Obesity in Plastic Surgery Lip Teh Plastic Surgery December 2006.
36
Obesity in Plastic Surgery Lip Teh Plastic Surgery December 2006
-
Upload
angela-morton -
Category
Documents
-
view
238 -
download
1
Transcript of Obesity in Plastic Surgery Lip Teh Plastic Surgery December 2006.
Obesity inPlastic Surgery
Lip Teh
Plastic Surgery
December 2006
The Problem of Obesity• Hypertension• Dyslipidemia, Type 2 diabetes, Insulin resistance, glucose
intolerance, Hyperinsulinemia• Atrial fibrillation, Coronary heart disease, Congestive heart failure• Stroke• Reflux oesophagitis, Gallstones, Cholecystitis and cholelithiasis• Gout, osteoarthritis• Obstructive sleep apnea and respiratory problems• Malignancies - endometrial, breast, prostate, and colon cancer• Complications of pregnancy• Poor female reproductive health (such as menstrual irregularities,
infertility, and irregular ovulation)• Stress incontinence, Uric acid nephrolithiasis• Psychological disorders (such as depression, eating disorders,
distorted body image, and low self-esteem)
Obesity: The Epidemic
• In the US:– Annual deaths due to obesity:
112,000– 65% adults overweight
• 30% obese
• 4% severe obesity
– 16% of children ages 6 to 19 years old are overweight
– Obesity prevalence has increased across all education levels and is higher for persons with less education
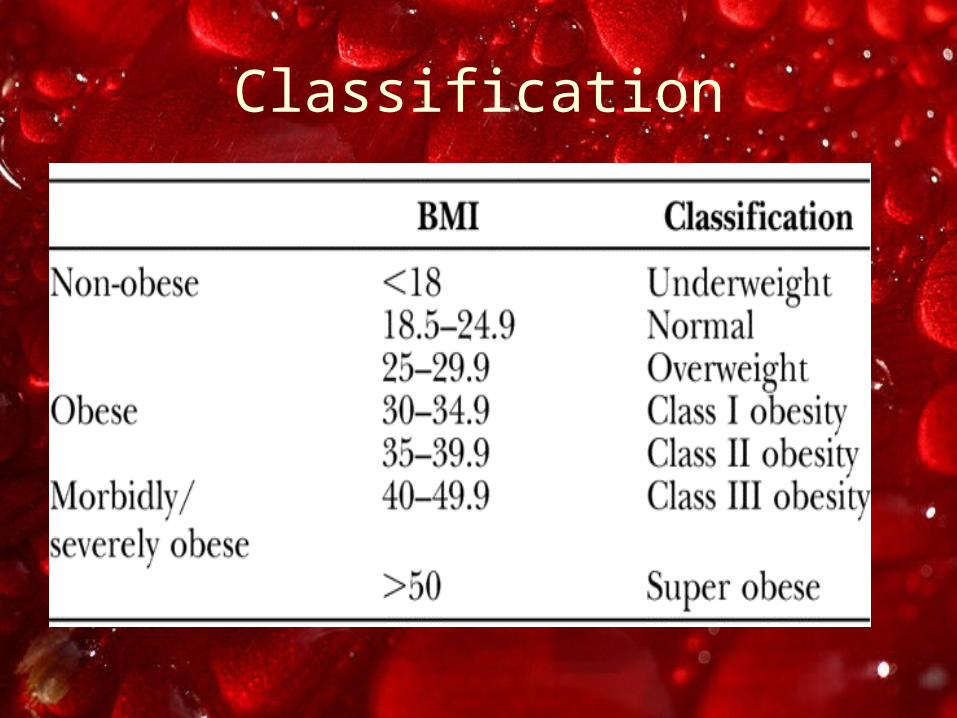
Classification
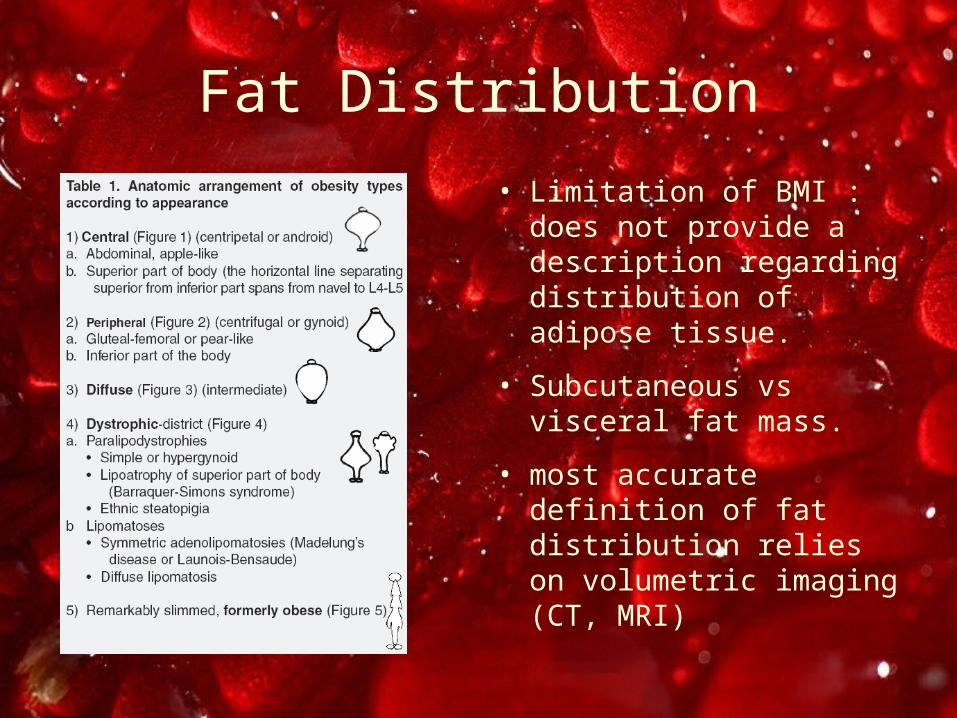
Fat Distribution
• Limitation of BMI : does not provide a description regarding distribution of adipose tissue.
• Subcutaneous vs visceral fat mass.
• most accurate definition of fat distribution relies on volumetric imaging (CT, MRI)
Central obesity
Subcutaneous: Visceral Fat ratio <1.5 in woman and 0.75 in men
mainly located in the abdomimal viscera, whereas limbs and face are often normal.
frequently associated with metabolic and vascular disorders
requires dietological, exercise, and possibly psychological therapy.
Peripheral obesity
Subcutaneous: Visceral fat ratio >2
mainly located in limbs and in regions below navel
infrequently associated with metabolic disorder
Often resistant to dieting
Diffuse obesity
most common form consists of a
homogenous increase of adipose tissue in the whole body.
ideal therapy should be a synergic approach by the dietologist, the bariatric surgeon and the plastic surgeon.
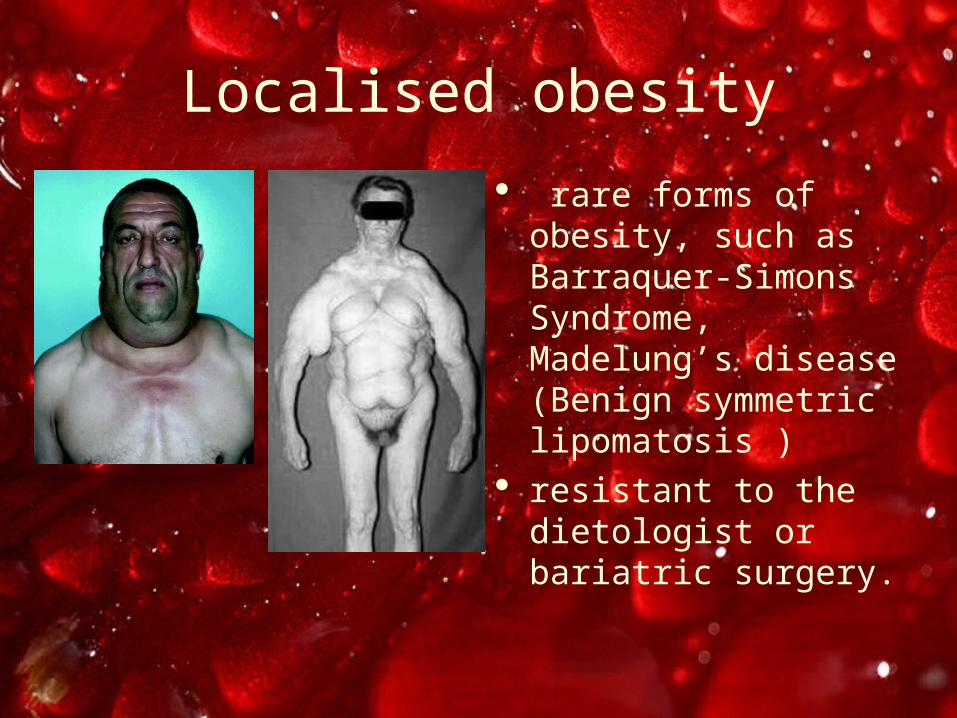
Localised obesity
rare forms of obesity, such as Barraquer-Simons Syndrome, Madelung’s disease (Benign symmetric lipomatosis )
resistant to the dietologist or bariatric surgery.
Formerly obese
redundant cutaneous mantle secondary to massive fat loss
Seen more frequently now following bariatric surgery
Bariatric Surgery
• Indications:– BMI>40– BMI> 35 who have significant
comorbidities.
• most effective therapy for long-term significant weight loss in morbidly obese patients.
• number of procedures performed in the US increased 500% between 1993 and 2003.

Bariatric Surgery
• Metaanalysis of 22,000 patients
1. Lipid disorders improved in 70%
2. Diabetes improved in 76.8%
3. Hypertension improved in 78.5%
4. Obstructive sleep apnea improved in 86%
Buchwald et al, JAMA 2004
Obesity and Surgery
• Studies from multiple coronary artery bypass surgery shows:
– In hospital mortality unchanged compared to normal population
– Increased risk of perioperative morbidity, sternal infections, prolonged mechanical ventilation and increased length of stay
Obesity and Surgery
• DVT and PE– Mechanisms
• increased intra-abdominal pressure
• venous stasis • hypercoagulable state
(higher levels of factor VIII and factor IX, but not of fibrinogen )
• Poor mobility
– Relative risk (obese vs nonobese) Am J Med 2004
• DVT – 2.5x • PE – 2.2x
– In obese(BMI>25) women on OCP – 10x risk of DVT (Thromb Haemost 2003)
Obesity and Surgery
• Nosocomial infection
– 3x increase risk in obese
– 4x increase risk in severe obese
– Mostly due to increase in surgical site infection
– Also increase risk of pneumonia and UTI
Obesity and Surgery
• Surgical site infection
– Mechanisms• decreased oxygen
tension • immune impairment • tension along suture
line• longer operative time
– Relative risk = 2-3x

Surgical Site infection
• Obesity Research 2003– Prospective study of 395 patients in a general
surgery unit
Underweight Normal Overweight Obesity Extreme Obesity
Clean 0/5 (0%) 7/60 (12%) 25/168 (15%) 21/46 (46%) 4/6 (67%)
Clean/contaminated 0/2 (0%) 4/15 (27%) 4/40 (10%) 6/6 (100%)
Contaminated 0/2 0%) 10/18 (56%) 13/20 (65%) 2/2 (100%)
Dirty 0/2 (0%) 0/1 (0%)
Total 0/9 (0%) 19/95 (20%) 44/230 (19%) 29/55 (53%) 4/6 (67%)
Surgical Site infection
• Olsen, J Thorac Cardiovasc Surg 2002– Retrospective study– Obesity: OR 3.1x for superficial surgical-site
infection
• Vilar-Compte (World J Surg 2004)– Prospective study, 280 patients in a breast
oncological surgery unit– Obesity: OR 2.5x for surgical site infection
Surgical Site infection• Barber (Arch Surg 1995)
– MSKC oncological service N=1226
– Surgical site infection rates were 3.8% in class I; 8.8% in class II; 20.7% in class III; and 46.9% in class IV procedures.
– obesity contributed as strongly as the surgical procedure category to a patient's likelihood of acquiring a surgical site infection.
• Yap (Heart Lung Circ Dec 2006)– morbidly obese group -
increased rates of deep sternal infection (OR 6.4)

Risks with Plastic Surgery?
Breast Reduction
• Only 20% of women undergoing reduction mammoplasty are of normal weight
• Strombeck 1964– systemic and local complications
• 4.4% for the nonobese • 13.5% for those > 10 kg overweight.
• Zubowski (PRS 2000; retrospective n=395)– Major local complications (skin loss, nipple loss,
abscess, and hematoma )• 6.2% for the nonobese • 9.2% for those > 10 kg overweight.
– Complications correlated with increasing weight of reduction

Breast Reduction
• Platt (Ann Plast Surg 2003 prospective n=30)– BMI > 26.3, 33% wound breakdown rate– BMI < 26.3, 10% wound breakdown rate; P < 0.05
• Wagner (PRS 2005, retrospective n=186)– no increase in the complication rate in the obese
patients• O’Grady (PRS 2005, retrospective n=133)
– BMI not associated with nipple necrosis, hematoma formation, fat necrosis, cyst formation, nipple sensation, or hypertrophic scarring
– Higher BMI predicted a delayed healing, wound dehiscence, and infection. (relative risk 1.2x)
Breast Reduction
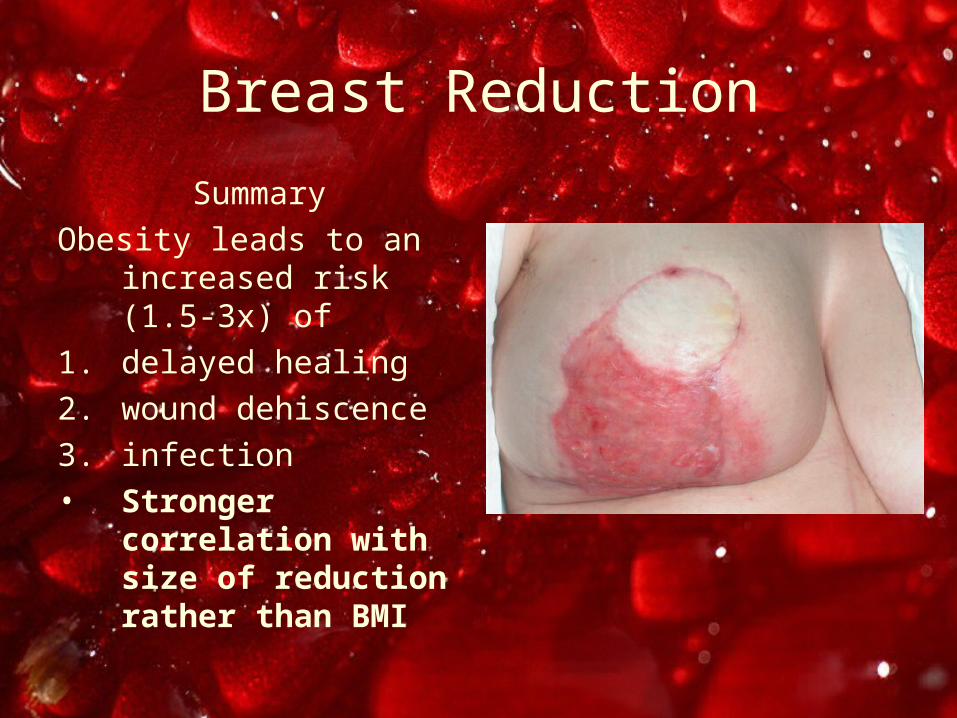
Summary
Obesity leads to an increased risk (1.5-3x) of
1. delayed healing
2. wound dehiscence
3. infection• Stronger correlation
with size of reduction rather than BMI
Breast Reconstruction
• Paige, Bostwick PRS 1998– Pedicled TRAM, retrospective n=257– Obesity significantly associated with
• Donor site complications• Fat necrosis• Partial flap loss• Breast mound infection
Breast Reconstruction
• Chang (MDACC; PRS Apr 2000)– Free TRAM, retrospective n=939 flaps (718 patients)– Flap complications: Obese vs normal weight
1. overall flap complications (39.1 vs 20.4%;p = 0.001),2. total flap loss (3.2 versus 0%;p = 0.001)3. flap seroma (10.9 versus 3.2%;p = 0.004)4. mastectomy flap necrosis (21.9 versus 6.6%;p = 0.001).
– Flap complications: Overweight vs normal weight 1. overall flap complications (27.8 versus 20.4%;p = 0.033)2. total flap loss (1.9 versus 0%p = 0.004)3. flap hematoma (0 versus 3.2%;p = 0.007)4. mastectomy flap necrosis (15.1 versus 6.6%;p = 0.001)
Breast Reconstruction
– Donor complications: Obese vs normal weight 1. overall donor-site complications (23.4 versus 11.1%;p =
0.005)
2. infection (4.7 versus 0.5%;p = 0.016)
3. seroma (9.4 versus 0.9%;p <0.001)
4. hernia (6.3 versus 1.6%;p = 0.039).
– Donor complications: Overweight vs normal weight 1. overall donor-site complications (19.8 versus 11.1%;p =
0.003)
2. infection (2.4 versus 0.5%;p = 0.039)
3. bulge (5.2 versus 1.8%;p = 0.016)
4. hernia (4.3 versus 1.6%;p = 0.039)

Breast Reconstruction
• Mehrara (PRS Oct 2006)– Free flap Breast recons, retrospective 1195
recons in 952 patients– Obesity (BMI>30) major independent
predictor of partial flap loss (OR 2.6), donor site complications(OR 3) and hernia/laxity (OR 2.5)
• Major complications - OR 2.2• Minor complications – OR 1.9• Late complications – OR 2.9
Breast Reconstruction
Summary
• In TRAM reconstructions, obesity leads to an increased risk of
1. Flap complications (2-3x)
2. Donor site complications (2-3x)
Obesity and Abdominoplasty
• Vastine (Ann Plast Surg 99)– Retrospective study, n=90– 80% of obese patients had complications
compared with the borderline and nonobese patients, who had complication rates of 33% and 32.5% respectively
– Previous gastric bypass surgery had no significant effect on the incidence of postabdominoplasty complications.
Obesity and Abdominoplasty
• Roqliani (Ann Plast Surg Sept 06)– Retrospective study, n=80– obese population had a complication rate of
76% (23 of 30); 15 of 23 were major complications and included wound breakdown and hematoma/seroma. The overweight and normal-weight groups had complication rates of 35% (7 of 20) and 33% (10 of 30)
Obesity and Body Contouring
• Taylor (Obese Surg 2004)– Retrospective study, n=30 post massive
weight loss– Overall morbidity 42%
• 20% wound breakdown• 17% seroma• 1 patient died from PE
– Challenging surgery requiring individualized approaches with intensive follow-up.
Obesity and Body Contouring
• Sanger (Ann Plast Surg Jan 2006)– Retrospective study, n=18 post massive
(>25kg) weight loss – 27% wound complications(seromas,
hematoma, infection, and fat necrosis)– increase in wound complications attributed to
the inherent complications seen with obese patients.
Obesity and Body Contouring
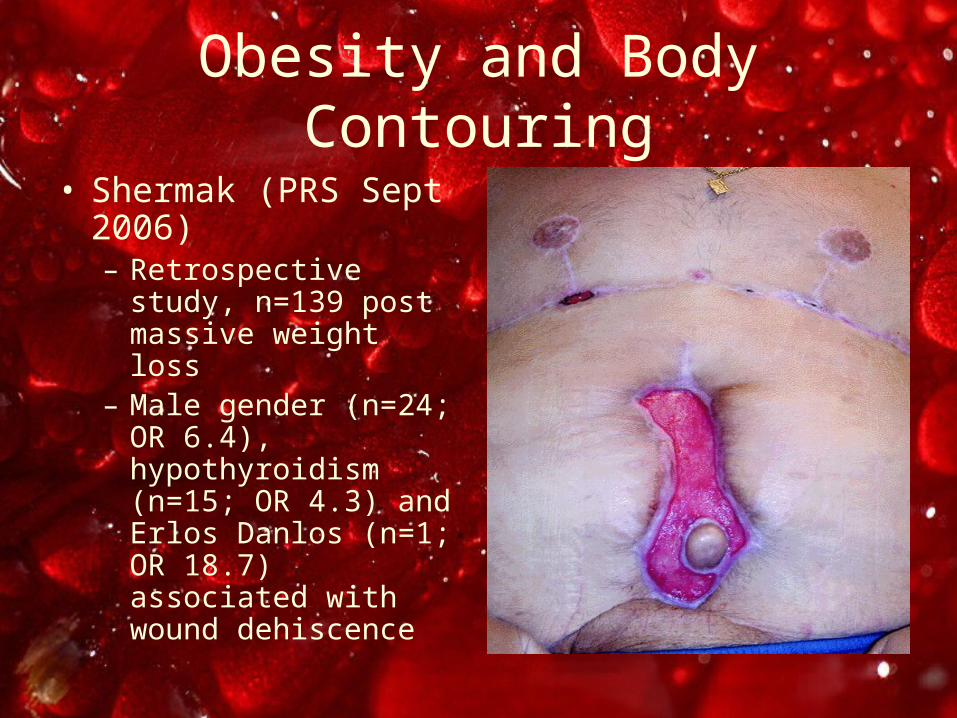
• Shermak (PRS Sept 2006)– Retrospective study,
n=139 post massive weight loss
– Male gender (n=24; OR 6.4), hypothyroidism (n=15; OR 4.3) and Erlos Danlos (n=1; OR 18.7) associated with wound dehiscence
Obesity and Body Contouring
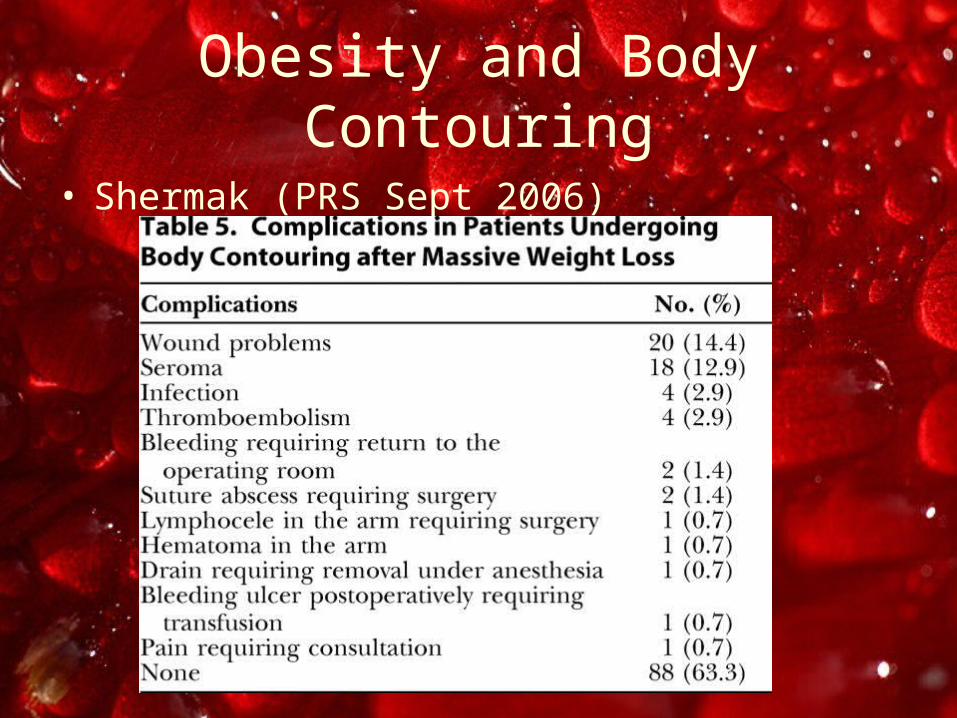
• Shermak (PRS Sept 2006)
Obesity and Body Contouring
Summary
• Significant increase in incidence of local wound complications
• Some evidence that incidence of local complications in body contouring operations remain unchanged despite weight loss.
Obesity in Plastic Surgery
Conclusions
• Increase in risk of general and local complications following surgery
• Protocols are required in managing these patients who present for elective plastic and reconstructive surgery.