: a qualitative study of bar-riers and facilitators. Public Health.2018;162:111–7.
30. Collins J, Alona I, Tooher R, Marshall H. Increasedawareness and health care provider endorsement isrequired to encourage pregnant women to be vac-cinated. Hum Vaccin Immunother.2014;10(10):2922–9.
31. Mehrotra A, Fisher AK, Mullen J, Rodriguez L, JilesAJ, Albert AP, et al. Provider insight on surmount-ing specialty practice challenges to improve Tdapimmunization rates among pregnant women.Heliyon. 2018;4(5):e00636.
32. Switzer C, Macina D. Safety and effectiveness ofpertussis immunization during pregnancy 2016Contract No: CRD42016038317.
33. O’Connor D, Green S, Higgins JPT. Chapter 5:Defining the review question and developing cri-teria for including studies. Cochrane Handbook forSystematic Reviews of Interventions. Version 5.0.0ed2008 ed2008.
34. Fortner KB, Swamy GK, Broder KR, Jimenez-TruqueN, Zhu Y, Moro PL, et al. Reactogenicity andimmunogenicity of tetanus toxoid, reduced diph-theria toxoid, and acellular pertussis vaccine (Tdap)in pregnant and nonpregnant women. Vaccine.2018;36(42):6354–60.
35. Halperin SA, Langley JM, Ye L, Mackinnon-Cameron D, Elsherif M, Allen VM, et al. A ran-domized controlled trial of the safety andimmunogenicity of tetanus, diphtheria, and acel-lular pertussis vaccine immunization during preg-nancy and subsequent infant immune response.Clin Infect Dis. 2018;67(7):1063–71.
36. Hoang HT, Leuridan E, Maertens K, Nguyen TD,Hens N, Vu NH, et al. Pertussis vaccination duringpregnancy in Vietnam: results of a randomized
566 Infect Dis Ther (2019) 8:543–568

controlled trial Pertussis vaccination during preg-nancy. Vaccine. 2016;34(1):151–9.
37. Maertens K, Cabore RN, Huygen K, Hens N, VanDamme P, Leuridan E. Pertussis vaccination duringpregnancy in Belgium: results of a prospectivecontrolled cohort study. Vaccine.2016;34(1):142–50.
38. Petousis-Harris H, Walls T, Watson D, Paynter J,Graham P, Turner N. Safety of Tdap vaccine inpregnant women: an observational study. BMJOpen. 2016;6(4):e010911.
39. Regan AK, Tracey LE, Blyth CC, Richmond PC,Effler PV. A prospective cohort study assessing thereactogenicity of pertussis and influenza vaccinesadministered during pregnancy. Vaccine.2016;34(20):2299–304.
40. Villarreal Perez JZ, Ramirez Aranda JM, de la ManuelOC, Zamudio Osuna MJ, Perales Davila J, BallesterosElizondo MR, et al. Randomized clinical trial of thesafety and immunogenicity of the Tdap vaccine inpregnant Mexican women. Hum Vaccin Immun-other. 2017;13(1):128–35.
41. Wanlapakorn N, Maertens K, Chaithongwong-watthana S, Srimuan D, Suratannon N, Vongpun-sawad S, et al. Assessing the reactogenicity of Tdapvaccine administered during pregnancy and anti-bodies to Bordetella pertussis antigens in maternaland cord sera of Thai women. Vaccine.2018;36(11):1453–9.
42. Kharbanda EO, Vazquez-Benitez G, Lipkind HS,Klein NP, Cheetham TC, Naleway AL, et al. Mater-nal Tdap vaccination: coverage and acute safetyoutcomes in the vaccine safety datalink,2007–2013. Vaccine. 2016;34(7):968–73.
43. Layton JB, Butler AM, Li D, Boggess KA, Weber DJ,McGrath LJ, et al. Prenatal Tdap immunization andrisk of maternal and newborn adverse events. Vac-cine. 2017;35(33):4072–8.
44. Moro PL, Cragan J, Tepper N, Zheteyeva Y, MuseruO, Lewis P, et al. Enhanced surveillance of tetanustoxoid, reduced diphtheria toxoid, and acellularpertussis (Tdap) vaccines in pregnancy in the Vac-cine Adverse Event Reporting System (VAERS),2011–2015. Vaccine. 2016;34(20):2349–53.
45. Sukumaran L, McCarthy NL, Kharbanda EO,McNeil MM, Naleway AL, Klein NP, et al. Associa-tion of Tdap vaccination with acute events andadverse birth outcomes among pregnant womenwith prior tetanus-containing immunizations.JAMA. 2015;314(15):1581–7.
46. Sukumaran L, McCarthy NL, Kharbanda EO,Weintraub ES, Vazquez-Benitez G, McNeil MM,
et al. Safety of tetanus toxoid, reduced diphtheriatoxoid, and acellular pertussis and influenza vacci-nations in pregnancy. Obstet Gynecol.2015;126(5):1069–74.
47. Zheteyeva YA, Moro PL, Tepper NK, Rasmussen SA,Barash FE, Revzina NV, et al. Adverse event reportsafter tetanus toxoid, reduced diphtheria toxoid,and acellular pertussis vaccines in pregnantwomen. Am J Obstet Gynecol. 2012;207(1):59 e1–7.
48. Griffin JB, Yu L, Watson D, Turner N, Walls T, HoweAS, et al. Pertussis Immunisation in PregnancySafety (PIPS) Study: a retrospective cohort study ofsafety outcomes in pregnant women vaccinatedwith Tdap vaccine. Vaccine. 2018;36(34):5173–9.
49. Advisory Committee on Immunization Practices(ACIP), Updated recommendations for use of teta-nus toxoid, reduced diphtheria toxoid, and acellu-lar pertussis vaccine (Tdap) in pregnantwomen–Advisory Committee on ImmunizationPractices (ACIP). MMWR Morb Mortal Wkly Rep.2013;62(7):131–5.
50. Berenson AB, Hirth JM, Rahman M, Laz TH, RuppRE, Sarpong KO. Maternal and infant outcomesamong women vaccinated against pertussis duringpregnancy. Hum Vaccin Immunother.2016;12(8):1965–71.
51. Datwani H, Moro PL, Harrington T, Broder KR.Chorioamnionitis following vaccination in thevaccine adverse event reporting system. Vaccine.2015;33(27):3110–3.
52. DeSilva M, Vazquez-Benitez G, Nordin JD, LipkindHS, Klein NP, Cheetham TC, et al. Maternal Tdapvaccination and risk of infant morbidity. Vaccine.2017;35(29):3655–60.
53. Donegan K, King B, Bryan P. Safety of pertussisvaccination in pregnant women in UK: observa-tional study. BMJ. 2014;349:g4219.
54. Kharbanda EO, Vazquez-Benitez G, Lipkind HS,Klein NP, Cheetham TC, Naleway A, et al. Evalua-tion of the association of maternal pertussis vacci-nation with obstetric events and birth outcomes.JAMA. 2014;312(18):1897–904.
55. Morgan JL, Baggari SR, McIntire DD, Sheffield JS.Pregnancy outcomes after antepartum tetanus,diphtheria, and acellular pertussis vaccination.Obstet Gynecol. 2015;125(6):1433–8.
56. Shakib JH, Korgenski K, Sheng X, Varner MW, PaviaAT, Byington CL. Tetanus, diphtheria, acellularpertussis vaccine during pregnancy: pregnancy andinfant health outcomes. J Pediatr.2013;163(5):1422–1426 e1–4.
Infect Dis Ther (2019) 8:543–568 567

57. Wang M, Khromava A, Mahmood A, Dickson N.Pregnant women receiving tetanus-diphtheria-acellular pertussis (Tdap) vaccine: 6 years of Adacelvaccine pregnancy registry data. Pharmacoepi-demiol Drug Saf. 2011;20:S60.
58. Walls T, Graham P, Petousis-Harris H, Hill L, AustinN. Infant outcomes after exposure to Tdap vaccinein pregnancy: an observational study. BMJ Open.2016;6(1):e009536.
59. Becerra-Culqui TA, Getahun D, Chiu V, Sy LS,Tseng HF. Prenatal tetanus, diphtheria, acellularpertussis vaccination and autism spectrum disorder.Pediatrics. 2018;142:3.
60. Sukumaran L, McCarthy NL, Kharbanda EO, Vaz-quez-Benitez G, Lipkind HS, Jackson L, et al. Infanthospitalizations and mortality after maternal vac-cination. Pediatrics. 2018;141:3.
61. Jones CE, Munoz FM, Kochhar S, Vergnano S,Cutland CL, Steinhoff M, et al. Guidance for thecollection of case report form variables to assesssafety in clinical trials of vaccines in pregnancy.Vaccine. 2016;34(49):6007–14.
62. National Immunisation Office. Whooping cough(Pertussis). Dublin: HSE National ImmunisationOffice; 2017.
63. Eberhardt CS, Blanchard-Rohner G, Lemaitre B,Boukrid M, Combescure C, Othenin-Girard V, et al.Maternal immunization earlier in pregnancy max-imizes antibody transfer and expected infantseropositivity against pertussis. Clin Infect Dis.2016;62(7):829–36.
64. Public Health England. Pertussis vaccination pro-gramme for pregnant women update: vaccine cov-erage in England, October to December 20162017.
568 Infect Dis Ther (2019) 8:543–568