
arrhythmogenic right ventricular dysplasia/Cardiomyopathy
32
+ Ambulatory: Case based study LT. S.T. Anthony Kaviratne MD 28 January 2015
-
Upload
anthony-kaviratne -
Category
Health & Medicine
-
view
168 -
download
0
Transcript of arrhythmogenic right ventricular dysplasia/Cardiomyopathy

+
Ambulatory: Case based study
LT. S.T. Anthony Kaviratne MD
28 January 2015

+Case presentation
19 year old female nonsmoker with no significant past medical
history presented today to discuss the sudden death of her sister.
The patient’s sister passes away suddenly at the age of 21.
Subsequent autopsy showed fatty infiltration of the right
ventricular wall consistent with ARVD.
The patient wish to discuss the implication of this diagnosis on
her and her family.

+ Arrhythmogenic right ventricular
cardiomyopathy/dysplasia
Identify what ARVD is in order to raise clinical suspicion
Basic of Pathology and natural clinical course
Be aware of diagnosis using 2010 revised task force criteria
Components of Treatment
Who to screen, screening interval and what tests consider
Objectives

+ Arrhythmogenic right ventricular
cardiomyopathy
What is it?
ARVC is a genetic form of cardiomyopathy that primarily affects the
right ventricle (RV)but can involve the LV with relative sparring of the
septum
ARVC is characterized macroscopically by fibrofatty replacement of
the right ventricle (RV) myocardium, which initially produces regional
wall motion abnormalities that later become global, producing RV
dilation
Culminates in life-threatening ventricular arrhythmias, prompting
sudden cardiac death (SCD) and/or biventricular heart failure
The prevalence in the general population is estimated to be 1:1000 to
1:2000
Male : Female = 1:3

+ARVD
Autosomal dominant encode desmosomal proteins
(plakoglobin, desmoplakin, plakophilin-2, desmoglein, and
desmocollin.
Autosomal recessive autosomal dominant disease and
plakoglobin and desmoplakin disease
Impaired desmosome function when subjected to
mechanical stress causes myocyte detachment and cell
death
Autosomal dominance most common with a variable
penetrance ranging from 20%-35%
Mutations render desmosomes inappropriately sensitive to mechanical stresses, resulting in myocyte death
Reprogrammed myocyte cell biology so that these cells adopt a fibrofatty lineage
Pathology


+ARVDNatural History
ARVC is a genetic form of cardiomyopathy that primarily affects
the right ventricle (RV)but can involve the LV
Natural history characterized by four phases:
Concealed phase (asymptomatic, but at risk of SCD)
Overt clinical expression of an electrical system disturbance
Signs and symptoms of right ventricular failure
Frank biventricular congestive heart failure
ARVD is an important cause of sudden cardiac death in young
adults, accounting for 11% of all cases and 22% of cases
among athletes.
The prognosis is worse in patients with LV involvement
Annual mortality rate of 2.3% (Fontain et al)

+ARVD
The diagnosis of ARVC should be considered in a variety of clinical
situations:
Patients who present with symptomatic or asymptomatic VT of LBBB configuration in
the absence of apparent heart disease
Patients with multiple QRS morphologies when VT is induced during electrophysiology
testing
Survivors of SCD, particularly SCD occurring during exercise
Presenting symptoms varies
syncope (26%-32%)
Palpitations (26%-67%)
sudden cardiac death (10%-26%)
Atypical chest pain (27%)
Dyspnea (11%)
heart failure - occurs in a minority, but is the predominant mode of death in those protected from SCD by an ICD
ARVC accounts for 20% of cases of sudden cardiac death (among young athletes dying suddenly, the prevalence is higher)
Clinical Presentation

+ARVDDiagnosis
Definite diagnosis of ARVC using the 2010 revised Task Force
criteria requires the presence of:
Two major criteria OR
One major and two minor criteria OR
Four minor criteria from different categories
Borderline diagnosis of ARVC using the 2010 revised Task
Force criteria requires the presence of:
One major and one minor criteria OR
Three minor criteria from different categories
Possible diagnosis of ARVC using the 2010 revised Task
Force criteria requires the presence of:
One major criteria OR
Two minor criteria from different categories



+ECHO FEATURES OF ARVC
Dilated RV

+ECHO FEATURES OF ARVCFocal RV apical aneurysm
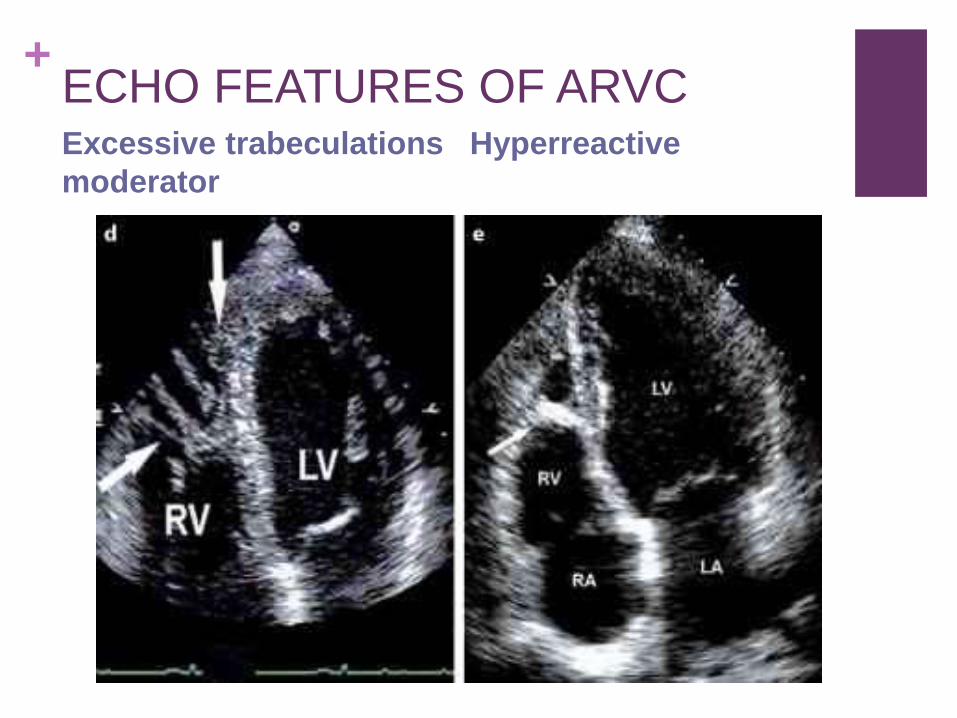
+ECHO FEATURES OF ARVCExcessive trabeculations Hyperreactive
moderator
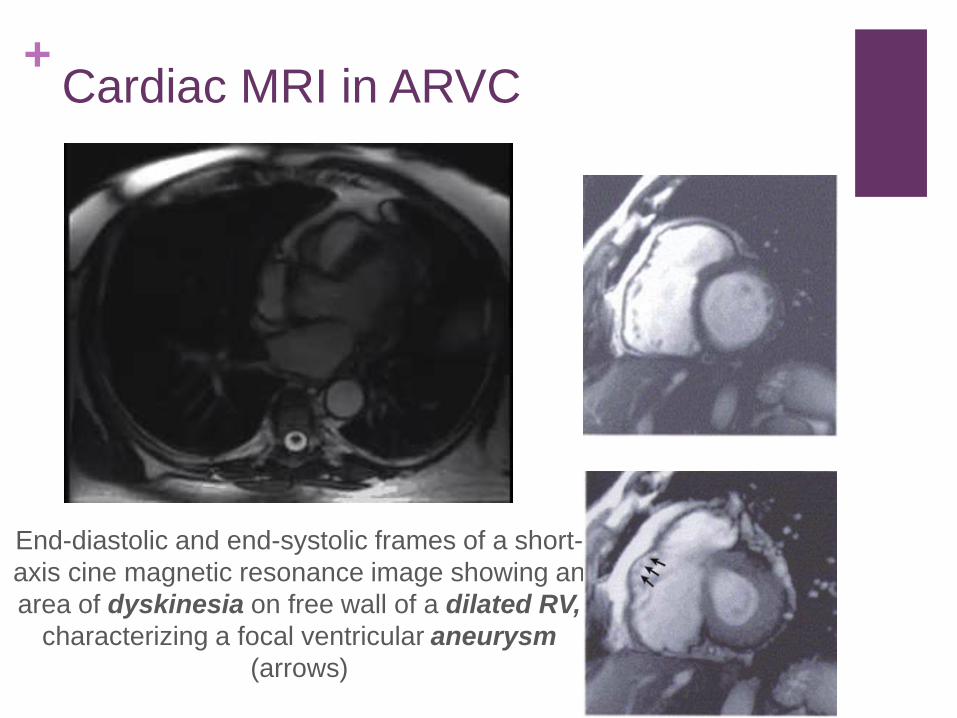
+Cardiac MRI in ARVC
End-diastolic and end-systolic frames of a short-
axis cine magnetic resonance image showing an
area of dyskinesia on free wall of a dilated RV,
characterizing a focal ventricular aneurysm
(arrows)

+Cardiac MRI in ARVCFatty infiltration
Axial T1-weighted black
blood spin-echo
cardiovascular MRI
showing extensive
transmural fatty
replacement of the RV
myocardium (arrow)

+Cardiac MRI in ARVCLate GAD enhancement indicating focal fibrosis



Copyright © American Heart Association
Endomyocardial biopsy findings in a proband affected by a diffuse form of
ARVC/D. All 3 biopsy samples are from different regions of the RV free wall.
There is extensive fibrofatty tissue replacement with myocardial atrophy, which
is a major criterion (ie, residual myocytes <60% by morphometric analysis or
<50% if estimated).
Contributed by C. Basso, Padua, Italy.

+ARVDEKG features
The ECG shows a RBBB pattern. with an epsilon wave
(arrow) in leads V1–V3. Reproducible low-amplitude
signals between end of QRS complex to onset of the T
wave
T-wave inversion in V1 through V4 and prolongation of the terminal activation duration ≥55 ms measured from the nadir of the S wave to the end of the QRS complex in V1.


+ARVDTherapy
Activity restriction: No competitive sports
Conservative measure: Betablocker therapy
Antiarrhythmic agents:
Radiofrequency ablation,
ICD therapy
HF treatment
Surgical treatment

+Antiarrhythmic agents
Reduce the frequency and suppress inducibility of sustained and nonsustained ventricular arrhythmias
The effects are difficult to assess:
small series of patients.
limited time to follow-up.
006 ACC/AHA/ESC guidelines for the management of ventricular arrhythmias and sudden cardiac death suggested that sotalol or amiodarone
Wichter et al: sotalol was more effective than BBs or amiodarone both in inducible and noninducible VT.
It is not known whether sotalol is able to prevent SD, even in patients tested by programmed electrical stimulation.
+ARVC in ICD
Recommend ICD implantation for secondary prevention in all patients of ARVD/C with prior sustained VT or ventricular fibrillation
ICD implantation is reasonable for the prevention of SCD in patients with ARVD/C who have 1 or more risk factors for SCD
Induction of VT during electrophysiological testing,
Detection of nonsustained VT on noninvasive monitoring
Male gender
Severe RV dilation, and extensive RV involvement
Young age at presentation (less than 5 years),
LV involvement,
Prior cardiac arrest, and unexplained syncope serve as markers of risk
Patients with genotypes of ARVD/C associated with a high risk for SCD should be considered for ICD therapy
2008 Guidelines (No changes in 2012)

+Role Catheter ablation
Radiofrequency ablation has proven largely palliative due to patchy and progressive nature of the disease
RFA currently reserved for patients who experience frequent ventricular arrhythmias (and ICD shocks) despite optimal therapy with both ICDs and antiarrhythmic medication
Role of RFA may continue to increase in the future, as mapping techniques (CARTO) continue to evolve

+HF treatment
When the disease has progressed to RV or biventricular failure,
treatment consists of the current therapy for HF, including
diuretics, BBs, ACEIs and anticoagulants.
In case of intractable RV failure, cardiac transplantation may be
the only remaining alternative.

+Surgical treatment
More than 20 years ago, surgical treatment was
introduced, initially consisting of right ventriculotomy.
Total disconnection of the right free wall then was tried.
This approach was abandoned because of
The risk of developing RV failure,
The increased availability of cardiac transplantation,
The improvement in the technology of ICD.
Occasionally, disconnection surgery or RV
cardiomyoplasty is a useful therapeutic option
Transplant: When all else fails

+ARVD
All of their first-degree relatives of that person
need to be screened. Incomplete penetrance
noted
Screening interval of 2-5 year (most 2-3y)
Suggested screening tools
Standard 12 lead ECG
Signal averaged ECG with 40mHz filter
Holter monitor for 24 hours
Echocardiogram
Exercise stress test
Cardiac MRI
Identification of pathogenic mutations in
affected patients with cascade screening of
relatives
Screening of asymptomatic relatives
Time to Disease Progression Among 37 Subjects
With Complete Re-Evaluation
Anneline et al. JACC. 2014 Jul 22
+Diagnosis of Familial ARVC
In the context of proven ARVC/D in a first-degree relative, the diagnosis of familial ARVC/D is based on the documentation of one of the following in a family member:
T-wave inversion V1, V2, and V3 in individuals ≥ 14 years
Late potentials by signal-averaged ECG (SAECG).
Ventricular tachycardia of LBBB morphology on ECG, Holter, or during exercise testing or >200 PVCs in 24 hours
Either mild global dilatation or reduction in RV ejection fraction with normal LV or mild segmental dilatation of the RV or regional RV hypokinesis.

+
QUESTIONS?

+SUMMERY
Disorder of unknown course that is characterized pathologically by fibrofatty
replacement of the RV myocardium and electrical instability
High suspicion is needed when family member SCD, syncope, abnormal RV,
or EKG findings (epsilon wave, delayed potentials)
Diagnosis needs a combination imaging (echo and MRI), tissue biopsy, EKG
findings (repol and depol abnormalities), arrhythmia, or FH
Treatment includes antiarrhythmic therapy, HF therapy, early ICD.
Screen in stepwise fashion all fist degree relatives.
Don’t forget to restrict activity not only in proband but at risk family members
Role of genetic screening is helpful but incompletely understood


















