
SAFE - AAGBI. 2013.5 - O...Background Page 5 Course Venue Page 6 The May 2013 SAFE Obstetric...
20
SAFE Safer Anaesthesia From Education Obstetric Anaesthesia Course Parbatipur, Banglaesh May 20 th - 22 nd 2013 Association of Anaesthetists of Great Britain and Ireland World Federation of Societies of Anaesthesiologists
Transcript of SAFE - AAGBI. 2013.5 - O...Background Page 5 Course Venue Page 6 The May 2013 SAFE Obstetric...

SAFE
Safer Anaesthesia From Education
Obstetric Anaesthesia Course
Parbatipur, Banglaesh
May 20th
- 22nd
2013
Association of Anaesthetists of Great Britain and Ireland
World Federation of Societies of Anaesthesiologists

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 2
Table of Contents Executive Summary Page 3 Acknowledgements Page 4 Background Page 5 Course Venue Page 6 The May 2013 SAFE Obstetric Anaesthesia Course Page 8 Monitoring & Evaluation and Results Page 10 Participants’feedback Pre and Post Course Knowledge Assessment Pre and Post Course Skills Assessment
Post Intervention Activity Page 14 Summary Page 15 Appendices Pages 16-17 Course Photographs Pages 18-20

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 3
Executive Summary • This was the first SAFE (Safer Anaesthesia From Education) Obstetric anaesthesia course to ever run in Bangladesh or Asia. It has now proven itself to be suitable for and successful in this context. • It was attended by 31 delegates from across all medical disciplines involved in the hospital care of obstetric patients and their babies: 14 anaesthesiologists 9 anaesthetic nurses/anaesthetic officers 8 physicians from other specialties • Delegates attending this course were from all over Bangladesh but predominantly Dhaka (the capital city), Rangpur and Parbatipur (located in the North West of the country close to the course venue). • The course was directed by Dr Kate Grady. • The teaching Faculty consisted of 4 senior anaesthesiologists who volunteered on the behalf of the Bangladesh Society of Anaesthesiologists (BSA) in addition to 6 travelling Faculty. • This was only the second time the revised course has been run, incorporating maternal trauma and communication skills sessions which were both very favourably received. • Each delegate was assigned an individual mentor to whom they had access throughout the course. • Knowledge and clinical skills were formally assessed before and after the course. Knowledge scores were high from the outset but improved nonetheless. Skills scores showed statistically significant improvements overall. • Feedback from delegates and their appraisal of the course was excellent. • An ex-demo, model intubating head from AMBU® and autoclavable laryngoscopes from Timesco® were both purchased at discounted prices for use on the course and subsequently donated for use at LAMB hospital where the course was held. • Monitoring and evaluation will be undertaken in the following months. Follow up of all delegates who attended this course will take place using cell phone and email communication. • It is proposed that the course will be run again in partnership with the Bangladesh
Society of Anaesthesiologists in 2014.

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 4
Acknowledgements We are indebted to the Bangladesh Society of Anaesthesiologists who contributed bilingual teaching Faculty and helped considerably in the recruitment of delegates for this course. We thank LAMB hospital and their medical director Dr Nelson Mondol for fully supporting and hosting the course. They provided excellent food and accommodation and contributed many enthusiastic course delegates from amongst their own clinical staff. We thank the LAMB hospital Training Centre who provided excellent educational facilities and air conditioned classrooms. We are grateful to the World Federation of Societies of Anaesthesiologists (WFSA) for their financial support and especially thankful to their immediate past President Dr Angela Enright We are grateful to the Association Anaesthetists of Great Britain and Ireland (AAGBI) for their support. A particular thank you goes to Dr William Harrop-Griffiths, President of the AAGBI for his support for the project. The Faculty worked incredibly hard and performed well as a team. We are especially grateful to Dr Rebecca Jones who performed so much preparation of course materials from within the country. We thank Daniel Hruschka, Assistant Professor of Anthropology at Arizona State University who helped us to perform the statistical analysis for this report. Lastly we would like to thank all our course delegates, many of whom travelled for many hours to attend the course and were a joy to teach.

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 5
Background
The lifetime risk of maternal death is the largest discrepancy of all public health statistics. Despite the Millennium Development Goals and significant efforts to attain them, the WHO estimates that 358,000 women die each year from complications of pregnancy and childbirth. The overall maternal mortality ratio (MMR) in Bangladesh is recently estimated at 200 per 100,000 live births. However, it is likely that the MMR is much higher in certain parts of the country where access to acute obstetric services is difficult, especially for the poorest members of society. Small district hospitals frequently run with staffing shortages. The availability of emergency obstetric care encompassing the provision of urgent caesarean section facilities and other life saving obstetric interventions is rarely guaranteed 24 hours per day seven days per week. Consequently patients may have to travel long distances to receive the urgent obstetric care they need. Mothers will often present at hospital late when they are in a critical condition having received little or no antenatal or intrapartum care. The reasons for this include an overall lack of resources, in particular, adequately trained and specialist staff. Experienced obstetricians, anaesthesiologists and other senior staff are enticed away from rural hospitals to work nearer to the big cities. To fill this rural service void non government organisation (NGO) hospitals have had to be resourceful in order to meet their patients’ needs. Non specialist staff may cross cover and fulfil more than one service role, for example, anaesthesiologists providing neonatal resuscitation or anaesthetic nurses providing anaesthesia under the supervision of obstetricians. In order to provide safe obstetric anaesthesia under these circumstances good multidisciplinary teamwork is of paramount importance. This is reflected by the delegates attending this SAFE Obstetric anaesthesia course from specialities other than anaesthesia who are currently working in rural parts of Bangladesh. They are now better equipped to deal with obstetric emergencies and deliver safer obstetric anaesthesia.
Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 6
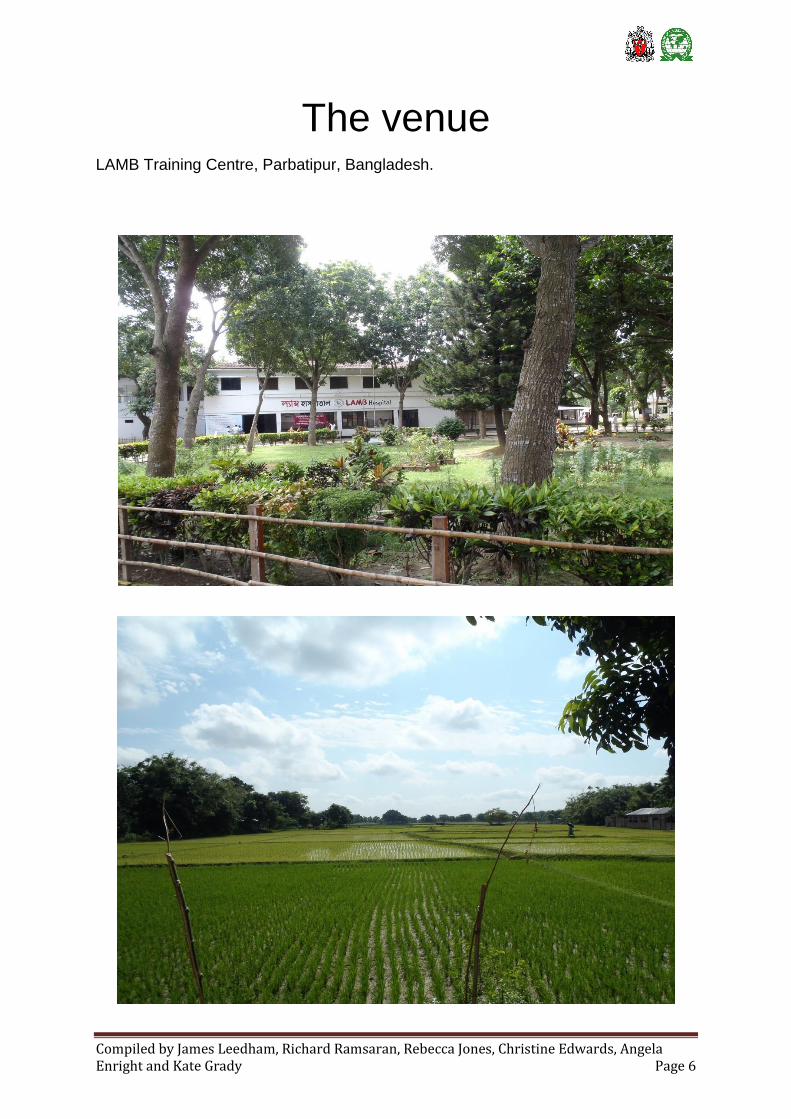
The venue
LAMB Training Centre, Parbatipur, Bangladesh.

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 7
LAMB Hospital Training Centre under construction during November 2012.

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 8
The May 2013 Course The goal of the project is to deliver the SAFE Obstetric Anaesthesia course to all obstetric anaesthetic providers in Bangladesh by 2025. Communication and language barriers make recruiting delegates from the rural hospitals difficult. Travel can be time consuming and unreliable in Bangladesh, especially so with a forthcoming general election and frequent transportation strikes. If the course is too far away the cost of travel and the time away from service provision becomes problematic. If the course is held in one of the big cities anaesthetic providers from rural areas who also need this training might be excluded. For these reasons the course was organised at LAMB hospital, near the town of Parbatipur, close to both Saidpur airport and Parbatipur train station in the rural north west of Bangladesh. Delegates attending this course came from all over Bangladesh but were predominantly from Dhaka (the capital city), Rangpur and Parbatipur (located in the North West of the country closer to where the course was held). Others travelled from Dinajpur, Rajshahi, Bogra, Kishoreganj, Kulaura, Dumki, and Cox’s Bazar. The initial prediction of delegate numbers for this course was 36. However, confirmation of exact numbers was impossible because of transportation strikes and delegates’ clinical commitments. The number of delegates who attended the course was 31. The teaching Faculty comprised of a further 10 individuals which took the total number attending the course to 41. Delegates were divided into groups of 5-9 for breakout and skills stations which proved to be a good number.
The Training of the Trainers Course
The Training of Trainers (TOT) day was not run on this course. A similar course had recently been undertaken at LAMB hospital staff by visiting UK paediatricians. This SAFE course was used to introduce BSA members to its format, specific clinical teaching techniques and styles. Delegates who displayed qualities desirable in an instructor were noted as potential Faculty for future courses. It would be appropriate to run a TOT day in association with the next SAFE course in Bangaldesh.
Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 9
The SAFE Obstetric Anaesthesia Course
The SAFE Obstetric Anaesthesia Course commenced on Monday 20th May. The course was directed by Dr Kate Grady. The teaching faculty consisted of 6 travelling Faculty: Dr Kate Grady Consultant Anaesthetist, University Hospital South Manchester, UK Dr Angela Enright Consultant Anaesthetist, Royal Jubilee Hospital, Victoria, Canada Dr Christine Edwards Specialty doctor in Obstetrics and Gynaecology, Gloucestershire Royal Hospital, Gloucester UK Dr Rebecca Jones Consultant Anaesthetist, Lamb Hospital, Parbatipur, Bangladesh Dr James Leedham Specialist trainee Anaesthetics, North West Deanery, UK Dr Richard Ramsaran Specialist trainee Anaesthetics, North West Deanery, UK
Four senior anaesthesiologists volunteered on the behalf of the BSA to join the Faculty team taking its total number to 10. All were provided with electronic and paper versions of the course manual. BSA Faculty initially observed and supported the visiting Faculty during sessions but these roles were often reversed as their confidence and familiarity grew. A session was given for cardiac disease in pregnancy in place of HIV and malaria. This was deemed to be of greater importance and relevance in Bangladesh. A WHO surgical safety checklist role play was performed by the travelling Faculty. Course Timetable 2013
Sat 18th May
Sun 19th May Mon 20th May
Tues 21st May
Wed 22nd May
Thurs 23rd May
Flights from UK to
Saidpur via Dhaka
Faculty meeting
& preparation of
venue/classrooms
SAFE course day 1
SAFE course day 2
SAFE course day 3
Return flights from Saidpur via Dhaka to
UK

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 10
Monitoring, Evaluation and Results
The course evaluation involves the following 5 steps:
‣ Delegatesʼ feedback (about the course overall and individual sessions)
‣ Pre and post course knowledge (MCQ) assessment
‣ Pre and post course skills assessment
‣ Logbooks (reviews to occur in the months following the course)
‣ Field work to include cell phone and email interviews
Delegatesʼ feedback
All delegates were pleased to receive their copy of the e-SAFE DVD, a book ʻObstetric Anaesthesia in Developing Countriesʼ and their logbook to complement content that is taught on the course. Instructions and reminders to complete feedback forms after each session were given and repeated throughout the course. The scores are very impressive. The chart below displays specific feedback from sessions. It was on a scale of 1-10 (very poor – excellent). The range and the median scores are illustrated by red bars and green diamonds respectively.
0
2
4
6
8
10
Lectures Breakout sessions
Median

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 11
This second chart illustrates overall course feedback again using a scale of 1-10 (very poor – excellent).
Overall the course feedback was extremely positive and encouraging. Some of the positive comments from delegates are listed below: ‘It is an effective training for every anaesthetist so if all anaesthetists receive this training then it is beneficial for the provision of safe obstetric anaesthesia’ ‘Material excellent’ ‘SAFE course has helped me to enrich my knowledge, I would like to attend this type of course again in the future’ ‘I am very satisfied to get this training’ ‘good system using breakout sessions’ ‘overall a great job! thankyou!’ ‘it is a good, useful and invaluable course’
‘very good to have anaesthetist and obstetricians together in group’ ‘coped well with diverse group from different settings’
Enjoyable Knowledge Improved
Clinical ability
Improved
Relevant Improve patient care
Useful course for
your hospital
0
2
4
6
8
10
General Feedback
Median

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 12
Five delegates made constructive suggestions: One would have appreciated lecture handout sheets. Another thought that the breakout sessions were too short for all that needed to be discussed. Other comments centred around the fact that air conditioning was not available in all of the classrooms and one individual felt that a PA system might have been helpful for the lectures. There is a lot of ground to cover in only three days but all the topics have been judged necessary.
Pre and Post Course Skills Assessment
26 candidates underwent a skills test before and after the course. The four skills
tested were:
1. Maternal cardiac arrest
2. Management of eclamptic seizure
3. Rapid sequence induction
4. Neonatal life support
Each candidate repeated the same pre and post course skills test and was assessed by the same person. Results are displayed in the table below:
Mean
Pre Skills Test Score 6
Post Skills Test Score 8
Paired student’s T test p Value <0.001
The improvement in candidates skills test scores were <0.05 and therefore
statistically significant.

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 13
Pre and Post Course Knowledge Assessment
Candidates were given a multiple choice question (MCQ) paper containing 50
questions to test their knowledge before and after the course. This was conducted
under examination conditions and adequate time was allowed for completion. After
registration on the first day the pre course skills test was immediately followed by the
pre course MCQ paper. On the last day of the post course the MCQ paper was
taken before the post course skills test.
26 of the 31 delegates who attended the course completed both pre and post
knowledge tests. Data was again analysed using a paired student’s T test.
Mean (%)
Pre Knowledge Test Score 37 (75)
Post Knowledge Test Score 39 (78)
Paired student’s T test p Value 0.11
Knowledge scores were high from the outset but showed an improvement between
pre and post course MCQ tests.
Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 14
Post Intervention Activity
The Monitoring and Evaluation applied to the SAFE course is as follows:
‣ Level 1: Reaction and enjoyment – measured by numerical analogue scores
‣ Level 2: Change in knowledge – assessed by pre and post course MCQ tests
‣ Level 3: Change in skill ability –assessed by before and after course skills tests
‣ Level 4: Change in behaviour and ability in the workplace – recorded in logbook
and elicited via email communication
‣ Level 5: Institutional (and ultimately widespread) change – assessed by analysis of
institutional and national data where possible Levels 1 - 3 were assessed during the course and the results are published in this document in the monitoring and evaluation section. . Level 4 and 5 Change in behaviour and in the workplace will be measured by the keeping of logbooks. The logbook contains brief introductory information and spaces for 30 examples of care that was improved having attended the SAFE Obstetric Anaesthesia course. Logbooks were presented to 28 delegates at the end of the course. 3 delegates unexpectedly had to depart early so did not receive their paper logbooks but instead electronic versions via email. We will ask for logbook extracts to be fed back, cases of high educational value will then be disseminated via email to all course delegates with relevant continuing medical educational material attached.

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 15
Summary
Thirty one delegates were trained, they were from both physician and non physician backgrounds. For the first time in the course’s history a good number of in house obstetric and paediatric physicians also attended. Skills in four key areas of anaesthetic practice were assessed and shown to have improved by a statistically significant amount as a result of this course. These skills along with the many others acquired during the course will help to reduce maternal and infant mortality and morbidity in Bangladesh. This first Bangladesh SAFE Obstetric Anaesthesia course was extremely well received by both local Faculty and delegates. It represents a very exciting step towards disseminating this course throughout the country and to other parts of Asia. However, much hard work remains to be done to achieve this goal.

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 16
Appendix 1 - Faculty List
Dr Kate Grady Consultant Anaesthetist, University Hospital South Manchester, UK Dr Angela Enright Consultant Anaesthetist, Royal Jubilee Hospital Victoria, Canada Dr Christine Edwards Specialty doctor in Obstetrics and Gynaecology, Gloucestershire Royal Hospital, Gloucester UK Dr Rebecca Jones Consultant Anaesthetist, Lamb Hospital, Parbatipur, Bangladesh Dr James Leedham Specialist trainee Anaesthetics, North West Deanery, UK Dr Richard Ramsaran Specialist trainee Anaesthetics, North West Deanery, UK
Prof.Dr.M.Khalilur Rahman (Consultant Anaesthetist, Birdem Hospital, Shahbagh, Dhaka) Prof.Dr.Paresh Chandra Sarker (Consultant, Sir Sholimullah Medical College and Mitford Hospital, Dhaka) Prof.Dr.Debabrata Banik, (Consultant Anesthesia, Analgesia and Intensive care Medicine, Bangabandhu Sheikh Mujib Medical University, Shahbagh, Dhaka) Prof.Dr.M.Abdur Rahman, (Professor and Head, Department of Anaesthesiology and Intensive Care, Dhaka Medical College and Hospital)

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 17
Appendix 2 – Delegate List
NAME HOSPITAL
Anaesthesiologists
Kamrul Ahsan Birdem Hospital
Debi Halder Uttara Adhunik Medical College Hospital
Ruma Rumshum Mrong Square Hospital Ltd.
AKM Faizul Hoque Bangabandhu Shukh Muyil medical university (BSMMU)
Kazi Nur Asfia BSMMU
Manash Kumar Basu National Institute of Cancer Research Hospital
MD.Sadrul Islam Talukder Rangpur Medical College
M.Ataur Rahman Rangpur Medical College
Khandker Al-Helal Didarul Alam Rangpur Medical College
MD.Sayedur Rahman Rangpur Medical College
MD.Abdullah-hel-Baki (Salim) Dinajpur Medical College
Sabia Siddika MAG Osmani
M.Mahmud Ali SZMCH (Shaheed Ziaur Rahman Medical college)
ANM Nanshad Khan Shahid Syed Nazrul Islam medical college
Physicians from other Specialities
Sufia Khatun Shahid Syed Nazrul Islam medical college
Sayeba Akhter BSMMU
Musarrat Sultana Dhaka Medical College
James Eaton BCHP (Brahmonbazar Christian Health Project)
Suvas Chandra Sarker LAMB Hospital
Beatrice Ambauen LAMB Hospital
Keya Famida Yasmin LAMB Hospital
Louise Tina Day LAMB Hospital
Non-physician Anaesthetists
Beauty Ara LAMB Hospital
Hanna Kisku LAMB Hospital
Alfred Dhali LAMB Hospital
Shilpi Roy LAMB Hospital
Debashis Biswas LAMB Hospital
Biliom Mondol LAMB Hospital
Prince Roy Christian Mission hospital nursing institute
Sungsook Kim Memorial christian hospital, Malumghat
Pakhi Karmaker LHCiB

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 18
Appendix 3 – Course Photographs

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 19

Compiled by James Leedham, Richard Ramsaran, Rebecca Jones, Christine Edwards, Angela Enright and Kate Grady Page 20






![[NOT PROTECTIVELY MARKED] Vibrant, Safe and Sustainable … Safe... · 2014. 4. 10. · Page 1 of 33 [NOT PROTECTIVELY MARKED] Agenda Pages Page 1 of 2 Vibrant, Safe and Sustainable](https://static.fdocuments.us/doc/165x107/5fed2f160ef9525bbb055270/not-protectively-marked-vibrant-safe-and-sustainable-safe-2014-4-10.jpg)











