
Rituximab: Anti-CD20 Monoclonal Antibody - American ... · The New Data on the Role Of Rituximab in...
23
The New Data on the The New Data on the Role Of Rituximab in SLE Role Of Rituximab in SLE and Lupus Nephritis and Lupus Nephritis Gerald B.Appel, M.D. Gerald B.Appel, M.D. Professor of Clinical Medicine Professor of Clinical Medicine Columbia University Columbia University – College of Physicians and Surgeons College of Physicians and Surgeons NY NY-Presbyterian Hospital Presbyterian Hospital New York, New York New York, New York Rituximab: Anti-CD20 Monoclonal Antibody Rituximab - FDA approved for the treatment of relapsed or the treatment of relapsed or refractory, CD20-positive B- cell NH Lymphomas and Rheumatoid Arthritis • Chimeric murine/human monoclonal antibody • Used in many glomerular diseases in uncontrolled trials • In SLE and LN studied in both uncontrolled and controlled randomized trials
-
Upload
truongquynh -
Category
Documents
-
view
215 -
download
0
Transcript of Rituximab: Anti-CD20 Monoclonal Antibody - American ... · The New Data on the Role Of Rituximab in...

The New Data on the The New Data on the Role Of Rituximab in SLE Role Of Rituximab in SLE
and Lupus Nephritisand Lupus Nephritis
Gerald B.Appel, M.D.Gerald B.Appel, M.D.Professor of Clinical MedicineProfessor of Clinical Medicine
Columbia University Columbia University ––College of Physicians and SurgeonsCollege of Physicians and Surgeonsg y gg y gNYNY--Presbyterian HospitalPresbyterian Hospital
New York, New YorkNew York, New York
Rituximab:Anti-CD20 Monoclonal Antibody
Rituximab - FDA approved for the treatment of relapsed orthe treatment of relapsed or refractory, CD20-positive B-cell NH Lymphomas and Rheumatoid Arthritis
• Chimeric murine/human monoclonal antibody
• Used in many glomerular diseases in uncontrolled trials
• In SLE and LN studied in both uncontrolled and controlled randomized trials
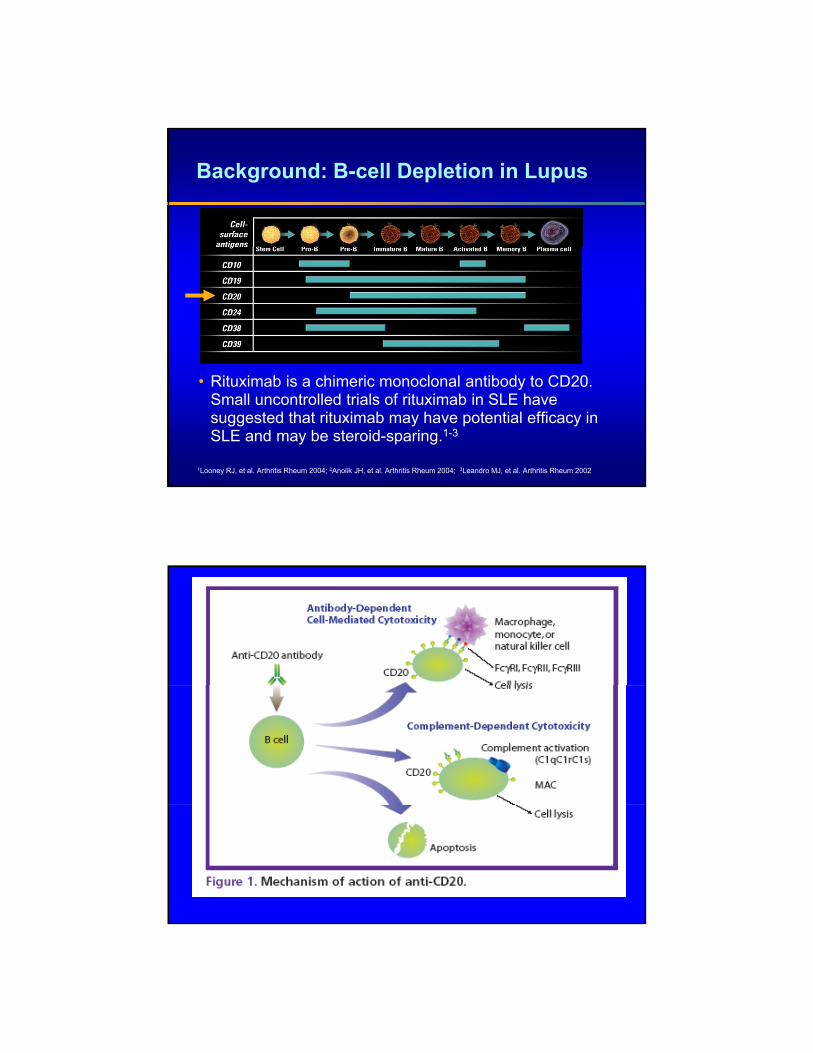
Background: B-cell Depletion in Lupus
1Looney RJ, et al. Arthritis Rheum 2004; 2Anolik JH, et al. Arthritis Rheum 2004; 3Leandro MJ, et al. Arthritis Rheum 2002
• Rituximab is a chimeric monoclonal antibody to CD20. Small uncontrolled trials of rituximab in SLE have suggested that rituximab may have potential efficacy in SLE and may be steroid-sparing.1-3

Questions about Rituximab Therapy in SLE and LN
• What is the drug’s role in treating SLE without severe LN?without severe LN?
• What is the drug’s role in induction therapy for severe LN?
• What is the drug’s role in refractory disease and relapsing disease?
• Is there data from controlled randomized blinded trials to support its use?
Rituximab in Severe LN: Early B Cell Depletion Affects Long-Term Renal
Outcome
20 Pt t t d ith RTX f LN d f ll d• 20 Pts treated with RTX for LN and followed at lest 12 months.
• 19F/1M Active IV ( 15 pts ) or V ( 5 pts)• 12 Pts refractory to standard Rx , 6 cases
relapsing disease, 2 pts first line therapy• 3 concurrent cyclophosphamide, 10
continued RTX as maintenance,
Melander et al CJASN 4: 579-587, 2009

Rituximab in Severe LN: Early B Cell Depletion Affects Long-Term Renal Outcome
• At 22 months complete or partial renal remission in 12/20 ( 60%) .( )
• LN relapsed in 1 pt who responded to another RTX course
• Side effects: 5 infections and 4 moderate neutropenias
• Association of B cell depletion 1 month post rituximab was strongly associated with renal g yresponse ( negatively associated with Black race and hypoalbuminemia)
• RPGN did not respond.
Melander et al CJASN 4: 579-587, 2009
Rituximab in Severe LN: Early B Cell Depletion Affects Long-Term Renal
Outcome
Conclusion :Rituximab is an interesting therapeutic
option in relapsing or refractory lupus nephritis when early B cell depletion is obtainedobtained.
Melander et al CJASN 4: 579-587, 2009

Safety and Efficacy of Rituximab in SLE:136 Pts in the French Autoimmunity
Registry• 136 pts rx for SLE used SELENA-SLEDAI• Severe infections in 9% most w/I 3 months of RTX• 5 Deaths - 3 due to infection 2 refractory disease.• 80/113 pts responded ( 71%) – no difference between
RTX monotherapy and concurrent therapy.• Improvements by Organ System –
Articular ( 72% )cutaneous ( 70%)hematologic ( 88%)hematologic ( 88%) renal ( 74%)
• 41% relapse with response again in 91% with retreatment
Arthritis and Rheumatism 62:2458-2466, 2010
Efficacy and Safety of Rituximab in Moderately to Severely Active SLE: EXPLORER -A Randomized, Blinded Phase II/III Study
Rituximab + Prednisone Taper Arm (n = 169)
Treatment Period
Screening
Follow-up PeriodPlacebo + Prednisone Taper Arm (n=88)
Prednisone taper
Week 1
Weeks 1 and 2
(Days 1 and 15)
Week 10
Weeks 24 and 26
(Days 168 and 182)
Week 52
Week 78
= Study drug infusion; 2 x 1000 mg Rituximab/Placebo intravenous (IV)
= Prednisone (started at screening and taken daily during the study)
Merrill JT et al. Arthritis and Rheum 62:222-233, 2010
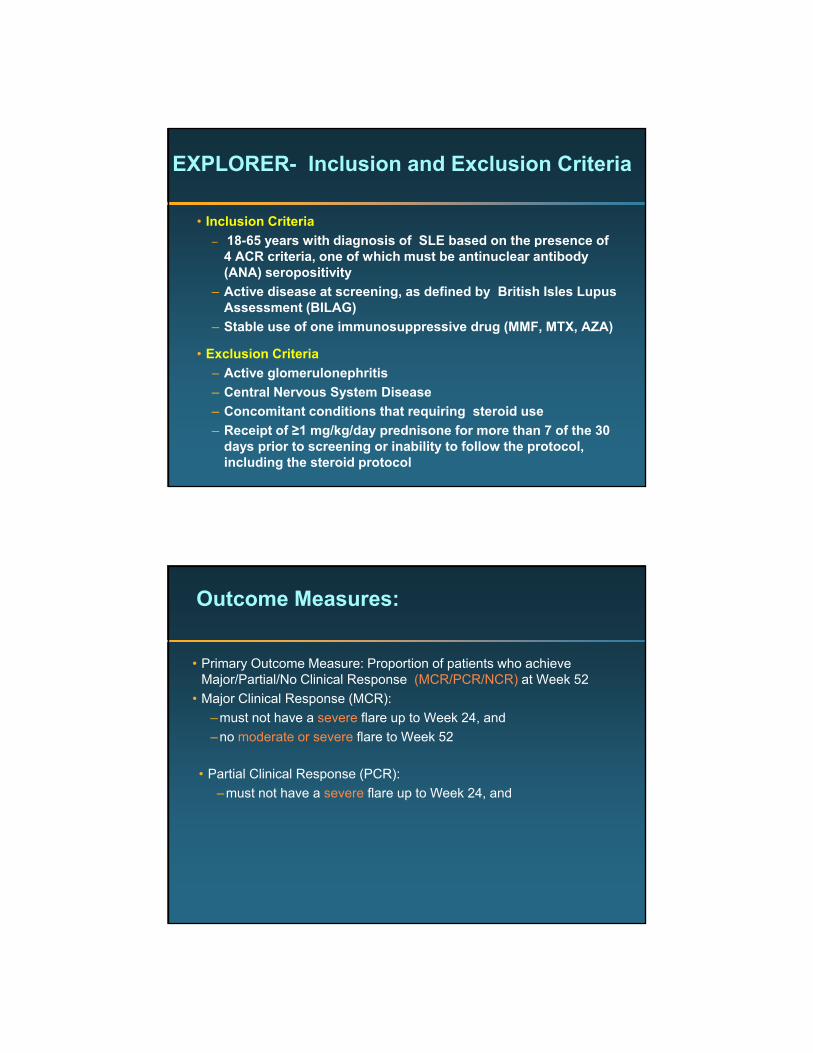
EXPLORER- Inclusion and Exclusion Criteria
• Inclusion Criteria– 18-65 years with diagnosis of SLE based on the presence of y g
4 ACR criteria, one of which must be antinuclear antibody (ANA) seropositivity
– Active disease at screening, as defined by British Isles Lupus Assessment (BILAG)
– Stable use of one immunosuppressive drug (MMF, MTX, AZA)
• Exclusion Criteria– Active glomerulonephritis– Central Nervous System Disease– Concomitant conditions that requiring steroid use – Receipt of ≥1 mg/kg/day prednisone for more than 7 of the 30
days prior to screening or inability to follow the protocol, including the steroid protocol
Outcome Measures:
• Primary Outcome Measure: Proportion of patients who achieve Major/Partial/No Clinical Response (MCR/PCR/NCR) at Week 52j p ( )
• Major Clinical Response (MCR):–must not have a severe flare up to Week 24, and–no moderate or severe flare to Week 52
• Partial Clinical Response (PCR):–must not have a severe flare up to Week 24, and
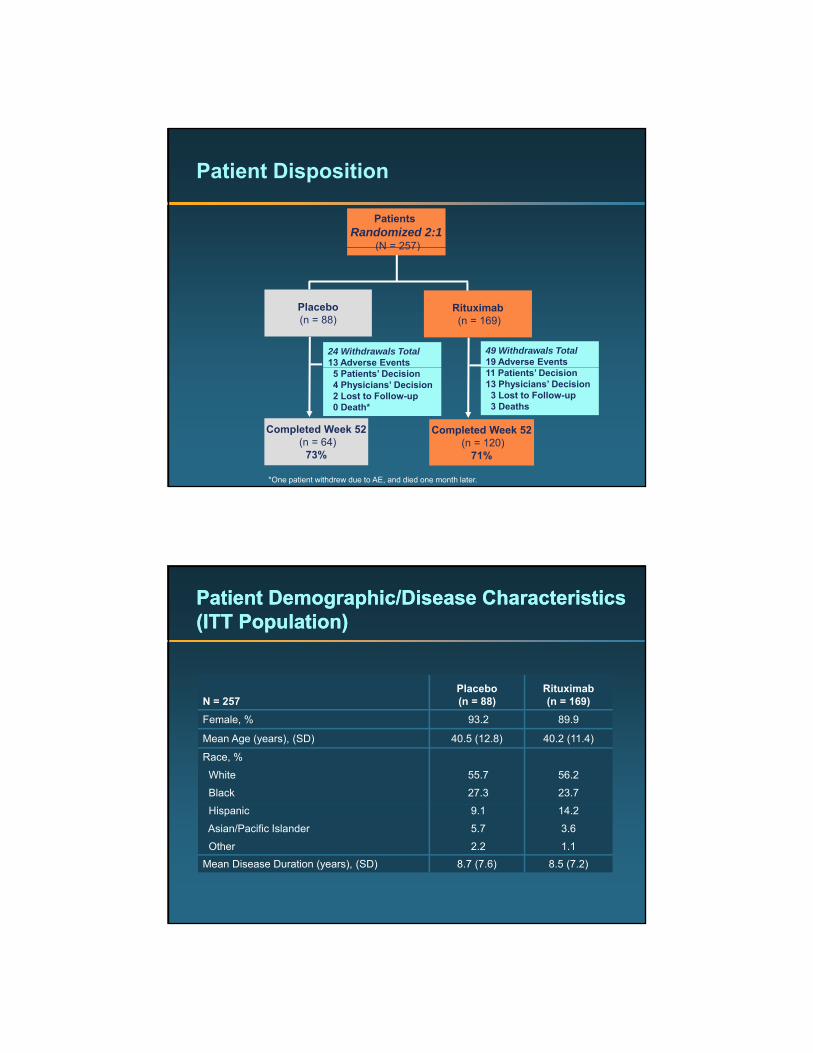
Patient Disposition
Patients Randomized 2:1
(N = 257)(N 257)
Placebo(n = 88)
Rituximab(n = 169)
24 Withdrawals Total13 Adverse Events
49 Withdrawals Total19 Adverse Events
Completed Week 52(n = 64)
73%
Completed Week 52(n = 120)
71%
5 Patients’ Decision4 Physicians’ Decision2 Lost to Follow-up0 Death*
11 Patients’ Decision13 Physicians’ Decision3 Lost to Follow-up3 Deaths
*One patient withdrew due to AE, and died one month later.
Patient Demographic/Disease CharacteristicsPatient Demographic/Disease Characteristics(ITT Population)(ITT Population)
Pl b Rit i bN = 257
Placebo(n = 88)
Rituximab(n = 169)
Female, % 93.2 89.9
Mean Age (years), (SD) 40.5 (12.8) 40.2 (11.4)
Race, %
White
Black
55.7
27.3
56.2
23.7
Hispanic
Asian/Pacific Islander
Other
9.1
5.7
2.2
14.2
3.6
1.1Mean Disease Duration (years), (SD) 8.7 (7.6) 8.5 (7.2)

Patient Background Drug UsePatient Background Drug Use(ITT Population)(ITT Population)
Placebo RituximabN = 257
Placebo(n = 88)
Rituximab(n = 169)
Chronic Prednisone Use, % 53.4 58.6Assigned Prednisone Dose 0.5 mg/kg0.75 mg/kg
61.429.5
62.732.0
1.0 mg/kg 9.1 5.3Background Immunosuppressive
Drug, %Mycophenolate Mofetil (MMF)Methotrexate (MTX)Azathioprine (AZA)
36.427.336.4
39.627.832.0

Primary Endpoint: Patients Achieving Clinical Response (ITT Population)
P=0.9750*
Responders
All early terminations treated as NCR.*p value is based on Wilcoxon Rank sum test stratified by race and baseline assigned prednisone dose.
No ClinicalResponse
PartialClinical
Response
MajorClinical
Response
MCR+PCR
Secondary Endpoint: Time to Moderate or Severe Flare Over 52 Weeks (Kaplan-Meier Plot) (ITT Population)
Placebo 126 days(median)
Rituximab 112 days
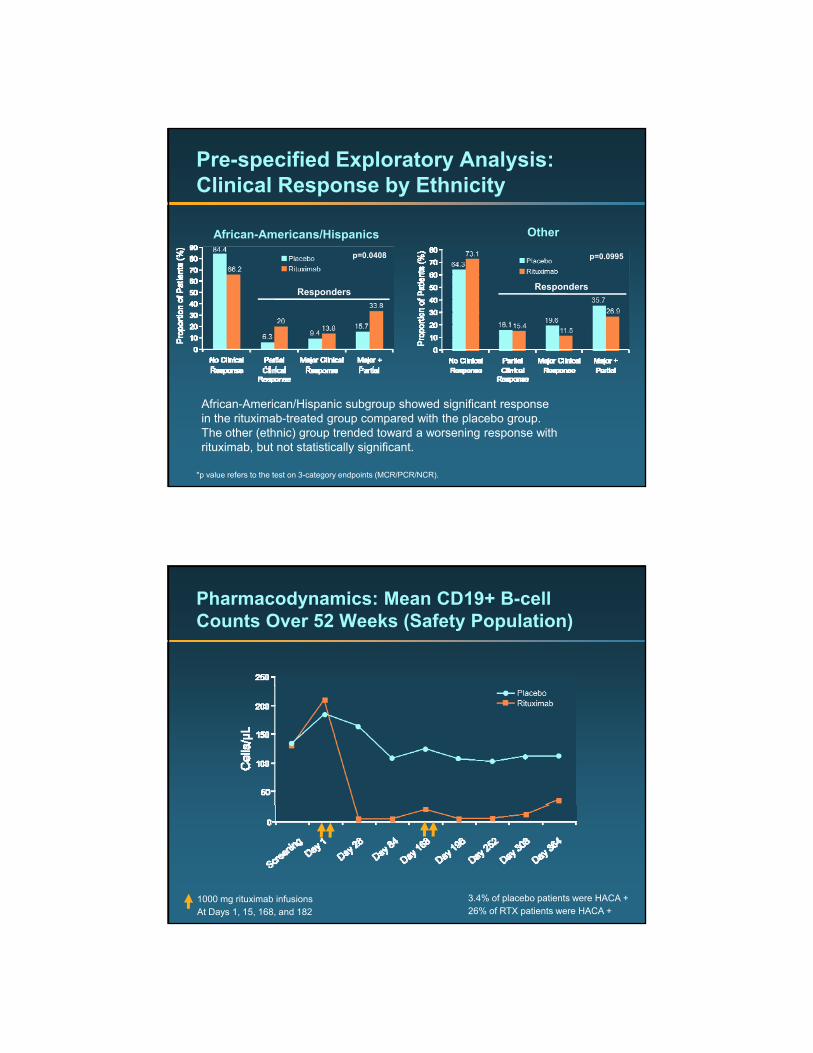
Pre-specified Exploratory Analysis: Clinical Response by Ethnicity
African-Americans/Hispanics Other
p=0.0408
Responders
p=0.0995
Responders
*p value refers to the test on 3-category endpoints (MCR/PCR/NCR).
African-American/Hispanic subgroup showed significant response in the rituximab-treated group compared with the placebo group.The other (ethnic) group trended toward a worsening response with rituximab, but not statistically significant.
Pharmacodynamics: Mean CD19+ B-cell Counts Over 52 Weeks (Safety Population)
1000 mg rituximab infusionsAt Days 1, 15, 168, and 182
3.4% of placebo patients were HACA +26% of RTX patients were HACA +

Biomarkers: Decreased Anti-double Stranded DNA Autoantibodies in Rituximab-treated Patients
Anti-dsDNA IgG*
p < 0.005
*Subset of patients who were anti-dsDNA+ at baseline
1000 mg rituximab infusionsAt Days 1, 15, 168, and 182
Biomarkers: Increased Complement Levels in Rituximab-treated Patients
C4 ComplementC3 Complement
***
*p=0.0029**p=0.0045P values based on Wilcoxon rank sum test
Prednisone Prednisone
1000 mg rituximab infusionsAt Days 1, 15, 168, and 182
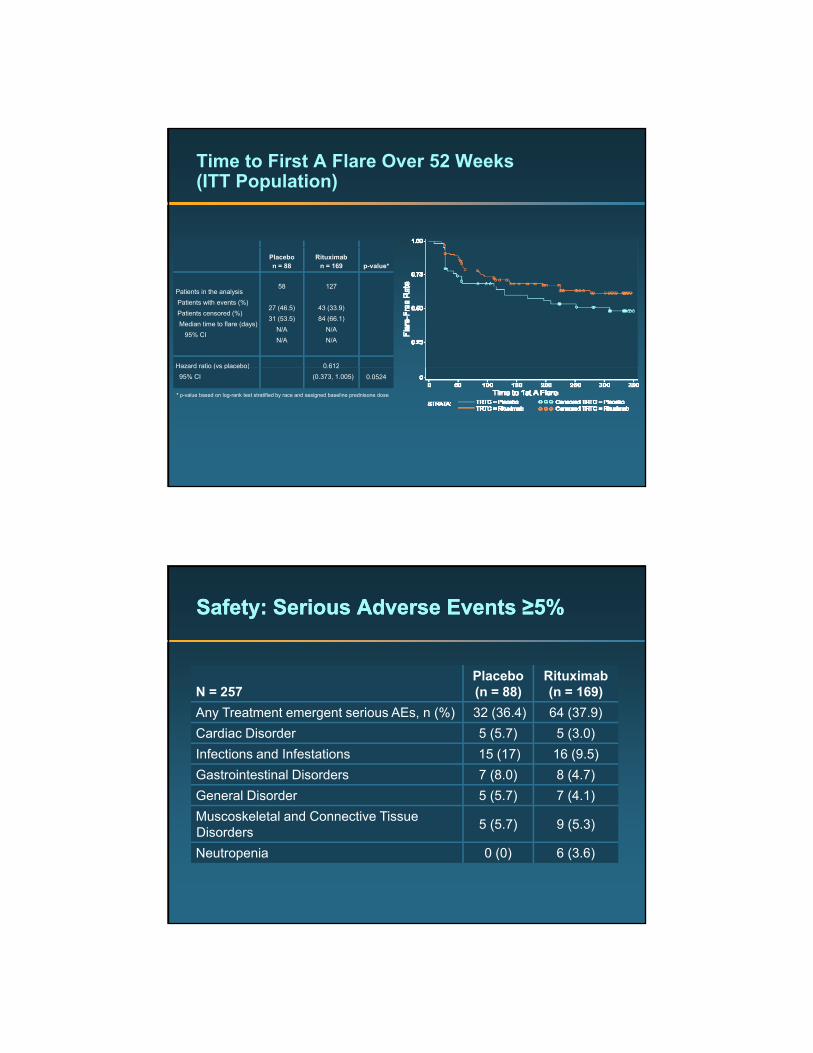
Time to First A Flare Over 52 Weeks (ITT Population)
Placebon = 88
Rituximabn = 169 p-value*
Patients in the analysis Patients with events (%)Patients censored (%)Median time to flare (days)
95% CI
58
27 (46.5)31 (53.5)
N/AN/A
127
43 (33.9)84 (66.1)
N/AN/A
Hazard ratio (vs placebo) 0 612Hazard ratio (vs placebo)95% CI
0.612(0.373, 1.005) 0.0524
* p-value based on log-rank test stratified by race and assigned baseline prednisone dose
Safety: Serious Adverse Events Safety: Serious Adverse Events ≥5%≥5%
Placebo RituximabN = 257 (n = 88) (n = 169) Any Treatment emergent serious AEs, n (%) 32 (36.4) 64 (37.9)Cardiac Disorder 5 (5.7) 5 (3.0)Infections and Infestations 15 (17) 16 (9.5)Gastrointestinal Disorders 7 (8.0) 8 (4.7)General Disorder 5 (5.7) 7 (4.1)Muscoskeletal and Connective Tissue Disorders 5 (5.7) 9 (5.3)
Neutropenia 0 (0) 6 (3.6)
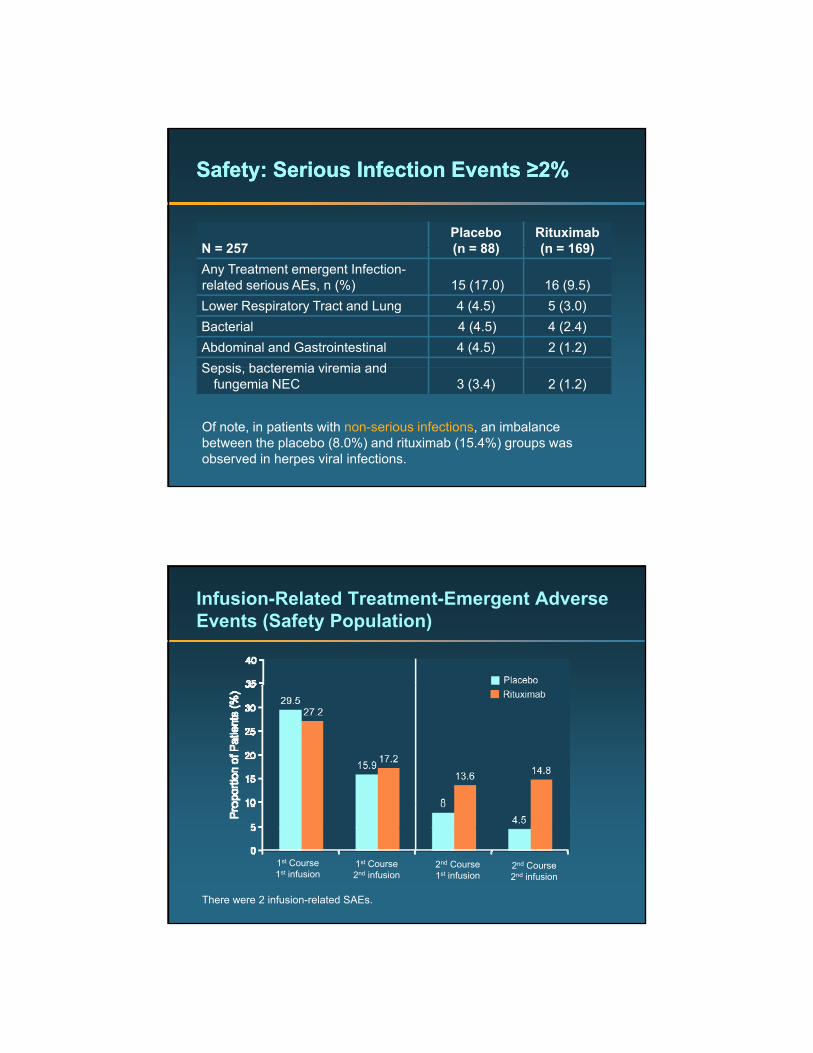
Safety: Serious Infection Events Safety: Serious Infection Events ≥2%≥2%
N = 257Placebo(n = 88)
Rituximab(n = 169)N = 257 (n = 88) (n = 169)
Any Treatment emergent Infection-related serious AEs, n (%) 15 (17.0) 16 (9.5)Lower Respiratory Tract and Lung 4 (4.5) 5 (3.0)Bacterial 4 (4.5) 4 (2.4)Abdominal and Gastrointestinal 4 (4.5) 2 (1.2)Sepsis bacteremia viremia andSepsis, bacteremia viremia and
fungemia NEC 3 (3.4) 2 (1.2)
Of note, in patients with non-serious infections, an imbalance between the placebo (8.0%) and rituximab (15.4%) groups was observed in herpes viral infections.
Infusion-Related Treatment-Emergent Adverse Events (Safety Population)
There were 2 infusion-related SAEs.
1st Course1st infusion
1st Course2nd infusion
2nd Course2nd infusion
2nd Course1st infusion

Placebo Rituximab*
Safety: Deaths
N = 257Placebo(n = 88)
Rituximab*(n = 169)
Cardiopulmonary arrest 1 (1.1) 0
Perforated Bowel 0 1 (0.6)
Multiple Drug Intoxication 0 1 (0.6)
Unknown Cause 0 1 (0.6)Unknown Cause 0 1 (0.6)
*One additional neonatal death of premature infant delivered at 33 weeks.
Conclusions (1)
• Primary and Secondary Endpoints– There were no statistically significant differences y g
between rituximab and placebo groups in primary or secondary endpoints in the ITT population.
• Exploratory Endpoints– The subgroup of patients of African or Hispanic
descent appear to be the most ill (or steroid resistant) and might show EXPLORER d d t t l ti– EXPLORER ensured a moderate to severely active extra-renal SLE population by entering patients with significant disease on background immune suppression, treating all patients with steroid doses significant enough to discourage entry of patients with minimal criteria.
Conclusions (2)
• Because of the need to treat this significant disease activity with moderate to high dose steroids the study design included tapering ofmoderate to high dose steroids, the study design included tapering of steroids to minimal doses by the second half of the study and used a high bar for response criteria, since steroids were expected to provide significant clinical benefit. Rituximab significantly depleted CD19+ B cells.
• Overall, adverse events and serious adverse events were balanced between the two groups and consistent with adverse eventsbetween the two groups and consistent with adverse events observed in rheumatoid arthritis clinical trials.– A higher proportion of patients in the placebo group had serious
infection-related events, and a higher proportion of patients in the rituximab-treated group had non-serious herpes viral infections.
Efficacy and Safety of Rituximab in Patients with Proliferative Lupus Nephritis: Results from the Randomized, Double-blind Phase III LUNAR,(LUpus Nephritis Assessment with Rituximab)StudyRovin et al ASN 2009

LUNAR Study Design
Rituximab + MMF (n=72)
Treatment Period
Screening
Follow-up PeriodPlacebo + MMF (n=72)
Prednisone taper
Weeks 1 and 2
(Days 1 and 15)
Week 16
Weeks 24 and 26
(Days 168 and 182)
Week 52
Week 78
= Study drug infusion.
= Corticosteroids: • 1000 mg IV methlyprednisolone given at days 1 and then days 2, 3, or 4• Oral prednisone initiated at 0.75 mg/kg/day after IV steroids and then tapered to
10 mg/day by day 112
Key Inclusion and Exclusion Criteria
• Inclusion Criteria– Age 16-75 years with SLE by ACR criteria, including history
f iti ti l tib di (ANA)of positive antinuclear antibodies (ANA)– ISN/RPS Class III or IV lupus nephritis (active or
active/chronic disease) as evidenced by renal biopsy ≤12 months prior to randomization (concurrent class V allowed)
– Proteinuria, with urine protein:creatinine ratio >1.0• Exclusion Criteria
– >50% of glomeruli with sclerosis and/or interstitial fibrosis on renal biopsy
– Estimated glomerular filtration rate <25 mL/min per 1.73 m2
or ESRD– CNS diseae– Thrombocytopenia at high risk for significant bleeding

Primary Endpoint (Renal Response)
• Proportion of patients who achieve a renal response at Week 52, grouped into one of three mutually exclusive categories
Complete Renal Response (CRR)– Complete Renal Response (CRR)Normalization of serum creatinine OR ≤15% greater than baseline if day 1 serum creatinine within normal range of central labInactive urinary sedimentUrinary protein to creatinine ratio <0.5
– Partial Renal Response (PRR)Serum creatinine ≤15% above baseline value No significant worsening of urinary sediment50% improvement in the urine protein to creatinine ratio, with one of the following conditions met
» If baseline ratio ≤3.0, then urine protein to creatinine ratio <1.0» If baseline ratio >3.0, then urine protein to creatinine ratio <3.0
– Non-Response (NR)Not achieving either a complete or partial renal response
» All early study terminations and patients starting a new immunosuppressant were considered non-responders
Secondary Endpoints
• Clinical measures– Proportion of patients who achieve a CRR at Week 52– Time to CRR– Proportion of patients with a baseline urine protein to creatinine
ratio >3.0 who achieve a ratio <1.0 at Week 52– Time-adjusted AUCMB of BILAG over 52 weeks– Change from baseline in SF-36 Physical function score
• Serologic measures– Change in anti-dsDNA from baseline to Week 52– Change in complement levels (C3, C4) from baseline to
Week 52
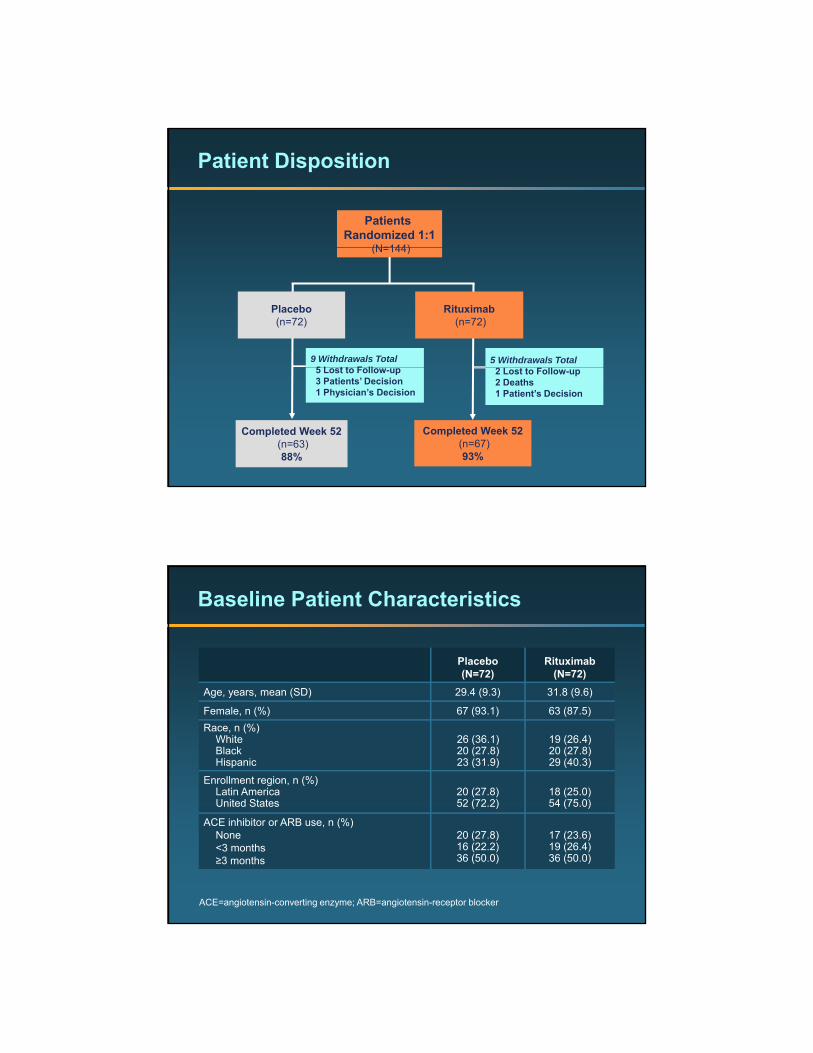
Patient Disposition
Patients Randomized 1:1
(N=144)(N=144)
Placebo(n=72)
Rituximab(n=72)
9 Withdrawals Total5 L t t F ll
5 Withdrawals Total
Completed Week 52(n=63)88%
Completed Week 52(n=67)93%
5 Lost to Follow-up3 Patients’ Decision1 Physician’s Decision
2 Lost to Follow-up2 Deaths1 Patient’s Decision
Baseline Patient Characteristics
Placebo(N=72)
Rituximab(N=72)
Age, years, mean (SD) 29.4 (9.3) 31.8 (9.6)
Female, n (%) 67 (93.1) 63 (87.5) Race, n (%)
WhiteBlackHispanic
26 (36.1)20 (27.8)23 (31.9)
19 (26.4)20 (27.8)29 (40.3)
Enrollment region, n (%)Latin AmericaUnited States
20 (27.8)52 (72 2)
18 (25.0)54 (75 0)United States 52 (72.2) 54 (75.0)
ACE inhibitor or ARB use, n (%)None<3 months≥3 months
20 (27.8)16 (22.2)36 (50.0)
17 (23.6)19 (26.4)36 (50.0)
ACE=angiotensin-converting enzyme; ARB=angiotensin-receptor blocker

Patient Disease Characteristics
Placebo(N=72)
Rituximab(N=72)
Urine protein:creatinine ratio, mean (SD) 4.2 (3.0) 3.8 (2.8)
Serum creatinine, mg/dL, mean (SD) 1.0 (0.5) 1.0 (0.5)
Estimated GFR (mL/min), mean (SD)<60, n (%)≥60, n (%)
96.0 (51.1)20 (27.8)52 (72.2)
87.7 (34.9)17 (23.6)55 (76.4)
Serum albumin, g/L, mean (SD) 2.6 (0.7) 2.7 (0.8)
ISN/RPS classification n (%)ISN/RPS classification, n (%)Class IIIClass IVClass V (coexistent)
24 (33.3)48 (66.7)23 (31.9)
25 (34.7)47 (65.3)26 (36.1)
BILAG index global score, mean (SD) 15.3 (6.2) 15.3 (6.4)
ISN/RPS=International Society of Nephrology/Renal Pathology SocietyBILAG=British Isles Lupus Assessment Group
Primary Endpoint: Renal Response at Week 52
54.160
Placebo (N=72) Rituximab (N=72)
30.6
15.3
26.430.6
43.0
10
20
30
40
50
Prop
ortio
n of
Pat
ient
s
P=0.55*P=0.55*
0Complete Renal Response (CRR)
Partial Renal Response (PRR)
No Response (NR)
* Wilcoxon Rank-sum test to compare the proportions of (CRR, PRR, NR) between rituximab and placeboMean MMF dose: Placebo: 2.4±0.62 g; Rituximab: 2.7±0.41 g

Renal Response Rates Over Time
Rituximab infusions (1000 mg)PLC=placebo, RTX=rituximab, CRR=complete renal response, PRR=partial renal response
Secondary Endpoints
EndpointPlacebo(N=72)
Rituximab(N=72) P-value
ClinicalClinical
Percent of patients with baseline Upr:Ucr >3 who achieve a Upr:Ucr <1 at Week 52
22/41
(53.7)
18/38
(47.4) 0.51
Time to first CRR (months), median 12.12 11.99 0.63
Change from baseline in SF-36 Physical function score 5.7 (9.4) 4.8 (10.4) 0.59
Time-adjusted AUCMB of BILAG index global -8.6 (5.1) -8.5 (5.8) 0.93
Serological (Compared to baseline)
Anti-double-stranded DNA, geometric mean* 0.50 0.31 0.007
Complement C3, mean (SD)** 25.9 (32.5) 37.5 (28.7) 0.025
Complement C4, mean (SD)** 6.6 (8.9) 9.9 (7.5) 0.015
*% of baseline.** absolute change from baseline.
Upr=Urine protein; Ucr=Urine creatinineAUCMB=Area under curve minus baseline
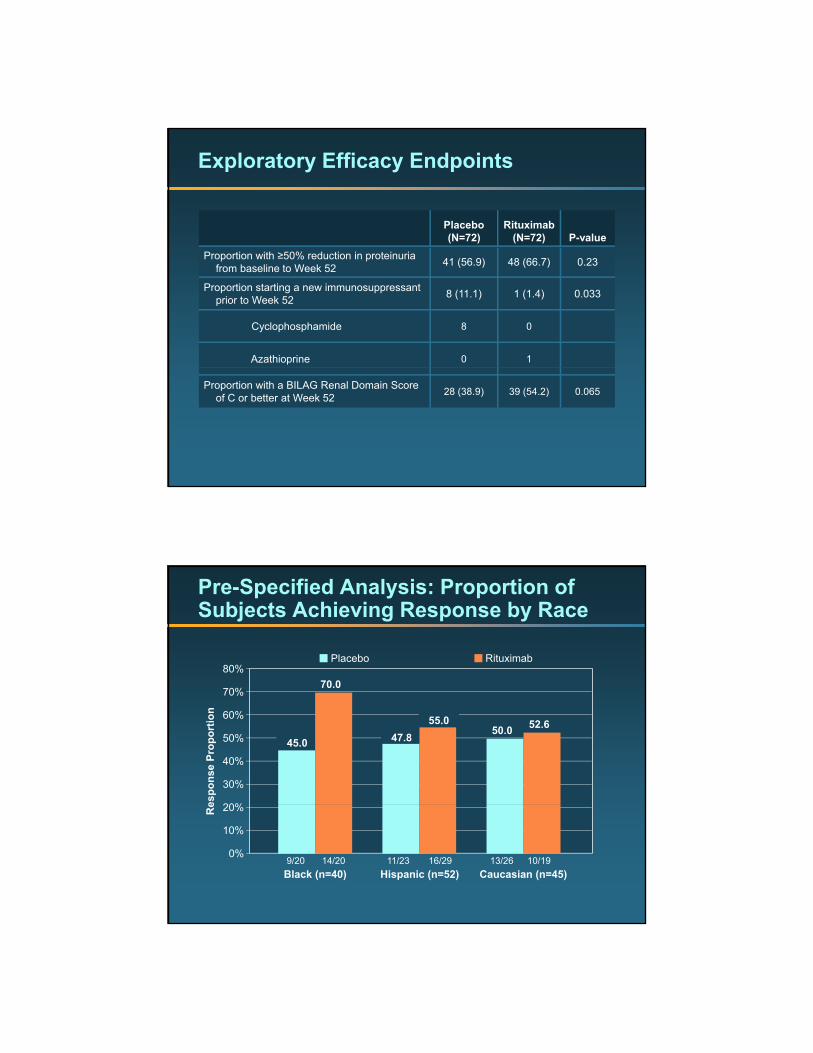
Exploratory Efficacy Endpoints
Placebo(N=72)
Rituximab(N=72) P-value
Proportion with ≥50% reduction in proteinuria from baseline to Week 52 41 (56.9) 48 (66.7) 0.23
Proportion starting a new immunosuppressant prior to Week 52 8 (11.1) 1 (1.4) 0.033
Cyclophosphamide 8 0
Azathioprine 0 1
Proportion with a BILAG Renal Domain Score of C or better at Week 52 28 (38.9) 39 (54.2) 0.065
Pre-Specified Analysis: Proportion of Subjects Achieving Response by Race
70 080%
Placebo Rituximab
45.0 47.8 50.0
70.0
55.0 52.6
20%
30%
40%
50%
60%
70%
espo
nse
Prop
ortio
n
9/20 14/20 11/23 16/29 13/26 10/190%
10%
20%
Black (n=40) Hispanic (n=52) Caucasian (n=45)
Re
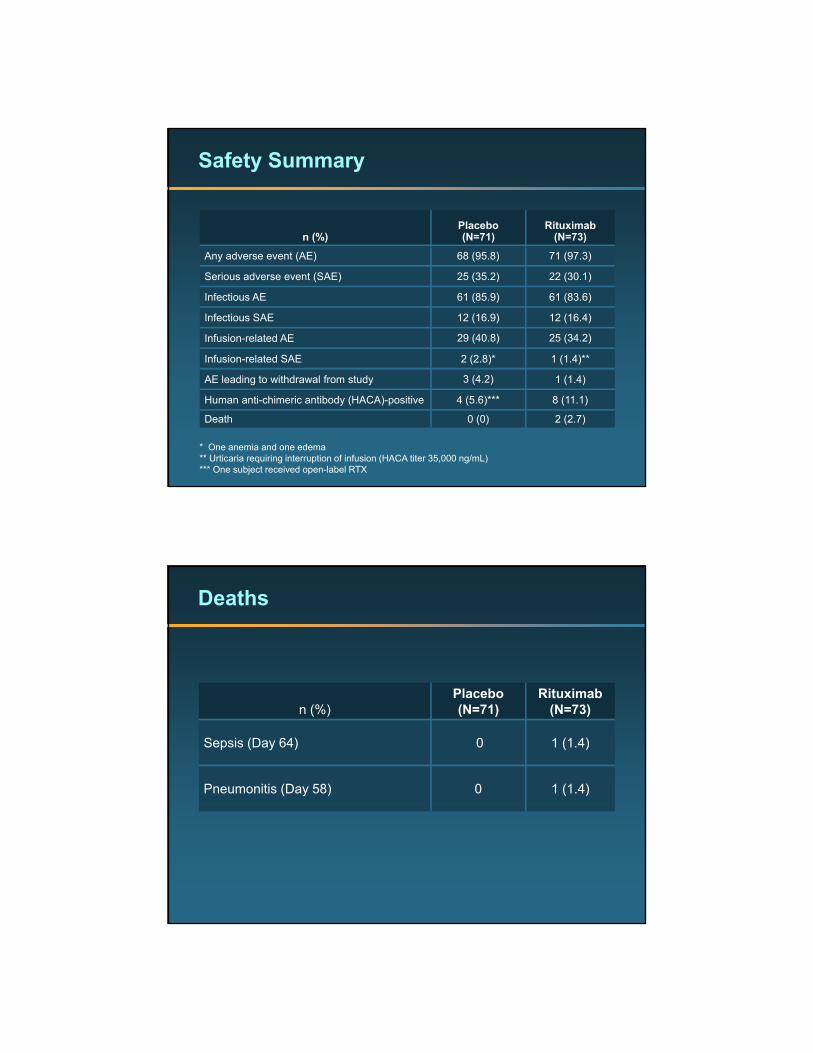
Safety Summary
n (%)Placebo(N=71)
Rituximab(N=73)
Any adverse event (AE) 68 (95.8) 71 (97.3)
Serious adverse event (SAE) 25 (35.2) 22 (30.1)
Infectious AE 61 (85.9) 61 (83.6)
Infectious SAE 12 (16.9) 12 (16.4)
Infusion-related AE 29 (40.8) 25 (34.2)
Infusion-related SAE 2 (2.8)* 1 (1.4)**
AE leading to withdrawal from study 3 (4.2) 1 (1.4)
Human anti-chimeric antibody (HACA)-positive 4 (5.6)*** 8 (11.1)
Death 0 (0) 2 (2.7)
* One anemia and one edema** Urticaria requiring interruption of infusion (HACA titer 35,000 ng/mL)*** One subject received open-label RTX
Deaths
n (%)Placebo(N=71)
Rituximab(N=73)
Sepsis (Day 64) 0 1 (1.4)
Pneumonitis (Day 58) 0 1 (1.4)
Conclusions
• To date, LUNAR is the largest randomized, placebo-controlled trial to evaluate rituximab as a therapeutic intervention in LN
• Although there were numerically more responders in the rituximab group (57% vs. 46%), the study did not show a statistically significant difference in primary or clinical secondary endpoints at week 52
• Rituximab had a statistically significant effect on levels of anti-dsDNA and complement at week 52; however, the clinical significance of this is unclearis unclear
• Adverse events and serious adverse events were similar in frequency between groups, with no new or unexpected safety signals
Conclusions on the Use of Rituximab in SLE and LN
• Rituximab appears to work as rescue therapy for some pts with relapsing or refractoryfor some pts with relapsing or refractory disease.
• Rituximab must be used with other therapies e.g. steroids etc
• It’s role as a first line agent in Induction for LN remains to be defined.
• It may have a role in maintenance therapy.• Rituximab is “an interesting therapeutic
option”


















