Richard Y. Ha, MD Matthew J. Trovato, MDpustaka.kk.usm.my/pustaka2/inhouse/e-journal/SRPS/11-R3...
52
Volume 11 • Issue R3 Reconstructive PLASTIC SURGERY OF THE EAR Richard Y. Ha, MD Matthew J. Trovato, MD
Transcript of Richard Y. Ha, MD Matthew J. Trovato, MDpustaka.kk.usm.my/pustaka2/inhouse/e-journal/SRPS/11-R3...

Volume 11 • Issue R3
Reconstructive
PLASTIC SURGERY OF THE EAR
Richard Y. Ha, MDMatthew J. Trovato, MD

OUR EDUCATIONAL PARTNERS Selected Readings in Plastic Surgery appreciates the generoussupport provided by our educational partners.
facial aesthetics

OUR EDUCATIONAL PARTNERS Selected Readings in Plastic Surgery appreciates the generoussupport provided by our educational partners.
facial aesthetics
R. S. Ambay, MDR. G. Anderson, MDS. J. Beran, MDS. M. Bidic, MDG. Broughton II, MD, PhDJ. L. Burns, MDJ. J. Cheng, MDC. P. Clark III, MDD. L. Gonyon, Jr, MDA. A. Gosman, MDK. A. Gutowski, MDJ. R. Gri�n, MDR. Y. Ha, MDF. Hackney, MD, DDSL. H. Hollier, MDR. E. Hoxworth, MDJ. E. Janis, MDR. K. Khosla, MDJ. E. Leedy, MDJ. A. Lemmon, MDA. H. Lipschitz, MDR. A. Meade, MDD. L. Mount, MDJ. C. O’Brien, MDJ. K. Potter, MD, DDSR. J. Rohrich, MDM. Saint-Cyr, MDM. Schaverien, MRCSM. C. Snyder, MDM. Swelstad, MDA. P. Trussler, MDR. I. S. Zbar, MD
Senior Manuscript Editor Dori Kelly
Contributing Editors
Editor Emeritus
Editor-in-Chief
Business Manager Becky Sheldon Corporate Sponsorship Barbara Williams
30 Topics
Grafts and FlapsWound Healing, Scars, and BurnsSkin Tumors: Basal Cell Carcinoma, Squamous Cell Carcinoma, and MelanomaImplantation and Local AnestheticsHead and Neck Tumors and ReconstructionMicrosurgery and Lower Extremity ReconstructionNasal and Eyelid ReconstructionLip, Cheek, and Scalp ReconstructionEar Reconstruction and OtoplastyFacial FracturesBlepharoplasty and Brow LiftRhinoplastyRhytidectomyInjectablesLasersFacial Nerve DisordersCleft Lip and Palate and Velopharyngeal Insu�ciencyCraniofacial I: Cephalometrics and Orthognathic SurgeryCraniofacial II: Syndromes and SurgeryVascular AnomaliesBreast AugmentationBreast Reduction and MastopexyBreast ReconstructionBody Contouring and LiposuctionTrunk ReconstructionHand: Soft TissuesHand: Peripheral NervesHand: Flexor TendonsHand: Extensor TendonsHand: Fractures and Dislocations, the Wrist, and Congenital Anomalies
Je�rey M. Kenkel, MD
F. E. Barton, Jr, MD
www.SRPS.org
Selected Readings in Plastic Surgery (ISSN 0739-5523) is a series of monographs published by Selected Readings in Plastic Surgery, Inc. For subscription information, please visit our web site: www.SRPS.org.

SRPS • Volume 11 • Issue R3 • 2011
1
ANATOMYSkeletonThe auricular cartilage framework consists of three tiers of delicately convoluted cartilage: the conchal complex, the antihelix-antitragus complex, and the helix-lobule complex (Fig. 1).
MusculatureThe vestigial intrinsic muscles of the external surface of the auricle are the helicis major and minor, tragicus, and antitragicus muscles. On the cranial surface are the intrinsic transverse and intrinsic oblique muscles. The extrinsic muscles of the ear include the anterior, superior, and posterior auricularis muscles.1
Circulatory SystemThe arterial supply of the auricle comes from the posterior auricular artery and from the superficial temporal artery. Park et al.2 described two separate networks: one in the triangular fossa and scapha and one to the concha. The anterior auricular surface of the ear is dominantly supplied by perforators from the posterior auricular artery. The posterior auricular artery has perforators piercing the ear from its medial surface at the triangular fossa, cymba, concha, cavum conchae, helical root, and earlobe. Only one small branch of the superficial temporal artery crosses the helical rim superiorly and supplies the triangular fossa and scapha network (Fig. 2).2 Because of
PLASTIC SURGERY OF THE EAR
Richard Y. Ha, MD1
Matthew J. Trovato, MD2
1,2Dallas Plastic Surgery Institute and 1Department of Plastic Surgery, University of Texas Southwestern Medical Center at Dallas, Dallas, Texas
HelixSuperior crus
Scapha
Tuberculumauriculae
Triangularfossa
Inferiorcrus
Crushelicis
Incisuraanterior
Tuberculumsupertragicum
Tragus Antitragus
Lobule
Cavumconchae
Cymbaconchae
Antihelix
Incisuraintertragica
Helix
Cavumconchae
Crushelicis(root)
Superior crusantihelicis
Antihelix
Cymbaconchae
Caudahelicis
Spinahelicis
Laminatragi
Fossatriangularis
Fissuraantitragico-helicina
Superior crus
Helix
Antihelix
Eminentiacavum conchae
Eminentiacymba conchae
Transversesulcus(inferior crus)
Eminentia fossa triangularis
Eminentiascapha
Cauda helicis
Ponticulus
Figure 1. Anatomy of the external ear and landmarks for the auricular cartilage.

2
SRPS • Volume 11 • Issue R3 • 2011
interconnections between the two arterial networks, the ear would be well vascularized by either arterial system alone.3
A thorough knowledge of the arterial perforators of the auricle is essential for designing local chondrocutaneous flaps. Venous drainage is via the posterior auricular veins into the external jugular system and the superficial temporal and retromandibular veins.
InnervationThe ear is innervated by the great auricular nerve (C2–C3), the auriculotemporal nerve (V3), the lesser occipital nerve, and the auricular branch of the vagus nerve (Arnold nerve) (Fig. 3).4
Lymphatic DrainageThe lymphatic drainage of the external ear correlates with its embryological development. The concha and meatus drain to the parotid and infraclavicular nodes, and the external canal and cranial surface of the auricle drain to the mastoid and infra-auricular cervical nodes (Fig. 4).4
EMBRYOLOGYThe auricle arises from the first (mandibular) and second (hyoid) branchial arches. Hillocks appear on these arches during the 6th week of gestation. The anterior hillocks (on the first branchial arch) give rise to the tragus, root of the helix, and superior helix. The posterior hillocks (on the second branchial arch) contribute to the antihelix, antitragus, and lobule (Fig. 5).5,6
Lesser occipital n.
Mastoid branchof lesser ocipital n.
Greater auricular n.
Lesser occipital n.
Mastoid branchof lesser ocipital n.
Greater auricular n.
Auriculo-temporal n.
A
BFigure 3. Sensory nerve supply of the external ear. n., nerve. (Modified from Brent.4)
I II
1
2
34
5
6
Parotidlymph nodes
Cervicallymph nodes
Figure 4. Lymphatic drainage of the external ear. I, first branchial arch; II, second branchial arch; numbers 1 through 6, gestational weeks 1 through 6.
A B
III
III
11
2
2
3
3
4
45
5
6
6
Figure 5. Embryological origin of the external ear. I, first branchial arch; II, second branchial arch; numbers 1 through 6, gestational weeks 1 through 6.
Figure 2. Perforating sites of the posterior auricular artery. Left, Anterior surface. Right, Posterior surface. Tr, triangular fossa; CyC, cymba conchae; HR, helical root; CaC, cavum conchae; Lb, earlobe. (Reprinted with permission from Park et al.2)

SRPS • Volume 11 • Issue R3 • 2011
3
AESTHETIC RELATIONSHIPSLeonardo da Vinci noted that the vertical height of the ear in adults was approximately equal to the distance between the lateral orbital rim and the root of the helix at the level of the brow. The ear width is approximately 55% of its length. The helical rim protrudes 1 to 2 cm from the skull,7 and the angle of protrusion averages 21 to 25 degrees.8 The long axis of the ear is tilted posteriorly at an angle of 20 degrees from vertical (range, 2−30 degrees). The angle between the axis of the ear and the bridge of the nose is approximately 15 degrees; in other words, the ear axis does not parallel the bridge of the nose in most normal adults.9
Broadbent and Mathews10 and Tolleth11 reviewed the artistic relationships of the ear to the surface anatomy of the face. Asymmetries of the ear usually are the rule and not the exception. Farkas8 reported that approximately 50% of people exhibit at least a 3-mm discrepancy in the horizontal and vertical positions of the ear. Ear projection (defined by cephaloauricular angle) varies up to 5 degrees in 25% of people.12
Sullivan and colleagues (Brucker et al.13) showed, in a morphometric study of the external ear, differences between men and women and changes in morphology over time. As expected, relative to head size, the vertical height of the pinna was 6.5% larger in men. However, the lobular height and width was relatively similar in both sexes. With advanced age, only the lobule exhibited significant changes with width decreasing and length increasing, consistent with the accepted concept of lobular “ptosis.”
HISTORY OF EAR RECONSTRUCTIONConverse14 provided a detailed account of the early history of ear reconstruction. According to Converse, The Susruta, an Indian text of ancient medicine, noted a 900 bce case of partial reconstruction of the earlobe with a cheek flap. In 1597, Tagliacozzi of Italy transferred a flap from the arm to reconstruct the auricle of a monk. Approximately 250 years later, Dieffenbach repaired a traumatic defect of the ear with a mastoid flap folded on itself. Converse14 explained that Roux and many
of his contemporaries of the mid-19th century considered reconstruction of the auricle a surgical impossibility, but by 1930, Pierce had reported posttraumatic repairs that used autologous rib cartilage for reconstruction of the concha-antihelix and a thin roll of supraclavicular skin for helical reconstruction. Later, Peer placed diced autologous costal cartilage in a mold that was implanted in a subcutaneous abdominal pocket. When fusion of the fragments by connective tissue was complete, the framework was used in auricular reconstruction. During the 1940s, ear reconstruction with fresh and preserved cartilage homografts and heterografts was reported. The results were uniformly dismal, characterized by late resorption and high complication rates. The modern era of auricular reconstruction began with classic descriptions of the principles and technique of total ear reconstruction with autologous costal cartilage, as presented by Tanzer.15,16
ACQUIRED DEFORMITIESPrinciples of Acute ManagementThe principles of management of acutely traumatized ears can be summarized as follows:
• Thorough cleansing, minimal débridement, and skin suturing only after cleansing
• Begin at known structures and progress to unknown
• Close the skin in delayed reconstruction• Repair primarily after wedge excision
of the wound if the defect is small and peripheral
• Leave the wound open and reconstruct at a later date
• When immediate closure is not feasible, cleanse the wound and change dressings frequently to avoid desiccation
• Graft skin defects only where underlying perichondrium is present
• Reattach small avulsed ear pieces as compromised grafts, especially in children

4
SRPS • Volume 11 • Issue R3 • 2011
Avulsion with Exposed CartilageAvulsion injuries with partial-thickness loss of ear substance are managed acutely to ensure swift coverage of any exposed cartilage. When the avulsion is superficial and the perichondrium intact, a split-thickness skin graft from the postauricular skin is a good color match and an acceptable treatment. When no perichondrium is present and the avulsion has left a small peripheral area of exposed cartilage, wedge excision might correct the problem. Other methods to cover exposed ear cartilage are preauricular flaps17 and postauricular flaps, which can be tunneled through the ear to cover exposed areas in the concha bow and the external auditory meatus.18 Even a thick flap can be used to provide substantial cover for exposed cartilage, as long as it is transferred according to the cran principle presented by Millard,19 and skin grafting is then performed. Another option when posterior skin is intact is to excise the exposed cartilage and graft the raw surface with the posterior skin. This method, however, produces a less-than-desirable aesthetic result.17 If immediate surgical treatment is not possible, frequent dressing changes are indicated to keep the cartilage viable until the wound granulates or appropriate delayed closure can be planned.17
Composite DefectsRepair of an acquired ear deformity requires both accurate analysis of the defect and a systematic approach to the reconstruction.20 Traumatic auricular injuries can present acutely or as secondary deformities after initial treatment by débridement and direct approximation. Small composite defects usually are repaired by means of a reduction procedure or skin-cartilage graft. Reduction methods include the Antia-Buch procedure21 and other techniques that resect a portion of the ear in such a way that the edges of the wound are brought together for closure. Brent20 discussed the various sources of cartilage for partial ear reconstruction. Unlike congenital malformations, acquired deformities usually do not require costal cartilage for structural support of a total-ear framework. Cartilage from the same or opposite ear generally is suitable for
the reconstruction and probably warps less and resists trauma better than does rib cartilage. A likely donor source is the concha of either ear combined with a local skin flap or used as a chondrocutaneous composite graft. Gorney et al.22 described various methods of harvesting contralateral conchal cartilage for ear reconstruction of posttraumatic defects. Patients with large defects requiring near-total ear reconstruction are candidates for costal cartilage grafting, such as that used for microtia, covered with a temporoparietal flap. One of the most difficult decisions is how to manage moderate-size defects involving one-fourth to one-half of the ear. Reconstructive options include tubed flaps from the neck, parieto temporalis fascial pedicled flaps, and postauricular mastoid skin flaps. The last is recommended because the mastoid skin is thin and a good color match for the anterior auricular surface.23
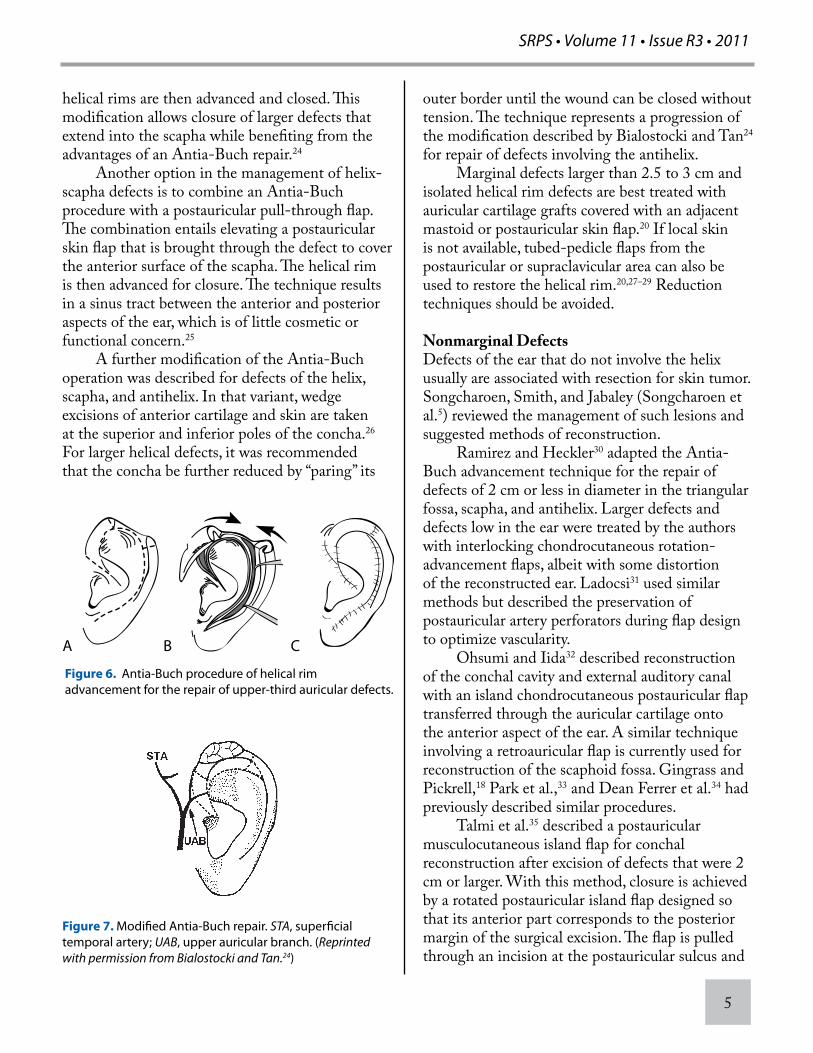
Marginal DefectsDefects of the upper and middle third of the helix are readily repaired with the chondrocutaneous advancement flap of Antia and Buch21 (Fig. 6). The single-stage procedure frees the helix from the scapha via an incision in the helical sulcus extending through the anterior skin and cartilage. The posteromedial skin superficial to the perichondrium is undermined, and the helix is advanced as a chondrocutaneous component based on a posterior skin flap. For small to moderate-sized defects, only the caudal segment needs to be advanced. Larger defects of the helix require mobilization of both the inferior and the superior portions. The cephalic segment is elevated on a preauricular skin flap and rotated backward into the defect in a V-to-Y fashion. If this reconstruction of a large defect causes the ear to be smaller in size than the normal ear, correction can be achieved by performing a wedge excision of the normal ear and setback of the prominent ear.21
When the defect extends into the hollow of the scapha, the Antia-Buch procedure can be combined with crescent-shaped chondrocutaneous excisions on either side of the defect, preserving posterior perichondrium and skin (Fig. 7).24 The
SRPS • Volume 11 • Issue R3 • 2011
5
helical rims are then advanced and closed. This modification allows closure of larger defects that extend into the scapha while benefiting from the advantages of an Antia-Buch repair.24
Another option in the management of helix-scapha defects is to combine an Antia-Buch procedure with a postauricular pull-through flap. The combination entails elevating a postauricular skin flap that is brought through the defect to cover the anterior surface of the scapha. The helical rim is then advanced for closure. The technique results in a sinus tract between the anterior and posterior aspects of the ear, which is of little cosmetic or functional concern.25
A further modification of the Antia-Buch operation was described for defects of the helix, scapha, and antihelix. In that variant, wedge excisions of anterior cartilage and skin are taken at the superior and inferior poles of the concha.26 For larger helical defects, it was recommended that the concha be further reduced by “paring” its
outer border until the wound can be closed without tension. The technique represents a progression of the modification described by Bialostocki and Tan24 for repair of defects involving the antihelix. Marginal defects larger than 2.5 to 3 cm and isolated helical rim defects are best treated with auricular cartilage grafts covered with an adjacent mastoid or postauricular skin flap.20 If local skin is not available, tubed-pedicle flaps from the postauricular or supraclavicular area can also be used to restore the helical rim.20,27–29 Reduction techniques should be avoided.
Nonmarginal DefectsDefects of the ear that do not involve the helix usually are associated with resection for skin tumor. Songcharoen, Smith, and Jabaley (Songcharoen et al.5) reviewed the management of such lesions and suggested methods of reconstruction. Ramirez and Heckler30 adapted the Antia-Buch advancement technique for the repair of defects of 2 cm or less in diameter in the triangular fossa, scapha, and antihelix. Larger defects and defects low in the ear were treated by the authors with interlocking chondrocutaneous rotation-advancement flaps, albeit with some distortion of the reconstructed ear. Ladocsi31 used similar methods but described the preservation of postauricular artery perforators during flap design to optimize vascularity. Ohsumi and Iida32 described reconstruction of the conchal cavity and external auditory canal with an island chondrocutaneous postauricular flap transferred through the auricular cartilage onto the anterior aspect of the ear. A similar technique involving a retroauricular flap is currently used for reconstruction of the scaphoid fossa. Gingrass and Pickrell,18 Park et al.,33 and Dean Ferrer et al.34 had previously described similar procedures. Talmi et al.35 described a postauricular musculocutaneous island flap for conchal reconstruction after excision of defects that were 2 cm or larger. With this method, closure is achieved by a rotated postauricular island flap designed so that its anterior part corresponds to the posterior margin of the surgical excision. The flap is pulled through an incision at the postauricular sulcus and
A B C
Figure 6. Antia-Buch procedure of helical rim advancement for the repair of upper-third auricular defects.
Figure 7. Modified Antia-Buch repair. STA, superficial temporal artery; UAB, upper auricular branch. (Reprinted with permission from Bialostocki and Tan.24)

6
SRPS • Volume 11 • Issue R3 • 2011
rotated 180 degrees on its long axis to drape the conchal bowl and antihelix.
Upper-Third DefectsBrent20 described several options for reconstruction of upper-third defects. The specific technique chosen in each case depends on the size of the defect and how much local skin remains for the reconstruction. For small helical rim defects, the Antia-Buch chondrocutaneous advancement flaps are adequate. Larger defects requiring cartilaginous support are best repaired with preauricular banner flaps combined with auricular cartilage grafts at the helical rim, as described by Crikelair.36 In the event of major defects of the upper third of the ear, the reconstructive options depend on whether sufficient skin is available for a local flap (e.g., a contralateral cartilage graft covered with a postauricular skin flap). If not enough skin is available adjacent to the defect to cover the graft, a compound pedicle flap is reliable for reconstruction (Fig. 8).37,38
First StageA compound flap is outlined containing the whole concha and carrying the external-anterior skin, cartilage, and retroauricular skin. The pedicle of the flap is situated on the outer border of the helix and must be 1 cm wide. The pedicle is composed of the skin of the external edge and of the anterior and posterior aspects of the helix and the scapha. The cartilage is cut inside the pedicle, to allow easier
rotation of the flap. Being an area rich in blood supply, no circulatory impairment of the mobilized flap is observed. The compound flap is rotated from its place in the concha to the place to be reconstructed. The two cutaneous layers are sutured with nylon, and the fibrocartilage does not need to be sutured. At the donor site in the concha, a raw area situated on the external aspect of the head remains. The raw area is next covered with a free skin graft.
Second StageThe helix is corrected first, by suitable adjustment of the pedicle. The lobule is then pulled downward, to make the auricle the same length as the opposite normal side. An incision is made along the edge of the lobule, cutting the cartilage and allowing the lobule to descend the necessary degree.37
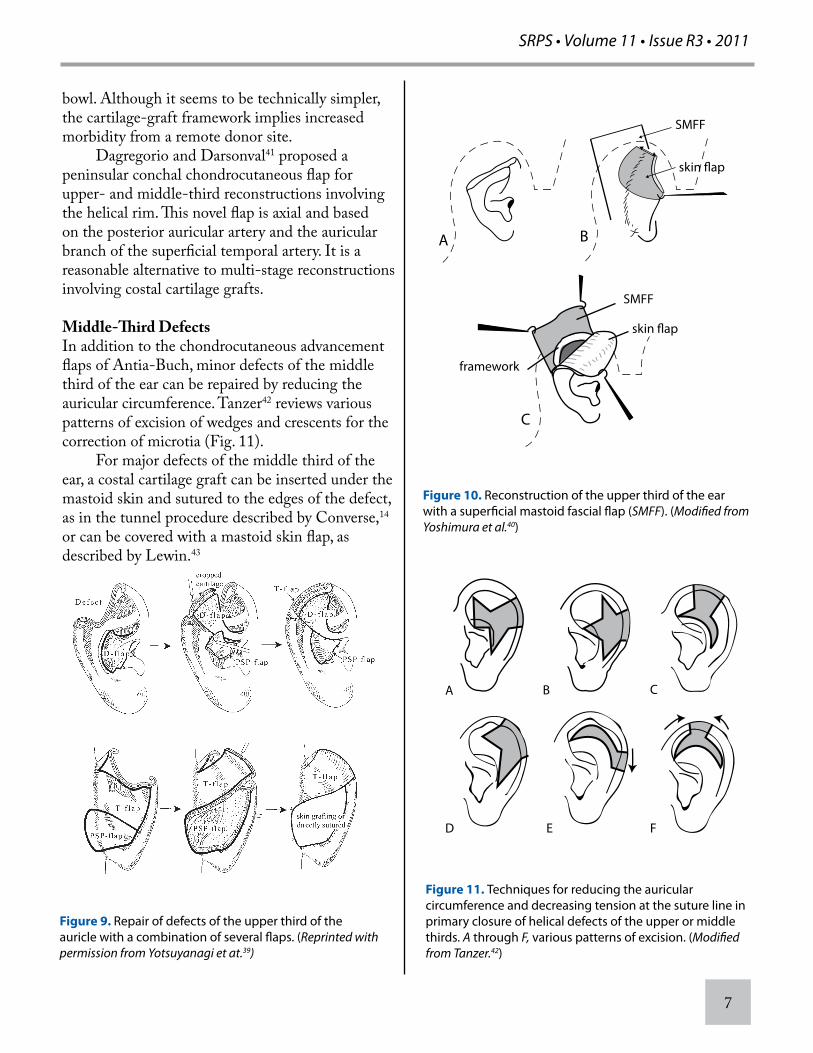
Alternatives to the compound flap presented by Orticochea37 for one-stage reconstruction of the upper third of the auricle include several local flap combinations. Yotsuyanagi et al.39 described a complex method of reconstruction that consists of three different flaps. A chondrocutaneous flap is elevated from the conchal bowl and advanced into the defect to provide cartilage support and anterior skin coverage. A postauricular transposition flap is then used to provide posterior skin coverage of the wound, resulting in a secondary conchal bowl defect that is repaired with a postauricular subcutaneous pedicled flap similar to those described above for nonmarginal defects. The defect that results from harvesting the postauricular subcutaneous pedicled flap is repaired with a full-thickness skin graft (Fig. 9).39
Similar one-stage reconstruction of the upper ear has been described by Yoshimura et al.40 The authors combined a postauricular skin flap transferred anteriorly with a mastoid fascial flap for the posterior surface, and the two flaps were then used to sandwich a fabricated costal cartilage framework (Fig. 10). The donor area for the mastoid fascial flap is skin grafted. This technique differs from the technique presented by Yotsuyanagi et al.,39 described above, in that the cartilage is replaced with a free rib cartilage graft and not a chondrocutaneous flap from the conchal
A B C
Figure 8. Orticochea procedure of conchal rotation for the repair of upper- and middle-third auricular defects.
SRPS • Volume 11 • Issue R3 • 2011
7
bowl. Although it seems to be technically simpler, the cartilage-graft framework implies increased morbidity from a remote donor site. Dagregorio and Darsonval41 proposed a peninsular conchal chondrocutaneous flap for upper- and middle-third reconstructions involving the helical rim. This novel flap is axial and based on the posterior auricular artery and the auricular branch of the superficial temporal artery. It is a reasonable alternative to multi-stage reconstructions involving costal cartilage grafts.
Middle-Third DefectsIn addition to the chondrocutaneous advancement flaps of Antia-Buch, minor defects of the middle third of the ear can be repaired by reducing the auricular circumference. Tanzer42 reviews various patterns of excision of wedges and crescents for the correction of microtia (Fig. 11). For major defects of the middle third of the ear, a costal cartilage graft can be inserted under the mastoid skin and sutured to the edges of the defect, as in the tunnel procedure described by Converse,14 or can be covered with a mastoid skin flap, as described by Lewin.43
Figure 9. Repair of defects of the upper third of the auricle with a combination of several flaps. (Reprinted with permission from Yotsuyanagi et at.39)
BA
SMFF
C
SMFF
framework
Figure 10. Reconstruction of the upper third of the ear with a superficial mastoid fascial flap (SMFF). (Modified from Yoshimura et al.40)
A B C
D E F
Figure 11. Techniques for reducing the auricular circumference and decreasing tension at the suture line in primary closure of helical defects of the upper or middle thirds. A through F, various patterns of excision. (Modified from Tanzer.42)

8
SRPS • Volume 11 • Issue R3 • 2011
Songcharoen et al.5 presented a discussion of management alternatives for tumors of the external ear, including reconstruction of middle-third wounds. Hinderer et al.44 suggested placing the cartilage and skin suture lines at different levels to avoid notching of the helical rim. Mellette45 reviewed various techniques of partial ear reconstruction with local flaps. Techniques for repair of middle-third defects that do not rely on the reduction of auricular size include multistage techniques.4
Lower-Third Defects, Including the EarlobeAuricular losses of the lower third, including the earlobe, can be repaired with a superiorly based flap doubled on itself, as described by Preaux,46 or with a modified “valise handle” technique, as described by Brent.20 Brent20 recommended using cartilage grafts to adequately reconstruct the lower third of the ear. Contralateral conchal cartilage grafts can be subcutaneously implanted and later raised as bipedicled chondrocutaneous flaps. A skin graft is placed on the medial side of the flap to cover the cartilage, creating a valise-handle effect. This technique offers good definition to the posterior aspect of the conchal wall and inferior crus on the anterior surface of the ear. Brent47 also described a double-lobed postauricular flap for total earlobe defects. Davis48 described a technique that uses a posterior (medial) lining flap turned over from the anterior surface of the remaining helix and scapha and a mastoid flap for anterior (lateral) earlobe reconstruction.49 Cordova et al.50 reported total or subtotal earlobe reconstruction with an innervated retroauricular skin flap. Sleilati51 proposed total earlobe reconstruction with double-crossed skin flaps, one from the preauricular area and the other from the retroauricular and/or neck skin.
Non-helical Defects (Concha, Antihelix, Tragus)Numerous techniques have been described for conchal defect reconstruction. Most smaller defects are easily managed with split or full-thickness skin grafts either onto conchal cartilage perichondrium or the retroauricular skin (if cartilage is absent). For larger defects, Masson52 described a “revolving door”
island flap based retroauricularly. Typically, a skin graft is required for donor site coverage. Renard53 and Talmi et al.35 also described postauricularly based myocutaneous and dermal pedicled flaps for anterior conchal and ear defects. Azaria et al.54 proposed a pull-through transpositional flap based retroauricularly for reconstruction of smaller conchal defects. Turan et al.55 also discussed a postauricular pull-through type flap but with a neurovascular island. Adler et al.56,57 and Dagregorio and Darsonval41 discussed various local and regional flaps for non-helical ear reconstruction. A simple pre-auricular transposition flap folded on itself was proposed for full-thickness tragal defects. Other flaps for antihelical and triangular fossa reconstruction were also discussed.
Cleft Earlobe DeformityCleft earlobe deformities can be congenital or acquired. Deformities of the earlobe and their reconstructive alternatives were reviewed by Boo-Chai,58 Brent,20 Effendi,59 Fearon and Cuadros,60 and Attalla.61 Clefts of previously pierced earlobes probably are the most common acquired defects seen. As a result of the gravity of large earrings or from traction injuries from earrings, partial or complete tears of the earlobe can result. Cleft earlobes can also be congenital in origin. Kurihara62 classified congenital deformities into four categories:
Type I, vertical cleft with anterior and posterior divisions of the earlobe
Type II, horizontal cleft with superior and posterior divisions of the earlobe
Type III, combination horizontal and vertical (mixed cleft type) cleft earlobe
Type IV, hypoplasia, dysplasia, or agenesis of the earlobe
Types I, II, and III are considered to be “Simple Clefts” and can be reconstructed with Z-plasties or wedge excisions of the cleft with eversion of the margins. Traumatic clefts usually are within this category. Clefts with tissue deficiencies might require local flaps, such as triangular flap, V-Y

SRPS • Volume 11 • Issue R3 • 2011
9
advancement flap, rectangular flap, and hinge flaps. Typically, immediate re-piercing is avoided because of potential early recurrence of the cleft. Delayed piercing after an appropriate period of healing is recommended. Also, re-piercing at a different location outside the line of the scars can reduce risk of recurrence. Pardue63 described a technique that permits the continued use of earrings after repair of the cleft. A tiny flap of adjacent skin is rolled into the superior aspect of the cleft and the torn edges are excised and reapproximated. Elsahy64 described a technique that also preserved an earring at the time of repair. Z-plasties and other geometric flap repairs counteract cicatricial forces that can lead to notching at the lobular border. However, some of these techniques still have linear grooving of the repair within the substance of the earlobe. Lee et al.65 proposed a two-flap and Z-plasty technique that augments the lobular soft tissue at the repair site, preventing depression of the earlobe. The inner margins of the cleft are raised as flaps, de-epithelialized, and advanced into an ipsilateral subcutaneous pocket of the earlobe. A straight line repair is performed except at the inferior margin, where a z-plasty is performed. Agarwal and Chandra66 described a technique of placing a conchal cartilage “disc” graft in a subcutaneous pocket within the lobule repair. Simultaneous re-piercing is performed. The authors advocated this technique for improved support of the earring and reducing the risk of recurrent clefting.
Total or Near-Total Defects In 1976, Miller et al.67 reported the first successful microvascular replantation of a scalp and part of an ear. The authors used vein grafts and a total of 13 anastomoses. Two years later, Nahai et al.68,69 described replantation of an entire scalp and ear with microvascular anastomoses of only one artery and one vein. Not long after, Pennington et al.70 successfully replanted a totally avulsed ear with vein grafts to the superficial temporal artery and vein. In situations in which no adequate artery is identifiable in the amputated part, an arteriovenous
anastomosis has been shown to be a suitable alternative.71 The cosmetic results obtained with primary microvascular replantation of the ear have been excellent.68,69
Successful ear replantation depends on the presence of either the superficial temporal or posterior auricular arteries for microvascular anastomosis. For cases in which the injury includes these vessels and the likelihood of a successful replantation is low, Jenkins and Finucan72 proposed dissection of the cartilage and skin from the amputated part, reattachment of the cartilage to the side of the head, and coverage with a temporoparietal fascial (TPF) flap, which is in turn covered with the saved ear skin as a full-thickness graft. It is presumed that the temporoparietal flap nourishes both the underlying cartilage and the overlying skin. The ears of two patients were salvaged in this manner; in the second case, an acrylic splint was applied for 3 months to increase the cartilaginous detail and the result was satisfactory. A similar strategy was used by Sućur et al.73 when dealing with an almost completely avulsed ear. The authors buried the separated ear cartilage under the volar forearm skin as a composite radial forearm free flap. Approximately 10 weeks later, the composite forearm flap was transferred to the head where it was revascularized by microanastomoses to the superficial temporal blood vessels. The skin of the flap served as cover for the newly attached ear cartilage. Two revision procedures were subsequently performed to trim the excess subcutaneous tissue. Musgrave and Garrett74 reviewed several reports of replantation of avulsed ears as composite grafts without microsurgical revascularization and concluded that such replacement is almost always doomed. In 1967, the authors were able to document only three cases of successful composite auricular replantation. Other reports before and since invariably lack sufficient follow-up to make an informed judgment about ear appearance.75–77
For cases of near-total loss in which the amputated part has been recovered, Mladick et al.78 recommended the “pocket principle” of ear salvage. Based on this principle, the amputated

10
SRPS • Volume 11 • Issue R3 • 2011
segment, if in good condition, is dermabraded to remove the epithelium and is reattached to the ear stump. The repaired section is then buried under the postauricular skin in a subcutaneous pocket and is left in place for no longer than 21 days, during which time it is nourished through the pocket. If the ear is removed from the pocket before 3 weeks of implantation, the previously dermabraded surface spontaneously re-epithelializes. This technique, in essence, increases the chances for survival of large composite flaps by providing an interim period of nourishment of the amputated part in a subcutaneous pocket. However, a recent literature review of 74 cases in 56 publications strongly discouraged both the pocket method and periauricular skin or fascia flaps for immediate reconstruction, citing inconsistent aesthetic outcomes in comparison with delayed reconstruction with rib cartilage.79
Delayed reconstruction in cases of near-total and total auricular defects differs significantly from reconstruction in cases of microtia. The microtic vestige is unfurled for an extra measure of skin. After trauma, the remaining skin can be poor in both quality (scarring and poor elasticity) and quantity. The meatus precludes an anterior incision, further decreasing the effective amount of cover. Although some authors advocate banking of traumatically avulsed cartilage remnants, this does not often yield useful reconstructive material. The practice of auricular reconstruction currently favors the use of high-profile autogenous cartilage or polyethylene frameworks overlaid with a TPF flap and split thickness skin graft in preference to techniques that use salvaged, pocketed, or transferred cartilage. Reconstruction of the traumatic, complete deformity requires fabrication of an auricular framework and, frequently, soft-tissue coverage with a TPF flap,72,80–83 scalp roll, or skin grafts. If the mastoid skin is relatively unaffected, it can be used primarily for soft-tissue coverage. Elevation of the framework and splicing to the remaining cartilage and external auditory canal can be performed at a later stage. Zhou et al.84 described a technique of secondary auricular reconstruction in patients who have total or near-total defects in whom local
tissues are not available, such as after a burn. The procedure consists of subcutaneously implanting a carved cartilaginous framework in the forearm. At a second operation, the composite unit of cartilage and forearm skin is transferred as a free flap to the head to replace the missing ear. Despite the limited number of cases reported, the method promises to offer a reconstructive solution for selected patients.
ACUTE AURICULAR HEMATOMAAcute hematoma of the pinna is a condition that occurs when a collection of blood forms beneath the perichondrial layer of the pinna. A systematic Cochrane database analysis conducted by Jones and Mahendran85 failed to identify any method of treatment as providing a superior cosmetic outcome, although the key to treatment remains to extirpate the hematoma and prevent its recurrence. A recent 22-patient study by Giles et al.86 found superior outcomes with incision, drainage, and absorbable whip-type mattress suture repair without bolsters. Recurrent hematomas are related to intracartilaginous as opposed to simple subperichondrial collection, as demonstrated by Ghanem et al.,87 and should be recognized as such and treated with surgical incision and drainage.
Cauliflower EarThe cauliflower ear deformity is common among wrestlers, who constitute a much younger patient population than that usually presenting for excision of auricular skin cancer. The cauliflower deformity is the result of repeated episodes of auricular hematoma after direct trauma, eventually leading to the typical appearance of a curled and thickened ear. The pathophysiology of the deformity is subperichondrial bleeding on the anterior surface of the ear and new cartilage formation within the confines of the perichondrium.88 Griffin89 suggested treatment by open drainage of the hematoma and total excision of the fibroneocartilaginous layer and perichondrium. The skin is closed under bolsters to recontour cartilage detail.
MICROTIACauses Variable degrees of penetrance of the gene(s)

SRPS • Volume 11 • Issue R3 • 2011
11
responsible for hypoplasia account for the different sizes of microtic remnants that occur. Even with extremely small microtic remnants, a lobular component is almost always present, although vertically oriented and superiorly displaced. Anotia, the severest of ear deformities, is extremely rare and probably represents complete failure of development of the auricular helix through a lack of mesenchymal proliferation.90 Other severe forms of microtia probably represent arrests in embryonic development occurring at approximately 6 to 8 weeks of gestation. Less extreme forms of microtia are likely the result of embryonic accidents at a later stage, approximately the 3rd month of fetal development.91
EpidemiologyThe incidence of microtia varies with the extent of the deformity. Severe abnormalities occur in approximately 1:7000 to 1:8000 births.92,93 The right side is affected approximately twice as often as the left, and bilateral deformities occur in 10% of cases. The male:female ratio is variously reported as 2:1 to 3:1.
ClassificationNumerous classification schemes have been proposed for microtia. Rogers94 recognized four degrees of external ear deformity: microtia, lop ear, cup ear, and protruding ear. In 1977, Tanzer95 suggested a popular classification of auricular defects according to decreasing severity of involvement, from anotia (group I) to prominent ears (group V) (Table 1).
Associated ConditionsAtresia of the cartilaginous or bony external canal is commonly associated with microtia. The atresia ranges from complete absence to several degrees of narrowing, blind pouches, or tracts. In a case series presented by Tanzer,95 all patients had some deformity of the ear canal, middle ear, or both and 50% had overt evidence of the first and second branchial arch syndrome (hemifacial microsomia). A recent study suggested that isolated microtia might represent the mildest phenotypic expression of hemifacial microsomia.96 In addition, increasing
evidence indicates that hemifacial microsomia, Goldenhar syndrome, and oculoauriculovertebral dysplasia are variants of the same condition, with a phenotypic spectrum of severity including various degrees of microtia.97
ANOMALIES OF THE MIDDLE EAR AND ASSOCIATED STRUCTURESEmbryologically, the external ear is formed earlier than the middle ear, so that even though it is possible to encounter a normal auricle and a malformed middle ear, in the presence of microtia, one should not expect to find a normal middle ear.98 Although Schuknecht99 finds no correspondence between severity of the microtia and degree of middle ear pathology, most otologists relate the severity of the auricular defect to the status of the middle ear.95 In a retrospective study of 224 cases of aural atresia, Kountakis et al.100 noted a positive correlation between the grade of microtia and middle ear development. They concluded that the better developed the external ear is, the better developed the middle ear is. Gill,101 however, believes the tragus is the only reliable indicator of middle ear pathology: when the tragus exists, there is usually an adequate middle ear cleft. In addition to the conductive-type deafness usually associated with microtia, inner ear (cochlear) abnormalities and sensorineural deafness can also occur. Fukuda102 stated that the presence of a small external auditory canal can indicate a severe mixed-type (conductive and sensorineural) deafness, whereas atresia of the canal with common microtia usually is associated with deafness of a more simple conductive type. Abnormalities of the middle ear range from minor dysplasia of the ossicles to complete obliteration of the tympanic cavity. Several degrees of fibroplasia and fusion of ossicles are common, but the stapes usually is normal. The facial nerve sometimes traverses an anomalous course, which must be considered during reconstructive surgery.
HEARINGDiagnostic evaluation of hearing usually involves audiogram or auditory brainstem response (ABR) testing. Audiograms are useful in children old

12
SRPS • Volume 11 • Issue R3 • 2011
enough to correctly respond to sound stimuli from a cognitive standpoint. The ABR is recommended to accurately determine the degree of sensorineural hearing loss and conductive loss in newborns and infants. ABR can also help identify which is the better hearing ear.103
High-resolution computed tomography (CT) provides anatomic detail of the middle ear. This information is useful to the otologist in assessing whether the child is a reasonable candidate for atresia repair. CT typically is performed when the patient is between the ages of 4 and 6.103
Hearing AidsFor children to develop verbal communication skills, they must be able to hear. Bone conduction hearing aids are generally used for this purpose, either permanently or pending surgery for aural atresia. Children with unilateral microtia and aural atresia who have normal hearing in the contralateral
ear typically have no need for a hearing aid and are expected to develop speech normally. In contrast, children who have bilateral microtia and aural atresia must be fitted with bone conduction hearing aids shortly after birth if speech is to develop.103
Bone conduction aids require intact and unscarred mastoid skin; therefore’ surgical incisions for tympanoplasty or for the insertion of an auricular framework are contraindicated because they compromise future use of hearing aids. For patients who need bilateral bone conduction hearing aids, an external, bone-anchored appliance combined with an osseointegrated Brånemark titanium fixture is a good choice.104
Granström et al.104 showed excellent retention of the implanted prostheses over the long term. In addition, all patients who were supplied with percutaneous bone-anchored hearing aids considered them to be superior to conventional bone-conducting appliances. Even patients who had
Table 1
Clinical Classification of Auricular Defects42
Classification Defect
I Anotia
II Complete hypoplasia (microtia)
A With atresia of the external auditory canal
B Without atresia of the external auditory canal
III Hypoplasia of the middle third of the auricle
IV Hypoplasia of the superior third of the auricle
A Constricted (cup or lop) ear
B Cryptotia
C Hypoplasia of the entire superior third
V Prominent ears

SRPS • Volume 11 • Issue R3 • 2011
13
previously undergone surgical treatment for aural atresia considered their hearing to be better with the bone-anchored hearing aids than it was after surgery. In 1990, a team of researchers from Sweden105 reported their results with a percutaneous transducer, the Nobelpharma Auditory System HC 200 (Nobelpharma AB, Goteborg, Sweden), which they had been implanting since 1977. The device consists of a bone-anchored hearing aid on the surface linked to an implanted Bränemark titanium probe integrated in the mastoid process. Audiological measurements indicate a considerable difference in performance between this percutaneous system and transcutaneous devices, probably as a result of the gap between receiver and transducer. The large gap of the transcutaneous system means increased power consumption, lower maximum output capability, and high levels of second harmonic distortion. According to the authors, the only reason to choose a transcutaneous device over a percutaneous system is to avoid permanent skin penetration, and they report that only one of 250 implanted devices had to be removed because of soft-tissue problems.
Indications for Atresia RepairConventional wisdom dictates that no attempt should be made to restore hearing on the affected side in patients who have a normal-hearing ear. Only approximately 20 dB of improvement can be expected from atresia repair.103 Many authors99,106,107 therefore think that middle ear reconstructive procedures are contraindicated in patients with unilateral microtia. Infants with bilateral microtia in whom auditory acuity cannot be corrected with a hearing aid by 12 months of age should have middle ear exploration on one side. A different philosophy is championed by Jahrsdoerfer and colleagues.108,109 Using high-resolution CT of the temporal bone in conjunction with physical examination, the authors developed a grading scheme of anatomic features to aid them in selecting candidates for atresia repair. The rating scale is as follows:
• 2 points if the stapes is present • 1 point for each of the following,
if present:�� an open oval window�� adequate middle ear space�� normal course of the facial nerve�� a malleus-incus complex�� good mastoid pneumatization�� incus-stapes connection�� good external ear appearance�� ear canal stenosis with malleus bar
A perfect score is 10. A score ≥8 indicates that the patient is a good candidate for atresia surgery. A score of ≤5 is a contraindication for surgery. Jahrsdoerfer et al.109 reported postoperative hearing improvement to normal or near-normal levels in 74 of 90 patients with scores of ≥8 (82%). Objective measure of improvement was obtained with the speech-reception-threshold test. Considering the author’s considerable experience, the success rates are likely the best that can be achieved. Audiometric testing differentiates conductive from sensorineural impairment. If the predominant deficit is sensorineural, middle-ear reconstruction is contraindicated. Lack of pneumatization of the mastoid air cells by age 4 years denotes inadequate development and is another contraindication to middle-ear reconstruction. Additional considerations in the decision for or against surgery are the real possibilities of chronic postoperative drainage, facial nerve injury, and subsequent stenosis of the reconstructed canal. The ultimate decision for atresia repair is a complex one and must be mitigated by consideration of the risks, including facial nerve injury, stenosis of the external auditory canal, and chronic infections or drainage from the surgical site.110
Siegert111 evaluated atresia repair and middle ear surgery performed in specialized centers and found disappointing outcomes: only 48% of patients had successful reconstructions (conductive deficit <30 dB). The authors advocated atresia repair during the second stage of ear reconstruction (framework elevation) for patients with a 50-dB conduction deficit. In their series, 76% of the patients achieved a final conductive hearing loss of ≤30 dB. During the first surgery, rib cartilage is placed around a Silastic tube (Dow Corning Corporation, Midland, MI) to prefabricate an
14
SRPS • Volume 11 • Issue R3 • 2011
external auditory canal. At the same time, a tympanic membrane is reconstructed by using the elastic cartilage of the lobular remnant. This is assembled during the second surgery and implanted after mastoid drilling. During the third and final operation, the concha is deepened with Z-plasties and a full-thickness skin graft is used to line the new external auditory canal. More recent studies confirm that approximately 50% of patients undergoing aural atresia repair achieve the 30-dB hearing reception threshold with an average improvement of 22 dB. Digoy and Cueva112 did not find significant differences in short- and long-term outcomes. Chang et al.113 followed 93 patients for an average of 57 months. They found long-term hearing success in 73% of patients for primary cases and only 50% for revision cases. The authors cautioned against aural atresia repair in revisionary or severely microtic patients; they advocated a low threshold for bone anchored hearing aids in such patients.
EXTERNAL EAR RECONSTRUCTIvE OPTIONSAlthough staged reconstruction with autologous rib cartilage is considered the technique of choice, other options make this a somewhat controversial issue. Thorne et al.114 discussed the advantages and disadvantages of each:
“The standard results obtained by these experts [experts in microtia] are difficult to match because the deformity is rare. As in other areas in plastic surgery, but perhaps even more so, the first attempt at reconstruction is of paramount importance because a suboptimal result may be uncorrectable.“Because consistently good results with autogenous reconstruction have proved elusive in the hands of many surgeons around the world, other techniques for auricular reconstruction have been evaluated. To date, replacing the cartilage framework with an alloplastic framework has not proved to be effective…“Prosthetic reconstruction of the auricle
has been available for centuries, but ineffective, messy, and inconvenient adhesives have detracted from its practicality. In addition, there is tremendous variability in the aesthetic quality of prostheses and, given the problems with retention, any prosthesis must be aesthetically excellent for the patient to tolerate its use.”
Classic techniques of ear reconstruction depend on construction of an auricular framework with either autologous costal cartilage or alloplast. Considering that good aesthetic results are possible with both materials, the choice of one method over another is based primarily on the number and severity of associated complications. Other factors influencing the selection of an auricular framework include the following: 1) number of operations involved; 2) donor-site morbidity; 3) postoperative distortion of cartilage; 4) tendency toward migration or malposition; 5) infection or extrusion of the framework; and 6) durability. Beahm and Walton115 reviewed the embryology, anatomy, clinical evaluation, and reconstructive options for microtia repair.
ProstheticSince the advent of osseointegrated implants, ear reconstruction with auricular prostheses has become a valid option in cases of missing ears. Osseointegrated auricular prostheses are dental-type implants constructed out of pure titanium that are placed into the mastoid bone. The implants are left buried under the skin to allow for a period of osseointegration. After firm union with the bone is established, the implant is uncovered and abutments that protrude through the skin are affixed to it. These abutments are then used to attach an ear prosthesis by a variety of mechanisms, such as bull-and-studs, magnetic retention, or bar-and-clip systems. In contrast to other prosthetic methods, osseointegrated auricular prostheses do not need a skin adhesive for attaching the ear. However, the patients must commit to lifelong follow-up and meticulous hygiene around the metal abutments protruding through the skin.116,117

SRPS • Volume 11 • Issue R3 • 2011
15
Wilkes and Wolfaardt116 described their experience with osseointegrated alloplastic ear reconstruction and suggested criteria for treatment selection. The authors concluded that osseointegrated alloplastic ear reconstruction is indicated in the following types of cases: 1) reconstruction after major cancer resection; 2) poor local tissue; 3) absence of the lower half of the ear; 4) salvage after unsuccessful autogenous reconstruction; and 5) in patients who are poor anesthetic risks. Autogenous ear reconstruction is indicated in cases of classic microtia when the lower third of the ear is relatively normal, for patients whose compliance is in question, and for patients with a strong preference for reconstruction with autogenous tissue. The authors reported achieving excellent results in appropriately selected patients but indicated that osseointegrated procedures should be performed only in a properly organized, multidisciplinary setting that includes a maxillofacial prosthetist. Han and Son118 described use of an implant-carrying plate system to overcome the problem of retention of implants in young temporal bone. Excellent stability of the implants was achieved, and no submergence (beneath the skin) occurred with their technique. Thorne et al.114 reviewed different reconstructive options and outlined the relative advantages and disadvantages of each. Relative indications for prosthetic reconstruction included the following: 1) failed autogenous reconstruction, 2) excessively low hairline, and 3) severe hypoplasia of soft tissue or bone in the auricular region. Miles, Sinn, and Gion (Miles et al.119) reviewed their technique for one-stage cranial implantation for prosthetic auricular reconstruction. They reported good stability and a 6.1% incidence of infection. Gentile et al.120,121 also reported low complication rates for cranial implant reconstruction for both microtia and burn injury.
Alloplastic Alloplastic frameworks are an alternative to frameworks made of costal cartilage. The most commonly used materials are silicone and porous polyethylene (Medpor; Porex Technologies Corp.,
Fairburn, GA). Cronin,122 Cronin et al.,123 and Cronin and Ascough124 introduced the Silastic framework (Dow Corning) for ear reconstruction and described their experiences with it. The prosthesis is inserted in a generous pocket dissected from the mastoid area, leaving a thin layer of subcutaneous fat on the skin flap, and the auricle is elevated at a second (or third) stage approximately 3 months later. Descriptions of the technique can be found in the articles by Cronin and colleagues122-124 and in articles by Ohmori and colleagues125-127 (Ohmori125,126 and Ohmori et al.127). Brauer (personal communication) later abandoned the use of silicone frames for reconstruction of the ear because of gradual erosion of the implant from either internal or external pressures, with eventual exposure. The exact incidence of this complication is not clear. The author did note that in patients in whom the silicone frames survived (some for more than 15 years), the ears had what he called a normal look and feel to them, more so than with cartilage reconstruction. Clinical experience with auricular framework implants of porous polyethylene (Medpor) was reported by Wellisz.128 Porous polyethylene has an important advantage over Silastic implants (Dow Corning): it allows tissue ingrowth into its pores. Of 41 Medpor frameworks used for auricular reconstruction, five extruded: two in patients with microtia and three in burned ears. None of the implants had to be removed, and the exposures healed with local wound care. The author concluded that soft-tissue coverage is of paramount importance to the success of auricular reconstruction with porous polyethylene frameworks and recommended using a TPF flap to ensure an adequate blood supply to the cutaneous cover and to anchor the ends of the implant that might otherwise spring through the skin. Reinisch129 described his technique of Medpor auricular reconstruction, which he performed in more than 100 patients, achieving early promising results. Initially, the complication rate was 44%, which went down to almost nil after a TPF flap was added to the procedure. Despite substantial recent data on temporoparietal flap and full-thickness skin

16
SRPS • Volume 11 • Issue R3 • 2011
techniques from Romo and Reitzen130 and Yang et al.,131 which delineate the benefits of Medpor as a reliable, aesthetic option for ear reconstruction, long-term risks of exposure and infection cannot be ignored.
Autogenous HarvestAutologous costal cartilage for ear framework construction is traditionally harvested from the sixth, seventh, and eighth ribs. Brent132 harvested a portion of the ninth rib to function as a strut for the tragus, which was incorporated into the auricular framework. Other modifications include taking a wedge of cartilage to be banked in the postauricular skin at the time of framework placement, for use in ear elevation at a later stage, and preserving a rim of cartilage at the superior aspect of the sixth rib to minimize postoperative pain, clicking, and chest wall contour deformities (Fig. 12).4
In addition to the cartilage-sparing techniques described above, Brent132 also reported differences in framework construction according to patient age. For example, in older patients, the ribs often
are fused and calcified and the framework must be carved from a single block of cartilage. Tanzer95 preferred contralateral cartilage but noted that ipsilateral cartilage is also acceptable. The author formerly removed the rib cartilage extra-perichondrially (taking perichondrium with the graft), but because of several instances of postoperative chest wall depression, Tanzer now advocates a subperichondrial technique of leaving the perichondrium behind when harvesting the rib graft. Thomson et al.,133 on the other hand, reported deformity of the chest wall when extraperichondrial dissections were performed. Clearly, chest wall deformities can occur whether perichondrium is left in the donor site or is removed with the graft. Fukuda and Yamada134 use ipsilateral cartilage that has been dissected extraperichondrially on the graft (outer) surface but subperichondrially on the visceral (inner) surface. This is a logical approach because it keeps perichondrium at the donor site (for possible cartilage regeneration) and on the newly built framework in contact with mastoid tissues (for potential cartilage revascularization). Donor site reconstruction with spare rib cartilage is recommended.135 In fact, Kawanabe and Nagata136 described a new method of complete perichondrial preservation and creation of donor-site pocket for return of residual cartilage framework and found no donor site contour deformity at a mean of 2 years in 273 patients. Moreover, a histological study was conducted that revealed regenerated cartilage to be cylindrical and histologically normal at 12 months, allowing it to be used during the second-stage operation.137 Although perichondrium on the outer surface of the framework helps with skin adherence, even with total extraperichondrial harvest, most of the surfaces are denuded of perichondrium in the process of carving and fabricating the framework.
Timing of SurgeryMiddle ear and auricular reconstructive procedures are planned jointly by the otologist and the plastic surgeon, and the timing of the surgery takes into account the hearing status of the patient and cosmetic considerations with its psychological sequelae. As plastic surgeons, we focus on factors that determine the appropriate
Graft
A B
C D
Figure 12. Dieffenbach’s technique for reconstruction of the middle third of the auricle. A, Defect and outline of the flap. B, Flap advanced over the defect. C, Flap is divided at a second stage. D, Flap is folded around the posteromedial aspect of the ear and a skin graft covers the donor site. (Modified from Brent.4)

SRPS • Volume 11 • Issue R3 • 2011
17
time for reconstructing the external ear: 1) rate at which costal cartilage develops, 2) risk of the child’s becoming a target of ridicule,138 and 3) corresponding size between the fabricated framework and the normal ear. It generally is agreed that by approximately age 6 years, affected children become targets of ridicule by their peers. At that age, the child is aware of being different and is motivated to conform, which will make him or her more cooperative with the surgery and the restrictions it entails.139 Before age 6 years, sufficient rib cartilage might not be available to build an ear framework of the proper vertical dimension and horizontal projection. Tanzer,95 Edgerton,140 and Brent141 recommended auricular reconstruction at about ages 5 to 6 years, and that view is shared by most otologists and plastic surgeons. Thomson and Winslow,142 however, reported performing auricular framework construction when the child is 2 to 3 years old, confident that sufficient cartilage is available by then to match the normal ear. The reconstructive framework with intact perichondrium will proceed to grow concomitantly with the normal ear if left undisturbed. Adamson, Horton, and Crawford (Adamson et al.143) reviewed the growth patterns of the auricle. After examining 2300 ears, the authors concluded that the average child attains 85% of ear development by age 3 years; ear height continues to increase until adulthood, but its width and distance from the scalp change little after age 10 years. Based on anthropometric studies, Farkas144 noted that the ear reaches approximately 85% of its full size by age 6 years, 90% by age 9 years, and 95% by age 14 years. Approximately 88% to 94% of the adult ear width is reached during the first year of life, and girls’ ears grow faster than boys’. With respect to ear length, however, the figure is 75% by the end of year 1 and 93% by age 10. The ear continues to grow longer during the next decade,12,144 although for practical purposes, the ear is considered to be almost fully developed at age 6 years.8
A fundamental question in deciding the appropriate timing of surgery is whether the costal cartilage framework continues to grow once implanted. Tanzer145 followed 37 patients
for approximately 8 years and noted incremental growth of the reconstructed ear at a rate almost equal that of the normal ear. Thomson and Winslow142 later confirmed that finding. Brent141 reported that in a series of patients operated on at ages 5 through 10 years, 37 of 76 ears grew at an even pace with the opposite normal ear, 32 of 76 grew larger by several millimeters, and 8 of 76 grew smaller by several millimeters. The follow-up duration in that study was ≥5 years. DellaCroce et al.146 confirmed vertical and horizontal growth of the ear (5 and 2.75 mm, respectively) after cartilage framework implantation. That observation led to the following question: Should the reconstructive framework be smaller, larger, or the same size as the normal ear? Tanzer145 recommended constructing a costal cartilage framework that is 2 to 3 mm larger than the normal ear. Brent,139 on the other hand, thought that one should try to match the opposite ear regardless of patient age. He saw no reason to construct an ear larger than the normal one and suggested that in younger patients, one could consider making the framework several millimeters smaller, because the growth rate of costal cartilage might be expected to be faster than that of auricular cartilage.
Middle-Ear SurgerySurgery of the middle ear associated with reconstruction for microtia must be planned jointly by the plastic surgeon and the otologist. This is most important for patients with bilateral microtia. If hearing aids can provide adequate hearing for speech development, atresia repair can be postponed until after the costal cartilage framework has been placed. The reason for the delay is that attempted atresia repair before auricular reconstruction will lead to scarred, poorly vascularized tissue in the mastoid area and will compromise the quality of the soft-tissue coverage for the framework.103,139 Even in cases of unilateral microtia, atresia repair can be incorporated into the reconstructive sequence for the microtia. In cases with both bilateral and unilateral microtia, surgery of the middle ear should not be attempted until after the costal cartilage framework has been placed.

18
SRPS • Volume 11 • Issue R3 • 2011
Operative Sequence The stages of auricular reconstruction depend on the severity of the deformity, the position and quality of the microtic elements, and the surgeon’s preference. The exact sequence of operations is less important than following the operative plan and carefully tailoring the procedures to the specific anatomic deformity. Tanzer95 initially described a four-stage reconstruction in 1971:
• Rotation of the lobule into a transverse position
• Fabrication and placement of a costal cartilage framework
• Elevation of the ear from the side of the head
• Construction of a tragus and conchal cavity.
Tanzer145 subsequently combined the first two to complete the reconstruction in three stages but noted that when extensive mobilization of the lobule was necessary, such as in cases of marked malposition or an extremely small remnant, the four-stage reconstruction was still in order. Additional operative stages to create a tunnel and for final closure are also needed when middle ear reconstruction is contemplated. The most significant addition to the literature of ear reconstruction in the last few years comes from Brent’s 2 decades of experience with 600 cases followed for a median 5 years.139 In a long-term retrospective analysis, Brent139 recounts his treatment plan, surgical technique, and perioperative management of the microtic deformity. Brent141 prefers a four-stage technique consisting of the following:
• Framework placement• Lobule transposition• Tragus construction and conchal
excavation• Elevation of the ear framework with
creation of the auriculocephalic sulcus Brent147 subsequently added tragal reconstruction as part of the initial framework
fabrication and placement in some patients. He avoids repositioning vestigial remnants (earlobe) because the resultant scars can impair circulation and skin elasticity and render insertion of the three-dimensional framework difficult.139
Brent139 emphasized that the reconstructed ear will not project adequately unless a high-profile framework has been used. In cases of inadequate projection, or when the patient wears glasses or desires a well-defined auriculocephalic sulcus, a fourth stage is necessary to elevate the ear and release it with skin grafts. Occasionally, the middle two stages are reversed to accommodate the patient’s preferences.139
For patients deemed to be candidates for atresia repair, Aguilar103 proposed an integrated protocol of auricular reconstruction in five operative stages, as follows:
• Framework construction and placement• Lobule creation• Atresia repair• Tragal creation• Auricular elevation
The approach presented by Aguilar103 combines the technique presented by Brent147 with correction of aural atresia as stage 3. Once the atresia repair is completed, the new ear canal is lined with a skin graft. The ear is then placed in its original position and adjusted so that the new ear canal is under the concha of the reconstructed ear. An oval segment of skin is excised from the reconstructed ear to create an opening into the new external auditory canal. If the position of the external auditory canal and the concha of the framework do not align, the framework can be relocated by undermining a flap anteriorly as in a rhytidectomy procedure. The surgical technique of atresia repair was described by Jahrsdoerfer et al.109 Salient points are exposure through a postauricular incision and dissection at the level of the mastoid periosteum deep to the auricular framework. To form the external auditory canal, the auricular framework is elevated and retracted anteriorly to permit drilling. In a series of articles, Nagata148–152 traced the

SRPS • Volume 11 • Issue R3 • 2011
19
evolution of a new method for reconstruction of the ear in microtia. Technical details are provided regarding construction of the costal cartilage framework, development of skin flaps for insertion and closure, and elevation of the constructed auricle. Indications for this approach in three different types of microtia—the lobule type, the concha type, and the small concha type—are also presented. Nagata’s two-stage technique consists of the following:
• Fabrication of a three-dimensional costal cartilage framework and simultaneous rotation of the lobule. Framework construction includes fashioning of a tragus and accentuation of the concha. Framework insertion is combined with rotation of the lobule and development of skin flaps, which maximize the skin covering the vestigial cartilage. Lobule transposition, tragus construction, and conchal excavation are all achieved during the first operative stage.
• Ear elevation with placement of a cartilage graft in the auriculocephalic sulcus covered with a pedicled TPF flap and skin graft.
Unlike Brent,147 Nagata148 encountered no deformations or irregularities of the grafted framework and no infection or cartilage exposure in 36 patients followed for up to 7 years. Park et al.153 described a one-stage procedure for total ear reconstruction that is derived from a single-stage method presented by Song and Song.154 The technique uses two flaps—a thin skin flap and an arterialized mastoid fascial flap—to cover a cartilage framework that is carved and inserted on the spot. The auriculocephalic sulcus is created at the same time. The skin flap is expanded intraoperatively, and external molds are used after surgery to maintain proper dimensions and contour of the reconstructed ear. The photographs in the article by Park et al.153 show a contour definition that is not as fine as that achieved with the technique presented by Brent.147 Moreover, attempts at middle ear reconstruction seem to cross the vascular axis of the flaps used in reconstructing the auricle.
Surgical Techniques A detailed description of the various techniques of ear reconstruction is beyond the scope of this overview. The articles by Tanzer,95 Brent and Byrd,80 Burnstein,155 Bauer,156 Yanai et al.,157 Isshiki et al.,158 Aguilar,49 and Nagata148 should be carefully studied by anyone not familiar with the procedures. Zim159 and Walton and Beahm160 provided an excellent overview and comparison of several of the most commonly used techniques. Brent132,147 presented his extensive series of more than 1000 cases of microtia reconstruction, describing modifications and refinements to his technique.
Soft-Tissue Coverage Sufficient soft tissue to adequately cover an auricular framework is a prerequisite to reconstruction. The skin must be thin, pliable, a good match in color and texture, and of good vascularity and elasticity to fit snugly over the underlying skeleton. In primary ear reconstruction, the source of skin might be compromised by a relative skin deficit (in severe microtia), a low hairline, or trauma.
Temporoparietal Fascial (TPF) FlapThe most versatile method for obtaining additional soft-tissue coverage is use of the TPF flap based on the superficial temporal artery or its branches.80–82,127,161–163 The flap can be elevated ipsilaterally and turned down or transferred as a free flap from the opposite side. A thick split-thickness or full-thickness skin graft completes the reconstruction. Flap edema-obscuring detail resolves over a period of weeks to months.
“After first mapping the vessels with a doppler, exposure to the fascia is gained by a Y-shaped incision that extends superiorly above the proposed auricular region. The dissection begins just deep to the hair follicles and continues down to a plane where subcutaneous fat adheres to the temporoparietal fascia. Since initial identification of this plane can be difficult, care must be taken to damage neither the follicles nor the underlying axial

20
SRPS • Volume 11 • Issue R3 • 2011
vessels. Although tedious, once the scalp dissection is accomplished, the inferiorly based temporoparietalis fascial flap is raised easily from the underlying deep fascia that envelops the temporalis musculature.“Subsequently, the fascial flap is first draped over the framework and then coapted to it by means of suction with a small infusion catheter. Then the flap is affixed to the peripheral skin “vest under pants” fashion so as to secure a tight closure. Finally, a patterned, thick split thickness skin graft is sutured on top of the fascia-covered framework and, likewise, is coapted to the fascia by means of a suction catheter. Then the new ear’s convolutions are packed with petrolatum gauze. Finally, a head dressing is applied.”80
Park et al.164 analyzed their experience with 122 TPF flaps for auricular reconstruction. The vascular anatomy was found to be variable among 93 flaps examined. The dominant blood supply was the superficial temporal artery in 82 (88%) of the 93 flaps, the posterior auricular artery in eight (9%), and the occipital artery in three (3%). Venous drainage was similarly variable: the superficial temporal vein in 62 (67%) flaps, the posterior auricular vein in 23 (25%), the occipital vein in six (6%), and the diploic vein in two (2%). Technical refinements in the series presented by Park et al.164 aimed primarily at making the flap thinner and more reliable, so the innominate fascia and subcutaneous fat were excluded from the flap. This increases the risk of injury to the flap vessels, and the authors recommend immediate repair of even small branches to prevent focal vascular insufficiency to the flap. Advances in endoscope-assisted temporoparietal fascia harvest technique for auricular reconstruction have been shown to reduce scarring, alopecia, and surgical time with comparable blood loss.165 Other modifications are the use of split thickness scalp skin whenever a skin graft is required, which results in better color match, and compression of the flap postoperatively
with an external mold to keep it thin and prevent secondary contracture of the grafted skin over the cartilaginous framework. The mold should be worn for 3 months after surgery. Tegtmeier and Gooding163 and Nakai82 reported their results achieved with the TPF flap beneath intact skin or to supplement a small remnant in primary microtia using Silastic and costal cartilage frameworks. Brent139 outlined his technique for managing the low hairline in 600 cases of auricular reconstruction. The framework is located in the position that will produce the best result in terms of symmetry and aesthetics, even if this means placing it where it is partially covered by hair. When hair covers only the upper helix and scapha, it can be removed by electrolysis. When hair covers the upper third of the new ear, the hair-bearing skin is excised, taking care not to expose the underlying cartilage. A graft of postauricular skin taken from the contralateral ear is used to cover the raw area on the reconstructive framework. When a skin shortage and low hairline that can threaten the reconstruction are identified preoperatively, use of a TPF flap covered by skin graft should be considered.139 Brent recommends presurgical hair removal with a laser to create the ideal hairline before embarking on the ear repair. Brent and Byrd80 discussed several ways of elevating and transferring the TPF flap for secondary ear construction and reviewed its advantages, potential role in reconstructive surgery, and complications. Nagata166 recounted his experience with the TPF flap and innominate fascial flap for secondary reconstruction of unfavorable results of microtia surgery. Secondary reconstruction in such cases is more difficult than the primary microtia repair because during the revision procedure, all of the superficial scar must be removed, further reducing the skin surface available for the reconstruction. The soft-tissue problems are compounded by subcutaneous scar tissue, which decreases extensibility of the tissue and hampers insertion of the three-dimensional framework, and by previous skin grafts, which are likely to be contracted, depressed, and shiny. Nagata166 proposed transferring a TPF flap

SRPS • Volume 11 • Issue R3 • 2011
21
to cover the costal cartilage framework during the first stage of the secondary ear reconstruction. The second stage consists of elevating the ear and placing a cartilage graft in the auriculocephalic sulcus. The posterior auricle and sulcus are then covered with an innominate fascial flap and a skin graft. Nagata was able to complete secondary auricular reconstruction in two operative stages by capitalizing on the virtues of the TPF flap and the innominate fascial flap interposed between cartilage and skin.
Deep Temporal FasciaHirase, Kojima, and Hirakawa (Hirase et al.167) recently described a salvage procedure that makes use of the deep temporal fascia when the TPF flap has become partially necrotic and the cartilage framework is exposed. Although a single case was reported, the outcome was good, and the technique offers hope for successful completion of a one-stage reconstruction of the auricle using a TPF flap regardless of complications.
Posterior Temporoparietal and Galeal Fascial FlapAlexander et al.168 described a combined flap based on the posterior branches of the superficial temporal artery to assist with elevation of the cartilage framework. The flap consists of temporoparietal fascia posteriorly and its fusion with the galea. It can be used as a buttress for framework elevation or as soft-tissue coverage for salvage of exposed frameworks.
Tissue ExpansionTissue expansion offers another possible solution for the patient with a small microtic remnant, severe shortage of skin, and low hairline. Brent169 reported inserting an inflatable implant beneath relatively inelastic skin and gradually expanding it with saline infusions during the next 3 weeks. On removal of the expander and subsequent framework placement, the thick capsule that had formed around the implant obscured detail. The patient subsequently had to undergo a secondary procedure for revision and to improve helical definition. Other authors have reported poor long-term
results with tissue expansion mainly because of contraction of the expanded skin.170 The capacity of skin expanders to produce thin, pliable, resilient, and long-lasting cover for skeletal frameworks is a subject of debate. Pan et al.171 and Jiang et al.172 reported excellent results achieved in a large series with tissue-expanded non-hair-bearing mastoid skin flaps. However, any complication resulting from use of the expander, such as infection or extrusion, can permanently jeopardize the available skin in a “virgin” microtia.
ThermosensitivityUsing three-stage reconstruction based on the techniques presented by Brent139 and Nagata,166 a Scandinavian group found significantly higher thermal thresholds in reconstructed helical and antihelical regions. The lower thermosensitivity of the reconstructed ear did not translate to any clinical disadvantages.173
ProjectionTai et al.137 achieved improved projection by using hydroxyapatite-tricalcium phosphate ceramic to augment conchal support and limit total amount of cartilage required in a 42-patient series.
COMPLICATIONSThe reported complication rates in several series of auricular reconstruction are summarized in Table 2. The following points emerge from a review of the data. Extrusion rates are higher for Silastic frameworks than for autogenous cartilage frameworks.123,125,133,141,145,162,174–176 Extrusion rates for Silastic frameworks seem to be decreasing as techniques for soft-tissue coverage improve.123,126 The temporoparietal flap in particular has been shown to be useful in this regard, even in some primary procedures.127 Extrusion of Silastic frameworks is thought to be the caused by the following:
• Too thin a skin cover• Scar tissue in the flap• Tension of the skin over the implant• Trauma126

22
SRPS • Volume 11 • Issue R3 • 2011
• Dead space around the framework126
• Infection126
The largest survey of complications of auricular reconstruction with autogenous cartilage is the large series of 606 cases reported by Brent.139 Problems with the soft-tissue coverage of the costal cartilage framework were common when compression mattress sutures were used to coapt the skin to the helical cartilage. After
discontinuing the bolster sutures and inserting suction drains, the complication rate dropped significantly. Brent reported only three infections (0.5%), two hematomas (0.3%), and five skin losses (0.8%) with cartilage exposure. He stated that most complications can be prevented with appropriate postoperative care. Considering the author’s extensive experience with autogenous cartilage ear reconstruction, the excellent results and
Table 2
Complications of Ear Reconstruction with Frameworks of Autogenous Cartilage and Silastic
Study No. of Frameworks Exposure to Infection, n (%)
Extrusion and Removal, n (%)
Follow-up (yr)
Autogenous cartilage
Wray and Hoopes, 1973174 13 0 0 ?
Fukuda and Yamada, 1978134 329 44 (13) ? ≤16
Tanzer, 1978145 43 5 (12) 0 6−19
Brent, 1980141 63 5 (8) 0 ≤4
Brent, 1992139 606 8 (1) 0 1−17
Alloplasts
Silastic
Edgerton, 1969140 18 9 (50) 2 (11) ≤16
Curtin and Bader, 1969175 42 ? 5 (12) ≤3
Monroe, 1972176 17 ? 4 (24) ≤5
Wray and Hoopes, 1973174 16 13 (81) 13 (81) ?
Cronin, 1978124 71 24 (34) 19 (27) 1−15
Ohmori, 1978126 78 2 (3) 1 (1) 0−3
Medpor
Wellisz, 1993128 41 5 (12) 0 1−4

SRPS • Volume 11 • Issue R3 • 2011
23
low complication rate obtained would have to be considered optimal. Thomson et al.133 documented residual problems with the chest donor sites after ear reconstruction for microtia. In a long-term study of 80 patients (88 donor sites), the authors evaluated the appearance of the chest scars, chest topography, and contour changes of the costal margin. The results of their analysis are summarized as follows:
• Chest scars: 14% were considered “less than acceptable”; the younger the patient was at the time of surgery, the better the chest scars were.
• Chest topography: normal in 75% of patients, mild retrusion in 19%, and severe retrusion in 6%; deformities were less severe in patients who underwent surgery at an older age.
• Rib cage contour: all patients exhibited some degree of change in the costal margin, typically manifesting as a flat, triangular defect; the authors speculated that their closure method, which involved suturing the tip of the ninth rib to the sixth rib cartilage to cover the defect at the harvesting site, might have contributed to the altered contour.
CONSTRICTED EAR DEFORMITYThe constricted ear anomaly can be either the “lop” or “cup” type.177 Tanzer178 categorized constricted ears as shown in Table 3. A lop ear is a malformed auricle in which the characteristic major deformity is an acute downward folding or deficiency of the helix and scapha, usually at the level of the tuberculum auriculae (Darwin’s tubercle). The deformity is associated with a malformed antihelix, usually at the superior crus. A cup ear is essentially a malformed, protruding ear combining characteristics of both a lop ear and a prominent ear. Typical features are an overdeveloped, deep, cup-shaped concha; a deficient superior part of the helical margin and antihelical crura; and apparently small vertical height. The body of the antihelix often is wider than normal,
and whether unfolded or fully developed, it tends to exaggerate the cupping deformity. In some cases, the helical margin or helical fold drapes forward and over the scapha like a hood. In an excellent review of the constricted ear anomaly, Cosman179 analyzed the anatomic deformity and the requirements for its correction; illustrated the various surgical techniques that have been proposed; and discussed the indications, advantages, and disadvantages of each. According to the author, the choice of procedure should be based on accurate definition of the anatomic defect and the size difference between the normal and abnormal ears. Cosman179 dismissed Tanzer’s Group III deformities as forms of microtia that demand total or near-total reconstruction. For less severe deformities (Tanzer’s Group I, IIA, and IIB) within specific anatomic limits, Cosman recommended the procedures listed in Table 4.180 Correction of the deformity is by the simplest operation that can be expected to approximate the contralateral normal ear (Fig. 13).4
Cosman179 concluded the following:1) It seldom is necessary to detach the helical crus from the face.2) It often is the case that more tissue is available for reconstruction of the constricted ear than is initially apparent.3) Whenever possible, one should avoid procedures that add tissue, because they are more complex and therefore prone to complications and skin color mismatch.
Horlock et al.181 concurred with Cosman179 that the deformity designated as type III by Tanzer178 requires autogenous costal cartilage reconstruction as described by Brent.139 The authors suggested a graded sequence of procedures to treat Tanzer type I, IIA, and IIB deformities. A mastoid hitch, in which a postauricular pocket is created and the newly built helix is sutured to the mastoid fascia, is a recommended adjunct to maintain helical elevation and prevent recurrence. With type I deformities, the helical lidding is dissected free on both sides with a postauricular incision and

24
SRPS • Volume 11 • Issue R3 • 2011
Gra
ft
A B C D E
Figure 13. Brent technique for reconstruction of the earlobe with a reverse contoured flap. A, Earlobe defect. B, Auriculomastoid flap outlined. C, Elevated flap hanging as a curtain from the inferior auricular border. D, Flap folded under and sutured. E, Completed earlobe, exaggerated by one-third to allow for shrinkage. (Modified from Brent.4)
Table 3
Tanzer Classification of Constricted Ears and Suggested Correction178
Type Anatomy Correction
I Helical involvement only Detach the folded helix and reattach it in an upright position
IIA Involvement of the helix and scapha with no supplemental skin necessary
Adjust the anterior helix, filet the deformed helix and scapha, and reconstruct the upper pole of the ear with “banner” flaps of cartilage
IIB Involvement of the helix and scapha with supplemental skin needed at auricular margin
Use skin flap from the medial surface of the ear with various methods for expanding the ear cartilage
III Extreme cupping deformity with involvement of the helix, scapha, anti-helix, and conchal wall
Unfurl and use the remnants for the superior and middle thirds, and reconstruct the remainder with contralateral conchal cartilage
Table 4
Suggestions Presented by Cosman for Correction of Constricted Ear Deformities179
Anatomy Correction
Lidding is major problem, no protrusion, height difference <1 cm Direct excision of overhanging helical curl
Lidding, no protrusion, height difference 1−1.5 cm Banner flap or radial incision
Lidding, protrusion, height difference 1−1.5 cm Vertical expansion and correction of prominence (Cosman technique)
Lidding, protrusion, height difference 1.5−2 cm (compression of scapha) Kislov technique to add tissue180

SRPS • Volume 11 • Issue R3 • 2011
25
the cartilage is scored with a scalpel to reproduce the antihelical fold. Type II deformities are also treated by cartilage scoring and mastoid hitch, plus V-Y advancement of the helical root. This releases skin tightness at the anterior helix and allows superior expansion of the cartilaginous framework, with the effect of increasing ear size. For type IIB deformities, the authors recommend additional framework expansion with a double banner flap. The existing skin often is sufficient provided the V-Y advancement and undermining over the mastoid fascia have released the skin tightness. Park182 proposed correction of type I deformities with a simpler technique that elevates a superiorly hinged rectangular or T-shaped cartilage flap from the concha. The flap is bent back on itself and sutured to the lidded helix or scapha. The recoiling force of the flap on the conchal side holds the lidded portion of the helix erect (Fig. 14).4
Al-Qattan183 described an approach for ears with mild to moderate constriction that combines Mustardé suturing and excision of the lidded cartilage. The lopped cartilage margin is excised through a retroauricular transverse incision in the superior portion of the ear; this is in contrast to cartilage expansion procedures. A traditional mastoid hitch suture is used to prevent recurrent lopping. A number of techniques have been proposed to correct type II constriction, including radial cartilage scoring in a fan-like manner for expansion as described by Stephenson.184 Musgrave185 modified the technique presented by Stephenson. A double banner flap was described by Tanzer178 to expand the constricted helix. More recently, Ohjimi et al.186 proposed a double pennant technique for helical elongation and recreation of the anti-helix. The authors’ technique uses composite flaps that minimize skin dissection from the underlying cartilage. The authors reported between 7 and 22 mm of helical rim elongation. Nagata187 described an approach to management of constricted ear deformity. For type I constrictions, Xiaogeng et al.188 dissected the skin envelope off the underlying cartilage to perform V-Y cartilage advancement along the anti-helix, with Mustardé suturing for shaping. The authors advocated two-stage reconstruction for type II deformities, with a 1- to 1.5-cm composite cartilage graft from the contralateral ear (wedge from the upper third of the ear) to the affected ear. Shaping is performed similar to the shaping in their type I corrections in the second stage. For type III deformities, many authors advocate techniques involving new costal cartilage frameworks, as in microtia reconstruction. Xiaogeng et al.189 presented their experience with staged reconstruction of type III constricted ears with mastoid skin tissue expansion and then autogenous rib cartilage graft reconstruction.
STAHL EARStahl ear is a helical rim deformity first reported in the 19th century that currently could be aptly renamed Spock’s ear. The main features are a third
A B
C D
x
xy
y
x
Covering
Figure 14. Davis technique for reconstruction of the lower third of the auricle and earlobe. A, Defect and outline of the lining flap. B, Outline of the cover flap of the fat flap used for fill. C, Lining flap is covered by the cover flap with the fat flap between them. D, Secondary defect is closed by direct approximation. (Modified from Brent.4)

26
SRPS • Volume 11 • Issue R3 • 2011
crus, flat helix, and malformed scaphoid fossa (Fig. 15).147 The condition is much more common among Asians than among other populations.190
Chongchet191 described the classic approach of excision of the aberrant third crus and redraping of the skin. Ferraro et al.192 modified the technique by avoiding an anterior skin incision and using the resected cartilage as a graft to support the reconstruction. Ono et al.193 described a technique of wedge excision of the third crus with helical advancement. Kaplan and Hudson194 proposed a modification that uses a wedge excision of the cartilage and posterior skin only. Both of these techniques resulted in smaller ears. Other surgical techniques for correction include Z-plasty,190 periosteal tether,195 cartilage turnover and rotation,196 and cartilage scoring with cartilage flap transposition.197
Al-Qattan and Hashem198 offered a complete review of their experience with the various techniques, highlighting efficacy and limitations. The authors proposed an alternative approach to Stahl ear reconstruction that involved resection of the abnormal third crus, helical rim reconstruction with the resected third crus cartilage, and anti-helical reconstruction with an ipsilateral conchal cartilage graft.
CRYPTOTIACryptotia is abnormal adherence of the ear
to the temporal skin associated with cartilage malformation in the scapha-antihelix complex and possibly occurring secondary to abnormalities of the intrinsic and extrinsic ear muscles.199,200 The condition is rare among Caucasians but common among Asians (ratio, 1:400). As with microtia, the right ear is affected more often than the left and the deformity is bilateral in approximately 40% of cases.201 Hirose et al.202 developed a classification system in which two categories of cryptotia are described based on the type of cartilage constriction by abnormally developed intrinsic ear muscles: Type I for transverse muscle or superior crus deformity and type II for oblique muscle or inferior crus deformity. Early splinting is successful,203 and when therapy is initiated in a neonate, molding is the preferred method of correction. Later correction requires surgical division of the abnormal muscle(s) with the addition of skin to the deficient retroauricular sulcus. Cartilaginous reconstruction might also be required. Numerous techniques have been proposed, including Z-plasty,204 local and regional skin or subcutaneous flaps,205−216 tissue expansion,193 V-Y advancement flaps,217 and skin grafting.218,219 Cho and Han220 described their technique of a V-Y temporal advancement flap for deepening of the auriculotemporal sulcus and either ear cartilage graft or Medpor for helical rim splinting and stabilization. The authors favor Medpor for greater stability and experienced no exposures in four cases. They noted that more aggressive manipulation of the cartilage is required with greater vertical deficiency. EAR MOLDING AND SPLINTINGIn neonates, many ear deformities can be corrected by splinting because the ear cartilage is soft and malleable,203,221 but in older children and adults, operative correction usually is required. Byrd et al.222 described a series of 488 patients with 831 ears that were treated with external molding. The series included patients with prominent cup ear (373 ears, 45%); lidding or lop ear (224 ears, 27%); mixed ear deformities, all including associated conchal crus (83 ears, 10%); Stahl ear (66 ears, 8%); helical rim abnormalities (58 ears, 7%); and conchal crus (25
Figure 15. Rib cartilages used in total ear construction. 1, synchondritic block used for body of framework; 2, floating rib used for helix; 3, strut used for tragus; 4, extra cartilage wedge to be banked fur use during the elevation procedure. (Reprinted with permission from Brent.147)

SRPS • Volume 11 • Issue R3 • 2011
27
ears, 3%). Ninety percent of patients achieved good to excellent results and avoided surgery. Success increased when therapy was initiated within the first week of life. The authors described use of the EarWell Infant Ear Correction System (Becon Medical Ltd., Tucson AZ) with a two-piece cradle, retractors, and adhesives. They encountered few complications.
OTOPLASTYProminent EarsThe prominent ear has been classically characterized by excessive height of the conchal wall or absence of an antihelical fold (a concha-scapha angle >90°) or both. Madzharov223 defined the protruding ear deformity as a cephalic-auricular angle >34° caused by a flattened antihelix or protrusion of the concha or both. The deformity usually occurs bilaterally. The condition results from embryonic arrest during the final convolutions of the ear, with failure of folding of the antihelix. The “telephone deformity” refers to relative prominence of the upper and lower poles, whereas the “reverse telephone deformity” means excessive prominence of the concha relative to the upper and lower poles.224 These deformities usually occur as postsurgical complications. Frustration with otoplasty techniques has led to an awareness of additional features of prominence: the antihelix, conchal bowl, helical tail, ear lobule, and helical root.225 Otoplasty techniques for the correction of prominent ears can be grouped into operations that involve the following:
• Excision of cartilage• Molding the ear with sutures• Molding the ear with scoring or sculpting
of cartilage• Combination of any of the above
Various techniques are used at the key anatomic locations to correct ear prominence.
HistoryRogers226 noted that the origins of otoplasty were wrongly attributed to Dieffenbach and that it was probably Ely227 in 1881 who first described an
operation to correct prominent ears. Rogers228 also noted that the next milestone in the evolution of otoplasty occurred in 1910, when Luckett described a procedure for the correction of prominent ears that correctly assumed that the protruding ear resulted from an undeveloped or unfolded antihelix. Many of the surgical methods proposed since Luckett’s time are in some way modifications of the operation he described, and most represent attempts at improving the overly sharp antihelical crest and excessively steep recess of the scapha produced by the classic technique.
Surgical GoalsIn an excellent review of techniques for the correction of prominent ears, McDowell7 listed the following basic goals of otoplasty:
• Complete correction of upper third protrusion
• Visibility of the helix beyond the antihelix when viewed from the front
• Smooth and regular helix • Prevention of distortion or decrease in the
depth of the postauricular sulcus • Placement of the ear at the correct
distance from the head and not overly close; the helix-to-mastoid distance should be 10 to 12 mm at the top, 16 to 18 mm in the middle, and 20 to 22 mm in the lower third
• Bilateral symmetry; the difference in helix-to-mastoid distance between sides should be <3 mm
To this list, one should add the following:• Smooth, rounded, correctly placed and
adequately prominent antihelical fold • Helical rim that projects laterally farther
than the lobule229
Timing of SurgeryOtoplasty can be performed in patients of all ages. Many factors should be considered when determining optimal timing for surgery. With

28
SRPS • Volume 11 • Issue R3 • 2011
advanced age, increasing mineralization and calcification of auricular cartilage can make suture suspension or cartilage-scoring techniques unreliable, unpredictable, and/or prone to relapse. Growth concerns arise when performing early childhood otoplasty. Historically, most corrections have been performed when the patient is older than 5 years. Adverse psychosocial interactions for children and adolescents with prominent ears are also important factors to consider. Gosain et al.230 conducted a survey and found that most surgeons perform otoplasty when the patient is older than 5 years. However, their small prospective series of 12 patients underwent otoplasty when they were younger than 4 years. With a mean follow-up duration of 41 months, prominence recurred in one patient (8%). Three patients who underwent unilateral otoplasty did not exhibit any growth discrepancy relative to the contralateral ear up to 63 months postoperatively. Gasques et al.231 examined the psychosocial effects of prominent ears and demonstrated a clear benefit for otoplasty. Several questionnaires, including the Child Behavior Check List, State-Trait Anxiety Inventory for Children, and Children’s Depression Inventory, were administered, and improvement was noted postoperatively for nearly all measures by both teachers and parents. The authors recommended that the optimal age for correction is 6 years. Excisional TechniquesAntihelixRogers228 explained that Luckett excised a crescent-shaped segment of skin and cartilage from the entire vertical length of the ear on its cranial side and sutured the edges of the cartilage to create an antihelical fold (Fig. 16).179
“A crescentic incision is made through the integument opposite to the line of the intended new or reconstructed antihelix. The inscribed integument is removed; the edges of the skin are now dissected free from the cartilage and retracted. A similar crescentic segment is removed from the cartilage, care being exercised in incising and excising the cartilage not to
buttonhole the skin on the external surface of the auricle. The skin and the cartilage are now sutured separately, and it is the method of suturing the cartilage that is emphasized. The cartilage suture is passed from the cranial side from within out-and-back again, care being taken not to perforate the skin on the external surface, then crossed over the excised portion and passed on the other side from within out-and-back again as a Lembert suture, in such a manner that when the suture is drawn tight and tied, not the edges but the sides or flat surfaces of the cartilage will be in apposition. The edges have been turned forwards or outwards to form the antihelix and at the same time the helix is set closer to the cranium, thus diminishing the cephalo-auricular angle. Four or five interrupted sutures are usually enough for the cartilage. A so-called fistula, one-half circle, needle is best for the cartilage. The skin is sutured with horsehair and leaves a very small cicatrix.”228
Conchal CartilageDavis232,233 described the technique of conchal bowl excision at the base of the vertical wall. Using methylene blue dye to create percutaneous transfixion tattoos on the conchal cartilage, the posterior vertical conchal wall is marked at a height of 8 mm. The marks delineate a conchal half-circle, and the conchal bowl (or floor) anteriorly is marked for resection. Through a retroauricular skin incision, the conchal cartilage is exposed and the methylene blue tattoo marks are visualized. An incision is created, connecting these points and the anterior conchal cartilage dissected in a subperichondrial plane. Care is taken to avoid injury to the anterior skin. The entire conchal bowl is excised. The posterior conchal wall remains and is placed passively on the mastoid surface, establishing the new conchal projection. Hinderer et al.44 resected skin and cartilage at different levels of the scapha, concha, and helical arch to avoid notching of the helical rim during reapproximation. The author warned against

SRPS • Volume 11 • Issue R3 • 2011
29
transections of the antihelix or transverse excisions through the superior crus for the same reason. Balogh and Millesi234 studied 77 patients who had undergone surgery for prominent ears with the cartilage excision method to determine whether any growth alterations had occurred and to find out the right timing of the operation. The mean age of patients at the time of surgery was 7.2 years. In every case, surgery had been performed 15 to 25 years previously. The standard ear morphometric variables of the operated patients were compared with those of 200 unoperated control participants. The authors found no difference in retroauricular angle between the surgical group and the control group, suggesting that the surgical objective had been accomplished. The surgical group showed significantly smaller morphological ear length (affected by surgery) and significantly larger morphological ear width (not affected by surgery). The formerly prominent ears were larger than the ears of the control participants in all other
dimensions. The authors concluded that auricular growth does not stop after the cartilage excision method of surgery for prominent ears, that surgery had restored harmony between the width and length of the ear (ear index), and that patient satisfaction was high (74 of 77 patients were satisfied with their outcomes).
EarlobePosterior skin excision of varying shapes has been described for correction of prominent earlobes.235 Dumbbell, fishtail, tennis racket, and wedge excision patterns have commonly been used.
Suturing TechniquesAntihelixMustardé236 described the creation of an antihelical fold with concha-scapha mattress sutures placed on the cranial cartilaginous surface and incorporating the full thickness of the cartilage and perichondrium on the lateral (anterior) surface (Fig. 17).182 With the method presented by Mustardé, the ear is folded back to produce an antihelix, the summit of the fold is marked with ink, and the positions for the mattress sutures are marked on the skin. The mattress suture positions should be at least 7 mm from the summit line, considering that less than that amount will produce too narrow a fold. Because of the curve of the antihelix, the markings on the concave aspect are closer together than those on the convex side. It might therefore be necessary to introduce an additional mattress suture to produce a superior crus, although this seldom is required because both crura usually appear when the ear is folded back. After insertion of a traction suture through the margin of the helix to hold the ear forward, an ellipse of skin approximately 3 to 4 cm × 1 cm is removed from behind the ear on the medial or conchal side of the proposed antihelix. The skin and soft tissues on both sides of the excised area are elevated off the perichondrium with blunt dissection to expose the dye marks. Mustardé used a half-curved needle to insert white silk mattress sutures. The sutures should include the full thickness of the cartilage and the perichondrium on both sides but not any skin on the anterior surface. At that point, the sutures can be temporarily
A
st
b
d
f
a
B
eb
b
b b
d a
be
C
c
ccf´
f
b
D E F G
H
I
J
Figure 16. Kislov technique for correction of the constricted ear. (Modified from Cosman.179)

30
SRPS • Volume 11 • Issue R3 • 2011
tightened and the ear inspected to confirm that the new antihelical fold is satisfactory. Finally, the sutures are tied at a tension that produces an aesthetically pleasing folding of the antihelix. Johnson237 proposed a refinement of the Mustardé suturing technique that places the sutures obliquely to control and shape the curve of the antihelix. Johnson thought that oblique placement of the sutures would better check upper pole prominence, such as telephone deformity, and prevent overfolding of the antihelix.
Conchal BowlConcha-mastoid sutures were described by Furnas238 to reduce the conchal prominence (Fig. 18). Spira and Stal239 described modifications of this technique that involve the addition of a flap of conchal cartilage sutured to the periosteum.
Earlobe and Helical TailProminent earlobes and helical tails (cauda helices) have been a commonly overlooked aspect of ear prominence. Webster240 and Beernink et al.241 emphasized the importance of proper repositioning of the helical tail to correct excessive prominence of the lower third of the ear. Goulian and Conway242 also advocated control of the helical tail as a way of properly positioning the lobule. The cadaveric studies conducted by the authors showed a distinction between the conchal and helical cartilage. They recommended dissection between them and suturing the helical tail to its new position on the concha to help achieve a proper relationship. Spira243 described his technique for dermal-to-mastoid suturing for earlobe repositioning. Gosain and Recinos244 described a modified technique of lobule-to-mastoid sutures, identifying a key point of control for correction of prominent earlobes.
Helical RootA laterally projecting helical root can be repositioned by suturing the medial cartilage to the temporalis fascia, with or without a combined skin excision. Kelley, Hollier, and Stal (Kelley et al.225) described this technique as a Hatch suture.
Cartilage Scoring or Sculpting TechniquesThese operations are based on the observation by Gibson and Davis245 that cartilage tends to curl away from a cut surface. This phenomenon was
Figure 17. Operative technique using a tumbling concha-cartilage flap (TF). (Reprinted with permission from Park.182)
Figure 18. Left, normal ear. Right, Stahl ear deformity.

SRPS • Volume 11 • Issue R3 • 2011
31
later confirmed by Fry,246 who attributed it to “interlocked stresses” that were released by incision of the perichondrium.
AntihelixStenstrom247 applied this principle to an otoplasty procedure for the correction of prominent ears. Stenstrom initially scored the anterior surface of the scapha through a small medial incision near the cauda helicis to produce a helical roll and a satisfactory antihelical fold. He later modified the technique248 to include a postauricular incision and wide undermining to expose the surface of the scapha, where scoring was completed with a “scratching instrument,” which is a procedure that we now call otobrasion (Fig. 19). The degree of scratching or scoring of the anterior surface of the scapha is adjusted to produce the desired amount of curl in the cartilage for an antihelical fold. The postauricular skin is carefully trimmed to effect the final delicate relationship of helix to antihelix. Stenstrom248 did not perform any suturing to create the antihelical fold. Stenstrom248 suggested marginal excision of a portion of the horizontal helix as a solution to the problem of continued protrusion of the upper pole of the ear. For persistent prominence of the lobule, he recommended crosswise scratching of the anterior surface of the helical tail. Chongchet191 described a technique of anterior scoring for antihelical reconstruction in 1963, the same year the technique presented by Stenstrom was published. Crikelair and Cosman249 also reported a similar approach that involves an incision through the posterior helix and anterior scoring of the scapha.
Weinzweig et al.250 studied the histological effects of antihelical cartilage scoring and found that a fibrocartilaginous layer develops that promotes and stabilizes cartilage bending away from the scored surface. Di Mascio and Castagnetti29 described use of a dermabrader for “burring” the anterior surface of the antihelix. The authors advocated this technique as more precise and safer for cartilage weakening, compared with parallel scoring. Karacalar et al.251 described a “subcision” technique for cartilage scoring. An 18-gauge hypodermic needle is inserted percutaneously over the antihelix, and perichondrial scoring is accomplished subdermally. Fritsch252 described his technique for “incisionless” otoplasty, which uses similar antihelical scoring with a hypodermic needle and percutaneous mattress suturing. Recent interest has been shown in other experimental technologies for cartilage shaping. Use of lasers of varying wavelengths for cartilage reshaping have been proposed since 1993. Mordon et al.253 described the use of a 1.54-mm erbium:glass laser for ear cartilage reshaping in 12 rabbit ears. No thermal skin injury was observed. After an initial tendency for shape recovery (at 1 week), stable alteration was observed for up to 6 weeks. Histological examination showed chondrocytic proliferation on the treated surface of the cartilage and thickening of the cartilage layer.
Combined TechniquesOtoplasty procedures that combine excision, suturing, and cartilage-scoring techniques avoid some of the disadvantages of each method and often produce the best aesthetic result. For example, because cartilage scoring of the anterior surface of the ear tends to produce sharp edges, a judicious blend of conservative anterior scoring and posterior excision and suturing might provide the best final ear shape and position. Tanzer254 described his classic otoplasty technique in 1962. Several authors have described notable variations of the basic procedures.222,255–257 Baker and Converse258 reported their 20-year experience with otoplasty. Madzharov222 described a method for the correction of prominent ears that is based on measurements of ear-to-skull distances
A B C
Figure 19. Stenstrom otoplasty technique.

32
SRPS • Volume 11 • Issue R3 • 2011
and the size of the ears. The amount of setback in each case is established preoperatively from normal anthropometric data derived from an Eastern European population. The antihelix is shaped by two derma-subcutaneous perichondrial flaps; the conchal spring is eased by means of a wedge-shaped cartilage excision in the area of the isthmus of the cartilage or the auricle, and the residual protrusion of the lobule is corrected by Z-plasty. Technical details of the operation are presented in the article, which merits further study by surgeons planning setback otoplasty. Hinderer et al.255 combined anterior cartilage scratching, posterior mattress sutures along the antihelical fold, trimming of the tail of the helix, thinning of the antitragus, and a double-spindle skin excision along the posterior medial surface. Pitanguy et al.256 created an “island” of cartilage on the anterior surface of the ear that is pushed forward to resemble a smooth antihelical fold by suturing the edges of the wound after resection of a generous ellipse of skin from the posterior surface. Kaye257 combined Mustardé-type sutures and Stenstrom-type scoring through limited incisions to create an antihelical fold. Chait and Nicholson259 reported their extensive experience (973 ears) with a “universal” technique for the correction of all types of prominent ears. Their procedure combines posterior skin excision, cartilage transection, anterior skin elevation off the concha, auricular cartilage scoring, a single mattress suture to anchor the new concha-scapha angle in place, and variable amounts of cartilage rotation and excision as needed. Commenting on the article by Chait and Nicholson, Stal260 expressed his preference for an algorithmic approach to otoplasty that uses combinations of different established techniques that specifically address different patients’ needs (Fig. 20).261 The algorithm addresses three basic anatomic abnormalities of the prominent ear deformity: 1) a deep concha with a prominent posterior wall; 2) an unfolded antihelix with a scaphoconchal angle >90°; and 3) a prominent lobule after setback. Spira262 presented a 30-year retrospective review of his experience with >200 otoplasties. The
timing, indications, and operative technique are described in detail. Postoperative care and early and late complications are also discussed. This article should be read by any surgeon who is planning to perform setback otoplasty. Graham and Gault263 described endoscopic-assisted otoplasty involving posterior scoring and scapha and mastoid suture. Use of the endoscope eliminates the need for a postauricular incision and hence the possibility of hypertrophic scar or keloid. The authors’ classification of prominent ears guides patient selection for this technique. Burstein155 presented a report of his 10-year experience with a cartilage-sparing technique that involves modified Mustardé suturing, anterior scoring, conchal bowl scoring, and concha-mastoid suturing. An 8% relapse rate was noted. Bauer et al.264 discussed use of anterior chondrocutaneous resection of the conchal bowl as the preferred method of treating conchal hypertrophy. The authors described a combined otoplasty technique for their series of 47 patients (87 ears). Three patients experienced early relapse of the upper pole caused by failure of the antihelical suturing; they reported no late recurrent prominence. Anterior chondrocutaneous resection did not result in any unsatisfactory scarring and
A B
Figure 20. Mustardé otoplasty technique.

eliminated any potential for skin fold redundancy in the conchal bowl. Peker and Celiköz265 described an otoplasty technique that involves incising the scapha to access the anterior cartilage surface, anterior scoring to weaken the cartilage, and posterior rolling of the free edge of cartilage to recreate an antihelical fold. Kelley, Hollier, and Stal (Kelley et al.225) described their algorithmic approach to otoplasty, which focuses primarily on cartilage preservation rather than on cartilage excision. Janis, Rohrich, and Gutowski ( Janis et al.266) provided an alternative summary and algorithm for correction of the prominent ear. A summary of various otoplasty techniques is presented in Table 5.
Other ConceptsNicoletis and Guerin-Surville267 were the first to describe the posterior auricular muscle as it relates to the pathogenesis of ear protrusion. Smith268 and Smith and Takashima269 also emphasized the importance of the muscle in ear protrusion, proposing that neuromuscular dysfunction and/or deficiency was the cause for prominence. Guyron and DeLuca270 found a linear correlation of the muscle length and the degree of ear protrusion.
The authors discussed the three main causes for prominence as being conchal valgus with a cranium-auricle angle >40°, lack of antihelical fold, and, more rarely, conchal hypertrophy. For conchal valgus, myoplasty of the posterior auricular muscle was proposed as an adjunctive maneuver in otoplasty or even an isolated procedure with simple conchal valgus deformity. Scuderi et al.271 described a technique for repositioning the posterior auricular muscle as an adjunct to otoplasty. The muscle is raised as a chondromuscular flap (distal cartilage paddle around the insertion at the ponticulus), advanced peripherally, and secured to the antihelical cartilage to reduce prominence. The authors reported no relapse among 55 patients. Shinohara et al.272 performed CT of randomly selected heads to examine correlation of prominence to selected relevant auricular angles: scapha-triangular fossa angle, concha cymba-triangular fossa angle, and scapha-concha angle. Based on these data, the authors concluded that the deformity of the inferior crus has a more direct correlation to prominence than does the superior crus. The authors proposed reconstruction of the inferior crus for correction of prominent ears.
SRPS • Volume 11 • Issue R3 • 2011
33
Table 5
Summary of Otoplasty Techniques
Anatomical Site Technique Study
Antihelical fold Concha-scaphal suture technique Mustardé277
Antihelical scoring or otobrasion Stenstrom248
Antihelical excision Luckett (Rogers228)
Conchal bowl Concha-mastoid suture technique Furnas238
Conchal bowl excision Davis232,233
Helical tail Suture repositioning to concha Goulian and Conway242
Concha and/or skin excision and suture repositioning Webster240
Lobule Posterior skin excision: dumbbell, fishtail, tennis racket Lavy and Sterns235
Lobule to mastoid suture techniqueSpira243;Gosain and Recinos244
34
SRPS • Volume 11 • Issue R3 • 2011
Late Results and ComplicationsThe most common unsatisfactory results of otoplasty are deformities occurring secondary to surgery, such as the following:
• Sharp ridges along the antihelical fold• Vertical post (lack of normal curvature of
the superior crus)• Irregular contours• Antihelical roll too small or malpositioned• Excessively large scapha• Narrow ear• Telephone deformity• Hidden helix • Buckled helix• External auditory canal stenosis
or distortion• Conchal skin redundancy• Hypertrophic scarring or keloids• Prominent tragus• Overcorrection• Obliterated or shallow postauricular sulcus• Asymmetry
Recurrent prominence is also a common problem after otoplasty. Many authors have advocated combining techniques to minimize relapse. Corchado and Infante273 thought that anterior scoring alone was not sufficient for durable antihelix reconstruction, especially in adults and those with thick cartilages. Similarly, Spira262 reported that Mustardé’s suture technique alone was insufficient for durable correction in adults. He subsequently proposed performing Stenstrom-type anterior scoring adjunctively. Webster and Smith224 provided a detailed account of the long-term results of otoplasty and its many potential associated complications. Their review is strongly recommended for additional reading on this subject. Elliott274 examined the unsatisfactory results of otoplasty, which he separated into an early group (complications) and a late group (undesirable sequelae). Complications include pain, bleeding, pruritus, infection, chondritis, and necrosis. Undesirable sequelae include patient dissatisfaction,
unsightly scars, suture problems, and dysesthesias occurring later. Tan275 compared the incidence and severity of complications resulting from posterior suturing techniques with those of anterior scoring procedures. Patient satisfaction with the aesthetic results was no different between the Mustardé and Stenstrom otoplasties. The author found that a substantially large number of patients treated by the posterior suture method of Mustardé required reoperation: 24% versus 10% with the anterior scoring technique. Numerous complications were specific to the Mustardé technique, particularly relating to the presence of white silk stitches that tended to cause sinus tract and wound infections (15%). In a 10-year survey of his results with 264 ears, Mustardé276 listed several potential problems with the otoplasty procedure that bears his name, such as kinks in the antihelix, sutures cutting out, sinus tract formation, recurrence of prominence, and horizontal projection of the lobule and antitragus. He also provided tips for avoiding them. A subsequent review of the results in 600 ears treated during a 20-year period revealed only six cases of sinus tract formation and no suture rejection.277 Most remarkably, only 10 ears required reoperation for recurrent prominence. The Mustardé otoplasty has not been as successful in other hands. The initial enthusiasm that Spira and Hardy278 expressed for the Mustardé method was tempered by two factors: the large number of relatively minor complications encountered and the high rate of partial recurrence of the deformity. Heftner279 surveyed 167 patients who had undergone Stenstrom otoplasties and found that 40% declared themselves very satisfied, 49% satisfied, and 4% fairly satisfied. Symmetry and setting were considered to be good in 71% of cases, whereas 4% had negligible incomplete correction, 19% had slight overcorrection, and 6% had marked overcorrection. A round natural antihelix was noted in 81% of patients and a sharp antihelix in 14%. Isolated small nodules occurred in 5% of cases, and 15% were considered to be overcorrected. Calder and Naasan280 reviewed their

SRPS • Volume 11 • Issue R3 • 2011
35
experience with 562 otoplasties performed with the anterior scoring technique. The most common complication was residual deformity (8%). In order of decreasing frequency, the authors also reported infection, keloid and/or hypertrophic scarring, hemorrhage, and anterior skin necrosis. Further analysis revealed that the cause of residual deformity was primarily a fault in the design of the procedure or in the execution of the technique. The authors stated that most of these complications are avoidable. Messner and Crysdale281 reviewed their experience with a combination technique of Mustardé and Furnas sutures in 31 patients who were followed for a minimum of 1 year (average follow-up duration, 3.7 years). Regarding recurrence of the deformity, the authors reported that at the time of evaluation, one-third of the ears had returned to their original position, one-third remained in their immediately postoperative position, and one-third were between the pre- and postoperative positions. Walter and Nolst Trenité282 presented a discussion of the management of post-otoplasty deformities. Common sequelae include obliterated postauricular sulci, irregularities of the antihelical fold or a sharp antihelical fold, telephone deformities, protruding lobules, obliterated external auditory canals, and post-perichondritis deformities. The appropriate course of action for addressing each of these deformities is detailed in the article. Firmin et al.283 presented a series of 49 patients with severe deformities resulting from otoplasty. Conchal cartilage grafts are useful for minor contour irregularities, but costal cartilage is recommended for deformities involving more than 25% of the ear or more than two planes of the normal folds. Limandjaja et al.284 provided a comprehensive review of published series of otoplasties. Complications were specifically examined, and the authors lamented the lack of uniformity in reporting.
EARLOBE REDUCTIONAccording to Loeb,285 the earlobe is divided into two components separated by the “otobasion
inferius” (OI), which is the anterior implantation of the earlobe to the cheek skin. The distance from the inter-tragal notch to the OI (cephalic segment) typically is 1 to 2.5 cm. The caudal segment is defined as the distance from the OI to the subaurale (inferiormost point of the earlobe). Loeb advocated earlobe reduction if the cephalic segment exceeds 2.0 cm in length. McKinney et al.286 determined that the average lobule height is 18 mm (caudal segment) and advocated earlobe reduction as an adjunct to rhytidectomy when the lobule:total ear height ratio exceeds 33%. Mowlavi et al.287 discussed the incidence of earlobe ptosis and pseudoptosis and proposed a classification system based on the measurements defined by Loeb285 and the relationship between the “attached” cephalic and “free” caudal segments (Table 6). The authors found that the average height of the cephalic segment was 11.1 mm and of the caudal segment was 7.15 mm. The caudal segment was found to exhibit increasing ptosis with advanced age; the average height increased to 10 mm in the 8th decade of life. In their study, all patients had caudal segment heights of 15 mm or less (Grade III ptosis or less). The authors determined that pseudoptosis was defined as a cephalic segment height >15 mm. Mowlavi et al.288 also proposed an algorithm for correction of ptotic and pseudoptotic earlobes and described their surgical technique of an anterior wedge excision and reduction. El Kollali289 proposed an alternative classification of normal earlobe morphology depending on the angle of the earlobe-cheek junction: acute, earlobe is not attached to the cheek; right angle, neutral relative to the cheek; or obtuse angle, adherent to the cheek. The author disputed the “ideal” aesthetic of a free, unattached earlobe relative to the cheek and determined that approximately one-third of the population has the “adherent” earlobe morphology and that this should be considered a normal variant.
TISSUE ENGINEERINGMost techniques for total ear reconstruction have relied on usage of autogenous costal cartilage grafts

36
SRPS • Volume 11 • Issue R3 • 2011
or alloplastic materials to construct a framework to be inserted under a skin envelope. Recent advances in tissue engineering have propelled the concept of using cellular constructs as an alternative source for an ear-shaped framework. The basic elements of construction include cells, cell-carrier, scaffolding type, and technique (e.g., pre-fabrication, injection molding, external molding, in vitro, in vivo). Kim et al.290 and Vacanti and colleagues (Shieh et al.291) engineered predetermined shapes of cartilage by using techniques for cell transplantation onto biodegradable polymers. Cao and Vacanti and colleagues (Cao et al.292) later created an ear framework that was a polymer-cell construct that used articular cartilage. Chang and Vacanti and colleagues (Chang et al.293) examined the feasibility of an injection molding technique for cartilage graft tissue engineering. Alginate implants were seeded with autologous chondrocytes and injected into Silastic molds (Dow Corning). They were removed after they had conferred reasonable stability and shape and were then implanted subcutaneously in
sheep. Histological examination 6 months later showed excellent cartilage formation and three-dimensional shape retention. The authors showed the effectiveness and simplicity of an injection molding technique for large implants without exhibiting central graft necrosis. Ting et al.294 fabricated various cartilage shapes in vitro by using human costal chondrocytes and fibrin glue. These early attempts at auricular cartilage construction yielded small and inflexible frameworks that lacked perichondrium and often could not be constructed to the dimension of a human ear. Xu and Yaremchuk and colleagues (Xu et al.295) were successful in constructing flexible constructs by using swine chondrocytes engineered with lyophilized perichondrium. The authors reviewed previous attempts at constructing a stable framework that can withstand the external soft-tissue tension or avoid resorption. Previously published methods have included use of degradable or nondegradable endoskeletal scaffolds, prefabrication molding, or injection
Table 6
Classification of Earlobe Ptosis and Designation of Pseudoptosis Based on Analysis of Preferred Otobasion Inferius to Subaurale and Intertragal Notch to Otobasion Inferius Distances287
Classification Segment (mm)
Ptosis grade Free caudal segment (otobasion inferius to subaurale distance)
0 0
I 1−5
II 6−10
III 11−15
IV 16−20
V >20
Pseudoptosis Attached cephalic segment (intertragal notch to otobasion inferius distance)
Abnormal >15
Normal ≤15

SRPS • Volume 11 • Issue R3 • 2011
37
molding techniques. In the study by Xu et al., large ear-shaped constructs were implanted in athymic mice that withstood the soft-tissue tension and maintained projection and shape. In a rat model, Neumeister et al.296 showed that transposing a vascular pedicle to a subcutaneously placed silicone block creates a vascularized capsule over the mold. The capsules were filled with chondrocytes and a fibrin glue carrier in the experimental group. Good viability of the new construct via an extrinsic capsular blood supply was shown, but shape was not reliably maintained with the capsule alone. When an external mold was retained for at least 4 weeks, the construct began maintaining its shape. Longer term evaluation of the construct shape was not undertaken in that study. The authors concluded that transposing a vascular pedicle will not only incorporate itself to a capsule but will become the dominant blood supply to it. This method of prefabrication showed development of an intrinsic vascularity to an engineered construct that could be transferred as a pedicled or free flap. Ciorba and Martini,297 in 2006, reviewed the status of tissue engineering and stem cells as it relates to auricular reconstruction. The authors identified several key components under investigation, including type of scaffolding, source cells, suitable animal models, and stability
of engineered tissues. Sterodimas and Pitanguy and colleagues (Sterodimas et al.298) provided an updated review in 2009.
EAR TRANSPLANTATIONBecause of the complex morphology and tissue characteristics of the ear, composite allograft transplantation might be an emerging alternative to autogenous or alloplastic reconstructions. Recent advances in transplant immunology have spurred interest in composite tissue transplantation of the face and hand. Ulusal and Wei and colleagues (Ulusal et al.299) described auricle allotransplantation in rats. Using a cyclosporine-based immunosuppressive regimen, graft survival was 100% at 30 days. The authors proposed their model as a basis for further immunological studies. Based on human cadaveric dye-injection studies, Ulusal et al.300 further showed that adequate auricular transplant perfusion would require both superficial temporal and posterior auricular arterial systems, suggesting that an external carotid artery pedicle could therefore be used. A successful cephalo-cervical composite tissue allograft transplant including two ears was performed secondary to radical resection of malignant melanoma using a tacrolimus and mycophenolate mofetil regimen with steroid adjuvant.301

38
SRPS • Volume 11 • Issue R3 • 2011
REFERENCES1. Allison GR. Anatomy of the external ear. Clin Plast Surg 1978;5:419–422.
2. Park C, Lineaweaver WC, Rumly TO, Buncke HJ. Arterial supply of the anterior ear. Plast Reconstr Surg 1992;90:38–44.
3. Erdmann D, Bruno AD, Follmar KE, Stokes TH, Gonyon DL, Marcus JR. The helical arcade: Anatomic basis for survival in near-total ear avulsion. J Craniofac Surg 2009;20:245–248.
4. Brent B. Reconstruction of the auricle. In, McCarthy JG (ed): Plastic Surgery. vol 3. Philadelphia: WB Saunders; 1990:2094–2152.
5. Songcharoen S, Smith RA, Jabaley ME. Tumors of the external ear and reconstruction of defects. Clin Plast Surg 1978;5:447–457.
6. Bailin PL, Levine HL, Wood BG, Tucker HM. Cutaneous carcinoma of the auricular and periauricular region. Arch Otolaryngol 1980;106:692–696.
7. McDowell AJ. Goals in otoplasty for protruding ears. Plast Reconstr Surg 1968;41:17–27.
8. Farkas LG. Anthropometry of normal and anomalous ears. Clin Plast Surg 1978;5:401–412.
9. Skiles MS, Randall P. The aesthetics of ear placement: An experimental study. Plast Reconstr Surg 1983;72:133–140.
10. Broadbent TR, Mathews VL. Artistic relationships in surface anatomy of the face: Application to reconstructive surgery. Plast Reconstr Surg (1946) 1957;20:1–17.
11. Tolleth H. Artistic anatomy, dimensions, and proportions of the external ear. Clin Plast Surg 1978;5:337–345.
12. Farkas LG. Anthropometry of the Head and Face. 2nd ed. New York: Raven Press; 1994.
13. Brucker MJ, Patel J, Sullivan PK. A morphometric study of the external ear: Age- and sex-related differences. Plast Reconstr Surg 2003;112:647–652.
14. Converse JM. Reconstruction of the auricle: I. Plast Reconstr Surg Transplant Bull 1958;22:150–163.
15. Tanzer RC. An analysis of ear reconstruction. Plast Reconstr Surg 1963;31:16–30.
16. Tanzer RC. Total reconstruction of the external ear. Plast Reconstr Surg Transplant Bull 1959;23:1–15.
17. Mladick RA. Salvage of the ear in acute trauma. Clin Plast Surg 1978;5:427–435.
18. Gingrass RP, Pickrell KL. Techniques for closure of conchal and external auditory canal defects. Plast Reconstr Surg 1968;41:568–571.
19. Millard DR. The crane principle for the transport of subcutaneous tissue. Plast Reconstr Surg 1969;43:451–462.
20. Brent B. The acquired auricular deformity: A systematic approach to its analysis and reconstruction. Plast Reconstr
Surg 1977;59:475–485.
21. Antia NH, Buch VI. Chondrocutaneous advancement flap for the marginal defect of the ear. Plast Reconstr Surg 1967;39:472–477.
22. Gorney M, Murphy S, Falces E. Spliced autogenous conchal cartilage in secondary ear reconstruction. Plast Reconstr Surg 1971;47:432–437.
23. Park C, Chung S. A single-stage two-flap method for reconstruction of partial auricular defect. Plast Reconstr Surg 1998;102:1175–1181.
24. Bialostocki A, Tan ST. Modified Antia-Buch repair for full-thickness upper pole auricular defects. Plast Reconstr Surg 1999;103:1476–1479.
25. Zenn MR. Helical advancement with a posterior auricular pull-through flap: A technique for reconstruction of combined helical and scaphal defects. Aesthetic Plast Surg 1999;23:131–133.
26. Fata JJ. Composite chondrocutaneous advancement flap: A technique for the reconstruction of marginal defects of the ear. Plast Reconstr Surg 1997;99:1172–1175.
27. Dujon DG, Bowditch M. The thin tube pedicle: A valuable technique in auricular reconstruction after trauma. Br J Plast Surg 1995;48:35–38.
28. Ellabban MG, Maamoun MI, Elsharkawi M. The bi-pedicle post-auricular tube flap for reconstruction of partial ear defects. Br J Plast Surg 2003;56:593–598.
29. Di Mascio D, Castagnetti F. Tubed flap interpolation in reconstruction of helical and ear lobe defects. Dermatol Surg 2004;30:572–578.
30. Ramirez OM, Heckler FR. Reconstruction of nonmarginal defects of the ear with chondrocutaneous advancement flaps. Plast Reconstr Surg 1989;84:32–40.
31. Ladocsi L. Perforator-preserving chondrocutaneous rotation flap reconstruction of auricular defects. Plast Reconstr Surg 2003;112:1566–1572.
32. Ohsumi N, Iida N. Ear reconstruction with chondrocutaneous postauricular island flap. Plast Reconstr Surg 1995;96:718–720.
33. Park C, Shin KS, Kang HS, Lee YH, Lew JD. A new arterial flap from the postauricular surface: Its anatomic basis and clinical application. Plast Reconstr Surg 1988;82:498–505.
34. Dean Ferrer A, Alamillos Granados FJ, Vélez García-Nieto A, Fernández Sanromán J. Reconstruction of the scaphoid fossa of the ear after tumor resection with a retroauricular flap. Br J Plast Surg 1994;47:285–287.
35. Talmi YP, Horowitz Z, Bedrin L, Kronenberg J. Auricular reconstruction with a postauricular myocutaneous island flap: Flip-flop flap. Plast Reconstr Surg 1996;98:1191–1199.
36. Crikelair GF. A method of partial ear reconstruction for

SRPS • Volume 11 • Issue R3 • 2011
39
avulsion of the upper portion of the ear. Plast Reconstr Surg (1946) 1956;17:438–443.
37. Orticochea M. Reconstruction of partial losses of the auricle. Plast Reconstr Surg 1970;46:403–405.
38. Davis J. Reconstruction of the upper third of the ear with a chondrocutaneous composite flap based on the crus helix. In, Tanzer RC, Edgerton MT (ed): Symposium on Reconstruction of the Auricle. St. Louis: CV Mosby; 1974:247.
39. Yotsuyanagi T, Nihei Y, Sawada Y. Reconstruction of defects involving the upper one-third of the auricle. Plast Reconstr Surg 1998;102:988–992.
40. Yoshimura K, Nakatsuka T, Ichioka S, Kaji N, Harii K. One-stage reconstruction of an upper part defect of the auricle. Aesthetic Plast Surg 1998;22:352–355.
41. Dagregorio G, Darsonval V. Peninsular conchal axial flap to reconstruct the upper or middle third of the auricle. Dermatol Surg 2005;31:350–355.
42. Tanzer RC. Congenital deformities of the auricle. In, Converse JM (ed): Reconstructive Plastic Surgery. 2nd ed. Philadelphia: WB Saunders; 1977:1671–1719.
43. Lewin ML. Reconstruction of the helix with a postauricular flap. Plast Reconstr Surg (1946) 1950;5:432–440.
44. Hinderer UT, del Rio JL, Fregenal FJ. Macrotia. Aesthetic Plast Surg 1987;11:81–85.
45. Mellette JR Jr. Ear reconstruction with local flaps. J Dermatol Surg Oncol 1991;17:176–182.
46. Preaux J. A simple procedure for reconstruction of the lower part of the auricle [in French]. Ann Chir Plast 1971;16:60–62.
47. Brent B. Earlobe reconstruction with an auriculo-mastoid flap. Plast Reconstr Surg 1976;57:389–391.
48. Davis JE. On auricular reconstruction. Int Microform J Aesthet Plast Surg Otoplasty 1972:1.
49. Aguilar EF III. Ear reconstruction. Clin Plast Surg 2004;31:87–91.
50. Cordova A, D’Arpa S, Moschella F. An innervated retroauricular skin flap for total ear lobule reconstruction. Br J Plast Surg 2003;56:818–821.
51. Sleilati F. Immediate earlobe reconstruction with double-crossed skin flaps. J Plast Reconstr Aesthet Surg 2006;59:1003–1005.
52. Masson JK. A simple island flap for reconstruction of concha-helix defects. Br J Plast Surg 1972;25:399–403.
53. Renard A. Postauricular flap based on a dermal pedicle for ear reconstruction. Plast Reconstr Surg 1981;68:159–165.
54. Azaria R, Amir A, Hauben DJ. Anterior conchal reconstruction using a posteroauricular pull-through transpositional flap. Plast Reconstr Surg 2004;113:2071–2075.
55. Turan A, Turkaslan T, Kul Z, Isler C, Ozsoy Z. Reconstruction of the anterior surface of the ear using a postauricular pull-through neurovascular island flap. Ann Plast Surg 2006;56:609–613.
56.Adler N, Azaria R, Ad-El D. Tragus reconstruction after tumor excision with preauricular folded flap. Dermatol Surg 2007;33:723–726.
57. Adler N, Ad-El D, Azaria R. Reconstruction of nonhelical auricular defects with local flaps. Dermatol Surg 2008;34:501–507.
58. Boo-Chai K. The cleft earlobe. Plast Reconstr Surg Transplant Bull 1961;28:681–688.
59. Effendi SH. Reconstruction of the middle-aged torn earlobe: A new method. Br J Plast Surg 1988;41:174–176.
60. Fearon J, Cuadros CL. Cleft earlobe repair. Ann Plast Surg 1990;24:252–257.
61. Attalla MF. Congenital earlobe cleft: A new technique for repair. Br J Plast Surg 1990;43: 223–225.
62. Kurihara K. Congenital deformities of the external ear. In, Cohen M (ed): Mastery of Surgery: Mastery of Plastic and Reconstructive Surgery. vol 1. Boston: Little, Brown; 1994:776–799.
63. Pardue AM. Repair of torn earlobe with preservation of the perforation for an earring. Plast Reconstr Surg 1973;51:472–473.
64. Elsahy NI. Reconstruction of the cleft earlobe with preservation of the perforation for an earring. Plast Reconstr Surg 1986;77:322–324.
65. Lee PK, Ju HS, Rhie JW, Ahn ST. Two flaps and Z-plasty technique for correction of longitudinal ear lobe cleft. Br J Plast Surg 2005;58:573–576.
66. Agarwal R, Chandra R. A new technique for repair of acquired split-ear-lobe deformity: The free conchal cartilage sandwich graft. J Plast Reconstr Aesthet Surg 2010;63:499–505.
67. Miller GD, Anstee EJ, Snell JA. Successful replantation of an avulsed scalp by microvascular anastomosis. Plast Reconstr Surg 1976;58:133–136.
68. Nahai F, Hurteau J, Vasconez LO. Replantation of an entire scalp and ear by microvascular anastomosis of only one artery and one vein. Br J Plast Surg 1978;31:339–342.
69. Nahai F, Hayhurst JW, Salibian AH. Microvascular surgery in avulsive trauma to the external ear. Clin Plast Surg 1978;5:423–426.
70. Pennington DG, Lai MF, Pelly AD. Successful replantation of a completely avulsed ear by microvascular anastomosis. Plast Reconstr Surg 1980;65:820–823.
71. Trovato MJ, Agarwal JP. Succesful replantation of the ear as a venous flap. Ann Plast Surg 2008;61:164–168.

40
SRPS • Volume 11 • Issue R3 • 2011
72. Jenkins AM, Finucan T. Primary nonmicrosurgical reconstruction following ear avulsion using the temporoparietal fascial island flap. Plast Reconstr Surg 1989;83:148–152.
73. Sućur D, Ninković M, Marković S, Babović S. Reconstruction of an avulsed ear by constructing a composite free flap. Br J Plast Surg 1991;44:153–154.
74. Musgrave RH, Garrett WS Jr. Management of avulsion injuries of the external ear. Plast Reconstr Surg 1967;40:534–539.
75. McDowell F. Successful replantation of a severed half ear. Plast Reconstr Surg 1971;48:281–283.
76. Salyapongse A, Maun LP, Suthunyarat P. Successful replantation of a totally severed ear. Plast Reconstr Surg 1979;64:706–707.
77. Lewis EC II, Fowler JR. Two replantations of severed ear parts. Plast Reconstr Surg 1979;64:703–705.
78. Mladick RA, Horton CE, Adamson JE, Cohen BI. The pocket principle: A new technique for the reattachment of a severed ear part. Plast Reconstr Surg 1971;48:219–223.
79. Steffen A, Katzbach R, Klaiber S. A comparison of ear reattachment methods: A review of 25 years since Pennington. Plast Reconstr Surg 2006;118:1358–1364.
80. Brent B, Byrd HS. Secondary ear reconstruction with cartilage grafts covered by axial, random, and free flaps of temporoparietal fascia. Plast Reconstr Surg 1983;72:141–152.
81. Brent B, Upton J, Acland RD, Shaw WW, Finseth FJ, Rogers C, Pearl RM, Hentz VR. Experience with the temporoparietal fascial free flap. Plast Reconstr Surg 1985;76:177–188.
82. Nakai H. Reconstruction of microtia with a contour-accentuated framework and supplemental coverage. Plast Reconstr Surg 1986;78:604–609.
83. Rose EH, Norris MS. The versatile temporoparietal fascial flap: Adaptability to a variety of composite defects. Plast Reconstr Surg 1990;85:224–232.
84. Zhou G, Teng L, Chang HM, Jing WM, Xu J, Li SK, Zhuang HX. Free prepared composite forearm flap transfer for ear reconstruction: Three case reports. Microsurgery 1994;15:660–662.
85. Jones SE, Mahendran S. Interventions for acute auricular hematoma. Cochrane Database Syst Rev 2004;2:CD004166.
86. Giles WC, Iverson KC, King JD, Hill FC, Woody EA, Bouknight AL. Incision and drainage followed by mattress suture repair of auricular hematoma. Laryngoscope 2007;117: 2097–2099.
87. Ghanem T, Rasamny JK, Park SS. Rethinking auricular trauma. Laryngoscope 2005;115:1251–1255.
88. Ohlsén L, Skoog T, Sohn S. Pathogenesis of cauliflower
ear: An experimental study in rabbits. Scand J Plast Reconstr Surg 1975;9:34–39.
89. Giffin CS. Wrestler’s ear: Pathophysiology and treatment. Ann Plast Surg 1992;28:131–139.
90. Melnick M, Myrianthopoulos NC, Paul NW. External ear malformations: Epidemiology, genetics and natural history. Birth Defects Orig Artic Ser 1979;15:1–140.
91. Converse JM. Construction of the auricle in unilateral congenital microtia. Trans Am Acad Ophthalmol Otolaryngol 1968;72:995–1013.
92. Grabb WC. The first and second branchial arch syndrome. Plast Reconstr Surg 1965;36:485–508.
93. Kaseff LG. Investigation of congenital malformations of the ears with tomography. Plast Reconstr Surg 1967;39:282–286.
94. Rogers BO. Microtia, lop, cup and protruding ears: Four directly inheritable deformities? Plast Reconstr Surg 1968;41:208–231.
95. Tanzer RC. Total reconstruction of the auricle: The evolution of a plan of treatment. Plast Reconstr Surg 1971;47:523–533.
96. Bennun RD, Mulliken JB, Kaban LB, Murray JE. Microtia: A microform of hemifacial microsomia. Plast Reconstr Surg 1985;76:859–865.
97. Figueroa AA, Friede H. Craniovertebral malformations in hemifacial microsomia. J Craniofac Genet Dev Biol Suppl 1985;1:167–178.
98. Jahrsdoerfer RA. Congenital ear atresia. In, Tanzer RC, Edgerton MT (ed): Symposium on Reconstruction of the Auricle. vol 10. St. Louis, CV Mosby, 1974:150–159.
99. Schuknecht HF. Reconstructive procedures for congenital aural atresia. Arch Otolaryngol 1975;101:170–172.
100. Kountakis SE, Helidonis E, Jahrsdoerfer RA. Microtia grade as an indicator of middle ear development in aural atresia. Arch Otolaryngol Head Neck Surg 1995;121:885–886.
101. Gill NW. Congenital atresia of the ear: A review of the surgical findings in 83 cases. J Laryngol Otol 1969;83:551-587.
102. Fukuda O. Discussion of congenital deformities of the auricle. In, Tanzer RC, Edgerton MT (ed): Symposium on Reconstruction of the Auricle. vol 10. St. Louis, CV Mosby, 1974.
103. Aguilar EF III. Auricular reconstruction of congenital microtia (grade III). Laryngoscope 1996;106[suppl 82]:1–26.
104. Granström G, Bergström K, Tjellström A. The bone-anchored hearing aid and bone-anchored epithesis for congenital ear malformations. Otolaryngol Head Neck Surg 1993;109:46–53.
105. Håkansson B, Tjellström A, Carlsson P. Percutaneous

SRPS • Volume 11 • Issue R3 • 2011
41
vs. transcutaneous transducers for hearing by direct bone conduction. Otolaryngol Head Neck Surg 1990;102:339–344.
106. Bellucci RJ. Congenital auricular malformations: Indications, contraindications, and timing of middle ear surgery. Ann Otol Rhinol Laryngol 1972;81:659–663.
107. Derlacki EL. The role of the otologist in the management of microtia and related malformation of the hearing apparatus. Trans Am Acad Ophthalmol Otolaryngol 1968;72:980–994.
108. Aguilar EA III, Jahrsdoerfer RA. The surgical repair of congenital microtia and atresia. Otolaryngol Head Neck Surg 1988;98:600–606.
109. Jahrsdoerfer RA, Yeakley JW, Aguilar EA III, Cole RR, Gray LC. Grading system for the selection of patients with congenital aural atresia. Am J Otol 1992;13:6–12.
110. Staffenberg DA. Microtia repair. J Craniofac Surg 2003;14:481–486.
111. Siegert R. Combined reconstruction of congenital auricular atresia and severe microtia. Laryngoscope 2003;113:2021–2027.
112. Digoy GP, Cueva RA. Congenital aural atresia: Review of short- and long-term surgical results. Otol Neurotol 2006;28:54–60.
113. Chang SO, Choi BY, Hur DG. Analysis of the long-term hearing results after the surgical repair of aural atresia. Laryngoscope 2006;116:1835–1841.
114. Thorne CH, Brecht LE, Bradley JP, Levine JP, Hammerschlag P, Longaker MT. Auricular reconstruction: Indications for autogenous and prosthetic techniques. Plast Reconstr Surg 2001;107:1241–1252.
115. Beahm EK, Walton RL. Auricular reconstruction for microtia: Part I. Anatomy, embryology, and clinical evaluation. Plast Reconstr Surg 2002;109:2473–2482.
116. Wilkes GH, Wolfaardt JF. Osseointegrated alloplastic versus autogenous ear reconstruction: Criteria for treatment selection. Plast Reconstr Surg 1994;93:967–979.
117. Wolfaardt JF, Coss P, Levesque R. Craniofacial osseointegration: Technique for bar and acrylic resin substructure construction for auricular prostheses. J Prosthet Dent 1996;76:603–607.
118. Han K, Son D. Osseointegrated alloplastic ear reconstruction with the implant-carrying plate system in children. Plast Reconstr Surg 2002;109:496–503.
119. Miles BA, Sinn DP, Gion GG. Experience with cranial implant-basd prosthetic reconstruction. J Craniofac Surg 2006;17:889–897.
120. Gentile P, Bottini DJ, Gravante G, Nicoli F, Caruso R, Cervelli V. The use of bone-anchored implants for absent ear. J Craniofac Surg 2008;19:744–747.
121. Gentile P, Bottini DJ, Colicchia GM, Trimarco A, Cervelli V. Burns: Bone-anchored, extra-oral implantology. J Burn Care Res 2008;29:627–631.
122. Cronin TD. Use of Silastic frame for total and subtotal reconstruction of the external ear: Preliminary report. Plast Reconstr Surg 1966;37:399–405.
123. Cronin TD, Greenberg RL, Brauer RO. Follow-up study of Silastic frame for reconstruction of external ear. Plast Reconstr Surg 1968;42:522–529.
124. Cronin TD, Ascough BM. Silastic ear construction. Clin Plast Surg 1978;5:367–378.
125. Ohmori S. Use of silicone rubber frame for the reconstruction of microtia cases. In, Hueston ST (ed): Transactions of the Fifth International Congress of Plastic and Reconstructive Surgery. Melbourne: Butterworth; 1971:467.
126. Ohmori S. Reconstruction of microtia using the Silastic frame. Clin Plast Surg 1978;5:379–387.
127. Ohmori S, Matsumoto K, Nakai H. Follow-up study on reconstruction of microtia with a silicone framework. Plast Reconstr Surg 1974;53:555–562.
128. Wellisz T. Clinical experience with the Medpor porous polyethylene implant. Aesthetic Plast Surg 1993;17:339–344.
129. Reinisch J. Microtia reconstruction using a polyethylene implant: An 8-year surgical experience. Presented at the 78th Annual Meeting of the American Association of Plastic Surgeons, Colorado Springs, CO, May 5, 1999.
130. Romo T III, Reitzen SD. Aesthetic microtia reconstruction with Medpor. Facial Plast Surg 2008;24:120–128.
131. Yang SL, Zheng JH, Ding Z, Liu QY, Mao GY, Jin YP. Combined fascial flap and expanded skin flap for enveloping Medpor framework in microtia reconstruction. Aesthetic Plast Surg 2008;33:518–522.
132. Brent B. Microtia repair with rib cartilage grafts: A review of personal experience with 1000 cases. Clin Plast Surg 2002;29:257–271.
133. Thomson HG, Kim TY, Ein SH. Residual problems in chest donor sites after microtia reconstruction: A long-term study. Plast Reconstr Surg 1995;95:961–968.
134. Fukuda O, Yamada A. Reconstruction of the microtic ear with autogenous cartilage. Clin Plast Surg 1978;5:351–366.
135. Uppal RS, Sabbagh W, Chana J, Gault DT. Donor-site morbidity after autologous costal cartilage harvest in ear reconstruction and approaches to reducing donor-site contour deformity. Plast Reconstr Surg 2008;121:1949–1955.
136. Kawanabe Y, Nagata S. A new method of costal cartilage harvest for total auricular reconstruction:

42
SRPS • Volume 11 • Issue R3 • 2011
Part I. Avoidance and prevention of intraoperative and postoperative complications and problems. Plast Reconstr Surg 2006;117:2011–2018.
137. Tai Y, Tanaka S, Fukushima J, Kizuka Y, Kiyokawa K, Inoue Y, Yamauchi T. Refinements in the elevation of reconstructed auricles in microtia. Plast Reconstr Surg 2006;117:2414–2423.
138. Carey JS. Microtia: A personal case study. Aesthetic Plast Surg 1985;9:197–206.
139. Brent B. Auricular repair with autogenous rib cartilage grafts: Two decades of experience with 600 cases. Plast Reconstr Surg 1992;90:355–374.
140. Edgerton MT. Ear construction in children with congenital atresia and stenosis. Plast Reconstr Surg 1969;43:373–380.
141. Brent B. The correction of microtia with autogenous cartilage grafts: I. The classic deformity. Plast Reconstr Surg 1980;66:1–12.
142. Thomson HG, Winslow J. Microtia reconstruction: Does the cartilage framework grow? Plast Reconstr Surg 1989;84:908–915.
143. Adamson JE, Horton CE, Crawford HH. The growth patterns of the external ear. Plast Reconstr Surg 1965;36:466–470.
144. Farkas LG. Growth of normal and reconstructed auricles. In, Tanzer RC, Edgerton MT (ed): Symposium on Reconstruction of the Auricle. St. Louis: CV Mosby; 1974:24.
145. Tanzer RC. Microtia: A long-term follow-up of 44 reconstructed auricles. Plast Reconstr Surg 1978;61:161–166.
146. DellaCroce FJ, Green S, Aguilar EF III. Framework growth after reconstruction for microtia: Is it real and what are the implications? Plast Reconstr Surg 2001;108:1479–1484.
147. Brent B. Technical advances in ear reconstruction with autogenous rib cartilage grafts: Personal experience with 1200 cases. Plast Reconstr Surg 1999;104:319–334.
148. Nagata S. A new method of total reconstruction of the auricle for microtia. Plast Reconstr Surg 1993;92:187–201.
149. Nagata S. Modification of the stages in total reconstruction of the auricle: Part I. Grafting the three-dimensional costal cartilage framework for lobule-type microtia. Plast Reconstr Surg 1994;93:221–230.
150. Nagata S. Modification of the stages in total reconstruction of the auricle: Part II. Grafting the three-dimensional costal cartilage framework for concha-type microtia. Plast Reconstr Surg 1994;93:231–242.
151. Nagata S. Modification of the stages in total reconstruction of the auricle: Part III. Grafting the three-dimensional costal cartilage framework for small concha-
type microtia. Plast Reconstr Surg 1994;93:243–253.
152. Nagata S. Modification of the stages in total reconstruction of the auricle: Part IV. Ear elevation for the constructed auricle. Plast Reconstr Surg 1994;93:254–266.
153. Park C, Lee TJ, Shin KS, Kim YW. A single-stage two-flap method of total ear reconstruction. Plast Reconstr Surg 1991;88:404–412.
154. Song Y, Song Y. An improved one-stage total ear reconstruction procedure. Plast Reconstr Surg 1983;71:615–623.
155. Burstein FD. Cartilage-sparing complete otoplasty technique: A 10-year experience in 100 patients. J Craniofac Surg 2003;14:521–525.
156. Bauer BS. Reconstruction of the microtic ear. J Pediatr Surg 1984;19:440–445.
157. Yanai A, Fukuda O, Nagata S, Tanaka H. A new method utilizing the bipedicle flap for reconstruction of the external auditory canal in microtia. Plast Reconstr Surg 1985;76:464–468.
158. Isshiki N, Koyama H, Suzuki S, Taira T. Surgical techniques for a deep concha, a pseudomeatus, and high projection in congenital microtia. Plast Reconstr Surg 1986;77:546–557.
159. Zim SA. Microtia reconstruction: An update. Curr Opin Otolaryngol Head Neck Surg 2003;11:275–281.
160. Walton RL, Beahm EK. Auricular reconstruction for microtia: Part II. Surgical techniques. Plast Reconstr Surg 2002;110:234–249.
161. Broadbent TR, Woolf RM. Bilateral microtia: A team approach to the middle ear. In, Tanzer RC, Edgerton MT (ed): Symposium on Reconstruction of the Auricle. St. Louis: CV Mosby; 1974.
162. Edgerton MT, Bacchetta C. Principles in the use and salvage of implants in ear reconstruction. In, Tanzer RC, Edgerton MT (ed): Symposium on Reconstruction of the Auricle. St. Louis: CV Mosby; 1974:58.
163. Tegtmeier RE, Gooding RA. The use of a fascial flap in ear reconstruction. Plast Reconstr Surg 1977;60:406–411.
164. Park C, Lew D-H, Yoo W-M. An analysis of 123 temporoparietal fascial flaps: Anatomic and clinical considerations in total auricular reconstruction. Plast Reconstr Surg 1999;104:1295–1306.
165. Helling ER, Okoro S, Kim G II, Wang PT. Endoscope-assisted temporoparietal fascia harvest for auricular reconstruction. Plast Reconstr Surg 2008;121:1598–1605.
166. Nagata S. Secondary reconstruction for unfavorable microtia results utilizing temporoparietal and innominate fascia flaps. Plast Reconstr Surg 1994;94:254–265.
167. Hirase Y, Kojima T, Hirakawa M. Secondary ear

SRPS • Volume 11 • Issue R3 • 2011
43
reconstruction using deep temporal fascia after temporoparietal fascial reconstruction in microtia. Ann Plast Surg 1990;25:53–57.
168. Alexander G, Rajacic N, Ibrahim MK, Al-Zamil S. The combined posterior temporoparietal and galeal fascial flap: A new flap in the elevation of the constructed auricle (second stage of microtia correction). Br J Plast Surg 2002;55:582–584.
169. Brent B. The correction of microtia with autogenous cartilage grafts: II. Atypical and complex deformities. Plast Reconstr Surg 1980;66:13–21.
170. Hata Y, Hosokawa K, Yano K, Matsuka K, Ito O. Correction of congenital microtia using the tissue expander. Plast Reconstr Surg 1989;84:741–751.
171. Pan B, Jiang H, Guo D, Huang C, Hu S, Zhuang H. Microtia: Ear reconstruction using tissue expander and autogenous costal cartilage. J Plast Reconstr Aesthet Surg 2008;61[suppl 1]:S98–S103.
172. Jiang H, Pan B, Lin L, Cai Z, Zhuang H. Ten-year experience in microtia reconstruction using tissue expander and autogenous cartilage. Int J Pediatr Otorhinolaryngol 2008;72:1251–1259.
173. Oberg M, Becker M, Arktander M, Centerman M, Svensson H, Wikström S. Thermosensitivity in a reconstructed microtic ear. Scand J Plast Reconstr Surg Hand Surg 2008;42:190–193.
174. Wray RC, Hoopes JE. Silastic frameworks in total reconstruction of the auricle. Br J Plast Surg 1973;26:296–297.
175. Curtin JW, Bader KF. Improved techniques for the successful silicone reconstruction of the external ear. Plast Reconstr Surg 1969;44:372–377.
176. Monroe CW. Our experiences with the silicone ear framework: A report of 17 ears in 15 patients. Plast Reconstr Surg 1972;49:428–432.
177. Hinderer UT, del Rio JL, Fregenal FJ. Otoplasty for lop ears. Aesthetic Plast Surg 1987;11:75–80.
178. Tanzer RC. The constricted (cup and lop) ear. Plast Reconstr Surg 1975;55:406–415.
179. Cosman B. The constricted ear. Clin Plast Surg 1978;5:389–400.
180. Kislov R. Surgical correction of the cupped ear. Plast Reconstr Surg 1971;48:121–125.
181. Horlock N, Grobbelaar AO, Gault DT. 5-year series of constricted (lop and cup) ear corrections: Development of the mastoid hitch as an adjunctive technique. Plast Reconstr Surg 1998;102:2325–2332.
182. Park C. The tumbling concha-cartilage flap for correction of lop ear. Plast Reconstr Surg 2000;106:259–265.
183. Al-Qattan MM. An alternative approach for correction of constricted ears of moderate severity. Br J Plast Surg 2005;58:389–393.
184. Stephenson KL. Correction of a lop ear type deformity. Plast Reconstr Surg 1960;26:540–545.
185. Musgrave RH. A variation on the correction of the congenital lop ear. Plast Reconstr Surg 1966;37:394-398.
186. Ohjimi H, Era K, Kinoshita K, Fukuda T, Shiratake Y. Double pennant technique: Elongating the helix using rim flaps to correct the constricted ear. Ann Plast Surg 2004;53:465–468.
187. Nagata S. Alternative surgical methods of treatment for the constricted ear. Clin Plast Surg 2002;29: 301–315.
188. Xiaogeng H, Hongxing Z, Qinghua Y, Haiyue J, Yanyong Z. A new method of correcting type I and type II constricted (cup and lop) ears. Aesthetic Plast Surg 2006;30:449–454.
189. Xiaogeng H, Hongxing Z, Qinghua Y, Haiyue J, Yanyong Z. Subtotal ear reconstruction for correction of type 3 constricted ears. Aesthetic Plast Surg 2006;30:455–459.
190. Nakajima T, Yoshimura Y, Kami T. Surgical and conservative repair of Stahl’s ear. Aesthetic Plast Surg 1984;8:101–107.
191. Chongchet V. A method of antihelix reconstruction. Br J Plast Surg 1963;16:268–272.
192. Ferraro GA, Perrotta A, Rossano F, D’Andrea F. Stahl syndrome in clinical practice. Aesthetic Plast Surg 2006;30:348–349.
193. Ono I, Gunji H, Tateshita T. An operation for Stahl’s ear. Br J Plast Surg 1996;49:564–567.
194. Kaplan HM, Hudson DA. A novel surgical method of repair of Stahl’s ear: A case report and review of current treatment modalities. Plast Reconstr Surg 1999;103:566–569.
195. Nakayama Y, Soeda S. Surgical treatment of Stahl’s ear using the periosteal string. Plast Reconstr Surg 1986;77:222–226.
196. Sugino H, Tsuzuki K, Bandoh Y, Tange I. Surgical correction of Stahl’s ear using the cartilage turnover and rotation method. Plast Reconstr Surg 1989;83:160–164.
197. Tsujiguchi K, Tajima S, Tanaka Y, Hira M. A new method for correction of Stahl’s ear. Ann Plast Surg 1992;28:373–376.
198. Al-Qattan MM, Hashem FK. An alternative approach for correction of Stahl’s ear. Ann Plast Surg 2004;52:105–108.
199. Torikai K, Ando S, Yoshida T. Anatomy of the auricular muscles and its surgical application. Jpn J Plast Reconstr Surg 1982;25:46.
200. Elsahy NI. An alternative technique for correction of cryptotia. Ann Plast Surg 1989;23:66–73.
201. Mutimer KL, Mulliken JB. Correction of cryptotia using

44
SRPS • Volume 11 • Issue R3 • 2011
tissue expansion. Plast Reconstr Surg 1988;81:601–604.
202. Hirose T, Tomono T, Matsuo K, Katohda S, Takahashi N, Iwasawa M, Satoh R. Cryptotia: Our classification and treatment. Br J Plast Surg 1985;38:352–360.
203. Matsuo K, Hirose T, Tomono T, Iwasawa M, Katohda S, Takahashi N, Koh B. Nonsurgical correction of congenital auricular deformities in the early neonate: A preliminary report. Plast Reconstr Surg 1984;73:38–51.
204. Yotsuyanagi T, Yamashita K, Shinmyo Y, Yokoi K, Sawada Y. A new operative method of correcting cryptotia using a large Z-plasty. Br J Plast Surg 2001;54:20–24.
205. Nakajima T, Yoneda K, Yoshimura Y. Correction of cryptotia using a subcutaneous pedicled flap. Br J Plast Surg 1991;44:406–409.
206. Pollock WJ. Techniuqe for correction of cryptotia: Case report. Plast Reconstr Surg 1969;44:501–503.
207. Onizuka T, Tokunaga S, Yamada K. A method for repair of cryptotia. Plast Reconstr Surg 1978;62:734–738.
208. Argamaso RV. Cryptotia: Its surgical correction. Ann Plast Surg 1979;2:109–113.
209. Wesser DR. Repair of a cryptotic ear with a trefoil flap: Case report. Plast Reconstr Surg 1972;50:192–193.
210. Hayashi R, Matsuo K, Hirose T. Familial cryptotia. Plast Reconstr Surg 1993;91:1337–1339.
211. Yoshimura K, Ouchi K, Wakita S, Uda K, Harii K. Surgical correction of cryptotia with superiorly based superificial mastoid fascia and skin paddle. Plast Recontr Surg 2000;105:836–841.
212. Paredes AA Jr, Williams JK, Elsahy NI. Cryptotia: Principles and management. Clin Plast Surg 2002;29:317–326.
213. Uemura T, Matsumoto N, Tanabe T, Saitoh T, Matsushita S, Mitsukawa N. Surgical correction of cryptotia combined with intraoperative distention using isotonic saline injection and rotation flap method. J Craniofac Surg 2005;16:473–476.
214. Hyakusoku H, Fumiiri M. The square flap method. Br J Plast Surg 1987;40:40–46.
215. Yanai A, Tange I, Bandoh Y, Tsuzuki K, Sugino H, Nagata S. Our method of correcting cryptotia. Plast Reconstr Surg 1988;82:965–972.
216. Chana JS, Fourie LR. A technique for the correction of cryptotia. Ann Plast Surg 1997;39:261–265.
217. Chang SO, Suh MW, Choi BY, Park MH, Ha Oh S, Kim CS. A new technique for correcting cryptotia: V-Y swing flap. Plast Reconstr Surg 2007;120:437–441.
218. Park S, Takushima M, Minegishi M. Reconstruction of cryptotia using a skin graft. Ann Plast Surg 1994;32:441–444.
219. Hodgson EL, McGregor AD. Correction of cryptotia
using full-thickness skin grafts. Ann Plast Surg 2001;47:471–472.
220. Cho BC, Han KH. Surgical correction of cryptotia with V-Y advancement of a temporal triangular flap. Plast Reconstr Surg 2005;115:1570–1581.
221. Brown FE, Colen LB, Addante RR, Graham JM Jr. Correction of congenital auricular deformities by splinting in the neonatal period. Pediatrics 1986;78:406–411.
222. Byrd HS, Langevin CJ, Ghidoni LA. Ear molding in newborn infants with auricular deformities. Plast Reconstr Surg 2010;126:1191–1200.
223. Madzharov MM. A new method of auriculoplasty for protruding ears. Br J Plast Surg 1989;42:285–290.
224. Webster RC, Smith RC. Otoplasty for prominent ears. In, Goldwyn RM (ed): Long-term Results in Plastic and Reconstructive Surgery. Boston: Little, Brown; 1980:146.
225. Kelley P, Hollier L, Stal S. Otoplasty: Evaluation, technique, and review. J Craniofac Surg 2003;14:643–653.
226. Rogers BO. Ely’s 1881 operation for correction of protruding ears: A medical “first”. Plast Reconstr Surg 1968;42:584–586.
227. [No authors listed]. A classic reprint: An operation for prominence of the auricles (with two wood-cuts) by Edward T. Ely (Arch Otol 10:97, 1881). Aesthetic Plast Surg 1987;11:73–74.
228. Rogers BO. The classic reprint: A new operation for prominent ears based on the anatomy of the deformity by William H. Luckett, M.D. (Surg Gynecol Obstet 10:635–637, 1910). Plast Reconstr Surg 1969;43:83–86.
229. Georgiade GS, Riefkohl R, Georgiade NG. Prominent ears and their correction: A forty-year experience. Aesthetic Plast Surg 1995;19:439–443.
230. Gosain AK, Kumar A, Huang G. Prominent ears in children younger than 4 years of age: What is the appropriate timing for otoplasty? Plast Reconstr Surg 2004;114:1042–1054.
231. Gasques JA, Pereira de Godoy JMP, Cruz EM. Psychosocial effects of otoplasty in children with prominent ears. Aesthetic Plast Surg 2008;32:910–914.
232. Davis JE. Prominent ears. Clin Plast Surg 1978;5:471–477.
233. Davis JE. Aesthetic and Reconstructive Otoplasty. New York: Springer-Verlag; 1987.
234. Balogh B, Millesi H. Are growth alterations a consequence of surgery for prominent ears? Plast Reconstr Surg 1992;90:192–199.
235. Lavy J, Stearns M. Otoplasty: Techniques, results and complications: A review. Clin Otolaryngol Allied Sci 1997;22:390–393.

SRPS • Volume 11 • Issue R3 • 2011
45
236. Mustardé JC. The correction of prominent ears using mattress sutures. Br J Plast Surg 1963;16:170–178.
237. Johnson PE. Otoplasty: Shaping the antihelix. Aesthetic Plast Surg 1994;18:71–74.
238. Furnas DW. Correction of prominent ears by concha-mastoid sutures. Plast Reconstr Surg 1968;42:189–193.
239. Spira M, Stal S. The conchal flap: An adjunct in otoplasty. Ann Plast Surg 1983;11:291–298.
240. Webster GV. The tail of the helix as a key to otoplasty. Plast Reconstr Surg 1969;44:455–461.
241. Beernink JH, Blocksma R, Moore WD. The role of the helical tail in cosmetic otoplasty. Plast Reconstr Surg 1979;64:115–117.
242. Goulian D Jr, Conway H. Prevention of persistent deformity of the tragus and lobule by modification of the Luckett technique of otoplasty. Plast Reconstr Surg Transplant Bull 1960;26:399–404.
243. Spira M. Reduction otoplasty. In, Goldwyn RM (ed): The Unfavorable Result in Plastic Surgery: Avoidance and Treatment. Boston: Little, Brown; 1984:307–321.
244. Gosain AK, Recinos RF. A novel approach to correction of the prominent lobule during otoplasty. Plast Reconstr Surg 2003;112:575–583.
245. Gibson T, Davis W. The distortion of autogenous cartilage grafts: Its cause and prevention. Br J Plast Surg 1958;10:257–274.
246. Fry HJ. Interlocked stresses in human nasal septal cartilage. Br J Plast Surg 1966;19:276–278.
247. Stenstrom SJ. A “natural” technique for correction of congenitally prominent ears. Plast Reconstr Surg 1963;32:509–518.
248. Stenstrom SJ, Heftner J. The Stenstrom otoplasty. Clin Plast Surg 1978;5:465–470.
249. Crikelair GF, Cosman B. Another solution for the problem of the prominent ear. Ann Surg 1964;160:314–324.
250. Weinzweig N, Chen L, Sullivan WG. Histomorphology of neochondrogenesis after antihelical fold creation: A comparison of three otoplasty techniques in the rabbit. Ann Plast Surg 1994;33:371–376.
251. Karacalar A, Demir A, Yildiz L. Subcision surgery for the correction of ear deformities. Aesthetic Plast Surg 2004;28:239–244.
252. Fritsch MH. Incisionless otoplasty. Facial Plast Surg 2004;20:267–270.
253. Mordon S, Wang T, Fleurisse L, Creusy C. Laser cartilage reshaping in an in vivo rabbit model using a 1.54 µm Er:Glass Laser. Lasers Surg Med 2004;34:315–322.
254. Tanzer RC. The correction of prominent ears. Plast
Reconstr Surg Transplant Bull 1962;30:236–246.
255. Hinderer UT, del Rio JL, Fregenal FJ. Otoplasty for prominent ears. Aesthetic Plast Surg 1987;11:63–69.
256. Pitanguy I, Müller P, Piccolo N, Ramalho E, Solinas R. The treatment of prominent ears: A 25-year survey of the island technique. Aesthetic Plast Surg 1987;11:87–93.
257. Kaye BL. A simplified method for correcting the prominent ear. Plast Reconstr Surg 1967;40:44–48.
258. Baker DC, Converse JM. Correction of protruding ears: A 20-year retrospective. Aesthetic Plast Surg 1979;3:29-39.
259. Chait L, Nicholson R. One size fits all: A surgical technique for the correction of all types of prominent ears. Plast Reconstr Surg 1999;104:190–195.
260. Stal S. One size fits all: A surgical technique for the correction of all types of prominent ears [letter]. Plast Reconstr Surg 1999;104:1969.
261. Stal S, Klebuc M, Spira M. An algorithm for otoplasty. Oper Tech Plast Reconstr Surg 1997;4:88–103.
262. Spira M. Otoplasty: What I do now: A 30-year perspective. Plast Reconstr Surg 1999;104:834–840.
263. Graham KE, Gault DT. Endoscopic assisted otoplasty: A preliminary report. Br J Plast Surg 1997;50:47–57.
264. Bauer BS, Song DH, Aitken ME. Combined otoplasty technique: Chondrocutaneous conchal resection as the cornerstone to correction of the prominent ear. Plast Reconstr Surg 2002;110:1033–1040.
265. Peker F, Celiköz B. Otoplasty: Anterior scoring and osterior rolling technique in adults. Aesthetic Plast Surg 2002;26:267–273.
266. Janis JE, Rohrich RJ, Gutowski K. Otoplasty. Plast Reconstr Surg 2005;115:60e–72e.
267. Nicoletis C, Guerin-Surville H. Prominent ears: Transposition of the posterior auricular muscle on the scapha: A new technique. Aesthetic Plast Surg 1978;2:295–299.
268. Smith DW. Protruding auricle: A neuromuscular sign. Lancet 1978;1:747–749.
269. Smith DW, Takashima H. Ear muscles and ear form. Birth Defects Orig Artic Ser 1980;16:299–302.
270. Guyuron B, DeLuca L. Ear projection and the posterior auricular muscle insertion. Plast Reconstr Surg 1997;100:457–460.
271. Scuderi N, Tenna S, Bitonti A, Vonella M. Repositioning of posterior auricular muscle combined with conventional otoplasty: A personal technique. J Plast Reconstr Aesthet Surg 2007;60:201–204.
272. Shinohara H, Matsuo K, Hataya Y, Taki K. Correlation between projection of the ear, the inferior crus, and the

46
SRPS • Volume 11 • Issue R3 • 2011
antihelical body: Analysis based on computed tomography. Scand J Plast Reconstr Hand Surg 2007;41:288–292.
273. Corchado C, Infante J. A surgical technique for the correction of all types of prominent ears? Plast Reconstr Surg 2000;106:948–951.
274. Elliott RA Jr. Complications in the treatment of prominent ears. Clin Plast Surg 1978;5:479–490.
275. Tan KH. Long-term survey of prominent ear surgery: A comparison of two methods. Br J Plast Surg 1986;39:270–273.
276. Mustardé JC. The treatment of prominent ears by buried mattress sutures: A ten-year survey. Plast Reconstr Surg 1967;39:382–386.
277. Mustardé JC. Results of otoplasty by the author’s method. In, Goldwyn RM (ed): Long-term Results in Plastic and Reconstructive Surgery. Boston: Little, Brown; 1980.
278. Spira M, Hardy SB. Mustardé otoplasty: A critical second look. In, Marchac D (ed): Transactions of the Sixth International Congress of Plastic and Reconstructive Surgery. Paris: Masson: 1975:297−299.
279. Heffner J. Follow-up study on 167 Stenstrom otoplasties. Clin Plast Surg 1978;5:470.
280. Calder JC, Naasan A. Morbidity of otoplasty: A review of 562 consecutive cases. Br J Plast Surg 1994;47:170–174.
281. Messner AH, Crysdale WS. Otoplasty: Clinical protocol and long-term results. Arch Otolaryngol Head Neck Surg 1996;122:773–777.
282. Walter C, Nolst Trenité GJ. Revision otoplasty and special problems. Facial Plast Surg 1994;10:298–308.
283. Firmin F, Sanger C, O’Tolle G. Ear reconstruction following severe complications of otoplasty. J Plast Reconstr Aesthet Surg 2008;61[suppl 1]:S13-S20.
284. Limandjaja GC, Breugem CC, Mink van der Molen AB, Kon M. Complications of otoplasty: A literature review. J Plast Reconstr Aesthet Surg 2009;62:19–27.
285. Loeb R. Earlobe tailoring during facial rhytidoplasties. Plast Reconstr Surg 1972;49:485–489.
286. McKinney P, Giese S, Placik O. Management of the ear in rhytidectomy. Plast Reconstr Surg 1993;92:858–866.
287. Mowlavi A, Meldrum DG, Wilhelmi BJ, Zook EG. Incidence of earlobe ptosis and pseudoptosis in patients seeking facial rejuvenation surgery and effects of aging. Plast Reconstr Surg 2004;113:712–717.
288. Mowlavi A, Meldrum DG, Kalkanis J, Wilhelmi BJ, Russell RC, Zook EG. Surgical design and algorithm for correction of earlobe ptosis and pseudoptosis deformity. Plast Reconstr Surg 2005;115:290–295.
289. El Kollali R. Earlobe morphology: A simple classification of normal earlobes [letter]. J Plast Reconstr Aesthet Surg 2009;62:277–280.
290. Kim WS, Vacanti JP, Cima L, Mooney D, Upton J, Puelacher WC, Vacanti CA. Cartilage engineered in predetermined shapes employing cell transplantation on synthetic biodegradable polymers. Plast Reconstr Surg 1994;94:233–237.
291. Shieh SJ, Terada S, Vacanti JP. Tissue engineering auricular reconstruction: In vitro and in vivo studies. Biomaterials 2004;25:1545–1557.
292. Cao Y, Vacanti JP, Paige KT, Upton J, Vacanti CA. Transplantation of chondrocytes utilizing a polymer-cell construct to produce tissue-engineered cartilage in the shape of a human ear. Plast Reconstr Surg 1997;100:297–302.
293. Chang SC, Tobias G, Roy AK, Vacanti CA, Bonassar LJ. Tissue engineering of autologous cartilage for craniofacial reconstruction by injection molding. Plast Reconstr Surg 2006;112:793–799.
294. Ting V, Sims CD, Brecht LE, McCarthy JG, Kasabian AK, Connelly PR, Elisseeff J, Gittes GK, Longaker MT. In vitro prefabrication of human cartilage shapes using fibrin glue and human chondrocytes. Ann Plast Surg 1998;40:413–420.
295. Xu JW, Johnson TS, Motarjem PM, Peretti GM, Randolph MA, Yaremchuk MJ. Tissue-engineered flexible ear-shaped cartilage. Plast Reconstr Surg 2005;115:1633–1641.
296. Neumeister MW, Wu T, Chambers C. Vascularized tissue-engineered ears. Plast Reconstr Surg 2006;117:116–122.
297. Ciorba A, Martini A. Tissue engineering and cartilage regeneration for auricular reconstruction. Int J Ped Otorhinolaryngol 2006;70:1507–1515.
298. Sterodimas A, de Faria J, Correa WE, Pitanguy I. Tissue engineering and auricular reconstruction: A review. J Plast Reconstr Aesthet Surg 2009;62:447–452.
299. Ulusal AE, Ulusal BG, Hung L, Wei FC. Establishing a composite auricle allotransplantation model in rats: Introduction to transplantation of facial subunits. Plast Reconstr Surg 2005;116:811–817.
300. Ulusal BG, Ulusal AE, Lin JY, Tan BK, Wong CH, Song C, Wei FC. Anatomical and technical aspects of harvesting the auricle as a neurovascular facial subunit transplant in humans. Plast Reconstr Surg 2007;120:1540–1545.
301. Jiang HQ, Wang Y, Hu XB, Li YS, Li JS. Composite tissue allograft transplantation of cephalocervical skin flap and two ears. Plast Reconstr Surg 2005;115:31e–35e.

We thank theAesthetic Surgery Journal
andPlastic and Reconstructive Surgery
for their support.
Order Today: (800) 818-7243 (US & Canada)
(805) 499 9774 (Other countries)www.aestheticsurgeryjournal.com
Aesthetic Surgery Journal (ASJ) is a peer-reviewed international journal focusing on scientifi c developments and clinical techniques in aesthetic surgery. An offi cial publication of the 2200-member American Society for Aesthetic Plastic Surgery (ASAPS), ASJ is also the offi cial English-language journal of twelve major international societies of plastic, aesthetic, and reconstructive surgery representing South America, Central America, Europe, Asia, and the Middle East, and the offi cial journal of The Rhinoplasty Society.
Submit your manuscript!www.aestheticsurgeryjournal.com
Now Indexed in MEDLINE!Submit Your Manuscript Today
Published by

Whether you’re performing a routinecosmetic procedure or a difficultburn repair, having the right tool forunexpected complications is critical.
The intuitive, all-new, next-generation electronic journalsplatform from LippincottWilliams &Wilkins comes loadedwith personalized options for its journal subscribers, includingcustomizable state-of-the-art capabilities, self-serviceoptions tailored to your information preferences, rich mediacontent, improved search options, better article readabilityin HTML and better tools to help you manage content that’svital to your practice and patient care.
Register online at prsjournal.comNot a subscriber? Visit prsjournal.com to subscribe andfind out more
This is your website.The new Plastic and ReconstructiveSurgery Online
This is your life.
#3 code: A9PRSQ772CF
myLWW_PRS_8.125x10.875_FINAL:Layout 2 8/6/09 11:19 AM Page 1

extends thanks to
for their support of plastic surgery educationas a Platinum Education Partner.