Right ventricular failure in acute lung injury and acute ... · 1970s that ARDS is a clinical ......
8
Vol. 78 - No. 8 MINERVA ANESTESIOLOGICA 941 REVIEW T he mortality of acute respiratory distress syndrome (ARDS) remains significant 1, 2 despite improved knowledge of its pathophysi- ology and routine application of protective me- chanical ventilation. One of the crucial issues in management of patients suffering from ARDS is to compensate and to limit pulmonary vascular dysfunction. It has been well known since the 1970s that ARDS is a clinical entity that involves not only alveolar lesions but also pulmonary capillary lesions, leading to pulmonary hyper- tension. 3 e reversible pulmonary vascular re- modeling which usually occurs has many differ- ent mediators. 4 e hemodynamic consequences of such remodeling have forced physicians to pay attention to the right ventricle. Many studies have now demonstrated the deleterious impact of pulmonary hypertension and of right ven- tricular (RV) dysfunction on prognosis. In a re- cent study using the pulmonary artery catheter, Bull et al. reported that the degree of pulmonary vascular dysfunction, according to the transpul- monary gradient (mean pulmonary artery pres- sure minus pulmonary artery occlusion pres- sure, PAOP), was independently associated with prognosis. 5 Osman et al. using the same invasive approach demonstrated that central venous pres- sure (CVP) higher than PAOP was a strong and independent predictor of mortality. 6 Finally, we suggested in a large series that acute cor pulmo- nale (ACP) diagnosed by echocardiography was associated with mortality in patients ventilated with a plateau pressure (Pplat) of 27 cmH 2 O or more. 7 In this review, we describe how and why the right ventricle should be protected in patients with ARDS, leading to a different approach for ventilation called the “RV protective approach”. Right ventricular failure in acute lung injury and acute respiratory distress syndrome X. REPESSÉ 1, 2 , C. CHARRON 1 , A. VIEILLARD-BARON 1, 2 1 Assistance Publique-Hôpitaux de Paris, University Hospital Ambroise Paré, Intensive Care Unit, Section orax- Vascular Disease-Abdomen-Metabolism, Boulogne-Billancourt, France; 2 Faculty of Medicine Paris Ile-de-France Ouest, University of Versailles Saint-Quentin en Yvelines, Saint-Quentin en Yvelines, France ABSTRACT Acute respiratory distress syndrome (ARDS) is a clinical entity involving not only alveolar lesions but also capil- lary lesions, both of which have deleterious effects on the pulmonary circulation, leading to constant pulmonary hypertension and to acute cor pulmonale (ACP) in 20-25% of patients ventilated with a limited plateau pressure (Pplat). Considering the poor prognosis of patients suffering from such acute right ventricular (RV) dysfunction, RV protection by appropriate ventilatory settings has become a crucial issue in ARDS management. e goal of this review is to emphasize the importance of analyzing RV function in ARDS, using echocardiography, in order to limit RV afterload. Any observed acute RV dysfunction should lead physicians to consider a strategy for RV protection, including strict limitation of Pplat, diminution of positive end-expiratory pressure (PEEP) and control of hypercap- nia, all goals achieved by prone positioning. (Minerva Anestesiol 2012;78:941-8) Key words: Respiratory distress syndrome, adult - Heart ventricles - Pulmonary heart disease - Echocardiography, COPYRIGHT © 2012 EDIZIONI MINERVA MEDICA This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies (either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is not permitted. It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo, or other proprietary information of the Publisher.
-
Upload
truongminh -
Category
Documents
-
view
218 -
download
0
Transcript of Right ventricular failure in acute lung injury and acute ... · 1970s that ARDS is a clinical ......

Vol. 78 - No. 8 MINERVA ANESTESIOLOGICA 941
R E V I E W
Anno: 2012Mese: AugustVolume: 78No: 8Rivista: MINERVA ANESTESIOLOGICACod Rivista: Minerva Anestesiol
Lavoro: titolo breve: RIGHT VENTRICULAR FAILURE IN ACUTE LUNG INJURY AND ARDSprimo autore: REPESSÉpagine: 941-8
The mortality of acute respiratory distress syndrome (ARDS) remains significant 1, 2
despite improved knowledge of its pathophysi-ology and routine application of protective me-chanical ventilation. One of the crucial issues in management of patients suffering from ARDS is to compensate and to limit pulmonary vascular dysfunction. It has been well known since the 1970s that ARDS is a clinical entity that involves not only alveolar lesions but also pulmonary capillary lesions, leading to pulmonary hyper-tension.3 The reversible pulmonary vascular re-modeling which usually occurs has many differ-ent mediators.4 The hemodynamic consequences of such remodeling have forced physicians to pay attention to the right ventricle. Many studies have now demonstrated the deleterious impact of pulmonary hypertension and of right ven-tricular (RV) dysfunction on prognosis. In a re-
cent study using the pulmonary artery catheter, Bull et al. reported that the degree of pulmonary vascular dysfunction, according to the transpul-monary gradient (mean pulmonary artery pres-sure minus pulmonary artery occlusion pres-sure, PAOP), was independently associated with prognosis.5 Osman et al. using the same invasive approach demonstrated that central venous pres-sure (CVP) higher than PAOP was a strong and independent predictor of mortality.6 Finally, we suggested in a large series that acute cor pulmo-nale (ACP) diagnosed by echocardiography was associated with mortality in patients ventilated with a plateau pressure (Pplat) of 27 cmH2O or more.7
In this review, we describe how and why the right ventricle should be protected in patients with ARDS, leading to a different approach for ventilation called the “RV protective approach”.
Right ventricular failure in acute lung injury and acute respiratory distress syndrome
X. REPESSÉ 1, 2, C. CHARRON 1, A. VIEILLARD-BARON 1, 2
1Assistance Publique-Hôpitaux de Paris, University Hospital Ambroise Paré, Intensive Care Unit, Section Thorax-Vascular Disease-Abdomen-Metabolism, Boulogne-Billancourt, France; 2Faculty of Medicine Paris Ile-de-France Ouest, University of Versailles Saint-Quentin en Yvelines, Saint-Quentin en Yvelines, France
A B S T R A C TAcute respiratory distress syndrome (ARDS) is a clinical entity involving not only alveolar lesions but also capil-lary lesions, both of which have deleterious effects on the pulmonary circulation, leading to constant pulmonary hypertension and to acute cor pulmonale (ACP) in 20-25% of patients ventilated with a limited plateau pressure (Pplat). Considering the poor prognosis of patients suffering from such acute right ventricular (RV) dysfunction, RV protection by appropriate ventilatory settings has become a crucial issue in ARDS management. The goal of this review is to emphasize the importance of analyzing RV function in ARDS, using echocardiography, in order to limit RV afterload. Any observed acute RV dysfunction should lead physicians to consider a strategy for RV protection, including strict limitation of Pplat, diminution of positive end-expiratory pressure (PEEP) and control of hypercap-nia, all goals achieved by prone positioning. (Minerva Anestesiol 2012;78:941-8)Key words: Respiratory distress syndrome, adult - Heart ventricles - Pulmonary heart disease - Echocardiography,
COPYRIGHT© 2012 EDIZIONI MINERVA MEDICA
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

REPESSÉ RIGHT VENTRICULAR FAILURE IN ACUTE LUNG INJURY AND ARDS
942 MINERVA ANESTESIOLOGICA August 2012
For this purpose, we briefly discuss the physiolo-gy and the pathophysiology of the right ventricle in normal conditions and during ARDS, before demonstrating the crucial role of echocardiogra-phy in the diagnosis of right heart failure.
Physiology and pathophysiology of the right ventricle
RV characteristics
The right ventricle is composed of two cham-bers wrapping the left ventricle around its short axis. The filling chamber is in a posterior-ante-rior axis and has a triangular shape. The outflow chamber looks like a crescent in an inferior-su-perior axis (Figure 1). In normal conditions, the right ventricle ejects blood into a low-resistance and high-compliance system, which explains why, unlike the left ventricle, its isovolumetric contrac-tion pressure is very low and its isovolumetric re-laxation is insignificant.8 In other words, the right ventricle nearly acts as a passive conduit. This is why its systolic function is very sensitive to any slight increase in pulmonary vascular resistance, which will easily exceed its capacity of adapta-tion, leading to systolic overload and dysfunction. However, thanks to its low diastolic elastance, the right ventricle is able to adapt to a certain degree by dilating:9 its diastolic function is tolerant.
RV function and ventilation
During spontaneous breathing, the right ven-tricle is acting in the best conditions. Venous return is optimal thanks a continuous negative pleural pressure 10 and RV afterload is limited because of a low transpulmonary pressure.11
The situation is quite different during positive pressure ventilation,12 especially in patients with a lung injury with decreased compliance. Decrease in systemic venous return results from a less nega-tive, even positive, pleural pressure.10 It could also be related to a partial or complete collapse of the thoracic part of the superior vena cava.13 Effect on venous return is increased by application of positive end-expiratory pressure (PEEP).14
Increase in RV afterload is related to an eleva-tion in transpulmonary pressure (alveolar pressure
minus pleural pressure). This mainly occurs if the tidal volume is excessive and/or if lung compliance is severely decreased, two conditions where the pulmonary capillaries may be crushed by alveoli.15
How to diagnose RV function impairment in critically-ill patients ventilated for an ARDS
As explained above, uncoupling between the right ventricle and the pulmonary circulation may lead to a pattern of ACP. Testa gave the first clinical description of ACP in 1831.16 Currently, ACP is optimally diagnosed using echocardiog-raphy, even though some surrogates may be de-tected using invasive devices.
Invasive approach
Many studies have evaluated RV function and the pulmonary circulation in ARDS us-ing the pulmonary artery catheter (PAC). RV systolic dysfunction was historically defined by a CVP>PAOP in patients with RV myocardial infarction.17, 18 In ARDS, this was proposed by Monchi et al.19 and recently by Osman et al. in a series of patients undergoing protective mechan-ical ventilation.6 In the latter study, RV failure was distinguished from RV dysfunction by an RV stroke index below 30 mL/m-2.6 Using fast-response thermodilution, Jardin et al. showed in 18 ARDS patients that RV volume estima-tion was a better indicator of RV preload than
Figure 1.—Magnetic resonance imaging of heart chambers. Dotted arrow represents the axis of the RV filling chamber and solid arrow represents axis of the RV outflow chamber. RV: right ventricle, LV: left ventricle, PA: pulmonary artery
COPYRIGHT© 2012 EDIZIONI MINERVA MEDICA
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

RIGHT VENTRICULAR FAILURE IN ACUTE LUNG INJURY AND ARDS REPESSÉ
Vol. 78 - No. 8 MINERVA ANESTESIOLOGICA 943
to evaluate the effects of lung injury and of posi-tive pressure ventilation on RV function, so as to adapt ventilatory strategy, as explained below.
ACP combines RV dilatation (RV diastolic over-load) and paradoxical septal motion at end-systole (RV systolic overload). Figure 3 depicts the pattern of ACP recorded by TTE and TEE. RV size is eval-uated using a four-chamber view by a transthoracic or a transesophageal approach. When dilated, the right ventricle loses the triangular shape of its fill-ing chamber. We defined RV dilatation as moder-ate when the ratio between right and left ventricu-lar end-diastolic areas is >0.6 and as severe for a ratio >1.23 In the latter situation, simple qualita-tive detection is sufficient. RV dilatation is usually associated with right atrial and inferior vena caval dilatation and tricuspid regurgitation, easily visual-ized using the color Doppler mode.24
Paradoxical septal motion is well-visualized on a short-axis view of the left ventricle, ideally at the RV outflow track. It is related to an inverted pres-sure gradient between right and left ventricles, oc-curring at end-systole,25, 26 and reflecting RV ejec-tion obstruction. Usually, detection of paradoxical septal motion is qualitative: there is or there is not. In some situations, as clinical research, LV systo-lic eccentricity index can be calculated to evaluate the degree of RV systolic overload.27
Briefly, Doppler analysis of the pulmonary ar-tery flow can also be helpful and very informative on the (in)ability of the right ventricle to overcome its afterload. It may be obtained from the great vessel view. Figures 4, 5 report the two parameters
were measurements of pressure.20 De Monte et al. demonstrated similar results in 36 patients.21 Fast-response thermodilution may also be used to calculate RV ejection fraction.
The pulmonary circulation may also be evaluat-ed in ARDS patients by an invasive approach. Pul-monary vascular resistance (PVR) is probably not accurate in this very special situation where any change in cardiac output leads to change in PVR.3 This reflects the flow-dependent competition be-tween alveoli (and their distending pressure) and pulmonary capillaries. More interestingly, 30 years ago, Marland and Glauser assessed the gradient between diastolic pulmonary artery pressure and PAOP to evaluate the effects of PEEP22 (Figure 2). More recently, Bull et al. used the transpulmonary pressure gradient as the difference between mean pulmonary artery pressure and PAOP.5 In close to 500 ARDS patients, they found that 73% of pa-tients had an elevated gradient (≥12 mmHg).5
Echocardiography, the cornerstone of the diagnosis
In ARDS, echocardiography can easily be performed by a transthoracic (TTE) or a trans-esophageal (TEE) approach. We routinely prefer the latter, as we consider it to be less operator-de-pendent and more reproducible, providing pa-tients are intubated and ventilated. We consider that RV evaluation in this field should mainly be qualitative, using a focused and simple approach, mainly based on the four-chamber, short-axis view and the great vessel views. The main goal is
Figure 2.—Pressure gradient between diastolic pulmonary artery pressure (PAP) and pulmonary capillary wedge pressure (PCWP) induced by application of a high PEEP.
PAP
PAP
PCWP
PCWP
PEEP 0 cm H20 PEEP 20 cm H
20
mmHg
O
2O
COPYRIGHT© 2012 EDIZIONI MINERVA MEDICA
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

REPESSÉ RIGHT VENTRICULAR FAILURE IN ACUTE LUNG INJURY AND ARDS
944 MINERVA ANESTESIOLOGICA August 2012
in a large series of more than 200 patients where incidence was 22%.30 In another study, we re-ported a much higher incidence, i.e. 50%, but the population was selected and consisted of patients with particularly severe ARDS and a PaO2/FIO2 below 100 mmHg after 2 days of ventilation.31 This demonstrates something easily understanda-ble, that the incidence of RV dysfunction increases as we go from acute lung injury to ARDS and to severe ARDS, according to alterations in respira-tory mechanics. Interestingly, a recent TTE study performed in 21 patients with H1N1 influenza-related ALI/ARDS found that 83% exhibited RV dilatation and 30% had ACP.32
Many studies in acute lung injury have clearly demonstrated that respiratory settings and ventila-tory strategy may significantly affect RV function. First, using TEE we recently emphasized that the impact of positive pressure ventilation on the right
that we usually look for, i.e. respiratory variation of pulmonary flow and a biphasic flow pattern.24
Incidence of ACP and impact of respiratory settings
Incidence of ACP may be considered before and after implementation of protective mechani-cal ventilation. Before, Jardin et al. used TTE to characterize RV function in a small series of 25 patients with ARDS ventilated with high airway pressure.28 They reported an incidence as high as 60% of ACP and all patients with a severely di-lated right ventricle died.28 After, most studies are summarized in Table I. In particular, we reported in 75 patients ventilated with a Pplat <30 cmH2O and a PEEP of 7 cmH2O an incidence of ACP of 25% after 2 days of mechanical ventilation.29 This was recently confirmed by Mekontso-Dessap et al.
Figure 3.—Acute cor pulmonale in a patient ventilated for severe ARDS, visualized by transthoracic (left side) and transesophageal (right side) echocardiography on the same day. Top: Four-chamber view, showing the severely dilated right ventricle. Bottom: short-axis view of the left ventricle, showing paradoxical septal motion at end-systole (arrow) with the “D-shape” of the left ven-tricle. RV: right ventricle LV: left ventricle, RA: right atrium, LA: left atrium
COPYRIGHT© 2012 EDIZIONI MINERVA MEDICA
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.
RIGHT VENTRICULAR FAILURE IN ACUTE LUNG INJURY AND ARDS REPESSÉ
Vol. 78 - No. 8 MINERVA ANESTESIOLOGICA 945
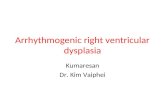
hypercarbia, which is a strong vasoconstrictor of the pulmonary circulation, and right ventricular overload has been demonstrated in humans.36
A different ventilatory strategy: the RV protective approach
The concept of this approach can be summa-rized in few words: “what is good for the right ventricle is good for the lung”.
The first goal of the RV protective approach (Table II) is to limit Pplat. In the case of RV dysfunction with hemodynamic consequences,
ventricle is directly related to tidal volume.33 Simi-larly, in a large series of more than 350 patients, we reported that incidence of ACP was strongly related to Pplat:7 10% for a Pplat between 18 and 26 cmH2O, >30% for a Pplat between 27 and 35 cmH2O and finally 60% for a Pplat >35 cm-H2O.7 Second, PEEP may also overload the right ventricle at both inspiration and expiration.34 We recently demonstrated in severe ARDS patients that a ventilatory strategy promoting “high” PEEP was deleterious for the right ventricle despite a strict limitation of Pplat.35 Finally, hypercapnia may worsen the effect of mechanical ventilation on RV afterload, since a direct relation between
Figure 5.—Pulsed Doppler analysis of pulmonary artery flow obtained by a transesophageal approach during PEEP titration (0, 6 and 13 cmH2O). Note the drop in pulmonary artery blood flow, at end-inspiration and also end-expiration, when PEEP increases.
Figure 4.—Pulmonary artery flow recorded by pulsed wave Doppler by a transesophageal approach in a patient ventilated for severe ARDS. After 2 days on mechanical ventilation (panel A), plateau pressure was elevated and pulmonary artery flow had a biphasic pattern (arrow), reflecting a huge obstruction of the ejection. After 3 sessions of prone positioning (panel B), plateau pressure significantly decreased and the pulmonary flow was completely normalized. Vt: tidal volume, Pplat: plateau pressure.
ZEEP PEEP 6 cm H2O PEEP 13 cm H
2O
COPYRIGHT© 2012 EDIZIONI MINERVA MEDICA
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.
REPESSÉ RIGHT VENTRICULAR FAILURE IN ACUTE LUNG INJURY AND ARDS
946 MINERVA ANESTESIOLOGICA August 2012
ing the respiratory rate, without inducing intrin-sic PEEP, which also has deleterious effects on the right ventricle.29
In some patients, those with the most severe ARDS, blood gas control, respiratory mechan-ics and RV protection are difficult to combine. Then, prone positioning should be proposed. By recruiting the lung, thus decreasing airway pressure, and by increasing PaO2 and decreas-ing PaCO2, thus decreasing pulmonary vaso-constriction, it may significantly improve RV function, as we demonstrated.31 In other words, prone positioning reconciles the lung protective approach with the RV protective approach. We recently reported that such a strategy can be in-cluded in a routine protocol.38
Pplat must absolutely be decreased to a level <27 cmH2O, a safe limit for the right ventricle.7 The second goal is to evaluate the effect of increasing PEEP on lung recruitment and overdistension, but we lack tools to do this at the bedside. CT-scan is probably the most effective tool,37 but is currently unavailable in usual practice. However, when overdistension is predominant, RV func-tion is impaired,35 a warning signal the response to which must be to decrease PEEP. Studying RV function may therefore help intensivists to assess the balance between recruitment and overdisten-sion. Finally, as emphasized above, hypercapnia must be limited by reducing the instrumental dead space (heat and moisture exchanger re-placement by heated humidifier) and by increas-
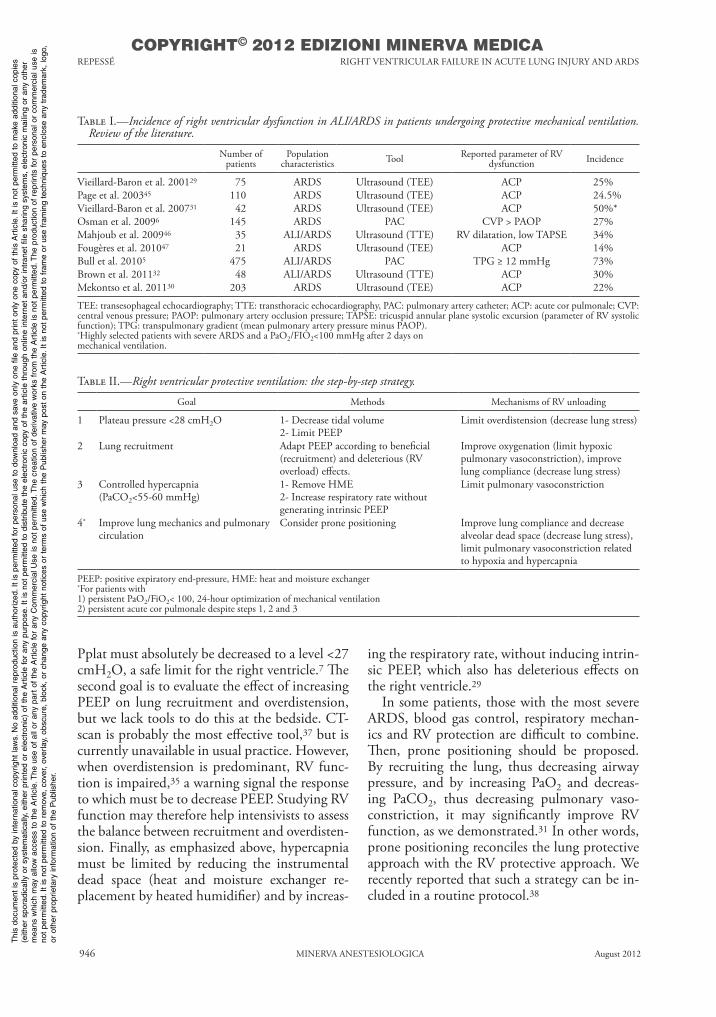
Table I.—Incidence of right ventricular dysfunction in ALI/ARDS in patients undergoing protective mechanical ventilation. Review of the literature.
Number of patients
Population characteristics Tool Reported parameter of RV
dysfunction Incidence
Vieillard-Baron et al. 200129 75 ARDS Ultrasound (TEE) ACP 25%Page et al. 200345 110 ARDS Ultrasound (TEE) ACP 24.5%Vieillard-Baron et al. 200731 42 ARDS Ultrasound (TEE) ACP 50%*Osman et al. 20096 145 ARDS PAC CVP > PAOP 27%Mahjoub et al. 200946 35 ALI/ARDS Ultrasound (TTE) RV dilatation, low TAPSE 34%Fougères et al. 201047 21 ARDS Ultrasound (TEE) ACP 14%Bull et al. 20105 475 ALI/ARDS PAC TPG ≥ 12 mmHg 73%Brown et al. 201132 48 ALI/ARDS Ultrasound (TTE) ACP 30%Mekontso et al. 201130 203 ARDS Ultrasound (TEE) ACP 22%
TEE: transesophageal echocardiography; TTE: transthoracic echocardiography, PAC: pulmonary artery catheter; ACP: acute cor pulmonale; CVP: central venous pressure; PAOP: pulmonary artery occlusion pressure; TAPSE: tricuspid annular plane systolic excursion (parameter of RV systolic function); TPG: transpulmonary gradient (mean pulmonary artery pressure minus PAOP).*Highly selected patients with severe ARDS and a PaO2/FIO2<100 mmHg after 2 days onmechanical ventilation.
Table II.—Right ventricular protective ventilation: the step-by-step strategy.
Goal Methods Mechanisms of RV unloading
1 Plateau pressure <28 cmH2O 1- Decrease tidal volume2- Limit PEEP
Limit overdistension (decrease lung stress)
2 Lung recruitment Adapt PEEP according to beneficial (recruitment) and deleterious (RV overload) effects.
Improve oxygenation (limit hypoxic pulmonary vasoconstriction), improve lung compliance (decrease lung stress)
3 Controlled hypercapnia(PaCO2<55-60 mmHg)
1- Remove HME2- Increase respiratory rate without generating intrinsic PEEP
Limit pulmonary vasoconstriction
4* Improve lung mechanics and pulmonary circulation
Consider prone positioning Improve lung compliance and decrease alveolar dead space (decrease lung stress), limit pulmonary vasoconstriction related to hypoxia and hypercapnia
PEEP: positive expiratory end-pressure, HME: heat and moisture exchanger*For patients with1) persistent PaO2/FiO2< 100, 24-hour optimization of mechanical ventilation2) persistent acute cor pulmonale despite steps 1, 2 and 3
COPYRIGHT© 2012 EDIZIONI MINERVA MEDICA
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

RIGHT VENTRICULAR FAILURE IN ACUTE LUNG INJURY AND ARDS REPESSÉ
Vol. 78 - No. 8 MINERVA ANESTESIOLOGICA 947
References
1. Brun-Buisson C, Minelli C, Bertolini G, Brazzi L, Pimen-tel J, Lewandowski K et al. Epidemiology and outcome of acute lung injury in European intensive care units. Results from the ALIVE study. Intensive Care Med 2004;30:51-61.
2. Phua J, Badia JR, Adhikari NK, Friedrich JO, Fowler RA, Singh JM et al. Has mortality from acute respiratory distress syndrome decreased over time?: A systematic review. Am J Respir Crit Care Med 2009;179:220-7.
3. Zapol WM, Kobayashi K, Snider MT, Greene R, Laver MB. Vascular obstruction causes pulmonary hypertension in severe acute respiratory failure. Chest 1977;71(2 Sup-pl):306-7.
4. Moloney ED, Evans TW. Pathophysiology and pharmaco-logical treatment of pulmonary hypertension in acute respi-ratory distress syndrome. Eur Respir J 2003;21:720-7.
5. Bull TM, Clark B, McFann K, Moss M. Pulmonary vas-cular dysfunction is associated with poor outcomes in pa-tients with acute lung injury. Am J Respir Crit Care Med 2010;182:1123-8.
6. Osman D, Monnet X, Castelain V, Anguel N, Warszawski J, Teboul JL et al. Incidence and prognostic value of right ventricular failure in acute respiratory distress syndrome. Intensive Care Med 2009;35:69-76.
7. Jardin F, Vieillard-Baron A. Is there a safe plateau pressure in ARDS? The right heart only knows. Intensive Care Med 2007;33:444-7.
8. Redington AN, Rigby ML, Shinebourne EA, Oldershaw PJ. Changes in the pressure-volume relation of the right ventricle when its loading conditions are modified. Br Heart J 1990;63:45-9.
9. Laks MM, Garner D, Swan HJ. Volumes and compliances measured simultaneously in the right and left ventricles of the dog. Circ Res 1967;20:565-9.
10. Guyton AC, Lindsey AW, Abernathy B, Richardson T. Ve-nous return at various right atrial pressures and the normal venous return curve. Am J Physiol 1957;189:609-15.
11. Whittenberger JL, Mc GM, Berglund E, Borst HG. Influ-ence of state of inflation of the lung on pulmonary vascular resistance. J Appl Physiol 1960;15:878-82.
12. Cournand A, Motley HL. Physiological studies of the ef-fects of intermittent positive pressure breathing on cardiac output in man. Am J Physiol 1948;152:162-74.
13. Vieillard-Baron A, Augarde R, Prin S, Page B, Beauchet A, Jardin F. Influence of superior vena caval zone condition on cyclic changes in right ventricular outflow during respira-tory support. Anesthesiology 2001;95:1083-8.
14. Michard F, Chemla D, Richard C, Wysocki M, Pinsky MR, Lecarpentier Y et al. Clinical use of respiratory changes in arterial pulse pressure to monitor the hemodynamic effects of PEEP. Am J Respir Crit Care Med 1999;159:935-9.
15. West JB, Dollery CT, Naimark A. Distribution of blood
Pharmacological approach to RV failure management
Hemodynamic management of shock-related ACP in ARDS relies on few drugs. Nitric oxide (NO) inhalation has been shown to improve RV systolic function in patients with ARDS,39 even though no effect on mortality was found.40 In our practice, we reserve it for persistent shock related to ACP despite optimization of respiratory settings. Norepinephrine has been recognized to be the elective drug for improv-ing RV performance by its ability to restore RV perfusion pressure.41, 42 It was confirmed in an experimental model of massive pulmonary em-bolism.42 However, no clinical study has been performed in ARDS. Finally, a calcium sensi-tizer (levosimendan) has been described as su-perior to dobutamine in isolated myocardial infarction-related right heart failure.43 In the context of ARDS, it was proposed by Morelli et al. for its ability to dilate the pulmonary circu-lation and to increase RV contractility.44
Conclusions
In ARDS, hemodynamic effects on the right ventricle in pulmonary vascular remodeling, combined with positive pressure ventilation, are well characterized. It is now established that pulmonary vascular dysfunction and RV systolic overload are strongly associated with poor prog-nosis. Many studies suggest that monitoring of RV function is mandatory to optimize hemo-dynamics but also, more interestingly, to opti-mize respiratory settings. Echocardiography, by a transthoracic or a transesophageal approach, may help intensivists to apply a RV protective approach, which should be prospectively evalu-ated in the future in a large prospective study. In this strategy, prone positioning has a key role in the most seriously ill patients.
— Respiratory settings significantly im-pact its occurrence.
— ACP is clearly associated with poor prognosis.
— A right ventricular protective approach can be proposed, based on strict limitation of plateau pressure, limitation of PEEP, control of hypercapnia, and finally on prone position in the most severely ill patients.
Key messages
— Incidence of ACP is high in ARDS patients submitted to protective ventilation: 25%.
COPYRIGHT© 2012 EDIZIONI MINERVA MEDICA
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.
REPESSÉ RIGHT VENTRICULAR FAILURE IN ACUTE LUNG INJURY AND ARDS
948 MINERVA ANESTESIOLOGICA August 2012
witz B, Hirshberg E et al. Right and left heart failure in severe H1N1 influenza A infection. Eur Respir J 2011;37:112-8.
33. Vieillard-Baron A, Loubieres Y, Schmitt JM, Page B, Du-bourg O, Jardin F. Cyclic changes in right ventricular output impedance during mechanical ventilation. J Appl Physiol 1999;87:1644-50.
34. Jardin F, Brun-Ney D, Cazaux P, Dubourg O, Hardy A, Bourdarias JP. Relation between transpulmonary pressure and right ventricular isovolumetric pressure change during respiratory support. Cathet Cardiovasc Diagn 1989;16:215-20.
35. Mekontso Dessap A, Charron C, Devaquet J, Aboab J, Jar-din F, Brochard L et al. Impact of acute hypercapnia and augmented positive end-expiratory pressure on right ven-tricle function in severe acute respiratory distress syndrome. Intensive Care Med 2009;35:1850-8.
36. Viitanen A, Salmenpera M, Heinonen J. Right ventricular response to hypercarbia after cardiac surgery. Anesthesiol-ogy 1990;73:393-400.
37. Gattinoni L, Caironi P, Cressoni M, Chiumello D, Ranieri VM, Quintel M, et al. Lung recruitment in patients with the acute respiratory distress syndrome. N Engl J Med 2006;354:1775-86.
38. Charron C, Bouferrache K, Caille V, Castro S, Aegerter P, Page B, et al. Routine prone positioning in patients with severe ARDS: feasibility and impact on prognosis. Intensive Care Med 2011;37:785-90.
39. Bhorade S, Christenson J, O’Connor M, Lavoie A, Pohl-man A, Hall JB. Response to inhaled nitric oxide in patients with acute right heart syndrome. Am J Respir Crit Care Med 1999;159:571-9.
40. Adhikari NK, Burns KE, Friedrich JO, Granton JT, Cook DJ, Meade MO. Effect of nitric oxide on oxygenation and mortality in acute lung injury: systematic review and meta-analysis. British Medical J 2007;334:779.
41. Cross CE. Right ventricular pressure and coronary flow. Am J Physiol 1962;202:12-6.
42. Hirsch LJ, Rooney MW, Wat SS, Kleinmann B, Mathru M. Norepinephrine and phenylephrine effects on right ventric-ular function in experimental canine pulmonary embolism. Chest 1991;100:796-801.
43. Russ MA, Prondzinsky R, Carter JM, Schlitt A, Ebelt H, Schmidt H, et al. Right ventricular function in myocardial infarction complicated by cardiogenic shock: Improvement with levosimendan. Crit Care Med 2009;37:3017-23.
44. Morelli A, Teboul JL, Maggiore SM, Vieillard-Baron A, Rocco M, Conti G, et al. Effects of levosimendan on right ventricular afterload in patients with acute respiratory dis-tress syndrome: a pilot study. Crit Care Med 2006;34:2287-93.
45. Page B, Vieillard-Baron A, Beauchet A, Aegerter P, Prin S, Jardin F. Low stretch ventilation strategy in acute respira-tory distress syndrome: eight years of clinical experience in a single center. Crit Care Med 2003;31:765-9.
46. Mahjoub Y, Pila C, Friggeri A, Zogheib E, Lobjoie E, Tin-turier F et al. Assessing fluid responsiveness in critically ill patients: False-positive pulse pressure variation is detected by Doppler echocardiographic evaluation of the right ven-tricle. Crit Care Med 2009;37:2570-5.
47. Fougères E, Teboul JL, Richard C, Osman D, Chemla D, Monnet X. Hemodynamic impact of a positive end-expiratory pressure setting in acute respiratory distress syn-drome: importance of the volume status. Crit Care Med 2010;38:802-7.
flow in isolated lung; relation to vascular and alveolar pres-sures. J Appl Physiol 1964;19:713-24.
16. Testa A. Delle malattie del cuore. Milano: Google eBook; 1831.
17. Kopman EA, Ferguson TB. Interaction of right and left ventricular filling pressures at the termination of cardio-pulmonary bypass. Central venous pressure/pulmonary capillary wedge pressure ratio. J Thorac Cardiovasc Surg 1985;89:706-8.
18. Lopez-Sendon J, Coma-Canella I, Gamallo C. Sensitivity and specificity of hemodynamic criteria in the diagnosis of acute right ventricular infarction. Circulation 1981;64:515-25.
19. Monchi M, Bellenfant F, Cariou A, Joly LM, Thebert D, Laurent I et al. Early predictive factors of survival in the acute respiratory distress syndrome. A multivariate analysis. Am J Respir Crit Care Med 1998;158:1076-81.
20. Jardin F, Gueret P, Dubourg O, Farcot JC, Margairaz A, Bourdarias JP. Right ventricular volumes by thermodilution in the adult respiratory distress syndrome. A comparative study using two-dimensional echocardiography as a refer-ence method. Chest 1985;88:34-9.
21. De Monte A, Baigorri F, Bertolissi M, Artigas A. [The thermodilution determination of right ventricular volumes and ejection fraction in the critical patient. Volumetric vs pressure measurement assessment]. Minerva Anestesiol 1993;59:287-96.
22. Marland AM, Glauser FL. Significance of the pulmonary artery diastolic-pulmonary wedge pressure gradient in sep-sis. Crit Care Med 1982;10:658-61.
23. Jardin F, Dubourg O, Bourdarias JP. Echocardiographic pattern of acute cor pulmonale. Chest 1997;111:209-17.
24. Vieillard-Baron A, Prin S, Chergui K, Dubourg O, Jardin F. Echo-Doppler demonstration of acute cor pulmonale at the bedside in the medical intensive care unit. Am J Respir Crit Care Med 2002;166:1310-9.
25. Brinker JA, Weiss JL, Lappe DL, Rabson JL, Summer WR, Permutt S et al. Leftward septal displacement during right ventricular loading in man. Circulation 1980;61:626-33.
26. Jardin F, Farcot JC, Boisante L, Curien N, Margairaz A, Bourdarias JP. Influence of positive end-expiratory pres-sure on left ventricular performance. N Engl J Med 1981;304:387-92.
27. Ryan T, Petrovic O, Dillon JC, Feigenbaum H, Conley MJ, Armstrong WF. Apical systolic eccentricity index: a better marker of right ventricular compromise in pulmonary hy-pertension. Echocardiography 2010;27:534-8.
28. Jardin F, Gueret P, Dubourg O, Farcot JC, Margairaz A, Bourdarias JP. Two-dimensional echocardiographic evalua-tion of right ventricular size and contractility in acute respi-ratory failure. Crit Care Med 1985;13:952-6.
29. Vieillard-Baron A, Schmitt JM, Augarde R, Fellahi JL, Prin S, Page B et al. Acute cor pulmonale in acute respiratory distress syndrome submitted to protective ventilation: inci-dence, clinical implications, and prognosis. Crit Care Med 2001;29:1551-5.
30. Mekontso-Dessap A, Boissier F, Leon R, Carreira S, Campo FR, Lemaire F et al. Prevalence and prognosis of shunting across patent foramen ovale during acute respiratory distress syndrome. Crit Care Med 2010;38:1786-92.
31. Vieillard-Baron A, Charron C, Caille V, Belliard G, Page B, Jardin F. Prone positioning unloads the right ventricle in severe ARDS. Chest 2007;132:1440-6.
32. Brown SM, Pittman J, Miller Iii RR, Horton KD, Marke-
Funding.—Support was provided solely from institutional and/or departmental sources.Received on April 18, 2012 - Accepted for publication on June 1, 2012.Corresponding author: Prof. A. Vieillard-Baron, Intensive Care Unit, Section Thorax-Vascular Disease-Abdomen-Metabolism, University Hospital Ambroise Paré, 9, avenue Charles-de-Gaulle 92100 Boulogne-Billancourt, France. E-mail: [email protected] article is freely available at www.minervamedica.it
COPYRIGHT© 2012 EDIZIONI MINERVA MEDICA
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.